-
8/14/2019 Deteriro Flexores Cervicales (Mt Jull 04)
1/6
www.elsevier.com/locate/mathManual Therapy 9 (2004) 8994
Original article
Impairment in the cervical exors: a comparison of whiplash
andinsidious onset neck pain patients
G. Jull a, *, E. Kristjansson b , P. DallAlba aa Department of
Physiotherapy, The University of Queensland, Queensland 4072,
Australia
b The Faculty of Medicine, The University of Iceland,
Reykjav!
k, Iceland
Received 22 August 2002; received in revised form 20 June 2003;
accepted 30 June 2003
Abstract
There has been little investigation into whether or not
differences exist in the nature of physical impairment associated
with neckpain of whiplash and insidious origin. This study examined
the neck exor synergy during performance of the cranio-cervical
exiontest, a test targeting the action of the deep neck exors.
Seventy-ve volunteer subjects participated in this study and
were equally divided between Group 1, asymptomatic controlsubjects,
Group 2, subjects with insidious onset neck pain and Group 3,
subjects with neck pain following a whiplash injury.
Thecranio-cervical exion test was performed in ve progressive
stages of increasing cranio-cervical exion range. Subjects
performancewas guided by feedback from a pressure sensor inserted
behind the neck which monitored the slight attening of the cervical
lordosiswhich occurs with the contraction of longus colli.
Myoelectric signals (EMG) were detected from the muscles during
performance of the test.
The results indicated that both the insidious onset neck pain
and whiplash groups had higher measures of EMG signal
amplitude(normalized root mean square) in the sternocleidomastoid
during each stage of the test compared to the control subjects
(allP o 0.05) and had signicantly greater shortfalls from the
pressure targets in the test stages ( P o 0.05). No signicant
differences wereevident between the neck pain groups in either
parameter indicating that this physical impairment in the neck exor
synergy is
common to neck pain of both whiplash and insidious origin.r 2003
Elsevier Ltd. All rights reserved.
Keywords: Neck exors; Whiplash; Neck pain
1. Introduction
Neck pain is a common condition causing substantialpersonal and
nancial costs ( C
#
ot!
e et al., 1998 ; Holm-strom et al., 1992 ). Broadly, onset may
be insidious ormay follow trauma. Pain is often persistent or
recurrentin nature. Neck pain of traumatic origin following amotor
vehicle crash (whiplash) often poses a particularchallenge in
management. There are several inuencesthat may impact on the
perception of neck pain anddisability in persons with whiplash
associated disorders(WAD) compared to those with an insidious onset
of neck pain. These include the magnitude of the
injury,psychological responses to injury and pain, socialfactors
and litigation ( C
#
ot!
e et al., 2001 ; Radanov and
Sturzenegger, 1996 ). There has been little investigationinto
whether or not differences exist in the nature of physical
impairment associated with neck pain of whiplash and insidious
origins which may contributeto the greater difculty often
encountered in therehabilitation of patients with WAD.
Changes in cervical exor muscle function have beeninvestigated
in neck disorders of both whiplash andinsidious origins. Vernon et
al. (1992) in an initialcomparative study of neck isometric
strength and exor/extensor strength ratios, found that subjects
with bothWAD and insidious onset neck pain had lesser strengththan
asymptomatic subjects. There was a progressiveanterior-to-posterior
muscle imbalance in the neck painsubjects, with the cervical exors
becoming relativelyweaker as compared to the extensors. This was
moreapparent in subjects with WAD, suggesting that therecould be a
difference in the degree of impairmentbetween these subject
groups.
ARTICLE IN PRESS
*Corresponding author. Tel.: +61-7-3365-2275; fax:
+61-7-3365-2775.
E-mail address: [email protected] (G. Jull).
1356-689X/$- see front matter r 2003 Elsevier Ltd. All rights
reserved.doi:10.1016/S1356-689X(03)00086-9
-
8/14/2019 Deteriro Flexores Cervicales (Mt Jull 04)
2/6
Cervical exor muscle function has also been exam-ined using the
cranio-cervical exion test (C-CFT) ( Jull,2000). The
cranio-cervical movement aims to assess theanatomical action of
longus capitis in synergy withlongus colli, rather than that of the
supercial exors,sternocleidomastoid (SCM) and anterior scalene
mus-
cles, which ex the neck but not the head. The longuscolli muscle
has a unique role in the support of thecervical segments and curve
( Mayoux-Benhamou et al.,1994). In the C-CFT, the subject performs
ve incre-ments of increasingly inner range cranio-cervical exionin
a supine lying position ( Falla et al., 2003a ; Jull, 2000
).Patients are guided to the test level by feedback from apressure
unit (Stabilizer, Chattanooga, USA) which isplaced behind the neck
to monitor the progressiveattening of the cervical lordosis which
results from thecontraction of longus colli ( Mayoux-Benhamou et
al.,1994, 1997 ). Performance in the test has been examinedin
subjects with WAD ( Jull, 2000 ) and cervicogenicheadache ( Jull et
al., 1999 ). The results of these studiesindicated that patients
were less able to achieve and holdthe progressive positions of the
test as compared to therespective control subjects. These results
inferreddysfunction in the deep neck exors, as no directmeasure of
these muscles could be made. In the studyof subjects with WAD (
Jull, 2000 ) and in a study of patients with chronic neck pain (
Sterling et al., 2001 ),amplitudes of muscle signals
(electromyography, EMG)were measured in the sternocleidomastoid
(SCM) duringthe test, following Cholewicki et al.s (1997)
hypothesisthat increased activity of the supercial muscles could
be
a measurable compensation for poor segmental stability,or in
this case of the C-CFT, poorer activation of thelongus colli. It
was shown that both neck pain patientgroups had higher amplitudes
of muscle signals in theSCM.
There has not been a direct comparison of perfor-mance in the
C-CFT between patients with neck painfrom whiplash and insidious
origin. This study wasundertaken to make this comparison. A
clinicallyapplicable version of the C-CFT was used.
2. Methods
2.1. Subjects
Seventy-ve volunteer subjects between the ages of 1866 years
were enrolled in the study. They comprisedthree groups, each of 25
subjects. Control subjects(Group 1) and insidious onset neck pain
subjects(Group 2) were volunteers from the general anduniversity
communities who responded to advertising.The control subjects were
eligible for the study providedthey had no current or past history
of musculoskeletalpain or injury in the neck or upper limb.
Insidious onset
neck pain subjects were eligible provided that theircondition
had not been caused by trauma from a motorvehicle crash. Subjects
with WAD (Group 3) were thoseattending for assessment at a Whiplash
Research Unit.Subjects for Groups 2 and 3 were not considered if
theyhad a history of neck surgery, previous diseases affecting
the neck or throat, and rheumatic or neurologicaldisorders.
Ethical clearance for the study was obtainedfrom the Medical Ethics
Committee, The University of Queensland, and all subjects gave
informed consent toparticipate in the study.
2.2. Instrumentation and measurements
For Groups 2 and 3, data were collected regarding thelength of
history of neck pain and subjects rated theiraverage pain intensity
on a visual analogue scale (VAS),anchored with no pain and the
worst pain imaginable.
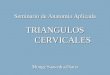
2.2.1. Cranio-cervical exion testThe subjects were positioned in
a supine lying
position. The pressure sensor was inserted between thetesting
surface and the back of the neck and waspreinated to a baseline of
20 mmHg ( Fig. 1 ). Subjectswere asked to perform progressive
repetitions of cranio-cervical exion to increase the pressure by 2
mmHgincremental targets from 22 mmHg to a maximum of 30 mmHg. Each
target pressure was held for 5 s with a10 s rest between each task.
The pressure sensor wasconnected to a pressure transducer (RS
components)and electrical signals from the pressure transducer
were
amplied and relayed to a visual feedback device and toan Amlab
data acquisition system (Associated Measure-ments Pty Ltd,
Australia). The visual feedback deviceconsisted of an electronic
voltmeter, marked in 2 mmHgincrements from 20 to 30 mmHg, and
calibrated to
ARTICLE IN PRESS
Fig. 1. The cranio-cervical exion test demonstrating the
visualfeedback with the pressure sensor and measurement with
surfaceEMG.
G. Jull et al. / Manual Therapy 9 (2004) 899490
-
8/14/2019 Deteriro Flexores Cervicales (Mt Jull 04)
3/6
display the pressure in the pressure bag, based on thepressure
transducer output. Sampling frequency forpressure measures was 1000
Hz. The mean pressure thateach subject achieved over the 5 s
holding time of theve test levels was calculated to determine
whethersubjects had reached each prescribed level of the test.
The differences between the mean pressure achieved andthe
nominated target pressure for each stage werecalculated for each
group.
Myoelectric signals were collected from the SCMmuscles using
AgAgCl electrodes (Conmed, USA) in abipolar conguration. Electrodes
were positioned alongthe lower one-third of the muscle bellies of
the SCM(Falla et al., 2002 ). Signals were amplied (Amlab),
andpassed through a 20500 Hz bandwidth lter. They weresampled at
1000 Hz. EMG data (amplitude of the signal)were analysed off-line
(Matlab). The maximum rootmean squared (RMS) value was identied for
each traceusing a 1 s sliding window, incremented in 100 ms
steps.RMS values were normalized for each subject, bydividing the 1
s maximum RMS from each level of thecranio-cervical exion test by
the 1 s maximum RMSduring a standardized head lift. The normalized
RMSdata for the left and right SCMs were averaged foranalysis.
2.3. Procedure
Subjects received written and verbal informationabout test
procedures and informed consent wasobtained. Demographic details
were obtained from all
subjects and the neck pain subjects rated their pain onthe
VAS.
Subjects were positioned in supine lying with the headand neck
in a mid position such that the face line washorizontal and an
imaginary horizontal line bisected theneck longitudinally. If
necessary, layers of towel wereplaced under the head to gain the
position. Subjectswere fully familiarized with the C-CFT by the
researcherwho was skilled in the clinical test procedure.
Theyparticipated in a practice session with the pressurebiofeedback
during which time the researcher correctedperformance.
EMG electrodes were applied over the lower one-third of the SCM
following skin preparation involvingmild abrasion with ne sandpaper
and cleaning with anisopropyl alcohol swab. The subject was rst
required toperform a head lift by tucking their chin in and
liftingthe head to just clear the bed. A 10 s recording was madefor
later normalization procedures. The pressure bagwas placed behind
the subjects cervical spine andinated until a stable pressure of
20mmHg wasachieved. The researcher instructed the subject toperform
the C-CFT to target 22 mmHg and hold theposition steady. A research
assistant operated thecomputer system. A 10 s recording was made
for each
stage to capture the 5 s holding time. Subjects thenrested for
10 s. With a similar procedure, the subjectsequentially targeted
the other four levels of the test tothe maximum of 30 mmHg.
2.4. Statistical analysis
The analysis of the SCM RMS values required a logtransformation
to remove the skewness in the originalmeasure. A saturated design
model was tted initiallyand non-signicant terms were removed. A
mixed modelANOVA was used to investigate within and betweengroup
differences in the normalized RMS values for theSCM muscles for the
factors of age, gender and stagesof the C-CFT. Boxplots of the
pressure data indica-ted possible differences in the means for the
shortfallin pressures from the designated pressure levels of
theC-CFT across groups and pressure levels. Variancesbetween
measurements within groups indicated thatmodels needed to include
terms for this heteroscedacity.The linear effects model used to
model target pressureerror included specic variance functions
modellingvariance as a power of the pressure level covariate.
3. Results
The demographic details for each subject group aswell as the
length of history and VAS scores for the neckpain groups are
presented in Table 1 . The only obviousdifference between the
groups was the length of history
of the insidious onset neck pain group compared to thewhiplash
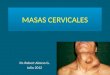
group. The results of primary analyses forSCM normalized RMS values
revealed signicantdifferences between groups P 0:001 and stages of
the test P 0:001: There were no signicant effects forgender P 0:51
or age P 0:62: The analysisrevealed a strong positive linear
relationship betweenSCM normalized RMS values and stage of the
C-CFT,but the relationship levelled off for the whiplash groupat
the highest pressure target ( Fig. 2 ). Both the neck painand
whiplash groups had signicantly higher SCMnormalized RMS values
than the control group at eachstage of the C-CFT (all P o 0:05).
However there wereno signicant differences in SCM normalized
RMS
ARTICLE IN PRESS
Table 1Characteristics of the subject groups
Controlsn 25
Neck painn 25
Whiplashn 25
Gender (females %) 60 80 68Age (years, mean 7 SD) 39.3 7 14.0
40.3 7 9.2 36.3 7 10.2Length of history (years) 8.5 7 6.0 1.8 7
1.1Average pain (VAS 010) 6.3 7 1.5 6.2 7 2.3
G. Jull et al. / Manual Therapy 9 (2004) 8994 91
-
8/14/2019 Deteriro Flexores Cervicales (Mt Jull 04)
4/6
values between the neck pain and whiplash groups withthe
exception of the 22 mmHg stage P 0:02: Theanalysis was repeated for
the insidious onset neck painand whiplash groups using length of
history of neck painas a covariate and results remained
unchanged.
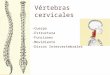
The differences between the target pressure and themean pressure
achieved for each stage of the test foreach group are presented in
Fig. 3 . Within the teststages, the mean shortfalls in pressure for
the neck painand whiplash groups were not signicantly different
atany stage of the test P > 0:05; but those of both groupswere
signicantly greater than the control groupP o 0:002: The exception
was at the 22 mmHg targetwhere the mean for the neck pain group was
notsignicantly different from the control group P 0:11:
4. Discussion
Dysfunction in the neck exor muscles has beenfound to be
associated with neck pain of both whiplash
and insidious origins ( Jull et al., 1999, 2000 ; Sterlinget
al., 2001 ; Vernon et al., 1992 ; Watson and Trott,1993). However
there has been little investigation intowhether or not differences
exist between the groupswhich might impact on the rehabilitation
process.
The results of this study revealed a strong linear
relationship between the magnitude of the SCMnormalized RMS
values and each progressive stage of the test for all groups but
there were higher levels of SCM normalized RMS values in the neck
pain andwhiplash groups in all stages of the C-CFT compared tothe
asymptomatic control group. This is in accord withthe ndings of
previous studies of subjects with WADand insidious onset neck pain
( Jull, 2000 ; Sterling et al.,2001). No signicant differences were
evident betweenthe neck pain and WAD groups indicating that
thisphysical impairment or altered pattern of muscle co-ordination
is common to neck pain of both whiplashand insidious origin and
would not seem to be a reasonwhy patients with chronic WAD often
are morechallenging to treat than patients with insidious
originneck pain.
Cranio-cervical exion is the action of longus capitisin synergy
with longus colli. The presence of progres-sively increasing SCM
normalized RMS values in eachtest stage in all subject groups
suggests that thesemuscles were recruited to further stabilize the
neck asthe contractile demand of the longus capitis increased inthe
inner ranges of cranio-cervical exion. The presenceof higher SCM
normalized RMS values in the neck paingroups infers that altered
patterns of co-ordination may
be present between the deep and supercial exormuscles in
patients with neck pain, and this higheractivity may be a
measurable compensation ( Cholewickiet al., 1997 ) for poorer
active contractile capacity of thelongus colli and capitis muscles.
The clinical version of the C-CFT used in this study has the decit
of no directmeasure of the activity of longus capitis and colli.
Themuscles are deep and not accessible for use of conventional
surface EMG. Falla et al. (2003b) used anovel surface EMG electrode
in a laboratory version of the C-CFT. A bipolar surface electrode
was inbuilt intoa nasopharageal suction catheter and the electrode
wasinserted via the nasal passage and suctioned onto theback of the
throat adjacent to the uvula, over the longuscapitis and colli. In
their study on asymptomaticsubjects, they demonstrated a stronger
linear relation-ship between the amplitude of the deep neck
exormuscle signal and the increasing incremental stages of the
test, which conrms anatomical predictions for thetest. In a further
study of 10 neck pain and 10 controlsubjects, Falla et al. (2003c)
again demonstrated astrong linear relationship between the EMG
amplitudeof the deep neck exor muscles and the incrementalstages of
the C-CFT for both control and neck painsubjects. However, the
amplitude of deep neck exor
ARTICLE IN PRESS
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
22mmHg 24mmHg 26mmHg 28mmHg 30mmHg
Test stages
N o r m a l
i s e d
R M S
Controls
Neck Pain
Whiplash
Fig. 2. The means (se) for the normalized RMS values
forsternocleidomastoid in each stage of the cranio-cervical exion
testfor control, insidious onset neck pain and whiplash groups.
0
0.5
1
1.5
2
2.5
3
3.5
22mmHg 24mmHg 26mmHG 28mmHg 30mmHgTest stages
P r e s s u r e s h o r
t f a l
l s m m
H g Controls
Neck Pain
Whiplash
Fig. 3. The means (se) for the shortfall in pressure from the
targetpressures for each stage of the cranio-cervical exion test
for control,insidious onset neck pain and whiplash groups.
G. Jull et al. / Manual Therapy 9 (2004) 899492
-
8/14/2019 Deteriro Flexores Cervicales (Mt Jull 04)
5/6
EMG was less in the neck pain group than for thecontrol group
and the difference was signicant forthe higher levels of the test.
Although not signicant,there was a strong trend for greater EMG
activity in theSCM and anterior scalene muscles in the neck
paingroup. These ndings lend support to the contention
that the higher levels of SCM normalized RMSvalues measured in
all stages of the C-CFT in our studyof neck pain patients as
compared to the controlsubjects may reect a compensation strategy
for poorercontractile capacity of the deep cervical exors.
Furtherstudy on larger sample sizes to better understand
thecompensation strategies in the C-CFT as well as theirsensitivity
and specicity to neck pain patients iswarranted.
The pressure unit, which is inserted behind the neck inthe
C-CFT, monitors the slight attening of the cervicalspine
accompanying the contraction of the longus colli(Mayoux-Benhamou et
al., 1994 ). The results of thedifferences between the pressure
target and that attainedby the subjects in this study revealed that
the controlgroup could quite accurately perform and control
thecranio-cervical exion action to the designated pressuresof each
task ( Fig. 3 ). In contrast, both neck pain groupsdemonstrated
larger pressure shortfalls at all stages of the C-CFT. This again
would infer poorer activecontractile capacity of the longus colli
to atten thecervical curve, particularly in the latter three stages
of the test. At the 30 mmHg stage of the test, the WADgroup had a
particularly large shortfall indicating thatmany of the subjects
could not perform this stage of the
test. This was associated with a levelling off of the
EMGnormalized RMS values in the WAD group at the teststage. Thus
the results of the study show that the neckpain groups of both
insidious and whiplash origin havedifculty attaining the pressure
targets of the test and inassociation they both exhibit higher
normalized RMSvalues in the SCM, indicating similar impairment in
theneck exor synergy.
The neck pain groups were of similar age and genderand reported
similar levels of pain associated with theircondition, although the
insidious onset neck pain grouphad a longer history of their
condition than the whiplashgroup. These differences in length of
history did notimpact on results. Similar ndings of the lack of
effect of length of history were reported by Nederhand et al.(2002)
in their study of muscle activation patterns of upper trapezius in
patients with WAD (mean length of history 1 :77 1:3 years) and
patients with chronic non-specic neck pain (6 :77 5:6 years). These
authorsconcluded that cervical muscle dysfunction was appar-ently
not related to a specic traumatic injury as wasalso found in this
study. Thus these changes in musclefunction appear not to be time
dependent beyond acertain point and the common factor may be
thepresence of pain.
5. Conclusion
This study has determined that altered patternsmuscle
co-ordination within the neck exor synergyare present in patients
with neck pain of whiplash andinsidious origin as evident in the
C-CFT. It appears that
this physical impairment between the two groups issimilar and of
itself would not account for the greaterdifculty often encountered
in the rehabilitation of patients following whiplash.
Acknowledgements
The authors acknowledge the nancial support forthis research
from the Centre of National Research onDisability and
Rehabilitation Medicine (CONROD,Queensland, Australia) and from the
Association of
Icelandic Insurance Companies.
References
Cholewicki J, Panjabi MM, Khachatryan A. Stabilizing function of
thetrunk exor-extensor muscles around a neutral spine.
Spine1997;22:220712.
C#
ot!
e P, Cassidy JD, Carrol L. The Saskatchewan health and back
painsurvey: the prevalence of neck pain and related disability
inSaskatchewan adults. Spine 1998;23:168998.
C#
ot!
e P, Cassidy D, Carroll L, Frank J, Bombardier C. A
systematicreview of the prognosis of acute whiplash and a new
conceptualframework to synthesize the literature. Spine
2001;26:E445.
Falla D, DallAlba P, Rianoldi A, Merletti R, Jull G. Location of
innervation zones of sternocleidomastoid and scalene musclesabasis
for clinical and research electromyography applications.Clinical
Neurophysiology 2002;113:5763.
Falla D, Campbell C, Fagan A, Thompson D, Jull G. An
investigationof the relationship between upper cervical exion range
of motionand pressure change during the cranio-cervical exion test.
ManualTherapy 2003a;8:926.
Falla D, Jull G, DallAlba P, Rianoldi A, Merletti R. An
electromyo-graphic analysis of the deep cervical exor muscles in
performanceof cranio-cervical exion. Physical Therapy 2003b;
accepted forpublication.
Falla D, Jull G, Hodges P. Neck pain patients demonstrate
reducedEMG activity of the deep cervical exor muscles
duringperformance of cranio-cervical exion. 2003c; submitted
for
publication.Holmstrom EB, Lindell J, Moritz U. Low back and
neck/shoulder
pain in construction workers: Occupational workload and
psycho-social risk factors: Part 2 relationship to neck and
shoulder pain.Spine 1992;17:6727.
Jull GA. Deep cervical neck exor dysfunction in whiplash.
Journal of Musculoskeletal Pain 2000;8:14354.
Jull G, Barrett C, Magee R, Ho P. Further characterisation of
muscledysfunction in cervical headache. Cephalalgia
1999;19:17985.
Mayoux-Benhamou MA, Revel M, Vallee C, Roudier R, Barbet
JP,Bargy F. Longus colli has a postural function on
cervicalcurvature. Surgical Radiologic Anatomy 1994;16:36771.
Mayoux-Benhamou MA, Revel M, Vallee C. Selective
electromyo-graphy of dorsal neck muscles in humans. Experimental
BrainResearch 1997;113:35360.
ARTICLE IN PRESS
G. Jull et al. / Manual Therapy 9 (2004) 8994 93
-
8/14/2019 Deteriro Flexores Cervicales (Mt Jull 04)
6/6
Nederhand MJ, Hermens HJ, Ijzerman MJ, Turk DC, Zivold
G.Cervical muscle dysfunction in chronic whiplash-associated
dis-order grade 2: the relevance of the trauma. Spine
2002;27:105661.
Radanov B, Sturzenegger M. Predicting recovery from
commonwhiplash. European Neurology 1996;36:4851.
Sterling M, Jull G, Wright A. Cervical mobilisation:
Concurrenteffects on pain, motor function and sympathetic nervous
system
activity. Manual Therapy 2001;6:7281.
Vernon HT, Aker P, Aramenko M, Battershill D, Alepin A,Penner T.
Evaluation of neck muscle strength with a modiedsphygmomanometer
dynamometer: reliability and validity.The Journal of Manipulative
and Physiological Therapeutics1992;15:3439.
Watson DH, Trott PH. Cervical headache: an investigation of
naturalhead posture and upper cervical exor muscle performance.
Cephalalgia 1993;13:27284.
ARTICLE IN PRESS
G. Jull et al. / Manual Therapy 9 (2004) 899494











![LA~ ~JI11Jl[]JUll 11] - crsi.mq.edu.au](https://img.dokumen.tips/doc/110x75/61d023e4d20e604e50378672/la-ji11jljull-11-crsimqeduau.jpg)