Embed Size (px)
Citation preview

Diabetes in Asia and the Pacific:Implications for the GlobalEpidemicDiabetes Care 2016;39:472–485 | DOI: 10.2337/dc15-1536
The last three decades havewitnessed an epidemic rise in the number of peoplewithdiabetes, especially type 2 diabetes, and particularly in developing countries, wheremore than 80% of the people with diabetes live. The rise of type 2 diabetes in SouthAsia is estimated to be more than 150% between 2000 and 2035. Although aging,urbanization, and associated lifestyle changes are the major determinants for therapid increase, an adverse intrauterine environment and the resulting epigeneticchanges could also contribute in many developing countries. The InternationalDiabetes Federation estimated that there were 382 million people with diabetes in2013, a number surpassing its earlier predictions. More than 60% of the people withdiabetes live in Asia, with almost one-half in China and India combined. TheWesternPacific, the world’s most populous region, has more than 138.2 million people withdiabetes, and the numbermay rise to 201.8million by 2035. The scenario poses hugesocial and economic problems to most nations in the region and could impedenational and, indeed, global development. More action is required to understandthedrivers of the epidemic to provide a rationale for prevention strategies to addressthe rising global public health “tsunami.” Unless drastic steps are taken throughnational prevention programs to curb the escalating trends in all of the countries,the social, economic, and health care challenges are likely to be insurmountable.
Diabetes is now a disease of major concern both globally and regionally and is aleading cause of death in most countries (1). In 2013, the International DiabetesFederation (IDF) estimated that ;382 million people had diabetes worldwide, andby 2035, this was predicted to rise to 592 million. Eighty percent live in low- andmiddle-income countries, and of the total, more than 60% live in Asia, with almostone-third in China (2). Major increases in the prevalence of diabetes have occurredin developing countries due to rapid and ongoing socioeconomic transition and willlikely lead to further rises (2). The prevalence of both type 1 and type 2 diabetes(T2DM) has increased significantly during recent decades. T2DM, being much morecommon (2), has been themain driver for the increase in global diabetes prevalenceand, therefore, will be the focus of this review.It should be noted that with regard to diabetes prevalence, only broad comparisons
can be made among studies on which national and global estimates by the IDF arebased. This is because there are marked differences in age-groups, survey methodol-ogies, diagnostic criteria, and other aspects of these studies in the various countries inAsia and the Pacific. Despite this, almost all developing countries in theWestern Pacificregion (WPR) (3) and also in South Asia (4–6) have shown escalating rates.The WPR is the world’s most populous World Health Organization (WHO) re-
gion, comprising 39 heterogeneous countries and territories, with populations
1India Diabetes Research Foundation, Chennai,India2Department of Medicine & Therapeutics, TheChinese University of Hong Kong, Prince ofWalesHospital, Shatin, Hong Kong3Hong Kong Institute of Diabetes and Obesity,The Chinese University of Hong Kong, Shatin,Hong Kong4Li Ka Shing Institute of Health Sciences, The Chi-nese University of Hong Kong, Shatin, Hong Kong5Saw Swee Hock School of Public Health, Na-tional University of Singapore, Singapore6Baker IDI Heart and Diabetes Institute, Mel-bourne, Australia
Corresponding author: Paul Z. Zimmet, [email protected].
Received 14 July 2015 and accepted 28 Novem-ber 2015.
A.N. and R.C.W.M. contributed equally to thiswork.
© 2016 by the American Diabetes Association.Readersmayuse this article as longas thework isproperly cited, the use is educational and not forprofit, and the work is not altered.
Arun Nanditha,1 Ronald C.W. Ma,2,3,4
Ambady Ramachandran,1
Chamukuttan Snehalatha,1
Juliana C.N. Chan,2,3,4 Kee Seng Chia,5
Jonathan E. Shaw,6 and Paul Z. Zimmet6
472 Diabetes Care Volume 39, March 2016
REV
IEW

ranging from more than 1 billion peo-ple in China to 10,000 in small PacificIsland nations like Tuvalu. The regionhas undergone rapid changes develop-mentally, socioeconomically, politi-cally, and culturally during the lastfew decades (3).The increasing prevalence of diabetes
can be attributed to a multitude of in-terrelated factors, including rapid indus-trialization and urbanization and theensuing changes in lifestyle factors(4,6). The effect of the intrauterine en-vironment and the resulting epigeneticchanges may also convey increased riskof T2DM and other chronic diseases inadult life (1,7). Epigenetic changes canbe transmitted to future generations,thus becoming intergenerational. Therisk factors for T2DM are summarizedin Table 1 and are detailed below. Inter-estingly, the propensity of these risk fac-tors to cause diabetes appears higheramong the populations in South Asiaand in the WPR compared with Westernpopulations, and this is discussed in alater section.T2DM is increasingly present in even
children and adolescents (1,3–5), andthe increase in gestational diabetesmellitus (GDM) poses new challenges
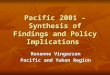
such as higher risk of diabetes amongwomen and long-term consequencesfor the offspring (2,6,8,9). Prediabetesprevalence is also higher than that ofdiabetes in many of the WPR countries(10). T2DM is the focus of this review,which aims to address the major eth-nic, demographic, anthropometric, so-cioeconomic, genetic, and epigeneticfactors that are likely to be responsiblefor the dramatic rise in T2DM. We de-scribe the epidemiological scenario inAsia and in the Pacific. For the purposeof this review, the WPR refers to EastAsia, Southeast Asia, Australia, NewZealand, and the Pacific Islands; SouthAsia refers to Afghanistan, Bangladesh,Bhutan, India, Maldives, Mauritius,Nepal, Pakistan, and Sri Lanka (Fig. 1).Many of the nations in these regionsdo not have national data, so theyhave not been discussed in detail inthis review.
It should be noted that much of thediabetes prevalence data discussed inthis review come from IDF estimates(10). These have significant limitations,in that for countries without availablelocal data, estimates are based on mod-eling using pooled estimates from coun-tries that might be seen to be similar ingeography, ethnicity, and economic de-velopment. Similarly, numerous countrydata are based on WHO STEPwise ap-proach to Surveillance (STEPS) studies(11). These are not necessarily compa-rable with each other owing to method-ological differences. These limitationsmust be considered when examiningthe data.
Impaired fasting glucose and im-paired glucose tolerance (IGT) arehigh-risk conditions for diabetes andcardiovascular disease (12). China andmost of the other countries in WPRhave a high prevalence of IGT (3). Thisis true of many countries in Asia (13).However, many countries use only fast-ing plasma glucose (FPG) in epidemio-logical studies and therefore do nothave data on IGT. The use of FPG under-estimates the true level of diabetes andprediabetes compared with the oral glu-cose tolerance test (OGTT).
LITERATURE SEARCH STRATEGYAND SELECTION CRITERIA
We searched PubMed and Googlesearch using key words “diabetes inWestern Pacific Region,” “diabetes in
South Asia,” diabetes in individual coun-tries of these regions, “risk factors forT2DM in Western Pacific population,”“risk factors for T2DM in South Asians,”“gestational diabetes among Asian pop-ulation,” and “prevention of diabetes.”Published reports by the IDF, theWHO, and the American Diabetes Asso-ciation on the above topics were used.We selected the relevant articles andreviews from peer-reviewed journalsidentified by the search for preparingthe review.
THE DIABETES EPIDEMIC IN THEPACIFIC REGION AND IN ASIA
WPRToday, the nations in theWPR region arehighly heterogeneous in economic pro-file, varying from the high per capitagross domestic product in countriessuch as Singapore to low gross domesticproduct in the poorest nations. Devel-oped countries inWPR, such as Australiaand New Zealand, have a much lowerprevalence of diabetes compared withsome developing countries and alsothe Pacific Islands (14).The IDF esti-mated that in the WPR in 2013, therewere 138 million people with diabetes,36% of the global total (10). The biggestcontribution to this number is China,with 113.9 million adults with diabetesand 493.4 million with prediabetes (15).Some small Pacific Islands, such as Toke-lau, according to the IDF estimates andtheWHO STEPS studies (11), have a veryhigh diabetes prevalence (Table 2). Asmentioned earlier, these are not neces-sarily comparablewith each other owingto methodological differences betweenand within countries. This point is high-lighted in Cambodia by a 2005 report(16) showing that T2DM has emergedat rates similar to those in developednations such as Australia; yet, a subse-quent STEPS modeling study showedthat Cambodia had the lowest preva-lence in the WPR (10).
In the 2013 IDF estimates, China topsthe global list of countries for the totalnumber of people with diabetes, fol-lowed by India (2). The number of peo-ple with diabetes in Japan has increasedsignificantly since 1997, especiallyamong the male population. In 2013, itoccupied the 10th position in the IDF list,with 7.2 million people with diabetes(17). Indonesia has not registered a sig-nificant increase since 1997 (18,19).
Table 1—Plausible etiological factorsresponsible for the increased propen-sity to develop T2DM
Genetic and acquired factorsGenetic factors (familial aggregations)Ethnic susceptibilityAdverse gene–environment interaction
(i.e., epigenetics, metabolicmaladaptations)
Lower threshold for diabetogenic riskfactors (i.e., age, BMI, central adiposity)
Low muscle massIncreased insulin resistanceDecreased b-cell compensationdisproportionate to insulin insensitivity
Presence of metabolic obesityIncreased inflammatory response
Environmental risk factorsUrbanization and modernizationGlobalization and industrializationUnhealthy behavioral habits (sedentary
lifestyle, consumption of energy-dense food, smoking, tobacco chewing,and excessive alcohol consumption)
Sleep disturbancesPsychological stress
Societal factorsCultural and religious taboosPsychosocial factorsLack of universal health coverage
care.diabetesjournals.org Nanditha and Associates 473

IDF estimates for diabetes within thePacific vary widely, from the world’s high-est of 47.3% in American Samoa to a com-paratively lower prevalence of 7.3% inFrench Polynesia (3,10). Figure 1 showsthe map of the WPR, and Table 2 reportsthe temporal changes in the prevalence ofdiabetes in these countries. The risingtrend in the developing countries is con-siderably steeper compared with the de-veloped countries (1,12,14,15,17–34). Inrecent decades, apart from the WHOSTEPS studies (11), there have been veryfew national diabetes studies for the Pa-cific Ocean nations (14). Nevertheless,some of the highest estimates of preva-lence globally continue to be seen in thisregion, even though the use of FPG aloneunderestimates the true diabetes preva-lence (35) and the laboratory methodswere not standardized among the studies.Obesity is a major driver of the T2DM
epidemic, and the Pacific Island nationsare among the leaders in the world obe-sity and diabetes charts (14). Accordingto the latest WHO criteria for obesity(11), more than 70% of the people inAmerican Samoa, Nauru, and Tokelauare obese. Other islands also show ahigh prevalence of obesity, includingKiribati (50.6%), the Marshall Islands(45%), the Federated States ofMicronesia
(42.6%), the Solomon Islands (32.8%), andFiji (29.6%) (14).
Since the 1960s, the Pacific region hasbeen recognized as a “hot spot” for di-abetes, with Prior and Davidson (36)first reporting a higher diabetes preva-lence in Polynesians compared withNew Zealanders of European descent.In 1975, on the Central Pacific island ofNauru, the then highest ever nationaldiabetes prevalence of 34.4% was re-ported (37). Income from Nauru’s richphosphate deposits had resulted in itsMicronesian population becoming ex-tremely prosperous and obese. Withthe phosphate deposits now exhausted,and with the consequent contractionof the national economy, a significantfall has occurred in diabetes preva-lence (1). In the 1980s, Zimmet et al.(38) confirmed the higher prevalenceof diabetes in other Pacific Islands usingstandardized protocols. However, be-cause most of these studies were under-taken more than two decades ago, theyare unlikely to reflect current diabetesrates (14).
The paucity of secular data in the Pa-cific presents a difficulty in monitoringtrends. The age-standardized preva-lence of T2DM in Western Samoa in-creased between 1978 and 1991 from
8.1 to 9.5% in men and from 8.2% to13.4% in women in the urban area,and from 2.3% to 7% in men and from4.4% to 7.5% in women in a rural com-munity (39). In Tonga in 2002, Colagiuriet al. (40) reported a dramatic secularincrease (100% in 25 years) in diabetesfrom 7.5% in 1973% to 15.1%, of which80% were undiagnosed cases.
King et al. (16), in 2005, reported ondiabetes in Cambodia, a relatively poorand fairly traditional country, showingprevalence of 5% (rural) and 11% (semi-urban). The prevalence of IGT was 10%(rural) and 15% (semiurban). About two-thirds of all cases of diabetes were un-diagnosed. These figures are muchhigher than those reported by a subse-quent WHO STEPS study (11). Such dif-ferences, which may relate to the firststudy being a dedicated diabetes surveyand using the OGTT and the secondstudy being a general survey of noncom-municable diseases and relying on thefasting glucose alone, need to be keptin mind.
InMalaysia, the reportedprevalence ofdiabetes was 11.6% in 2006 (26), 15.2%(8% undiagnosed) in the 2011 nationalstudy (41), and 22.9% in 2013 (26). Theage distribution of the study groups wassimilar. The higher prevalence seen in the2013 survey may partly be explained bythe use of the OGTT. In Thailand, the Na-tional Health Examination Survey showedthat the diabetes prevalence in peopleaged $15 increased from 2.5% in 1991to 4.6% in 1997 and to 6.8% in 2004(32). In 2009, their National Health Exam-ination Survey (33) found the prevalenceof impaired fasting glucose was 10.6%and diabetes was 7.5% (of which 35.4%were undiagnosed cases) in adults aged$20 years. These prevalences were likelyto be underestimates because diagnosisrelied only on a single FPG, history of phy-sician diagnosis, and information onmedications (33). The age-standardizedprevalence in Singapore has remainedconstant at ;11% during the lasttwo decades. In Singapore, diabeteswas more common in Indians (17.2%)than in Malays (16.6%) or Chinese(9.7%) (31).
The prevalence of diabetes in Korea in-creased from ,1% in 1960 to .10% byearly 2000. TheKoreaNationalHealth andNutrition Examination Survey (KNHANES)2010–2012 also reported a prevalence of10.1% based on FPG (29,30), suggesting a
Figure 1—Map shows the Western Pacific and South Asian regions.
474 Implications of Diabetes in Asia and WPR Diabetes Care Volume 39, March 2016

Tab
le2—Preva
lence
ofdiabetesin
theWPR,withtemporalch
angessh
ownwhereve
rava
ilable*
Country
Year
(Ref)
Samplesize
(n)
Characteristics
Diagn
osticcriteria
Diabetes
(%)
American
Samoa
2004
(14)
2,07
2WHOSTEP
S;stratified
cluster
sampling;
age:
25–64
years
Cap
illaryFPG$6.1mmol/L
47.3
Australia
2011
–20
12(20)†
NR
Age:$18
years
HbA1c$6.5%
($47
.5mmol/mol)
5.4
BruneiDarussalam
2003
(21)†
NR
Population-based
datafrom
integrated
health
screen
ingsystem
frommed
icalcase
records;age:NR
CapillaryFPG$6.1mmol/Lorknowndiabetes
5.4
2010
(21)†
NR
Age:$20
years
CapillaryFPG$6.1mmol/Lorknowndiabetes
12.5
Cam
bodia
2004
(16)
2,24
6Cross-sectional;tw
ocommunities:ruraland
semiurban;age:
$25
years
FPG$7.0mmol/Lor/and2-hPG
$11
.1mmol/L
Rural:5.0
Suburban:11
.020
11(24)†
5,12
3WHOSTEP
S;multistage
cluster
method
(180
clusters);age:
25–65
years
FPG$7.0mmol/Lor/and2-hPG
$11
.1mmol/L
Total:2.9(95%
CI2.3–3.4)
Rural:2.3(95%
CI1.7–2.9)
Urban:5.6(95%
CI4.0–7.2)
China
2001
(25)†
15,838
Nationallyrepresentative
stratified
sampling;
age:
35–74
years
FPG$7.0mmol/Lor2-hPG
$11
.1mmol/L
5.5
2010
(15)†
98,658
Complex,multistage,probability
samplingdesign;
age:
$18
years
FPG$7.0mmol/Lor2-hPG
$11
.1mmol/L
11.6
China,HongKo
ngSA
R19
90(22)
1,51
3Participan
tsfrom
apublic
utilitycompanyanda
regionalhospital;age:
$30
years
FPG$7.8mmol/Lor2-hPG
$11
.1mmol/L
4.5
2007
–20
10(23)
3,37
6HongKo
ngprofessionaldrivercommunityproject;
age:
18–70
years
FPG$7.8mmol/Lor2-hPG
$11
.1mmol/L
8.1
CookIslands
1980
(14)
1,10
2Po
pulation-based
study;age:
$20
years
FPG$7.8mmol/Lor2-hPG
$11
.1mmol/L
6.8
2003
(14)
2,03
6WHOSTEP
S;stratified
samples;age:
NR
CapillaryFPG$6.1mmol/Loronmed
ication
23.6
Federated
States
ofMicronesia
1994
(14)
2,18
8Po
pulation-based
studyin
Kosrae
population;
age:
20–85
years
FPG$7.0mmol/L
12.0
2002
(14)
1,63
8WHOSTEP
S;population-based
cross-sectional
study;age:
25–64
years
FPG$7.0mmol/L
32.1
Fiji
2002
(14)
2,27
7Po
pulation-based
multistage
samplingin30
clusters;
age:
15–64
years
CapillaryFPG$6.1mmol/Loronmed
ication;HbA1c
$6.5%($
47.5
mmol/mol)orknownto
havediabetes
16.0
2009
(14)
1,35
3WHOSTEP
S;population-based
study;age:$40
years
44.8
Fren
chPo
lynesia
2010
(14)
3,46
9WHOSTEPS;population-based
multistage
sampling;
age:
18–64
years
CapillaryFPG$6.1mmol/Loronmed
ication
7.3
Indonesia
1997
(18)
941
Population-based
studyofgovernmen
tandretired
individuals;age:
NR
FPG$7.8mmol/Lor2-hPG
$11
.1mmol/L
5.4
2009
(19)
24,417
Samplesfrom
13urban
provinces;age:
$15
years
FPG$7.8mmol/Lor2-hPG
$11
.1mmol/L
5.7
Japan
1997
(17)
National
Age:$20
years
FPG$7.0mmol/Lor/and2-hPG
$11
.1mmol/L
M:F9.9:7.1
2007
(17)
National
Age:$20
years
FPG$7.8mmol/Lor2-hPG
$11
.1mmol/L
M:F15
.3:7.3
Kiribati
1983
(14)
2,93
8Po
pulation-based
survey;age:
$20
years;South
Tarawaandthefourouterislands;age:15
–64
years
FPG$7.0mmol/Lor2-hPG
$11
.1mmol/L
Urban
:M:F9.6:8.7
Rural:M:F3.0:3.3
2004
–20
06(14)
1,14
6WHOSTEP
S;population-b
ased
multistage
sampling;
age:
18–64
years
FPG$7.0mmol/L
28.1
Con
tinu
edon
p.47
6
care.diabetesjournals.org Nanditha and Associates 475

Table
2—Continued
Country
Year
(Ref)
Samplesize
(n)
Characteristics
Diagnosticcriteria
Diabetes
(%)
Malaysia
2006(26)
34,539
Malaysian
NationalHealthMorbiditySurvey
(NHMS)
III;age:
$18
years
FPG$7.1mmol/Lorknownto
havediabetes
11.6
2013(26)
4,34
1Tw
o-stage
stratified
samplingdesign;age:$
18years
HbA
1c$6.5%
,FPG
$7.8mmol/Lor
2-hPG
$11.1mmol/L
22.9
MarshallIslands
2002(14)
994
WHOSTEP
S;population-based
;age:
15–64
years
FPG$7.0mmol/L
19.6
Mongo
lia20
05(27)
3,41
1WHOSTEP
S;population-based
;age:
15–64
years
Cap
illaryFBG$6.1mmol/Loronmed
ication
8.2
2009(27)
5,36
8WHOSTEP
S;population-based
;age:
15–64
years
Cap
illaryFBG$6.1mmol/Loronmed
ication
6.5
Nauru
1987
(1)
1,20
1Po
pulation-based
data;age:
$20
years
FPG$7.8mmol/Lor2-hPG
$11
.1mmol/L
24.0
2004(14)
883
System
aticrandom
sampledesign;age:15–
64years
FPG$7.0mmol/Loronmed
ication
16.2
(age
15–24
years)
22.7
(age
25–64
years)
New
Zealand
2002
–20
03(28)
12,929
Stratified
cluster
sampling;
age:
$15
years
FPG$7.0mmol/Lor2-hPG
$11
.1mmol/L
8.1
2008
–20
09(28)
4,72
1Age:$15
years
FPG$7.0mmol/Lor2-hPG
$11
.1mmol/L
7.0
Niue
1980
(1)
1,12
8Po
pulation-based
survey;age:
$20
years
FPG$7.8mmol/L
7.2
2012(14)
863
WHOSTEP
S;population-based
;age:
$15
years
Cap
illaryFBG$6.1mmol/Loronmed
ication
38.4
PapuaNew
Guinea
1991(14)
497
Population-based
cluster;age:
$25
years
Ran
dom
bloodglucose
$8mmol/Lorknowndiabetes
Urban:30
.3Rural:Wan
igela:
11.7
Kalo:1.6
2008(14)
2,94
4WHOSTEP
S;population-based
survey;age:
15–64
years
Cap
illaryFBG$6.1mmol/Loronmed
ication
14.4
Rep
ublic
ofKo
rea
2005(29)
4,62
8KN
HANES;age:
$30
years
FPG$7.0mmol/Lor/an
dhistory
ofdiabetes
9.1
2007
–20
09(29)
13,512
Age:$30
years
FPG$7.0mmol/L
9.9
2011
–20
12(30)†
14,330
NationalHealthSurvey;age:
$30
years
FPG$7.0mmol/L
10.1
Samoa
1991
(14)†
1,77
6Po
pulation-based
cluster
sampling;age:25
–74
years
FPG$7.8mmol/Lor/an
d2-hPG
$11
.1mmol/L
Apia:M:F9.5:13.4
Poutasi:M:F5.3:5.6
Tuasivi:M:F7.0:7.5
2002(14)
2,81
7WHOSTEP
S;random
samplepopulation-based
study;age:
15–64
years
Cap
illaryFBG$6.1mmol/LorvenousFPG$7.0mmol/L
oronmed
ication
22.1
Singapore
2004
(31)†
NR
Nationalsurvey;age:
18–69
years
FPG$7.8mmol/Lor2-hPG
$11
.1mmol/L
8.2
2010
(31)†
NR
Nationalsurvey;age:
18–69
years
FPG$7.8mmol/Lor2-hPG
$11
.1mmol/L
11.3
SolomonIslands
1986(14)
243
Population-based
study;age$18
years
WHOSTEP
S;population-based
;age:
25–64
years
FPG$7.0mmol/Lor/an
d2-hPG
$11
.1mmol/L
2.09
2006(14)
950
Cap
illaryFBG$6.1mmol/Loronmed
ication
13.5
Thailand
1991
(32)†
National
Age:$30
years
FPG$7.0mmol/L
2.3
2004
(32)†
National
Age:$15
years
FPG$7.0mmol/L
6.8
2009
(33)†
National
Age:$20
years
FPG$7.0mmol/L
7.5
Tokelau
1976(14)
346
Population-based
study;age:
35–74
years
OGTT
(100
g):1-hPG
$13
.9mmol/L
M:F7.0:14.3
2005(14)
573
WHOSTEP
S;population-based
nationalsurvey;
age:
15–64
years
Cap
illaryFBG$6.1mmol/Loronmed
ication
33.6
Con
tinu
edon
p.47
7
476 Implications of Diabetes in Asia and WPR Diabetes Care Volume 39, March 2016

constant prevalence of diabetes duringthe last decade. Diabetes was more prev-alent in individuals in lower socioeco-nomic groups, a finding similar to that indeveloped Western countries.
South AsiaSouth Asia constitutes one-fifth of theworld’s population and includes ninecountries, all ofwhich are undergoing life-style transitions that make their popula-tions more vulnerable to develop T2DM.In the last few decades, the diabetesprevalence in South Asia has also risenconsiderably. Table 3 reports the secularchanges that occurred in these nations(5,42–51). However, true nationally rep-resentative data, which include urban andrural prevalence, are lacking frommost ofthese countries, including India.
South Asian populations also have ahigh prevalence of prediabetes and amore rapid progression to diabetes(13). This is highlighted by a recent studythat reported a diabetes incidence of22.2 per 1,000 person-years and that59% of those with prediabetes con-verted to diabetes after a follow-up of9.1 years (52).
A 2008 report from Southern Indiashowed a marked increase in diabetesprevalence in both urban and rural areascompared with earlier studies (53).Studies from other parts of India havealso shown increases in diabetes preva-lence (13,46).
India is the largest country in the re-gion and has more than 65.1 millionpeople with diabetes, occupying thesecond position next to China in theIDF global list of top 10 countries forpeople with diabetes. Pakistan and Ban-gladesh are in 12th and 13th positions,respectively (10). The IDF estimates thatthe number of people with diabetes inSouth Asia will increase to 120.9 million,10.2% of the adult population, by 2030.The highest increase in diabetes preva-lence is noted in Mauritius (48) (Table3), an Indian Ocean island with a pre-dominantly Asian Indian population. Asurvey conducted in urban and ruralMaldives showed that the prevalenceof diabetes was 10.6% (47). Howeverresults from the STEPS survey con-ducted in Male, the Maldives capitalcity, showed the prevalence of diabeteswas 4.5% in all adults (11). Again, thereason for the difference seen in theSTEPS study is unclear.
Table
2—Continued
Country
Year
(Ref)
Samplesize
(n)
Characteristics
Diagn
osticcriteria
Diabetes
(%)
Tonga
1991
(14)†
1,02
4Nationalsample;age:
$15
years
FPG$7.0mmol/Lor/and2-hPG
$11
.1mmol/L
15.1
2004
(14)†
453
WHOSTEP
S;population-based
nationalsurvey;
age:
15–64
years
Cap
illaryFBG$6.1mmol/Loronmed
ication
16.4
Van
uatu
1991
(14)
1,37
8Anoccupation-based
(civilservants)urban
sample
andarea-based
semiruralandruralsam
ples;age:NR
FPG$7.0mmol/Lor/and2-hPG
$11
.1mmol/L
Vila:M:F2.1:12.1
Nguna:M:F2.1:1.1
Tanna:
M:F1.0:0.9
2011
(14)†
4,42
2WHOSTEP
S;population-based
nationalsurvey;
survey
included
allsixprovinces;age:
25–64
years
Cap
illaryFBG$6.1mmol/Loronmed
ication
21.2
Vietnam
2001
(34)
2,93
2Cross-sectional;age$15
years
FPG$7.8mmol/Lor/and2-hPG
$11
.1mmol/L
3.8
FPG$7.8mmol/Lor2-hPG
$11
.1mmol/L
2011
(12)
2,71
0Cross-sectional;age:
40–64
years
FPG$7.0mmol/Lor/and2-hPG
$11
.1mmol/L
3.7
Wallis
andFutuna
1980
(14)†
549
Population-based
study;age:
$20
years
FPG$7.8mmol/Lor2-hPG
$11
.1mmol/L
2.7
2010
(14)†
487
WHOSTEP
S;population-based
nationalsurvey;
age:
15–64
years
FPG$7.0mmol/Loronmed
ication
17.5
F,female;FBG,fastingbloodglucose;H
bA1c,glycated
hem
oglobinA1c;M,m
ale;NR,notreported
;PG,plasm
aglucose;SAR,SpecialAdministrativeRegion.*Itneedsto
berecognized
that
onlybroad
comparisons
canbemad
efrom
thesedataowingto
sign
ificantdifferencesin
age-groups,survey
methodologies,diagn
osticcriteria,etc.†Nationalstudies.
care.diabetesjournals.org Nanditha and Associates 477

Several distinctive features are notedamong the South Asians, such as earlyoccurrence of diabetes at lower BMI lev-els (6), higher rates of insulin resistance,abdominal obesity, and familial aggrega-tionof diabetes than inmanyother ethnicgroups. In recent decades, an increasingdiabetes prevalence has been reported inrural areas in middle-income groups andamong underprivileged people (13,51).Occurrence of T2DM at a young age iscommonly observed among South Asians,with the picture further complicated by thepresence of maturity-onset diabetes of theyoung or latent autoimmune diabetes ofadulthood (13).
Urban-Rural DifferenceIn developing countries in Asia and WPR,the urban-rural difference in diabetesprevalence is narrowing due to the in-creasing reach of Western lifestyles andassociated behavioral changes into ruralsettings. In India, Nepal, Sri Lanka, theSolomon Islands, Samoa, and Thailand,more than 50%of the national populationwith diabetes resides in rural areas (10).Recent studies from India (53) and China(4,6,54) have shown greater rates of in-crease in diabetes prevalence in ruralthan in urban areas. Hwang et al. (55)reported that across multiple surveys,there was evidence of a fivefold rise inthe prevalence of diabetes from 1985 to2010 in rural populations of developingcountries.
Diabetes in the DiasporaPopulation-based studies indicate ahigher prevalence of diabetes amongthe South Asian diaspora comparedwith other ethnic and the local popula-tions in many Western nations, includ-ing the U.S. and the U.K. (13,56–60).Among South Asians, T2DM is usuallydiagnosed at an earlier age and is asso-ciated with increased mortality com-pared with the white population inthese countries.
Risk Factors for Diabetes in Asians andPacific IslandersSimilar risk factors for T2DM have beenidentified in Europids and in Asian popu-lations (5,6,54).Many of these risk factorsare closely linked to economic develop-ment and the increasing urbanizationseen across much of Asia and the Pacific.Some risk factors for T2DM have becomeof great concern among developing coun-tries in Asia and the Pacific. As discussed
Table
3—Preva
lence
ofdiabetesin
South
Asia,withtemporalch
anges
shownwhereve
rava
ilable
Country
Year
(Ref)
Samplesize
(n)
Characteristics
Diagn
osticcriteria
Diabetes
(%)
Afghanistan
2013
(42)
1,16
9Age:.40
years
Cap
illaryFBG$6.1mmol/Loronmed
ication
13.3
Bangladesh
2005
(5)
6,31
2Cross-sectional;age:
$20
years
FPG$7.0mmol/Lor/and2-hPG
$11
.1mmol/L
Urban:8.3
Rural:2.3
2011
(43)*
8,83
5Po
pulation-based
nationalsurvey;age:
$35
years
FPG$7.0mmol/Lor2-hPG
$11
.1mmol/L
9.7
Bhutan
2008
(44)
2,47
4Stratified
two-stage
sampling;
age:
25–74
years
FPG$7.0mmol/Lor/and2-hPG
$11
.1mmol/L
8.2
India
2000
(45)
11,216
Random
sampling,sixmetropolitan
cities;
age:
$20
years
FPG$7.0mmol/Lor/and2-hPG
$11
.1mmol/L
12.1
2008
–10
(46)
13,055
Stratified
multistage
sampling(188
urban,1
75rural)
inthreestates
andoneunionterritory;agenotreported
FastingCBG$7mmol/Lor/and2-hCBG$12
.2mmol/L
oronmed
ication
TamilNadu:10
.4Maharashtra:
8.4
Jharkhan
d:5.3
Chan
digarh:13
.6
Maldives
2004
(47)*
1,55
6Cross-sectional;national;age:
25–64
years
FPG$7.0mmol/Lor/and2-hPG
$11
.1mmol/L
4.5
Mauritius
1987
(48)
5,08
3Indep
enden
tpopulation-based
survey;age:
20–74
years
FPG$7.8mmol/Lor2-hPG
$11
.1mmol/L
13.0
2009
(48)
6,37
1Age:20
–74
years
FPG$7.8mmol/Lor2-hPG
$11
.1mmol/L
21.3
Nep
al20
11(49)
14,425
Populationfrom
EasternNep
al;age:
.20
–10
0years
FPG$7.0mmol/Lor2-hPG
$11
.1mmol/L
6.3
Pakistan
2000
(50)
1,04
2Age:30
–64
years
FPG$7.0mmol/Lor2-hPG
$11
.1mmol/L
6.5
2006
(50)
5,43
3Age:30
–64
years
FPG$7.0mmol/Lor/and2-hPG
$11
.1mmol/L
Urban:10
.6Rural:7.7
SriLan
ka20
01(5)
6,04
7Cross-sectional;stratified
random
samplesfrom
four
provinces;age:
$30
years
FPG$7.0mmol/Loronmed
ication
13.8
2006
(51)*
4,53
2Cross-sectional;nationalrepresentative;age:
$20
years
FPG$7.0mmol/Lor2-hPG
$11
.1mmol/L
10.3
CBG,capillarybloodglucose;FBG,fastingbloodglucose;PG
,plasm
aglucose.*N
ationalstudy.
478 Implications of Diabetes in Asia and WPR Diabetes Care Volume 39, March 2016

later, the prevalence of GDM has also in-creasedmarkedly in Asia and thePacific inrecent decades (9,10).Much of the recent increase in diabe-
tes prevalence is related to changes indietary pattern, sedentary behavior, andobesity superimposedona background ofgenetic/epigenetic susceptibility (61).Most Asian countries have witnessed, todifferent degrees, a nutritional transition,with increases in intake of refined carbo-hydrates, animal fats, and meat, and re-duced consumption of dietary fiber andvegetables (61,62). Similar to theU.S., theconsumption of sugar-sweetened bever-ages in China has increased dramaticallyduring the last few decades (62).Several dietary risk factors may be par-
ticularly relevant to Asians. The SouthAsian diet, characterized by high intakeof carbohydrates, trans fats, and saturatedfats (63), appears particularly conduciveto the risk of T2DM.White rice constitutesup to 60% of the glycemic load among theChinese and was found to be associatedwith an increased risk of diabetes in ameta-analysis (64). This association be-tween white rice intake and risk ofT2DM was also noted in India (65). Al-though rice has been a staple food forcenturies, there has been a shift to in-creased intake of polished rice, whichproduces a greater glycemic excursionthan do the more traditional types ofrice. Furthermore, Asians appear to havegreater glycemic excursion to white ricecompared with other populations (66).Physical inactivity is an important risk
factor for T2DM in most populations(4,5). With increasing urbanization, phys-ical activity has declined, particularly inoccupational settings (67), and sedentarybehavior has increased. This highlightsthe importance of encouraging physicalactivity and reducing sedentary behaviorin large-scale community diabetes pre-vention initiatives in Asia and the Pacific.Studies that have examined the asso-
ciation between adiposity and diabetesin multiethnic cohorts noted that Asiansdevelop diabetes at a considerablylower BMI compared with Europids(54,68). This is ascribed to visceral adi-posity in Asian populations (69). As a re-sult, in Asians, lower BMI cutoffs arebeing used to define obesity (70) aswell as lower waist circumference fordefining central obesity (57,70). How-ever, two large observational studieshave shown that the incremental risk
of diabetes associated with increasingadiposity does not differ between Euro-pid and Asian populations (71,72). Thus,the ethnic difference in the adiposity-diabetes relationship is probably bettercharacterized as an increased risk of di-abetes at all levels of BMI (or waist cir-cumference) rather than as diabetesoccurring at lower levels of BMI. It isvery similar to the increased diabetesrisk of Asian populations seen at allages, and both observations point tofactors other than those related to obe-sity or age that increase diabetes sus-ceptibility in Asian populations.
Several novel putative risk factorshave recently emerged as important be-havioral and environmental determi-nants for T2DM. These include sleepdisturbances and environmental expo-sure to organic pollutants and otherchemicals (62). Given the major prob-lems of pollution in many developingcountries, the latter has the potentialto be an important contributor to thediabetes epidemic during adult life oras an in utero exposure.
Developmental Origins of T2DM:Relevance in Asia and PacificCommunitiesThe initial observations on the associationbetween low birth weight and adult riskof diabetes and metabolic disturbanceswere made by Hales and Barker (73). Itis now increasingly appreciated that thein utero environment plays an importantrole in modifying developmental trajec-tory and physiology, thereby altering therisk of obesity, T2DM, and other chronicdiseases in adulthood (7).
Studies in relation to the Dutchwinter(74) and Chinese (75) famines providesupport for the hypothesis that nutri-tional deprivation in utero may predis-pose an individual to T2DM in adult life.In those exposed to severe famine insome parts of China during early life,there is a marked increase in the riskof diabetes as adults compared withthose not exposed to the same severenutritional restriction during in uterodevelopment. This risk of diabetes inmidlife is highest among offspring ex-posed to in utero undernutrition andwho were subsequently exposed to anaffluent diet (75). This phenomenon ofhistorical exposure to undernutrition inearly life followed by exposure to a“metabolically challenging” environment
characterized by an energy-dense dietmay be highly relevant to the currenthigh rates of T2DM in parts of Asia andthe Pacific.
The emergence of T2DM in Cambodiaat rates similar to those in developednations (16) came decades after thepolitical and socioeconomic upheavalcaused severe food shortages in Cambo-dia in 1975. During World War II, theNauruanswere subjected to famine con-ditions on Nauru and on other PacificIslands, such as Truk, where they hadbeen relocated. Some three decadeslater, Nauru had the highest diabetesprevalence in the world (37). These his-torical examples show the potential ofunexpected health outcomes from warsand famine when later followed by rela-tive overnutrition. Furthermore, thestudy by Yajnik (76) in India strongly sug-gest that early development issues andepigenetics may play an important rolein the contemporary burden of diabetesexperienced in India.
In addition to a link between in uteroundernutrition and offspring risk, epi-demiological studies, particularlyamong the Pima Indians, have high-lighted increased risk of obesity andT2DM in offspring exposed to maternaldiabetes or obesity (77–79). This is alsoparticularly relevant in Asia, wherethere is a higher proportion of young-onset diabetes and a higher prevalenceof GDM compared with Europe and theU.S. (9). Thus, intergenerational cyclesmay operate in Asia to increase the riskof diabetes in future generations (76).
GDMWith the epidemiological transitions oc-curring in Asia, leading to a younger ageof diabetes onset, the burden of preg-nancy complicated by hyperglycemia isincreasing (80). Hyperglycemia in preg-nancy includes cases of diabetes predatingpregnancy as well as GDM. On the basisof a systematic literature review of stud-ies reporting the prevalence of GDM indifferent countries, the IDF estimatedthat 16% of pregnancies globally wereaffected by hyperglycemia in 2013,with a crude prevalence of 11.8% in theIDF WPR and 23.1% in the South Asian re-gion (80). TheprevalenceofGDMreportedin Asia has ranged from 1% to more than20%, depending on the period, ethnicity,and population in which the study wasconducted, as well as the screening
care.diabetesjournals.org Nanditha and Associates 479

strategy and diagnostic criteria being used,which has been extensively reviewed else-where (9). A study from Australia compar-ing women of different ethnicities with adiagnosis of GDMnoted that women fromSoutheast Asia had the lowest BMI andwere more likely to be diagnosed basedon elevated 2-h glucose during OGTT,whereas women from Pacific Islands andAnglo-Europeans had the highest BMI andweremore likely to be diagnosed based onelevated fasting glucose (81).A marked secular increase in preva-
lence of GDM has been reported in sev-eral studies; for example, universalscreening of pregnant women for GDMin Tianjin, China, showed that the prev-alence increased markedly from 2.4 to6.8% from 1999 to 2008 (82). Use of thediagnostic criteria proposed by the In-ternational Association of the Diabetesand Pregnancy Study Groups (IADPSG),recently adopted by the WHO (83), islikely to lead to further increases inGDM prevalence. In a study from Viet-nam, for example, applying the IADPSGcriteria resulted in an increase in preva-lence of GDM from 6.1 to 20.3% (84).The offspring of mothers with GDM
have increased risks of obesity, hyper-tension, diabetes, and other noncom-municable diseases (78,79). Given thehigh risk ofGDMamongAsianpopulationsand the potential transgenerational ef-fects of GDM and maternal nutrition,there is an urgent need to implementpreconception interventions to optimizematernal health (85,86). Also, the highprevalence of GDM and its potentiallong-term effects makes a strong casefor universal screening for GDM in Asianpopulations. This has already been adoptedin some Asian countries (9).
Pattern of Diabetes Complications inAsia and Pacific CommunitiesThere are ethnic differences in the pat-tern of diabetes complications (54). Earlyobservations from the WHO Multi-national Study of Vascular Disease inDiabetes (WHO MSVDD) had suggestedcomparatively high rates of albuminuriain Asian centers (87). In an analysis of65,171 subjects with T2DM evaluatedin primary care in New Zealand between2000 and 2006 (including 3,166 SouthAsians and 1,941 East Asians), the risksof having microalbuminuria, macroalbu-minuria, and advanced proteinuria weresignificantly increased 1.4- to 4-fold in
Pacific Islanders, South Asians, and EastAsians compared with Europeans (88).Moreover, recent studies in multiethnicpopulations that compared diabetic re-nal disease among individuals of differ-ent ethnicities suggest that ethnicminorities in the U.S., including SouthAsians and Chinese, are more likely tosuffer from proteinuric diabetic renaldisease than from nonproteinuric dia-betic renal disease (89).
A meta-analysis of studies on theprevalence of diabetic retinopathynoted that South Asians had the low-est prevalence (90). A lower preva-lence of peripheral sensory neuropathywas also reported in Asian patients inthe Fremantle Diabetes Study (FDS) inAustralia compared with patients ofEuropean descent (91).
The prevalence of diabetes complica-tions in the Pacific region is higher thanthat reported for other regions (e.g.,Asia, Africa, and the Middle East) (14).Consistent with this, Pacific Islanders inthe U.S. have a comparatively high prev-alence of foot complications and ampu-tations (92).
In the WHO MSVDD, the prevalenceof cardiovascular complications washigh in South Asians, but in generalwas low in centers in China, Hong Kong,and Japan (93). More recent studies haveconfirmed these earlier observations. Forexample, other studies in multiethnicpopulations have noted the high preva-lence of cardiovascular complicationsamong South Asian populations, believedto be partly driven by their predispositionto visceral adiposity (6,13). In contrast,patients with T2DM in China appear tohave lower rates of cardiovascular com-plications compared with Europeans (94),and the application to Chinese popula-tions of risk scores developed in Europeanpopulations tends to overestimate therisk of coronary heart disease (95). Stud-ies that have compared the risk of periph-eral vascular disease have noted thatSouth Asians are at lower risk of amputa-tions than Europeans (96).
In addition to ethnic differences inthe risk of diabetes complications, thepattern of diabetes complications inAsia is also notable for the large propor-tion of individuals with young-onsetT2DM. In the Joint Asia Diabetes Evalu-ation (JADE) program, among 41,029patients recruited from across ninecountries/regions in Asia, 18% had
onset of T2DM below the age of 40(97), had longer disease duration, andhad higher rates of retinopathy andend-stage renal disease than those withonset of diabetes after the age of 40 (97).In the Hong Kong Diabetes Registry, pa-tients with young-onset diabetes hadhigher risks of incident cardiovascularand renal complications at any age, drivenby the longer disease duration (98). Giventhe proportion of patients with young-onset T2DM, the potential burden ofdiabetes-related complications is ofgreat concern.
Prevention of DiabetesPrimary prevention of diabetes is a prac-tical and cost-effective method of re-ducing incident diabetes in populationsof varied ethnicity and biological char-acteristics (99). Systematic long-termstudies conducted in Western nations,such as the U.S. (100) and Finland(101), have shown the benefits of usingintensive lifestyle modification (LSM)resulting in significant weight reductionin obese and overweight persons withIGT, leading to a 58% relative risk reduc-tion in diabetes (100). These programsin the Western countries (100) and inChina have also shown the enduringeffect of LSM, with the effects demon-strated to last at least 10–20 years(102,103).
Studies in the Asian populations, suchas the Da Qing studies in China (102,103),the Indian Diabetes Prevention Pro-gramme (IDPP) (104) in India, and theJapanese prevention programs (105,106),have shown that LSM is effective in pre-venting T2DM even in nonobese popula-tions with high levels of insulin resistanceand that this is achieved without sig-nificant weight reduction. Importantly,the 23-year Da Qing IGT and DiabetesStudy follow-up showed a sustained ben-eficial effect of LSM on diabetes incidenceand on cardiovascular and all-cause mor-tality in the Chinese population (102).Pragmatic, cost-effective, and scalableprograms are being tested in developedcountries and in South Asian countries(107). A recent study in India showedthat the cumulative incidence of diabe-tes in 2 years was significantly loweramong the people with prediabeteswho received frequent text messageson mobile phones on healthy lifestyleprinciples (18%) than among the controlgroup on standard care (27%) (108).
480 Implications of Diabetes in Asia and WPR Diabetes Care Volume 39, March 2016

Table
4—Randomize
dco
ntro
lledpreve
ntio
nstu
diesin
T2DM
inAsia
npopulatio
nsusin
glife
style
interventio
n
Studypopulatio
ncharacteristics
Mean
duratio
nParticip
antsbytreatm
ent
group
Cumulative
incid
ence
ofdiab
etesRelative
riskred
uctio
nStu
dy(year)
(Ref)
(years)(n)
(%)
(%)
DaQingIGTandDiab
etesStu
dy(1997)
(102)Chinese:
Totaln
=577
Contro
l:67.7
Diet:
31.0BMI:26.0
6Contro
l:133
Diet:
43.8Exercise:
46.0Age:
45.0Diet:
130Exercise:
41.1Diet
+exercise:
42.0Cluster
randomized
byclin
icExercise:
141Diet
+exercise:
46.0Diet
+exercise:
126
DaQingDiab
etesPreven
tion
Study(2008)
(103)Contro
lContro
l:138
Contro
l:93.0
43.0BMI:24.4
20Interven
tion:439
Interven
tion:80.0
Interven
tion
BMI:24.5
DaQingDiab
etesPreven
tion
Study(2014)
(103)Contro
lTo
taln=568
(byinterview
from
med
icalrecords)
Contro
l:89.9
45.0BMI:25.7
23Contro
l:138
Interven
tion:72.6
Interven
tion
Interven
tion:430
CVDmortality
41.0BMI:26.2
Contro
l:19.6
Interven
tion:11.9
All-cau
semortality
29.0Contro
l:38.4
Interven
tion:28.0
IDPP-1
(2006)(104)
BMI:25.8
2.6(m
edian
)To
taln=531
Contro
l:55.0
LSM:28.5
Age:
45.9Contro
l:136
LSM:39.3
Metfo
rmin:26.4
Persisten
tIGT,in
divid
ualran
domizatio
nLSM
:133
Metfo
rmin:40.5
LSM+metfo
rmin:28.2
Metfo
rmin:133
LSM+metfo
rmin:39.5
LSM+metfo
rmin:129
Indian
SMSstu
dy(2013)
(108)BMI:25.8
2Contro
l:266
Contro
l:27.4
Age:
45.9Interven
tion:271
Interven
tion:18.5
36.0Persisten
tIGT,m
en
Japan
esepreven
tionstu
dy(2005)
(105)Jap
anese
men
:4
Contro
l:102
Contro
l:9.3
67.4BMI:23.5
Interven
tion:356
Interven
tion:3.0
Age:
51.5IGT,in
divid
ualran
domizatio
n
Zensharen
StudyforPreven
tionof
LifestyleDiseases
(2011)(106)
Japan
esemen
:3
Contro
l:330
Contro
l:16.6
44.0BMI:27.0
Interven
tion:311
Interven
tion:12.2
Age:
49.0IGT,in
divid
ualran
domizatio
n
Age
givenas
mean
(years)andBMIgiven
asmean
(kg/m2).
CVD,card
iovascu
lardisease.
care.diabetesjournals.org Nanditha and Associates 481

Table 4 describes the major diabetesprevention studies in Asia using LSM(102–106,108).For any program to be successful at a
population level, major changes are re-quired at relevant personal, cultural, so-cietal, and community levels (109). Anexample of the principles laid out inthe Western Pacific Declaration on Dia-betes (110) being translated in actioncan be found in Singapore’s diabetesprevention efforts discussed below.
Preventing Diabetes in SingaporeAccording to the 2010 Singapore NationalHealth Survey, the crude diabetes preva-lence increased from 8.6% in 1992 to11.3% in 2010 (111). However, the age-standardized prevalence remained con-stant at ;11% during the two decades.Obesity prevalence has been rising in thelast decade from 6 to 11%. The effect ofrising obesity on diabetes prevalence willlikely only be evident in one to two de-cades. It is estimated that Singapore willhave half a million people with diabetesby 2020 and that this will rise to 1 millionby 2050, double an earlier projection thatwas based on aging alone (112). The pub-lic health policy implication is clearly notjust toward increasing the capability ofdealing with diabetes once it has arisen(increased capacity and new models ofcare) but also moving upstream to pri-mary prevention.The traditional approach to preventing
lifestyle-related diseases in Singapore isto provide public education with a strongemphasis on individual responsibility.Singapore’s Healthier Hawker Pro-gram provides a case study of this ap-proach. It is part of The Healthy LivingMaster Plan, a major paradigm shift rec-ognizing the need for multisectoral andintegrated approaches to intervention.Hawker centers are a quintessential
feature of the Singaporean food land-scape and house a variety of cookedfood stalls popular for their conve-nience, competitive prices, and diver-sity. In 2010, ;60% of Singaporeansate at least four times per week athawker centers, food courts, and coffeeshop stalls. Improving the nutritionalquality of foods sold at hawker centersprovides an important opportunity forwidespread dietary modification amongSingaporeans (113).The traditional model of workplace
safety and health in Singapore is focused
on prevention of accidents and occu-pational diseases. However, with theincreasing incidence and earlier onsetof diabetes and delay in the retire-ment age, there will be an increasingnumber of people with diabetes in theworking population. It was estimatedthat there were 180,000 people withdiabetes in Singapore’s working popu-lation in 2010. The cost to the econ-omy was $1 billion, primarily due toproductivity loss. This is ofmajor concernnot only to the government but also in-dividual employers. The Total WorkplaceSafety and Health (TWSH) system waslaunched jointly by the Ministries ofManpower and Health as a nationalprogram to provide a new model ofcare for the safety and health of theworking population (114).
CONCLUSIONS
The scenario presented in this reviewposes huge social and economic prob-lems to most nations in Asia and thePacific and is likely to impede nationaland indeed regional and global devel-opment. More action, particularly re-search, is required to understand thedrivers of the epidemic, particularlythose relating to developmental originsof T2DM, to provide a rationale for pre-vention strategies to address this risingpublic health “tsunami.” Primordialprevention strategies instituted in po-tential mothers, through prevention ofmalnutrition in utero and in childhood,and through healthy diets and adequatephysical activity (“life course approach”)are important additional elements to beincluded in future strategies for T2DMprevention (85). More action is alsoneeded to effectively implement life-style changes on a societal level tostem the tide of the epidemic. Unlessdrastic steps are taken through nationalprevention programs in Asia and the Pa-cific to curb the escalating trends in all ofthe countries, the social, economic, andhealth care challenges will be insur-mountable (1).
Because estimates of the diabetesburden have important implicationsfor future public health planning, it isessential that such estimates providereliable data. This review highlightsthe paucity of these data in a numberof Asian and Pacific nations and theneed for improving the collection of
epidemiological data and its interpreta-tion for public health planning to re-source and direct urgently neededprevention activities. This applies par-ticularly to lower- and middle-incomenations in these regions. India and Chinaalready have a huge burden from dia-betes, and they provide the largest di-aspora communities worldwide. Whatis already happening in Asia and thePacific in terms of the diabetes epi-demic and the complications and so-cioeconomic outcomes provides adaunting lesson for what can happenglobally.
Funding. R.C.W.M. acknowledges supportfrom the Research Grants Council Theme-based Research Scheme (T12-402/13N), theResearch Grants Council General ResearchFund (CU471713), and the European Foun-dation for the Study of Diabetes/ChineseDiabetes Society/Lilly Programme for Collab-orative Research Between China and Europe.J.E.S. is supported by a National Health andMedical Research Council Senior ResearchFellowship.Duality of Interest. No potential conflicts ofinterest relevant to this article were reported.Author Contributions. A.N., R.C.W.M., K.S.C.,J.E.S., and P.Z.Z. researched data, contributed todiscussion, and wrote, reviewed, and edited themanuscript. A.R., C.S., and J.C.N.C. contributedto discussion and reviewed and edited the man-uscript. All authors approved submission of themanuscript for publication.
References1. Zimmet PZ, Magliano DJ, Herman WH, ShawJE. Diabetes: a 21st century challenge. LancetDiabetes Endocrinol 2014;2:56–642. Guariguata L, Whiting DR, Hambleton I,Beagley J, Linnenkamp U, Shaw JE. Global esti-mates of diabetes prevalence for 2013 and pro-jections for 2035. Diabetes Res Clin Pract 2014;103:137–1493. Chan JC, Cho NH, Tajima N, Shaw J. Diabetesin the Western Pacific Region–past, present andfuture. Diabetes Res Clin Pract 2014;103:244–2554. Chan JC, Malik V, Jia W, et al. Diabetes inAsia: epidemiology, risk factors, and pathophys-iology. JAMA 2009;301:2129–21405. Ramachandran A, Snehalatha C, Ma RC. Di-abetes in South-East Asia: an update. DiabetesRes Clin Pract 2014;103:231–2376. Ramachandran A, Ma RCW, Snehalatha C.Diabetes in Asia. Lancet 2010;375:408–4187. Gluckman PD, Hanson MA, Cooper C,Thornburg KL. Effect of in utero and early-lifeconditions on adult health and disease. N Engl JMed 2008;359:61–738. Chan JCN, Yeung R, Luk A. The Asian diabetesphenotypes: challenges and opportunities.Diabetes Res Clin Pract 2014;105:135–1399. Tutino GE, Tam WH, Yang X, Chan JC, Lao TT,Ma RC. Diabetes and pregnancy: perspectivesfrom Asia. Diabet Med 2014;31:302–318
482 Implications of Diabetes in Asia and WPR Diabetes Care Volume 39, March 2016

10. InternationalDiabetesFederation. IDFDiabetesAtlas. 6th ed. Brussels, Belgium, InternationalDiabetes Federation, 2013. Available from www.idf.org/diabetesatlas. Accessed 31 March 201411. World Health Organization. STEPS countryreports [Internet]. Available from http://www.who.int/chp/steps/reports/en/. Accessed 31March 201412. Sherwin RS, Anderson RM, Buse JB, et al.;American Diabetes Association. The preventionor delay of type 2 diabetes. Diabetes Care 2003;26(Suppl. 1):S62–S6913. Misra A, Ramchandran A, Jayawardena R,Shrivastava U, Snehalatha C. Diabetes in SouthAsians. Diabet Med 2014;31:1153–116214. Tin ST, Lee CM, Colagiuri R. A profile of di-abetes in Pacific Island Countries and Territo-ries. Diabetes Res Clin Pract 2015;107:233–24615. Xu Y, Wang L, He J, et al.; 2010 China Non-communicable Disease Surveillance Group.Prevalence and control of diabetes in Chineseadults. JAMA 2013;310:948–95916. King H, Keuky L, Seng S, Khun T, Roglic G,Pinget M. Diabetes and associated disorders inCambodia: two epidemiological surveys. Lancet2005;366:1633–163917. Morimoto A, Nishimura R, Tajima N. Trendsin the epidemiology of patients with diabetes inJapan. Japan Med Assoc J 2010;53:36–4018. AdamFM, Adam JM, Pandeleki N,MappangaraI. Asymptomatic diabetes: the difference betweenpopulation-based and office-based screening. ActaMed Indones 2006;38:67–7119. Mihardja L, Delima, Manz HS, Ghani L,Soegondo S. Prevalence and determinants ofdiabetes mellitus and impaired glucose toler-ance in Indonesia (a part of basic health re-search/Riskesdas). Acta Med Indones 2009;41:169–17420. Australian Bureau of Statistics. AustralianHealth Survey: Biomedical results for chronicdiseases, 2011-12 [article online]. Availablefrom http://www.abs.gov.au/AUSSTATS/[email protected]/DetailsPage/4364.0.55.0052011-12. Ac-cessed 31 March 201521. Ministry of Health Brunei Darussalam. HealthInformation Booklet 2010. Bandar Seri Begawan,Brunei Darussalam, 2010. Available from http://www.moh.gov.bn/SiteCollectionDocuments/Health%20Indicator%20Booklet/HIB_2010.pdf.Accessed 12 April 201522. Ramachandran A, Snehalatha C, Shetty AS,Nanditha A. Trends in prevalence of diabetes inAsian countries. World J Diabetes 2012;3:110–11723. Siu SC, Wong KW, Lee KF, et al. Prevalenceof undiagnosed diabetes mellitus and cardio-vascular risk factors in Hong Kong professionaldrivers. Diabetes Res Clin Pract 2012;96:60–6724. University of Health Sciences and the Pre-ventiveMedicine Department of the Ministry ofHealth, Kingdom of Cambodia. Prevalence ofNon-Communicable Disease Risk Factors inCambodia. World Health Organization STEPSSurvey, Country Report. World Health Organiza-tion, Geneva, Switzerland, September 2010.Available from http://www.who.int/chp/steps/2010_STEPS_Report_Cambodia.pdf. Accessed 12April 201525. Hu D, Sun L, Fu P, et al. Prevalence and riskfactors for type 2 diabetes mellitus in the
Chinese adult population: the InterASIA Study.Diabetes Res Clin Pract 2009;84:288–29526. Wan Nazaimoon WM, Md Isa SH, WanMohamad WB, et al. Prevalence of diabetesin Malaysia and usefulness of HbA1c as adiagnostic criterion. Diabet Med 2013;30:825–82827. World HealthOrganization.Mongolian STEPSSurvey on the Prevalence of NoncommunicableDisease and Injury Risk Factors-2009. WorldHealth Organization, Geneva, Switzerland, 2010.Available from http://www.who.int/chp/steps/2009_STEPS_Report_Mongolia.pdf?ua=1. Ac-cessed 31 January 201428. Coppell KJ, Mann JI, Williams SM, et al.Prevalence of diagnosed and undiagnosed dia-betes and prediabetes in New Zealand: findingsfrom the 2008/09 Adult Nutrition Survey. N ZMed J 2013;126:23–4229. Kim DJ. The epidemiology of diabetes inKorea. Diabetes Metab J 2011;35:303–30830. Hwang J, Shon C. Relationship between so-cioeconomic status and type 2 diabetes: resultsfrom Korea National Health and Nutrition Exam-ination Survey (KNHANES) 2010-2012. BMJOpen 2014;4:e00571031. SingaporeMinistry ofHealth.DiseaseBurden.Diabetes prevalence in Singapore [Internet], 2015.Available from https://www.moh.gov.sg/content/moh_web/home/statistics/Health_Facts_Singapore/Disease_Burden.html. Accessed 12 April 201532. Deerochanawong C, Ferrario A. Diabetesmanagement in Thailand: a literature reviewof the burden, costs, and outcomes. GlobalHealth 2013;9:1133. Aekplakorn W, Chariyalertsak S, KessomboonP, et al.; ThaiNational Health Examination Survey IVStudy Group. Prevalence and management of di-abetes andmetabolic risk factors in Thai adults: theThai National Health Examination Survey IV, 2009.Diabetes Care 2011;34:1980–198534. Quang Binh T, Tran Phuong P, Thi Nhung B,et al. Prevalence and correlates of hyperglyce-mia in a rural population, Vietnam: implicationsfrom a cross-sectional study. BMC Public Health2012;12:93935. Zimmet PZ. Kelly West Lecture 1991. Chal-lenges in diabetes epidemiology–from West tothe rest. Diabetes Care 1992;15:232–25236. Prior IA, Davidson F. The epidemiology ofdiabetes in Polynesians and Europeans in NewZealand and the Pacific. N ZMed J 1966;65:375–38337. Zimmet P, Taft P, Guinea A, Guthrie W,Thoma K. The high prevalence of diabetes mel-litus on a Central Pacific Island. Diabetologia1977;13:111–11538. Zimmet P, Dowse G, Finch C, Serjeantson S,King H. The epidemiology and natural history ofNIDDM–lessons from the South Pacific. Diabe-tes Metab Rev 1990;6:91–12439. Collins VR, Dowse GK, Toelupe PM, et al.Increasing prevalence of NIDDM in the Pacificisland population of Western Samoa over a13-year period. Diabetes Care 1994;17:288–29640. Colagiuri S, Colagiuri R, Na’ati S, MuimuiheataS, Hussain Z, Palu T. The prevalence of diabetes inthekingdomofTonga.DiabetesCare2002;25:1378–138341. Feisul MI, Azmi S, Ed. National Diabetes Reg-istry Report, Volume1, 2009-2012 [Internet], 2013.
Kuala Lumpur, Ministry of Health Malaysia. Avail-able from http://www.moh.gov.my. Accessed 31March 201542. Saeed KM. Prevalence of risk factors fornon-communicable diseases in the adult popu-lation of urban areas in Kabul City, Afghanistan.Cent Asian J Glob Health 2013;14:38643. Akter S, Rahman MM, Abe SK, Sultana P.Prevalence of diabetes and prediabetes andtheir risk factors among Bangladeshi adults: anationwide survey. Bull World Health Organ2014;92:204–213, 213A44. Giri BR, Sharma KP, Chapagai RN, Palzom D.Diabetes and hypertension in urban Bhutanesemen and women. Indian J Community Med2013;38:138–14345. Ramachandran A, Snehalatha C, Kapur A,et al.; Diabetes Epidemiology Study Group inIndia (DESI). High prevalence of diabetes andimpaired glucose tolerance in India: NationalUrban Diabetes Survey. Diabetologia 2001;44:1094–110146. Anjana RM, Pradeepa R, Deepa M, et al.;ICMR–INDIAB Collaborative Study Group. Prev-alence of diabetes and prediabetes (impairedfasting glucose and/or impaired glucose toler-ance) in urban and rural India: phase I results ofthe Indian Council of Medical Research-INdiaDIABetes (ICMR-INDIAB) study. Diabetologia2011;54:3022–302747. Aboobakur M, Latheef A, Mohamed AJ,et al. Surveillance for non-communicable dis-ease risk factors in Maldives: results from thefirst STEPS survey in Male. Int J Public Health2010;55:489–49648. Magliano DJ, Soderberg S, Zimmet PZ, et al.Explaining the increase of diabetes prevalenceand plasma glucose in Mauritius. Diabetes Care2012;35:87–9149. Sharma SK, Ghimire A, Radhakrishnan J,et al. Prevalence of hypertension, obesity, dia-betes, and metabolic syndrome in Nepal. Int JHypertens 2011;2011:82197150. Shera AS, Jawad F, Maqsood A. Prevalenceof diabetes in Pakistan. Diabetes Res Clin Pract2007;76:219–22251. Jayawardena R, Ranasinghe P, Byrne NM,Soares MJ, Katulanda P, Hills AP. Prevalenceand trends of the diabetes epidemic in SouthAsia: a systematic review and meta-analysis.BMC Public Health 2012;25;12:38052. Anjana RM, Shanthi Rani CS, DeepaM, et al.Incidence of diabetes and prediabetes and pre-dictors of progression among Asian Indians:10-year follow-up of the Chennai Urban RuralEpidemiology Study (CURES). Diabetes Care2015;38:1441–144853. Ramachandran A, Mary S, Yamuna A,Murugesan N, Snehalatha C. High prevalenceof diabetes and cardiovascular risk factors asso-ciated with urbanization in India. Diabetes Care2008;31:893–89854. Ma RC, Chan JC. Type 2 diabetes in EastAsians: similarities and differences with popula-tions in Europe and the United States. Ann N YAcad Sci 2013;1281:64–9155. Hwang CK, Han PV, Zabetian A, Ali MK,Narayan KM. Rural diabetes prevalence quintu-ples over twenty-five years in low- and middle-income countries: a systematic review andmeta-analysis. Diabetes Res Clin Pract 2012;96:271–285
care.diabetesjournals.org Nanditha and Associates 483

56. Lee JW, Brancati FL, Yeh HC. Trends in theprevalence of type 2 diabetes in Asians versuswhites: results from the United States NationalHealth Interview Survey, 1997-2008. DiabetesCare 2011;34:353–35757. King GL, McNeely MJ, Thorpe LE, et al. Un-derstanding and addressing unique needs of di-abetes in Asian Americans, native Hawaiians,and Pacific Islanders. Diabetes Care 2012;35:1181–118858. Karter AJ, Schillinger D, Adams AS, et al.Elevated rates of diabetes in Pacific Islandersand Asian subgroups: The Diabetes Study ofNorthern California (DISTANCE). Diabetes Care2013;36:574–57959. Kanaya AM, Herrington D, Vittinghoff E,et al. Understanding the high prevalence ofdiabetes in U.S. south Asians compared withfour racial/ethnic groups: the MASALA andMESA studies. Diabetes Care 2014;37:1621–162860. Bhopal R, Unwin N, White M, et al. Hetero-geneity of coronary heart disease risk factors inIndian, Pakistani, Bangladeshi, and European or-igin populations: cross sectional study. BMJ1999;319:215–22061. Hu FB. Globalization of diabetes: the role ofdiet, lifestyle, and genes. Diabetes Care 2011;34:1249–125762. Ma RC, Lin X, Jia W. Causes of type 2 di-abetes in China. Lancet Diabetes Endocrinol2014;2:980–99163. Misra A, Khurana L, Isharwal S, Bhardwaj S.South Asian diets and insulin resistance. Br JNutr 2009;101:465–47364. Hu EA, Pan A, Malik V, Sun Q. White riceconsumption and risk of type 2 diabetes: meta-analysis and systematic review. BMJ 2012;344:e145465. Mohan V, Radhika G, Sathya RM, Tamil SR,Ganesan A, Sudha V. Dietary carbohydrates, gly-caemic load, food groups and newly detectedtype 2 diabetes among urban Asian Indian pop-ulation in Chennai, India (Chennai Urban RuralEpidemiology Study 59). Br J Nutr 2009;102:1498–150666. Henry CJ, Lightowler HJ, Newens K, et al.Glycaemic index of common foods tested inthe UK and India. Br J Nutr 2008;99:840–84567. Ng SW, Howard AG,Wang HJ, Su C, Zhang B.The physical activity transition among adults inChina: 1991-2011. Obes Rev 2014;15(Suppl. 1):27–3668. Nyamdorj R, Pitkaniemi J, Tuomilehto J,et al.; DECODA and DECODE Study Groups. Eth-nic comparison of the association of undiag-nosed diabetes with obesity. Int J Obes 2010;34:332–33969. Lear SA, Humphries KH, Kohli S,Chockalingam A, Frohlich JJ, Birmingham CL.Visceral adipose tissue accumulation differsaccording to ethnic background: results ofthe Multicultural Community Health Assess-ment Trial (M-CHAT). Am J Clin Nutr 2007;86:353–35970. WHO Expert Consultation. Appropriatebody mass index for Asian populations and itscomplications for policy and intervention strat-egies. Lancet 2004;363:157–16371. Huxley R, Barzi F, Lee CM, et al.; Obesity inAsia Collaboration. Waist circumference thresh-olds provide an accurate and widely applicable
method for the discrimination of diabetes. Di-abetes Care 2007;30:3116–311872. Cameron AJ, Sicree RA, Zimmet PZ, et al.Cut-points for waist circumference in Europidsand South Asians. Obesity (Silver Spring) 2010;18:2039–204673. Hales CN, Barker DJ. Type 2 (non-insulin-dependent) diabetes mellitus: the thrifty phe-notype hypothesis. Diabetologia 1992;35:595–60174. Ravelli AC, van der Meulen JH, Michels RP,et al. Glucose tolerance in adults after prena-tal exposure to famine. Lancet 1998;351:173–17775. Li Y, He Y, Qi L, et al. Exposure to the Chi-nese famine in early life and the risk of hyper-glycemia and type 2 diabetes in adulthood.Diabetes 2010;59:2400–240676. Yajnik CS. Nutrient-mediated teratogenesisand fuel-mediated teratogenesis: two pathwaysof intrauterine programming of diabetes. Int JGynaecol Obstet 2009;104(Suppl. 1):S27–S3177. Pettitt DJ, Aleck KA, Baird HR, Carraher MJ,Bennett PH, Knowler WC. Congenital suscepti-bility to NIDDM. Role of intrauterine environ-ment. Diabetes 1988;37:622–62878. Ma RC, Chan JC, Tam WH, Hanson MA,Gluckman PD. Gestational diabetes, maternalobesity, and the NCD burden. Clin Obstet Gyne-col 2013;56:633–64179. Ma RC, Tutino GE, Lillycrop KA, Hanson MA,Tam WH. Maternal diabetes, gestational diabe-tes and the role of epigenetics in their long termeffects on offspring. Prog Biophys Mol Biol2015;118:55–6880. Guariguata L, Linnenkamp U, Beagley J,Whiting DR, Cho NH. Global estimates of theprevalence of hyperglycaemia in pregnancy. Di-abetes Res Clin Pract 2014;103:176–18581. Wong VW. Gestational diabetes mellitus infive ethnic groups: a comparison of their clinicalcharacteristics. Diabet Med 2012;29:366–37182. Zhang F, Dong L, Zhang CP, et al. Increasingprevalence of gestational diabetes mellitus inChinese women from 1999 to 2008. DiabetMed 2011;28:652–65783. World Health Organization. DiagnosticCriteria and Classification of HyperglycaemiaFirst Detected in Pregnancy. World Health Orga-nization, Geneva, Switzerland, 2013. Availablefrom http://apps.who.int/iris/bitstream/10665/85975/1/WHO_NMH_MND_13.2_eng.pdf. Ac-cessed 20 April 201584. Hirst JE, Tran TS, Do MA, Morris JM, JefferyHE. Consequences of gestational diabetes in anurban hospital in Viet Nam: a prospective cohortstudy. PLoS Med 2012;9:e100127285. Hanson MA, Gluckman PD, Ma RC, MatzenP, Biesma RG. Early life opportunities for pre-vention of diabetes in low and middle incomecountries. BMC Public Health 2012;12:102586. Hanson MA, Bardsley A, De-Regil LM, et al.The International Federation of Gynecology andObstetrics (FIGO) recommendations on adoles-cent, preconception, and maternal nutrition:“Think Nutrition First.” Int J Gynaecol Obstet2015;131(Suppl. 4):S21387. Bennett PH, Lee ET, Lu M, Keen H, Fuller JH.Increased urinary albumin excretion and its as-sociations in the WHO Multinational Study ofVascular Disease in Diabetes. Diabetologia2001;44(Suppl. 2):S37–S45
88. Kenealy T, Elley CR, Collins JF, Moyes SA,Metcalf PA, Drury PL. Increased prevalence ofalbuminuria among non-European peoples withtype 2 diabetes. Nephrol Dial Transplant 2012;27:1840–184689. Bhalla V, Zhao B, Azar KM, et al. Racial/eth-nic differences in the prevalence of proteinuricand nonproteinuric diabetic kidney disease. Di-abetes Care 2013;36:1215–122190. Yau JW, Rogers SL, Kawasaki R, et al.; Meta-Analysis for Eye Disease (META-EYE) StudyGroup. Global prevalence and major risk fac-tors of diabetic retinopathy. Diabetes Care2012;35:556–56491. Tan ED, Davis WA, Davis TM. Changesin characteristics and management of Asianand Anglo-Celts with type 2 diabetes over a15-year period in an urban Australian commu-nity: The Fremantle Diabetes Study. J Diabetes.12 January 2015 [Epub ahead of print]. DOI:10.1111/1753-0407.1226792. Kanaya AM, Adler N, Moffet HH, et al. Het-erogeneity of diabetes outcomes among Asiansand Pacific Islanders in the US: the DiabetesStudy of Northern California (DISTANCE). Diabe-tes Care 2011;34:930–93793. Chi ZS, Lee ET, Lu M, Keen H, Bennett PH.Vascular disease prevalence in diabetic patientsin China: standardised comparison with the 14centres in the WHO Multinational Study of Vas-cular Disease in Diabetes. Diabetologia 2001;44(Suppl. 2):S82–S8694. Clarke PM, Glasziou P, Patel A, et al.;ADVANCE Collaborative Group. Event rates,hospital utilization, and costs associated withmajor complications of diabetes: a multicountrycomparative analysis. PLoSMed2010;7:e100023695. Yang X, So WY, Kong AP, et al. Developmentand validation of a total coronary heart diseaserisk score in type 2 diabetes mellitus. Am J Car-diol 2008;101:596–60196. Chaturvedi N, Abbott CA, Whalley A,Widdows P, Leggetter SY, Boulton AJ. Risk ofdiabetes-related amputation in South Asiansvs. Europeans in the UK. Diabet Med 2002;19:99–10497. Yeung RO, Zhang Y, Luk A, et al. Metabolicprofiles and treatment gaps in young-onsettype 2 diabetes in Asia (the JADE programme):a cross-sectional study of a prospective cohort.Lancet Diabetes Endocrinol 2014;2:935–94398. Chan JC, Lau ES, Luk AO, et al. Prematuremortality and comorbidities in young-onset di-abetes: a 7-year prospective analysis. Am J Med2014;127:616–62499. Ramachandran A, Snehalatha C. Diabetesprevention programs. Med Clin North Am2011;95:353–372, viii100. Knowler WC, Fowler SE, Hamman RF, et al.;Diabetes Prevention Program Research Group.10-year follow-up of diabetes incidence andweight loss in the Diabetes Prevention ProgramOutcomes Study. Lancet 2009;374:1677–1686101. Tuomilehto J, Lindstrom J, Eriksson JG,et al.; Finnish Diabetes Prevention Study Group.Prevention of type 2 diabetes mellitus bychanges in lifestyle among subjects with im-paired glucose tolerance. N Engl J Med 2001;344:1343–1350102. Pan XR, Li GW, Hu YH, et al. Effects of dietand exercise in preventing NIDDM in peoplewith impaired glucose tolerance. The Da Qing
484 Implications of Diabetes in Asia and WPR Diabetes Care Volume 39, March 2016

IGT and Diabetes Study. Diabetes Care 1997;20:537–544103. Li G, Zhang P, Wang J, et al. Cardiovascularmortality, all-cause mortality, and diabetes in-cidence after lifestyle intervention for peoplewith impaired glucose tolerance in the DaQing Diabetes Prevention Study: a 23-year follow-up study. Lancet Diabetes Endocrinol 2014;2:474–480104. Ramachandran A, Snehalatha C, Mary S,Mukesh B, Bhaskar AD, Vijay V; Indian DiabetesPrevention Programme (IDPP). The Indian Dia-betes Prevention Programme shows that life-style modification and metformin preventtype 2 diabetes in Asian Indian subjects withimpaired glucose tolerance (IDPP-1). Diabetolo-gia 2006;49:289–297105. Kosaka K, NodaM, Kuzuya T. Prevention oftype 2 diabetes by lifestyle intervention: a Jap-anese trial in IGT males. Diabetes Res Clin Pract2005;67:152–162
106. Saito T, Watanabe M, Nishida J, et al.;Zensharen Study for Prevention of Lifestyle Dis-eases Group. Lifestyle modification and preven-tion of type 2 diabetes in overweight Japanesewith impaired fasting glucose levels: a random-ized controlled trial. Arch Intern Med 2011;1715:1352–1360107. Ramachandran A, Snehalatha C, Shetty SA,Nanditha A. Primary prevention trials in type 2diabetes. InGlobal Health Perspectives in Prediabe-tes and Diabetes Prevention. Bergman M, Ed. Sin-gapore,World ScientificPublication, 2014, p. 49–74108. Ramachandran A, Snehalatha C, Ram J,et al. Effectiveness of mobile phone messagingin prevention of type 2 diabetes by lifestylemodification in men in India: a prospective,parallel-group, randomised controlled trial.Lancet Diabetes Endocrinol 2013;1:191–198109. Chan JC, Zhang Y, Ning G. Diabetes in China:a societal solution for a personal challenge. LancetDiabetes Endocrinol 2014;2:969–979
110. Western Pacific Declaration on Diabetes[Internet], 2001. Available from http://www.wpdd.org/. Accessed 20 April 2015111. Ministry ofHealth Singapore.NationalHealthSurvey 2010 [Internet], 2011. Available fromhttp://www.moh.gov.sg/content/moh_web/home/Publications/Reports/2011/national_health_survey2010.html. Accessed 10 April 2015112. Phan TP, Alkema L, Tai ES, et al. Forecast-ing the burden of type 2 diabetes in Singaporeusing a demographic epidemiological model ofSingapore. BMJ Open Diabetes Res Care 2014;2:e000012113. Ang HS. Singapore’s Healthier HawkerProgramme. Paper presented at the Culinary In-stitute of America, 15th Annual Worlds of FlavorConference, 1–3 November 2012, St. Helena, CA114. Chia SE, Chia A, Sng J. A total workplacesafety and health service - what are the impli-cations for the employees and employers? AnnAcad Med Singapore 2014;43:475–476
care.diabetesjournals.org Nanditha and Associates 485