Embed Size (px)
Citation preview
Prof David Russell-Jones
Dr Roselle Herring
Centre for Endocrinology,
Diabetes and Research
(CEDAR)
University of Surrey
Diabetic and Metabolic Emergencies

Diabetes is a huge problem
IDF. IDF Diabetes Atlas, 6th edition revision, 2014. www.idf.org/diabetesatlas
Four out of five people with diabetes now live in developing countries
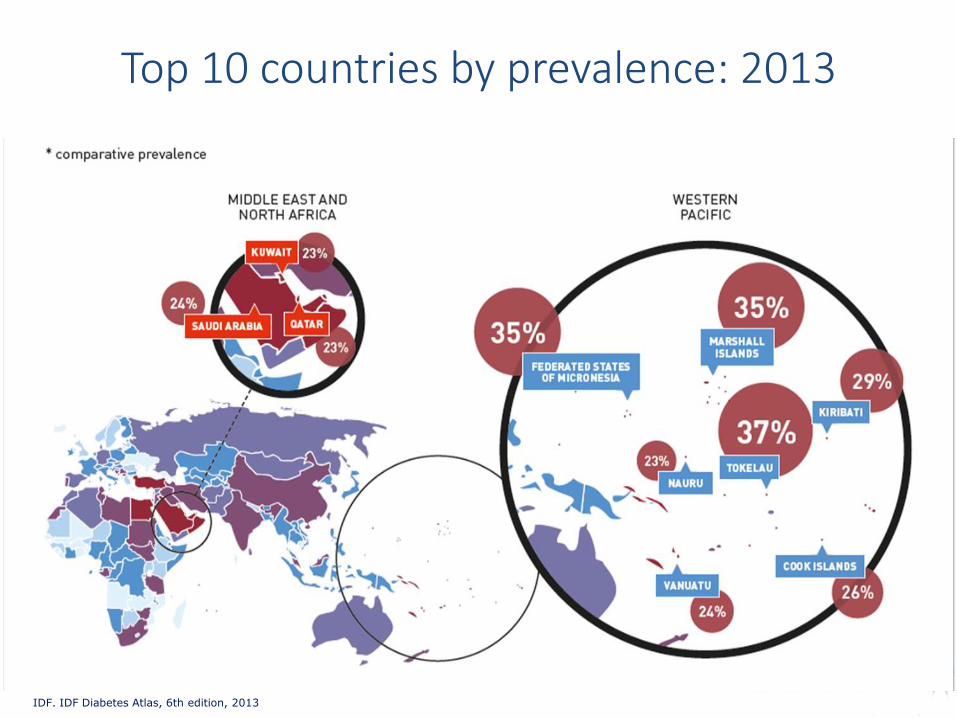
IDF. IDF Diabetes Atlas, 6th edition, 2013
Top 10 countries by prevalence: 2013

• 387 million people have diabetes
• By 2035, this number will rise to 592 million
Diabetes is a huge and growing problem
2014 2035
WORLD
387 million
WORLD
592 million people living with diabetes
Middle East and North Africa 85%
Southeast Asia 64%
South and Central America 55%
Western Pacific 46%
Europe 33%
Africa 93%
53%
North America and Caribbean 30%
IDF. IDF Diabetes Atlas, 6th edition revision, 2014. www.idf.org/diabetesatlas

€1,373 1.3x increase
€1,723
€3,355
2.4x increase
€3,436
2.5x increase
€5,642
4.1x increase
All insured patients
Diabetes, no complications
Diabetes, microvascular complications
Diabetes, macrovascular complications
Diabetes, micro- and macrovascular
complications
Annual costs per patient
Treating type 2 diabetes and its complications is costly
Liebl et al. Dtsch Med Wochenschr 2001;126:585–89 (CODE-2 Study)

The management of adult diabetes services in the NHS - Public Accounts Committee
......“just 16% of people with diabetes have achieved the recommended levels for blood glucose, blood pressure and cholesterol leaving an unacceptably high proportion of people with diabetes at higher risk of developing related complications”......................
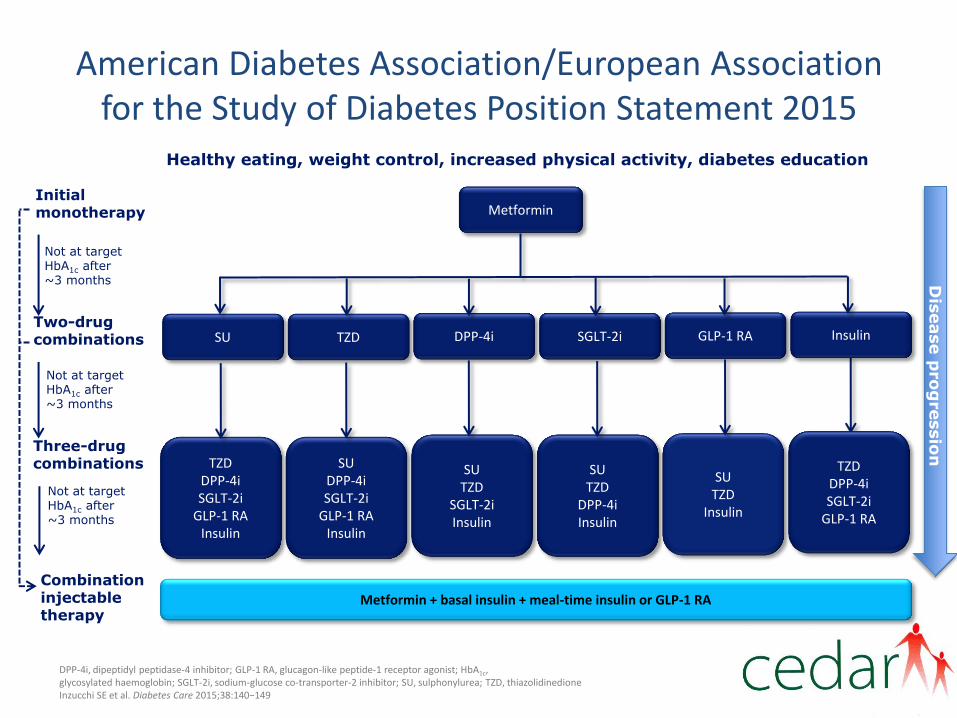
American Diabetes Association/European Association for the Study of Diabetes Position Statement 2015
DPP-4i, dipeptidyl peptidase-4 inhibitor; GLP-1 RA, glucagon-like peptide-1 receptor agonist; HbA1c, glycosylated haemoglobin; SGLT-2i, sodium-glucose co-transporter-2 inhibitor; SU, sulphonylurea; TZD, thiazolidinedione Inzucchi SE et al. Diabetes Care 2015;38:140−149
Healthy eating, weight control, increased physical activity, diabetes education
Not at target HbA1c after ~3 months
Two-drug combinations
Three-drug combinations
Combination injectable therapy
Initial monotherapy
Not at target HbA1c after ~3 months
Not at target HbA1c after ~3 months
GLP-1 RA SGLT-2i DPP-4i TZD SU Insulin
Dis
ease p
ro
gressio
n
Metformin
SU TZD
Insulin
SU TZD
DPP-4i Insulin
SU TZD
SGLT-2i Insulin
SU DPP-4i SGLT-2i
GLP-1 RA Insulin
TZD DPP-4i SGLT-2i
GLP-1 RA Insulin
TZD DPP-4i SGLT-2i
GLP-1 RA
Metformin + basal insulin + meal-time insulin or GLP-1 RA

Mr JW
Mr JW

Presentation
• 66 year old male
• A+E ref: chest pain + vomiting
• HPC:
– Well previous day
– Evening: gradual onset, constant achy chest pain, 9/10 + nausea – similar to angina. Kept awake at night.
– No SOB, clamminess.
– Morning: vomiting: initially clear, then brown
– No abdominal pain, fevers, etc.

Past Medical History
– Type 2 diabetes mellitus
• Diagnosed 10 yrs ago
– Hypertension
– Hypercholestrolaemia
– Angiogram 2006 – NAD
– Ulcerative colitis
Treatment
– Sitagliptin 100mg OD
– Metformin 3.5g BD
– Perindopril 4mg OD
– Simvastatin 10mg OD
– Diclofenac 50mg TDS
– Rabeprazole 20mg OD
– Tamsulosin 400mcg OD
– Cetirizine 10mg OD
– Beclomethazone inhaler BD

Examination
• Looked clapped out
• Retching + vomiting brown fluid
• Persistent pain – despite morphine
• Apyrexial
• BP 142/62, HR 93 regular
• RR 20, O2 sats 100% on 100% O2
• Cardio / resp / abdo unremarkable
• Stool seen in A+E – no blood
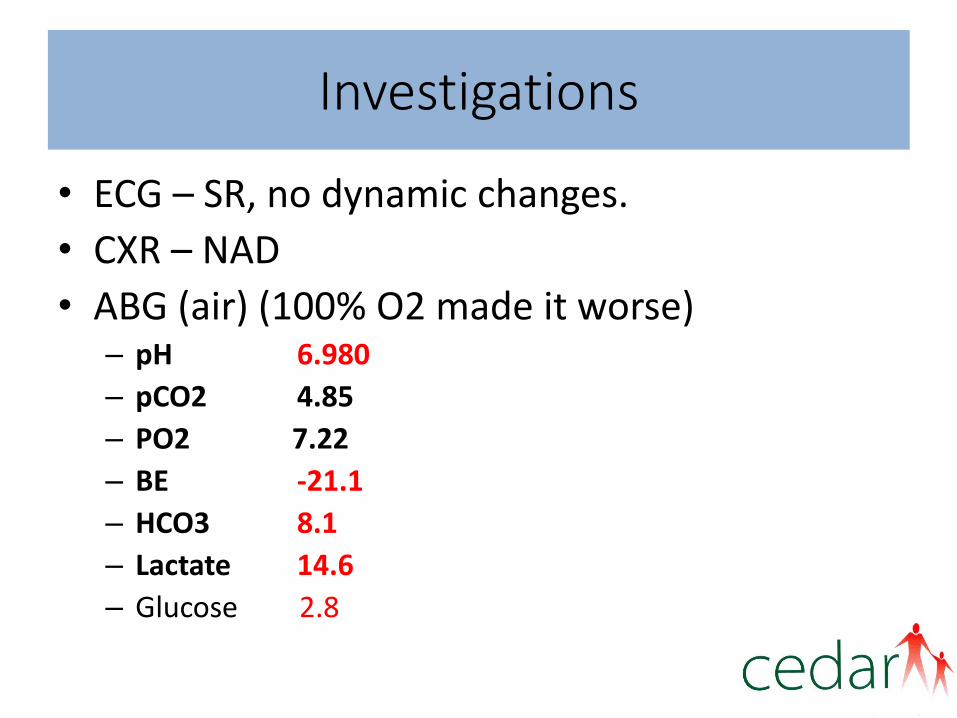
Investigations
• ECG – SR, no dynamic changes.
• CXR – NAD
• ABG (air) (100% O2 made it worse) – pH 6.980
– pCO2 4.85
– PO2 7.22
– BE -21.1
– HCO3 8.1
– Lactate 14.6
– Glucose 2.8

Investigations
• Bloods:
– Na 142, K 6.1,
– Urea 22.2, Creat 420 (123 prev)
– C.Ca 2.59, PO4 2.60, Amylase 60
– Bilirubin 7, ALP 51, ALT 17, Albumin 45
– Hb 12.5, WCC 21.9, neut 17.6 plt 476
– INR 1.1
What is the underlying diagnosis?
A. Sepsis
B. Lactic acidosis 2nd metformin
C. Acute renal failure 2nd NSAID / ACEI / dehydration
D. Ischaemic bowel
E. Gastrointestinal bleed

Management Plan
1) Aggressive fluid resuscitation
2) Careful fluid balance
3) IV co-amoxiclav
4) Urine: MC+S + casts
5) Stop metformin
6) Antiemetics
7) ITU + Surgical r/v

Later
• Surgical r/v - ? Ischaemic gut – happy to watch
• ITU – insulin sliding scale, bicarbonate and haemofiltration
• Discharges after 4/7 to ward
– Urea 9.6, Creat 254, WCC 9.5.
• Ward – careful fluid balance (renal reg), s/c insulin:
• D/c 14/7 after admission.

Anion Gap Acidosis

Metformin

Metformin
• French Lilac plant 1900’s lowered blood sugar
but toxic
• Metformin related shorter duration less toxic 1957
• Phenformin & buformin longer acting and more toxic
• Metformin 1970s europe USA 1995
• Efficacy – Lowers A1c by 1.5%
– UKPDS 36% reduction in mortality
A problem!

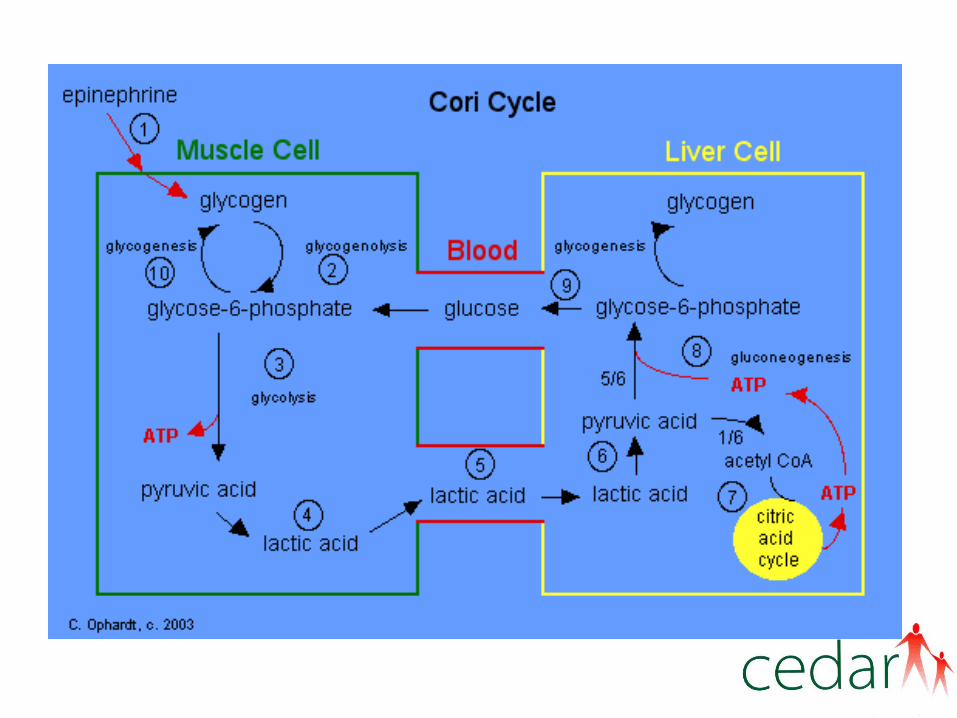
Gerti Cori
Nobel prize 1947

Key points
• Metformin induced Lactic acidosis is rare, but serious, with a mortality up to 50% . It is a type of high anion gap metabolic acidosis.
• Those at Risk:
– Elderly
– Frail
– Other Co morbidities (renal impairment)


Two cases of DKA- eh?

Case 1
• 34 year old male JR
• 24 hour history of abdominal pain & vomiting
• PMHx:
– Previous alcohol excess;
– acute pancreatitis
– type 2 diabetes
– bronchiectasis

Case 1
• Provisional diagnosis: recurrent pancreatitis
• However ABG showed:
– pH 6.95 (7.35- 7.45)
– HCO3 5.7 (22- 26mmol/L)
– Base excess -27.4 (+/- 2mmol/L)
– Lactate 0.5 (<1.3)
– Glucose: 10.4
• Urinary ketones: 7.8 (<0.6mmol/L)
• Amylase 37 (<118)
• CT abdomen: atrophic pancreas, no secondary signs of acute pancreatitis


Case 2
• 36 y/o female KH
• PMHx:
– Polycystic ovarian syndrome
– Hypertension
– type 2 diabetes
• October 2014: underwent distal pancreatectomy for 15cm cyst. Shown to be mucinous cystadenoma
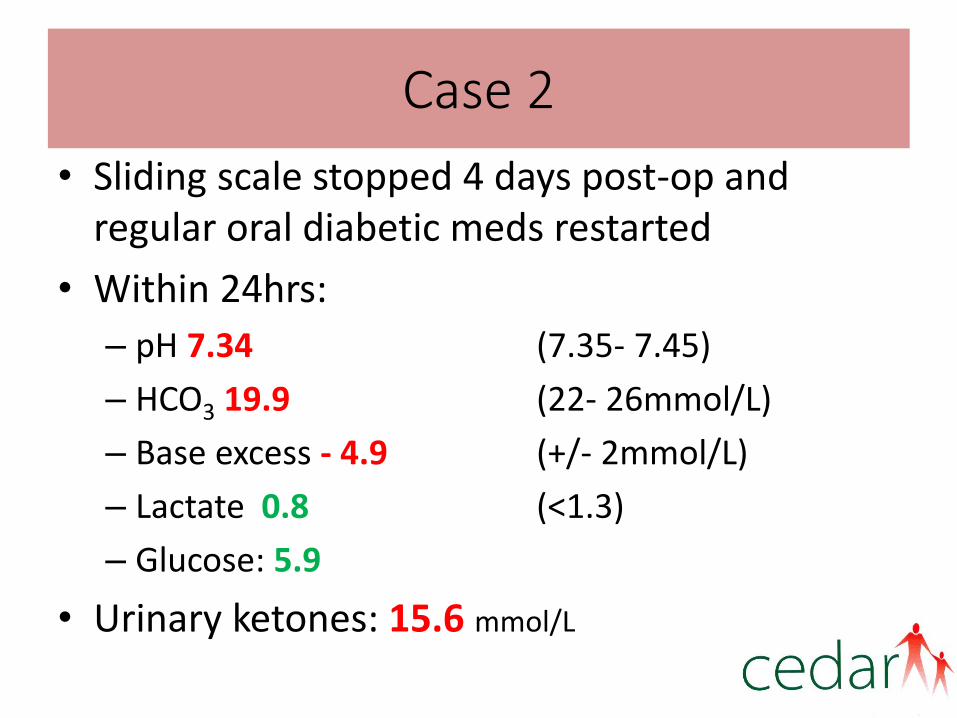
Case 2
• Sliding scale stopped 4 days post-op and regular oral diabetic meds restarted
• Within 24hrs:
– pH 7.34 (7.35- 7.45)
– HCO3 19.9 (22- 26mmol/L)
– Base excess - 4.9 (+/- 2mmol/L)
– Lactate 0.8 (<1.3)
– Glucose: 5.9
• Urinary ketones: 15.6 mmol/L

Diabetes classification
Diabetes + acidosis + ketonuria =DKA
• DKA suggests not type 2 diabetes
• Likely pancreatic diabetes (type 3c)
• Major criteria
1. Pancreatic exocrine dysfunction (insulin & C-peptide)
2. Abnormal pancreatic imaging
3. Negative diabetes autoimmune screen

But why was glucose normal?
A. Reduced calorie state
B. Exogenous insulin administration
C. Intercurrent sepsis
D. Liver cirrhosis
E. Renal tubular acidosis

Euglycaemic DKA
• Defined as DKA with plasma glucose <11.1mmol/mol
• First described in 1973
• Rare, seen in type 1 diabetes in association with reduced calorie states
The twist in the tale…
JR’s DHx:
• Metformin 1g BD
• Gliclazide 120mg OD
• Levemir 20units ON
• Dapagliflozin 10mg OD
KH’s DHx: • Metformin 1g BD • Dapagliflozin 10mg OD


SGLT-2 inhibitors
• Inhibit the sodium-glucose co-transporter 2 (SGLT-2) in the renal tubule
• SGLT-2 responsible for reabsorption of filtered glucose
• SGLT-2 inhibition→ insulin-independent lowering of blood glucose
• Approved for use as adjunctive treatment in type 2 diabetes
SGLT-2 inhibitors
• Main side effect is ↑genito-urinary tract infections due to glycosuria
• Currently only used in type 2 diabetes
• Trials underway in type 1 diabetes
• DKA with lower glucose levels has been seen in the clinical trials
• Risk of masking DKA in insulin-deficient patients
Perkins A, Cherney D, et al. Sodium-Glucose Cotransporter 2 Inhibition and Glycemic Control in Type 1
Diabetes: Results of an 8-Week Open-Label Proof-of- Concept Trial Diabetes Care 2014 37:1480–1483

SGLT2 inhibition and euglycaemic DKA
Hine et al. Lancet May 27 2015


And what happened to JR & KH?
• JR treated with fluids, insulin sliding scale and electrolyte replacement as per DKA protocol
• Previous diabetes medications stopped; started on subcutaneous insulin regimens
• Full recovery and discharge from hospital
• Follow up in secondary care

Empagliflozin, cardiovascular outcomes and mortality in
type 2 diabetes
20
15
10
5
0
Patients
with e
vent (%
)
0 6 12 18 24 30 36 42 48
Time (months)
4687 4580 4455 4328 3851 2821 2359 1534 370
2333 2256 2194 2112 1875 1380 1161 741 166
Empagliflozin
Placebo
No. at risk
HR: 0.86 (95% CI: 0.74; 0.99)
p=0.04 for superiority
Primary outcome (death from cardiovascular causes,
nonfatal myocardial infarction, or nonfatal stroke)
9
8
5
3
0
Patients
with e
vent (%
)
0 6 12 18 24 30 36 42 48
Time (months)
4687 4651 4608 4556 4128 3079 2617 1722 414
2333 2303 2280 2243 2012 1503 1281 825 177
Empagliflozin
Placebo
No. at risk
HR: 0.62 (95% CI: 0.49; 0.77)
p<0.001
Death from cardiovascular causes
7
6
4
2
1
Placebo
Empagliflozin
Zinman et al. N Engl J Med. 2015 Sep 17

Key points
• Suspect DKA in any patient with diabetes presenting with abdominal pain and vomiting
• Diagnosing correct mechanism for diabetes is important in guiding management
• Caution with SGLT-2 inhibitors; avoid or use carefully in patients at risk of insulin deficiency
• At risk of euglycaemic DKA: Check ketones

Decrease hepatic
Glucose production
Increase peripheral
Glucose uptake
Muscle Liver
Primary Effects of Insulin On Blood Glucose
Pancreas

In normal physiological What is the major action of insulin?
A. Suppressing hepatic glucose output (LIVER)
B. Pushing glucose into tissues (PERIPHERY)
Sir Edward Sharpey-Shafer
1895: Suggested that the islets
of Langerhans may function as
a gland that regulates blood
Sugar… “insuline”

His view was “insuline” was inhibitory suppressing glucose production
(3) The substance (insuline) produced by the pancreas islets
may be a chalonic autocoid which tends to inhibit the formation
of glucose from glycogen, and incidentally to promote the
storage of glycogen, so that in its absence the glycogen which is
present in the liver is rapidly converted into glucose.
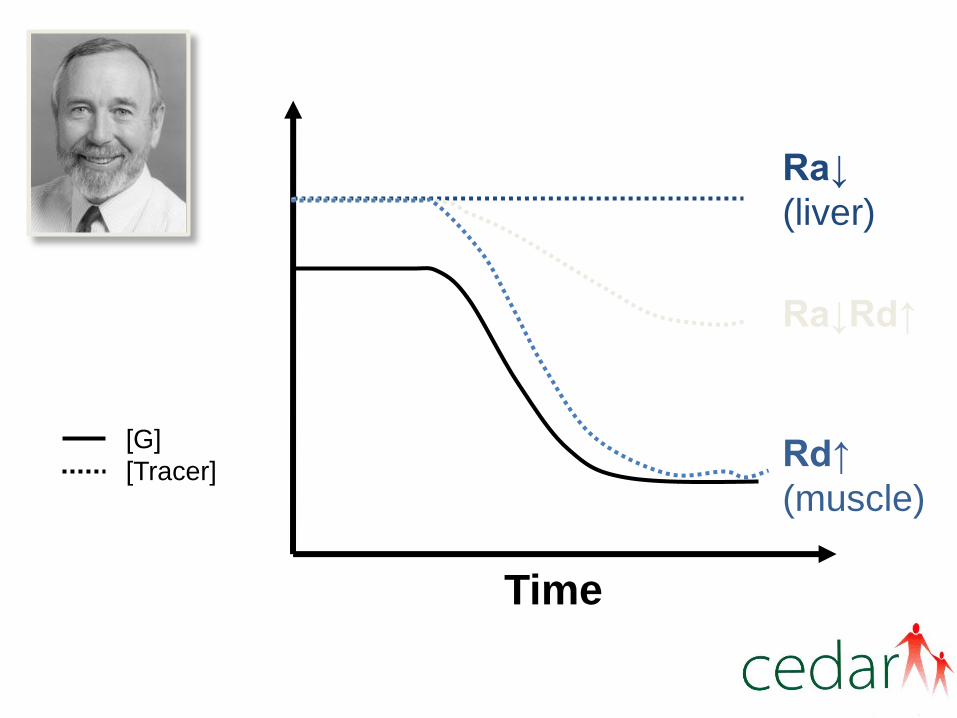
Rd↑
(muscle)
Time
Ra↓
(liver)
Ra↓Rd↑
[G]
[Tracer]

How Do
We Find Out?
A Pilot ‘Dynamic
Tracer Study’ in
Mrs H - a newly
diagnosed IDDM

Insulin Distribution In Normal Physiology
Peripheral tissues
Pancreas
Food
Systemic circulation
Insulin
Glucose
Portal circulation

Insulin Distribution In Diabetes With Exogenous Administration
Peripheral tissues
Pancreas
Food
Insulin
Glucose
Liver

Insulin degludec: structure
NH
O
OH
O NH
O
OH
O
L-γ-Glu
desB30 Insulin
Glutamic acid ‘spacer’
DesB30
T
Des(B30) LysB29(γ-Glu Nε-hexadecandioyl) human insulin
s
A1
B1
A21
s s
s
s s
T Y G E E C Y C C N L Q L S I S Q V I N C
P T Y Y F F F G G G R E E C C V L L A V L H S L H Q N V K
NH
O
OH
O NH
O
Hexadecandioyl C-16 fatty diacid
side chain
1
2
3
Human insulin with one amino-acid
removed and a C-16 fatty diacid side
chain attached via a spacer
Jonassen et al. Pharm Res 2012;29:2104–14
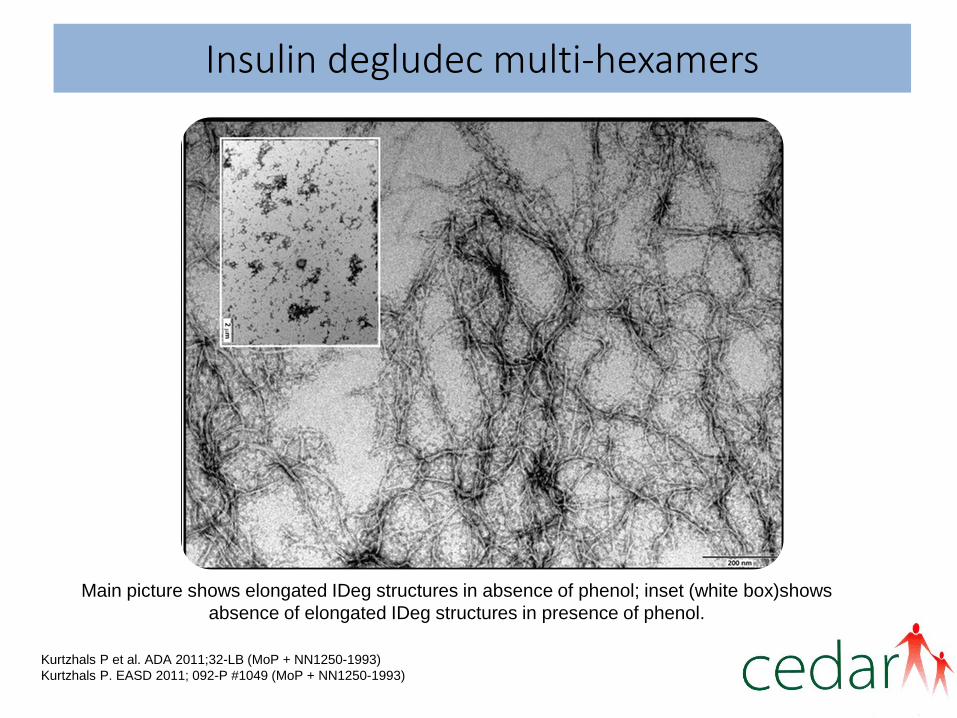
Insulin degludec multi-hexamers
Kurtzhals P et al. ADA 2011;32-LB (MoP + NN1250-1993)
Kurtzhals P. EASD 2011; 092-P #1049 (MoP + NN1250-1993)
Main picture shows elongated IDeg structures in absence of phenol; inset (white box)shows
absence of elongated IDeg structures in presence of phenol.

Degludec pharmacokinetic profile: single dose and steady state
People with type 1 diabetes (n=12)
0.4 U/kg once daily for 6 days
Day 1
Day 6 (steady state)
0 4 8 12 16 20 24
100
1000
10000
Time since last injection (hours)
Insulin
deglu
dec (
pm
ol/L)
Jonassen I et al. Diabetes. 2010;59(suppl 1):A11.

RSCH DKA data (03/14 – 08/15)
• 45 people with type 1 diabetes have presented as an emergency with DKA.
– 29 people were under the age of 70 years.
– 4 people were readmitted > 2 times with DKA within the same year.
– People with repeated admissions with DKA were converted to insulin degludec following intensive education around their insulin regimes.
– This has been 100% successful at preventing readmission rates.

Key points
• DKA practise is changing
• Very long acting insulin analogues may be helpful for recurrent attenders

A Case That Went Badly…

Mr BT
• 54 year old man
• Stroke call
• Right arm numbness
BUT:
• Stroke SpR noted patient had 6/7 “shivers & sweats”
•Pyrexial in ambulance
•Bloods:
–WCC 21 (neuts 17), CRP 227
–Na 126, K 5.2,
–Ur 12.7, Creat 82
–Glu 18.8mmol
• CT head – No evidence acute ischaemic event

Imaging

What would you do next?
A. Urgent incision and drainage
B. Urgent orthopaedic review
C. Urgent vascular review
D. Referral to MDFT
E. 48 hours IV antibiotics and review response

Treatment timeline
Admitted to Stroke unit X-ray: Gas in tissues
Day 1 2 3 4 5 6 7 8 9 10 11
Ortho opinion: Request MRI Refer to MDFT (next one 10/7)
Trauma meeting outcome 0800hrs MRI (“if allowed with cardiac stents”) Referral to diabetic foot team Referral to MDFT
Transferred to ITU: Septic shock / AKI
Requiring inotropic support
Seen by diabetes team: deep infection and spreading gangrene
Seen by vascular, advised urgent I and D
Seen by ortho: for MRI/MRA next day, not for theatre
Worsening sepsis & AKI
Ortho: expedite transfer to vascular centre
Transferred to Vascular centre at 12:45pm
I&D
Cardiac arrest in theatre
Below knee amputation
Subsequent transfer to renal unit for dialysis
Multiple CVAs
Back to vascular centre for palliative care
Died

THE GUILDFORD FOOTPATH - Immediate care of patients with acute DIABETES FOOT problems
N
Treat as severe infection diabetes antibiotic guidelines
N
• Patients with diabetes must have both feet examined by a doctor on admission even if there are no symptoms (neuropathy)
• You must take down any dressings • Subsequent daily inspection by nurses is mandatory • The minimum assessment (RIGHT) is needed to use this pathway
ON CALL T&O Do any of the following apply: • Wet gangrene • White cold pulseless foot • Critically ischaemic limb
This is a FOOT ATTACK!
This patient may lose a limb or die if you do not act
ON CALL T&O URGENT (within 6hrs) incision and drainage On call T&O to undertake
ON CALL T&O TRANSFER NOW to regional vascular hub Contact on call vascular consultant via switch
ON CALL T&O Are any of the following present: • Hot red swollen foot • Boggy tissue when pressed • Collection of pus on exam • Crepitus or gas in the tissues on a plain XR
Minimum assessment: Foot pulses R L Sensation R L FBC Hb WCC CRP Creatinine Plain x ray of foot
Y
ON CALL MEDICINE Dry gangrene of toe (toes)
ON CALL MEDICINE Non-infected foot ulcer in patient admitted with another diagnosis
ON CALL T&O Warm, slightly swollen, non infected foot
ON CALL MEDICINE • Non-urgent (<3 days) inpatient vascular review • DSN review if needed
ON CALL MEDICINE • Manage conservatively • Refer inpatient podiatry • Diabetes consultant IP review • F&A Ortho review • Prevention see purple box adjacent
F&A ORTHO Possible Charcot Strict non weight bearing
DIABETES TEAM
CARE OF ALL PATIENTS WITH DIABETES FOOT PROBLEMS
• Pressure mattress • Minimal weight bearing • No anti-embolism stockings if
neuropathy or impaired pulses • Inform diabetes registrar when
patient admitted
Y ON CALL MEDICINE • Spreading cellulitis • Ulcer infected
ORTHO REVIEW AT TRAUMA MEETING • ? Osteomyelitis • Is urgent vascular opinion
needed?
WHO LOOKS AFTER THE PATIENT? • ON CALL T&O = admitting ortho surgeon
until T&O meeting next working day • F&A ORTHO = foot and ankle ortho .
Weekday rota • ON CALL MEDICINE = admitting physician • DIABETES = Diabetes ward
Theatre planned?
F&A ORTHO
CIRCLE OUTCOME and FILE IN NOTES
Y
Y
Y Y
British Journal of Diabetes 16, (2) 2016. S Davidson
Y
Y
Y

Definition Of Success: The Circle of Life
At age 4….success is….not peeing in your pants.
At age 12….success is….having friends.
At age 16….success is….having a drivers license
At age 20….success is….having sex.
At age 35….success is….having money.
At age 80….success is….not peeing in your pants.
At age 75….success is….having friends.
At age 70….success is….having a drivers license.
At age 60….success is….having sex.
At age 50….success is….having money.

















![Metabolic Emergencies and Their Management[1]](https://img.dokumen.tips/doc/110x75/547ad044b4af9fa5158b4c25/metabolic-emergencies-and-their-management1.jpg)










