Embed Size (px)
Citation preview

INSTITUTE OF PHYSICS PUBLISHING PHYSICS IN MEDICINE AND BIOLOGY
Phys. Med. Biol. 51 (2006) R263–R286 doi:10.1088/0031-9155/51/13/R16
REVIEW
Development of radiobiology for oncology—a personalview
Jack F Fowler1
Emeritus Professor of Human Oncology and Medical Physics, University of Wisconsin MedicalSchool, Madison, WI 53792, USA
E-mail: [email protected]
Received 10 January 2006, in final form 1 March 2006Published 20 June 2006Online at stacks.iop.org/PMB/51/R263
AbstractWhen I came into radiotherapy in 1950, I was puzzled that some patients weretreated to 3000 rads (cGy) in 3 weeks but others received 4000 in 5 or 6000 in6 weeks. When I asked why, there were no convincing answers given, except‘this is what we usually do’. It wasn’t until I went to a course on ‘Radiobiologyfor Radiotherapy’ in Cambridge that I learnt about the basic theories of DouglasLea and the very considerable history of research into radiobiology and clinicalradiotherapy. And there were still some questions outstanding, such as therelative importance of intracellular repair between ‘daily’ fractions, whether a2 day gap each week was a good or a bad idea, and the role of proliferation, ifany, during irradiation. I thought that a few simple animal experiments mighthelp to give answers! That led me to a continuing interest in these questionsand answers, which has taken me more than 50 years to pursue. This is the verypersonal story of what I saw happening in the subject, decade by decade. I washappy to experience all this together with scientists in many other countries,and our own, along the way.
1. Introduction
We didn’t call it the ‘Golden Age of Radiobiology’ when we were working at it, but that’swhat some reviewers are calling it now. When I came into the field as a hospital physicist inSeptember 1950, I was told “don’t go into ‘radiotherapy’—that subject will soon be considereda crude old method—cancer will be cured by ‘a spot of the jabs’.” (They were talking aboutimmunotherapy then.) But just look at radiation oncology now (Bentzen 2005a). The presentaccount concerns the question of ‘iso-effect doses’, at the heart of non-standard fractionationand what is now called ‘biological optimization’. This review provides my personal reflectionsand experiences on the development of radiobiology, particularly radiobiological modelling,
1 Present address: Kirk Cottage, 1 Church St, Bovingdon, Herts HP3 OLU, UK.
0031-9155/06/130263+24$30.00 © 2006 IOP Publishing Ltd Printed in the UK R263

R264 Review
0 1 2 3
-6
-4
-2
0
2α = 1 log per Gyβ = 0.333 per Gyso α/β = 3 Gy
9β
4ββ 3α
2αα
2E = αd + βdSIMPLY LQ
logcell
survivalE
Dose (grays)
Figure 1. A simple representation of the linear-quadratic shape of a single-dose cell survivalcurve. Alpha and beta are the coefficients of the non-repairable and the repairable componentsof radiation damage respectively. Alpha is the number of logs(e) of cell kill per gray; beta is thenumber of logs per gray-squared. The beta-component represents mis-repair as well as repair: acell with a high beta would be good at both. This describes the rapidly falling survival curve seenat a high β/α, i.e. a low α/β ratio, characteristic of slowly proliferating cells. The beta componentfades with a half-time of minutes or hours, so that a very low dose-rate is close to the alpha curve.
over the last 50 years. I’m sorry if it appears boring, because it is mostly old stuff. I’vetherefore added some scraps of peoples’ data. I hope my occasional ‘forward-flash’ will notbe too confusing; each section is still based on a given decade only.
After another 55 years, radiotherapy has developed much better means of irradiatingtumours and avoiding normal tissues, while simultaneously recording the dose received byevery small volume element, to correct almost immediately any underdosed or overdosedvoxel (Mackie 1999, 2003) . . . with a growing library of new methods of imaging so as toenable the powerful computerized physics to aim at the right targets, embedded in tissues nowknown to be constantly in motion from breathing and pulse artefacts, as well as with set-upuncertainties . . . in departments with five or six times more specialist radiation oncology staff,both medical and non-medical, than in the 1950s. How did we manage to cure any cancersat all then? Indeed I was still being told, in the 1970s, by a physician from another subjecton a Medical Research Council (MRC) Cell Board that ‘no cancer was cured by radiotherapyexcept skin cancer’! Thus the teaching, or lack of it, at Medical School can stick for latergenerations to prejudice appreciation of real improvements. I wish to describe the role ofradiobiology in helping to sort out the questions of iso-effect in non-standard fractionatedradiotherapy, and ultimately of optimum radiotherapy. Since about half this story concernsthe linear-quadratic (LQ) formula representing the shape of cell survival curves, I’ll introducethat without delay as figure 1. But wait for it to emerge slowly from the story! In writing thisI’ve been impressed again with how much I owe to dozens of people who went before all ofus, and dozens more who helped me personally. I’ve enjoyed playing a small part in some ofthe developments in radiobiology that I’ve been lucky to be still alive (at my age) to see.
Most developed countries have well-organized regional radiotherapy centres, each ofwhich services several million patients. Half of all cancer patients receive radiotherapy atsome stage of their disease, an increasing proportion of whom achieve long-term cure; withan increasing proportion of early diagnosed patients in whom the chances of cure are nowexceeding 90%, for example in T1–T2 tumours in breast, oropharynx, prostate and even lung(Kaanders 2002, Demanes et al 2005, Song et al 2006, Nagata et al 2004, Nihet et al 2004).It is also being realized that the cost of radiotherapy is less than that of surgery and very muchless than that of chemotherapy (Lieven and Van den Bogaert 2005, Lieven et al 2005).

Review R265
2. Early experiences of a young radiation physicist turning into a radiobiologist
When I was a young hospital physicist at Newcastle-on-Tyne in 1950, I was puzzled by theradiotherapists (as radiation oncologists were called then) who prescribed 4000 rads (as cGywere called then) for some patients and 6000 for others. We physicists knew that we couldmeasure doses to better than 1%, and deliver them within 5% most of the time, so we didn’tunderstand this uncertainty. When I asked ‘why such different doses?’, I was told ‘that’s thecube root law’ or ‘because Ralston Paterson’s book says so’, and their knowledge obviouslydidn’t go much further. I became interested in the theoretical aspects of cell kill and dose rateraised in Hal Gray’s series of eight papers (on bean-roots and more) which were just appearingat the time in the British Journal of Radiology (BJR) (Gray and Scholes 1951). The physicistsrespected them, but most radiotherapists (radiation oncologists) thought that bean roots ortadpoles were irrelevant to patients with cancer to be treated that month, that year—no waitingfor 25 years thank you! Clinical observations were however accurately made, and I was oncecaught out as a physicist by a radiation oncologist who said ‘you haven’t calibrated that x-rayset for 3 months have you, because the skin reactions have changed over that time’. And hewas right. But he thought the same once or twice later, and he was never right again! It keptus physicists on our toes, and gave us great respect for clinical observations by conscientiousobservers.
It wasn’t until I went on a two-week course on ‘The Radiobiological Basis ofRadiotherapy’ given by Professor Joseph Mitchell at Cambridge about 1952 that I learntabout the many clinical and animal studies that had contributed already to the practice ofradiotherapy. And about the oxygen effect and some of the theories of radiation action ofLea and Catcheside (1942) and Lea (1947). And about the long clinical arguments betweenthe German school of radiotherapy that favoured a few big fractions (or even one), and theAustrian and French schools of Freund and Schwarz, later Regaud, Coutard and Baclesse thathad, apparently a few years before World War 2, established that many small fractions werebetter (Thames and Hendry 1987). At about the same time, Eric Hall at Oxford published aconvincing explanation of how cell sterilization could explain the changes in bean root lengthcaused by irradiation. I became fascinated by the unknowns still present in the use of differentschedules of fractionation. How much of the increase in total dose with increasing overalltime was due to repopulation in the irradiated tissues, and how much instead to intracellularrepair between successive small fractions?
My first hands-on irradiation was a rabbit to be given a whole-body dose at King’s CollegeHospital in Denmark Hill, for a haematologist, Dr Davidson, in 1956. No rabbit was everplanned so carefully, on a slowly revolving platform in front of a stationary 250 KV beam,with Perspex body-phantoms to do preliminary dosimetry, and the animal survived, as wasintended. I admired in 1957 Dr Charles Wilson’s three-point arbitrary scale of biologicalresponse that he was using to score effects of radiation on bone healing: 0 no observableeffect, 1 slight, 2 marked, 3 strong. I felt that it was a move into quantification that biologyappeared to need and that physicists could certainly do, even an amateur like me.
3. Radiobiology in the 1960s
At that time the major interest for radiobiologists interested in radiotherapy was the natureof ‘iso-effectiveness’. How could one fractionation schedule be compared with a differentschedule, in particular to choose the same normal-tissue complications if a different schedule,or even a different type of radiation, was to be used? Curiosity ranged from fundamentalmodels of shapes of cell survival curves to clinical multi-fraction data. There were almost no

R266 Review
data on multifraction animal experiments; just the rams and rabbits of Regaud and Ferroux(1927) and the pig skin experiments of Wachsmann (1943).
Together with Babette Stern from the Royal Free Hospital, whom I met on the Cambridgecourse, we tried to extract rates of cellular recovery after irradiation from a number ofpublished clinical dose–response versus overall time relationships. Our conclusion wasthat there were two rates of recovery, one occurring in a few hours that we would nowcall molecular (intracellular) ‘repair’, and the other occurring over days and weeks, thoughtto be ‘repopulation’. We expressed this arithmetic in terms of the simplest mathematicalnonlinearity, which is linear quadratic (with a sigh of relief that it didn’t seem to need adose-cubed term as well)—a derivation from Lea and Catcheside (1942). We wrote a paperthat was turned down, very politely, by the British Journal of Radiology—the Editor, ProfessorLamerton, came by my office and told me personally, and I was very impressed at this unusualcourtesy—on the grounds of ‘speculation with no convincing evidence’. It was publishedseveral years later (Fowler and Stern 1963), but only after I had been invited by Tikvah Alperto talk in a symposium at the BIR on ‘Radiobiology Applied to Radiotherapy’, so I hadbecome ‘respectable’. Its main contribution was to show a summarized curved line relatinglog response of skin to log overall time, in place of the straight line claimed by Strandqvist(1944) to have a slope of 0.22 and by Cohen (1952) to have a slope of 0.33. About whichmore later.
At meetings at the BIR in Welbeck Street, about 1960, I heard Hal Gray describe the cellsurvival curves of mammalian cells first grown and irradiated by Mortimer Elkind (Elkind andSutton 1960). The sense of occasion was much heightened by Harold Hewitt’s announcementthat he had extracted viable cells from mouse cancers, and that just two cells were enough togrow another tumour in another mouse, the cell survival curve having a similar slope (1/Do) tothose of Mort Elkind. Radiobiology then became heavily concerned with cell survival curvesand many ingenious interpretations of radiobiological phenomena were made with sketchesof such curves, often on lunch and dinner napkins. People speculated that if the ‘hit numbers’were about 2 (where the alleged straight line of slope 1/Do extrapolated back to zero dose),this might represent the two strands of DNA as targets for radiation damage . . .. Yes, it wasall very exciting, but that idea didn’t survive the enormous range of extrapolation numbersfound in different cell lines (meaning a large range of repair capabilities), nor the discoverythat cell survival curves in vitro were often curved instead of straight (Barendsen et al 1960).Barendsen et al‘s paper was published in the same volume of Radiation Research as the muchmore quoted paper by Elkind and Sutton, but the Dutch were right up there too as pioneers. Itwas soon found that hit numbers for different cell lines in vitro were spread from 1.0 to manyhundreds, so Tikah Alper changed their name from ‘hit number’ to ‘extrapolation number’,which still stands.
Withers (1967), working with Hal Gray at Mount Vernon in the early 1960s, developeda way of counting individual surviving cells in situ, in mouse skin irradiated in a 1 cm circleof skin surrounded by a truly overdosed annulus of skin to limit the target area. Cell survivalcurves for mouse skin could thus be generated by counting these ‘clones’, and the influenceof hypoxia and of split-dose repair was demonstrated directly in situ. He went on to workwith Mort Elkind in Washington and there developed a similar method of counting individualsurviving cells (clones) in the small intestine of mice, which has been much used.
Fowler et al (1965) developed a skin-reaction system for mouse foot based on scores of0, 1, 2, 3, and could then derive surrogate cell survival curves indirectly, in situ in mouseskin. Individual mouse skin reactions could be observed sequentially for days or weekswithout having to sacrifice the animals for pathology. The derived cell survival curves werearguably, but not convincingly enough, curved, so the old ‘target dose’ survival curves with

Review R267
a ‘hit number’ and a straight semilog slope of 1/Do still held sway for another 20 years andlonger. In Madison for example, where I went to work 25 years later, I had to argue stronglyto get people to take any notice of linear quadratic instead of ‘n and Do’. Back in the 1960sthere was much dispute about whether cell kill (strictly sterilization) and hence cell numberdepletion, was or was not responsible for the major observations of tumour control (plausible)or of normal-tissue damage to skin and other organs (highly arguable at the time), especiallyfor late complications. Alper and Hornsey (1973) produced the most convincing evidenceat these early times (figure 2.1 in chapter 2 of the Thames and Hendry book (1987)). Theyshowed that several x-ray or neutron schedules of equal lethal effect in the whole animals alsoprovided equal cell kill of cell colonies in the small intestine of rats. This wasn’t well accepteduntil some ten years later (Alper 1973, quoted by Thames and Hendry (1987)) loc. cit.
A major impediment to radiobiology in the early 1960s was that multiple fractionexperiments, beyond 2-fraction or ‘split-dose’ irradiations, could rarely be done inexperimental laboratories, with the notable exceptions of Professor F Wachsmann in Germanywith pig skin and the Du Sault sisters in Detroit with mouse tumours, whose work we followedwith interest. Elsewhere, single-dose experiments were most common, so that the effects ofmultiple small fractions were not well known at all. Elkind’s ‘repeating curved cell-survivalshoulders’ (1960) however provided a good lead to what might be happening: repair betweensuccessive fractions, confirmed by our own experiments (Fowler et al 1965) and Withers’(1967) experiments on mouse skin in London. There was much argument about whether the‘initial slope’ at very low single doses was finite or actually zero, as suggested unfortunatelyby the theoretical ‘n and Do’ formula. This was really settled experimentally much later bythe work at Vancouver using their computerized colony counting to trace individual colonies(Palcic and Skarsgard 1984), and theoretically by the linear-quadratic theory. Zero slope itwas not! Barendsen et al in Rijswijk and Jean Dutreix et al in Paris were much involved insuch discussions and experiments.
4. The opportunity to do relevant fractionation experiments on cells and animals
When I moved to Hammersmith in 1959 I felt I was moving to the one of the ‘centres of theworld of radiobiology’. Important basic discoveries had been made at Hammersmith: Howardand Pelc (1953) first described the phases M, G1, S and G2 of the cell cycle; Thomlinsonand Gray (1955) explained hypoxia in human tumours in terms of competing diffusion outof blood vessels and consumption of oxygen by cells; Wright and Howard-Flanders (1957)delineated accurately the change of mammalian cell radiosensitivity with oxygen tension incells. When Gray was dismissed from Hammersmith in 1954, because of a disagreement abouthis extensive plan for research instead of starting to treat patients ‘too soon’ with neutrons, itsent a tsunami of discontent across the radiation research community. This happened becauseof MRC Head Office misunderstandings and their hierarchical approach. Fortunately Graywas soon re-established by the British Empire Cancer Campaign in a new laboratory built forhim at his former hospital, Mount Vernon at Northwood, now the Oliver Scott Building ofthe Gray Institute. But it took five years before experiments on clinical applications couldbe planned in the MRC Radiotherapeutic Research Unit at Hammersmith. I replaced DickNewbery, the head physicist there, in 1959 when he retired. With David Bewley and otherswe were able to compare 5 fractions of x-rays in a week with 5 fractions in 4 weeks in a seriesof experiments on pig skin. These demonstrated more effect of fraction size than of overalltime, but some of both (Later this was not in conflict with Frank Ellis’s NSD concept (1969)which assumed that Strandquist’s slope of 0.22 related to fraction size and number, while thedifference between that and Lionel Cohen’s slope of 0.33—that is, 0.11—was attributed to

R268 Review
overall time.) In the laboratory ‘fractionated’ had usually meant two fractions, and we hadmanaged to push it up to five.
At Hammersmith Hospital MRC Unit we made it to 20 fractions (F) of neutrons in 4weeks on pig skin, in experiments designed to obtain relative biological effect values (RBEs)for neutrons versus x-rays. Quite heroic efforts from many staff, mostly young physicists andcyclotron engineers, who sometimes had to carry pigs from the roof on the tenth floor to the15 MV cyclotron or the 8 MV linear accelerator on the ground floor, if the lift failed—fortunately it did so only occasionally.
Herman Suit at the MD Anderson Hospital in Texas was one of the first radiobiologicalinvestigators to have a dedicated laboratory facility to do multiple-small-fraction animalexperiments designed to simulate radiotherapy fractionation realistically. Even HughThomlinson at Hammersmith in the early and mid 1960s, who did splendid experimentsdemonstrating the effect of hypoxia in rat tumours and its time course of reoxygenation(hours), was limited to a spaced pair of large doses, 10 or 20 or 30 Gy. Meanwhile, atHammersmith, my physics team of amateur biologists, advised by Hugh Thomlinson, TikvahAlper, and Shirley Hornsey, embarked on an ambitious scheme of irradiating a number of4 × 6 cm skin fields on the sides of young adult pigs (80–100 lb) to determine neutron RBEs(radiobiological effectiveness = x-ray dose divided by the neutron dose to cause the sameeffect), with control animals treated by standard fractionation of 200 rads × 30F in 6 weeks,in the afternoons after patients’ treatments had finished (so as to avoid the pig smell botheringany patients in the 8 MV linear accelerator). (A rad was the same dose as a present cGy.) Theneutron pigs were treated in the cyclotron chamber under remotely controlled anaesthesia,a considerable development of technique on its own. Out of this work came the realizationthat RBE was highly dependent on dose-per-fraction, in a way that could be quantitativelypredicted by the highly curving x-ray cell survival curves in contrast to the almost straightneutron cell survival curves. I once had an informal meeting with Hal Gray at the BIR andexplained our current results on the neutron RBEs, about 1964. He laughed and laughed, inthat hugely infectious laugh of his, but didn’t tell me why. Later I gathered that that wasexactly what he had predicted more than ten years earlier, from his Broad Bean experiments,before mammalian cell clones were available. Ten years later I discovered that because of hisloud laugh, Hal Gray’s office at the British Empire Cancer Research Campaign RadiobiologyResearch Unit at Northwood had been built with double brick walls, to avoid interrupting hiscolleagues’ thoughts and discussions.
Much later it became clear that a neutron cell-survival curve should not be drawn with a tinycurved shoulder at the lowest dose followed by a straight 1/Do dose–response curve, but shouldinstead have a long straight initial portion, gradually bending over into a barely perceptible,but progressively increasingly steeper, curvature at higher doses. This realization (fromreconstructed multifraction skin experiments) was one of the most convincing demonstrationsof the LQ model when it became relevant to in situ experiments, ten years later. Especiallyconvincing for Julie Denekamp, who always claimed she didn’t like the minimal algebra usedin LQ modelling, even though she could in fact handle it very well.
We had planned to follow-up the irradiated pigs for one or two years. We felt that thecontrol pigs (x-ray schedules only) were likely to give us as much valuable information aboutfractionated radiotherapy as the neutron experiments. When the pigs grew to full weight, ofone or two hundredweight, they were taken to a farm some miles away, instead of stayingon the Cyclotron Building roof at Hammersmith Hospital. However, the Medical ResearchCouncil, in a spectacular piece of mistiming, decided to close down its RadiotherapeuticResearch Unit at Hammersmith in 1961, when the Director, Dr Constance Wood, retired in1962. They were entirely entitled to do this legally, and closing Units always looked good

Review R269
in the top-level reports. Staff left and our pig follow-up was not done. Much later, thesubject of radiation oncology has recovered (and the MRC Cyclotron has become the newGeneral Electric Company (GEC) Positron-Producing Centre). However, our late effects onpigs were only clarified 20 years later, by Withers et al (1982a), on pigs in Texas, when thelinear-quadratic formulation was available to explain very logically the different effect of sizeof dose-per-fraction on late and early skin reactions.
I then spent an illuminating year with Professor Joseph Rotblat at St BartholomewsMedical School, learning about the dedication of university teachers, especially at examinationtime! With Patricia Lindop we developed the mouse foot skin scoring system of threeobjectively characterized levels (Fowler et al 1965), which has since become used in othercentres too (Moulder and Fischer 1976, van Rongen and Kal 1984).
In 1963 I returned to Hammersmith to establish a new University Department of MedicalPhysics and soon acquired a small team of postgraduate students, some on radioisotopescanning with John Mallard and later Harold Glass, the others on radiobiology with me. Thefirst was Julie Denekamp, fresh from a first Class BSc in Biology. (She couldn’t followher first preference which was Marine Biology, because of sea-sickness, although she wasthe daughter of a Dutch sea-captain.) Others during seven years included Tony Howes,Jolyon Hendry, Mossaad Hegazy, Adrian Begg, Fiona Stewart and Sally Hill, all of them nowdistinguished in associated topics. The last three moved with me to Mount Vernon whenI was invited there in 1969. I was very flattered to be asked to be asked to follow Oliver Scottwhen he retired as Director of the British Empire Cancer Campaign (BECC) Research Unitin Radiobiology (RUR). Glory indeed, to follow Hal Gray there too . . . and fewer Universitycommittee meetings than Professors had! The BECC became the Cancer Research Campaign(CRC) and the RUR became the Gray Lab (now the Gray Institute Trust). Nick McNallyjoined the Gray Lab from Hammersmith a few years later.
5. Opportunities to do some definitive experiments
During our seven years at the Royal Postgraduate Medical School at Hammersmith Hospital,this little team in one quarter of the Medical Physics Department carried out many experimentson the radiation reactions in mouse skin and rat tumours, in happy collaboration with the MRCCyclotron Unit. They were building up the picture of 10% of labelled cells proliferating inthe basal layer, then progressing at their usual rate through the differented layer towards thesuperficial squamous epithelium, there to flake off naturally in about 5 days in mice (Hegazyand Fowler 1973). Irradiation would cause proliferation in the basal layer to decrease, so thatflaking off would occur after a few days delay, longer in fractionated irradiation and lowerdoses. After higher doses a moist desquamation reaction could occur. This would later healup, or not, depending how many cells per mm2 survived the total radiation depletion minusrepopulation. Julie Denekamp modified our 3-point scale to include 1
4 points, giving a 12-pointscale (Denekamp 1973) and we learnt to avoid the moist desquamation reactions in nearly allof our mouse experiments. Some of the skin cell kinetic work was done in collaboration withNorwegian cell kineticists (Iverson et al 1976), using thymidine autoradiography.
An important step in radiotherapeutic understanding was made by Denekamp (1973)while at Hammersmith, published in the BJR 3 years later, using the technique she developedof ‘top-up doses’. First a single-dose response curve would be established for the strain ofmice to be used, at the kilovoltage of x-rays to be used. This would be designated ‘single-dose-only’. The full treatment to be investigated was 20 fractions of 300 rads of x-rays(300 cGy) given in 4 weeks, so a dose–response curve was next obtained for that full schedule,reading the skin reactions every day for 3 weeks after the last irradiation, and averaging them

R270 Review
0 10 20 30
0
4
8
12
16
I I I I I I I I I I I I I I 3 Gy fractions + Top-up Dose
CONTRAST BETWEEN OLD THEORETICAL AND REAL BIOLOGICAL TIME FACTOR
Acute reactions of mouse feet,
130 cGy per day
T
TheoreticalNSD & TDFPower Law 0.11
Experimental BiologicalResult (Denekamp 1973)
Ext
ra d
ose
fo
r Is
o-e
ffec
t (G
y)
Time after first fraction (Days)
Figure 2. Experimental results from mouse skin (full curve, Denekamp 1973) during daily dosesof 3 Gy five times a week, contrasted with the power-law assumption of total dose = (overall time)to the power 0.11, (dashed curve, NSD = k T 0.11, Ellis 1969). The real biological response consistsof no compensatory repopulation until about 12 fractions, then a steep increase in dose-per-dayrequired to produce a constant skin reaction, slowing after the end of the 15-fraction irradiation.
to obtain an ED-50 for the full schedule. (ED50 is the dose at which 50% of the mice reach astated level of skin reaction) The experiment was to determine the ED50 at various intervalsbefore the end of a full fractionated schedule. After say 15 fractions in 3 weeks, a test singledose would be delivered immediately after the last of the 15 fractions, followed by the usualdaily readings of skin reactions on the mouse legs to establish another dose–response curve.This dose–response curve would have its centre point (ED-50) at a dose to the left of thesingle-dose-only curve, and the difference from the single-dose-only curve would indicate thedose equivalent of the 15F schedule. The top-up method has since been validated many times,later using neutrons as top-up doses to minimize intracycle variations of cell radiosensitivity(Joineret al 1986).
Thus the dose equivalent of the 15 fractions including any repopulation occurring duringits 3 weeks of irradiation was determined. This procedure was repeated for 5 and 10 fractionsin 1 and 2 weeks respectively, to build up a profile of the time course of repopulation during‘daily’ fractionated irradiation of mouse skin. It was thus discovered that repopulation didnot follow a power law as previously thought, but instead had a delayed start, then a rapidincrease of repopulation continuing for as long as the depletion by daily irradiation continued.As figure 2 shows, this time course was strongly contrasting with the assumption madeby the 0.11 power law of the ‘Cohen minus Strandqvist slopes = Ellis’s NSD’ (NominalStandard Dose) concept. It wasn’t the only criticism of Ellis’s NSD that was emerging, butit strengthened the criticisms. All of this picture of repopulation in skin was confirmed bydetailed radioautographic sections, with labelled cells and labelled mitoses, counted in thelaborious cell-counting microscopy that was a major adjunct to the skin-reaction scoring ofthe in situ experiments.
At the same time that we were obtaining RBE’s from the contrasting shapes of the deriveddose–response curves in pig and mouse skin, we were also collaborating with Dr EddieBarendsen from Rijswiik in The Netherlands on the MRC cyclotron, who was visiting usand measuring similar shapes in in vitro cell survival curves as a fundamental investigationinto size of targets in nuclei of mammalian cells (Barendsen et al 1963). These differentexperiments meshed together extraordinarily well.

Review R271
6. Animal radiobiology in the 1970s
In 1970 computer work was done by sending paper tapes to the University Computer Centreelsewhere in London and waiting for the output tape to be sent back for printing out. Wewere skilful at slide rules and reading accurately off mm graphs, and we tested each other ingraph-drawing competitions which Julie Denekamp often won (although she said she didn’tlike maths). Our earliest experiments were on mouse skin reactions as described above, soinvestigating the time courses of these reactions, and also of several types of mouse tumour,had made us very aware of the rapid rate of repopulation in many of those tissues, evenduring continuing daily irradiations: ‘Radiotherapy may be thought of as a two-horse race,between tumour repopulation on one hand and the acute skin or mucosal reactions on the otherhand . . . ’.
In 1970, five years after Hal Gray had died, my little team and I moved to Mount VernonHospital, to the BECC Radiobiology Research Unit. I was appointed Director, with BarryMichael, Harold Hewitt, Ged Adams and David Dewey already there and Julie Denekamp andNick McNally also to become Heads of the Sections. It was soon renamed the Gray Lab andwas enlarged to contain a new animal house with three 250 kV x-ray machines inside the sterileanimal quarters. This design, and a high productivity of clean and inbred mice from AngelaWalder, enabled us to do multi-fraction animal experiments on mice, as we had always wantedto do them. Just as many experiments were carried out on normal-tissue radiation effects ason tumour cure or regrowth delay. At that time the hypoxic cell radiosensitizers were justbeing discovered and characterized (as electron-affinic) and not too toxic (not too lipophilic),and much work went into the testing of them both in vitro and in normal tissues and varioustypes of tumours in mice. By about 1994 it appeared that the good radiosensitizer Roche 0582(later called Misonidazole) worked best when the radiotherapy schedule was substandard, forexample either too short or too long in weeks. For optimal radiotherapy however it gaveonly a small gain in tumour effect (the sensitizer enhancement ratio, SER). This was thoughtto be due to the successful reoxygenation of at least most of the hypoxic tumour cells by agood radiotherapy schedule (Fowler et al 1976). This was published as our first paper in theInternational Journal of Radiation Oncology, Biology and Physics (the Red Journal), after adelay of some 2 years. However, nobody seemed to want to know that interpretation. Therewere arguments about the relevance of mouse pharmacological doses of radiosensitizer todoses in human subjects, but eventually the plasma concentrations were found to be relevantfor the SER, rather than some folklore-ish rules.
The optimists still wanted to go ahead and test it in human tumours, and this was indeeddone thoroughly in many well-organized clinical trials. The results several years later were asdisappointing as the best of our mouse tumour fractionation results had been. At the same timethe Gray Lab concentrated on developing new methods of exploring late radiation reactionsby studying mice during their lifespan after irradiation, instead of sacrificing samples forpathology at intervals. The mice were always given partial-body irradiation to shield all partsexcept the target organ or tumour, sometimes using electron irradiation.
These methods included: (1) late Fibrosis in mouse feet—Julie Denekamp, FionaStewart, Mike Joiner versus acute reactions (desquamation in mouse legs)—Jack Fowler, JulieDenekamp, Bruce Douglas. (2) Breathing-rate changes in lungs up to 3 months (pneumonitis)compared with 6 months (fibrosis)—Elizabeth Travis, Boris Vojnevitch, Charles Parkins, JackFowler (Travis et al 1979). (3) Anaemia changes in plasma, not whole blood, at 6 monthsthat measure kidney damage with good sensitivity (Alpen and Stewart 1984). (4) Urinationfrequency to measure bladder damage (on a moving filter paper underneath mouse cages), atselected times after irradiation, with dye and UV irradiation to identify the urine spots more

R272 Review
readily (Stewart et al 1978, 1980). This simple but effective device was known as ‘the peeingmachine’. (5) Fecal frequency and stool length to measure rectal and colon damage—NickTerry and Anna Gasinska et al (1993). You can guess what this test was called colloquially.(6) A new ‘early’ endpoint was also developed for acute mucosal reactions in the lips ofmice, for applications in combined chemotherapy and radiotherapy results (Parkins et al 1983,including Professor Shen Yu from China).
Fiona Stewart and Julie Denekamp discovered, in labelled cell autoradiography in theGray Lab, that gross late complications occurred at about the same time as the labelling indexrose again after irradiation in its natural cycle, which had the duration of a year in mousebladder (Stewart et al 1978, 1980). This identified the natural pre-irradiation turnover time(Tpot, potential doubling time, Steel 1967) of a normal tissue as the main controlling factor ofwhether the important radiation damage in an organ occurred early or late. For some typesof late injury, the slow proliferation in normal blood vessel walls was the precipitating factor.Denekamp et al (1983) showed that the only rapidly proliferating cells in blood vessel wallswere in tumours, or in foetuses, or in wound healing. This gave impetus to the developmentof anti-angiogenic drugs for cancer treatment, which are still being developed.
We were greatly helped by a series of enthusiastic and bright young MDs or PhDs whocontinued the tradition of spending a year or two at the Gray Lab, including Eli Glatstein,Rick Brown, Lester Peters, Dennis Shrieve, John Moulder, Elizabeth Travis, Janet Rasey,Marvin Goldman, Anna Gasinska and others. Apologies for many omissions! In the mid-1970s, a young engineer-turned-radiation-oncologist called Bruce Douglas came to work onfractionation in radiotherapy at the Gray Lab, with a post-doctoral scholarship from Vancouver.His grandfather had named the Douglas Fir, and Bruce was an enthusiast about roses. Afterbrief discouragement away from using LD50 experiments, he agreed to use the acute skin-reaction system and quickly designed a system of three small pillars which held one hind legof a mouse. The mouse was enclosed in a lead box, with only its leg exposed to the x-raybeam in a circle of five lead boxes, to irradiate the legs of five mice simultaneously. With thisset-up much work was done. The upshot was a series of fractionation experiments using oneto 64 fractions, of size from 23 Gy to 1 Gy per fraction.
The ‘traditional’ plot of total isoeffective dose against fraction number showed a clearlycurving line (figure 3), instead of the straight log–log lines mandated by a power law. WhatBruce did was to plot it instead as reciprocal total dose, because simple algebra demonstratedthat this would only be a straight line if the cell survival curve of the critical (basal) cells hada linear-quadratic form. The data then demonstrated a straight line relating reciprocal totaldose to dose per fraction, and linear quadratic reared its head for multiple equal fractions(figure 4).
Further, reconstruction of the resulting iso-effect doses, divided by the fraction numberfor each fraction size, showed a very large shoulder, continuously bending to form the cellsurvival curve (figure 5, Douglas and Fowler 1976).
This demonstration that the linear-quadratic formula applied to gross reactions in tissuein situ came from these mouse experiments. However its application to clinical radiotherapydid not materialize until four or five years later. These experiments were the ones in which abulldozer in the hospital grounds dug up both the main electricity cable and the hospital watersupply. We had only 6 h intervals in that phase of experiments. The day was saved by twoitems. The local electricity company willingly provided a motor generator on a large truck,and the Gray Lab had earlier been fitted with a 4000 gallon water tank on the roof, althoughthe Cancer Research Campaign’s sharp accountants had needed much convincing by me afew years previously that we really wanted such a large water tank for just such experimentalcontinuity.

Review R273
1 10 10010
100Mouse foot skinacute reactions
Minimum 6 hour intervalsMaximum overall Time 8 days
Slope 0.33 (Cohen 1953)
Slope 0.22 (Strandqist 1944)
DOUGLAS & FOWLER 1976 Rad Res 66: 401-426 LQ CONTRASTED WITH POWER LAW
16
64321784 52
20
30
50
70
Log
10 T
ota
l Do
se (
Gy)
Log 10 number of equal fractions
Figure 3. Data from the multiple-equal-dose-fraction experiments on mouse foot acute skinreactions of Douglas and Fowler (1976), replotted from their table 2. The contrast from the straightlog–log lines of the previously utilized power laws is clear.
0 500 1000 1500 2000 2500
0.000
0.005
0.010
0.015
0.020
0.025
0.030
0.035
0.040
0.045
0.050
THE FIRST TEST OF LINEAR QUADRATIC FOR FRACTIONATED RT
32F64
17F
8F
5F4F
2 F
1 F
Douglas & Fowler Rad Res 66: 401-426, 1976
So α/β = 0.014 / 0.00135 = 10.4 Gy
-2
-1Intercept = 0.014 Gy
Slope = 0.00135 Gy
2520151050 I
-10.4 Gy intercept = - α //β Graphical confirmation
Rec
ipro
cal t
otal
dos
e 1/
Gy
Dose per fraction Gy
Figure 4. The same data as in figure 3 but replotted as reciprocal total dose versus dose-per-fraction, from the LQ equations (1) and (2), that log cell kill E = n (α + βd2) = nd (α + βd); sothat E/nd = (α + βd) where n is the number of equal fractions of d Gy, which is total dose. Theintercept on the Y axis is E/α and the slope is E/β, so their ratio gives α/β.
Meanwhile, Rod Withers, back in the USA, had an enforced gap in animal experimentsdue to delays in building a new animal laboratory for him when he moved from Houston to LosAngeles. He put this to good use by thinking more about the multi-fractionation experimentsthat he and Herman Suit, and we, and Barendsen and Van der Kogel and others had done.Instead of plotting ‘total tolerance doses’ against fraction number, he plotted them againstdose-per-fraction. He then saw that the slowly proliferating, late-reacting, normal tissues allhad much steeper slopes (more sensitive to fraction size) than the rapidly proliferating, earlyreacting, tissues. Most tumours were in the rapidly proliferating group. This major observationfitted in not only with our own animal experiments on skin versus kidney tolerance for example,

R274 Review
0 5 10 15 20 25
-12
-10
-8
-6
-4
-2
0
1/1
1/2
1/4
1/8
1/160
TOTAL ISOEFFECTIVE DOSE DIVIDED BY NUMBER OF FRACTIONS IN MULTI-EQUAL FRACTION EXPT: CONSTRUCTED MOUSE SKIN CELL SURVIVAL CURVE
16F
17F
32F
64F
8F
5F4F
2F
1F
Pro
port
ion
of to
tal t
reat
men
tco
ntrib
uted
by
each
frac
tion
Expt.pts TheoryLQ
2Dashed line LQ theory E = 0.145 d + 0.0139 d
Dose per fraction (Gy)
Figure 5. Surrogate cell-survival curve obtained by dividing each total iso-effective dose by thenumber of fractions, and plotting as a function of dose-per-fraction, to represent the proportion oftotal log cell kill caused by each fraction size.
but also with clinical observations from San Francisco (on lung and brain) and from Sweden(skin reactions in breast treatments), and the whole major late-versus-acute picture emerged(Withers et al 1982b). The difference between the late and early normal-tissue reactions hadnot emerged from Frank Ellis’s NSD or TDF concept, nor immediately from Barendsen’sextrapolated total dose, ETD. But all the attempts to fit animal and clinical data to any ofthose earlier concepts did help to lead to the differences now becoming clear. In spite of validcriticisms, Ellis’s NSD was still widely used, and a somewhat different variant (different intime factor) was proposed by Kirk et al (1971) of Glasgow, the Cumulative radiation Effect,CRE. Meanwhile Ellis’s NSD had been converted to ‘only-too-convenient’ tables by Ortonand Ellis (1973). When I went to work in Madison in 1988, every radiation oncology residenthad a copy of them in his or her pocket! However, the US Residents took quite rapidly to LQwhen I visited various medical schools to explain it (in terms of the Seven Steps to Heaven,see below).
7. Radiobiology in the 1980s
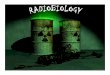
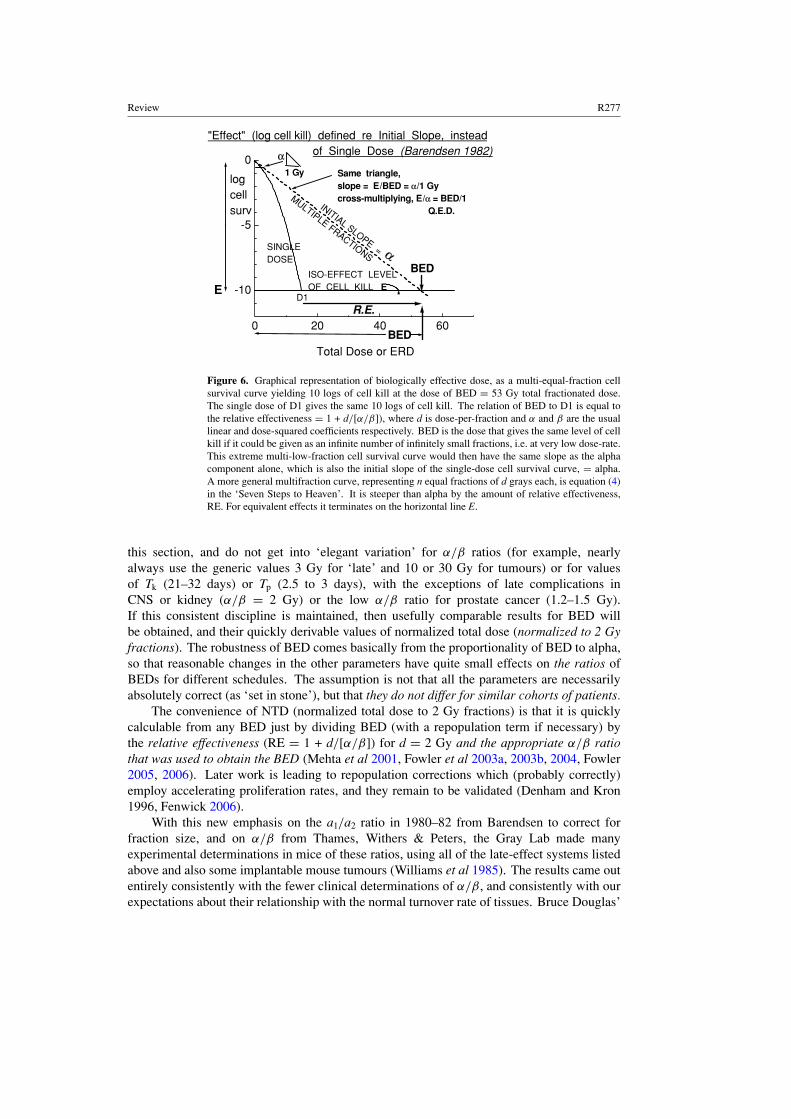
In my opinion the pivotal point of the iso-effect or ‘equivalent fractionation dose’ conundrumwas established when Eddie Barendsen at Rijswijk did a few more lines of inspired algebra withthe LQ formula and proposed the ‘log cell kill’ as the basic standard of comparison betweendifferent fractionation schedules, avoiding entirely any idea of an ‘equivalent single dose’which had haunted all previous attempts to rationalize the subject. He called his construct the‘extrapolated tolerance dose’, ETD, meaning extrapolated to zero dose-per-fraction or verylow dose rate. He used a term called relative effectiveness (RE = 1 + d/[α/β]) which is stillone of the most useful terms in the LQ formulations. He proposed that it should be applied tonormal-tissue complications, for any stated dose-per-fraction and total dose that representedthe tolerance dose for a given organ. However, although he did not pick up the differencejust described between late and early reactions, Barendsen’s construct and the emphasis onthe ratio α/β (which he preferred to call a1/a2) soon led to the rationalization of the whole

Review R275
subject in terms of linear quadratic as we know it today. The α/β terminology was preferredby Howard Thames who preferred it to the more mathematically traditional a1/a2, thus makingprinting-output difficulties that persist to this day. Does your printer ever come up with a pairof open squares instead? Several years of intensive experiments to establish the α/β values formany normal tissues and types of mouse tumour followed at the Gray Lab. Barendsen’s paperwas drafted in 1980—I have a copy—but the Red Journal took two years to review and publishit (Barendsen 1982). During this time we all carefully kept unworthy thoughts out of our heads.Had the Norte Americanos pirated Barendsen’s ideas and held up his publication? I do notbelieve that was true—Howard Thames and Eddie Barendsen had similar ideas independentlyand at the same time, when the concept of log cell kill and LQ was ready for all of us. Butthe suspicions helped speed up the birth of the journal Radiotherapy and Oncology (the GreenJournal) in Europe in the enthusiastic hands of Emmanel van der Schueren in Leuven. I washonoured to be the first author in it, with a paper credited with page 1, issue 1, volume 1, 1983.The theme was ‘La Ronde’—the close and interweaving contact between laboratory researchand clinical research, which must keep results feeding back and forth to each other. Yes,I was proud of that honour, but was amused to see a recent volume of R & O described by itscurrent Editor as: ‘The present issue celebrates the 75th anniversary volume of Radiotherapyand Oncology’ (Overgaard 2005). I knew it wasn’t 75 years since I had written that article,although plenty has changed! But the next sentence resolved the ambiguity: ‘The journalwas introduced in 1983 . . . ’ and the present Editor’s remark concerned the first issue involume 75.
What hasn’t changed, to our chagrin, is the amorphous situation of the solution to thehypoxic cell problem. Although hypoxic cells are disastrous if they remain present in a tumourduring treatment, does ordinary fractionated radiotherapy eliminate them by reoxygenationin most tumours? Evidence has been presented that among 8000 patients, only 5% sufferedfrom this disadvantage (7% in head-and-neck, Overgaard 1994). With any luck, and someseriously strong will, it ought to be possible to predict, before an individual radiotherapytreatment has gone many days, whether extra measures need to be taken in that patient to dealwith hypoxic tumour cells that are failing to reoxygenate sufficiently (Nordsmark et al 2005,Bentzen 2005b).
7.1. The Seven Steps to LQ Heaven, defined as ‘easily understanding the LQ formula forBED, and remembering it next week’
When it was realized that Barendsen’s ETD concept could be applied to any level of doseor biological damage, including tumour cell kill, not just ‘Tolerance of normal tissues’, itwas renamed ERD (extrapolated response dose), by which it is still known in some countries,especially The Netherlands. It took another seven or eight years, and the acquirement of flowcytometry results on the rapid proliferation of Tpot (potential doubling time, i.e. the birth rateof cells in the relevant tissue (Steel 1967.) to add a term representing repopulation of cellsduring continuing ‘daily’ irradiation to then produce the biologically effective dose of the‘Seven Steps to Heaven’. by which the LQ formulation is most conveniently taught (Fowler1989, 2006). The term BED turned out to be popular, but is occasionally used wrongly, thatis not according to equation (4) or (7).
E = log cell kill from n fractions of d grays
E = n(αd + βd2). (1)
E = nd(α + βd) (2)

R276 Review
To obtain a ‘BED’ we must divide by either α or β; and α gives us a more convenient number,actually in units of dose, than dividing by β, which would give a number in dose-squared(which Thames suggested as Total Effect); Barendsen chose E/α:
E/α = nd(1 + dβ/α) (3)
E/α = nd(1 + d/(α/β)). (4)
Equation (4) gives us ‘BED’ (or ERD) = log cell kill by radiation ignoring repopulation(Barendsen 1982).
Fowler (1989) suggested adding a subscript to BED comprising the α/β ratio assumed, toclarify that this is a derived ‘biological’ dose, not a real physical dose; and to identify the tissueα/β value assumed. Not adding such subscripts results in confusion between ‘biologicallyequivalent’ and real physical doses. Unfortunately you can see this error occurring in somepublished papers.
Then we need to subtract the log cell repopulation from the log cell kill. To do this wehave to assume several more parameters. First we assume an α/β ratio for the tissue irradiated(e.g. α/β = 10 Gy for rapidly proliferating and most tumour tissues, but α/β = 2 or 3 Gyfor late complications. Then we can assume a nominal alpha-value (e.g. 0.3 or 0.35 loge/Gy).Next we assume repopulation starts at the kick-off or onset time Tk days and continues untilthe end of the schedule at T days; so that the time available for proliferation is T − Tk days.Finally we assume a constant doubling time of Tp, after Tk. Note that Tp is not Tpot, whichis the doubling rate before any disturbance by radiation or other agent. It is the averagedoubling time between T and Tk, as a result of cell depletion which stimulates repopulation.Unfortunately Eric Hall omitted Tk in his otherwise very fine book (Hall 1994, 4th & latereditions) but its omission leads to much confusion, especially if a range of overall times isbeing considered which happens to include Tk in the middle!
E = nd(α + βd)) − (T − Tk)(loge 2)/Tp (5)
E/a = nd(1 + d/α/β)) − (T − Tk)(ln 2)/a Tp) (6)
BED = log cell kill by radiation minus log cell generation by
repopulation in the time (T − Tk) days. (Fowler 1989). (7)
Since the most influential variable in this formula is the ratio α/β, equally with dose-per-fraction, it is usual to designate a BED by means of a subscript, such as 100 Gy3 for latecomplications (assuming α/β = 3 Gy) or 75 Gy10 for acute BED or tumour BED (assumingα/β =10 Gy). This not only clarifies at once what tissue we are talking about, but it alsodistinguishes between a physical dose and its ‘biologically equivalent’ conceptual dose. Theratio α/β then becomes a parameter that is a surrogate for ‘type of tissue’. Failure to usethese subscripts leads to much unnecessary confusion. Note than BED means biologicallyeffective dose, and the ‘equivalence’ is a simply derived concept from the LQ arithmetic, bestexpressed as the NTD (‘normalized total dose in 2 Gy fractions’), or occasionally as LQED(figure 6).
This algorithm has remained remarkably robust for more than 20 years. It has givenhelpful predictions of the relative strength of many clinical fractionation schedules, fromnon-standard schedules for head and neck radiotherapy or lung Ca to low- and high-doserate brachytherapy for carcinoma of cervix uteri or prostate (Mehta et al 2001, Fowler et al2003a, 2003b, 2004, Fowler 2005). The trick is to keep the predictive modelling simple—assume only a few well-accepted values for the parameters, including those mentioned in
Review R277
0 20 40 60
-10
-5
0
R.E.
logcellsurv
"Effect" (log cell kill) defined re Initial Slope, instead of Single Dose (Barendsen 1982)
SINGLEDOSE
D1
Same triangle,slope = E / BED = α/1 Gycross-multiplying, E/α = BED/1 Q.E.D.
BED
BED
α1 Gy
α
INITIAL SLOPE =
MULTIPLE FRACTIONS
ISO-EFFECT LEVEL OF CELL KILL EE
Total Dose or ERD
Figure 6. Graphical representation of biologically effective dose, as a multi-equal-fraction cellsurvival curve yielding 10 logs of cell kill at the dose of BED = 53 Gy total fractionated dose.The single dose of D1 gives the same 10 logs of cell kill. The relation of BED to D1 is equal tothe relative effectiveness = 1 + d/[α/β]), where d is dose-per-fraction and α and β are the usuallinear and dose-squared coefficients respectively. BED is the dose that gives the same level of cellkill if it could be given as an infinite number of infinitely small fractions, i.e. at very low dose-rate.This extreme multi-low-fraction cell survival curve would then have the same slope as the alphacomponent alone, which is also the initial slope of the single-dose cell survival curve, = alpha.A more general multifraction curve, representing n equal fractions of d grays each, is equation (4)in the ‘Seven Steps to Heaven’. It is steeper than alpha by the amount of relative effectiveness,RE. For equivalent effects it terminates on the horizontal line E.
this section, and do not get into ‘elegant variation’ for α/β ratios (for example, nearlyalways use the generic values 3 Gy for ‘late’ and 10 or 30 Gy for tumours) or for valuesof Tk (21–32 days) or Tp (2.5 to 3 days), with the exceptions of late complications inCNS or kidney (α/β = 2 Gy) or the low α/β ratio for prostate cancer (1.2–1.5 Gy).If this consistent discipline is maintained, then usefully comparable results for BED willbe obtained, and their quickly derivable values of normalized total dose (normalized to 2 Gyfractions). The robustness of BED comes basically from the proportionality of BED to alpha,so that reasonable changes in the other parameters have quite small effects on the ratios ofBEDs for different schedules. The assumption is not that all the parameters are necessarilyabsolutely correct (as ‘set in stone’), but that they do not differ for similar cohorts of patients.
The convenience of NTD (normalized total dose to 2 Gy fractions) is that it is quicklycalculable from any BED just by dividing BED (with a repopulation term if necessary) bythe relative effectiveness (RE = 1 + d/[α/β]) for d = 2 Gy and the appropriate α/β ratiothat was used to obtain the BED (Mehta et al 2001, Fowler et al 2003a, 2003b, 2004, Fowler2005, 2006). Later work is leading to repopulation corrections which (probably correctly)employ accelerating proliferation rates, and they remain to be validated (Denham and Kron1996, Fenwick 2006).
With this new emphasis on the a1/a2 ratio in 1980–82 from Barendsen to correct forfraction size, and on α/β from Thames, Withers & Peters, the Gray Lab made manyexperimental determinations in mice of these ratios, using all of the late-effect systems listedabove and also some implantable mouse tumours (Williams et al 1985). The results came outentirely consistently with the fewer clinical determinations of α/β, and consistently with ourexpectations about their relationship with the normal turnover rate of tissues. Bruce Douglas’

R278 Review
rapid way of finding α/β was to plot the graph of reciprocal total iso-effective dose againstdose-per-fraction, for a constant radiation effect from the different schedules, at the same,preferably short, overall time. A straight line demonstrated that the LQ model was valid.Alpha was the intercept on the reciprocal-total-dose (Y) axis and beta was the slope of thebest straight line through the points, which also extrapolated back to minus α/β Gy on thedose-per-fraction (X) axis. Howard Thames showed that this method had the flaw of usingdose-per-fraction both in the denominator and the numerator of the ratio, so the apparent 95%confidence limits were not correct even if α/β was. He developed instead a computer methodcalled direct analysis which is now the standard method. Many papers were written, somein collaboration with Howard, during the 1980s. The reciprocal plot method, which BruceDouglas called the ‘Fe method’ (for fraction effective, and also out of respect for Frank Ellis,who became 100 years old in 2005 as I write), remains a quick method of estimating anapproximate α/β value. (Sadly, Frank Ellis died 5 months later).
Many were the arguments at international meetings between Howard Thames and me aboutthe importance of repopulation, or even its existence. Howard did not want to assign much ifany importance to tumour repopulation, and the observations were always that more dose wasneeded if a treatment took longer. Among the many ingenious alternative arguments, a changein radiosensitivity as treatment proceeded was one. However, if repopulation occurred, theaccelerated proliferation led to an increase in the intrinsic radiosensitivity term (alpha), whichwould require less total dose instead. Another argument was a possible increase in hypoxia, theopposite of re-oxygenation; which is unlikely in a shrinking tumour. Julie Denekamp and I hadhowever seen the effects of repopulation in tumours very clearly and unambiguously throughcell kinetics observations in various mouse experiments. I think we won in the end. I rememberbeing thoroughly ‘told off’ by the distinguished radiation oncologist Maurice Tubiana at ameeting in Italy about 1976: ‘Of course, Jack, there is no proliferation in tumours duringradiotherapy—everybody knows that the [thymidine] Labelling Index falls to zero in tumoursafter irradiation, and does not rise again while irradiation continues . . . ’. It wasn’t until afterI had retired from the Gray Lab in 1988 and had time to think in Madison, that I could collectenough clinical data to show that repopulation was very important in human tumours too. ‘Ohno, Jack—these are not randomized controlled clinical trials, they are just retrospective data.’Meanwhile, Rod Withers’ ‘dog-leg’ curve (Withers et al 1988) (also of mostly retrospectivedata from thousands of patients worldwide) was even more convincing than my 12 retrospectiveseries that averaged a 12% loss of local control per week of prolongation in head-and-neckcancer (Fowler and Lindstrom 1992). Both results still hold today. I support the idea thatto neglect retrospective data and carefully observed clinical series, just because they are notrandomized into two groups, is to miss out often on important trends.
It was Travis and Tucker (1987) from Howard Thames’ institute, who wrote down,apparently without believing it themselves, the appropriate algorithm for two-step repopulationshown in steps 5 to 7 above, that we needed in order to upgrade Barendsen’s ERD to the morecomprehensive BED. Jan van der Geijn told me about it, and it suddenly went ‘Click!’ justafter I arrived in Madison (Fowler 1989).
All of this growing experience emphasized the importance of overall time in most typesof tumour, with the important exception of prostate cancer. Before I retired from the GrayLab in 1988 Begg et al (1992) and George Wilson had done much work on the pre-treatmentrate of cell birth called Tpot (potential doubling time, before allowing for cell loss fromapoptosis or nutritional deficiency). They showed that it was faster in most animal and humantumours than in most normal tissues, before any compensatory repopulation stimulated bythe treatment. Julie Denekamp and I together with Drs (later Professors) Stanley Discheand Michelle Saunders at the Mount Vernon Regional Radiotherapy Centre designed the

Review R279
CHART schedule (Continuous Hyperfractionated Accelerated Radiation Therapy). This wasthe shortest that we could design, using three fractions a day with reduced size fractions of1.5 Gy to avoid late injury, yet to give an approximate 10 logs of cell kill. The overalltime was 12 days, or strictly 11.5 days starting at ‘day zero’ with the first fraction. Theminimum interval was 6 h, and was found to fit in with staff if they were allowed flexiblehours. This has been much used since then in ten of the regional centres in the UK for lungcancer, because it gives a better tumour result than the standard 60 Gy at 2 Gy fractions.CHART was determined by the UK Ministry of Health to be the most economic treatmentfor inoperable lung cancer. This schedule was based on the radiobiological theory that theshortest overall time that could be tolerated should be tested, with the smallest doses perfraction that would build up to an adequate dose. However it omitted the consideration ofTk, that the shortest overall time need not theoretically be shorter than the kick-off or onsettime of tumour cell repopulation, thought now to be 21 to 32 days in head and neck cancerand non-small-cell lung cancer and unlikely to be much shorter; but may be longer in prostatecancer (see section 11). However, for head-and-neck tumours other non-standard fractionationschedules have been found to give better, although not more economical, results than thestandard schedules of 3–5 weeks (up to about 11 logs of tumour cell kill, Fowler 2006).Although economical and effective versus only 60 Gy NTD, the three fractions a day for12 days without a weekend gap is thought to be organizationally cumbersome for some centres(Lievens et al 2005).
It is a relatively new idea in clinical radiotherapy (10 or 15 years) that shorter overall timesthan 6 or 7 weeks would be worth exploring, first in head and neck tumours and more recentlyin lung tumours, probably many other types too. As an experimental tumour biologist, I haveoften wondered why it took so long. As an analyser of clinical results, I look at the confidenceintervals and am disappointed to find why! The 95% confidence intervals are so wide, mostlybecause of too few patients, that most radiobiological parameters are poorly defined. Peoplewant more proof than any one trial of even 400 or so patients in two arms can provide.
8. Radiobiology in the 1990s and 2000s
Radiobiological modelling was then just finding its feet in designing various non-standardfractionation schedules, with head-and-neck schedules leading the way because a 2- or3-year result was the earliest response among common human tumours for monitoring results.We now had a reasonably reliable way of comparing schedules, and even for estimatinga therapeutic gain (tumour BED divided by late normal tissue BED.) The final weaponin the present three-weapon armoury was however proposed only three years ago (Fowleret al 2003b), making the prediction of an acute BED at last reasonably possible, beforeactually treating a patient with any proposed new schedule, and together with a dose-escalationintroductory trial. The whole procedure then consists of three predictive calculations:
8.1. Estimation of late complications BED
BED = total dose × RE where RE = (1 + d/[α/β]) with α/β = 3 Gy for most late effects,(except CNS and kidneys where α/β = 2 Gy), and d is the dose per fraction. No allowancefor overall time is normally made, because late responding normal tissues have little or norepopulation during the weeks of radiotherapy. For very high total doses, >70 Gy NTD (in 2Gy fraction equivalent) a volume limitation may be known, like those for area of rectal walllisted by Vargas et al (2005). For normal tissues with a range of doses across an organ (which

R280 Review
is not rare), the equivalent uniform dose EUD is a good way of correcting for the local effectof fraction size (Niemierko). It can be used with a differential (DVH) dose volume histogram.
From this BED the NTD in 2 Gy fractions is obtained by dividing by 1.67 if α/β = 3and by 2.0 if α/β = 2 Gy. Most total BEDs should not exceed 117 Gy (NTD 70 Gy), butexceptions occur in brachytherapy for Ca prostate or cervix where BEDs of about 133 Gy3are given, but with a limitation to only 1 or 2 sq cm of rectal wall (Fowler 2005).
8.2. Estimation of tumour BED
BED = total dose × (1 + d/[α/β]) minus(loge 2)(T − Tk)/α Tp. (8)
Here T is overall time (the first fraction is given on day 0). Tk is the kick-off time for tumourcell repopulation, which occurs at an assumed average doubling time of Tp days. Tp has beenderived from data on delayed treatments in some tumours. For head and neck and for lungtumours, Tp = 3 days. Tk is less certainly known, but 21–32 days have been suggested soI often assume Tk = 28 days.
From this BED an NTD is obtained by dividing by 1.2, i.e. by RE for 2 Gy withα/β = 10, (RE = 1 + 2/10). Preferably a corresponding TCP can be looked up from aknown dose–response curve derived from a meta-analysis, usually for NTD in 2 Gy fractions.Failing this, a gamma-50 slope of 2.0 or 1.5 could reasonably be assumed for many types oftumour. From the BED, the ‘nominal log cell kill’ (for a given α/β and α value) can readilybe calculated because BED = (loge cell kill)/alpha by definition.
I have found no satisfaction in allowing for hypoxia in tumours—that is, no lack ofmeaningful correlations by ignoring hypoxia. Furthermore, Overgaard (1994) showed thatonly 5% of 7921 patients overall (but 7% in head and neck) appeared to be influencedby any of the methods to overcome hypoxia. It appears to me that most tumours mightreoxygenate themselves satisfactorily. However, many publications have demonstrated thatwhen a significant proportion of hypoxic cells can be measured in a subset of tumours, forexample by electrical probes, the clinical outcome is worse. The topic obviously continues tofascinate the field because the effect is potentially large, where reoxygenation does not solveit naturally. The increasing use of various positron-emitting markers could lead to specificmethods for individual patients, and so to choices of chemical radiosensitizers, or treatmentfor heavy ions rather than photons, and generally individual diagnosis and planning. A veryrecent publication (Nordsmark et al 2005) has shown that a high degree of hypoxia (definedby the 2.5 mmHg pO2 level) was significantly linked to treatment failure in an overview of397 head-and-neck cancer patients from seven centres. The difference in survival at 3 yearswas 10% (37 versus 47%). Nevertheless, until we routinely identify and treat these patientsdifferently, there seems no point in allowing for hypoxia in quantitative tumour modelling,especially in other body sites. I hope this might change.
8.3. Estimation of acute mucosal reaction BED
This is the third weapon in the triple armoury (Fowler et al 2003b). It is important becauseif the patients do not tolerate the acute stage of reactions, then that schedule will not be used.Or perhaps it will be used, but with gaps in the treatment which would spoil the tumour effectbecause of extra tumour cell repopulation, at a rate of about 0.7 Gy10, equivalent to 0.6 Gy perday in 2 Gy fraction equivalent dose. The story of the long-term development of this weaponis detailed by Fowler et al (2003), who found a ‘grey zone’ of tolerance dose at 59 to 63 Gy10
(NTD = 49–52.5 Gy in 2 Gy fractions) for head-and-neck patients, if a particular set ofparameters was used to calculate the acute BED. These parameters were α/β = 10 Gy;

Review R281
alpha = 0.35 Gy−1; Tk = 7 days and Tp = 2.5 days. This system works for schedules aswidely different as the CHART 36F × 1.5 Gy in 11.5 days, to the hyperfractionated 68F ×1.2 Gy or 60F × 1.3 Gy in seven weeks. The field sizes were typically large for head-and-necktreatments before the introduction of IMRT (intensity modified radiotherapy). It is a newgame to determine what tolerance doses to specific volumes of tissue might be achievablewith IMRT, but the present 59–63 Gy10 and 49–52.5 Gy NTD represent the levels appropriatebefore IMRT was widely used. It also appears to work for rectal mucosa in patients treatedfor prostate ontrol carcinoma by hypofractionation at 3 Gy per fraction (Leborgne and Fowler2005). This is important in hypofractionation, because if fewer fractions are used, they shouldsometimes be given on only three or four days per week instead of the usual five, to avoidmucosal over-reactions. For the rectal site, there are also volume constraints at high totaldoses (Vargas et al 2005).
9. Conclusions from modelling head-and-neck non-standard fractionation
It was difficult to find tolerable schedules as short as the theoretically desirable values closeto Tk, largely because of the limiting acute reactions (Kaanders 2002). During the 1990s anumber of non-standard fractionation schedules were used to treat head-and-neck cancer, withinteresting results. Four of these well-known schedules were ingeniously designed to achievea nominal 11.5 log10 of cell kill, but they caused too much normal tissue damage—some latebut others early—and had to be reduced in total dose or in dose-per-fraction. When adjustedclinically to be acceptable, they were all then found to deliver 11.0–11.2 log10 cell kill in thepresent modelling, in agreement with several other well-known schedules that had been foundstrong but acceptable. All this provides good evidence for the robustness of this modelling.Further, it was found that the acute mucosal tolerance BEDs were reduced from above tobelow the limiting values set out above as weapon 3 (Fowler et al 2003b). This means thatacute mucosal tolerance is at least as important as late complications, as suggested by Kanders(2002). This acute mucosal BED is reduced by 0.8 Gy10 per day (0.67 Gy per day in 2 Gyfractions equivalent) if a few more days are added to the overall time for this adjustment(Fowler 2006). The late complications were found to be reduced but not to any common level(105–113 Gy3 instead of 117 Gy3). In 1996 Hendry et al (1996) published a landmark paperin which LQ modelling was used to delineate the loss of local tumour control if one or moretreatment days was omitted from a planned radiotherapy treatment. As a result the UK RCR(Royal College of Radiology) proposed rules for correcting for such gaps, and many centresoverseas followed them in developing procedures for avoiding gaps. This is an example whereradiobiology modelling certainly changed the clinical practice of radiotherapy.
It appears that for tumour cell kill, the level of about 11.0–11.2 log10 is the maximumthat is likely to be possible with radiotherapy alone for head and neck tumours. It remains tobe proven whether chemotherapy can add to this without excessive acute reactions. PerhapsIMRT will also enable this tumour log cell kill record to be broken. We are now talking aboutadvanced head-and-neck tumours of stages III and IV. The limiting late complication BED is117 Gy3 (NTD = 70 Gy in 2 Gy fractions) and the limiting acute mucosal BED is 59–63 Gy10
(NTD = 49–52.5 Gy).This whole question of optimum fractionated radiotherapy for head-and-neck Ca is
discussed thoroughly in a chapter being published this year (Fowler 2006). The additionof chemotherapy, which for head-and-neck tumours should be done concomitantly, requiresthat we should choose the best radiotherapy-only schedules. Six such schedules provide justover eleven logs10 of estimated tumour cell kill, and another six schedules come second withabout 10.5 logs (Fowler 2006). The average 3-year locoregional control values are 54 and 47%

R282 Review
respectively for advanced patients, stage III and IV. The briefest summary is that an overalltime of 4 or 5 weeks (theoretically, close to Tk) gives the best ratio of log cell kill in tumoursto either acute or late complications, and that 2 fractions per day can give about 8% betterLRC than once a day. But the bottom line is that we still need reliable tests to choose whichpatients to offer short radiotherapy schedules to, for specific individuals only. Perhaps it willcome from PET scanning (positron emission tomography).
10. General conclusions about modelling from 1950 to now
Having solved the main problems of non-standard fractionation does not mean that we needno more animal radiobiology. The ability to direct irradiation to millimetre accuracy bringsnew challenges of just where to place the prescribed margin of a high-dose region. Should itbe at least 6–8 mm outside the visualized tumour bulk, as Giraud et al (2000) have suggestedbased on histologic studies in lung cancer? This question, as it concerns various sites ofhuman tumours, can be answered only by human studies, which are now feasible. But theobverse—where can critical boundaries be placed for normal tissues when quite unusuallysmall volumes can in principle now be selected?—can, and should, be answered by appropriatestudies in small animals, with the mini-CT (computer tomography) and mini-MRI (and – MRS)(magnetic resonance imaging and spectroscopy) methods now available, as some small-animallaboratories are now gearing up to do.
One of the most important things about modelling is to answer the criticism of somepanicky critics who throw up their hands and say ‘Well, you can get any answer you wantjust by choosing a different set of modelling parameters or variables.’ That’s not true ifyou are using the modelling to compare different schedules, say two protocols for treating agiven type of tumour, as you usually need to do. There is a natural stability in BED becauseBED = E/α, and because E and α are proportional to each other, by definition. This meansthat the ratio of BEDs for two different protocols will vary little for a wide range of reasonablevalues chosen for the other parameters. The assumption is not that all the radiobiologicalparameters are absolutely correct (as ‘set in stone’), but that the parameters for patients inone set of patients is similar to those in the other set of patients. Unlike some other attemptsat modelling, the number of initially viable cells per mm3 is irrelevant to LQ modelling fortime-dose evaluations, being cancelled out against radiosensitivity: (α against BED = E/α) inthe standard formulation. This stability is also true of EUD (equivalent uniform dose, the dosethat gives the same calculated log cell kill as the DVH you are looking at (Niemierko 1997)).
11. A clinically helpful but initially puzzling reversal of radiobiological factors
Before the 1990s we had become accustomed to the dictum that it was best to use a largenumber of small fractions (1.8–2 Gy) for most situations of malignant tumours close to criticalnormal tissues, limited only by keeping overall time short so as to avoid some tumour cellrepopulation. We were accustomed to assuming α/β = 10 Gy for tumours but α/β = 3 Gyfor late complications, the main hazard. Hypofractionation (doses per fraction above about2 Gy) was considered too damaging for late complications because of the lower α/β ratioHowever, the realization that it was the slow proliferation in the late responding tissues thatwas associated with the disproportionate effect of the larger dose-per-fraction—in accordancewith LQ modelling—that gave Duchesne and Peters (1999) the idea of suggesting large dosesper fraction to treat the slowest growing human tumours, prostate cancer. That realization hadbeen growing for a year or two (Haustermans et al 1997), and it was Brenner and Hall (1999)

Review R283
who analysed the available clinical data and first showed it to be true in clinical results. Acontinuous low dose rate from an I-125 permanent implant giving 145 Gy yielded the samelocal control as half that dose in 2 Gy fractions from linac treatments. Why so different?Radiobiological modelling showed that instead of an α/β ratio of 10 Gy (as in most othertumours), the α/β ratio for prostate tumours was uniquely as low as 1.5 Gy. This inverted theusual ratio with respect to the late complications in rectum, which itself has an α/β ratio ofabout 3 Gy. Much discussion followed this ‘realization from the basic radiobiology’ (Fowleret al 2001, 2003a), but later clinical results, not depending on low dose rate treatments, haveconfirmed that it is true and useful (Fowler 2005, Fowler et al 2006). It is rare that nature handsus a cancer situation where an improved treatment goes hand in hand with a shorter and moreconvenient one. Radiobiological modelling has aided the acceptance of this unique differencefrom the earlier general teaching (which is still correct for tumours other than prostate Ca).This exception is for a good radiobiological reason that proliferation in prostate tumours isexceptionally slow. This is another example where radiobiological modelling is changing theclinical practice of cancer treatment, in this case for prostate cancer.
12. The future
Bentzen (2005b) has written a wide-ranging review entitled ‘Theragnostic imaging . . . ’ whichdescribes the role of visualizing specific cellular biochemical processes, for example by PETscanning of tumours and normal tissue, which might enable treatments to be tailored to theelimination of individual tumours with minimal other radiation damage. Specific targetsalready in our sights, if not quite in our hands, include rapid repopulation in tumours, orthe failure of hypoxic cells to reoxygenate (Nordsmark 2005), or vulnerability to multi-genemanipulation. These will be exciting steps to explore in the next phase of radiobiology. Thecontinuing virtue of ionizing radiation over any drug or gene-based therapy is that ionizingradiation does certainly reach the cells that the physical plan encompasses, more accuratelythan ever before.
References
Alpen E L and Stewart F A 1984 Radiation nephritis and anaemia: a functional assay for renal damage after irradiationBr. J. Radiol. 57 185–7
Alper T A and Hornsey S 1973 The effect of hypoxia during irradiation on four-day death in mice given single andsplit doses of electrons Br. J. Radiol. 41 375–80
Barendsen G W 1982 Dose fractionation, dose rate, and isoeffect relationships for normal tissue responses Int. J.Radiat. Oncol. Biol. Phys. 8 1981–97
Barendsen G W, Beusker T l J, Vergroesen A J and Budke I 1960 Effects of different ionizing radiations on humancells in tissue culture: II. Biological experiments Radiat. Res. 13 841–9
Barendsen G W, Walter H M D, Fowler J F and Bewley D K 1963 Effects of different ionizing radiations on humancells in tissue culture: III. Experiments with cyclotron-accelerated alpha-particles and deuterons Radiat. Res.18 106–19
Begg A C, Holland I, Van Glabbeke M, Bartelink H and Horiot J C 1992 Predictive value of potential doubling timefor radiotherapy of head and neck tumor patients: results from the EORTC Cooperative Trial 22851 Semin.Radiat. Oncol. 2 22–5
Bentzen S M 2005a Radiation therapy: intensity modulated, image guided, biologically optimized and evidence based[Editorial] Radiother. Oncol. 77 227–30
Bentzen S M 2005b Theragnostic imaging for radiation oncology: dose-painting by numbers Oncology The Lancet6 112–6
Brenner D J and Hall E J 1999 Fractionation and protraction for radiotherapy of prostate carcinoma Int. J. Radiat.Oncol. Biol. Phys. 43 1095–101

R284 Review
Cohen L 1952 Radiotherapy in breast cancer: 1. The dose–time relationship: theoretical considerations Br. J. Radiol.25 636–42
Demanes D J, Rodriguez R R, Schour L, Brandt L D and Altieri G 2005 High-dose-rate intensity-modulatedbrachytherapy with external beam radiotherapybfor prostate cancer: California Endocurietherapy’s 10-yearresults Int. J. Radiat. Oncol. Biol. Phys. 61 1306–16
Denekamp J 1973 Changes in the rate of repopulation during multifraction irradiation of mouse skin Br. J. Radiol.46 381–7
Denekamp J, Hill S A and Hobson B 1983 Vascular occlusion and tumour cell death Eur. J. Cancer Clin. Oncol.19 271–5
Denham J W and Kron T 2001 Extinction of the weakest Int. J. Radiat. Oncol. Biol. Phys. 51 807–19Douglas B G and Fowler J F 1976 The effect of multiple small doses of x rays on skin reactions in the mouse and a
basic interpretation Radiat. Res. 66 401–20Duchesne G M and Peters L J 1999 What is the α/β ratio for prostate cancer? Rationale for hypofractionated high-
dose-rate brachytherapy Int. J. Radiat. Oncol. Biol. Phys. 44 747–8Elkind M M and Sutton H 1960 Radiation response of mammalian cells grown in culture: I. Repair of x-ray damage
in surviving Chinese hamster cells Radiat. Res. 13 556–93Ellis F 1969 Dose, time and fractionation: a clinical hypothesis Clin. Radiol. 20 1–7Fenwick J D 2006 Delay differential equations and the dose-time dependence of early radiotherapy reactions: I. model
development Med. Phys. submittedFowler J F 1989 The linear-quadratic formula and progress in fractionated radiotherapy: a review Br. J. Radiol.
62 679–94Fowler J F 2001 Biological factors influencing optimum fractionation in radiation therapy Acta Oncol. 40 712–7Fowler J F 2005 The radiobiology of prostate cancer: new aspects of fractionated radiotherapy Acta Oncol.
44 265–75Fowler J F 2006 Practical time-dose evaluation, or How to stop worrying and love LQ 2006 Technical Basis of
Radiation Therapy 4th edn ed S H Levitt, J A Purdy, C A Perez and S Vijayakumar (Heidelberg: Springer)chapter 1 at press
Fowler J F, Chappell R J and Ritter M A 2001 Is α/β for prostate tumors really low? Int. J. Radiat. Oncol. Biol.Phys. 50 1021–31
Fowler J F, Harari P M, Leborgne F and Leborgne J H 2003b Acute radiation reactions in oral and pharyngeal mucosa:tolerable levels in altered fractionation schedules Radiother. Oncol. 69 161–8
Fowler J F, Kragt K, Ellis R E, Lindop P J and Berry R J 1965 The effect of divided doses of 15 MeV electrons onthe skin response of mice Int. J. Radiat. Biol. 9 241–52
Fowler J F and Lindstrom M J 1992 Loss of local control with prolongation in radiotherapy Int. J. Radiat. Oncol.Biol. Phys. 23 457–67
Fowler J F et al 2006 Prostate cancer is best treated using hypofractionation: [Medical Physics Debate] ed C G OrtonMed. Phys. at press
Fowler J F, Ritter M A, Chappell R J and Brenner J D 2003a What hypofractionated protocols should be tested forprostate cancer? Int. J. Radiat. Oncol. Biol. Phys. 56 1093–104
Fowler J F, Sheldon P W, Denekamp J and Field S B 1976 Optimum fractionation of the C3H mouse mammarycarcinoma using X-rays, the hypoxic-cell radiosensitizer Ro-07-0582, or fast neutrons Int. J. Radiat. Oncol.Biol. Phys 1 579–92
Fowler J F and Stern B E 1963 Dose rate effects: some theoretical and practical considerations Br. J. Radiol.33 389–95
Fowler J F, Tome W, Fenwick J and Mehta M 2004 Stereotactic body radiotherapy; a challenge to conventionalradiation oncology Int. J. Radiat. Oncol. Biol. Phys. 60 1241–56
Gasinka A, Dubray B, Hill S A, Denekamp J, Thames H D and Fowler J F 1993 Early and late injuries in mouserectum after fractionated x-ray and neutron irradiation Int. J. Radiat. Oncol. Biol. Phys. 26 244–53
Giraud P et al 2000 Evaluation of microscopic tumor extension in non-small-cell lung cancer for three-dimensionalconformal radiotherapy planning Int. J. Radiat. Oncol. Biol. Phys. 48 1015–24
Gray L H and Scholes M E 1951 The effect of ionizing radiations on the broad bean root—Part VIII Br. J. Radiol.24 285–91
Hall E J 1988 Radiobiology for the Radiologist 3rd edn (Philadelphia: JB Lippincott Co.) p 535Hall E J 1994 Radiobiology for the Radiologist 4th edn (Philadelphia: JB Lippincott Co.) p 478Haustermans K M G, Hofland I, Van Poppel H, Oyen R, Van de Voorde W, Begg A C and Fowler J F 1997 Cell
kinetic measurements in prostate cancer Int. J. Radiat. Oncol. Biol. Phys. 37 1067–70Hegazy M A H and Fowler J F 1973 Cell population kinetics of plucked and unplucked mouse skin: II. Irradiated
skin Cell Tissue Kinet. 6 587–602

Review R285
Hendry J H, Bentzen S M, Dale R G, Fowler J F, Wheldon T E, Jones B, Munro A F, Slevin N J and Robertson A G1996 A modelled comparison of the effects of using different ways to compensate for missed treatment days inradiotherapy Clin. Oncol. (UKRCR) 8 297–307
Hornsey S 1973 The effectiveness of fast neutrons compared with low LET radiation on cell survival measured inthe mouse jejunum Radiat. Res. 55 58–68 See also figure 2.1 on p 24 in Thames H D and Hendry J H 1987Fractionation in Radiotherapy (London: Taylor and Francis) pp 297 and the present figure
Howard A and Pelc S R 1953 Synthesis of deoxyribonucleic acid in normal and irradiated cells and its relation tochromosome breakage Heredity (Suppl) 6 261–73
Iversen O H et al 1976 Cell kinetics in Burkett’s lymphoma Growth Kinetics and Biochemical Regulation ofNormal and Malignant Cells ed B Drewinsko and R M Humphrey (Baltimore: Williams and Wilkins)pp 675–86
Joiner M C, Denekamp J and Maughan R L 1986 The use of ‘Top-up’ experiments to investigate the effect of verysmall doses per fraction in mouse skin Int. J. Radiat. Biol. 49 565–80
Kaanders J H A M, Pop L A M, Marres H A M, Bruaset I, van den Hoogen J A, Merkx M A W and van der Kogel A J2002 Arcon: experience in 215 patients with advanced head-and-neck cancer Int. J. Radiat. Oncol. Biol.Phys. 52 769–78
Kirk J, Gtay W M and Watson E R 1971 Cumulative radiation effect: Part I. Fractionated treatment regimes Clin.Radiol. 22 145–55
Lea D E 1947 Actions of Radiations on Living Cells (Cambridge: The University Press)Lea D E and Catcheside D G 1942 The mechanism of the induction by radiation of chromosome aberrations in
Tradescantia J. Genet. 44 216–45Leborgne F and Fowler J F 2005 Acute toxicity following hypofractionated conformal radiotherapy of localized
prostate cancer. a nonrandomized contemporary comparison with standard fractionation Proc. 7th Time DoseFractionation Conference (Madison, Sept 2005) (AAPM)
Lievens Y, Kesteloot K and Van den Bogaert W 2005 CHART in lung cancer: Economic evaluation and incentivesfor implementation Radiother. Oncol. 75 171–8
Lievens Y and Van den Bogaert W [Editorial] 2005 Proton beam therapy: too expensive to come true? Radiother.Oncol. 75 131–3
Mackie R, Balog J, Ruchala K, Shepard D, Aldridge S, Fitchard E, Reckwert P, Oivera G, McNutt T and Mehta M1999 Tomotherapy Semin. Radiat. Oncol. 9 108–17
Mackie T R et al 2003 Int. J. Radiat. Oncol. Biol. Phys. 56 89–105Mehta M, Scrimger R, Mackie R, Paliwal B, Chappell R and Fowler J 2001 A new approach to dose escalation in
non-small cell lung cancer Int. J. Radiat. Oncol. Biol. Phys. 49 23–33Moulder J E and Fischer J J 1976 Radiation reaction of rat skin—the role of number of fractions and the overall
treatment time Cancer 37 2762–7Nagata Y, Takayama Y, Norihisa T, Mizowaki T, Sakamoto M and Hiraoko M 2004 Clinical outcomes of Phase
I/II study of stereotactic radiotherapy of 48 Gy in 4 fractions for primary lung cancer using a stereotactic bodyframe Int. J. Radiat. Oncol. Biol. Phys. 60 (Suppl) 1049 S285 (Abstract)
Niemierko A 1997 Reporting and analyzing dose distributions: a concept of equivalent uniform dose Med. Phys.24 103–10
Nihet K, Ogino S, Ishikura S, Nishimura H, Kawashima M, Ahahira S and Onozawa M 2004 Int. J. Radiat. Oncol.Biol. Phys. 60 (Suppl) 1043 S282 (Abstract)
Nordsmark M et al 2005 Prognostic value of tumor oxygenation in 397 head and neck tumors after primary radiationtherapy. An international multi-center study Radiother. Oncol. 77 18–24
Orton C G and Ellis F 1973 A simplification in the use of the NSD concept in practical radiotherapy Brit. J. Radiol.46 529–37
Overgaard J 1994 The effect of any method of dealing with hypoxic radioresistance in radiotherapy Oncol. Res.6 509–18
Overgaard J 2005 Radiotherapy and Oncology comes of age [Editorial] Radiother. Oncol. 75 1–5Palcic B and Skarsgard L D 1984 Reduced oxygen and enhancement ration at low doses of ionizing radiation Radiat.
Res. 100 328–39Parkins C S, Fowler J F and Shen Yu 1983 A murine model of lip epidermal/mucosal reactions to X-irradiation
Radiother. Oncol. 1 159–65Regaud C and Ferroux R 1927 Discordance des effets de rayons X, d’une part dans le testicule, par le fractionnement
de la dose Comptes Rendus Soc. Biol. 97 431Song W Y, Schaly B, Bauman G, Battista J J and Van Dyk J 2006 Evaluation of image-guided radiation therapy (IGRT)
technologies and their impact on the outcomes of hypofractionated prostate cancer treatments: a radiobiologicanalysis Int. J. Radiat. Oncol. Biol. Phys. 64 289–300

R286 Review
Steel G G 1967 Cell loss as a factor in the growth rate of human tumours Eur. J. Cancer 3 381–7Stewart F A, Denekamp J and Hirst D G 1980 Proliferation kinetics of the mouse bladder after irradiation Cell Tissue
Kinet. 13 75–89Stewart F A, Michael B D and Denekamp J 1978 Late radiation damage in the mouse bladder as measured by increased
urination frequency Radiat. Res. 75 649–59Strandqvist M 1944 Studien uber die cumulative Wirkung der Rontgenstrahlen bei Fraktionierung Acta Radiol. 55
(Suppl.) 1–300Thames H D and Hendry J H 1987 Fractionation in Radiotherapy (London: Taylor and Francis) 297 ppThomlinson R H 1968 Changes of oxygenation in tumours in relation to irradiation Front Radiat. Ther. Oncol. 3
109–21Thomlinson R H and Gray L H 1955 The histology of some human lung cancers and the possible implications for
radiotherapy Br. J. Cancer 9 539–49Travis E L and Tucker S L 1987 Isoeffect models and fractionated radiation therapy [Editorial] Int. J. Radiat. Oncol.
Biol. Phys. 13 283–7Travis E L, Vojnovic B, Davies E E and Hirst D G 1979 A plethysmograhic method for measuring function in locally
irradiated mouse lung Br. J. Radiol. 52 67–74Tsang R W, Joiner M C, Rojas A M and Johns H 1991 Repopulation in murine skin after X-ray treatments with
multiple fraction experiments per day [tested by Top-up doses] Radiat. Res. 125 163–72Van Rongen E and Kal H B 1984 Acute reactions in rat feet exposed to multiple fractions of x-rays per day Radiother.
Oncol. 2 141–50Vargas C, Yan D, Kestin L L, Krauss D, Lockman D M, Brabbins D S and Martinz A A 2005 Phase II dose escalation
study of image-guided adaptive radiotherapy for prostate cancer: use of dose-volume constraints to achieverectal isotoxicity Int. J. Radiat. Oncol. Biol. Phys. 63 141–9
Wachsman F 1943 Experimentelle Untersuchungen an eienem Fall von multiplem Hautkarzinomen unter besondererBerucksichtigung der Frage der Zweckmassigkeit dr Fraktionierung Strahlentherapie 73 649–62
Williams M V, Denekamp J and Fowler J F 1985 A review of α/β values for experimental tumours: implications forclinical studies of altered fractionation Int. J. Radiat. Oncol. Biol. Phys. 11 87–96
Withers H R 1967 Recovery and repopulation in vivo by mouse skin epithelial cells during fractionated irradiationRadiat. Res. 32 227–39
Withers H R, Taylor J M G and Maciejewski B 1988 The hazard of accelerated tumor clonogen repopulation duringradiotherapy Acta Oncol. 27 131–46
Withers H R, Thames H D and Peters L J 1982a Biological bases for high RBE values for late effects of neutronirradiation Int. J. Radiat. Oncol. Biol. Phys. 8 2071–6
Withers H R, Thames H D and Peters L J 1982b Differences in the fractionation response of acutely and late-respondingtissues Progress in Radio-Oncology vol II ed K-H Karcher et al (New York: Raven Press) pp 287–96
Wright E A and Howard-Flanders P 1957 The influence of oxygen on the radiosensitivity of mammalian tissuesActa Radiol. 48 26–32