Embed Size (px)
Citation preview


Diabetes: 'dia' = through - 'betes' = to go
1500 B.C. Ancient Egyptians had a number of remedies for combating the passing of too much urine (polyuria). Hindus in the Ayur Veda recorded that insects and flies were attracted to the urine of some people, that the urine tasted sweet, and that this was associated with certain diseases.
1000 B.C. The father of medicine in India, Susruta of the Hindus, diagnosed Diabetes Mellitus (DM).
Early Greeks had no treatment for DM, latter Greeks like Aretaeus, Celsus and Galen described DM. Celsus described the pathologic condition "diabetes"

Diabetes: 'dia' = through - 'betes' = to go
1798 A.D. John Rollo certifies excess sugar in the blood.
1889 A.D. Mehring and Minkowski produce DM in dogs by removing the
pancreas.
1921 A.D. Banting and Best find insulin is secreted from the islet cells of the
pancreas.

Diabetes is a disease that is the 5th leading
cause of death in the USA

23.6 Million Americans have
Diabetes (8% pop)
More have pre-diabetes
There are two (or 3) different types
of diabetes and the diseases are very
different

There are three categories of diabetes
mellitus:
Insulin-Dependent Diabetes Mellitus (IDDM) [also called "Type 1" diabetes]
and Non Insulin-Dependent Diabetes Mellitus
(NIDDM)["Type 2"]
Inherited Forms of Diabetes Mellitus (MODY)

There are three categories of diabetes mellitus:
IDDM (also called Type 1 diabetes) is characterized by little (hypo) or no circulating insulin;
most commonly appears in childhood.
It results from destruction of the beta cells of the islets. The destruction results from a cell-mediated
AUTOIMMUNE ATTACK of the beta cells. What triggers this attack is still a mystery
IDDM is controlled by carefully-regulated injections of insulin.
(Insulin cannot be taken by mouth)


Inhalable insulin was introduced in mid-2006
The first such product to be marketed was Exubera, a powdered form of recombinant human insulin, delivered through an inhaler into the lungs
where it is absorbed. Once it has been absorbed, it begins working within the body over the next few hours. Diabetics still need to take a longer
acting basal insulin by injection.It has been concluded that inhaled insulin "appears to be as effective, but
no better than injected short-acting insulin. The additional cost is so much more that it is unlikely to be cost-
effective."[\
In October 2007, Pfizer announced that it would be discontinuing the production and sale of Exubera due to poor sales.
Several other companies are developing inhaled forms of the drug to reduce the need for daily injections among diabetics.
PFIZER LOSS = 2.8 billion

For many years, insulin extracted from the glands of cows and pigs was used. However, pig insulin differs from human insulin by one amino acid;
beef insulin by three. Although both work in humans to lower blood sugar, they are seen by the immune system as "foreign" and induce an
antibody response in the patient that blunts their effect and requires higher doses.
Two approaches were taken to solve this problem:

There are three categories of diabetes mellitus:
Two approaches have been taken to solve this problem:
Convert pig insulin into human insulin by removing the one amino acid that distinguishes them and replacing it with the human
version.
This approach is expensive, so now the favored approach is to Insert the human gene for insulin into E.coli and grow recombinant
human insulin in culture tanks. Insulin is not a GLYCOPROTEIN so E. coli is able to manufacture a
fully-functional molecule (trade name = Humulin). Yeast is also used (trade name = Novolin).
Recombinant DNA technology has also made it possible to manufacture slightly-modified forms of human insulin that work
faster (Humalog® and NovoLog®) or slower (Lantus®) than regular human insulin.

Each cell has thousands of
proteins.In many cases a
missing or defective protein
has no effect

Inherited Forms of Diabetes Mellitus
Some cases of diabetes result from mutant genes inherited from one or both parents.
Examples: mutant genes for one or another of the transcription factors needed
for transcription of the insulin gene .
mutations in one or both copies of the gene encoding the insulin receptor.
These patients usually have extra-high levels of circulating insulin but defective receptors.
The mutant receptors may fail to be expressed properly at the cell surface or
may fail to transmit an effective signal to the interior of the cell.

Diagnostic Diabetes: diagnosing maturity-onset
diabetes of the young (MODY)

Diagnosing MODY
• What is MODY?• Different types of MODY
- Glucokinase MODY- Transcription factor MODY
• Separate from Type 1, Type 2 and genetic syndromes

MODY (inherited)
MODY is caused by a change in a single gene. 6 genes have been identified that account for 87% of
MODY:
HNF1-a Glucokinase
HNF1-b HNF4-a IPF1
Neuro D1
MOST ARE TF’s that modulate insulin transcription
Important to diagnose MODY

Diabetes in Young Adults (15-30 years)
Age of diagnosis 5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80 85 90
Type 2
Type 1
MODY
MIDD

Diagnostic criteria for MODY
Tattersall (QJM 1974)
•Early-onset diabetes
•Not insulin-dependent diabetes
•Autosomal dominant inheritance•Caused by a single gene defect altering beta-cell function, obesity unusual
Diagnosis of diabetes before 25 years in at least 1 & ideally 2 family members
Off insulin treatment or measurable C-peptide at least 3 (ideally 5) years after diagnosis
Must be diabetes in one parent (2 generations) and ideally a grandparent or child ( 3 generations)
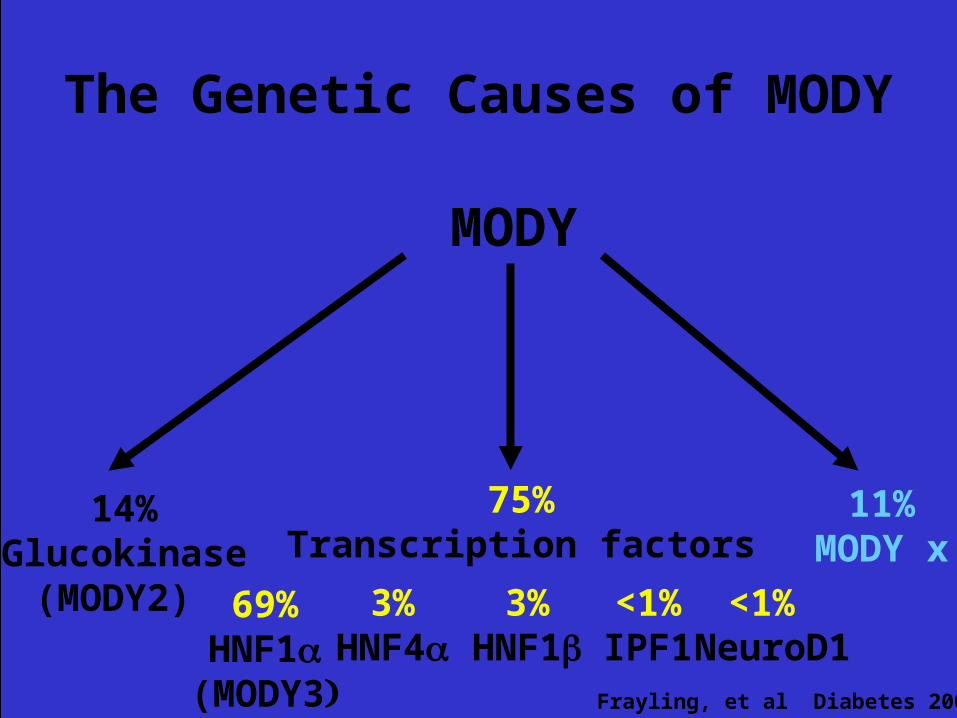
MODY
11%MODY x
75%Transcription factors
14%Glucokinase
(MODY2) 3%HNF1
69%HNF1
(MODY3
3%HNF4
<1%IPF1
The Genetic Causes of MODY
Frayling, et al Diabetes 2001
<1% NeuroD1

Two subtypes of MODY Glucokinase and Transcription
factor
0
4
8
12
16
20
0 20 40 60 80 100
Age (yr..)
Glucose (mmol/l)
..
Normal
Glucokinase
Transcription factor
(HNF-1
Pearson, et al Diabetes 2001

Transcription factormutations
Glucokinasemutations
Glucokinase and Transcription factor diabetes
MODY
Onset at birthStable hyperglycemiaDiet treatmentComplications rare
Adolescence/young adult onsetProgressive hyperglycemia1/3 diet, 1/3 other, 1/3 InsulinComplications frequent
(HNF-1HNF-1HNF-4

MODYDiagnostic Genetic Testing: why do
it?
• Makes diagnosis : defines monogenic and defines subtype
• Differentiates from type 1
• Helps define prognosis
• Helps family counselling
• Helps treatment decisions

Inherited Forms of Diabetes Mellitus
a mutant version of the gene encoding glucokinase, the enzyme that phosphorylates glucose in the first step of glycolysis.
Mutant version of insulin gene TFs
mutations in the gene encoding part of K+channel in the plasma membrane of the cell. The channels fail to close properly
causing the cell to become hyperpolarized and blocking insulin secretion.
mutations in several mitochondrial genes which reduce insulin secretion by cells. These diseases are inherited from the mother
as only her mitochondria survive in the fertilized egg. While symptoms usually appear in childhood or adolescence, patients with inherited diabetes differ from most children with NIDDM in having a history of diabetes in the family and not
being obese.

Inherited Forms of Diabetes Mellitus
MODY GENES like Mutant glucokinase
insulin gene TFs
K+channel of the cell.
IR
some mitochondria genes

Of 20+ million Americans with Diabetes, only
10% have type I diabetes

Most diabeticsHave Type II
diabetesT2DM or NIDDM

90% of diabetics in industrialized
nations have Type II diabetes

Type II diabetesDefined by
insulin resistanceinsulin
resistance-inability to respond to
insulin

Hyperglycemia causes
retinopathy, neuropathy, and
nephropathy

Type II diabetes-patients are
insulin resistance so can’t get
glucose into cells

How do you get high blood glucose?
Glucose comes from the food you eat and is also made in your liver and muscles.
Your blood carries the glucose to all the cells in your body.
Insulin controls glucose disposal into fat and skeletal muscle
The pancreas releases insulin into the blood.
Insulin helps the glucose from food get into your cells. If your body doesn't make enough insulin or if the insulin
doesn't work the way it should, glucose can't get into your cells. It stays in your blood instead. Your blood
glucose level then gets too high, causing pre-diabetes or diabetes.
Type II diabetes research related
to adipocytes

accumulate lipid
insulin sensitiveEndocrine functions
Adipocytes
accumulate lipid
insulin sensitive
Endocrine function

Most patients with Type II diabetes
are obese > 85%

Strong link between T2DM
and Obesity

Many diseases due to loss or defect of
one proteinSickle Cell Anemia
Huntington’s Disease
Type I DiabetesMODY

Many diseases due to loss or
defects in many proteins
Heart DiseaseCancer
Type II Diabetes

Very hard to cure diseases
that have multiple proteins
defective
What is pre-diabetes?
Pre-diabetes is a condition in which blood glucose levels are higher than normal but are not high
enough for a diagnosis of diabetes. People with pre-diabetes are at increased risk for
developing type 2 diabetes and for heart disease and stroke.
The good news is if you have pre-diabetes, you can reduce your risk of getting diabetes. With modest weight loss and moderate physical
activity, you can delay or prevent type 2 diabetes and even return to normal glucose levels.

How does Exercise work
Exercise results in an increase in GLUT4 vesicles moving to the PMThe effect is independent of insulin
The effects of insulin and exercise are additive.
Exercise, even in the absense of WEIGHT LOSScan reduce blood glucose levels and increase insulin
sensitivity

What are the signs of diabetes?
being very thirsty urinating often
feeling very hungry or tired losing weight without trying having sores that heal slowly
having dry, itchy skin losing the feeling in your feet or having tingling in
your feet having blurry eyesight
may have had one or more of these signs before you found out you have diabetes. Or may have had no signs at all.
A blood test to check your glucose levels will show if you have pre-diabetes or diabetes.

A1C, also known as glycated hemoglobin or glycosylated hemoglobin, indicates a patient's blood sugar control over the last 2-3 months.
A1C is formed when glucose in the blood binds irreversibly to hemoglobin to form a stable glycated
hemoglobin complex. Since the normal life span of red blood cells is 90-120
days, the A1C will only be eliminated when the red cells are replaced; A1C values are directly
proportional to the concentration of glucose in the blood over the full life span of the red blood cells.


A1C values are not subject to the fluctuations that are seen
with daily blood glucose monitoring.The A1C value is an index of mean blood glucose over the
past 2-3 months but is weighted to the most recent glucose values.
Values show the past 30 days as ~50% of the A1C, the preceding 60 days giving ~25% of the value and the
preceding 90 days giving ~25% of the value. This bias is due to the body's natural destruction and replacement of RBC. Because RBCs are constantly being destroyed and replaced, it does not take 120 days to detect a clinically
meaningful change in A1C following a significant change in mean blood glucose.

WHY IS IT SO HARD TO TREAT NIDDM

Medications for NIDDM
Many types of diabetes pills can help people with T2DM lower their blood glucose.
Each type of pill helps lower blood glucose in a different way.
Sulfonylureas- stimulate your pancreas to make more insulin.
Biguanides decrease the amount of glucose made by your liver.
glucosidase inhibitors slow the absorption of the starches you eat.

Medications for NIDDM
Thiazolidinediones TZDs-make you more sensitive to insulin.
Meglitinides -stimulate your pancreas to make more insulin.
D-phenylalanine derivatives -help your pancreas make more insulin quickly.
Combination oral medicines put together different kinds of pills.

Gila monsters are one of only
two venomous lizards in the world, the other being the closely related beaded lizards

A fairly new diabetes treatment from Eli Lilly and
Amylin that is extracted from the saliva of the Gila monster received approval from the Food and Drug Administration in April 2005
Byetta, which was co-developed by both companies, improves blood sugar control in patients with type 2 diabetes. The drug, developed from a compound in the toxic saliva of a rare lizard found only in the Southwest U.S. and Mexico.
Came on Market in June of 2005Used in patients who aren't getting enough insulin
through oral medication

DRAWBACK:
Has to be injected twice a day

Some History
• 1980s an endocrinologist named Dr. John Eng worked of the VA Medical Center in the Bronx His mentor - Dr. Rosalyn S. Yalow, won the 1977 Nobel Prize in Physiology or Medicine for the development of RIAs of peptide hormones.
• Dr. Eng wanted to discover new hormones.
RIA are insensitive and not a good way to discover new hormones. But chemical assays are sensitive. So he developed a new type of chemical assay and looked for hormones that no one had discovered.

Some History
• Dr. Eng first discovered a new hormone in the venom of the Mexican beaded lizard, which in 1990 he named exendin-3. But this hormone was vasoactive, which means that it contracts or dilates blood vessels.
• Prompted Dr. Eng to look at the venom of the Gila monster, which is not vasoactive. There he discovered a hormone, which he named exendin-4, that was similar in structure to glucagon-like peptide 1 (GLP-1).
Some History
• GLP-1 regulates blood glucose and satiety, as a potential drug it has a short half-life requiring multiple daily injections. He published his key paper on exendin-4 in a 1992 issue of The Journal of Biological Chemistry.
• But exendin-4 works for 12 or more hours. "That's how it is better," Dr. Eng says. So, Amylin Pharmaceuticals invested millions of dollars to develop it.

Some History
• When Dr. Eng began to realize exendin-4's potential to control diabetes, he told the Department of Veterans Affairs that the agency should patent it. " VA declined, because at that time inventions must be veteran specific," he recalls. The VA did retain a royalty-free license.
• "That put me in a difficult position," he says, "because it meant I had to essentially make a bet. Patenting it came out of my pocket with no guarantee that anything would come of it. I ended up with this patent, and I couldn't develop it. So I went around to drug companies."

Some History
• Finally, in 1996, Dr. Eng licensed the patent to Amylin, which calls it AC2993. The company completed the Phase 1 study in 1998 and filed an investigational new drug application with the FDA in 1999. Phase 2 studies, announced at the ADA's 2001 Annual Meeting, showed an approximate 1% reduction in A1c after 28 days. Since A1c measures average blood glucose of the past 2-3 months, this is a lot.
• Amylin had success in Phase 3 trials.

Some History
• Used by 2 injections a day. "The initial target population is for people with NIDDM who have not progressed to taking insulin," "It stimulates insulin production when it is needed and is only active when glucose is high." It also reduces appetite, causing some weight loss.
• Amylin is also working on alternatives to shots and a long-acting formulation of one shot a month, AC2993 LAR.

Some History
• Who would have imagined that a Gila monster could be so valuable to people with diabetes? But Dr. Eng did. Ironically, the venom he worked with came from a lab in Utah, and he says he has never seen a Gila monster.

Not as many proteins as we thought.Not surprising we have some "super-genes“like one
that encodes glucagon (increases glucose). As it turns out, the gene for glucagon also codes
for at least 2 other hormones, called glucagon-like peptides 1 and 2 (GLP-1, GLP-2). Not only do the GLPs come from the same gene as glucagon, but have a very similar aa sequence as well.
Despite these parallels, the GLPs have very different functions than glucagon, and there is a lot of excitement about using these hormones to treat problems ranging from diabetes and obesity to chemotherapy-induced intestinal damage.

From a diabetes perspective, the interesting GLP is GLP-1.
GLP-1 is secreted from cells in the gut in response to a meal, and helps to integrate many of the normal physiological responses that occur after eating.
For one, GLP-1 induces insulin secretion from the pancreas, and simultaneously reduces glucagon release. This release of insulin actually seems to
occur only when the ambient glucose concentration is high, thus reducing the chance that hypoglycemia
will develop (an especially attractive feature in a diabetes therapy).

Over a longer period, GLP-1 actually increases the number of insulin-
producing cells. GLP-1 also acts directly on the GI tract,
reducing the rate at which food spills out of the stomach and into the SI,
making the absorption and storage of energy more efficient.

Finally, and perhaps most intriguingly, GLP-1 acts on the CNS to signal a sense of fullness so that we don't overeat.
So isn’t GLP-1 prescribed to everyone with T2DM? Well, there are a few problems, The most daunting has been that our bodies destroy GLP-1 within a few minutes. This means that it needs to be continuously infused (Because it is a protein, GLP-1 cannot be given orally), which is clearly not going to work for most people. The enzyme that destroys GLP-1 is called dipeptidyl-peptidase IV (DPP IV), and intense focus has been placed on figuring out ways to disable the enzyme so that GLP-1 can do it's thing for longer periods of time.

One way to get around the problem of DPP IV is to administer a form of GLP-1 that is resistant to destruction. Such forms of GLP-1 have already been found, and the source is delightfully unexpected--the poisonous saliva of the Gila monster lizard. GLP-1 (called exendin-4) from these reptiles has a few key differences from the form found in humans, one consequence of which is immunity to DPP IV.
pharmaceutical companies made synthetic forms of exendin-4 (one imagines that it's easier to make the chemical from scratch than it is to harvest toxic lizard spit).
Phase 2 clinical trials of exendin-4 in patients with T2DM showed improvements in hemoglobin A1c levels comparable to those seen with currently available ant diabetic drugs. Other studies show reductions of caloric intake after exendin-4 administration.

Another strategy that is being pursued is the use of drugs that will inhibit DPP IV directly.
Studies have shown that 24 hours after taking such a drug, patients with mild T2DM have reduced fasting, post-meal, and average blood sugar levels.
The primary advantage of this approach (vs. exendin-4) is that DPP IV inhibitors can be given orally. On the other hand, DPP IV affects other hormones besides GLP-1, and there is concern that blocking the enzyme could cause other problems.
One reassuring piece of data is that mice that are genetically engineered to lack DPP IV are viable and appear to do well, and this provides some reassurance that the strategy is sound. Still, longer term studies with both DPP IV inhibitors need to be performed to assess possible toxicity. It is also unclear if the beneficial effects of GLP-1 will be sustained over time, and this too will have to be tested. Nonetheless, a drug that that causes weight loss as well as improved insulin secretion in type 2 diabetes is a potential blockbuster.
GLP-1 extendin-4 DDP1V

Diabetes MythsMyth #1 You can catch diabetes from someone else.
Myth #2 People with diabetes can't eat sweets or chocolate.
Myth #3 Eating too much sugar causes diabetes.
Myth #4 People with diabetes should eat special diabetic foods.
Myth #5 If you have diabetes, you should only eat small amounts of
starchy foods, such as bread, potatoes and pasta.
Myth #6 People with diabetes are more likely to get colds and other illnesses.
.Myth #7 Insulin causes atherosclerosis (hardening of the arteries)
and high blood pressure.

Diabetes Myths
Myth #8 Insulin causes weight gain, and because obesity is bad for you, insulin should not be taken.
Myth #9 Fruit is a healthy food. Therefore, it is ok to eat as much of it as you wish.
Myth #10 You don’t need to change your diabetes regimen unless your A1C is greater than 8 %
![-f+ Vat ftilltop Betes - LaGrange Collegehome.lagrange.edu/library/hilltop_news_digitized/1964-12...-f+ Vat ftilltop Betes SUPPORT THE LC PANTHERS TONIGHT] AGAINST B'SOUTHERN "Representing](https://img.dokumen.tips/doc/110x75/5ae7e0e37f8b9acc268f4613/-f-vat-ftilltop-betes-lagrange-vat-ftilltop-betes-support-the-lc-panthers-tonight.jpg)