Embed Size (px)
Citation preview

Detection of the sentinel lymph node
in breast cancer
Santosh K. Somasundaram, Dennis W. Chicken, and MohammedR. S. Keshtgar*
Department of Surgery, Royal Free and University College Medical School, University CollegeLondon, London, UK
Introduction: Introduction: Axillary lymph node status for lymphatic staging in
breast cancer is the best prognostic indicator and guides systemic treatment.
Sentinel lymph node (SLN) biopsy is a novel, minimally invasive technique for
lymphatic staging proven to improve quality of life. The accurate detection of
the SLN is paramount for the success of the procedure.
Methods: Relevant literature was reviewed with regards to the different dyes
and techniques used for the detection of SLN in breast cancer.
Results: Highest identification rates and lowest false negative rates are achieved
by using the combined blue dye and radiocolloid technique with pre-operative
imaging using a gamma camera. There is a well-recognized learning curve to
successfully perform SLN biopsy.
Conclusions: The concept of SLN has been well validated and is the standard of
care in early breast cancer. A multidisciplinary approach and structured training
is the key to the successful introduction of the technique.
Keywords: sentinel lymph node/breast cancer/sentinel node imaging/NEWSTART
Introduction
The primary aims of modern breast cancer surgery are to obtain localand regional control of the cancer and gather sufficient information tomake an accurate prediction of the risk of distant metastases in orderto guide systemic therapy. In breast cancer, this has traditionally beenachieved by resection of the primary tumour (either by mastectomy orby wide local excision) and axillary lymph node dissection (ALND).
ALND, however, has significant short- and long-term morbidity, themost significant being lymphoedema. With the trend towards earlierdetection and presentation of breast cancer, most patients do not havelymphatic metastases at diagnosis. In these patients, ALND is purely
British Medical Bulletin 2007; 84: 117–131
DOI:10.1093/bmb/ldm032
& The Author 2007. Published by Oxford University Press.
All rights reserved. For permissions, please e-mail: [email protected]
*Correspondence to:
Mohammed R. S. Keshtgar,
Department of Surgery,
Royal Free Hospital NHS
Trust, Pond Street, London
NW3 2QG, UK. E-mail:
Dow
nloaded from https://academ
ic.oup.com/bm
b/article/84/1/117/381316 by guest on 03 Decem
ber 2021

a diagnostic procedure, with no therapeutic benefit. Herein lies anirony: with widespread use of breast conserving surgery, the stagingprocedure carries greater morbidity than the therapeutic procedure ofthe primary cancer.
Sentinel lymph node biopsy (SLNB) is a minimally invasive techniqueto stage the axilla in breast cancer, without compromising the prognos-tic information obtained from ALND.
The sentinel node concept
The sentinel node was defined by Morton et al. as any lymph node(s)receiving direct lymphatic drainage from the primary tumour, andtherefore is the first node to become involved when a tumourmetastasises.
The concept behind SLNB is that lymphatic metastases occur in anorderly manner and that the sentinel node status predicts the histologi-cal status of the regional lymph nodes. If the sentinel node does notcontain metastases, the draining nodal basin is highly unlikely toharbour metastases and complete nodal dissection is not required.
The term ‘sentinel node’ was suggested by Cabanas1 30 years ago inhis work on penile cancer. He reported an anatomical description ofthe sentinel node, although subsequent studies by others showed thisanatomical approach to have insufficient predictive value for clinicaluse. The concept was revived by Morton et al.,2 who used vital dyes tosimulate the spread of malignant melanoma. This functional approachto identification of the sentinel node proved highly accurate, and wassoon adapted to breast cancer by Giuliano et al.3
Over the last 10 years, the concept of a sentinel node has been exten-sively validated. Turner et al.4 performed a histopathological validationof the SLNB and showed that if the SLN is free of tumour, the prob-ability of the non-sentinel node involvement is ,0.1%.
Numerous clinical studies have compared SLNB with ALND inbreast cancer. These studies have been combined into large metanalyseswhich have validated the technique, demonstrating high sentinel nodeidentification rates and more importantly consistently low false nega-tive rates (Table 1).
The results of three randomized controlled trials comparing SLNBwith ALND in 2352 patients have been published to date.9–11 Allthree have demonstrated that SLNB is an accurate staging techniquewhich results in a significant reduction in morbidity with less post-operative pain, paraesthesia, shoulder stiffness and lymphoedema.Drain usage, operative time, length of hospital stay and time to
S. K. Somasundaram et al.
118 British Medical Bulletin 2007;84
Dow
nloaded from https://academ
ic.oup.com/bm
b/article/84/1/117/381316 by guest on 03 Decem
ber 2021

resumption of normal duties after surgery were significantly less in theSLNB patients.
The rate of axillary recurrence following a negative sentinel nodebiopsy is reassuringly low in two large published studies. TheMemorial Sloane Kettering Cancer Centre reported a series of 2340patients with a negative sentinel node biopsy and not subjected toALND. At a median follow-up of 31 months, three patients (0.12%)had developed an axillary recurrence.12 The axillary recurrence ratereported by Veronesi et al. for 953 similar patients followed for amedian of 38 months was 0.31% (n ¼ 3). The 5 year survival of senti-nel node negative patients was 98%.13
A further benefit of SLNB is the potential for targeted intensive his-topathological examination (ultrastaging), by examination of mul-tiple sections of the node and use of immunohistochemical (IHC)stains. This increases the sensitivity of detection of small metastaticdeposits, which could go undetected if using traditional pathologicalexamination.
Methods for identification of the sentinel node
Injection methods
The original injection techniques aimed to mimic tumour metastases;hence, the agents were injected adjacent to the tumour in a peri-tumoural fashion.
Better understanding of the lymphatic drainage of the breast allowedthe development of superficial injection techniques. Lymph drains fromthe deep breast parenchyma superficially to the rich subdermal lym-phatics. Subdermal lymphatics drain to the axilla via the subareolarplexus through one or more final common lymphatic channels. Rapidtracer migration and superior identification rates are achieved by injec-tion of the blue dye and colloid either intradermally overlying thetumour or superficially at the periareolar margin.14,15 Most units havenow adopted these superficial injection techniques, which are easy,
Table 1 Published metanalyses of clinical validation studies of sentinel lymph node biopsycompared with axillary lymph node dissection for lymphatic staging in breast carcinoma
Author Year No. of
patients
SLN identification
rate (%)
Sensitivity
(%)
False negative
rate (%)
McMasters et al.5 1998 1385 86 94 6.2
Miltenburg et al.6 1999 912 84 95 5.1
Gemignani and Borgen7 2001 3800 88 93 7.6
Kim et al.8 2006 8059 96 93 7.3
Detection of the sentinel lymph node
British Medical Bulletin 2007;84 119
Dow
nloaded from https://academ
ic.oup.com/bm
b/article/84/1/117/381316 by guest on 03 Decem
ber 2021

highly reproducible, and often show the lymphatic tracts, which maybe useful for differentiating the sentinel node from second echelonnodes. The main drawback of the superficial technique is that it rarelydemonstrates internal mammary nodes. If an internal mammary drai-nage is suspected, a deeper intra or peri-tumoural injection technique isrecommended.
Radiocolloids
The use of radiocolloids for sentinel node identification offer severaladvantages. The colloids are efficiently trapped in the sentinel node(whereas blue dyes typically pass into second echelon nodes).Radiocolloids enable pre-operative sentinel node imaging, and facilitaterapid and easy intraoperative identification by the surgeon using agamma probe (described later under ‘surgical technique’). Severalstudies have shown better sentinel node identification rates, when com-pared with blue dye alone.16
There is variation in the colloids used worldwide. The original studiesconducted within the USA used sulphur colloids, and these are still usedto date. In Europe, albumin colloids are used most widely, and are soldas a commercially available kit. Antimony trisulphide is the colloid ofchoice in Australia. The particle size of the colloid used is important:particles of 40–80 nm are small enough to migrate rapidly, yet largeenough to be efficiently trapped within the sentinel node.
The universal radioactive tracer used is Technetium-99 m.Technetium has several advantages.
(i) It is a pure gamma radiation emitter, hence offers excellent tissuepenetration.
(ii) Comparatively safe form of radiation when compared with alpha andbeta particles.
(iii) Short half-life of 6 h, hence decays rapidly. Surgery therefore needs to beperformed within 24 h of radiocolloid injection.
(iv) Cheap and readily available in every nuclear medicine department.
Although the benefits of using radiocolloids are apparent, there areseveral disadvantages, particularly complicated and restrictive legis-lation governing the administration of radiopharmaceuticals to patientsand the handling of radioactive materials. The use of radiocolloidsresults in radioactive contamination of all swabs and drapes used foran operation, and careful protocols need to be designed to appropri-ately deal with this waste material. Surgeons and theatre staff need tobe appropriately trained to manage waste. A further disadvantage is
S. K. Somasundaram et al.
120 British Medical Bulletin 2007;84
Dow
nloaded from https://academ
ic.oup.com/bm
b/article/84/1/117/381316 by guest on 03 Decem
ber 2021

the need for an additional pre-operative investigation, the timing ofwhich needs to be coordinated with operating lists.
Sentinel node imaging
Radiocolloid injection allows pre-operative sentinel node imaging usinga gamma camera. Sentinel node imaging is different from ‘lymphoscin-tigraphy’, although the terms are erroneously used interchangeably.Classical lymphoscintigraphy aims to demonstrate the entire lymphatictree, to identify abnormalities in lymphatic drainage. This is quite dis-tinct from sentinel node imaging, where the aim is to identify the firstdraining lymph node.
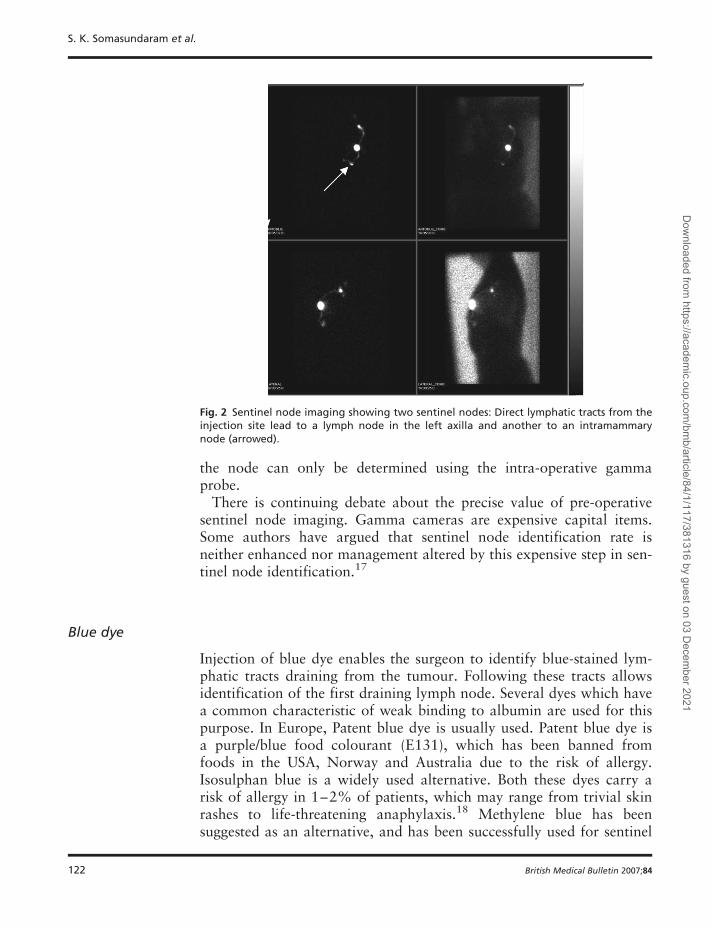
Figure 1 shows an example of sentinel node imaging. The imagingcriterion for a sentinel node is a radioactive (‘hot’) node ideally with atract draining from the injection site. Pre-operative imaging identifiesthe draining lymphatic basin and number of sentinel nodes. This ishelpful when sentinel nodes lie in unusual locations (such as intramam-mary, internal mammary or supraclavicular nodes) (Fig. 2). Frequentlymore than one sentinel node is shown on sentinel node imaging.Identifying a sentinel node on pre-operative imaging is highly predictiveof the success of the subsequent surgical procedure. It provides thesurgeon with a road map, although the precise anatomical location of
Fig. 1 Sentinel node imaging. Left anterior oblique views above and left lateral viewsbelow. Radiocolloid has been injected in the periareolar region. Two radioactive (‘hot’)nodes can be seen in the axilla. A single direct tract leads from the injection site to thelower node, which is therefore the sentinel node on imaging criteria.
Detection of the sentinel lymph node
British Medical Bulletin 2007;84 121
Dow
nloaded from https://academ
ic.oup.com/bm
b/article/84/1/117/381316 by guest on 03 Decem
ber 2021
the node can only be determined using the intra-operative gammaprobe.
There is continuing debate about the precise value of pre-operativesentinel node imaging. Gamma cameras are expensive capital items.Some authors have argued that sentinel node identification rate isneither enhanced nor management altered by this expensive step in sen-tinel node identification.17
Blue dye
Injection of blue dye enables the surgeon to identify blue-stained lym-phatic tracts draining from the tumour. Following these tracts allowsidentification of the first draining lymph node. Several dyes which havea common characteristic of weak binding to albumin are used for thispurpose. In Europe, Patent blue dye is usually used. Patent blue dye isa purple/blue food colourant (E131), which has been banned fromfoods in the USA, Norway and Australia due to the risk of allergy.Isosulphan blue is a widely used alternative. Both these dyes carry arisk of allergy in 1–2% of patients, which may range from trivial skinrashes to life-threatening anaphylaxis.18 Methylene blue has beensuggested as an alternative, and has been successfully used for sentinel
Fig. 2 Sentinel node imaging showing two sentinel nodes: Direct lymphatic tracts from theinjection site lead to a lymph node in the left axilla and another to an intramammarynode (arrowed).
S. K. Somasundaram et al.
122 British Medical Bulletin 2007;84
Dow
nloaded from https://academ
ic.oup.com/bm
b/article/84/1/117/381316 by guest on 03 Decem
ber 2021
node identification. The risk of allergy appears lower, although it doesinduce an intense tissue reaction, which may result in skin necrosis ifinjected superficially.19
Injection of blue dye causes skin staining, which typically lastsseveral months, but may rarely cause permanent tattooing. All bluedyes enter the circulation, which may make patients appear cyanoticand interfere with pulse oximetry. Patients should be warned that thedye is excreted in urine post-operatively.
Sentinel node identification using blue dye alone is a difficult tech-nique to learn and requires a wider exposure of the surgical wound totrace the afferent lymphatics to the tail of the breast. Metanalysisshows that the sentinel node identification rate is lower and the falsenegative rate higher than using radiocolloid in isolation or a combi-nation of techniques.20
Combination technique
Employing two complimentary techniques for sentinel node identifi-cation will logically improve the sentinel node identification rate andreduce false negative biopsies.21 This has been clearly shown in numer-ous studies. In a metanalysis reported by Cody et al.,20 the combinedtechnique gave the best identification rate of 91% and the lowest falsenegative rate of 5%.
Using two modalities is easier, and there is evidence that the well-recognized learning curve to perform sentinel node biopsy is shorterwhen using the combination technique; if one technique fails, the othermay succeed. The combination technique enables identification of sen-tinel nodes in unusual locations.
There is therefore consensus that the combined blue dye and radio-colloid is the preferred technique.22 Within the UK, this is the tech-nique advocated in the national training programme (NEW START)for sentinel node biopsy in breast cancer.
Surgical technique
Patent blue dye is injected in the periareolar region after anaesthetizingthe patient. The injection site is gently massaged to aid migration ofthe dye through the lymphatics. The patient is positioned with the ipsi-lateral arm abducted. The axilla is systematically scanned with agamma probe (Fig. 3). Prior to this, a background count of the radio-activity is recorded for comparison with any residual activity followingthe procedure. The site of highest radioactivity is marked and a small
Detection of the sentinel lymph node
British Medical Bulletin 2007;84 123
Dow
nloaded from https://academ
ic.oup.com/bm
b/article/84/1/117/381316 by guest on 03 Decem
ber 2021

incision made. The probe provides audio feedback, which enables thesurgeon to localize the SLN using the principle of ‘line of sight’. It pro-vides three-dimensional orientation about the precise location of theSLN in the axilla.
The surgical criteria for an SLN are a hot and blue node, a blue nodewith blue afferent lymphatic tracts or a hot node with 5–10 timesthe background radioactivity or more than 10% of the activity of thehottest node (Fig. 4). After harvesting the SLN, the probe is used toidentify any other hot nodes by checking the residual counts in theaxilla. After biopsy of the hot and blue nodes, the axilla is carefullypalpated to identify any grossly involved node(s) which may be neitherhot nor blue. A surgical drain is rarely required after an SLNB.
In many centers, sentinel lymph node biopsy is done prior to thebreast surgery to allow time for an intra-operative examination of theSLN. Intra-operative diagnosis of SLN metastasis enables the surgeonto proceed with ALND. This avoids a second operative procedure
Fig. 3 Systematic scanning of the axilla with a gamma probe enables the site of highestradioactivity to be determined.
S. K. Somasundaram et al.
124 British Medical Bulletin 2007;84
Dow
nloaded from https://academ
ic.oup.com/bm
b/article/84/1/117/381316 by guest on 03 Decem
ber 2021

and anaesthetic for these patients. Intra-operative diagnosis, however,introduces uncertainty for patients, as on induction of anaesthetic, theydo not know the extent of the operation they are to undergo. Wakingto find a surgical drain implies a more extensive surgical procedure aswell as worse prognosis node-positive disease. Despite this, given thechoice, most patients opt for intra-operative diagnosis, although thepsychological impact of this is yet to be determined.23 Operation listshave to be scheduled accordingly to allow extra time for ALND inpatients with SLN metastases detected intra-operatively.
Histo-pathological examination of the sentinel lymph node
The commonly used techniques for intra-operative detection of sentinellymph node metastases are touch imprint cytology (TIC) and frozensection histology. The main drawback is that they require expert, well-trained cyto-pathologists to report results accurately in a short time.A further novel technology that is being used is the reverse transcriptasepolymerase chain reaction (rt–PCR), a rapid nucleic acid amplificationmethod that appears to accurately reflect the metastatic status of the senti-nel nodes intra-operatively. Clinical trials of the technique are underway.
The biopsied sentinel lymph nodes are serially sectioned at aminimum of three levels depending on the size of the SLN so as
Fig. 4 A blue afferent lymphatic vessel draining into a blue-stained node which is radio-active (‘hot’) is the best operative definition of a sentinel node.
Detection of the sentinel lymph node
British Medical Bulletin 2007;84 125
Dow
nloaded from https://academ
ic.oup.com/bm
b/article/84/1/117/381316 by guest on 03 Decem
ber 2021
not to miss any metastases less than 2 mm. They undergo routineHaematoxylin and Eosin (H&E) staining and nodes with no evidenceof metastases on H&E staining undergo further IHC staining for cyto-keratin antibodies. The SLNs are thus ultrastaged as H&E positive,IHC positive or negative.
Pre-operative imaging of axilla
One of the exclusion criteria for SLNB is clinical, histological or radio-logical evidence of regional nodal metastases. There are clear advan-tages in identifying patients with nodal metastases preoperatively, asnode positive patients do not benefit from SLNB and can thereforeproceed directly to ALND.
Clinical examination of the axilla, even by experienced surgeons, isnotoriously inaccurate. The axilla can be more accurately assessed byan ultrasound scan, which is simple, inexpensive and readily available.The ultrasound criteria for a suspicious node include size .5 mm andmorphological characteristics (round, hypoechoic, eccentric corticalhypertrophy with loss of central hilum). Ultrasound in isolation has alow specificity which can be enhanced by proceeding to guided fineneedle aspiration cytology or trucut biopsy.24
Currently, no imaging technique is capable of identifying microscopictumor spread and hence SLNB remains the diagnostic procedure ofchoice for axillary staging.
Limitations/problems with current standard techniques
A well-recognized pitfall of sentinel node identification using the com-bination technique is a grossly metastatic sentinel node causing ablockage to the flow of lymphatic fluid through the afferent lym-phatics. This leads to opening of alternative lymphatic channels andconsequently both blue dye and radiocolloid may be diverted awayfrom the true sentinel node. To overcome this, careful palpation of theaxilla through the operative wound is recommended, to identify grosslymetastatic nodes.
The handling, disposal and administration of radioactive materials topatients are governed by a series of complex regulations. These regu-lations can appear daunting to the uninitiated, although it should berecognized that every nuclear medicine department functions withinthese laws every day! Some have argued for identification of the senti-nel node by using blue dye only, to avoid the challenges introduced bythe use of radiocolloid. The authors view is that denying patients the
S. K. Somasundaram et al.
126 British Medical Bulletin 2007;84
Dow
nloaded from https://academ
ic.oup.com/bm
b/article/84/1/117/381316 by guest on 03 Decem
ber 2021

benefit of using the combined technique to avoid legislative restrictionsis not acceptable practice.
Research continues into alternative tracers to identify the sentinelnode. Fluorescent dyes (such as Indocyanine Green) and more recentlyfluorescent quantum dots may enable combination technique sentinelnode biopsy, without radiocolloid nor the need for an expensivegamma camera.25,26 An alternative investigational approach is theuse of magnetic particles, which may be detected by an instrumentsensitive to magnetism.27
Training in sentinel node biopsy
There is a well-documented learning curve to sentinel node biopsy.28
Successful identification of the SLN is directly related to the surgeon’sexperience. The key to success is a multi-disciplinary approach withthe surgeon, nuclear medicine physician, histopathologist, nursing andtheatre staff acquiring the knowledge and skills to enable successfulintroduction of the technique.
The aim of structured training is to avoid a false negative sentinelnode biopsy. A false negative sentinel node biopsy would result inunderstaging, with a consequent false sense of security and the possi-bility of systemic undertreatment for those patients likely to benefitmost. In the UK, a structured training programme called ‘NEWSTART’ has been developed to teach a standardized technique. Thisprogramme consists of theoretical teaching, on-site proctored trainingof the surgeon for five cases, followed by performing an audit series ofsentinel node biopsy and immediate ALND in a further 25 patients.The aim of the audit series is to verify that the surgeon with the assist-ance of the multidisciplinary team is able to identify the sentinel nodewith a high identification rate and more importantly a low false nega-tive rate. A localization rate of .90% and false negative rate of,10% is required for certification.
A simulator has been developed, which is able to simulate all keynew skills required to successfully perform the procedure.29 This simu-lator enables surgical skills laboratory training which acts as an inter-face between theoretical training and performing the procedure on livepatients.
Controversies
In the wake of SLNB, new controversies have arisen. Ultrastaging ofthe axilla by enhanced pathological examination of the SLN enables
Detection of the sentinel lymph node
British Medical Bulletin 2007;84 127
Dow
nloaded from https://academ
ic.oup.com/bm
b/article/84/1/117/381316 by guest on 03 Decem
ber 2021
the identification of micrometastases (,2 mm), submicrometastases(,0.2 mm) and isolated tumour cells (detectable by IHC stainingonly). The significance of these tiny metastases for predicting prognosis(hence influencing systemic therapy) or predicting further axillarymetastases (hence influencing the decision to proceed to ALND) is,however, unclear. The American College of Surgeons Oncology Group(ACOSOG) is examining this issue in a large trial (Z10) which is yet tobe reported.
Biopsy of internal mammary chain sentinel nodes remains an area forresearch. A small percentage of patients are upstaged by internalmammary node biopsy, but changes in systemic therapy are made in aneven smaller proportion. There is the potential for additional morbiditysuch as haemothorax or pneumothorax as a result of internalmammary chain biopsy. The value of radiotherapy to the internalmammary nodes is the subject of ongoing trials in Europe andCanada.30
The role of SLNB in ductal carcinoma in situ (DCIS) is controversial.Pure DCIS has by definition no capacity for metastasis. MicroinvasiveDCIS has a very low rate of nodal positivity. Ten per cent of patientspre-operatively diagnosed with DCIS are found to have a co-existinginvasive carcinoma, and these patients benefit from nodal staging.SLNB is warranted for extensive DCIS requiring treatment by mastect-omy and microinvasive DCIS.31
Opinions differ about SLNB in patients undergoing neoadjuvant che-motherapy. These patients typically have large tumours, and hence aremore likely to be node positive. Although it appears that sentinel nodebiopsy can still be accurately performed after neoadjuvant chemother-apy, nodal metastases may respond well to chemotherapy and thereforeregress completely. Regression of nodal metastases is a positive prog-nostic sign. Sentinel node biopsy as a separate procedure prior toneoadjuvant therapy enables accurate lymphatic staging, although ofcourse does not alter decisions about chemotherapy!
The optimal management of patients with a positive sentinel node isyet to be established. Most surgeons currently proceed to completionALND. Unless intra-operative diagnosis of sentinel nodes is utilized,this may require a second surgical procedure. Axillary irradiation mayoffer equivalent regional control with lower morbidity and without theneed for a second operation. This question is being addressed bythe AMAROS trial, conducted by the European Organisation for theResearch and Treatment of Cancer (EORTC).
An alternative approach is close observation of the sentinel nodepositive axilla, reserving axillary dissection for those patients whodevelop overt axillary metastases. The rationale for this is that ALNDconfers no clear survival benefit, and finding additional metastatic
S. K. Somasundaram et al.
128 British Medical Bulletin 2007;84
Dow
nloaded from https://academ
ic.oup.com/bm
b/article/84/1/117/381316 by guest on 03 Decem
ber 2021

nodes beyond the sentinel node is unlikely to change decisions aboutsystemic therapy. This question was addressed by the American Collegeof Surgeons Oncology Group (ACOSOG) multicentre trial Z11.Results are awaited, but target patient recruitment was not achievedand the study may therefore be underpowered to provide an answer.
A further approach to patients with a positive sentinel node is toattempt to predict those patients with non-sentinel node axillary metas-tases, and to reserve ALND for those patients at high risk. A predictivenomogram has been developed by Van Zee et al.32 and calculationscan be performed using a web-based tool. External validation of thispredictive tool has shown conflicting results, suggesting that it mayrequire further refinement.33
Until the results of the trials underway are known, most surgeonsproceed to axillary dissection when the sentinel node showsmetastases.
Key points for clinical practice
† Surgical lymphatic staging remains integral to modern cancermanagement.
† Sentinel node biopsy is the standard of care for lymphatic staging of breastcancer.
† The sentinel node concept in breast cancer has been extensively validated.
† Current techniques for sentinel node identification have been optimized.
† Sentinel node biopsy enables accurate, minimally invasive lymphaticstaging while avoiding the morbidity of routine lymph node dissection fornode negative breast cancer patients. The improved quality of life afterbreast cancer surgery has been confirmed in several large randomized con-trolled trials.
† Intensive pathological examination of the sentinel node enables the detec-tion of low volume metastases (ultrastaging). The clinical significance ofisolated tumour cells and micrometastases less than 0.2 mm is yet to bedetermined in beast cancer.
† The current standard of care for sentinel node positive breast cancerpatients is ALND, although this may change with the result of major trialswhich are underway.
† The major disadvantage of sentinel node biopsy is understaging as a resultof a false negative sentinel node biopsy. Adequate multidisciplinary train-ing is the key to avoid this.
† Sentinel node biopsy research continues, and may yield new tracers andresult in changes in the management of patients with a metastatic sentinelnode.
Detection of the sentinel lymph node
British Medical Bulletin 2007;84 129
Dow
nloaded from https://academ
ic.oup.com/bm
b/article/84/1/117/381316 by guest on 03 Decem
ber 2021

References
1 Cabanas RM (1977) An approach for the treatment of penile carcinoma. Cancer, 39,
456–466.2 Morton DL, Wen DR, Wong JH et al. (1992) Technical details of intraoperative lymphatic
mapping for early stage melanoma. Arch Surg, 127, 392–399.3 Giuliano AE, Kirgan DM, Guenther JM, Morton DL (1994) Lymphatic mapping and sentinel
lymphadenectomy for breast cancer. Ann Surg, 220, 391–398.
4 Turner RR, Ollila DW, Krasne DL, Giuliano AE (1997) Histopathologic validation of thesentinel lymph node hypothesis for breast carcinoma. Ann Surg, 226, 271–276.
5 McMasters KM, Giuliano AE, Ross MI et al. (1998) Sentinel-lymph-node biopsy for breastcancer—not yet the standard of care. N Engl J Med, 339, 990–995.
6 Miltenburg DM, Miller C, Karamlou TB, Brunicardi FC (1999) Meta-analysis of sentinel
lymph node biopsy in breast cancer. J Surg Res, 84, 138–142.7 Gemignani ML, Borgen PI (2001) Is there a role for selective axillary dissection in breast
cancer? World J Surg, 25, 809–818.
8 Kim T, Giuliano AE, Lyman GH (2006) Lymphatic mapping and sentinel lymph node biopsyin early-stage breast carcinoma: a metaanalysis. Cancer, 106, 4–16.
9 Veronesi U, Paganelli G, Viale G et al. (2003) A randomized comparison of sentinel-nodebiopsy with routine axillary dissection in breast cancer. N Engl J Med, 349, 546–553.
10 Mansel RE, Fallowfield L, Kissin M et al. (2006) Randomized multicenter trial of sentinel
node biopsy versus standard axillary treatment in operable breast cancer: the ALMANACTrial. J Natl Cancer Inst, 98, 599–609.
11 Purushotham AD, Upponi S, Klevesath MB et al. (2005) Morbidity after sentinel lymph nodebiopsy in primary breast cancer: results from a randomized controlled trial. J Clin Oncol, 23,4312–4321.
12 Naik AM, Fey J, Gemignani M et al. (2004) The risk of axillary relapse after sentinel lymphnode biopsy for breast cancer is comparable with that of axillary lymph node dissection: a
follow-up study of 4008 procedures. Ann Surg, 240, 462–468.13 Veronesi U, Galimberti V, Mariani L et al. (2005) Sentinel node biopsy in breast cancer:
early results in 953 patients with negative sentinel node biopsy and no axillary dissection.
Eur J Cancer, 41, 231–237.14 McMasters KM, Wong SL, Martin RC et al. (2001) Dermal injection of radioactive colloid is
superior to peritumoral injection for breast cancer sentinel lymph node biopsy: results of a
multiinstitutional study. Ann Surg, 233, 676–687.15 Chagpar A, Martin RC III, Chao C et al. (2004) Validation of subareolar and periareolar
injection techniques for breast sentinel lymph node biopsy. Arch Surg, 139, 614–618.16 Mansel RE, Goyal A, Fallowfield L, Newcombe RG (2004) Sentinel node biopsy versus stan-
dard axillary treatment: results of the randomized multicenter UKALMANAC trial. BreastCancer Res Treat, 88, pS13.
17 Shoher A, Diwan A, Teh BS, Lu HH, Fisher R, Lucci A Jr. (2006) Lymphoscintigraphy does
not enhance sentinel node identification or alter management of patients with early breastcancer. Curr Surg, 63, 207–212.
18 Montgomery LL, Thorne AC, Van Zee KJ et al. (2002) Isosulfan blue dye reactions during
sentinel lymph node mapping for breast cancer. Anesth Analg, 95, 385–388, table.19 Salhab M, Al Sarakbi W, Mokbel K (2005) Skin and fat necrosis of the breast following
methylene blue dye injection for sentinel node biopsy in a patient with breast cancer. IntSemin Surg Oncol, 2, 26.
20 Cody HS III. (2001) Clinical aspects of sentinel node biopsy. Breast Cancer Res, 3, 104–108.
21 Goyal A, Newcombe RG, Chhabra A, Mansel RE (2006) Factors affecting failed localisationand false-negative rates of sentinel node biopsy in breast cancer—results of the ALMANAC
validation phase. Breast Cancer Res Treat, 99, 203–208.22 Schwartz GF, Giuliano AE, Veronesi U. (2002) Proceedings of the consensus conference on
the role of sentinel lymph node biopsy in carcinoma of the breast April 19 to 22, 2001,
Philadelphia, Pennsylvania. Hum Pathol, 33, 579–589.
S. K. Somasundaram et al.
130 British Medical Bulletin 2007;84
Dow
nloaded from https://academ
ic.oup.com/bm
b/article/84/1/117/381316 by guest on 03 Decem
ber 2021
23 Chicken DW, Sivanadarajah N, Keshtgar MRS (2006) Patients’ view on intraoperative diag-
nosis of sentinel nodes in breast cancer: is it an automatic choice? Int J Surg, 5, 76–80.24 Alvarez S, Anorbe E, Alcorta P, Lopez F, Alonso I, Cortes J (2006) Role of sonography in the
diagnosis of axillary lymph node metastases in breast cancer: a systematic review. AJR Am JRoentgenol, 186, 1342–1348.
25 Kitai T, Inomoto T, Miwa M, Shikayama T (2005) Fluorescence navigation with indocyanine
green for detecting sentinel lymph nodes in breast cancer. Breast Cancer, 12, 211–215.26 Tanaka E, Choi HS, Fujii H, Bawendi MG, Frangioni JV (2006) Image-guided oncologic
surgery using invisible light: completed pre-clinical development for sentinel lymph nodemapping. Ann Surg Oncol, 13, 1671–1681.
27 Minamiya Y, Ogawa J. (2003) A novel method for sentinel lymph node mapping using mag-
netite. Nippon Geka Gakkai Zasshi, 104, 759–761.28 Clarke D, Newcombe RG, Mansel RE (2004) The learning curve in sentinel node biopsy: the
ALMANAC experience. Ann Surg Oncol, 11, 211S–215S.29 Keshtgar MRS, Chicken DW, Waddington WA, Raven W, Ell PJ (2005) A training simulator
for sentinel node biopsy in breast cancer: a new standard. Eur J Surg Oncol, 31, 134–140.
30 Estourgie SH, Tanis PJ, Nieweg OE, Valdes Olmos RA, Rutgers EJ, Kroon BB (2003) Shouldthe hunt for internal mammary chain sentinel nodes begin? An evaluation of 150 breastcancer patients. Ann Surg Oncol, 10, 935–941.
31 Lyman GH, Giuliano AE, Somerfield MR et al. (2005) American Society of ClinicalOncology guideline recommendations for sentinel lymph node biopsy in early-stage breast
cancer. J Clin Oncol, 23, 7703–7720.32 Van Zee KJ, Manasseh DM, Bevilacqua JL et al. (2003) A nomogram for predicting the like-
lihood of additional nodal metastases in breast cancer patients with a positive sentinel node
biopsy. Ann Surg Oncol, 10, 1140–1151.33 Degnim AC, Reynolds C, Pantvaidya G et al. (2005) Nonsentinel node metastasis in breast
cancer patients: assessment of an existing and a new predictive nomogram. Am J Surg, 190,543–550.
Detection of the sentinel lymph node
British Medical Bulletin 2007;84 131
Dow
nloaded from https://academ
ic.oup.com/bm
b/article/84/1/117/381316 by guest on 03 Decem
ber 2021