Embed Size (px)
Citation preview
Diabetes Mellitus type IIDiabetes Mellitus type IIOptimizing Glucose ControlOptimizing Glucose Control
Andrea ShaylorLock Haven University PA
ProgramFebruary 26, 2009

FACTS
Diabetes affects an estimated 24.1 million people -> an increase of more than 3 million in ~2 yrs
6.2 million remain undiagnosed/untreated
Another 57 million with prediabetes/ impaired FPG

Pathophysiology
Genetics + EnvironmentObesity!
defects in glucose uptake ↓ concentration of insulin receptors↓ glycolytic enzymes glucokinase and hexokinase

Pathophysiology
*Beta-cell dysfunction and loss vs. insulin resistance*
Chronic exposure to high glucose causes: -glucose-induced toxicity, resulting in irreversible beta-cell damage -generation of reactive oxygen species causing oxidative stress which affects the mRNA for insulin gene expression, resulting in less insulin production
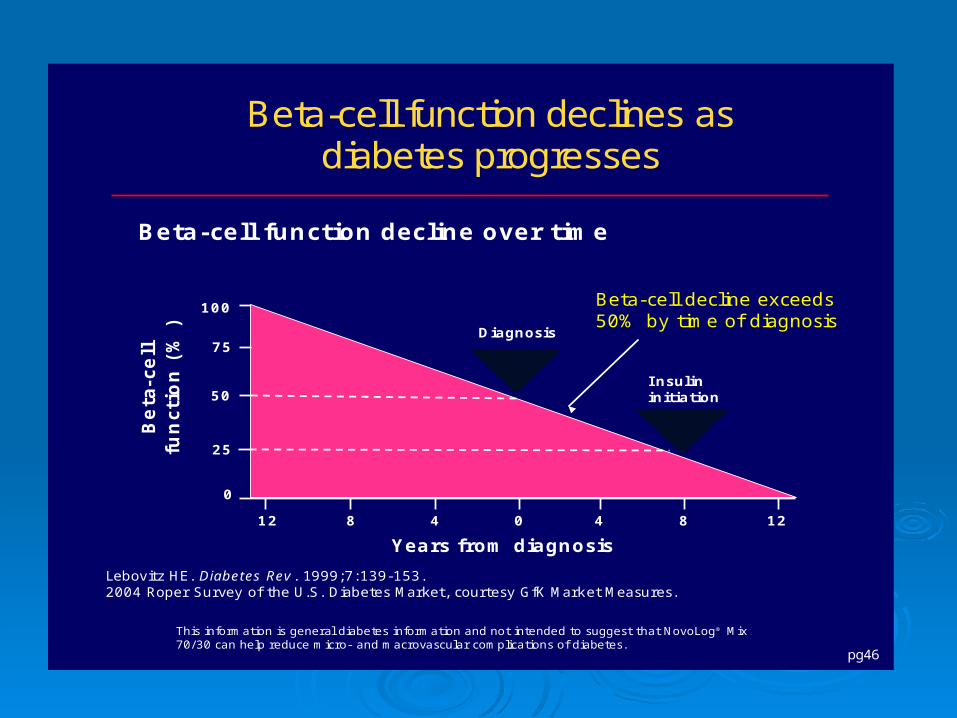
UKPDS: only 50% of pancreatic islet function remains at time of diagnosis
pg46
Beta-cell function declines as diabetes progresses
Lebovitz HE. Diabetes Rev. 1999;7:139-153.2004 Roper Survey of the U.S. Diabetes Market, courtesy GfK Market Measures.
Beta
-cell
fun
cti
on
(%
)
Beta-cell decline exceeds 50% by time of diagnosis
4 4 12 8 0 8 12
0
50
100
75
25 Type 2 Diabetes
IGT
Years from diagnosis
Postprandial
Hyperglycemia
Diagnosis
I nsulininitiation
Beta-cell function decline over time
This information is general diabetes information and not intended to suggest that NovoLog® Mix 70/30 can help reduce micro- and macrovascular complications of diabetes.

Diagnosis
ADA offers 3 criteria:
1)* FPG > 126mg/dL on 2 random occasions2) symptoms of hyperglycemia and a random plasma glucose >200mg/dL3) 2-hour plasma glucose level >200mg/dL after a 75-gram oral glucose tolerance test

Current Management
Lifestyle modification with diet and exercise ↓
FPG goal not met: monotherapy with metformin or sulfonylurea
↓Combination of above, or another oral agent
↓Addition of 3rd agent, various combinations, or new agent
ie incretin mimetic/Byetta or DPP-4 inhibitor/Januvia ↓
When all else fails: Insulin


Target for treatment Glycosylated hemoglobin A1C, average blood glucose
over past 3 mos, shows better correlation to micro and macrovascular complications than glycemic values
ADA and ACC recommendation: HgbA1C <6.5-7% UKPDS: for every 1% reduction in A1C:
- 21% reduction in death related to diabetes-14% reduction in risk for MI, 12% for stroke-32% reduction in risk for retinopathy-24-27% reduction in risk for nephropathy-30% reduction in risk for neuropathy
Intensive glycemic control associated with a 57% reduction in major CVD outcomes

Suboptimal Control Causes irreversible micro and macrovascular
complications, m & m Despite this, 60% of pts do not meet goals Prospective study of 7000 pts: Avg pt remained at A1C
>8% for 5 yrs and >7% for 10 yrs At time of all OA failure, many pts have had diabetes for
10-15 yrs, and long term complications have already developed
Meneghini, L. (2007). Why and How to Use Insulin Therapy Earlier in the Management of Type 2 Diabetes. Southern Medical Association, 100: 164-173.

PICO Question:
In the adult population with DM type II, should insulin be initiated earlier, after failure of just one oral agent, as measured by HbA1C, versus the further addition/combo of OAs, for better glycemic control thereby preventing or delaying the associated DM complications?

Retrospective cohort study involving 2501 patients with DM type II above OGLA failure threshold
Found that 24% of patients had insulin delayed for at least 1.8 yrs, and 50% delayed for 5 yrs with polytherapy, even in the presence of diabetes-related complications
A1C levels were closer to 9% before intervention was triggered
Rubino, A., McQuay, L., Gought, C., et al. (2007). Delayed initiation of subcutaneous insulin therapy after failure of oral glucose-lowering agents in patients with Type 2 Diabetes. Diabetic Medicine, 24: 1412-1418.

Evidence for Use Although oral agents succeed at lowering glucose, there
is still a continued loss of B-cell function with time. Sulfonylureas have been to shown to possibly increase
the risk of B-cell apoptosis. TZDs associated with adverse effects However, insulin is proven to prevent glucotoxicity and
lipotoxicity, in addition to preserving B-cell functioning
Tibaldi, J. (2008). Preserving Insulin Secretion in type 2 Diabetes Mellitus. Expert Review of Endocrinology & Metabolism : Medscape, 3(2): 147-159.

OAD Reduction in A1C
Actos or Avandia .1-.9
Prandin 1.1
Metformin 1.4
Sulfonylureas 1-2
Insulin ~2+
Vinik, Aaron. (2007). Advancing Therapy in Type 2 DM with Early, Comprehensive Progression from OA to Insulin Therapy. Clinical Therapeutics, 29: 1236-1253.

A1C levels before and after insulin
Window of Opportunity When blood glucose levels are normalized and
maintained early, the glucotoxicity and oxidative stress causing B-cell deterioration and apoptosis can be reversed:
Clinical trials of short periods of intensive insulin therapy administered early have resulted in temporary remission due to restored B-cell functioning
However, when same intensive insulin therapy used in pts with avg of 7.6 yrs of DM, insulin response was much less
Tibaldi, J. (2008). Preserving Insulin Secretion in type 2 Diabetes Mellitus. Expert Review of Endocrinology & Metabolism : Medscape, 3(2): 147-159.

ADA/ACE Goals & Algorithm
FPG<100mg/dL and 2hr PPG <140mg/dL If HbA1C remains >7% following lifestyle
changes + metformin after 3 mos-> consider insulin Metformin when combined with insulin has
weight-ameliorating effects
Vinik, Aaron. (2007). Advancing Therapy in Type 2 DM with Early, Comprehensive Progression from OA to Insulin Therapy. Clinical Therapeutics, 29: 1236-1253.

Regimen?
Elevated FPG-- basal Elevated PPG-- basal/bolus or *premixed
PP glycemic control accounts for 50% of overall glycemic control
INITIATE treat-to-target trial: Metformin+ premix BIAsp30: 66% reached <7% Metformin + basal glargine: 40% reached <7%
1-2-3 Trial: Failure on OA, with BIAsp30 added: 41% reached <7%, 21% reached <6.5% in 16 wks
Fleury-Milfort, Evelyne. (2007). Practical Strategies to improve treatment of type 2 diabetes. Journal of the American Academy of Nurse Practitioners, 20: 295-304.

55% of practitioners delay until absolutely necessary due to:~Fear of hypoglycemia & weight gain~More complicated and time consuming
PIR: DAWN study:5000 DM pts, 3000 HCPs- >1/2 pts not using insulin worry about the time to start & >1/2 view the start as personal failureLigthelm, R., Davidson, J. (2008). Initiating insulin in primary care- The role of modern premixed
formulations. Primary Care Diabetes 2: 9-16. Study published in Diabetes Educator found 50-77% of
pts admitted to feelings of failure vs 35% with fear of injectionsLarkin, M., Capasso, V., Chen, C., et al. (2008). Measuring Psychological Insulin Resistance. The Diabetes Educator, 34: 511-517.

Long term benefits outweigh Newer insulin analogues are safer,
simpler, better approximated to physiologic/endogenous insulin secretion, minimal weight gain
Smaller, more user-friendly needles Diabetes Education!

Ultimate Goal for Outcome
Reducing glucose toxicity Minimizing complications Preventing m & m by improving CV profile Limiting healthcare costs Improving QOL

References Brunton, S., Tenzer-Iglesias, P., Unger, J. (2008). Initiating and intensifying therapy in
type 2 Diabetes. The Journal of Family Practice, 57, S17-26. Fleury-Milfort, Evelyne. (2007). Practical Strategies to improve treatment of type 2
diabetes. Journal of the American Academy of Nurse Practitioners, 20: 295-304. Larkin, M., Capasso, V., Chen, C., et al. (2008). Measuring Psychological Insulin
Resistance. The Diabetes Educator, 34: 511-517. Ligthelm, R., Davidson, J. (2008). Initiating insulin in primary care- The role of modern
premixed formulations. Primary Care Diabetes 2: 9-16. Meneghini, L. (2007). Why and How to Use Insulin Therapy Earlier in the
Management of Type 2 Diabetes. Southern Medical Association, 100: 164-173. Rubino, A., McQuay, L., Gought, C., et al. (2007). Delayed initiation of subcutaneous
insulin therapy after failure of oral glucose-lowering agents in patients with Type 2 Diabetes. Diabetic Medicine, 24: 1412-1418.
Skyler, J., Bergenstal, R., Bonow, R., et al. (2008). Intensive Glycemic Control and the Prevention of Cardiovascular Events. Journal of the American College of Cardiology, 53: 298-304.
Tibaldi, J. (2008). Preserving Insulin Secretion in type 2 Diabetes Mellitus. Expert Review of Endocrinology & Metabolism : Medscape, 3(2): 147-159.Vinik, Aaron. (2007). Advancing Therapy in Type 2 DM with Early, Comprehensive Progression from OA to Insulin Therapy. Clinical Therapeutics, 29: 1236-1253.





























