Embed Size (px)
Citation preview

© The Children's Mercy Hospital, 2014. 11/14
In Acutely Ill Infants in a Level IV NICU
Laurel Willig, MD, MS
Diagnostic and Clinical Utility of Rapid Genome Sequencing

© The Children's Mercy Hospital, 2014. 03/14
2
© The Children's Mercy Hospital, 2014. 11/14
Disclosures
Laurel Willig, MD has documented no financial relationships to disclose or conflicts of interest to resolve.

© The Children's Mercy Hospital, 2014. 11/14
For disorders currently screened for in newborns, how can genomic sequencing replicate or augment known newborn screening results?
What knowledge about conditions not currently screened for in newborns could genomic sequencing of newborns provide?
What additional clinical information could be learned from genomic sequencing relevant to the clinical care of newborns?
Must address one or more of the following:
A. B. C.
NSIGHT U19

© The Children's Mercy Hospital, 2014. 03/14
4
© The Children's Mercy Hospital, 2014. 11/14
Components
Component 1: Data Acquisition and Analysis
Component 2: Clinical research to advance understanding of specific disorders identifiable in the newborn period using DNA technology
Component 3: Ethical, legal and social implications of genomic sequencing in newborns

© The Children's Mercy Hospital, 2014. 11/14
Members of the NSIGHT Program
• Robert Green, M.D., and Alan Beggs, Ph.D. Brigham and Women’s Hospital, Boston, MA NICU and healthy newborns, 240 exomes, data sharing, return of results
• Stephen Kingsmore, MB, ChB, BAO, DSc, FRCPath Children’s Mercy Hospital, Kansas City, MO NICU, 1000 patients, return of results
• Robert Nussbaum, M.D. (Jennifer Puck, M.D.) University of California, San Francisco, CA NBS, exome sequencing, return of results
• Cynthia Powell, M.D., M.S., and Jonathan Berg, M.D., Ph.D. University of North Carolina at Chapel Hill, NC NBS, 400 exomes, return of result options

© The Children's Mercy Hospital, 2014. 03/14
6
© The Children's Mercy Hospital, 2014. 11/14
50-hour STAT-Seq
• Identify patient who may benefit • Parental consent, blood sample
4.5 h • Sonication/Library Prep • Clinical finding entry: SSAGA
25.5h • HiSeq 2500 2x100bp x 140Gbp
17h • Secondary analysis: GSNAP, GATK • Tertiary analysis: RUNES
0.5+h • VIKING-assisted interpretation • Provisional report

© The Children's Mercy Hospital, 2014. 03/14
7
© The Children's Mercy Hospital, 2014. 11/14
Rapid Whole Genome Testing
Initial proof of concept was on 7 proband parent trios
Cost: ~$6000 per genome
Saunders et al. Sci Transl Med 4; 154ra135 2012

© The Children's Mercy Hospital, 2014. 03/14
8
© The Children's Mercy Hospital, 2014. 11/14
STATseq Application

© The Children's Mercy Hospital, 2014. 03/14
9
© The Children's Mercy Hospital, 2014. 11/14
Level II – IV NICU Admissions
•14.4% of newborns
•2% Level IV
•49.1% were preterm •Average hospital stay = 13.2 days •Average hospital charge = $76,000 •Overall mortality in the CMH NICU was 4% (23 deaths in 563 neonates of gestational age >36 weeks admitted in 2013)
© The Children's Mercy Hospital, 2014. 03/14
10
© The Children's Mercy Hospital, 2014. 11/14
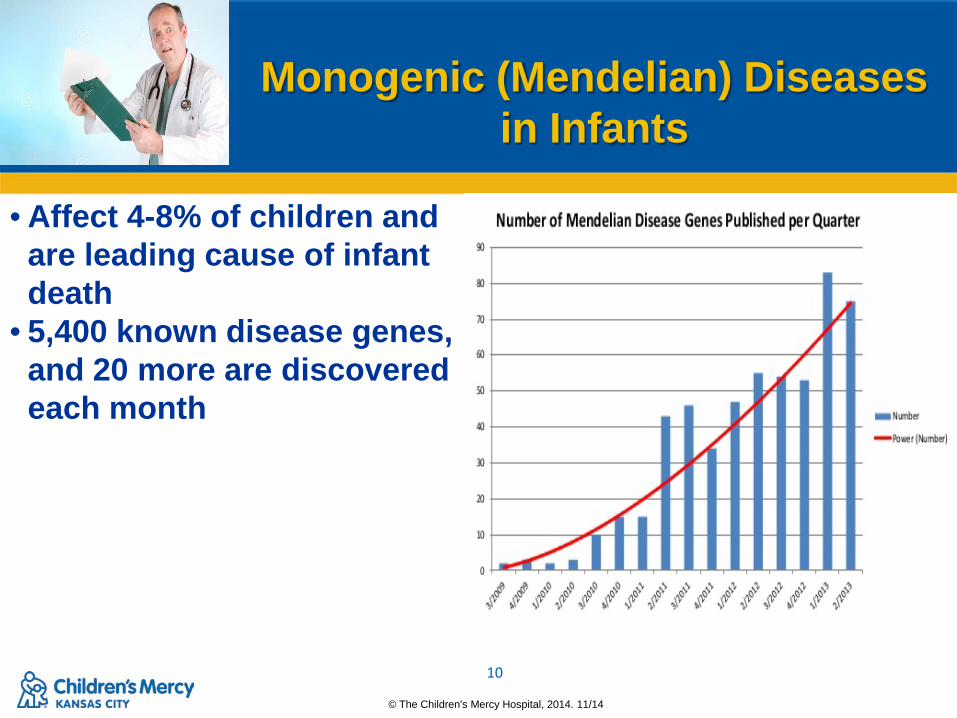
Monogenic (Mendelian) Diseases
in Infants • Affect 4-8% of children and
are leading cause of infant death
• 5,400 known disease genes, and 20 more are discovered each month

© The Children's Mercy Hospital, 2014. 03/14
11
© The Children's Mercy Hospital, 2014. 11/14
Infant Genetic Disease Diagnostic Complexity
Early in disease progression = incomplete symptoms Early in development
– Stereotyped adaptation to challenges to homeostasis Genocopies/genetic heterogeneity
– Several genes cause same “disease” Poorly defined clinical heterogeneity Phenocopies Early diagnosis = optimal outcome, prevention of
unplanned recurrence

Eligible infants N=49
Excluded infants N=14 Reasons: Age >4 months; patient
deceased at the time of enrollment; patient enrolled at outside institution
STATseq diagnosis N=20 of 35 (57%)
No STATseq diagnosis N=15 of 35 (43%)
Target condition present N=20
Target condition absent
N=0
Target condition present
N=1
Target condition absent N=14
STATseq (Index Test)
N=35
Results: November 2011 – October 2014
57% molecular diagnosis rate in STATseq group, 9% diagnostic rate using standard testing

© The Children's Mercy Hospital, 2014. 03/14
13
© The Children's Mercy Hospital, 2014. 11/14
Multisystem Congenital Anomalies
26%
Neurologic 20%
Cardiac/Heterotaxy 14%
Hydrops/Pleural Effusion
11%
Metabolic (inc. Hypoglycemia)
11%
Renal 3%
Arthrogryposis 6%
Respiratory 3%
Hepatic 3%
Dermatologic 3%
Phenotypic Distribution of Patients
© The Children's Mercy Hospital, 2014. 03/14
14
© The Children's Mercy Hospital, 2014. 11/14
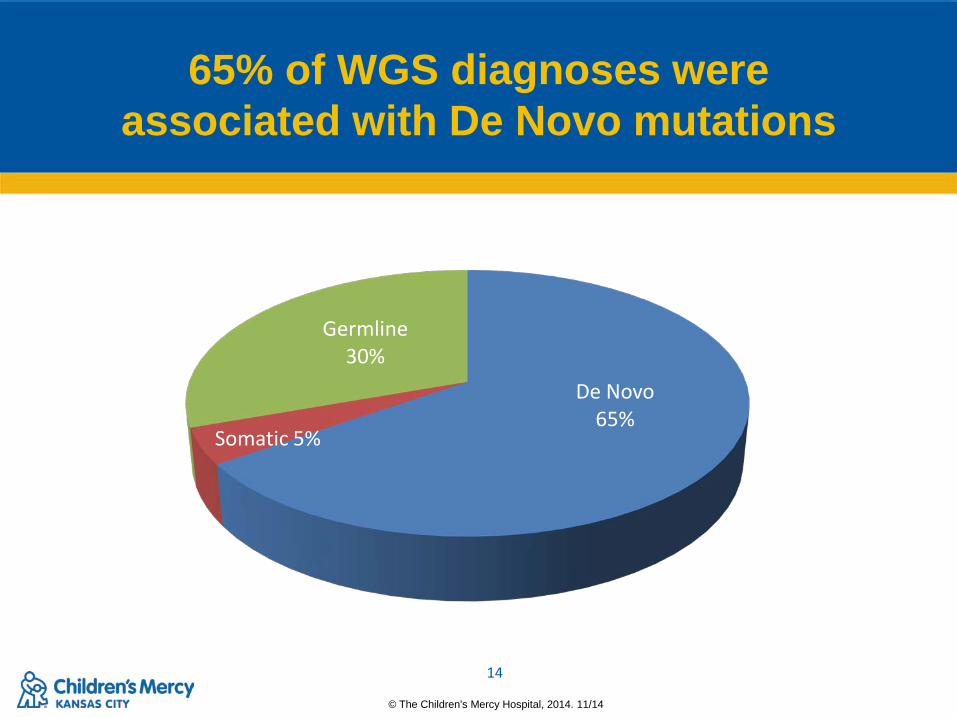
65% of WGS diagnoses were associated with De Novo mutations
De Novo 65%
Somatic 5%
Germline 30%

© The Children's Mercy Hospital, 2014. 03/14
15
© The Children's Mercy Hospital, 2014. 11/14
Important Time Points
Time Points Days (Range)
Age at enrollment 26
Median time from enrollment to variant analysis 5 (3-153)
Median time to clinically confirmed diagnosis 9 (5-912)
Average age at death 46 (16-100)
© The Children's Mercy Hospital, 2014. 03/14
16
© The Children's Mercy Hospital, 2014. 11/14
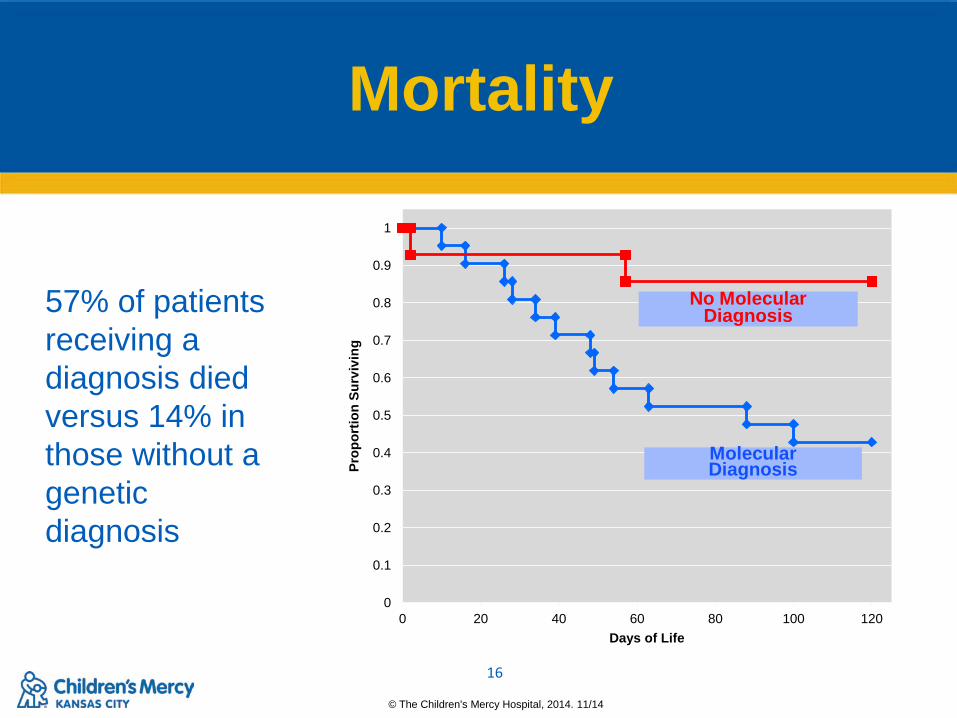
Mortality
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 20 40 60 80 100 120
Prop
ortio
n Su
rviv
ing
Days of Life
Molecular Diagnosis
No Molecular Diagnosis 57% of patients
receiving a diagnosis died versus 14% in those without a genetic diagnosis

© The Children's Mercy Hospital, 2014. 03/14
17
© The Children's Mercy Hospital, 2014. 11/14
Acute Clinical Impact
Clinical utility in 65%
Palliative care initiated in 33%
Other types of changes: medication, dietary, consults, imaging, genetic counseling, procedure performed
Diagnosis led to a positive clinical change in 20%

© The Children's Mercy Hospital, 2014. 03/14
18
© The Children's Mercy Hospital, 2014. 11/14
Framework
- Largest case series published to date
- Relatively quick diagnostic rate
- Huge selection bias - Unblinded with no set standard
testing - Survey data for clinical impact - No long term follow up with families
Strengths Weaknesses
Take home points - High diagnostic rate - High 120 day mortality rate - Reported affect on clinical management

© The Children's Mercy Hospital, 2014. 03/14
19
© The Children's Mercy Hospital, 2014. 11/14
6th Grade Perspective

© The Children's Mercy Hospital, 2014. 03/14
20
© The Children's Mercy Hospital, 2014. 11/14
Clinical Study Aims
Examine risks and benefits of rapid genomic sequencing in the NICU population.
Does STAT-Seq change the clinical care of newborns in the NICU?
– 28-day definitive diagnostic yield of STAT-Seq vs. standard testing
– Time to definitive diagnosis of WGS vs. standard tests
– Physician perception of change in clinical management in WGS-Dx vs. standard tests
– Surrogate measures of objective change in clinical management in WGS-Dx vs. standard tests

© The Children's Mercy Hospital, 2014. 03/14
21
© The Children's Mercy Hospital, 2014. 11/14
Social and Ethical Study Aims
Describe: – clinicians’ and parents’ perceptions of value of STAT-seq in ill
neonates
– the quality of communication of STAT-seq results
– expectations for STAT-seq in the context of clinical outcome data collected under Component 2
Is STAT-Seq viewed as beneficial, harmful, or immaterial – What factors influence these perceptions
How do these perceptions change pretest to post-test and at 12 month follow up

© The Children's Mercy Hospital, 2014. 03/14
22
© The Children's Mercy Hospital, 2014. 11/14
Initial Study Visit Plan
Consent/Initial Visit
Genome Consult/Consent
Blinded randomization
Blood draw
Refusal Assessment
Pretest Questionnaires
Parent Questionnaires
Clinician Questionnaires
Return of Results to Clinician
Phone conference or
care conference with neonatal attending to
discuss results/treatment
decisions
Return of Results to
Family
Patient care team to return findings
to families. Genome care
team present if requested.
72 Hours Post Test Results
Parent Questionnaires
Clinician Questionnaires
12 Months Post Results
Patient questionnaires
and medical follow up

© The Children's Mercy Hospital, 2014. 03/14
23
© The Children's Mercy Hospital, 2014. 11/14
Support: Children’s Mercy Hospital
Marion Merrell Dow Foundation William T. Kemper Foundation Pat &Gil Clements Foundation
Claire Giannini Foundation Black & Veatch
NICHD NHGRI NIDDK
Illumina
Stephen F. Kingsmore MB ChB BAO DSc FRCPath
Nhu Bui Jack Curran Elena Repnikova PhD
FACMG Carol Saunders PhD FACMG Isabelle Thiffault PhD Lee Zellmer CGC Sultan Habeebu MD FACMG Angela Newton Adam Walter John Lesko Emily Farrow PhD CGC Margaret Gibson Kyle Harris Lisa Krivohlavek Melanie Patterson
Suzanne Herd Julie Cakici RN Josh Petrikin MD Laurie Smith MD PhD Sarah Soden MD Erin Guest MD Shane Corder Tyler Hullinger Neil Miller Aaron Noll Greyson Twist Byunggil Yoo
Thank You Questions





























