Embed Size (px)
Citation preview

Dr. Naresh Mullaguri MDResident Physician PGY2Department of Neurology
University of Missouri
FRIDAY NOON CONFERENCE

Chief complaint
Weakness and numbness in bilateral lower extremities and unable to walk

HPI A 40 year old right handed legally blind female patient presented to the ER on
10/25/2014 with the chief complaint of Bilateral lower extremity weakness which started a day before with flu like symptoms, back ache followed by tingling in the right lower extremity and subsequently spread to the left lower extremity by next morning with profound weakness and unable to use the lower extremities. Also associated with bladder and bowel incontinence with bowel incontinence being new to the patient. Uses crutches and power chair to ambulate at home but unable to transfer from bed to chair since that day. Had a few falls in the process of ambulation.
History of similar episodes in the past since the age of 16years with relapses of these symptoms at least 1-3 times an year. Her last episode was in May, 2014.
At the age between 19-22 years old, she was paraplegic for several months and became ambulatory after several months of physical therapy. Uneventful 2013 for the patient with no flares and she delivered a healthy baby girl who is 8 months old now.
All her relapses in the past were dramatically improved with high dose IV steroids for 3-5 days with oral taper with some residual deficits after every episode.

HPI continued.. At baseline has urinary incontinence, stiffness in bilateral lower
extremities with spasms, patchy sensory loss in bilateral lower extremities. She became blind in her left eye at the age of 3yrs and only had central
vision in her right eye. She had symptoms of chronic urinary tract infections and was on intermittant antibiotics because of the incontinence
Recently had extraction of her wisdom tooth According to the patient this is the worst episode in many years which is
different from the rest of the flares by the rapidity of progression of symptoms, intensity of symptoms, development of bowel incontinence and intensity of back pain.
Was a Neurology patient since the age of 19years when she was diagnosed and most of her initial workup was done in Des Mois, Iowa city and used to follow Dr. Lardizabal, MD in Northeast Regional Hospital since 2007 then here in the University Hospital till 2014 and now established care with Dr. Chuquilin, MD and may be a Friday conference case in the past too.

PMH/FH/SH/Allergies Ashthma GERD Neurogenic Bladder Recurrent UTIs Neuromelitis Optica Hypothyroidism B12 deficiency Polycystic Ovarian disease
Sister died at the age of 21 years, Blind since childhood, Unable to ambulate since the age of 12-13 years and died of Pneumonia. Father died of Pancreatic cancer, Strong family history of Lupus, Depression.
She lives with her daughter in Kirksville, MO. Doesn’t smoke, drink and denied any illicit drug usage. Motivated to take care of her daughter, Didn’t work since childhood on disability, Volunteered in the past in a Blind school in Iowa city. Had a Boyfriend in Iowa city.
Allergic to Lovenox and Adhesive tape

Medications Advil 200 mg oral tablet, 2 Tablet(s) Oral q4h as needed, PRN: for fever Detrol LA 4 mg oral capsule, extended release Fish Oil: See Instructions, 1 tab bid Macrobid 100 mg oral capsule Prilosec: 20mg, Oral, Daily Singulair Vitamin B12 1000 mcg/mL injectable solution: 1 mg, 1 mL, IM, qMonth, 10
mL Vitamin B12 2500 mcg sublingual tablet: 2,500 mcg, 1 Tablet(s),
Sublingual, Daily Vitamin D3 1000 intl units oral tablet Zantac 150 albuterol: Inhalation baclofen: 20mg, Oral, bid brimonidine ophthalmic 0.2% solution cephalexin 500 mg oral tablet ciclopirox topical 8% kit: metformin: 500mg, Oral, bid

Historical differential diagnosis Demyelinating disorders like Multiple Sclerosis/NMO/Transverse Myelitis Autoimmune polyneuropathies like AIDP, GBS(unlikely due to Bowel
involvement), Vasculitis. Infectious processes like Lyme’s disease, Tick paralysis, Sarcoidosis Thoracic myelopathy secondary to compression: Epidural abscess, Tumor,
AVM Spinal cord infarction

Physical Examination Vitals:
▪ Temperature (Celsius) 36.1 Deg C Heart Rate 84 bpm Respiratory Rate 20 breaths/min SBP NIBP 108 mmHg DBP NIBP 73 mmHg SpO2 100 %
GENERAL EXAMINATION Patient in not apparent distress, cooperates with examination. Obese. HEAD: normocephalic, atraumatic, no lesions or exudates. EYES: normal. EARS, NOSE AND THROAT: normal, no lesions or exudates. NECK: supple, no lymphadenopathy or thyromegaly. EXTREMITIES: no clubbing, edema or cyanosis.

Neurological ExaminationMENTAL STATUS: Patient was alert, awake and oriented x3, follows commands. Speech is fluent and comprehension is intact.
CRANIAL NERVES: II: Visual fields were full, Fundoscopic exam showed pale optic disc bilaterally. Pupils were reactive to light and
accommodation. APD bilaterally with no INO. III, IV, VI: Right eye exotropia. Nystagmus in all directions of gaze. V: face sensation was normal to light touch and pinprick. VII: face was symmetric. Eye closure and lip closure were normal. VIII: hearing is intact. IX-X: palate elevates at midline. XI: shoulder shrug is 5/5 bilaterally. XII: Tongue was midline and strong. No fasciculations.
MOTOR: Normal strength 5/5 on MRC scale in the upper extremities. Iliopsoas 0, hip abduction 0, hip adduction 1, quadriceps 2 on the right and 1 on the left, hamstring 2. Dorsiflexion is 0
on the right side and 2 on the left side, plantar flexion is 0 on right side and 2 on the left side. Spasticity both lower extremities Fine finger movements were normal bilaterally. No pronator drift.
SENSATION: Decreased pinprick below rib cage level and both lower extremities. Vibration diminished in both the lower extremities up to knees. Strong on the right knee and absent on the left knee
COORDINATION: Absent dysmetria on finger -nose -finger. Normal rapid alternating movements. No tremor.
GAIT: Wheelchair-bound
REFLEXES: 3+ biceps, triceps, 4+ at the knees and ankles with sustained clonus. Babinski was positive bilaterally

Investigations WBC – 9.0 HGB – 14.1 MCV – 87.8 PLT – 284 ESR – 23 Electrolytes – Normal BUN – 11 Creat – 0.72 Vitamin B12 – 1124 Folate - >40 Vit – D – 26 TSH – 0.425 with normal T4 B2 – 23 UA – negative Aquaporin-4 receptor antibody in serum – Later

Imaging studies
C-Spine – T2 Sagittal sequence

Imaging Studies contd.. – MRI of T spine in T2

Coronal T2 section

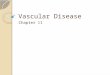
Post contrast T1 image –Sagittal view
Contrast enhancement at the level of
T6

MRI Brain T2 and FLAIR

A view of white matter

AQUAPORIN 4 RECEPTOR ANTIBODY >160 (Reference <4) Previous CSF studies done in 2007 in Northeast
Regional Hospital – Positive antibody, negative Oligoclonal bands, IgG or pleocytosis. On Rebif since 2007, tried Copaxone and Avonex in the past. Disease not well controlled. Patient is afraid of port placement and refused Plasma exchange and IVIg treatments in the past multiple times.
Exam during the clinic visit is almost unchanged from the hospital exam. Recommended Rituximab infusions and Plasma exchange. She asked for 2 weeks of time hoping that steroids will work.

Neuromyelitis Optica/Devic’s disease


Differences between MS and NMO

Longitudinally extensive Transverse Myelitis



Dr. Chuquilin, MDDr. Burger, MD
My sincere thanks to