Embed Size (px)
Citation preview

Developing a Medical Respite Program
Using Standards as a Framework
Leslie Enzian, MD
Alice Moughamian, RN,CNS

Objectives
Provide guidance for those hoping to start a Respite program
Understand how to use the Medical Respite Standards as a
framework or starting a new Respite program.
Respite Benefits
Avoid emergency room visits
Decrease length of stay, open up beds
Offer safe discharge option
Decrease readmissions
Optimize health outcomes: respite care, f/u
Offer expertise in behavioral management
Address patterns of high utilizers by engaging in primary
care, CD Rx, mental health services, accessing funding

Respite decreases
utilization and costs
Interfaith House study, Chicago (Buchanan, Doblin, Garcia, JGIM 2003) 2 year retrospective data review of Cook County Bureau
Services for 12 mo following respite care (N=226)
Control group respite eligible but no beds
Respite clients had 60% fewer hospital days
Cost Savings of $5,439-$13,680/client

Standard 1
Accommodations

Models of Respite Programs
Free standing facility
Shelter based
Motel rooms with medical monitoring
Family Respite (motel, family shelter)
Contracted service in a board and care
facility

M
E
D
I
C
A
L
S
E
R
V
I
C
E
S TYPE OF FACILITY Non-health care
facility
Health care
facility
Refer to
shelter beds
Motel/hotel
vouchers
Contract with
board & care facility
Shelter-based
Respite unit
Free-standing
respite unit

Shelter-based Respite
ADVANTAGES DISADVANTAGES
Lower Cost
Facility Available
Use of shelter staff
Access to shelter beds
Philosophical Differences
Less environmental control
Less Bed Control
Less Policy/Safety Control
May limit acuity



Free-Standing Respite
ADVANTAGES DISADVANTAGES
Control of Environment
Control of Policy
Define Scope of Care
Increased acuity
Increased cost
Takes a long time to start
Finding a facility
License/Zoning issues
Neighborhood opposition

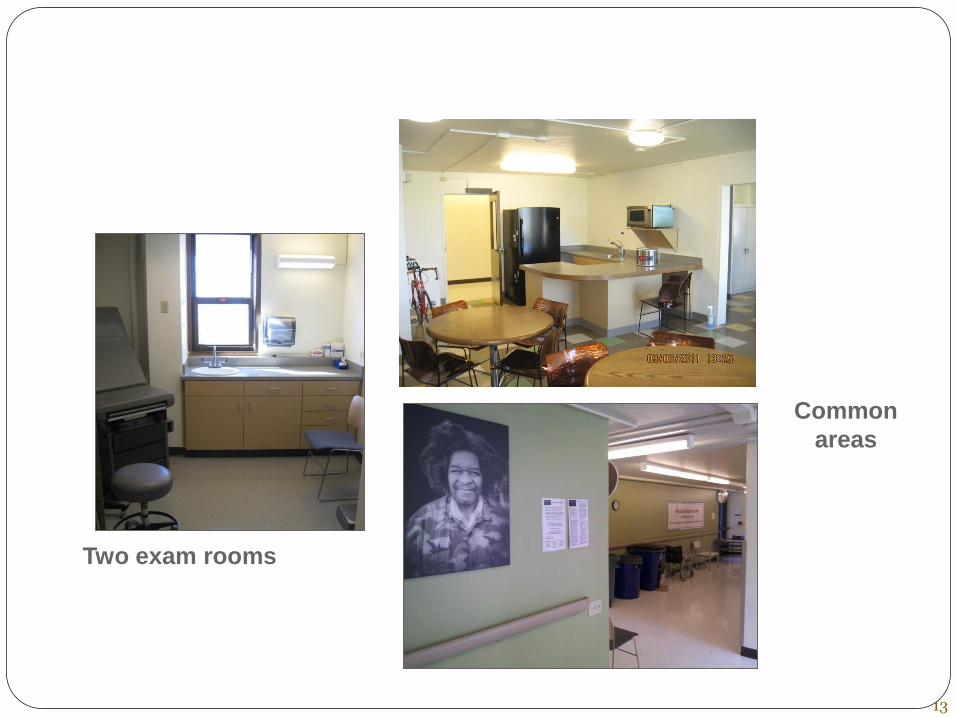
THE FACILITY
13
Two exam rooms
Common
areas
Hospitality
Access to bed
Meals
Bathrooms
Implications for shared bathrooms
Laundering capability
Transportation
Admission Agreements

Standard 2
Environmental Services

Infection Control
50 y/o M referred for large wound infected with MRSA, in
isolation in hospital. Staff donned gowns/gloves prior to
room entry. The respite program has shared rooms. Does the patient need a private room?
Can the patient leave his respite room?
Do staff need to wear protective gear?
What janitorial services are ideal?

Influenza
58 y/o man at Respite s/p I&D for leg abscess for wound
care and antibiotics
Presents with temp 101.3, cough and generalized aches and
pains
Its January, what do you do?
Influenza
Flu season a challenge for congregate living
Ability to isolate
MOU with local hospital for suspected flu cases
SF program requires 5 days of tamiflu and/or 48 hours
afebrile
Seattle requires 24 hours afebrile on Tamiflu

Other Considerations
TB
Cdiff
Hep A
Fecal – oral route
Implications in food service (ie Standard 1)
Impetigo
Standard 1 implications
Shingles
Medication Storage
Special considerations
Insulin
Controlled medications
Oral chemo agents
Special precautions
Outpatient chemo

Standard 3
Care Transition to Respite

63 yo female presents to ED with
nausea, chills, generally feeling
poorly
Cant recall her medical history
Chart indicates h/o schizophrenia and sarcoid disease
Off all meds, disengaged from all care

SH: Staying in various emergency shelters
Exam: 5X5cm irregular breast mass, scabies rash, flat affect with
delayed responses to questions
Labs: Unrevealing
What Do You Do?
Schedule patient for outpatient mammogram/breast clinic
follow-up?
Admit patient for a inpatient work-up?
Admit the patient to Medical Respite for a diagnostic
work-up and formulation of a treatment plan?

Potential Roles
Fill the service gap between hospitals and shelters
Fill the service gap between hospitals and clinics
Fill the service gap between SNF and shelters
Creativity and Flexibility to adapt services to unique patient needs
Referral Screening
Ambassador role! Friendly, diplomatic, flexible, even-keeled
Accessibility & Timely response
Requires Clinical skills:
assess pt stability, appropriateness (review labs/x-rays, discharge Rx
& discharge summary)
Ideally done by qualified medical personnel (RN, ARNP, MD)

Pneumonia Referrals
Where is the infiltrate? Clinical course? Does TB need to
be ruled out?
HIV and TB
CD4 counts < 200, CXR can be normal or infiltrate could
be in any location
Consider rule out TB prior to respite admission unless
clinical course clearly acute pneumonia

52 yo heroin dependent pt referred for
abscess wound care
Pt underwent operative drainage of abscess and has a 20 X 10 X 5 cm buttock wound
Patient was on high dose methadone and prn oxycodone in the hospital
Hospital prescribes 30 pills of oxycodone at discharge
Questions? Potential problems?

Pain Management
Ask the hospital to Rx higher dose and quantity of
narcotics at discharge?
Ask hospital to initiate a pain service consult?
Accept patient and send him to an ED or clinic for pain
meds day 2?
Does respite staff Rx narcotics
Where will narcotics be kept? Limit supply if pts hold
own scheduled meds, have agreement

Referral Screening
Efficient (same day admits)
Clear process
Provide outreach education for referring hospitals
Ability to accept late admissions
Declined referrals

Screening Challenges
Patient “not as billed”: immobility, ADL’s, cognitive deficits,
behavioral problems
Discharge meds not provided
Patient arrives late
Subspecialty care not arranged
“If you don’t accept pt, we will have to send him to streets”
Prioritizing numerous referrals

Patient “not as billed”
48 y/o chronically homeless female
PMH: well known to SFGH and UCSF medicine services
with multiple admissions over past 10 years for chronic
cellulitis/soft tissue infections, sarcoidosis, HCV, iron
deficient anemia, gastritis and current IVDU.
Now presents to SFGH with a new DVT

Respite plan
• Admitted to Respite upon hospital discharge
• Inpatient team scheduled PCP appt and Wound Care Clinic
appt
• Plan to schedule anticoagulation follow up
• Medical Respite Treatment Plan:
– Lovenox bridging to coumadin
– Finish PO antibiotics
– Wound care and engagement at outpatient wound clinic for
ongoing management

Respite course
• Admitted to Respite but then AWOL for subsequent 47
hours
• Returned to Respite sedated, nodding, with pinpoint
pupils and slurred speech.
• Three days later asks RN on duty why she has a PICC
line. RN examines pt. and indeed finds a PICC.
• No information in referral about PICC.
• At this point patient had no PICC care for 6 days and
was suspected of injecting heroin into PICC.
• Patient had also had no follow-up care for anticoagulation.

Troubleshooting
• In this case, problems included:
• Inpatient team did not communicate presence of PICC
• Inpatient team may have assumed that most outpatient providers know how to provide PICC care
• Respite team did not have opportunity to correct this assumption
• Respite team assumed that inpatient team was arranging anticoagulation follow-up, inpatient team assumed Respite would arrange anticoagulation follow up

Follow-Up
Anticoagulation follow-up made by Respite team
Patient referred to Infusion Clinic for PICC care
PCP updated on events since admission

Re-Admission Criteria
Past experience at respite provides information about
future stays
Patients with known past difficulties at respite:
incorporate this into treatment plan to assure success
with next admission
Treatment agreements, limit visitors, outside
appointments, no drop-offs or gifts from others

Standard 4
Quality Post-acute Care
Quality post-acute care
RN’s on-site, consult provider as needed
Provider on-site for referral consultation, admissions, urgent
issues, pain management, medication changes
Individualized Care plan, f/u assessments, collaborative
review of progress

Pain Management Challenges
Pain management adds to complexity of care
Difficult for PCP to titrate opiate Rx
Be prepared for potential overdoses
If lack 24 hr medical supervision, plan protocol for non-
medical staff in assessing sedation
How will patients be monitored for problems

46 yo male: EtOH dependence,
diabetes, infected foot ulcers
Slept in the woods
In an actively abusive relationship
Never consistently engaged in care
Admitted to respite, received wound care, continued to drink
heavily, non-compliant with NWB, ulcers did not heal

Referred for primary care, mental health
2 toe amputation recommended
Transported to hospital but never arrived for admission
Few weeks later showed up from the woods for a scheduled primary care appt.
Wound was larger, dirty and grossly infected, was off diabetic Rx, intoxicated
Partial foot amputation
Hospital calls to refer him back to respite
What Do You Do?
Decline admission because of non-compliance
Readmit to respite?
Respite Course
Drank daily across the street from respite
Attended most respite nursing visits for wound care, functioning in group setting, blood sugars not wildly out of control, mostly complied with NWB
Supervising nurse daily reports of drinking
Pt not discharged from respite, eventual shelter discharge after considerable wound healing
Before leaving: referred for case management, MH care, established primary care, ultimately housed

Focused Expectations
Nursing felt pt sabotaged health and that respite care was unsuccessful
Admission was great success! Patient did not get wound infection/leg amputation
Often can’t effectively fix maladaptive lifestyle issues, but can prevent serious complications from an acute process
Still has his legs, still housed, still connected to our primary care clinic, periodically drinking (less)

How to Support Successful Process?
Difficult to witness self-destructive behavior
Clarify case goals with team
Weigh impacts of various decisions
Offer venue for venting, discussion, support
Training on harm reduction

Harm Reduction in Respite
If program is clean and sober, significant numbers of
patients won’t be served
Many not be ready/able to abstain
Pts still deserving of care when using
Risks of not offering respite (care and cost)
Offer spectrum of motivational interviewing, referral
Retention/completion of treatment improved

Staffing Requirements
Core competencies for staff
Includes volunteers
Job descriptions
Medical director required
Appropriate training and certification

Staffing and Philosophy
Commitment to program mission
Creativity
Flexibility
Guidelines rather than rigid policies
Individualized responses to problems
Prioritize maximal patient retention

Standard 5
Wrap-around Services and
Care Coordination

Respite = Opportunity
Opportunity to reflect and change Nutrition and rest and recovery Prevention: Vaccines, TB/viral screen Connects individuals to health care Housing process may begin Benefits (health insurance, SSI/SSDI) Mental health assessment, Rx, referral CD counseling, referral Connection to case mgmt

54 y/o male with uncontrolled diabetes, s/p
amputation of R 5th toe for osteo and gangrene
• Comes to respite for post op recuperation and follow up.
• Exchanging security services for room/board. Now that
he is unable to work, has lost housing.
Medical Care Plan
• Medical Care Coordination:
• Wound care
• Podiatry and Diabetes follow up
• Establish PCP
• Blood sugar, diet, glucometer teaching

Social Service Plan
• Social Service Care Coordination
• Erroneously put on SSDI in 2002. Has since been unable to get
ID, job, benefits
• Ethics for discharge prior to SSDI being resolved
• Discharge Planner (MSW) worked to get birth cert,
fingerprints, hospital records, involved local, state and federal
agencies. Pelosi’s aide got meeting with SSA

61 y/o female with neck abscesses,
secondary to head lice, s/p I&D
Medical Treatment Plan:
Finish a course of PO antibiotics, wound care.
No current PCP, couch surfing, no medical or monetary
benefits

Medical Care Plan Connected with community PCP
Connected with community nursing care
Wounds resolved, medical treatment plan completing
Reported to staff she had a lump in her breast
Care plan reassessed for mass work up

Social Service plan
Established Mental Health and Case Management
Signed up for the local Health coverage plan
Signed up for County income benefits
Completed a housing application for the DPH DAH program

Standard 6
Care Transition into Community:
Discharge Planning
Discharge Process
Planning starts at admission with assigned discharge
team/planner
Pt updated on anticipate date & plan
Pt receives education on meds and medical issues prior to
discharge, written summary
Discharge summary forwarded to providers

San Francisco Discharge Summary
Template INITIAL REASON FOR ADMIT, REASON FOR DC, AND
BRIEF RESPITE COURSE:
PROBLEM STATUS AT DISCHARGE: [list each problem with updated status; if pt declined svcs, state that]
RECONCILED DISCHARGE MEDICATIONS: [please list all meds and doses, and indicate which meds were newly started at Respite, which doses were changed at Respite, and which were discontinued at Respite
PHYSICAL EXAMINATION: [must include VS and brief eval of pt]
COGNITIVE/FUNCTIONAL STATUS AT DISCHARGE:
TB STATUS:
DISCHARGE DESTINATION:

San Francisco Discharge Summary
Template [cont]
ANTICIPATED PROBLEMS AND SUGGESTED INTERVENTIONS:
PENDING LABS OR TESTS [with documentation of notification sent to receiving provider]:
PRIMARY RESPITE PROVIDERS (NP/PA, RN, MSW) DURING STAY, CONTACT INFORMATION
PRIMARY CARE PROVIDER INFO AND FOLLOW-UP APPOINTMENT:
OTHER FOLLOW-UP APPOINTMENT(S):
OTHER PROVIDER/CASE MANAGER CONTACT INFORMATION:
Standard 8
Quality Assurance
Example Program Outcomes
Reduced non-acute, uncompensated days at local
hospital
Reduced re-admissions and EMS usage
Reduced preventable hospitalizations
Implemented post-acute medical care plans
Implemented street to home plans
Implemented chronic care provider engagement plans
Implemented benefits advocacy plans

Medical Respite Care
Resources for new programs
nhchc.org Medical Respite Care website
Directory of Medical Respite Programs
Medical Respite Planning Guide
Technical Assistance
Medical Respite Research, Policy
Sabrina Edgington, NHCHC Respite Support Staff
Respite Care 101 Webinar:
http://www.nhchc.org/2011/02/medical-respite-care-filling-
void-homeless-health-care-services/






























