Embed Size (px)
DESCRIPTION
EMT Basic Diabetic A&P and related EMS Signs & symptoms with treatment.
Citation preview

Humongous Insurance
Diabetes

Diabetes (Terms)
• Diabetes mellitus – (DM) A chronic disease characterized by an altered relationship between sugar (glucose) and insulin.

Diabetes
• Insulin – A hormone secreted by the pancreas that is needed to promote the movement of glucose (sugar) from the blood into the cells.
• Glucose – A simple form of sugar, the body’s main source of energy.

Diabetes
• Type I (IDDM)- Insulin dependent diabetes mellitus, usually acquired in childhood, produce no insulin (inheritable, auto-immune)– Requires insulin administration

Diabetes
• Type II (NIDDM) – Non-insulin dependent diabetes mellitus, usually acquired in adulthood (related to overweight), produce some insulin – not enough, or tissue sensitivity diminished– Can be controlled by diet, exercise, oral meds

Role of the Pancreas
• Primary role is the regulation of blood glucose concentrations.

DiabetesRole of the Pancreas
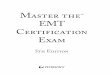
• Islets of Langerhans produce insulin– Alpha cells – Glucagon– Beta cells – Insulin– Delta cells – Somatostatin (inhibits the
secretaries of growth hormone)

Islets of Langerhans

DiabetesBeta Cells
• Insulin– Increase glucose transport into the cell– Increase liver glycogen levels (storage)– Decrease blood glucose concentration– Glucagon Antagonist

DiabetesAlpha Cells
• Glucagon –– Released when blood sugar levels drop– Increase blood glucose levels– Breaks down fats and fatty acids (storage
removal)– Insulin Antagonist

High/Low Blood Sugar

DiabetesGlucagon
• Triggered by exercise, stress, sleep, hypoglycemia
• Insulin antagonist (decreases insulin’s actions)

DiabetesLong Term Effects
• Blindness• Kidney disease• Peripheral neuropathy• Heart disease and stroke
(atherosclerosis)– HD: 2X - 4X non-diabetic– S: 2X - 6X non-diabetic
• Limb amputations

Diabetes• Hyperglycemia – Lack of insulin, glucose
cannot enter the cells. Remains in the blood stream increases the level of blood sugar.
• Hypoglycemia (Insulin Shock) – Lack of glucose in the blood stream, cells deprived of glucose.
• Normal sugar level – 80-120 mg/dL

DiabetesOnset
• Type I – May occur at birth, usually occurs in teenage or young adult years– Typically a sudden onset of – Polyuria (excessive urination), – Polydipsia (excessive thirst), – Polyphagia (excessive ingestion of food), dizziness,
blurred vision, rapid and unexplained weight loss.

DiabetesOnset
• Type II – – Generally occurs in patients older than 40 y/o– Overweight patients– Same onset S/S as Type I and fatigue, changes in
appetite.
Get Off MeWoman!!!

DiabetesHypoglycemia (Insulin Shock)
• Hypo (Low), Glyce (Sugar), Emia (Blood)
• Excessive response to glucose absorption– Physical exertion– Alcohol– Drug effects– Pregnancy– Poor dietary intake

DiabetesHypoglycemia (Insulin Shock)
• Adult– Blood sugar less than 80 mg/dL (non-diabetic)– Blood sugar less than 110 mg/dL (diabetic)
• Pediatric– Blood sugar less than 60 mg/dL (non-diabetic)– Blood sugar less than 90 mg/dL (diabetic)

DiabetesHypoglycemia (Insulin Shock)
• Too much insulin• Decreased dietary intake (missed
meal)• Vigorous activity

Diabetes
Hypoglycemia (Insulin Shock)• S/S
– Rapid onset– Nervousness– Irritability– Combative
behavior– Weakness– Confusion
– Appearance of intoxication
– Weak, rapid pulse– Cold, clammy skin– Drowsiness– Seizures
– Coma (severe case)

Hyperglycemia
• Hyper (High), Glyce (Sugar), Emia (Blood)
• Slow onset• Absence or lack of insulin• Glucose accumulates in the blood• Cells are starved
– Search for alternate fuel • Excessive urination (dehydration)

Hyperglycemia Diabetic Ketoacidosis
(DKA)• Results in a low pH
(acidosis)– Fruity breath
• Vomiting, dehydration, altered electrolyte balance, seizures
• Abnormal breathing pattern.– Kussmaul respirations
• Deep & fast• Warm, dry skin

Hyperosmolar Hyperglycemic Nonketotic
(HHNK) Coma• Life-threatening emergency• Older patients with type 2 diabetes or
undiagnosed diabetics• Causes• Precipitating factors• Signs and symptoms

Pathophysiology of HHNK Coma

Diabetic Emergency Management• Scene Size Up / BSI• Initial Assessment
– LOC– ABC’s– C/C– Priority/Transport

Diabetic Emergency Management
• Focused History and Physical Examination/Rapid Assessment– Responsive - Focused – Unresponsive – Rapid Medical Assessment
• OPQRST• SAMPLE

Diabetic Emergency Management
• OPQRST– Onset– Provocation– Radiating– Quality– Severity– Time
• SAMPLE– Signs & Symptoms– Allergies– Medications– Past Medical Hx– Last oral intake– Events Leading to 911
call

Diabetic Emergency Management
– Glynase– Tolinase– Glucotrol– Humalog– Rezulin– Glucophage
• Common Meds identified in SAMPLE:– Insulin– Diabanese– Orinase– Micronase– Diabeta

Diabetic Emergency Management
• Treatment– High flow oxygenation
• (BVM vs. NRB)
– Suction• Oral/nasal airway

Diabetic Emergency Management• Can the Patient Swallow?
– If so, oral glucose PO– If not, NPO, rapid transport
• Oral glucose:– Raises the blood sugar, may take as long as 20
min.– Indications – Altered mental status, history of
diabetes, ability to swallow– Page 475

Oral Glucose Drug Sheet

Oral Glucose• Class: Carbohydrates• Route: Oral• Supplied: Squeezable Tubes• Dose:
– Adult: Full Tube (25-50gm) given in small doses– Pediatric: 0.5 gm/kg given in small doses

Oral Glucose Cont.• Drug Action: Increases Blood Glucose Level• Indications:
– Altered mental status caused by hypoglycemia:– Adult
• Blood sugar less than 80 mg/dL (non-diabetic)• Blood sugar less than 110 mg/dL (diabetic)
– Pediatric• Blood sugar less than 60 mg/dL (non-diabetic)• Blood sugar less than 90 mg/dL (diabetic)

Oral Glucose Cont.• Precautions:
– Assure gag reflex is present• Side Effects: Aspiration• Contraindications:
– Absent gag reflex– Patents unable to protect their airway– Patents unable to swallow.

Diabetic Emergency Management
• Baseline Vital Signs (Q 5 or 15 min)• Detailed Patient Assessment• Ongoing Assessment
– ABC– LOC– Consider other causes

Scenarios

Scenario 1
• Dispatched to an unconscious person. 32 y/o female. She has a history of DM.
• S/S – Sudden onset of altered LOC, did not eat supper, cool moist skin, rapid thready pulse, did take insulin.

What is the level?

What is wrong with her?
• Hypoglycemic• Treatment
– High flow oxygenation – Suction Oral/nasal airway if needed – Oral glucose PO if able to swallow– If not, rapid transport

Scenario 2
• Dispatched to a 46 y/o old male. Large patient, family brings meds to you. They include Diabeta.
• Patient has not been feeling well for the past day or so.

Scenario 2
• S/S: Rapid and deep respirations, skin warm and dry, dry mucous membranes, patient exhibiting bizarre behavior, pulse rapid and thready, history of Polyuria, Polydypsia, and Polyphagia.

What is wrong with him?
• Hyperglycemia or DKA• Treatment:
– High flow oxygenation – Anything else?– Rapid transport

Scenario 3
• Dispatched to 80 y/o for altered mental status. History of diabetes that is normally controlled with insulin.
• S/S: Nausea, vomiting, irritability, altered mental status, weak, rapid pulse, and no range of motion of the right side of body.

What is wrong with her?
• CVA or Stroke• Treatment:
– High flow oxygenation – Anything else?– Rapid transport

Other factors to consider
• Intoxication• Other causes of AMS

Glucometer• A device used to determine blood
glucose levels.

Indications for blood sugar analysis
• Altered Mental Status• Unconscious patients of unknown cause• Suspected diabetic patients

Procedure
• Clean finger with alcohol
• Wipe dry• Wipe away first
drop of blood• Use second drop
of blood

Abnormal Glucose Values
• Outside the normal range (60-120)– Hyperglycemia – Greater than 300– Hypoglycemia – Less than 60

Conditions Diminishing Accuracy
• Margin of error (10-15%)
• Missing calibration
• Temperatures• Outdated strips• Improper
technique
• Insufficient sample size
• Contamination• Wrong sample
source• Neonates

Review

Review• IDDM
– Insulin Dependant Diabetic– Type I

Review• NIDDM
– Non-insulin Dependant Diabetic– Type II

Review
• 3 P’s–Polydipsia–Ployphagia–Polyuria

Review• Hypoglycemia• Adult
– Blood sugar less than 80 mg/dL (non-diabetic)– Blood sugar less than 110 mg/dL (diabetic)
• Pediatric– Blood sugar less than 60 mg/dL (non-diabetic)– Blood sugar less than 90 mg/dL (diabetic)

Review• Hyperglycemia
– >120 mg/dl

Review• DKA
– Diabetic Ketoacidosis– Kussmaul Respirations– D-stick normally > 350 mg/dl

The End
•Questions?






![EmS: PS-10 · information from EMS providers nationwide. As one EMS leader pointed out: “There is an illusion that EMS is so safe now - [we] have forgotten how inherently dangerous](https://img.dokumen.tips/doc/110x75/5f0c9c0f7e708231d43641ad/ems-ps-10-information-from-ems-providers-nationwide-as-one-ems-leader-pointed.jpg)