Embed Size (px)
Citation preview

Development Problems in Children
Dr Ros JeffersonGPVTS presentation Sept 08

Aims
• Identify child who does not obviously fall between normal limits & who needs further assessment
• To give framework for assessment of child who is ‘not quite right for his age’
• When to reassure/when to refer

Normal development
• Physical and neurodevelopmental growth & development throughout childhood
• Normal milestones important• Wide variation in ‘normal’ – so may need to
see again.

Influences on development
• Genetic• Environmental – family structure,
housing,family support• Stimulation• Malnutrition• SEC
Areas of development
• Gross motor• Fine Motor & Vision• Hearing & Communication• Social & Personal

Major normal milestones (average age)
Gross Motor Fine motor & vision
Hearing & language
Social
6 weeks Head level with body in ventral suspension
Fixes & follows Stills to sound smiles
3 months Head at 90deg in ventral suspension
Holds object placed in hand
Turns to sound at ear level
Laughs & squealsHand regard
6months No head lag. Sits w support. Up on forearms when prone
Reach w palmar grasp.Transfers between hands
Babbles Works for toyMay finger feed
9 months CrawlsSits steadily & pivots
Pincer grasp, index finger approach, bangs 2 cubes
2 syllable babble. Distraction hearing test possible
Waves bye-byePat-a-cakeIndicates wants
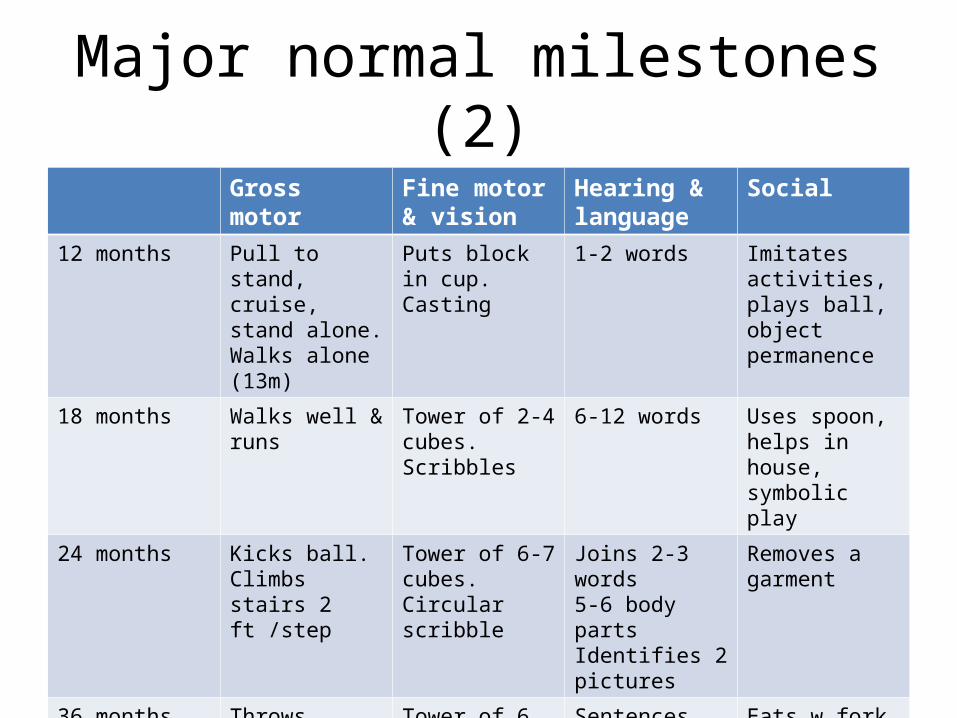
Major normal milestones (2)Gross motor Fine motor &
visionHearing & language
Social
12 months Pull to stand, cruise, stand alone. Walks alone (13m)
Puts block in cup.Casting
1-2 words Imitates activities, plays ball, object permanence
18 months Walks well & runs
Tower of 2-4 cubes.Scribbles
6-12 words Uses spoon, helps in house, symbolic play
24 months Kicks ball. Climbs stairs 2 ft /step
Tower of 6-7 cubes. Circular scribble
Joins 2-3 words5-6 body partsIdentifies 2 pictures
Removes a garment
36 months Throws overarm, stairs 1 ft/step, stands briefly on 1 ft
Tower of 6 cubes, 3 brick bridge, copies circle, cuts w scissors
Sentences, names 4 pictures
Eats w fork & spoon. Puts on clothing. Names friend
Scenario
• Mona, a single mother, brings her 12 weeks baby for her first (late!) immunisation and baby check. Before she comes into the room, you try and remind yourself what you would expect a 12 week baby to be doing.
• What do you jot down in each field of development?

Developmental delay
• Global• Specific• Deviance vs delay

Developmental delay
• Specific delay may have repercussions in other areas of development– Vision & motor/language– Hearing & language– Language & social– Attention control & difficulty learning to read

History
• Parental concerns – ‘parents usually right’
• Family History – how compares with sibs
• Pregnancy• Birth• Postnatal• Feeding• Development• Medical history

Examination
• Look at the parents!!• Observations of child • Head circumference• General examination• Neurological examination

Basic developmental kit
• Pencil/paper• 1in cubes• Simple formboard• Simple book

Global delay
• Down’s syndrome– Commonest & most familiar– Incidence 1 in 660 LB– Increasing risk with maternal age– Recurrence: twice DS risk in subsequent
pregnancy– Chromosomal non-dysjunction/
translocation/mosaicism

Downs syndrome
• Ring alarm bells – diagnosis confirmed from chromosomes
• Multisystem• Insert in PHR

Downs syndrome - development
• Differences within DS population– Mainstream education +GCSE’s vs no language– Limited exercise tolerance vs sporting excellence– 40% of children with DS are able to learn to read

Downs syndrome - milestonesMilestone Mean age Range
Sitting 13m 6-30m
Standing 22m 9-48m
Walking 30m 12-60m
Single words 34m 12-72m

Management
• Multidisciplinary• Congenital heart disease - 40-50% AV canal
defects, PDA, ASD,VSD. Cardiologist• Atlanto-axial instability – rare, insidious onset.
No routine X-ray- variability. Watch for change in gait/manipulative skills, neck pain, sphincter disturbances
• No contraindications to immunisation +/- flu vaccine
Local protocol
• 0-2y – ‘acute’ paediatrician follows up• 2- 5y ( F/T school) – community paediatrician• >5y - if no health problems, surveillance
leaflet to family and GP, for GP follow up

Basic medical surveillance for people with Downs syndrome (DSMIG)
• Growth– Measurements at least annually in childhood, at regular intervals thereafter. Plotted on Downs
specific charts
• Thyroid– Guthrie spot TSH + biochemistry card attached to distinguish from neonatal Guthrie 1-2yearly– OR Venous blood for T4, TSH, thyroid Abs 2-3yearly
• Hearing– Check 2 yearly throughout life – more often if problems. Audiology/school nurse
• Vision– After 4y of age vision checked at least every 2y throughout life - optician
• Heart– Cardiac check advised in early adulthood +/- routine echo
• DSMIG recommendations
Locomotor delay
• Variation in milestones – walking 7/12 – 30/12• First steps – short, widebased with planus feet• Mature gait not achieved till ~4.5y

Locomotor problems
• Normal variants – all present with ‘awkward gait’– Femoral/tibial rotations– Bow legs – normal in infant; correct by 18m
– Knock knees
• Correct spontaneously
Bottom shufflers
• Different patterns• +ve family history• Don’t crawl; possibly later sitting• Hypotonia – resolving• Vertical suspension – hip flexion/knee
extension posture• Dislike prone position• Mx = reassure!

Benign hypotonia
• Delayed, not deviant, pattern• Low muscle tone• Normal neurology• +/- bottom shuffle
Toe walking
• Idiopathic• Myopathic• Neurological
• Key = Neurological examination +/- CK

Scenario
John’s mother brings him to see you because she thinks he is ‘slow’. At the age of 18m he is not yet walking although he pulls himself to stand and cruises, he chucks objects from his high chair and has about 3 words with meaning’
What questions might you want to ask Mum about his gross motor development
• She tells you that he bottom-shuffles and so did his Dad. He sat at 6m and rolled at about the same time. Examination is completely normal.
• What do you tell his mother about his gross motor development?

Language delay
• May cover cognitive delay.• Always refer for audiology assessment• Language development influenced by
– Early input – carer/child interaction– Learning disability– Genetic endowment

Patterns of communication disorder
• Primary problem is with speech production because of mechanical (anatomical) defects or impaired neuromuscular control of the speech apparatus
• Specific Language Impairment (SLI) –problems of language comprehension/expression for which no identifiable explanation
• Children who stop talking – rare• Impaired language and social interaction – ASD
etc

Bilingual child - ESL
• Often late recognition• Problem in which language?• How to treat – which language?

ASD
• Pervasive developmental disorder determined by presence of abnormal/impaired development manifest pre 3y of age affecting:-social interaction- communication
- restricted repetitive behaviour/interests
ICD 10

Aetiology
• Often undetermined• Familial element• Syndromes associated, including:
– Fragile X, Tuberous sclerosis, PKU, NF, Downs

Management
• SALT• Behavioural techniques• Educational support• Parent courses and support
Important points
• +ve family history language delay/learning difficulties
• Early behaviour – passive/irritable• Feeding skills• Play underpins language development
(depends on symbolic understanding)• Parents often over estimate language
comprehension
Key points
• Majority of normal babies born around expected due date smile by 8 weeks. Failure to do so is a warning sign.
• Make allowances for prematurity• Developmental regression rings alarm bells –
refer!• Known existing disabilities may impair
performance in other fields of development wo relevance to intellectual development

Key points (2)• Late walking more common in babies who
bottom shuffle. How get about currently – familial element
• Delayed gross motor development is least significant pointer to general delay – but can be most obvious and worrying to parent.
• Child presenting with language delay may have unrecognised global delay
• Watch for persistence of immature patterns of play & behaviour as well as failure to progress at normal rate

Developmental Coordination Disorder
• ‘clumsy child’• Parent/teacher concerns• Overlap with other disorders –e.g Asperger
syndrome

Definition
• In the absence of any known neurological condition or intellectual impairment, dyspraxia is the inability to plan, organise and coordinate movement.
• Brown D, cited in Bowens & Smith. Childhood dyspraxia, 1999

History & Background• Incidence – 5%• No standardised approach for screening, diagnosis
& treatment
• Previously all children with concerns regarding motor coordination were seen by a paediatrician and then an OT
• Long waiting list up to 2 yrs for OT assessment• New secondary screening started in Dec 2004 using
MABC* (Movement Assessment Battery for Children) checklist & SDQ. Now use DCD-Q and SDQ
* Henderson & Sugden, 1992

DCD Screening process
Motor difficulties identified
Action:Neurological Examination by GP
Abnormal Neurology
Refer to Paediatrician
Parents & Teacher•complete SDQ•complete DCD-Q•Send own observations
DCD Team at Child Development Centre
Normal

DCD Screening process
Referral with DCD-Q/SDQ received by DCD Team
Child with SEN/SEN in process
Referral to Community OT Service
Movement problems:(below 10th centile DCD-Q)
Complex Presentation
Joint OT/Paediatric Clinic
Motor skills difficulties only
OT Assessment
Abnormal Scores on SDQ or other primary diagnosis
Paediatrician Assessment
At Risk: >10th centile DCD-Q
Advice Pack sent

Questions?