Embed Size (px)
Citation preview
Diabetes Self-managementEducation and Support in Type 2Diabetes: A Joint PositionStatement of the AmericanDiabetes Association, theAmerican Association of DiabetesEducators, and the Academy ofNutrition and DieteticsDiabetes Care 2015;38:1372–1382 | DOI: 10.2337/dc15-0730
Diabetes is a chronic disease that requires a person with diabetes to make a mul-titude of daily self-management decisions and to perform complex care activities.Diabetes self-management education and support (DSME/S) provides the founda-tion to help people with diabetes to navigate these decisions and activities and hasbeen shown to improve health outcomes (1–7). Diabetes self-management educa-tion (DSME) is the process of facilitating the knowledge, skill, and ability necessaryfor diabetes self-care. Diabetes self-management support (DSMS) refers to thesupport that is required for implementing and sustaining coping skills and behaviorsneeded to self-manage on an ongoing basis. (See further definitions in Table 1.)Although different members of the health care team and community can contributeto this process, it is important for health care providers and their practice settings tohave the resources and a systematic referral process to ensure that patients withtype 2 diabetes receive both DSME and DSMS in a consistent manner. The initialDSME is typically provided by a health professional, whereas ongoing support can beprovided by personnel within a practice and a variety of community-based resources.DSME/S programs are designed to address the patient’s health beliefs, culturalneeds, current knowledge, physical limitations, emotional concerns, family support,financial status, medical history, health literacy, numeracy, and other factors thatinfluence each person’s ability to meet the challenges of self-management.It is the position of the American Diabetes Association (ADA) that all individuals
with diabetes receive DSME/S at diagnosis and as needed thereafter (8). This posi-tion statement focuses on the particular needs of individuals with type 2 diabetes.The needs will be similar to those of people with other types of diabetes (type 1diabetes, prediabetes, and gestational diabetes mellitus); however, the researchand examples referred to in this article focus on type 2 diabetes. The goals of theposition statement are ultimately to improve the patient experience of care andeducation, to improve the health of individuals and populations, and to reducediabetes-associated per capita health care costs (9). The use of the diabetes edu-cation algorithm presented in this position statement defines when, what, and howDSME/S should be provided for adults with type 2 diabetes.
BENEFITS ASSOCIATED WITH DSME/S
DSME/S has been shown to be cost-effective by reducing hospital admissions andreadmissions (10–12), as well as estimated lifetime health care costs related to alower risk for complications (13). Given that the cost of diabetes in the U.S. in 2012was reported to be $245 billion (14), DSME/S offers an opportunity to decreasethese costs (11,12). It has been projected that one in three individuals will develop
1International Diabetes Center at Park Nicollet,Minneapolis, MN2MedStar Health Research Institute andMedStarNursing, Hyattsville, MD3ABQ Health Partners, Albuquerque, NM4LifeScan, a Johnson & Johnson Diabetes Solu-tions Company, Dubai, United Arab Emirates5University of Michigan Medical School, AnnArbor, MI6University of Chicago, Chicago, IL7Joslin Diabetes Center, Boston, MA8School of Medicine, University of Pittsburgh,Pittsburgh, PA9University of Wisconsin–Madison, Madison, WI
Corresponding author: Margaret A. Powers,[email protected].
The position statement was reviewed andapproved by the Professional Practice Committeeof the American Diabetes Association, the Profes-sional Practice Committee of the American Asso-ciation of Diabetes Educators, and the HouseLeadership Team, theAcademyPositions Commit-tee, and the Evidence-Based Practice Committeeof the Academy of Nutrition and Dietetics.
This article is being simultaneously published inDiabetes Care, The Diabetes Educator, and theJournal of theAcademyof Nutrition andDietetics.
© 2015 by the American Diabetes Association,the American Association of Diabetes Educa-tors, and the Academy of Nutrition and Dietet-ics. Readers may use this article as long as thework is properly cited, the use is educational andnot for profit, and the work is not altered.
Margaret A. Powers,1 Joan Bardsley,2
Marjorie Cypress,3 Paulina Duker,4
Martha M. Funnell,5 Amy Hess Fischl,6
Melinda D. Maryniuk,7 Linda Siminerio,8
and Eva Vivian9
1372 Diabetes Care Volume 38, July 2015
POSITION
STATEMEN
T

type 2 diabetes by 2050 (15). The U.S.health care system will be unable to af-ford the costs of care unless incidencerates and diabetes-related complica-tions are reduced.DSME/S improves hemoglobin A1c
(HbA1c) by as much as 1% in peoplewith type 2 diabetes (3,7,16–20). Besidesthis important reduction, DSME has apositive effect on other clinical, psychoso-cial, and behavioral aspects of diabetes.DSME/S is reported to reduce the onsetand/or advancement of diabetes compli-cations (21,22), to improve quality of life(19,23–26) and lifestyle behaviors such ashaving a more healthful eating patternand engaging in regular physical activity(27), to enhance self-efficacy andempow-erment (28), to increase healthy coping(29), and to decrease the presence ofdiabetes-related distress (16,30) and de-pression (31,32). These improvementsclearly reaffirm the importance andvalue-addedbenefit of DSME. In addition,better outcomes have been shown to beassociatedwith the amount of time spentwith a diabetes educator (3,4,7,11).
This position statement arms healthcare teams with the information requiredtobetter understand the educational pro-cess and expectations for DSME andDSMS and their integration into routinecare. The ultimate goal of the process is amore engaged and informed patient (33).It is recommended that all health careproviders and/or systems develop pro-cesses to guarantee that all patients withtype 2 diabetes receive DSME/S servicesand ensure that adequate resources areavailable in their respective communitiesto support these services.
PROVIDING DIABETES EDUCATIONAND SUPPORT
Historically, DSME/S has been providedthrough a formal programwhere patientsand familymembers participate in an out-patient service conducted at a hospital/health facility. In keeping with evolvinghealth care delivery systems and inmeet-ing the needs of primary care, DSME/S isnow being incorporated into office prac-tices, medical homes, and accountablecare organizations. Receiving DSME/S in
alternative and convenient settings,such as community health centers andpharmacies, and through technology-based programs is becoming moreavailable and affords increased access.
Regardless of the setting, communi-cating the information and supportingskills that are necessary to promote ef-fective coping and self-managementrequired for day-to-day living with dia-betes necessitate a personalized andcomprehensive approach. Effectivedelivery involves experts in educational,clinical, psychosocial, and behavioraldiabetes care (34,35). Clear communica-tion and effective collaboration amongthe health care team that includes aprovider, an educator, and a personwith diabetes are critical to ensurethat goals are clear, that progress to-ward goals is being made, and that ap-propriate interventions (educational,psychosocial, medical, and/or behav-ioral) are being used. A patient-centeredapproach to DSME/S at diagnosis pro-vides the foundation for current and fu-ture needs. Ongoing DSME/S can help the
Table 1—Key definitions
DSME (35)
c The ongoing process of facilitating the knowledge, skill, and ability necessary for diabetes self-care.
c This process incorporates the needs, goals, and life experiences of the person with diabetes or prediabetes and is guided by evidence-basedresearch.
c The overall objectives of DSME are to support informed decision making, self-care behaviors, problem solving, and active collaboration withthe health care team and to improve clinical outcomes, health status, and quality of life.
Note: CMS uses the term “training” instead of “education”when defining the reimbursable benefit (DSMT); the authors of this position statementuse the term “education” (DSME) as reflected in the National Standards. In the context of this article, the terms have the same meaning.
Ongoing DSMS (35)
c Activities that assist the person with diabetes in implementing and sustaining the behaviors needed to manage his or her condition on anongoing basis.
c The type of support provided can be behavioral, educational, psychosocial, or clinical.
Patient-centered care (69)
c Providing care that is respectful of and responsive to individual patient preferences, needs, and values and ensuring that patient values guideall clinical decisions.
Shared decision making
c Eliciting patient perspectives and priorities and presenting options and information so patients can participate more actively in care. Shareddecision making is a key component of patient-centered care (43,77) and has been shown to improve clinical, psychosocial, and behavioraloutcomes (78).
Diabetes-related distress (29,61)
c This refers to the negative emotional responses (overwhelmed, hopeless, and helpless) and perceived burden related to diabetes.
CDE (79)
c A health professional who has completed a minimum number of hours in clinical diabetes practice, passed the Certification Examination forDiabetes Educators (administered by the National Certification Board for Diabetes Educators [NCBDE]), and has responsibilities that includethe direct provision of diabetes education.
BC-ADM (80)
c A health care professional who has completed a minimum number of hours in advanced diabetes management, holds a graduate degree,passed the BC-ADM certification exam (administered by the AADE), and has responsibilities of an increased complexity of decision makingrelated to diabetes management and education.
care.diabetesjournals.org Powers and Associates 1373

person to overcome barriers and to copewith the ongoing demands in order to fa-cilitate changes during the course oftreatment and life transitions.
REIMBURSEMENT, NATIONALSTANDARDS, AND REFERRAL
Reimbursement for DSME/S is availablefrom the Centers forMedicare andMed-icaid Services (CMS) and many privatepayers. Additional discipline-specificcounseling, such as medical nutritiontherapy (MNT) provided by a registereddietitian nutritionist, medication ther-apy management delivered by phar-macists, and psychosocial counselingoffered by mental health professionals,is also reimbursed through CMS and/orthird-party payers (35,36).In order to be eligible for DSME/S re-
imbursement, DSME/S programs mustbe recognized or accredited by a CMS-designated national accreditation orga-nization (NAO). Current NAOs are theADA and the American Association ofDiabetes Educators (AADE). Both bodiesassess the quality of programs using cri-teria established by the NationalStandards for DSME/S (Table 2) (35).Currently, CMS reimburses for 10 pro-gram hours of initial diabetes educationand 2 hours in each subsequent year. Re-ferrals for DSME/S must be made by ahealth care provider and include specifiedindicators, such as diabetes type, treat-ment plan, and reason for referral. Sam-ple referral forms with information
needed for reimbursement are availableon the ADA Web site (http://professional.diabetes.org/Recognition.aspx?typ515&cid593574) and the AADE Web site(http://www.diabeteseducator.org/export/sites/aade/_resources/pdf/general/Diabetes_Services_Order_Form_v4.pdf).
According to the National Standardsfor DSME/S, at least one instructor re-sponsible for designing and planningDSME/Smust be a nurse, dietitian, phar-macist, or other trained or credentialedhealth professional (a certified diabeteseducator [CDE] or health care profes-sional with Board Certified-AdvancedDiabetes Management [BC-ADM] certi-fication) (Table 1) who meets specificcompetency and continuing educationrequirements (35). This person is con-sidered the primary instructor. Otherscan contribute to DSME and providesupport with appropriate training andsupervision. Trained community healthworkers, practice-based care managers,peers, and other support persons (e.g.,family members, social workers, andmental health counselors) have a rolein helping to sustain the benefits gainedfrom DSME (37–41). Such staff/resourcescan be especially helpful in areas withdiverse populations and serve as culturalnavigators in health care systems and asliaisons to the community.
As an alternative to a referral to a for-mal DSME/S program, office-based healthcare teams can explore partnerships with
educators within their community or as-sume responsibility for providing and/orcoordinating some or all of the patient’sdiabetes education and support needs. Al-though this approach requires knowledge,time, and resources to effectively provideeducation, it offers a unique opportunityto reach patients at the point of care. Thisposition statement and the NationalStandards for DSME/S are designed toserve as a resource for the health careteam. Although reimbursement for ed-ucation services is somewhat limited,financial benefits can be realizedwhen an office-based program contrib-utes to improved practice processesand patients’ achievement of out-comes that can influence mandatedquality measures.
DIABETES EDUCATIONALGORITHM
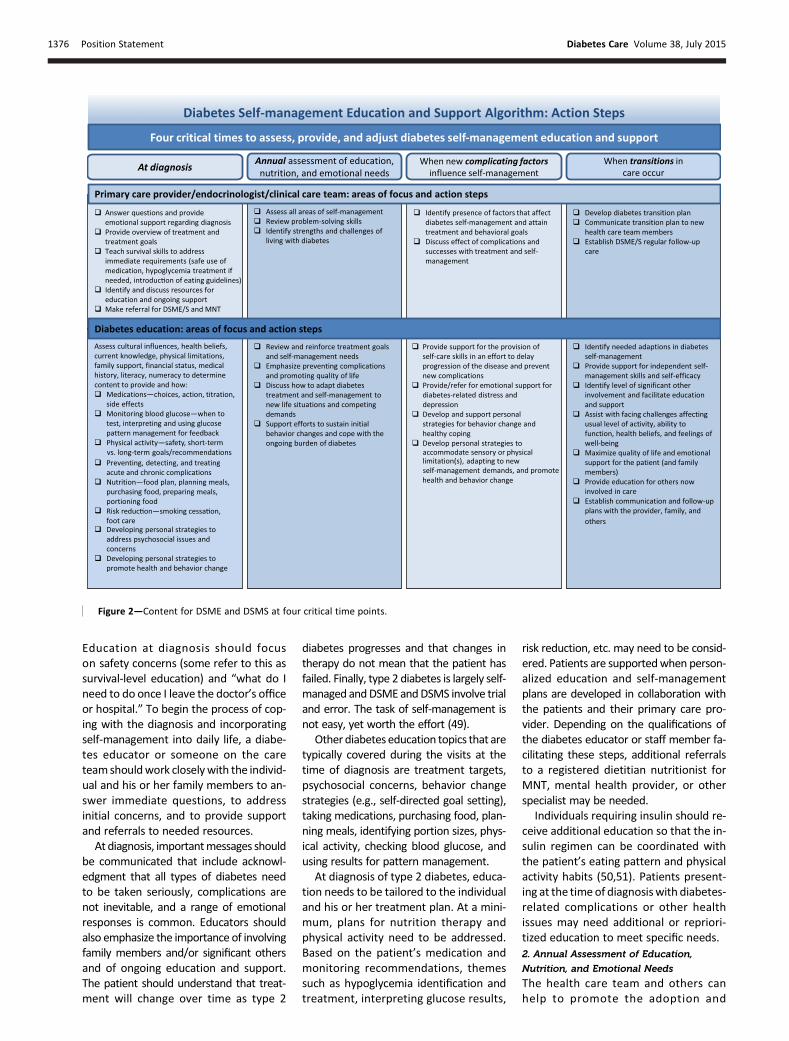
The diabetes education algorithm providesan evidence-based visual depictionofwhento identify and refer individuals withtype 2 diabetes to DSME/S (Figs. 1 and 2)(figures are also available as a slide set atprofessional.diabetes.org/dsmeslides).The algorithm defines four critical timepoints for delivery and key informationon the self-management skills that arenec-essary at each of these critical periods.The diabetes education algorithm canbe used by health care systems, staff, orteams, as well as individuals with diabe-tes, to guide when and how to refer toand deliver/receive diabetes education.
Table 2—National Standards for DSME/S: 10 standards
1. Internal structure. The organizational structure or system that supports self-management education; necessary for sustainability and ongoingself-management education and support.
2. External input. Ensures that providers of DSME will seek input from external stakeholders and experts to promote program quality.
3. Access. A system of assuring periodic reassessment of the population or community receiving self-management education to ensure thatidentified barriers to education are addressed.
4. Program coordination. The designation of an individual with responsibility for coordinating all aspects of self-management education (even ifthat person is the solo instructor).
5. Instructional staff. Identifies who can participate in the delivery of self-management education, recognizing the unique skill set of all potentialproviders of self-management education.
6. Curriculum. A set of written guidelines, including topics, methods, and tools to facilitate education for all people with diabetes; exactly what istaught will be based on patient’s needs, preferences, and readiness.
7. Individualization. Instructor(s) will assess the patient to determine an individualized education and support plan focused on behavior change.
8. Ongoing support. A follow-up plan for ongoing support will be developed by the patient and instructor; communication among the teamregarding goals, outcomes, and ongoing needs is essential.
9. Participant progress. Ongoing measurement of patient self-efficacy and success in self-management and achievement of goals; designed tocontinually assess needed support.
10. Quality improvement. Incorporation of systems to continuously look for ways to evaluate DSME/S effectiveness and to identify areas forimprovement.
Adapted with permission from Haas et al. (35).
1374 Position Statement Diabetes Care Volume 38, July 2015

Guiding Principles and Patient-Centered CareThe algorithm relies on five guiding prin-ciples and represents howDSME/S shouldbe provided through patient engagement,information sharing, psychosocial and be-havioral support, integration with othertherapies, and coordinated care (Table 3).Associated with each principle are key el-ements that offer specific suggestions re-garding interactions with the patient andtopics to address at diabetes-related clin-ical and educational encounters (Table 3).Helping people with diabetes to learn
and apply knowledge, skills, and behav-ioral, problem-solving, and copingstrategies requires a delicate balanceof many factors. There is an interplaybetween the individual and the contextin which he or she lives, such as clinicalstatus, culture, values, family, and socialand community environment. The be-haviors involved in DSME/S are dynamicand multidimensional (42). In a patient-centered approach, collaboration andeffective communication are consideredthe route to patient engagement (43–45).This approach includes eliciting emotions,
perceptions, and knowledge through ac-tive and reflective listening; asking open-ended questions; exploring the desire tolearnorchange;andsupporting self-efficacy(44). Through this approach, patients arebetter able toexploreoptions, choose theirown course of action, and feel empoweredto make informed self-management deci-sions (45,46). Table 4 provides a list ofpatient-centered assessment questionsthat can be used at diagnosis and atother encounters to guide the educationand ongoing support process.
Critical Times to Provide DiabetesEducation and SupportThere are four critical times to assess, pro-vide, and adjust DSME/S (47): 1) with anew diagnosis of type 2 diabetes, 2) annu-ally for health maintenance and preven-tion of complications, 3) when newcomplicating factors influence self-management, and 4) when transitions incare occur (Figs. 1 and 2). Although fourdistinct time-related opportunities arelisted, it is important to recognize thattype 2 diabetes is a chronic condition andsituations can arise at any time that require
additional attention to self-managementneeds. Whereas patient’s needs are con-tinuous (Fig. 1), these four critical timesdemand assessment and, if needed, inten-sified reeducation and self-managementplanning and support.
TheAADE7Self-CareBehaviorsprovideaframework for identifying topics to includeat each time: healthy eating, being active,monitoring, taking medication, problemsolving, reducing risks, and healthy coping.The educational content listed in each boxin Fig. 2 is not intended to be all-inclusive,as specific needs will depend on the pa-tient. However, these topics can guidetheeducational assessment andplan.Mas-tery of skills and behaviors takes practiceand experience. Often a series of ongoingeducation and support visits are necessarytoprovide the time for apatient to practicenewskills andbehaviors and to formhabitsthat support self-management goals.
1. New Diagnosis of Diabetes
The diagnosis of diabetes is often over-whelming (48). The emotional responseto the diagnosis can be a significant bar-rier for education and self-management.
Figure 1—DSME and DSMS algorithm of care.
care.diabetesjournals.org Powers and Associates 1375
Education at diagnosis should focuson safety concerns (some refer to this assurvival-level education) and “what do Ineed to do once I leave the doctor’s officeor hospital.” To begin the process of cop-ing with the diagnosis and incorporatingself-management into daily life, a diabe-tes educator or someone on the careteamshouldwork closelywith the individ-ual and his or her family members to an-swer immediate questions, to addressinitial concerns, and to provide supportand referrals to needed resources.At diagnosis, importantmessages should
be communicated that include acknowl-edgment that all types of diabetes needto be taken seriously, complications arenot inevitable, and a range of emotionalresponses is common. Educators shouldalso emphasize the importance of involvingfamily members and/or significant othersand of ongoing education and support.The patient should understand that treat-ment will change over time as type 2
diabetes progresses and that changes intherapy do not mean that the patient hasfailed. Finally, type 2 diabetes is largely self-managed andDSMEandDSMS involve trialand error. The task of self-management isnot easy, yet worth the effort (49).
Other diabetes education topics that aretypically covered during the visits at thetime of diagnosis are treatment targets,psychosocial concerns, behavior changestrategies (e.g., self-directed goal setting),taking medications, purchasing food, plan-ning meals, identifying portion sizes, phys-ical activity, checking blood glucose, andusing results for pattern management.
At diagnosis of type 2 diabetes, educa-tion needs to be tailored to the individualand his or her treatment plan. At a mini-mum, plans for nutrition therapy andphysical activity need to be addressed.Based on the patient’s medication andmonitoring recommendations, themessuch as hypoglycemia identification andtreatment, interpreting glucose results,
risk reduction, etc. may need to be consid-ered. Patients are supportedwhen person-alized education and self-managementplans are developed in collaboration withthe patients and their primary care pro-vider. Depending on the qualifications ofthe diabetes educator or staff member fa-cilitating these steps, additional referralsto a registered dietitian nutritionist forMNT, mental health provider, or otherspecialist may be needed.
Individuals requiring insulin should re-ceive additional education so that the in-sulin regimen can be coordinated withthe patient’s eating pattern and physicalactivity habits (50,51). Patients present-ing at the time of diagnosiswith diabetes-related complications or other healthissues may need additional or repriori-tized education to meet specific needs.2. Annual Assessment of Education,
Nutrition, and Emotional Needs
The health care team and others canhelp to promote the adoption and
Figure 2—Content for DSME and DSMS at four critical time points.
1376 Position Statement Diabetes Care Volume 38, July 2015

maintenance of new diabetes manage-ment tasks (52), yet sustaining these be-haviors is frequently difficult. Thus, annualassessments of knowledge, skills, and be-haviors are necessary for those who domeet the goals as well as for those whodo not.
Annual visits for diabetes educationare recommended to assess all areas ofself-management, to review behaviorchange and coping strategies and problem-solving skills, to identify strengths andchallenges of living with diabetes,and to make adjustments in therapy
(35,52). The primary care provider or clin-ical teamcan conduct this reviewand referto a DSME/S program as indicated. Morefrequent DSME/S visits may be neededwhen the patient is starting a new diabe-tes medication or experiencing unex-plained hypoglycemia or hyperglycemia,
Table 3—Guiding principles and key elements of initial and ongoing DSME/S (45,58,81)
Engagement. Provide DSME/S and care that reflects person’s life, preferences, priorities, culture, experiences, and capacity.
c Solicit and respond to questions
c Focus on decisions, reasons for the decisions, and results
c Ask about strengths and challenges
c Use shared decision making and principles of patient-centered care to guide each visit
c Engage the patient in a dialogue about current self-management successes, concerns, and struggles
c Engage the patient in a dialogue about therapy and changes in treatment
c Remain “solution neutral” and support patient identifying solution(s)
c Provide support and education to patient’s family and caregiver
Information sharing. Determine what the patient needs to make decisions about daily self-management.
c Discuss that DSME/S is an important and essential part of diabetes management
c Describe that DSME/S is needed throughout the life cycle and is on a continuum from prediabetes, newly diagnosed diabetes, healthmaintenance/follow-up, early to late diabetes complications, and transitions in care related to changes in health status and developmental orlife changes
c Avoid being didactic
c Provide “need-to-know” information and avoid providing the encyclopedia on diabetes
c Review that diabetes treatment will change over time
c Provide information to the patient using the above engagement key elements
c Take advantage of “teachable moments” to provide information specific to the patient’s care and treatment
c Assess DSME/S patient/family needs for the behavioral and psychosocial aspects of informed decision making
Psychosocial and behavioral support. Address the psychosocial and behavioral aspects of diabetes.
c Assess and address emotional and psychosocial concerns, such as diabetes-related distress and depression
c Present that diabetes-related distress and a range of emotions are common and that stress can raise blood glucose and blood pressure levels
c Discuss that diabetes self-management is challenging but worth the effort
c Support self-efficacy and self-confidence in self-management decisions and abilities
c Support action by the patient to identify self-management problems and develop strategies to solve those problems, including self-selectedbehavioral goal setting
c Note that it takes about 2–8 months to change a habit/learn/apply behavior
c Address the whole person
c Include family members and/or support system in the educational and ongoing support process
c Refer to community, online, and other resources
Integration with other therapies. Ensure integration and referrals with and for other therapies.
c Ensure access to ongoing MNT
c Recommend additional referrals as needed for behavioral therapy, medication management, physical therapy, etc.
c Address factors that limit the application of diabetes self-management activities
c Advocate for easy access to social services programs that address basic life needs and financial resources
c Identify resources and services that support the implementation of therapies in health care and community settings
Coordination of care across specialty care, facility-based care, and community organizations. Ensure collaborative care and coordination withtreatment goals.
c Understand primary care provider and specialist’s treatment targets
c Provide overview of DSME/S to referring providers
c Follow medication adjustment protocols or make necessary recommendation to primary care provider
c Correspond with referring provider about education plan, progress toward treatment goals, and needs to coordinate education and supportfrom entire clinical team; ensure documentation in the health record
c Ensure provision of culturally appropriate care
c Use evidence-based decision support
c Use performance data to identify opportunities for improvement
care.diabetesjournals.org Powers and Associates 1377

goals and targets are not being met, clin-ical indicators are worsening, and thereis a need to provide preconception plan-ning. Importantly, the educator is chargedwith communicating the revised plan tothe referring provider.Family members are an underutilized
resource for ongoing support and oftenstruggle with how to best provide thishelp (53,54). Including family membersin the DSME/S process on at least anannual basis can help to facilitate theirpositive involvement (55–57).Since the patient has now experienced
living with diabetes, it is important to be-gin each maintenance visit by asking thepatient about successes he or she has hadand any concerns, struggles, and ques-tions. The focus of each session shouldbe on patient decisions and issuesdwhatchoices has the patientmade,whyhas thepatient made those choices, and if thosedecisions are helping the patient to attainhis or her goalsdnot on perceived adher-ence to recommendations. Instead, it isimportant for the patient/family mem-bers to determine their clinical, psychoso-cial, and behavioral goals and to createrealistic action plans to achieve thosegoals. Through shared decision making,the plan is adjusted as needed in collabo-ration with the patient. To help to rein-force plans made at the visit and supportongoing self-management, the patientshould be asked at the close of a visit to“teach-back” what was discussed duringthe session and to identify one specificbehavior to target or prioritize (58).
3. Diabetes-Related Complications and
Other Factors Influencing Self-management
The identification of diabetes complica-tions or other patient factors that mayinfluence self-management should beconsidered a critical indicator for diabe-tes education that requires immediateattention and adequate resources. Dur-ing routine medical care, the providermay identify factors that influencetreatment and the associated self-management plan. These factors may
include the patient’s ability to manageand cope with diabetes complications,other health conditions, medications,physical limitations, emotional needs,and basic living needs. These factors maybe identifiedat the initial diabetes encoun-ter or may arise at any time. Such patientfactors influence the clinical, psychosocial,and behavioral aspects of diabetes care.
The diagnosis of additional healthconditions and the potential need for ad-ditional medications can complicate self-management for the patient. Diabeteseducation can address the integration ofmultiple medical conditions into overallcare with a focus on maintaining or ap-propriately adjusting medication, eatingplan, and physical activity levels to maxi-mize outcomes and quality of life. In ad-dition to the introduction of new self-careskills, effective coping, defined as a posi-tive attitude toward diabetes and self-management, positive relationships withothers, and quality of life, can be ad-dressed in DSME/S (29). Additional andfocused emotional support may beneeded for anxiety, stress, and diabetes-related distress and/or depression.
Diabetes-related health conditions cancause physical limitations, such as visualimpairment, dexterity issues, andphysicalactivity restrictions. Diabetes educatorscan help patients to manage limitationsthrough education and various supportresources. For example, educators canhelp patients to access large-print or talk-ing glucose meters that benefit thosewith visual impairments and specializedaids for insulin users that can help thosewith visual and/or dexterity limitations.
Psychosocial and emotional factorshave many contributors and includediabetes-related distress, life stresses,anxiety, and depression. In fact, these fac-tors are often considered complicationsof diabetes and result in poorer diabetesoutcomes (59,60). Diabetes-relateddistress (see definition in Table 1) isparticularly common, with prevalencerates of 18% to 35% and an 18-monthincidence of 38% to 48% (61). It has a
greater impact on behavioral and meta-bolic outcomes than does depression (61).Diabetes-related distress is responsive tointervention, including DSME/S and fo-cused attention (30). Although theNational Standards for DSME/S includethe development of strategies to ad-dress psychosocial issues and concerns(35), additional mental health resourcesare generally required to address severediabetes-related distress, clinical de-pression, and anxiety.
Social factors, including difficulty pay-ing for food, medications, monitoringand other supplies, medical care, hous-ing, or utilities, negatively affect meta-bolic control and increase resource use(62). When basic living needs are notmet, diabetes self-management be-comes increasingly difficult. Basic livingneeds include food security, adequatehousing, safe environment, and accessto medications and health care. Educa-tion staff can address such issues,provide information about availableresources, and collaborate with the pa-tient to create a self-management planthat reflects these challenges.
If complicating factors are present dur-ing initial education or a maintenancesession, theDSME/S educators can eitherdirectly address these factors or ar-range for additional resources. How-ever, complicating factors may arise atany time; providers should be preparedto promptly refer patients who developcomplications or other issues for diabe-tes education and ongoing support.
4. Transitional Care and Changes in Health
Status
Throughout the life span, changes inage, health status, living situation, orhealth insurance coverage may require areevaluation of the diabetes care goalsand self-management needs. Criticaltransition periods include transitioninginto adulthood, hospitalization, andmoving into an assisted living facility,skilled nursing facility, correctionalfacility, or rehabilitation center.
Table 4—Sample questions to guide a patient-centered assessment (82)
c How is diabetes affecting your daily life and that of your family?
c What questions do you have?
c What is the hardest part right now about your diabetes, causing you the most concern or most worrisome to you about your diabetes?
c How can we best help you?
c What is one thing you are doing or can do to better manage your diabetes?
1378 Position Statement Diabetes Care Volume 38, July 2015

DSME/S affords important benefits topatients during a life transition. Providinginput into the development of practicaland realistic self-management and treat-ment plans can be an effective asset forsuccessful navigation of changing situa-tions. A written plan prepared in collabo-ration with diabetes educators, thepatient, family members, and caregiversto identify deficits, concerns, resources,and strengths can help to promote a suc-cessful transition. The plan should includepersonalized diabetes treatment targets; amedical, educational, andpsychosocial his-tory; hypo- and hyperglycemia risk factors;nutritional needs; resources for additionalsupport; and emotional considerations(63,64).The health care provider can make a
referral to a diabetes educator to de-velop or provide input to the transitionplan, provide education, and supportsuccessful transitions. The goal is tominimize disruptions in therapy duringthe transition, while addressing clinical,psychosocial, and behavioral needs.
MNT AS AN ADJUNCT TO DSME/SPROGRAMS
The National Standards for DSME/S list“incorporating nutritional management
into lifestyle” as one of nine core topicsin a comprehensive program (35). SomeDSME/S programs include MNT servicesdelivered by a registered dietitian nutri-tionist, whereas other programs providebasic nutrition guidance and rely on re-ferrals for MNT. DSME/S referral formsoften include referral for MNT to help tocoordinate care (ADA and AADE referralforms). The ADA publishes nutrition rec-ommendations that detail nutrition ther-apy goals andnutrition and eatingpatternrecommendations (65). All members ofthe health care team should be versedin the basic principles of diabetes nutri-tion therapy so that they can facilitatebasic meal planning, clarify misconcep-tions, and/or provide reinforcement ofthe nutrition plan developed collabora-tively by the registereddietitian nutrition-ist and the patient (Table 5).
OVERCOMING BARRIERS THATLIMIT ACCESS AND RECEIPT OFDSME/S
The number of people with type 2 diabe-tes who receive DSME/S, despite itsproven benefits, is low. For example,only 6.8% of individuals with newly diag-nosed type 2 diabetes with private healthinsurance participated in DSME/S within
12 months of diagnosis (66). Further-more, only 4% of Medicare participantsreceived DSME/S and/or MNT (4). To in-crease the number of individuals with di-abetes who receive DSME/S servicesdescribed in this position statement, it isnecessary to consider the barriers thatcurrently limit provision. Barriers are as-sociated with a number of factors includ-ing the health system, the individualhealth care professional, communityresources, and the individual withdiabetes. Barriers can include a misun-derstanding of the necessity and effec-tiveness of DSME/S, confusion regardingwhen and how to make referrals, lack ofaccess to DSME/S services, and patientpsychosocial and behavioral factors (67).Provider misconceptions that can limitaccess to DSME/S include a misunder-standing of reimbursement issues andthe misconception that one or a few ini-tial education visits are adequate to pro-vide patients with the skills needed forlifelong self-management. Lack of orpoor reimbursement for DSME/S alsocan hamper patients’ participation.Even when DSME/S programs are oper-ating at peak service, they often struggleto cover costsdmaking it easy to eliminateprograms despite their wider influence on
Table 5—Overview of MNT
MNT is an evidence-based application of the nutrition care process provided by the registered dietitian nutritionist. It includes an individualizednutrition assessment, nutrition diagnosis, intervention and monitoring, and evaluation and is the legal definition of nutrition counseling bya registered dietitian nutritionist practicing in the U.S. (8).
1. Characteristics of MNT reducing HbA1c by 0.5–2% for type 2 diabetes:
c Series of three to four encounters with a registered dietitian nutritionist lasting from 45 to 90 min; the registered dietitian nutritionist shoulddetermine if additional encounters are needed
c Series of encounters should begin at diagnosis of diabetes or at first referral to a registered dietitian nutritionist for MNT for diabetes andshould be completed within 3–6 months
c At least one follow-up encounter is recommended annually to reinforce lifestyle changes and to evaluate and monitor outcomes that indicatethe need for changes in MNT or medication(s)
2. MNT provides nutrition assessment, nutrition diagnosis, and an intervention andmanagement plan including the creation of individualized foodplan and support for the following:
c Individualizedmodification of food plan/physical activity/medication dosing for improved postprandial control, hypoglycemia prevention, andoverall glycemic improvement
c Individualized modification of carbohydrate, protein, fat, and sodium intake and guidance to achieve lipid and blood pressure goals
c Individualized weight management planning and coaching
c Education and support on additional topics to promote flexibility in meal planning, food purchasing/preparation, recipe modification, andeating away from home
c Individualized modification of food plan for managing related complications and comorbidities such as celiac disease, gastroparesis, eatingdisorders/disordered eating, kidney disease, etc.
3. CMS reimburses for diabetes MNT when provided by a qualified practitioner (i.e., registered dietitian nutritionist). Many other payers alsoprovide reimbursement.MNT services are included on the ADA and AADE DSME/S referral forms. A separateMNT referral form is available fromthe Academy of Nutrition and Dietetics at http://www.eatrightpro.org/;/media/eatrightpro%20files/about%20us/what%20is%20an%20rdn%20and%20dtr/mnt_referral_form_15_ jul_14.ashx.
Note: The Academy of Nutrition and Dietetics recognizes the use of registered dietitian (RD) and registered dietitian nutritionist (RDN). RD and RDNcan only be used by those credentialed by the Commission on Dietetic Registration.
care.diabetesjournals.org Powers and Associates 1379

reducing costs and improving health out-comes (13).Although people with diabetes report
wanting to be actively engaged in theirhealth care, most indicate that they arenot actively engaged by their providersand that education and psychologicalservices are not readily available (68).In order to enhance patient and familyengagement in DSME/S, provider com-munication about the necessity of self-management to achieve treatment andquality-of-life goals and the essential na-ture of both DSME and ongoing supportthroughout a lifetime of diabetes is es-sential (Table 3).Removing barriers to access and in-
creasing quality care can be achievedby using data to coordinate care andbuild workforce capacity (69). The U.S.health care paradigm is changing withincreased attention on primary carepractices, technology, and quality mea-sures (70).Studies have shown that implement-
ing DSME programs that directly con-nect with primary care and rely ontechnology is effective in improving clin-ical, psychosocial, and behavioral out-comes (16,71–74). Patients receivingcare in these practice settings reportmore confidence in provider communi-cation and satisfaction with direct ac-cess to an educator for informationand ongoing support (16).Despite the proven value and effec-
tiveness of diabetes education and sup-port services, one of the biggest loomingthreats to their success is low utilization,which has recently forced many suchprograms to close. The current reim-bursement model and mandate forprovider referrals will continue to belimiting factors for access to and partic-ipation in DSME/S. The health care com-munity needs processes that supportreferrals and reimbursement practices,otherwise it will be increasingly moredifficult to sustain DSME/S services. At-tention to these challenges needs to bemet to provide access particularly forareas such as rural and underservedcommunities.
CONCLUSION
Diabetes is a complex and burdensomedisease that requires the person withdiabetes to make numerous daily deci-sions regarding food, physical activity,and medications. It also necessitates
that the person be proficient in a numberof self-management skills (35,75,76). Inorder for people to learn the skills neces-sary to be effective self-managers, DSMEis critical in laying the foundation withongoing support to maintain gains madeduring education. Despite proven bene-fits and general acceptance, the numbersof patients who are referred to and re-ceive DSME/S are disappointingly small.This position statement and algorithmprovide the evidence and strategies forthe provision of education and supportservices to all adults living with type 2diabetes. It is imperative that the healthcare community, responsible for deliver-ing quality care, mobilizes efforts to ad-dress the barriers and explores resourcesfor DSME/S in order tomeet the needs ofadults living with and managing type 2diabetes.
Acknowledgments. The authors gratefully ac-knowledge the commitment and support of thecollaborating organizationsdthe American Dia-betes Association, the American Association ofDiabetes Educators, and the Academy of Nutri-tion and Dietetics; their colleagues, includingmembers of the Executive Committee of the Na-tional Diabetes Education Program, who partic-ipated in discussions and reviews about thisinaugural position statement; and patients whoteach and inspire them. The authors also thankErika Gebel Berg (American Diabetes Associa-tion) for her invaluable editorial contribution.Duality of Interest. No potential conflicts ofinterest relevant to this article were reported.
References1. Brunisholz KD, Briot P, Hamilton S, et al. Di-abetes self-management education improvesquality of care and clinical outcomes deter-mined by a diabetes bundle measure. J Multi-discip Healthc 2014;7:533–5422. Weaver RG, Hemmelgarn BR, Rabi DM, et al.Association between participation in a brief di-abetes education programme and glycaemiccontrol in adults with newly diagnosed diabe-tes. Diabet Med 2014;31:1610–16143. Steinsbekk A, Rygg LO, Lisulo M, Rise MB,FretheimA.Groupbaseddiabetes self-managementeducation compared to routine treatmentfor people with type 2 diabetes mellitus. Asystematic review with meta-analysis. BMCHealth Serv Res 2012;12:2134. Duncan I, Birkmeyer C, Coughlin S, Li Q, SherrD, Boren S. Assessing the value of diabetes ed-ucation. Diabetes Educ 2009;35:752–7605. Fan L, Sidani S. Effectiveness of diabetesself-management education intervention ele-ments: a meta-analysis. Can J Diabetes 2009;33:18–266. Ellis SE, Speroff T, Dittus RS, Brown A, PichertJW, Elasy TA. Diabetes patient education:a meta-analysis and meta-regression. PatientEduc Couns 2004;52:97–105
7. Norris SL, Lau J, Smith SJ, Schmid CH,Engelgau MM. Self-management education foradults with type 2 diabetes: a meta-analysis ofthe effect on glycemic control. Diabetes Care2002;25:1159–11718. American Diabetes Association. Standards ofmedical care in diabetesd2015. Diabetes Care2015;38(Suppl. 1):S5–S879. Berwick DM, Nolan TW, Whittington J. Thetriple aim: care, health, and cost. Health Aff(Millwood) 2008;27:759–76910. Healy SJ, Black D, Harris C, Lorenz A, DunganKM. Inpatient diabetes education is associatedwith less frequent hospital readmission amongpatients with poor glycemic control. DiabetesCare 2013;36:2960–296711. Duncan I, Ahmed T, Li QE, et al. Assessingthe value of the diabetes educator. Diab Educ2011;37:638–65712. Robbins JM, Thatcher GE, Webb DA,Valdmanis VG. Nutritionist visits, diabetes clas-ses, and hospitalization rates and charges: theUrban Diabetes Study. Diabetes Care 2008;31:655–66013. Brown HS 3rd, Wilson KJ, Pagan JA, et al.Cost-effectiveness analysis of a communityhealth worker intervention for low-income His-panic adults with diabetes. Prev Chronic Dis2012;9:E14014. American Diabetes Association. Economiccosts of diabetes in the U.S. in 2012. DiabetesCare 2013;36:1033–104615. Boyle JP, Thompson TJ, Gregg EW, BarkerLE, Williamson DF. Projection of the year 2050burden of diabetes in the US adult population:dynamic modeling of incidence, mortality, andprediabetes prevalence. Popul Health Metr2010;8:2916. Siminerio L, Ruppert K, Huber K, Toledo FG.Telemedicine for Reach, Education, Access, andTreatment (TREAT): linking telemedicine withdiabetes self-management education to im-prove care in rural communities. DiabetesEduc 2014;40:797–80517. Tshiananga JK, Kocher S, Weber C, Erny-Albrecht K, Berndt K, Neeser K. The effect ofnurse-led diabetes self-management educationon glycosylated hemoglobin and cardiovascularrisk factors: a meta-analysis. Diabetes Educ2012;38:108–12318. Welch G, Zagarins SE, Feinberg RG, Garb JL.Motivational interviewing delivered by diabeteseducators: does it improve blood glucose controlamong poorly controlled type 2 diabetes pa-tients? Diabetes Res Clin Pract 2011;91:54–6019. Deakin T, McShane CE, Cade JE, WilliamsRD. Group based training for self-managementstrategies in people with diabetes mellitus. Co-chrane Database Syst Rev 2005;(2):CD00341720. Gary TL, Genkinger JM, Guallar E, Peyrot M,Brancati FL. Meta-analysis of randomized edu-cational and behavioral interventions in type 2diabetes. Diabetes Educ 2003;29:488–50121. The Diabetes Control and ComplicationsTrial Research Group. The effect of intensivetreatment of diabetes on the developmentand progression of long-term complications ininsulin-dependent diabetes mellitus. N Engl JMed 1993;329:977–98622. Stratton IM, Adler AI, Neil HA, et al. Associ-ation of glycaemia with macrovascular and mi-crovascular complications of type 2 diabetes
1380 Position Statement Diabetes Care Volume 38, July 2015

(UKPDS 35): prospective observational study.BMJ 2000;321:405–41223. Cooke D, Bond R, Lawton J, et al.; U.K. NIHRDAFNE Study Group. Structured type 1 diabeteseducation delivered within routine care: impacton glycemic control and diabetes-specific qual-ity of life. Diabetes Care 2013;36:270–27224. Cochran J, ConnVS.Meta-analysis of quality oflife outcomes following diabetes self-managementtraining. Diabetes Educ 2008;34:815–82325. Trento M, Passera P, Borgo E, et al. A 5-yearrandomized controlled study of learning, prob-lem solving ability, and quality of life modifica-tions in people with type 2 diabetesmanaged bygroup care. Diabetes Care 2004;27:670–67526. Toobert DJ, Glasgow RE, Strycker LA, et al.Biologic and quality-of-life outcomes from theMediterranean Lifestyle Program: a randomizedclinical trial. Diabetes Care 2003;26:2288–229327. Toobert DJ, Strycker LA, KingDK, BarreraM Jr,OsunaD,GlasgowRE. Long-termoutcomes fromamultiple-risk-factor diabetes trial for Latinas: ¡VivaBien!. Transl Behav Med 2011;1:416–42628. Tang TS, Funnell MM, Oh M. Lasting effectsof a 2-year diabetes self-management supportintervention: outcomes at 1-year follow-up.Prev Chronic Dis 2012;9:E10929. Thorpe CT, Fahey LE, Johnson H, DeshpandeM, Thorpe JM, Fisher EB. Facilitating healthycoping in patients with diabetes: a systematicreview. Diabetes Educ 2013;39:33–5230. Fisher L,HesslerD,GlasgowRE, et al. REDEEM:a pragmatic trial to reduce diabetes distress.Diabetes Care 2013;36:2551–255831. Hermanns N, Schmitt A, Gahr A, et al. Theeffect of a diabetes-specific cognitive behavioraltreatment program (DIAMOS) for patients withdiabetes and subclinical depression: results of arandomized controlled trial. Diabetes Care2015;38:551–56032. de Groot M, Doyle T, Kushnick M, et al. Canlifestyle interventions do more than reduce dia-betes risk? Treating depression in adults withtype 2 diabetes with exercise and cognitive be-havioral therapy. Curr Diab Rep 2012;12:157–16633. Wagner EH, Bennett SM, Austin BT, GreeneSM, Schaefer JK, Vonkorff M. Finding commonground: patient-centeredness and evidence-based chronic illness care. J Altern ComplementMed 2005;11(Suppl. 1):S7–S1534. Bowen ME, Rothman RL. Multidisciplinarymanagement of type 2 diabetes in children andadolescents. J Multidiscip Healthc 2010;3:113–12435. Haas L, Maryniuk M, Beck J, et al.; 2012Standards Revision Task Force. National Stan-dards for diabetes self-management educationand support. Diabetes Care 2012;35:2393–240136. American Association of Diabetes Educa-tors. Reimbursement tips for primary care prac-tice [Internet], 2009. Available from http://www.diabeteseducator.org/export/sites/aade/_resources/pdf/reimbursement_tips_2009.pdf.Accessed 24 March 201537. Tang TS, Funnell M, Sinco B, et al. Compara-tive effectiveness of peer leaders and communityhealth workers in diabetes self-management sup-port: results of a randomized controlled trial. Di-abetes Care 2014;37:1525–153438. Thom DH, Ghorob A, Hessler D, De Vore D,Chen E, Bodenheimer TA. Impact of peer healthcoaching on glycemic control in low-income
patients with diabetes: a randomized controlledtrial. Ann Fam Med 2013;11:137–14439. Tang TS, Ayala GX, Cherrington A, Rana G. Areview of volunteer-based peer support inter-ventions in diabetes. Diabetes Spectrum 2011;24:85–9840. Funnell MM. Peer-based behavioural strate-gies to improve chronic disease self-managementand clinical outcomes: evidence, logistics, evalua-tion considerations and needs for future research.Fam Pract 2010;27(Suppl. 1):i17–i2241. Heisler M. Overview of peer support mod-els to improve diabetes self-management andclinical outcomes. Diabetes Spectrum 2007;20:214–22142. Marrero DG, Ard J, Delamater AM, et al.Twenty-first century behavioralmedicine: a con-text for empowering clinicians and patients withdiabetes: a consensus report. Diabetes Care2013;36:463–47043. Inzucchi SE, Bergenstal RM, Buse JB, et al.Management of hyperglycemia in type 2 diabe-tes: a patient-centered approach: positionstatement of the American Diabetes Associa-tion (ADA) and the European Association forthe Study of Diabetes (EASD). Diabetes Care2012;35:1364–137944. Miller WR, Rollnick S. Why do peoplechange? In Motivational Interviewing: Prepar-ing People for Change. 2nd ed. New York, TheGuilford Press, 2002, p. 3–1245. Funnell MM, Anderson RM. Empowermentand self-management of diabetes. Clinical Dia-betes 2004;22:123–12746. Rollnick S, Mason P, Butler C. Health Behav-ior Change: A Guide for Practitioners. London,Churchill Livingstone, 199947. Weinger K, MacNeil T, Greenlaw SM. Behav-ioral strategies for improving self-management. InComplete Nurse’s Guide to Diabetes Care. 3rd ed.Childs BP, Cypress M, Spollett G, Eds. Alexandria,VA, American Diabetes Association. In press48. Skovlund SE, Peyrot M. The Diabetes Atti-tudes, Wishes, and Needs (DAWN) program:anewapproach to improvingoutcomesof diabetescare. Diabetes Spectrum 2005;18:136–14249. Weiss MA, Funnell MM. In the beginning:setting the stage for effective diabetes care.Clinical Diabetes 2009;27:149–15150. Philis-Tsimikas A, Walker C. Improved carefor diabetes in underserved populations. J AmbulCare Manage 2001;24:39–4351. Karter AJ, Subramanian U, Saha C, et al. Bar-riers to insulin initiation: the Translating Re-search Into Action for Diabetes Insulin StartsProject. Diabetes Care 2010;33:733–73552. American Association of Diabetes Educa-tors. AADE position statement. Individualizationof diabetes self-management education. Diabe-tes Educ 2007;33:45–4953. Kovacs Burns K, Nicolucci A, Holt RI, et al.;DAWN2 Study Group. Diabetes Attitudes,Wishes and Needs second study (DAWN2�):cross-national benchmarking indicators for fam-ily members living with people with diabetes.Diabet Med 2013;30:778–78854. Peyrot M, Kovacs Burns K, Davies M, et al.Diabetes Attitudes Wishes and Needs 2(DAWN2): a multinational, multi-stakeholderstudy of psychosocial issues and person-centereddiabetes care. Diabetes Res Clin Pract 2013;99:174–184
55. Vaccaro JA, Exebio JC, Zarini GD, HuffmanFG. The role of family/friend social support indiabetes self-management for minorities withtype 2 diabetes. J Nutrition Health 2014;2:1–956. Armour TA, Norris SL, Jack L Jr, Zhang X,Fisher L. The effectiveness of family interven-tions in people with diabetes mellitus: a system-atic review. Diabet Med 2005;22:1295–130557. Gallant MP. The influence of social supporton chronic illness self-management: a reviewand directions for research. Health Educ Behav2003;30:170–19558. Funnell MM, Anderson RM, Piatt GA. Em-powerment, engagement, and shared decisionmaking in the real world of clinical practice.Consultant 2014;53:358–36259. Chew BH, Shariff-Ghazali S, Fernandez A.Psychological aspects of diabetes care: effectingbehavioral change in patients. World J Diabetes2014;5:796–80860. Peyrot M, Rubin RR, Lauritzen T, Snoek FJ,Matthews DR, Skovlund SE. Psychosocial prob-lems and barriers to improved diabetesmanagement: results of the cross-nationalDiabetes Attitudes, Wishes and Needs (DAWN)study. Diabet Med 2005;22:1379–138561. Fisher L, Hessler DM, Polonsky WH, MullanJ. When is diabetes distress clinically meaning-ful? Establishing cut points for the Diabetes Dis-tress Scale. Diabetes Care 2012;35:259–26462. Berkowitz BA, Meigs JB, DeWalt D, et al. Ma-terial need insecurities, control of diabetes melli-tus, and use of health care resources: results ofthe Measuring Economic Insecurity in Diabetesstudy. JAMA Intern Med 2015;175:257–26563. American Association of Diabetes Educators.The American Association of Diabetes Educatorsposition statement: self-monitoring of blood glu-cose using glucose meters in the management oftype 2 diabetes [Internet], 2014. Available fromhttp://www.diabeteseducator.org/export/sites/aade/_resources/pdf/publications/Self-Monitoring_of_Blood_Glucose_FinalVersion.pdf.Accessed 24 April 201564. Hess-Fischl A. Practical management of pa-tient with diabetes in critical care. From a di-abetes educator’s perspective. Crit Care NursQ 2004;27:189–20065. Evert AB, Boucher JL, Cypress M, et al. Nu-trition therapy recommendations for the man-agement of adults with diabetes. Diabetes Care2013;36:3821–384266. Li R, Shrestha SS, Lipman R, Burrows NR, KolbLE, Rutledge S. Diabetes self-management educa-tion and training amongprivately insured personswith newly diagnosed diabetesdUnited States,2011-2012. MMWR Morb Mortal Wkly Rep2014;63:1045–104967. Peyrot M, Rubin RR, Funnell MM, SiminerioLM.Access todiabetes self-managementeducation:results of national surveys of patients, educators,and physicians. Diabetes Educ 2009;35:246–26368. Nicolucci A, Kovacs Burns K, Holt RI, et al.;DAWN2 Study Group. Diabetes Attitudes,Wishes and Needs second study (DAWN2�):cross-national benchmarking of diabetes-relatedpsychosocial outcomes for people with diabetes.Diabet Med 2013;30:767–77769. Institute of Medicine Committee on Quality ofHealthCare inAmerica.Crossing theQuality Chasm:A New Health System for the 21st Century. Wash-ington, DC, The National Academies Press, 2001
care.diabetesjournals.org Powers and Associates 1381

70. Cusack CM, Knudson AD, Kronstadt JL,Singer RF, Brown AL. Practice-based popula-tion health: information technology to sup-port transformation to proactive primarycare (prepared for the AHRQ National Re-source Center for Health Information Technol-ogy under contract no. 290-04-0016). AHRQpublication no. 10-0092-EF. Rockville, MD,Agency for Healthcare Research and Quality,201071. Phillips LS, Barb D, Yong C, et al. Translatingwhat works: a new approach to improve diabe-tes management. J Diabetes Sci Technol. 9March 2015. [Epub ahead of print] DOI:10.1177/193229681557600072. Shea S,Weinstock RS, Teresi JA, et al.; IDEATelConsortium. A randomized trial comparing tele-medicine case management with usual carein older, ethnically diverse, medically under-served patients with diabetes mellitus: 5 yearresults of the IDEATel study. J Am Med InformAssoc 2009;16:446–456
73. Hunt JS, Siemienczuk J, Gillanders W, et al.The impact of a physician-directed health infor-mation technology system on diabetes outcomesin primary care: a pre- and post-implementationstudy. Inform Prim Care 2009;17:165–17474. Siminerio L, Ruppert KM, Gabbay RA. Whocan provide diabetes self-management supportin primary care? Findings from a randomized con-trolled trial. Diabetes Educ 2013;39:705–71375. Piette JD, HeislerM,Wagner TH. Cost-relatedmedication underuse among chronically illadults: the treatments people forgo, how often,and who is at risk. Am J Public Health 2004;94:1782–178776. Delamater AM. Improving patient adher-ence. Clinical Diabetes 2006;24:71–7777. Charles C, Gafni A, Whelan T. Decision-making in the physician-patient encounter: re-visiting the shared treatment decision-makingmodel. Soc Sci Med 1999;49:651–66178. Parchman ML, Zeber JE, Palmer RF. Participa-tory decisionmaking, patient activation,medication
adherence, and intermediate clinical outcomes intype 2 diabetes: a STARNet study. Ann FamMed2010;8:410–41779. National Certification Board for DiabetesEducators. What is a Certified Diabetes Educa-tor? [Internet]. Available from www.ncbde.org/certification_info/what-is-a-cde. Accessed 13March 201580. American Association of Diabetes Educators.Board Certified-Advanced Diabetes ManagementCertification [Internet]. Available from http://www.diabeteseducator.org/ProfessionalResources/Certification/BC-ADM/. Accessed 2 March 201581. Powers MA, Davidson J, Bergenstal RM.Glucose pattern management teaches glycemia-related problem-solving skills in a diabetesself-management education program. DiabetesSpectrum 2013;26:91–9782. Funnell MM, Bootle S, Stuckey HL. The Di-abetes Attitudes, Wishes and Needs secondstudy. Clinical Diabetes 2015;33:32–36
1382 Position Statement Diabetes Care Volume 38, July 2015





























