8/20/2019 Development of Psoriatic Lesions
1/3
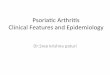
Development of psoriatic lesions. This figure depicts the
transition from normal skin to fully
developed lesion described in the text. Normal skin from a
healthy individual ( panel A) contains
epidermal Langerhans cells, scattered immature dendritic cells
(D), and skinhoming memory T cells
(T) in the dermis. Normalappearing skin from a psoriatic
individual ( panel B) manifests slight
capillary dilatation and curvature, and a slight increase in the
numbers of dermal mononuclear cells
and mast cells (!). " slight increase in epidermal thickness is
usually present. #n chronic pla$ue
psoriasis, the intensity of these changes may depend on
distance from an established lesion. The
transition %one of a developing lesion ( panel C) is
characteri%ed by progressive increases in capillary
dilatation and tortuosity, numbers of mast cells, macrophages
(!&), and T cells, and mast cell
degranulation (small arro's). #n the epidermis, there is
increasing thickness 'ith increasingly
prominent rete pegs, 'idening of the extracellular spaces,
transient dyskeratosis, spotty loss of the
granular layer, and parakeratosis. Langerhans cells (L) begin to
exit the epidermis, and inflammatory
dendritic epidermal cells (#) and D* T cells () begin to
enter the epidermis. The fully developed
lesion ( panel D) is characteri%ed by fully developed
capillary dilatation and tortuosity 'ith a tenfold
increase in blood flo', numerous macrophages underlying the
basement membrane, and increased
numbers of dermal T cells (mainly D+*) making contact 'ith
maturing dermal dendritic cells (D).
The epidermis of the mature lesion manifests markedly increased
(approximately tenfold)
keratinocyte hyperproliferation extending to the lo'er
suprabasal layers, marked but not necessarilyuniform loss of the
granular layer 'ith overlying compaction of the stratum corneum
and
parakeratosis, increased numbers of D* T cells, and
accumulation of neutrophils in the stratum
corneum (!unros microabscesses).