Embed Size (px)
Citation preview

Developments in Breast Developments in Breast Imaging: In Memory of Imaging: In Memory of
Dr. Carolyn Dr. Carolyn KimmeKimme--SmithSmithEnhancement Characteristics Enhancement Characteristics of Cancer on Breast MRI and of Cancer on Breast MRI and
Biopsy TechniquesBiopsy TechniquesDebra M. Ikeda, M.D.Debra M. Ikeda, M.D.
Director of Breast ImagingDirector of Breast ImagingProfessor of RadiologyProfessor of Radiology
Stanford University, Stanford, CAStanford University, Stanford, CAImage courtesy of Bruce L. Daniel, M.D.Image courtesy of Bruce L. Daniel, M.D.
Debra M. Ikeda, M.D.Debra M. Ikeda, M.D.Director of Breast ImagingDirector of Breast Imaging
Professor of RadiologyProfessor of RadiologyStanford University, Stanford, CAStanford University, Stanford, CA
Image courtesy of Bruce L. Daniel, M.D.Image courtesy of Bruce L. Daniel, M.D.
•• Images courtesy of American College of Radiology ACR BIImages courtesy of American College of Radiology ACR BI--RADS MRI, in RADS MRI, in American College of Radiology BIAmerican College of Radiology BI--RADS Imaging Atlas, Reston, VA, 2003, RADS Imaging Atlas, Reston, VA, 2003, ACR Breast MRI Lexicon Committee, International Working Group onACR Breast MRI Lexicon Committee, International Working Group on breast breast MRI, Bruce L. Daniel, M.D., MRI, Bruce L. Daniel, M.D., SunitaSunita Pal, M.D. and Pal, M.D. and AyaAya Kamaya, M.D.Kamaya, M.D.
Open Breast CoilOpen Breast Coil
MRI Devices4-coil phased array

Patient PositioningPatient Positioning IDCIDCRimRim SpiculatedSpiculated MicrolobulatedMicrolobulated
Image courtesy of Bruce L. Daniel, M.D.Image courtesy of Bruce L. Daniel, M.D.
WellWell--defineddefined
FibroadenomaFibroadenomaSeptatedSeptated MacrolobulatedMacrolobulated
Image courtesy of Bruce L. Daniel, M.D.Image courtesy of Bruce L. Daniel, M.D.
Breast MRI and MRIBreast MRI and MRI--BxBx
What is actually happening in US clinical practice?
What is breast MRI standard of care?
What are the new BIRADS MRI recommendations for 2010 ACR Atlas?
What are MRI breast biopsy results?
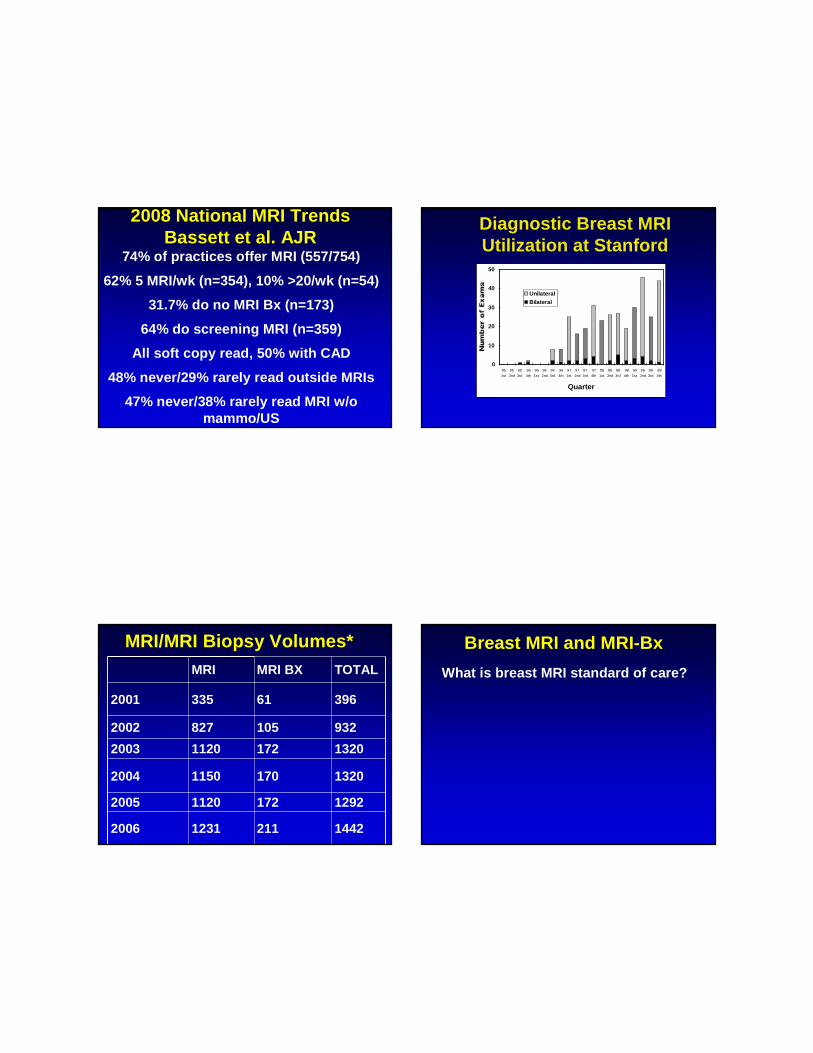
2008 National MRI Trends2008 National MRI TrendsBassett et al. AJRBassett et al. AJR
74% of practices offer MRI (557/754)
62% 5 MRI/wk (n=354), 10% >20/wk (n=54)
31.7% do no MRI Bx (n=173)
64% do screening MRI (n=359)
All soft copy read, 50% with CAD
48% never/29% rarely read outside MRIs
47% never/38% rarely read MRI w/o mammo/US
0
10
20
30
40
50
95
1st
95
2nd
95
3rd
95
4th
96
1st
96
2nd
96
3rd
96
4th
97
1st
97
2nd
97
3rd
97
4th
98
1st
98
2nd
98
3rd
98
4th
99
1st
99
2nd
99
3rd
99
4th
Quarter
UnilateralBilateral
Diagnostic Breast MRIUtilization at Stanford
MRI/MRI Biopsy Volumes*MRI/MRI Biopsy Volumes*MRI MRI BX TOTAL
2001 335 61 396
2002 827 105 932
2003 1120 172 1320
2004 1150 170 1320
2005 1120 172 1292
2006 1231 211 1442
Breast MRI and MRIBreast MRI and MRI--BxBx
What is breast MRI standard of care?

GadoliniumGadolinium--EnhancementEnhancement
Tumor AngiogenesisTumor Angiogenesis
Image courtesy Bruce L. Daniel MDImage courtesy Bruce L. Daniel MD
The Current Status of Breast MR The Current Status of Breast MR Imaging (Part 1 of 2 parts)Imaging (Part 1 of 2 parts)1. Spatial and temporal resolution are
important2. Understand perfusion and capilllary
leakage, tissue T1 and T2 relaxation3. Most sensitive for cancer; MRI and
Mammo offer complementary information
*Christiane Kuhl, M.D. Radiology 2007, August Vol 244; 2; 356-378 and Radiology 2007, September Vol 244; 3; 672-691
The Current Status of Breast MR The Current Status of Breast MR Imaging (Part 1 of 2 parts)Imaging (Part 1 of 2 parts)4. Specificity and PPV for MRI are
equivalent to Mammo5. Work-up for MRI findings are more
demanding than mammo or US, improvements for MRI are in great demand
6. Advances have been made in MRI interpretation guidelines
7. MRI biopsy is necessary*Christiane Kuhl, M.D. Radiology 2007,
August Vol 244; 2; 356-378
The Current Status of Breast MR The Current Status of Breast MR Imaging (Part 2)Imaging (Part 2)1. Clinical applications for MRI include
A. Problem Solving for equivocal mammo or US findings
B. MRI Biopsy necessary 40% US unseen C. Neoadjuvant chemotherapyD. Avoid over-treatment of MRI findings
Use MRI findings wisely - it is wrong totransfer mammo guidelines to MRI
E. High Risk screening
*Christiane Kuhl, M.D. Radiology 2007, September Vol 244; 3; 672-691

Screening ReferenceScreening Reference• Saslow D, Boetes C, Burke W, et al. American
Cancer Society Guidelines for Breast Screening with MRI as an Adjunct to Mammography. CA Cancer J Clin. 2007;57:75-89
MRI Breast Cancer ScreeningMRI Breast Cancer ScreeningAUTHOR YEAR #WOMEN #CANCERS %
KUHL 2000 192 HIGH RISK 9 4.6%
TILANUS-LINTHORP 2000 109 HIGH RISK 3 (6FP) 2.8%
WARNER 2001 196 BRCA1/2 7 3.6%
STOUTJESDIJK 2001 179 HIGH RISK13 (MRI ONLY) 7.3%
MORRIS 2003 367 HIGH RISK 14 (50 FP) 4%
LEE 2003182 (CA OPPOSITE)
7/ (8FP) 3.8%
HARTMAN 2004 41 HIGH RISK 1 2.4%
WARNER 2004 236 BRCA1/2 17/22 7.2%
KRIEGE 2004,06 1909 HIGH RISK 32/45 1.6%
LEHMAN 2005 367 HIGH RISK 4 (19FP,5%) 1.1%
MRI Breast Cancer ScreeningMRI Breast Cancer ScreeningAUTHOR YEAR #WOMEN #CANCERS %
PORT 2007 182 LCIS/ATYPIA 5 3%
TRECATE 2006 116 HIGH RISK 10 10%
LEHMAN 2007 171 HIGH RISK 6 3.5%
PEDICONI 2007118 CONTALATERAL OR HIGH RISK
22 5.3%
PORT 2007 182 LCIS/ATYPIA 5 3%
MRI Breast Cancer OppositeMRI Breast Cancer OppositeBreastBreast
AUTHOR YEAR #WOMEN #CANCERS %
RIEBEL 1998 34 3 11%
FISCHER 1999 463 19 4%
KUHL 2000 710 45 6%
SLANETZ 2002 17 4 24%
LIBERMAN 2002 223 12 5%
LEE 2003 182 7/ (8FP) 4%
VIEHWEG 2003 119 4 4%
LEHMAN 2007 969 30 3.1%

Breast MRI and MRIBreast MRI and MRI--BxBx
What are the new BIRADS MRI recommendations for 2010 ACR Atlas?
International Working Group for International Working Group for Breast MRIBreast MRI
and and American College of RadiologyAmerican College of RadiologyBreast MRI Lexicon CommitteeBreast MRI Lexicon Committee
19981998--20032003
ACR BIACR BI--RADS RADS -- MRIMRIImaging Atlas, Reston, VA 2003Imaging Atlas, Reston, VA 2003
2006/09 2006/09 Updates for ACR BIUpdates for ACR BI--RADSRADS™™1. Do bilateral studies2. Describe background enhancement3. Do T2-weighted non-contrast exams4. Check Kinetics5. Facilities doing breast MRI should be
able to do MRI-guided biopsy*6. Do combined reporting(MRI Screening advised for 20-25% lifetime risk
and women treated for Hodgkin disease**)*Christiane Kuhl, M.D. Radiology 2007, September
Vol 244; 3; 672-691 **Saslow D et al. Ca Cancer J Clin 2007; 57 (2) 75-
78
2006 Improvements for 2006 Improvements for ACR BIACR BI--RADSRADS™™
1. Do bilateral studies**
Easier to compare symmetry ofbackground enhancement pattern
Less likely to miss DCIS
**November 2006 BIRADS Committee RSNA, Chicago, Illinois

FCCFCC ACR BIACR BI--RADSRADS™™BREAST MRI LexiconBREAST MRI Lexicon
MORPHOLOGY (FORM)
DISTRIBUTION
KINETICS (SI vs time)
C. NONC. NON--MASS LIKE ENHANCEMENTMASS LIKE ENHANCEMENTDuctal Enhancement:Ductal Enhancement:
Courtesy Courtesy ACR, ACR, IllustratedIllustratedBreast MRI Breast MRI Atlas, Atlas, BIRADSBIRADS--MRI, ACR, MRI, ACR, Reston,VAReston,VA20032003
DUCTAL enhancement. DCISDUCTAL enhancement. DCIS..
DCISDCIS

Pure DCIS Pure DCIS MAMMO – 90% CALCS (Ikeda 1988)
-10-20% MASS, NODULES
DETECTION RANGES 77-96% (MORRIS 2004)
SIZE, GRADE, ANGIOGENESIS, PROTOCOL
14-75% DCIS PROGESSES TO IDC, 22% RECURRENT (Leonard 2004)
AFTER Rx- 50% recurrences invasive (Bijiker 2004)
Accelerated Partial Breast Irradiation - extent
Pure DCIS Pure DCIS MORPHOLOGY mostly non-masslike, few masses
CLUMPED- cobblestone, occ confluent or HETEROGENEOUS
SEGMENTAL, DUCTAL , LINEAR
REGIONAL – large area , not ductal, randomFOCAL AREA – confined area <25% breast
KINETICS variable- MAY INDICATE HIGH GRADE DCIS IF PRESENT
Raza et al. AJR 2008; 191: 689
DCIS CharacteristicsDCIS CharacteristicsMORPHOLOGY IMPORTANT
SEGMENTAL
DUCTAL ENHANCEMENT
FOCAL AREALINEAR
CLUMPED (COBBLESTONE)PROXIMITY TO IDC
KINETICS LESS IMPORTANT- MAY INDICATE HIGH GRADE DCIS IF PRESENT
Kuhl CK et al. Lancet 2007 Aug 11:370(9586):485-92
Background Enhancement Background Enhancement
None/Minimal < 25%
Mild 25-50%
Moderate* 50-75%
Marked* >75%
*Moderate and Marked Background Enhancement can hide invasive or noninvasive cancer
ACR BIRADS Committee. Draft for Breast MRI Lexicon Update, November 2006

20032003 20012001
20052005 20042004
Image courtesy Aya Kamaya, M.D.Image courtesy Aya Kamaya, M.D.
Normal Hormone Normal Hormone Enhancement FluctuationsEnhancement Fluctuations
0202 0404
IDC MIP OUTER BREASTIDC MIP OUTER BREAST--11 IDC MIP OUTER BREASTIDC MIP OUTER BREAST--22

IDC MIP OUTER BREASTIDC MIP OUTER BREAST--33 IDC MIP OUTER BREASTIDC MIP OUTER BREAST--44
IDC MIP OUTER BREASTIDC MIP OUTER BREAST--55 IDC MIP OUTER BREASTIDC MIP OUTER BREAST--66

IDC MIP OUTER BREASTIDC MIP OUTER BREAST--77 IDC MIP OUTER BREASTIDC MIP OUTER BREAST--88
IDC MIP OUTER BREASTIDC MIP OUTER BREAST--99 IDC MIP OUTER BREASTIDC MIP OUTER BREAST--1010

IDC MIP OUTER BREASTIDC MIP OUTER BREAST--1111 IDC MIP OUTER BREASTIDC MIP OUTER BREAST--1212
IDC MIP OUTER BREASTIDC MIP OUTER BREAST--1313 IDC MIP OUTER BREASTIDC MIP OUTER BREAST--1414

IDC MIP OUTER BREASTIDC MIP OUTER BREAST--1515 IDC MIP OUTER BREASTIDC MIP OUTER BREAST--1616
Kinetic DescriptionKinetic Description
Initial slope within 2 minutes or when curve starts to change.
Delayed slope after 2 minutes or after curve starts to change
SISI
InitialInitial DelayedDelayed
persistentpersistent
plateauplateau
washoutwashout
fastfast
mediummedium
slowslow
Kinetic DescriptionKinetic Description
Kinetic DescriptionKinetic Description
plateauplateau washoutwashoutPersistent

Heart CurveHeart Curve LN SpiralsLN Spirals
LN Spiral CurveLN Spiral Curve
DynamicDynamic(213 s)(213 s)
DynamicDynamic(277 s)(277 s)
High Res. High Res. (6 min 31 s)(6 min 31 s)
k=0k=0
Overview: Overview: ContrastContrast--enhanced MRI Protocol at Stanfordenhanced MRI Protocol at Stanford
T1T1 HighHigh--ResRes
InjectInjectGdGd
T2T2
Curve types, k21,Curve types, k21,parametric mapsparametric maps
MorphologyMorphologyACR MRI LexiconACR MRI Lexicon
Curve types, k21,Curve types, k21,parametric mapsparametric maps

Neoadjuvant ChemotherapyNeoadjuvant Chemotherapy30 patients undergoing neoadjuvant
chemotherapy, comparing response and surgical management before/post MRI
16 successful breast conservation
14 mastectomies
MRI would have helped therapy in 6 (20%) 5 mastectomy avoid chemotherapy,1 would avoid unsuccessful conservation
MRI would hinder therapy in 3: not prevent unsuccessful conservation (1) or prevent successful conservation (3)
Thibault F et al. AJR 2004; 183:1159-68
NonNon--Spic (CR) preSpic (CR) pre-- chemochemo
NonNon--Spic (CR) postSpic (CR) post--chemochemo ChemotherapyChemotherapyPre Post Pre Post
Images courtesy of Dr. Bruce L. DanielImages courtesy of Dr. Bruce L. Daniel

T2T2--weighted images*weighted images*Fluid (cysts) bright against fat
Normal fluid in ducts
Lymph nodes (UOQ, vessel,fat)
Cellular FA (bright, sclerotic dark)
Lactating patients bright glands, cancers dark
Breast edema
Beware mucinous cancers (pitfall)** Kuhl CK et al JMRI 1999; 9: 187-96, Yuen et al. JMRI 2007;25:502-10,
Espinosa et al. Radiology 2005;237:249-36
Breast CA with High Signal Breast CA with High Signal Intensity on T2Intensity on T2--weighted Imagesweighted Images30/480 breast cancers had high T2-weighted SI (8 mucinous; 22 nonmucinous cancers) compared 19 FA
Hi SNR and enhancing septations in mucinous cancers and irregular border, no dark septations and rim enhancement in non-mucinous cancers separated them from FA
Yuen et al JRMI 2007;25;502-10
Case 2007Case 2007-- UK4UK4
T2 FSE Fat SatT2 FSE Fat Sat T1 3D SPGR Fat T1 3D SPGR Fat Sat Sat -- Post GadPost Gad
T1 Spiral 10 seconds after Gd arrival in Breast
Images courtesy of Bruce L. Daniel, M.D.Images courtesy of Bruce L. Daniel, M.D.
What are TP biopsy rates for What are TP biopsy rates for MRI?MRI?
Current MRI sequences/hardware make high resolution/kinetic scans now more available
Several vendors offer CAD, dedicated breast coils, MRI-compatible grids, needles and vacuum assisted biopsy probes
MRI-guided pre-operative needle localization and vacuum assisted core availability increasing
Reported TP biopsy rates comparable to mammography

Right Breast in Left CoilRight Breast in Left Coil
Courtesy Bruce Daniel, MDCourtesy Bruce Daniel, MD
4-Coil Phased-ArrayOpen Platform Breast Coil, MRI-Devices Inc,Waukesha, WI
MRI Breast Lesion Marking System, E-Z-EM Inc., Westbury, NY
CT-MRI Topographic Marker, Radionics / Z-Medical Inc., Baltimore
Freehand / InteractiveNeedle Placement
VacuumVacuum--Assisted Core Needle Assisted Core Needle Biopsy Apparatus*Biopsy Apparatus*
ATEC MRI CompatibleVacuum Breast Biopsy SystemSuros Surgical Instruments Inc., Indianapolis, IN
2.8 cm
*MR Safe
Confirmation on Orthogonal ViewsConfirmation on Orthogonal Views
Axial ReformatAxial Reformat1.5T 3DSSMT1.5T 3DSSMT
Axial 0.5T 3Axial 0.5T 3--Pt Pt Dixon SPGRDixon SPGR
Sagittal 0.5T 3Sagittal 0.5T 3--Pt Pt Dixon SPGRDixon SPGR
Courtesy Bruce Daniel, MDCourtesy Bruce Daniel, MD

MRIMRI--guided Breast guided Breast Needle Localization BiopsyNeedle Localization Biopsy
AUTHOR YEAR #WOMEN %
OREL 1994 10 40%
FISCHER 1995 15 33%
KUHL 1997 97 54%
DANIEL 1998 19 42%
FISCHER 1998 130 48%
OREL 1999 137 43%
MORRIS 2001 115 31%
LEHMAN 2004 38 40%
VAN DEN BOSCH 2005 304 34%
MRIMRI--guided Breast guided Breast Needle Localization BiopsyNeedle Localization Biopsy
AUTHOR YEAR #WOMEN %CA
VAN DEN BOSCH 2006 304 34%
VIEHWEG 2006
97 LESIONS/63 WOMEN +FH/87 BX
(9 IDC/12 DCIS)
10 DISAPPEARED
24%
CARLSON 2007 85 24%
MRIMRI--guided Vacuumguided Vacuum--Assisted Core Assisted Core Needle Breast BiopsyNeedle Breast Biopsy
AUTHOR YR # NOTES %CA
LEHMAN 2005 38AV 38 MIN FOR 1 BX, 59 MIN FOR MULT, BILATER 64 MIN
37%
LIBERMAN 2005 112
14/112 (12%) CANCELLED (GONE)
24/95 (25%) CANCER, 9/95 WERE DISCORDANT (10%)
CLIP DEPLOYED IN 86?91 LESIONS
24%
OREL 2006 85
35 IDC/ 17 DCIS,
4 DCIS WAS IDC, 2 ADH WERE DCIS
2 DISCORDANT (2%) FN
61%
(52/75)
PERLET 2006 538
517/538 SUCCESSFUL
17 ADH (3%), 362 BENIGN (70%)
PPV VARIED DEPENDING ON INDICATION
27%
138/517
GEBAUER 2007 42 4224%
(11/42)
2007 Breast MRI and MRI2007 Breast MRI and MRI--guided guided Needle Localization BiopsyNeedle Localization Biopsy
FACILITY
#MRI
PER
YR
TIME
TO DO MRI (MIN)
# MRI READPER
DAY
#MRI
BX
PER
YR
TIME TO DO BX (MIN)
HOW
MRI
BX DONE
HOW MANY
MRI BX/
DAY
MIDWEST
ACADEMIC- K1500 45 8-20 85 45-60
GRID/
VACUUUP TO 2 PER DAY
MID EAST COAST - P 714 30 6-8 100
40
(60 MIN)
GRID/
VACUU
1 AT
6:30 AM
NORTHWEST
-P 2000 30
10
(8-15)150
60
(60-90 MIN)
GRID/
VACUU
60-90 MIN
1,2 SITES
STANFORD 1225 60 8-25 23590-120
(2-3 SITES)
FREE-
HAND/VACUU
3 PTS/AM
MULTIPLE
SITES

2008 Breast MRI and MRI2008 Breast MRI and MRI--guided guided Needle Localization BiopsyNeedle Localization Biopsy
FACILITY
#MRI
PER
YR
TIME
TO DO MRI (MIN)
# MRI READPER
DAY
#MRI
BX
PER
YR
TIME TO DO BX (MIN)
HOW
MRI
BX DONE
HOW MANY
MRI BX/
DAY
M MIDWEST
ACADEMIC1000 40 3-6 50 90
GRID/
VACUU
1/ DAY
AS NEED
MID WEST COAST - BR
1200 45 3-8 7090 GRID/
VACUU
1/DAY
2X/WK
MID EAST COAST-B
1000 60 3-6 100 90GRID/
VACUU
3-4/1DAY
7-2 PM
MIDWEST ACADEMIC=H
300 60 2 12 90PILLAR/POST
VACUU
1/DAY
SLOTS FOR 2
Breast MRI and MRIBreast MRI and MRI--BxBxWhat is actually happening in US clinical
practice? – screening, 70% bx
What is breast MRI standard of care?-bilat high spatial and temporal resolution
What are the new BIRADS MRI recommendations for 2010 ACR Atlas?-bilat scans, T2-weighted, background,
kinetics, do bx and combined reporting
What are MRI breast biopsy results? 30-40% TP for cancer
Axial T1 SEAxial T1 SESag DynamicSag Dynamic3D spiral3D spiral
Sag HiSag Hi--Res CentricRes Centric3DSSMT3DSSMT
Axial ReformatAxial Reformat3DSSMT3DSSMT
Methods: 1.5T Diagnostic MRIMethods: 1.5T Diagnostic MRI
Cho

Thank You!Thank You!





























