Embed Size (px)
Citation preview

AJR:195, September 2010 671
it is easy to implement and process, without the need for contrast agents. Apparent diffu-sion coefficient (ADC) has been shown to be a promising marker of fibrosis and cirrhosis by several independent investigators [3–7]. The ADC of livers with moderate or advanced fi-brosis and cirrhosis has been reported to be lower than that of normal livers or livers with mild fibrosis across these multiple studies, al-though reported ADC values vary between studies, partly because of differences in ac-quisition parameters. A hurdle to the wide-spread clinical application of DWI lies in the lack of standardization of parameters and re-producibility of ADC measurements, with reported interscanner and intrascanner vari-ability of approximately 5–15% [11–13]. The variability in reported ADC measurements is further complicated by the use of different b values and acquisition methods based on breath-hold, free-breathing, or respiratory-
Diagnosis of Liver Fibrosis and Cirrhosis With Diffusion-Weighted Imaging: Value of Normalized Apparent Diffusion Coefficient Using the Spleen as Reference Organ
Richard K. G. Do1
Hersh Chandanara1
Ely Felker2
Cristina H. Hajdu3
James S. Babb1
Danny Kim1
Bachir Taouli1,4
Do RKG, Chandanara H, Felker E, et al.
Gastrointest ina l Imaging • Or ig ina l Research
AJR 2010; 195:671–676
0361–803X/10/1953–671
© American Roentgen Ray Society
Accurate staging of liver fibrosis—commonly determined by liver biopsy—is critical because it de-termines the indication of antivi-
ral treatment and prognosis of patients with chronic viral hepatitis. For example, patients with cirrhosis are at higher risk of end-stage liver disease, portal hypertension, and hepa-tocellular carcinoma and are less likely to re-spond to antiviral therapy [1, 2]. However, liver biopsy is relatively invasive, limited by sample size, and difficult to repeat. Thus, noninvasive tools to assess the degree of fi-brosis of the whole liver are urgently needed. Several noninvasive MRI techniques have been investigated for the diagnosis of liver fi-brosis and cirrhosis, including diffusion-weighted imaging (DWI) [3–7], MR elastog-raphy [8], and perfusion-weighted imaging [9, 10]. DWI is a particularly appealing meth-od for the diagnosis of liver fibrosis because
Keywords: apparent diffusion coefficient, cirrhosis, diffusion-weighted MRI, liver fibrosis, MRI
DOI:10.2214/AJR.09.3448
Received August 5, 2009; accepted after revision February 15, 2010.
Presented at the 2009 ISMRM Annual Meeting, Honolulu, HI.
1Department of Radiology, New York University Langone Medical Center, New York, NY.
2School of Medicine, New York University Langone Medical Center, New York, NY.
3Department of Pathology, New York University Langone Medical Center, New York, NY.
4Present address: Department of Radiology, Mount Sinai Medical Center, One Gustave Levy Pl., Box 1234, New York, NY 10029. Address correspondence to B. Taouli ([email protected]).
OBJECTIVE. The purpose of this study is to compare the diagnostic accuracy of liver ap-parent diffusion coefficient (ADC) versus normalized liver ADC using the spleen as a refer-ence organ for the diagnosis of liver fibrosis and cirrhosis.
MATERIALS AND METHODS. Fifty-six patients, 34 with liver disease and 22 con-trol subjects, were assessed with breath-hold single-shot echo-planar diffusion-weighted im-aging using b values of 0, 50, and 500 s/mm2. Liver ADC and normalized liver ADC (defined as the ratio of liver ADC to spleen ADC) were compared between patients stratified by fibro-sis stage. Receiver operating characteristic (ROC) analysis was used to determine the perfor-mance of ADC and normalized liver ADC for prediction of liver fibrosis and cirrhosis. Re-producibility was assessed by measuring coefficient of variation (n = 7).
RESULTS. Liver ADC failed to distinguish individual stages of fibrosis, except between stages 0 and 4. There were significant differences in normalized liver ADC between control livers and intermediate stages of fibrosis (stages 2–3) and cirrhosis (stage 4) and between stages 1 and 4, and there was a trend toward significance between stages 0 and 1 (p = 0.051) and stages 1 and 3 (p = 0.06). ROC analysis showed that normalized liver ADC was superior to liver ADC for detection of stage ≥ 2 (area under the ROC curve, 0.864 vs 0.655; p = 0.013) and stage ≥3 (0.805 vs 0.689; p = 0.015), without a difference for diagnosing cirrhosis (0.935 vs 0.720; p = 0.185). Normalized liver ADC had higher reproducibility than ADC (mean co-efficient of variation, 3.5% vs 12.6%).
CONCLUSION. Our results suggest that normalizing liver ADC with spleen ADC im-proves diagnostic accuracy for detection of liver fibrosis and cirrhosis when using breath-hold diffusion-weighted imaging, with better reproducibility.
Do et al.Diffusion-Weighted MRI of Liver Fibrosis and Cirrhosis
Gastrointestinal ImagingOriginal Research
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by U
nive
rsity
of
Iow
a L
ibra
ries
on
09/2
8/14
fro
m I
P ad
dres
s 12
8.25
5.6.
125.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

672 AJR:195, September 2010
Do et al.
triggered techniques, which can affect ADC quantification [14–18].
Normalization of ADC using a reference or-gan that remains relatively constant across pa-tients or systems may help reduce variability in ADC calculations. For instance, a recent study showed that normalized ADC (using the spleen) appeared to decrease variability of ADC on the basis of choice of b values for benign and malig-nant liver lesions [19]. The spleen may be an ideal reference organ, because it maintains a relatively stable ADC even in the setting of liver disease [20]. Another recent study showed that normalization of pelvic lymph node ADC using renal cortex as a reference helped improve the diagnostic accuracy for detecting metastatic cervical cancer [21]. The objective of this study is to compare the diagnostic accuracy of liver ADC versus normalized liver ADC using the spleen as a reference organ for the diagnosis of liver fibrosis and cirrhosis.
Materials and MethodsPatients and Control Subjects
This HIPAA-compliant retrospective study was performed after obtaining a waiver for informed patient consent from our institutional review board. Inclusion criteria were as follows: patients with chronic liver disease who underwent MRI (which included a specific DWI protocol, as outlined later in this article) between May 25, 2006, and September 19, 2007, and who had histopathologic diagnosis of liver fibrosis or cirrhosis from explant or biopsy within 90 days after the MRI study were eligible. A total of 67 patients were identified. Of these 67 patients, those with a poor-quality DWI resulting from an inability to breath-hold (n = 13), those who had undergone splenectomy (n = 3), and those who had a low signal-to-noise ratio (SNR) on DWI, as described later in the article (n = 17), were excluded.
The final patient population included 34 patients (26 men and eight women; mean age, 57 years; range, 18–72 years). The following causes of liver disease were recorded: chronic hepatitis C (n = 19), chronic hepatitis B (n = 3), primary biliary cirrhosis (n = 3), alcoholism (n = 1), nonalcoholic fatty liver disease (n = 1), α-1 antitrypsin deficiency (n = 1), sclerosing cholangitis (n = 1), sarcoidosis (n = 1), cholestatis (n = 2), and unknown (n = 2).
In addition, 22 control subjects (three men and 19 women; mean age, 52 years; range, 28–72 years) were also included through a database search. Control subjects were matched for age (p = 0.20) but not for sex. These control patients underwent liver MRI (over the same time period, to ensure consistency of DWI sequence parameters) for benign liver lesions. These patients had normal liver function tests, had no history
of hepatitis or diffuse liver disease, and had no liver imaging findings other than hemangiomas or cysts or both. A total of 56 patients (34 with fibrosis or cirrhosis and 22 control subjects) were assessed.
MRI ProtocolAll examinations were performed on one of three
clinical 1.5-T systems (Magnetom Avanto, Sonata, and Symphony, all from Siemens Healthcare). DWI was performed using a single-shot echo-planar imaging (EPI) fat-suppressed sequence in the axial plane, during a single end expiratory breath-hold, using the following parameters: TR/TE, 1,600–3,400/67–82; slice thickness, 8 mm; interslice gap, 1.6 mm; interleaved slice acquisition; field of view, up to 400 mm with 75–80% rectangular field of view; matrix size, up to 192 × 192; parallel imaging factor, 2; 1–4 averages (depending on the system used); b values of 0, 50, and 500 s/mm2; and tridirectional diffusion gradients (with trace image used for analysis). The clinical MRI study also included breath-hold T1-weighted dual-echo in- and-out-of-phase gradient-echo, T2-weighted turbo spin-echo with fat suppression, half-Fourier acquisition single-shot turbo spin-echo (HASTE), and unenhanced and contrast-enhanced 3D T1-weighted gradient-echo (volumetric interpolated breath-hold examination).
ADC QuantificationUsing a commercial workstation (Syngo, Siemens
Healthcare), a single observer placed circular regions of interest (ROIs; measuring 10–20 mm2) to measure mean signal intensity (SI) in the right hepatic lobe and the spleen for each b value, avoiding areas of artifact, vessels, and focal lesions. The spleen was chosen as a reference organ because of its size, which facilitates placement of ROI, and its position relative to the diaphragm similar to the liver. Because of the decreased liver size in patients with cirrhosis, the kidneys were often only partially visualized on
the single-shot EPI images in this study. Therefore, the kidneys could not be used as a reference organ in this study. The paraspinal muscles are variable in size and degree of intramuscular fat and are often overlapped by ghosting artifact with single-shot EPI sequence. A single ROI was placed on four consecutive slices in the right posterior hepatic lobe of liver and the spleen, and SI was averaged. ROI placement varied across patients because of the large individual variability in size of liver from normal to markedly cirrhotic livers. The left hepatic lobe was not assessed because of the potential dephasing artifacts from cardiac motion [22, 23].
A monoexponential fit was performed to calculate liver and spleen ADCs on the basis of ln(SI) as a function of b value, using all b values. Normalized liver ADC was calculated as the ratio of liver ADC to spleen ADC.
In addition, the estimated liver SNR was calculated on images obtained with a b value of 500 s/mm2, by dividing the mean liver SI by the mean noise SI (average of four ROIs). Because low SNR can artificially decrease ADCs [24], 17 patients with low SNRs (≤ 2) were excluded.
Histopathologic EvaluationOf the patients included in the final analysis, 19
underwent liver transplantation for end-stage liver failure, and 15 underwent percutaneous liver biopsy (mean delay, 32 days; range, 0–85 days). Liver fibrosis stage was retrospectively evaluated by an experienced hepatopathologist using the Batts-Ludwig classification [25]. This scoring system has a 5-point scale for staging: stage 0, no fibrosis; stage 1, portal fibrosis; stage 2, periportal fibrosis; stage 3, septal fibrosis; and stage 4, cirrhosis.
Statistical AnalysisSAS version 9.0 was used for statistical com-
putations. Liver and spleen ADCs were compared
TABLE 1: Liver and Spleen Apparent Diffusion Coefficients (ADCs) and Normalized Liver ADC in Patients Stratified by Fibrosis Stage
Fibrosis Stage (No. of Patients)
Liver ADC (× 10−3 mm2/s)
Spleen ADC (× 10−3 mm2/s) Normalized Liver ADC
0 (n = 22) 1.79 ± 0.32 1.18 ± 0.22 1.54 ± 0.20
1 (n = 4) 1.60 ± 0.23 1.30 ± 0.41 1.28 ± 0.23
2 (n = 5) 1.65 ± 0.23 1.31 ± 0.34 1.31 ± 0.25
3 (n = 4) 1.75 ± 0.20 1.53 ± 0.25 1.17 ± 0.20
4 (n = 21) 1.55 ± 0.29 1.32 ± 0.36 1.20 ± 0.16
0–1 (n = 26) 1.76 ± 0.31 1.20 ± 0.25 1.50 ± 0.22
2–4 (n = 30) 1.59 ± 0.28 1.34 ± 0.70 1.22 ± 0.18
0–2 (n = 31) 1.74 ± 0.30 1.21 ± 0.27 1.47 ± 0.23
3–4 (n = 25) 1.58 ± 0.29 1.35 ± 1.44 1.20 ± 0.16
Note—Data are mean ± SD. Normalized liver ADC is defined as ratio of liver ADC to spleen ADC.
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by U
nive
rsity
of
Iow
a L
ibra
ries
on
09/2
8/14
fro
m I
P ad
dres
s 12
8.25
5.6.
125.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

AJR:195, September 2010 673
Diffusion-Weighted MRI of Liver Fibrosis and Cirrhosis
with a nonparametric paired Wilcoxon’s test. Liver and spleen ADCs and normalized liver ADCs were compared between patients stratified by fibrosis stage using a nonparametric Mann-Whitney test. Differences in ADC values were considered to be statistically significant when p < 0.05. Liver ADCs, normalized liver ADCs, and spleen ADCs were correlated with fibrosis scores using the Spearman’s rank correlation coefficient. Receiver operating characteristic (ROC) curve analysis was used to determine the area under the ROC curve (AUC), and the threshold ADC or normalized liver ADC was used to maximize the average of sensitivity and specificity and to provide the highest overall accuracy to distinguish between different stages of fibrosis. To determine the reproducibility of liver ADC and normalized liver ADC values, the coefficient of variation (CV) was calculated as the SD of ADC divided by the mean ADC from two paired consecutive MR studies (n = 7).
ResultsHistopathologic Results
The following fibrosis stage distribution was observed: stage 0 (n = 22, all control subjects were assumed to have no fibrosis), stage 1 (n = 4), stage 2 (n = 5), stage 3 (n = 4), and stage 4 (cirrhosis, n = 21).
Liver and Spleen ADCs and Normalized Liver ADCs
Spleen ADC was significantly lower than liver ADC for all patients (1.28 ± 0.31 vs 1.67 ±
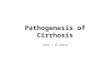
0.30 × 10−3 mm2/s; p < 0.0001 using a paired Wilcoxon’s test), as described elsewhere [23]. Compared with control subjects, patients with cirrhosis had significantly lower liver ADCs and normalized liver ADCs (Tables 1 and 2). Liver ADC failed to distinguish different stag-es of fibrosis, except between stages 0 and 4. Normalized liver ADC distinguished between individual groups of fibrosis (Fig. 1; Table 2), with significant differences between control subjects and intermediate stages of fibrosis (stages 2 and 3) and a trend toward signifi-cance between stages 0 and 1. There was also a significant difference between stages 1 and 4 and a trend toward significance between stages 0 and 3. There were no differences between stages 1 and 2, stages 2 and 3, and stages 3 and 4. There were significant differences between stages 0–1 and 2–4 using both ADC and nor-malized liver ADC. There were significant differences between stages 0–2 and 3–4 using normalized liver ADC and a trend toward significance using ADC.
Spleen ADC did not vary with the degree of fibrosis, with no significant differences when comparing different groups of patients strati-fied by fibrosis stage (p = 0.1328–0.9456), ex-cept between stages 0 and 3 (stage 3 patients had higher spleen ADC; p = 0.033).
There was a statistically significant mod-erate correlation between fibrosis stage and normalized liver ADC (Spearman’s rank correlation coefficient, r = −0.67; p < 0.0001)
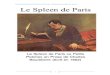
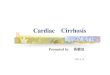
and a weak significant correlation with ADC (r = −0.33; p = 0.016). On the other hand, there was no correlation between spleen ADC and stage of fibrosis (r = 0.226; p = 0.093). The utility of normalized liver ADC over liver ADC is illustrated in two cases: a patient with normal liver and a patient with cirrhosis (Fig. 2). We observed that patients with a high liver ADC tended to have a high-er spleen ADC as well, with a significant positive correlation between liver and spleen ADCs (r = 0.67; p < 0.0001) (Fig. 3).
ADC and Normalized Liver ADC Reproducibility
In seven patients with cirrhosis who un-derwent repeat MRI studies (mean delay, 101 days; range, 74–153 days) to assess reproduc-ibility, normalized liver ADC showed high-er reproducibility, with a lower CV (mean, 3.5%, range 0.4–6.5%) than liver ADC (mean, 12.6%, range 0.1–31.7%).
ROC AnalysisROC analysis revealed higher perfor-
mance using normalized liver ADC com-pared with liver ADC, with higher AUC, sensitivity, and specificity for detection of cirrhosis (stage 0 vs 4 and stages 0–3 vs 4), moderate-to-advanced fibrosis (stages 2–4), and advanced fibrosis and cirrhosis (stages 3–4), reaching significance for all compari-sons except for diagnosis of stage 4 (cirrho-sis) (Fig. 4; Table 3).
DiscussionIn this study, we showed improved perfor-
mance of DWI by normalizing liver ADC with spleen ADC, with excellent sensitivity and specificity for the detection of moderate or advanced fibrosis and cirrhosis among our study group. Our data show higher liver ADCs than previously reported for normal and cirrhotic liver. Prior reported mean ADCs for normal and cirrhotic livers are variable, depending on the combination of b values used. For example, a prior study [5] reported mean liver ADCs for stage 0 of 1.60 ± 0.18 × 10−3 mm2/s (compared with 1.79 ± 0.32 × 10−3 mm2/s in the present study) and 1.22 ± 0.15 × 10−3 mm2/s (compared with 1.55 ± 0.29 × 10−3 mm2/s in the present study) for b values of 0 and 500 s/mm2, respectively. Girometti et al. [6] reported liver ADCs of 1.14 × 10−3 mm2/s in cirrhotic liver when using b values of 0, 150, 250, and 400 s/mm2 and ADCs of 0.91 × 10−3 mm2/s when using b values of 600 and 800 s/mm2. The higher ADC for both normal
TABLE 2: Apparent Diffusion Coefficient (ADC) Comparisons Among Patients Stratified by Fibrosis Stage
Fibrosis Stage Comparison Liver ADC Normalized Liver ADC
Stage 0 vs 1 0.303 0.051
Stage 0 vs 2 0.365 0.046
Stage 0 vs 3 0.972 0.005a
Stage 0 vs 4 0.027 < 0.0001a
Stage 1 vs 2 0.903 0.710
Stage 1 vs 3 1.0 0.060
Stage 1 vs 4 0.208 0.011
Stage 2 vs 3 0.624 0.327
Stage 2 vs 4 0.435 0.229
Stage 3 vs 4 0.208 0.739
Stages 0–1 vs 2–4 0.047 < 0.0001a
Stages 0–2 vs 3–4 0.0548 < 0.0001a
Stages 0–3 vs 4 0.0191 0.0002a
Note—Data are p values calculated by use of the Mann-Whitney test. Significant p values < 0.05 are in bold type. There were no significant differences when comparing spleen ADC between different groups of patients (p = 0.1328–0.9456), except between stages 0 and 3 (stage 3 patients had higher spleen ADC; p = 0.033). Normalized liver ADC is defined as ratio of liver ADC to spleen ADC.
aDenotes significance after Bonferroni correction.
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by U
nive
rsity
of
Iow
a L
ibra
ries
on
09/2
8/14
fro
m I
P ad
dres
s 12
8.25
5.6.
125.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

674 AJR:195, September 2010
Do et al.
and fibrotic or cirrhotic livers in the present study may be explained by the use of an addi-tional b value of 50 s/mm2, which may in-crease the ADCs as a result of contamination from microcapillary perfusion [26], and by the exclusion of patients with low SNR on DWI, because low SNR can artificially lower ADC [24]. The contribution of low SNR to ADC has not been addressed in prior studies
examining the role of DWI in diagnosing liv-er fibrosis, possibly because of the difficulty in accurately measuring SNR when using an EPI sequence with parallel imaging [27].
Prior diffusion studies have reported AUC values of 0.783–0.790 for the detection of liv-er fibrosis stage ≥ 2 [4, 5, 7], 0.717–0.92 for the detection of fibrosis stage ≥ 3 [4, 5, 7], and 0.73–0.93 [6] for the detection of cirrhosis
using ADC. Our current results showed AUC values of 0.655 for detection of stage ≥ 2, 0.689 for stage ≥ 3, and 0.720 for cirrhosis using liv-er ADC, compared with 0.864 for detection of stage ≥ 2, 0.805 for stage ≥ 3, and 0.935 for cirrhosis using normalized liver ADC. Of note, the AUC for diagnosis of cirrhosis with normalized liver ADC (0.935) in our study was equivalent to that reported by Giromet-ti et al. [6], with the difference that the latter study (using b values of 0, 150, 250, and 400 s/mm2) included only a population of patients with cirrhosis and control subjects, whereas we included patients with a full spectrum of liver disease. The underperformance of liv-er ADC in our study compared with these prior studies may be because our study was retrospective and used different systems, as opposed to prior studies by Lewin et al. [4], Taouli et al. [5, 7], and Girometti et al. [6]. We used a breath-hold clinical sequence, without the use of free breathing, respira-tory triggering, or pulse trigger. For exam-ple, two prior studies [5, 7] used breath-hold single-shot EPI with a pulse-trigger acquisi-tion, which has been shown to improve ADC quantification by decreasing motion artifacts from cardiac pulsation [28]. However, the use of the pulse trigger is impractical in the clinical setting, because it increases the set-up and acquisition times. It is also possible to improve ADC quantification using a re-spiratory-triggered acquisition [18]. In addi-tion, we did not include any healthy volun-teers in our study, because adding healthy volunteers such as in prior studies could ar-tificially improve the diagnostic performance of ADC. The number of excluded patients re-flects the difficulty of using breath-hold sin-gle-shot EPI for liver ADC quantification, us-ing “mainstream” clinical magnets especially using systems with limited gradient strengths (as was the case in one of the three systems used in our study). Image optimization and standardization of acquisition parameters for liver DWI is necessary in future studies [14, 29]. An easy solution is to use ADC normal-ization when using a breath-hold single-shot EPI acquisition to improve the performance of DWI, with an AUC equivalent to or higher than those used in prior studies.
We acknowledge that the current results are still inferior to the reported results of MR elastography for detection of stages ≥ 2 and ≥ 3 (0.994 and 0.985, respectively), although our results are comparable for detecting cirrhosis (AUC, 0.998 using MR elastography) [8]. It is possible that, in a prospective study with well-
2.82.62.4
2.22.01.81.6
1.41.21.0
0−1 2−4Fibrosis Stage
Liv
er A
DC
2.82.62.4
2.22.01.81.6
1.41.21.0
0−2 3−4Fibrosis Stage
Liv
er A
DC
2.82.62.4
2.22.01.81.6
1.41.21.0
0−3 4Fibrosis Stage
Liv
er A
DC
2.0
1.8
1.6
1.4
1.2
1.0
0−1
*
2−4Fibrosis Stage
Liv
er n
AD
C
2.0
1.8
1.6
1.4
1.2
1.0
0−2
*3−4
Fibrosis Stage
Liv
er n
AD
C
2.0
1.8
1.6
1.4
1.2
1.0
0−3
**
*
4Fibrosis Stage
Liv
er n
AD
C
Fig. 1—Box plots showing distribution of liver apparent diffusion coefficient (ADC; left column) and normalized liver ADC (nADC; right column) in patients stratified according to fibrosis stage (stages 0–1 vs 2–4, top row ; stages 0–2 vs 3–4, middle row ; stages 0–3 vs 4, bottom row). Asterisks = outliers.
Fig. 2—Axial single-shot echo-planar diffusion-weighted images for b values of 0 s/mm2 (first column), 50 s/mm2 (second column), and 500 s/mm2 (third column) and apparent diffusion coefficient (ADC) maps (fourth column) in 36-year-old woman with normal liver (top row) and 71-year-old woman with hepatitis C cirrhosis (bottom row). Although liver ADC was higher in cirrhotic liver than in normal liver (1.67 vs 1.42 × 10−3 mm2/s), normalized liver ADC was lower in cirrhotic liver (1.22 vs 1.64).
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by U
nive
rsity
of
Iow
a L
ibra
ries
on
09/2
8/14
fro
m I
P ad
dres
s 12
8.25
5.6.
125.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

AJR:195, September 2010 675
Diffusion-Weighted MRI of Liver Fibrosis and Cirrhosis
controlled diffusion parameters using better image quality (free-breathing or respiratory-triggered acquisition) [16, 18], a normalized ADC calculation will be more accurate.
The additional potential benefit of ADC normalization—which is important when fol-lowing patients prospectively—is the better reproducibility of normalized liver ADC, with an observed mean CV of 3.5% for normalized liver ADC compared with a CV of 12.6% for absolute ADC in our study and a CV of 12.8% in a recently published study (liver ADC mea-sured in healthy volunteers using free-breath-ing DWI) [11]. ADC normalization has been rarely used outside the brain [19, 21, 30]. Pa-
panikolaou et al. [19] showed that normalized ADC (using the spleen as reference) appeared to decrease variability of ADC of benign and malignant liver lesions according to the choice of b values, but without a benefit for liver lesion characterization. Park et al. [21] assessed the diagnostic value of DWI for the diagnosis of metastatic lymph nodes in cervical cancer and showed improved performance over absolute lymph node ADC when normalizing ADC with renal cortex.
We observed a statistically significant cor-relation between liver and spleen ADCs with our DWI protocol, suggesting that scanner-specific factors may be involved and may ex-
plain improved performance of normalized liver ADC over absolute ADC. Spuriously high liver ADCs have been observed in previ-ous studies and have been attributed to pseudo-anisotropy during respiratory-gated DWI [16, 31]. We hypothesize that the liver and spleen may undergo additional incoherent intravoxel motion unrelated to their intrinsic diffusion or perfusion properties, possibly resulting from patient motion because of their inability to re-main still or to consistently breath-hold. We propose that incoherent motion in the liver is more significant in diffusion-weighted imag-es with high b values, which are acquired to-ward the end of our DWI protocol, when it be-comes increasingly difficult for the patient to remain still or to maintain their end-expirato-ry breath-hold status and when stronger gradi-ents are used that may potentially vibrate the scanner table [32]. Other scanner factors, such as misregistration or slice cross-talk, may also increase ADCs. Thus, the superior accuracy of normalized ADC may be partly explained by the observed correlation between liver ADC and spleen ADC using our breath-hold DWI protocol.
This study has a number of limitations, in-cluding its retrospective nature, heterogeneous patient population with different causes of liv-er disease, limited number of patients who ful-filled our inclusion criteria, especially patients with intermediate stage of fibrosis (n = 13), and lack of patients with stage 0 chronic liver dis-ease at biopsy. Some may criticize our estimate of reproducibility, but we think it is critical to estimate this agreement in even a small number of patients, and the relatively long time interval between studies reinforces the observation of relative stability of the measured parameters, as reported elsewhere [11]. In addition, we con-ducted multiple statistical tests without using a multiple comparison correction (i.e., Bonferro-ni correction); therefore, our significant results may contain type 1 errors and should therefore be replicated before acceptance. Finally, our
1.0
1.2
1.4
1.6
1.8
2.0
2.2
2.4
2.6
2.8
2.21.8Spleen ADC
Liv
er A
DC
2.01.41.21.0 1.60.8
Fig. 3—Correlation between liver and spleen apparent diffusion coefficient (ADC; n = 56). There is a significant positive correlation between liver and spleen ADC (Spearman’s rank correlation coefficient r = 0.67; p < 0.0001).
0
20
40
60
80
100
10080
Stage ≥ 2 Stage ≥ 3
100% − Specificity
Sen
siti
vity
(%
)
60402000
20
40
60
80
100
10080100% − Specificity
Sen
siti
vity
(%
)
6040200
Stage ≥ 40
20
40
60
80
100
10080100% − Specificity
Sen
siti
vity
(%
)
6040200
Fig. 4—Receiver operating characteristic curves for liver apparent diffusion coefficient (ADC; solid line) and normalized liver ADC (dashed line) in distinguishing subset of patients stratified by fibrosis stage (detection of stage ≥ 2, left panel; detection of stage ≥ 3, middle panel; detection of cirrhosis [stage ≥ 4], right panel). Refer to Table 3 for area under the receiver operating characteristic curve values.
TABLE 3: Receiver Operating Characteristic Analysis for Diagnostic Performance of Liver Apparent Diffusion Coefficient (ADC) Versus Normalized Liver ADC for Detection of Fibrosis Stages ≥ 2, ≥ 3, and 4 (Cirrhosis)
Stage
Liver ADC Normalized Liver ADC
pCutoff
(× 10−3 mm2/s) AUC Sensitivity (%) Specificity (%) Cutoff AUC Sensitivity (%) Specificity (%)
2–4 1.68 0.655 67 61 1.41 0.864 90 77 0.013
3–4 1.53 0.689 56 71 1.41 0.805 96 71 0.015
4 1.68 0.720 76 60 1.40 0.935 95 66 0.185
Note—Cutoff refers to optimal cutoff liver ADC or normalized liver ADC (defined as liver ADC divided by spleen ADC) for distinguishing between subgroups with maximum sensitivity and specificity. There was a statistically significant difference between area under the receiver operating characteristic curve (AUC) of ADC and normalized liver ADC for all subset comparisons except for diagnosis of cirrhosis (stage 4).
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by U
nive
rsity
of
Iow
a L
ibra
ries
on
09/2
8/14
fro
m I
P ad
dres
s 12
8.25
5.6.
125.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

676 AJR:195, September 2010
Do et al.
choice of b values (0, 50, and 500 s/mm2) may be affected by perfusion contamination, which is known to affect ADCs in patients with liver cirrhosis [33, 34].
In conclusion, normalized liver ADC, us-ing the spleen as a reference organ, is supe-rior to absolute liver ADC in distinguishing normal from fibrotic livers using breath-hold single-shot EPI DWI. The utility of normal-ized liver ADC as a noninvasive marker for liver fibrosis remains to be shown in further prospective studies using free-breathing or respiratory-triggered diffusion acquisition.
References 1. Kim AI, Saab S. Treatment of hepatitis C. Am J
Med 2005; 118:808–815
2. Yee HS, Currie SL, Darling JM, Wright TL. Man-
agement and treatment of hepatitis C viral infec-
tion: recommendations from the Department of
Veterans Affairs hepatitis C resource center pro-
gram and the National Hepatitis C Program Of-
fice. Am J Gastroenterol 2006; 101:2360–2378
3. Koinuma M, Ohashi I, Hanafusa K, Shibuya H.
Apparent diffusion coefficient measurements with
diffusion-weighted magnetic resonance imaging
for evaluation of hepatic fibrosis. J Magn Reson
Imaging 2005; 22:80–85
4. Lewin M, Poujol-Robert A, Boelle PY, et al. Dif-
fusion-weighted magnetic resonance imaging for
the assessment of fibrosis in chronic hepatitis C.
Hepatology 2007; 46:658–665
5. Taouli B, Tolia AJ, Losada M, et al. Diffusion-
weighted MRI for quantification of liver fibrosis:
preliminary experience. AJR 2007; 189:799–806
6. Girometti R, Furlan A, Esposito G, et al. Relevance
of b-values in evaluating liver fibrosis: a study in
healthy and cirrhotic subjects using two single-shot
spin-echo echo-planar diffusion-weighted sequenc-
es. J Magn Reson Imaging 2008; 28:411–419
7. Taouli B, Chouli M, Martin AJ, Qayyum A, Coakley
FV, Vilgrain V. Chronic hepatitis: role of diffusion-
weighted imaging and diffusion tensor imaging for
the diagnosis of liver fibrosis and inflammation. J
Magn Reson Imaging 2008; 28:89–95
8. Huwart L, Sempoux C, Vicaut E, et al. Magnetic
resonance elastography for the noninvasive staging
of liver fibrosis. Gastroenterology 2008; 135:32–40
9. Annet L, Materne R, Danse E, Jamart J, Hors-
mans Y, Van Beers BE. Hepatic flow parameters
measured with MR imaging and Doppler US: cor-
relations with degree of cirrhosis and portal hy-
pertension. Radiology 2003; 229:409–414
10. Hagiwara M, Rusinek H, Lee VS, et al. Advanced
liver fibrosis: diagnosis with 3D whole-liver per-
fusion MR imaging—initial experience. Radiolo-
gy 2008; 246:926–934
11. Braithwaite AC, Dale BM, Boll DT, Merkle EM.
Short- and midterm reproducibility of apparent
diffusion coefficient measurements at 3.0-T diffu-
sion-weighted imaging of the abdomen. Radiolo-
gy 2009; 250:459–465
12. Sasaki M, Yamada K, Watanabe Y, et al. Variabil-
ity in absolute apparent diffusion coefficient val-
ues across different platforms may be substantial:
a multivendor, multi-institutional comparison
study. Radiology 2008; 249:624–630
13. Koh DM, Blackledge M, Collins DJ, et al. Repro-
ducibility and changes in the apparent diffusion
coefficients of solid tumours treated with com-
bretastatin A4 phosphate and bevacizumab in a
two-centre phase I clinical trial. Eur Radiol 2009;
19:2728–2738
14. Taouli B, Koh DM. Diffusion-weighted MR im-
aging of the liver. Radiology 2010; 254:47–66
15. Kandpal H, Sharma R, Madhusudhan KS, Kapoor
KS. Respiratory-triggered versus breath-hold dif-
fusion-weighted MRI of liver lesions: comparison
of image quality and apparent diffusion coeffi-
cient values. AJR 2009; 192:915–922
16. Kwee TC, Takahara T, Koh DM, Nievelstein RA,
Luijten PR. Comparison and reproducibility of
ADC measurements in breathhold, respiratory
triggered, and free-breathing diffusion-weighted
MR imaging of the liver. J Magn Reson Imaging
2008; 28:1141–1148
17. Nasu K, Kuroki Y, Sekiguchi R, Nawano S. The
effect of simultaneous use of respiratory trigger-
ing in diffusion-weighted imaging of the liver.
Magn Reson Med Sci 2006; 5:129–136
18. Taouli B, Sandberg A, Stemmer A, et al. Diffu-
sion-weighted imaging of the liver: comparison of
navigator triggered and breathhold acquisitions. J
Magn Reson Imaging 2009; 30:561–568
19. Papanikolaou N, Gourtsoyianni S, Yarmenitis S,
Maris T, Gourtsoyiannis N. Comparison between
two-point and four-point methods for quantification
of apparent diffusion coefficient of normal liver pa-
renchyma and focal lesions: value of normalization
with spleen. Eur J Radiol 2010; 73:305–309
20. Kim T, Murakami T, Takahashi S, Hori M, Tsuda
K, Nakamura H. Diffusion-weighted single-shot
echoplanar MR imaging for liver disease. AJR
1999; 173:393–398
21. Park SO, Kim JK, Kim KA, et al. Relative appar-
ent diffusion coefficient: determination of refer-
ence site and validation of benefit for detecting
metastatic lymph nodes in uterine cervical cancer.
J Magn Reson Imaging 2009; 29:383–390
22. Kilickesmez O, Yirik G, Bayramoglu S, Cimilli
T, Aydin S. Non-breath-hold high b-value diffu-
sion-weighted MRI with parallel imaging tech-
nique: apparent diffusion coefficient determina-
tion in normal abdominal organs. Diagn Interv
Radiol 2008; 14:83–87
23. Yoshikawa T, Kawamitsu H, Mitchell DG, et al.
ADC measurement of abdominal organs and le-
sions using parallel imaging technique. AJR 2006;
187:1521–1530
24. Dietrich O, Heiland S, Sartor K. Noise correction
for the exact determination of apparent diffusion
coefficients at low SNR. Magn Reson Med 2001;
45:448–453
25. Batts KP, Ludwig J. Chronic hepatitis: an update
on terminology and reporting. Am J Surg Pathol
1995; 19:1409–1417
26. Le Bihan D, Breton E, Lallemand D, Aubin ML,
Vignaud J, Laval-Jeantet M. Separation of diffu-
sion and perfusion in intravoxel incoherent mo-
tion MR imaging. Radiology 1988; 168:497–505
27. Dietrich O, Raya JG, Reeder SB, Reiser MF,
Schoenberg SO. Measurement of signal-to-noise
ratios in MR images: influence of multichannel
coils, parallel imaging, and reconstruction filters.
J Magn Reson Imaging 2007; 26:375–385
28. Murtz P, Flacke S, Traber F, van den Brink JS,
Gieseke J, Schild HH. Abdomen: diffusion-
weighted MR imaging with pulse-triggered single-
shot sequences. Radiology 2002; 224:258–264
29. Padhani AR, Liu G, Koh DM, et al. Diffusion-
weighted magnetic resonance imaging as a cancer
biomarker: consensus and recommendations.
Neoplasia 2009; 11:102–125
30. Lin G, Ho KC, Wang JJ, et al. Detection of lymph
node metastasis in cervical and uterine cancers by
diffusion-weighted magnetic resonance imaging
at 3T. J Magn Reson Imaging 2008; 28:128–135
31. Nasu K, Kuroki Y, Fujii H, Minami M. Hepatic
pseudo-anisotropy: a specific artifact in hepatic
diffusion-weighted images obtained with respira-
tory triggering. MAGMA 2007; 20:205–211
32. Ogura A, Maeda F, Miyai A, Hayashi K, Hongoh
T. Effect of vibration caused by time-varying
magnetic fields on diffusion-weighted MRI [in
Japanese]. Nippon Hoshasen Gijutsu Gakkai
Zasshi 2006; 62:565–569
33. Luciani A, Vignaud A, Cavet M, et al. Liver cir-
rhosis: intravoxel incoherent motion MR imag-
ing—pilot study. Radiology 2008; 249:891–899
34. Patel J, Sigmund EE, Rusinke H, Oei M, Babbs
JS, Taouli B. Diagnosis of cirrhosis with intra-
voxel incoherent motion diffusion MRI and dy-
namic contrast-enhanced MRI alone and in com-
bination: preliminary experience. J Magn Reson
Imaging 2010; 31:589–600Dow
nloa
ded
from
ww
w.a
jron
line.
org
by U
nive
rsity
of
Iow
a L
ibra
ries
on
09/2
8/14
fro
m I
P ad
dres
s 12
8.25
5.6.
125.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

This article has been cited by:
1. Filip Deckers, Bert De Foer, François Van Mieghem, Thomas Botelberge, Reinhilde Weytjens, Anwar Padhani, MarcPouillon. 2014. Apparent diffusion coefficient measurements as very early predictive markers of response to chemotherapy inhepatic metastasis: A preliminary investigation of reproducibility and diagnostic value. Journal of Magnetic Resonance Imaging40:10.1002/jmri.v40.2, 448-456. [CrossRef]
2. H.J. Wang, M.H. Pui, Y. Guo, S.R. Li, M.J. Liu, J. Guan, X.L. Zhang, Y. Feng. 2014. Value of normalized apparent diffusioncoefficient for estimating histological grade of vesical urothelial carcinoma. Clinical Radiology 69, 727-731. [CrossRef]
3. Y. Hong, Y. Shi, W. Liao, N.J. Klahr, F. Xia, C. Xu, Y. Li, Q. Guo. 2014. Relative ADC measurement for liver fibrosis diagnosisin chronic hepatitis B using spleen/renal cortex as the reference organs at 3 T. Clinical Radiology 69, 581-588. [CrossRef]
4. Fatma Zaiton, Hitham Dawoud, Inas M. El Fiki, Khaled M. Hadhoud. 2014. Diffusion weighted MRI and transient elastographyassessment of liver fibrosis in hepatitis C patients: Validity of non invasive imaging techniques. The Egyptian Journal of Radiologyand Nuclear Medicine 45, 279-287. [CrossRef]
5. Ahmed Abdel Khalek Abdel Razek, Mohamed Khashaba, Ahmed Abdalla, Mohamed Bayomy, Tarek Barakat. 2014. Apparentdiffusion coefficient value of hepatic fibrosis and inflammation in children with chronic hepatitis. La radiologia medica .[CrossRef]
6. Govind B. Chavhan, Zehour AlSabban, Paul S. Babyn. 2014. Diffusion-weighted Imaging in Pediatric Body MR Imaging:Principles, Technique, and Emerging Applications. RadioGraphics 34, E73-E88. [CrossRef]
7. G. Li, P. Xu, X. Pan, H. Qin, Y. Chen. 2014. The effect of age on apparent diffusion coefficient values in normal spleen: Apreliminary study. Clinical Radiology 69, e165-e167. [CrossRef]
8. C.L. Hoad, L. Marciani, S.T. Francis, P.A. GowlandWhole body magnetic resonance imaging (MRI) 266-306. [CrossRef]9. Brian Barry, Karen Buch, Jorge A. Soto, Hernan Jara, Arie Nakhmani, Stephan W. Anderson. 2014. Quantifying liver fibrosis
through the application of texture analysis to diffusion weighted imaging. Magnetic Resonance Imaging 32, 84-90. [CrossRef]10. Anthony Dohan, Philippe Soyer, Youcef Guerrache, Christine Hoeffel, Jean-Philippe Gavini, Rachid Kaci, Mourad Boudiaf.
2014. Focal Nodular Hyperplasia of the Liver. Journal of Computer Assisted Tomography 38, 96-104. [CrossRef]11. Xiao-li Chen, Tian-wu Chen, Xiao-ming Zhang, Zhen-lin Li, Hang Li, Nan-lin Zeng, Hong-jie Tang, Yu Pu, Nan Chen,
Qi Yang, Li Li, Xian-yong Xie, Jiani Hu. 2013. Spleen magnetic resonance diffusion-weighted imaging for quantitativestaging hepatic fibrosis in miniature pigs: An initial study. Hepatology Research 43:10.1111/hepr.2013.43.issue-11, 1231-1240.[CrossRef]
12. Janina Klasen, Rotem Shlomo Lanzman, Hans-Jörg Wittsack, Gerald Kircheis, Julia Schek, Michael Quentin, Gerald Antoch,Dieter Häussinger, Dirk Blondin. 2013. Diffusion-weighted imaging (DWI) of the spleen in patients with liver cirrhosis andportal hypertension. Magnetic Resonance Imaging 31, 1092-1096. [CrossRef]
13. Mona El-Hariri, Tamer F. Taha Ali, Hala I.M. Hussien. 2013. Apparent diffusion coefficient (ADC) in liver fibrosis: Usefulnessof normalized ADC using the spleen as reference organ. The Egyptian Journal of Radiology and Nuclear Medicine 44, 441-451.[CrossRef]
14. P. Soyer, M. Kanematsu, B. Taouli, D.-M. Koh, R. Manfredi, V. Vilgrain, C. Hoeffel, B. Guiu. 2013. Normalisation de l’ADC :une piste de recherche prometteuse pour l’IRM de diffusion abdominale. Journal de Radiologie Diagnostique et Interventionnelle94, 587-590. [CrossRef]
15. M. Barral, D. Sebbag-Sfez, C. Hoeffel, U. Chaput, A. Dohan, C. Eveno, M. Boudiaf, P. Soyer. 2013. Characterization offocal pancreatic lesions using normalized apparent diffusion coefficient at 1.5-Tesla: Preliminary experience. Diagnostic andInterventional Imaging 94, 619-627. [CrossRef]
16. Nicola Galea, Vito Cantisani, Bachir Taouli. 2013. Liver lesion detection and characterization: Role of diffusion-weightedimaging. Journal of Magnetic Resonance Imaging 37, 1260-1276. [CrossRef]
17. M. Barral, D. Sebbag-Sfez, C. Hoeffel, U. Chaput, A. Dohan, C. Eveno, M. Boudiaf, P. Soyer. 2013. Caractérisation des lésionspancréatiques focales par la mesure du coefficient de diffusion apparent en IRM à 1,5 tesla : expérience préliminaire. Journalde Radiologie Diagnostique et Interventionnelle 94, 636-644. [CrossRef]
18. P. Soyer, M. Kanematsu, B. Taouli, D.-M. Koh, R. Manfredi, V. Vilgrain, C. Hoeffel, B. Guiu. 2013. ADC normalization:A promising research track for diffusion-weighted MR imaging of the abdomen. Diagnostic and Interventional Imaging 94,571-573. [CrossRef]
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by U
nive
rsity
of
Iow
a L
ibra
ries
on
09/2
8/14
fro
m I
P ad
dres
s 12
8.25
5.6.
125.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

19. Robin Bülow, Birger Mensel, Peter Meffert, Diego Hernando, Matthias Evert, Jens-Peter Kühn. 2013. Diffusion-weightedmagnetic resonance imaging for staging liver fibrosis is less reliable in the presence of fat and iron. European Radiology 23,1281-1287. [CrossRef]
20. Lijun Guo, Cheng Liu, Weibo Chen, Queenie Chan, Guangbin Wang. 2013. Dual-source parallel RF transmission for diffusion-weighted imaging of the abdomen using different b values: Image quality and apparent diffusion coefficient comparison withconventional single-source transmission. Journal of Magnetic Resonance Imaging 37, 875-885. [CrossRef]
21. Mesude Tosun, Nagihan Inan, Hasan Tahsin Sarisoy, Gur Akansel, Sevtap Gumustas, Yeşim Gürbüz, Ali Demirci. 2013.Diagnostic performance of conventional diffusion weighted imaging and diffusion tensor imaging for the liver fibrosis andinflammation. European Journal of Radiology 82, 203-207. [CrossRef]
22. Chansik An, Sumi Park, Yoon Jung Choi. 2013. Diffusion-Weighted MRI in Intrahepatic Bile Duct Adenoma Arising fromthe Cirrhotic Liver. Korean Journal of Radiology 14, 769. [CrossRef]
23. Hersh Chandarana, Richard K. G. Do, Thais C. Mussi, Jens H. Jensen, Cristina H. Hajdu, James S. Babb, Bachir Taouli.2012. The Effect of Liver Iron Deposition on Hepatic Apparent Diffusion Coefficient Values in Cirrhosis. American Journal ofRoentgenology 199:4, 803-808. [Abstract] [Full Text] [PDF] [PDF Plus]
24. Nikolaos Kartalis, Louiza Loizou, Nick Edsborg, Ralf Segersvärd, Nils Albiin. 2012. Optimising diffusion-weighted MRimaging for demonstrating pancreatic cancer: a comparison of respiratory-triggered, free-breathing and breath-hold techniques.European Radiology 22, 2186-2192. [CrossRef]
25. S. Palmucci, L.A. Mauro, G. Failla, P.V. Foti, P. Milone, N. Sinagra, D. Zerbo, P. Veroux, G.C. Ettorre, M. Veroux. 2012.Magnetic Resonance With Diffusion-Weighted Imaging in the Evaluation of Transplanted Kidneys: Updating Results in 35Patients. Transplantation Proceedings 44, 1884-1888. [CrossRef]
26. Garfield A. Grandison, Paul Angulo. 2012. Can Nash Be Diagnosed, Graded, and Staged Noninvasively?. Clinics in Liver Disease16, 567-585. [CrossRef]
27. Qing-Bing Wang, Hui Zhu, Hai-Ling Liu, Bei Zhang. 2012. Performance of magnetic resonance elastography and diffusion-weighted imaging for the staging of hepatic fibrosis: A meta-analysis. Hepatology 56, 239-247. [CrossRef]
28. David Bonekamp, Susanne Bonekamp, Bernhard Geiger, Ihab R. Kamel. 2012. An Elevated Arterial Enhancement FractionIs Associated With Clinical and Imaging Indices of Liver Fibrosis and Cirrhosis. Journal of Computer Assisted Tomography 36,681-689. [CrossRef]
29. Stephan W. Anderson, Hernan Jara, Al Ozonoff, Michael O'Brien, James A. Hamilton, Jorge A. Soto. 2012. Effect of diseaseprogression on liver apparent diffusion coefficient and T2 values in a murine model of hepatic fibrosis at 11.7 Tesla MRI.Journal of Magnetic Resonance Imaging 35:10.1002/jmri.v35.1, 140-146. [CrossRef]
30. Ashkan A. Malayeri, Riham H. El Khouli, Atif Zaheer, Michael A. Jacobs, Celia P. Corona-Villalobos, Ihab R. Kamel, KatarzynaJ. Macura. 2011. Principles and Applications of Diffusion-weighted Imaging in Cancer Detection, Staging, and TreatmentFollow-up. RadioGraphics 31, 1773-1791. [CrossRef]
31. Mélanie Chiaradia, Laurence Baranes, Frederic Pigneur, Marjan Djabbari, Benhalima Zegai, Pierre Brugières, Pierre Zerbib,Thomas Decaens, Jean-François Deux, Hicham Kobeiter, Alain Rahmouni, Alain Luciani. 2011. Liver magnetic resonancediffusion weighted imaging: 2011 update. Clinics and Research in Hepatology and Gastroenterology 35, 539-548. [CrossRef]
32. S. Palmucci, L.A. Mauro, P. Veroux, G. Failla, P. Milone, G.C. Ettorre, N. Sinagra, G. Giuffrida, D. Zerbo, M. Veroux. 2011.Magnetic Resonance With Diffusion-Weighted Imaging in the Evaluation of Transplanted Kidneys: Preliminary Findings.Transplantation Proceedings 43, 960-966. [CrossRef]
33. Susanne Bonekamp, Michael S. Torbenson, Ihab R. Kamel. 2011. Diffusion-weighted Magnetic Resonance Imaging for theStaging of Liver Fibrosis. Journal of Clinical Gastroenterology 45, 885-892. [CrossRef]
34. Ahmed Ibrahim, Mamdouh Ali, Hala Ghanem, Amriaa Mousa, Tawhida Ghafar. 2011. Simple and rapid detection of livercirrhosis in children by tracking serum IgAtransferrin ratio. Journal of Experimental and Integrative Medicine 117. [CrossRef]
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by U
nive
rsity
of
Iow
a L
ibra
ries
on
09/2
8/14
fro
m I
P ad
dres
s 12
8.25
5.6.
125.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved