Embed Size (px)
Citation preview

DERİN KÖSEBAY OTURUMU

The reflection of the New Molecular and Morphological Classification of Endometrial Cancer to the Clinical
Practice Ayse AYHAN, MD. PhD
Retired Professor, Hacettepe University, Faculty of Medicine, TurkeyAdjunct Professor, Johns Hopkins University Department of Gynecologic Pathology, Baltimore, MD, USA
Adjunct Professor, Hiroshima and Hamamatsu University Faculty of Medicine, Japan
Consultant Pathologist, Seirei Mikatahara Hospital, Hamamatsu, Japan www.ayseayhan.com

Endometrial Ca:
Molecular vs Pathological Diagnostics
• Endometrial cancer Classification :
• Histopathological Classification
• Molecular Classification
• The impact of molecular classification on
routine practice:
• The role of the Pathologist-Molecular Tx

Endometrial Ca:
Molecular vs Pathological Diagnostics
• Endometrial cancer Classification :
• Histopathological Classification
• Molecular Classification
• The impact of molecular classification on
routine practice:
• The role of the Pathologist-Molecular Tx
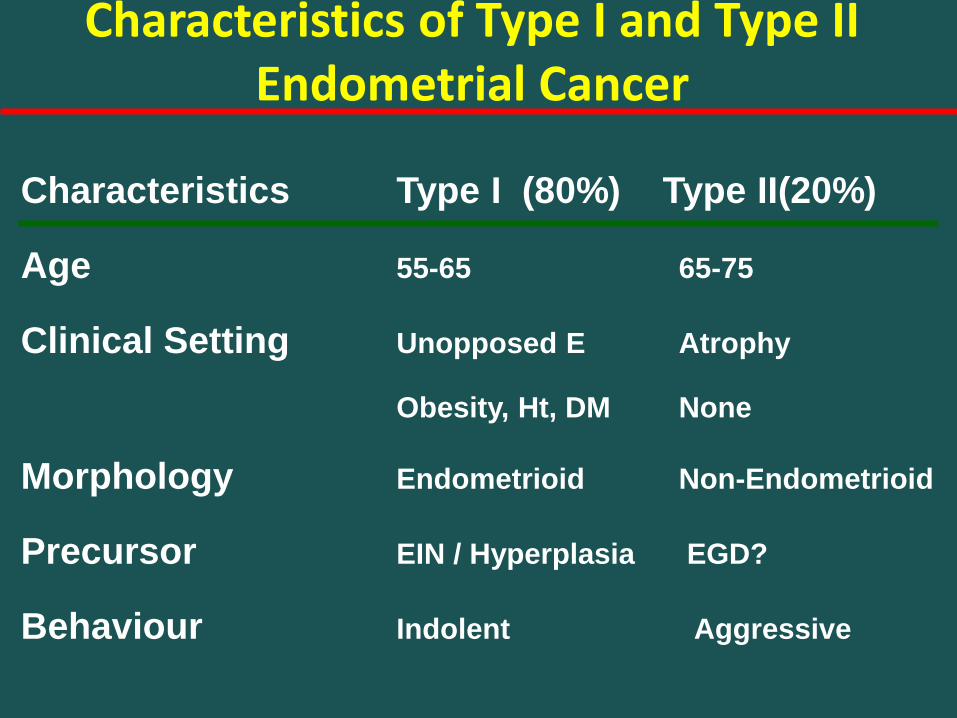
Characteristics Type I (80%) Type II(20%)
Age 55-65 65-75
Clinical Setting Unopposed E Atrophy
Obesity, Ht, DM None
Morphology Endometrioid Non-Endometrioid
Precursor EIN / Hyperplasia EGD?
Behaviour Indolent Aggressive
Characteristics of Type I and Type II Endometrial Cancer

Genetic Alteration Type I Ca (%) Type II Ca(%)
PTEN inactivation 50-80 10
KRAS mutation 15-30 0-5
-catenin mutation 25-40 0-3
Microsatellite Instability 20-40 0-5
ARID1A alterations 40-60 0
P53 mutation 10-20 80-90
HER2/neu 10-30 40-80
P16INK4A inactivation 10 40
E-cadherin 10-20 60-90
PPP2R1A 5-7 20-40
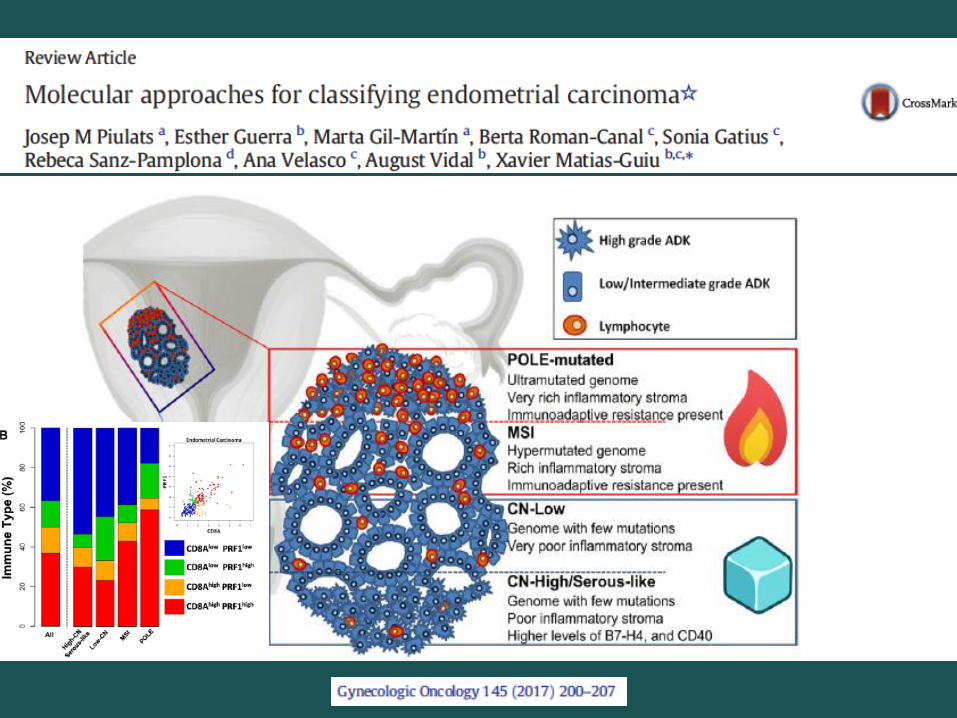
Endometrial Cancer Molecular Subsets
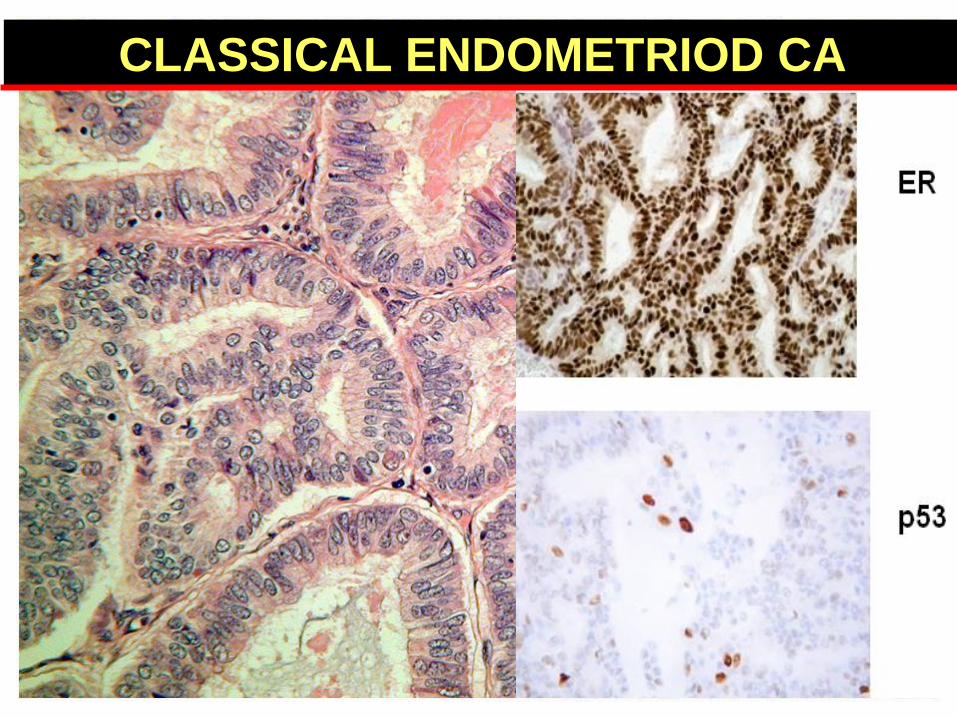
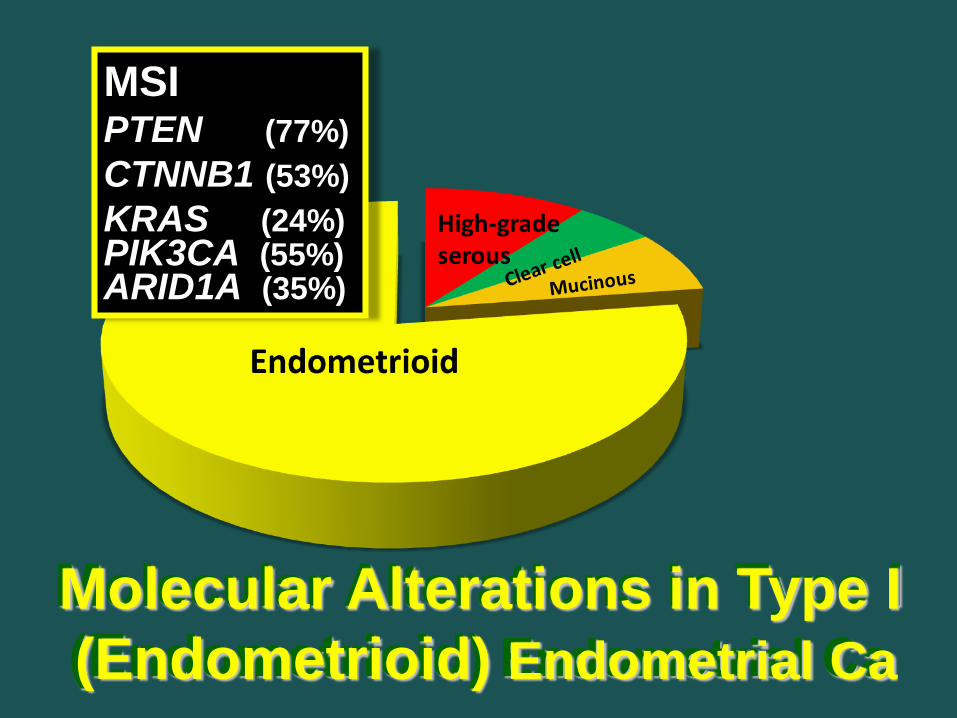
CLASSICAL ENDOMETRIOD CA

MSIPTEN (77%)
CTNNB1 (53%)
KRAS (24%)PIK3CA (55%)ARID1A (35%)
Molecular Alterations in Type I
(Endometrioid) Endometrial Ca

• Immunoreactivity was not detected in 36 (3.6%) of 995 tumors
• Uterine low-grade endometrioidcarcinomas had a high frequency of loss of ARID1A expression: 15/58 (26%) were negative
• There was no ARID 1A loss on serous type uterinecarcinomas.
ARID1A Expression Loss in Endometrioid Carcinomas
Tumor total no. IHC(-) %of IHC(-)
Immunohistochemical study of ARID1A on 995 carcinomas
Hepatocellular carcinoma Bile duct carcinomaLung
adenocarcinomasquamous carcinoma
Renal cell carcinomaBreast carcinomaOvary
high-grade serous carcinomalow-grade serous carcinomamucinous carcinoma
Uterine cervixsquamous carcinomaadenocarcinoma
Uterine corpusendometrioid carcinomaserous carcinoma/MMMT
Trophoblastic tumorchoriocarcinomaplacental site trophoblastic tumorepithelioid trophoblastic tumor
Prostate carcinomaColon carcinomaGastric carcinomaPancreatic carcinomaOral squamous carcinomaIHC: Immunoreactivity of ARID1A
4127
42107391
2211536
11411
5817
356
1735494548
4
02
1101
00 0
21
150
00002540
07.4
2.410
01.1
000
1.89.1
260
0000
4.111
8.30
AJSP 35:625, 2011
Endometrioid Ca Serous CaEndometrium

AH / EIN with loss of PTEN and/or ARID1A
Co-loss of ARID1A & PTEN was highly significant and nonrandom (p=0.0003)
All AH / EIN areas with ARID1A loss were geographically nested within the areas
of PTEN loss. A significant increase in Ki67 in areas with concurrent PTEN and
ARID1A co-loss compared to adjacent AH / EIN areas showing only PTEN loss.
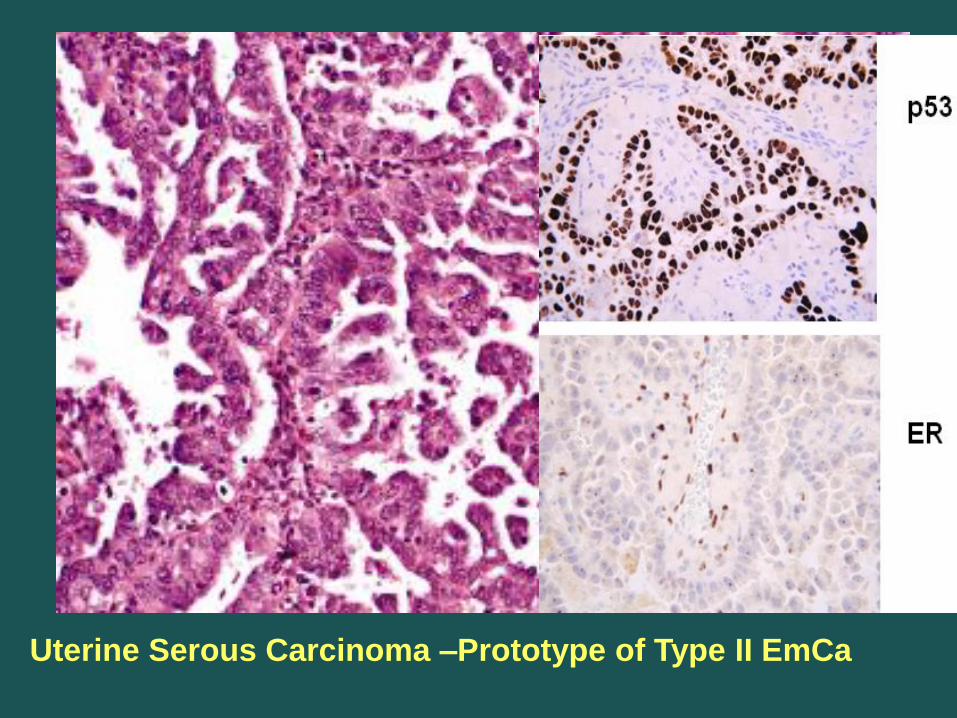
Uterine Serous Carcinoma –Prototype of Type II EmCa
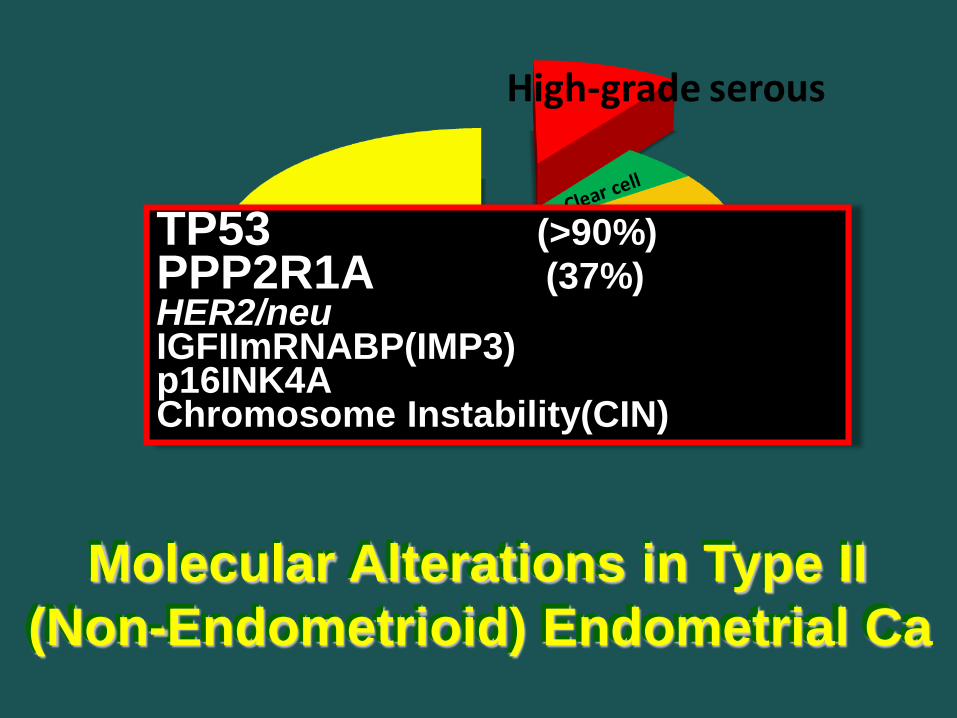
TP53 (>90%)
PPP2R1A (37%)HER2/neuIGFIImRNABP(IMP3)p16INK4AChromosome Instability(CIN)
Molecular Alterations in Type II
(Non-Endometrioid) Endometrial Ca

Endometrioid Adenoca• Variants (sq. diff; villoglandular, Secretory)
Mucinous Adenoca
Serous Intraepithelial Carcinoma
Serous Adenoca
Clear Cell Adenoca
Neuroendocrine tumors (Low/High)
Mixed Cell Adenocarcinoma
Undifferentiated Carcinoma
Dedifferentiated Carcinoma
Endometrial Adenocarcinoma (WHO, 2014)
Serous Intraepithelial Carcinoma
Squamous Cell Ca & TCC
Neuroendocrine tumors (Low/High)
Undifferentiated Ca
Dedifferentiated Ca

Endometrial Ca:
Molecular vs Pathological Diagnostics
• Endometrial cancer Classification :
• Histopathological Classification
• Molecular Classification
• The impact of molecular classification on
routine practice:
• The role of the Pathologist-Molecular Tx

n=373, array, seq based
Endometrial Carcinoma (TCGA)

7% 28% 39% 26%
Endometrial Carcinoma (TCGA)

1
2
3 3
Endometrial Carcinoma (TCGA)
MSIPTEN (77%)
CTNNB1 (53%)
KRAS (24%)PIK3CA (55%)ARID1A (35%)
Molecular Alterations in Type I
(Endometrioid) Endometrial Ca

Recurrently mutated genes are different between the four groups
POLE-MutatedEEC, G1-3, <10%
PTEN (94%)
KRAS (53%)PIK3CA (71%)ARID1A (76%)
MSI-High mutEEC, G1-3, 30%
MSI
PTEN (88%)
KRAS (35%)PIK3CA (54%)ARID1A (37%)
Endometrial Carcinoma (TCGA)
Copy LOWEEC, G1-2, 30%
PTEN (77%)
CTNNB1 (52%)PIK3CA (53%)ARID1A (42%)
Copy HIGH-SLSerous(94%,Mx 30%)
P53 (92%)
PPPR1A (22%)PIK3CA (47%)CIN, amplifications

Endometrial Carcinoma (TCGA)

• Clinical Heterogeneity: Due to molecular ?
• TCGA clasification :
• Subtypes can be reliably delineated
• Prognostic / predictive information:
• Embracing and incorporating them into clinical
practice is thus attractive.
• Integration of molecular features into current
classification systems is not without obstacles.
Endometrial Carcinoma Molecular Diagnostics

• Improve risk stratification systems by combining traditional
clinico-pathological parameters
• How molecular classification can be optimally utilized to direct patient care.
Pathologists and clinicians caring for women with
endometrial cancer need to engage with and understand
the possibilities and limitations of this new approach,
because integration of molecular classification of
endometrial cancers is anticipated to become an
essential part of pathology practice.
Endometrial Carcinoma Molecular Diagnostics
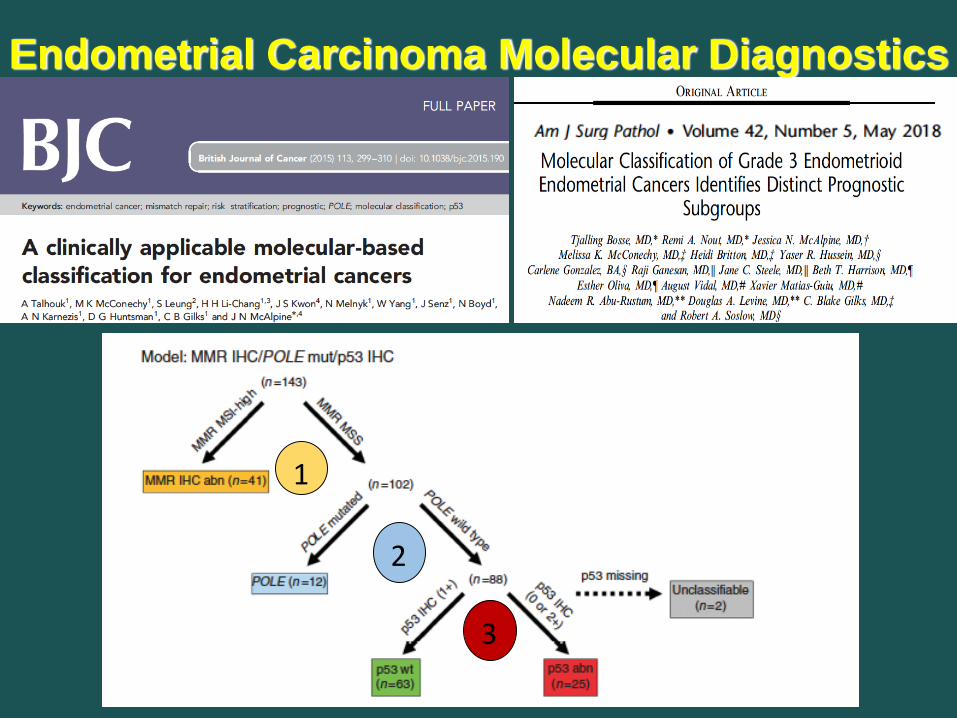
Endometrial Carcinoma Molecular Diagnostics
1
2
3

PROactive Molecular rISc classifyer EmCa
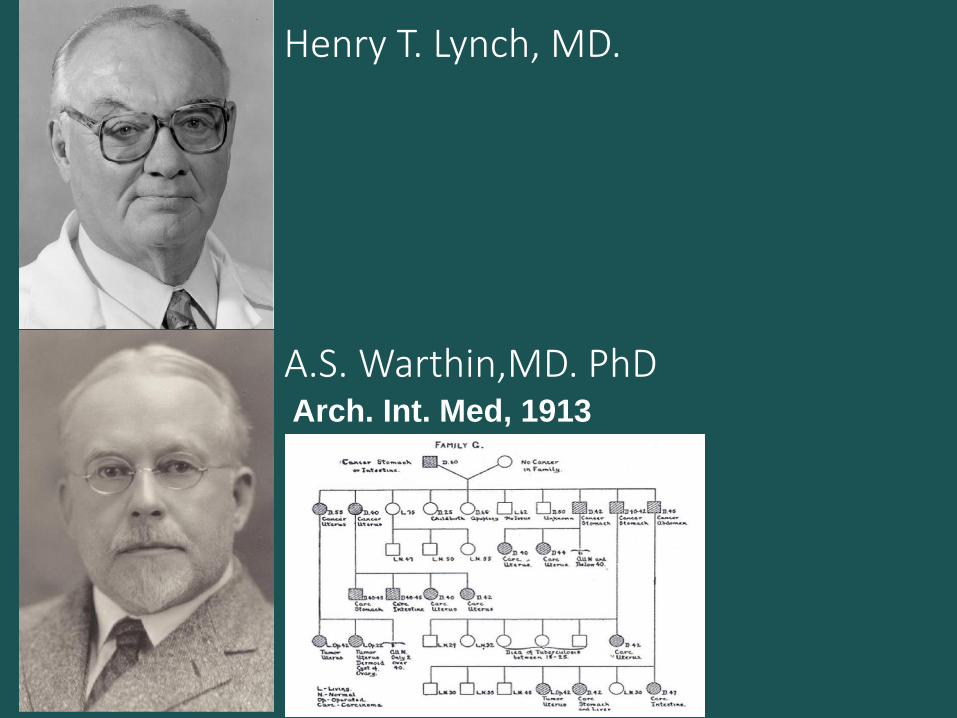
Henry T. Lynch, MD.
A.S. Warthin,MD. PhDArch. Int. Med, 1913

10children. 6 cancer, He died of cancer at 60.
Third generation, 33/70 cancer : Uterine – Gastric - Colon

1985 : H. Lynch : Hereditary Nonpolyposis Colorectal Ca2005 Douglas (Mishigan-AnnArbor). MSH2 is the genetic defect
Subsequent Cancers

•Garg K, Soslow RA. J Clin Pathol 2009; 62: 679. Kwon JS, J Clin Oncol, 2011, Surgery, 2010
Co
rrelatio
ns: M
MR
deficien
t, LG: IT-P
T TIL’s

⚫ Microsatellites are polymorphic repetitive short non-coding DNA sequences – widely dispersed throughout the genome
⚫ Repetitive nature cause “REPLICATION ERRORS” (RER)
⚫ DNA repair mechanisms
⚫ Effectively represent the defects in MMR
genes rather than mutation spesific
⚫ Microsatellite Instability occurs in >20% of sporadic endometrioidendometrial carcinomas.
⚫ Most frequent causes⚫ MLH1 inactivation by epigenetic silencing
⚫ MSH2, MSH6, PMS2 mutation and expression loss
⚫ MI occurs as an early event in endometrioid endometrial cancer.
“MSI” in Endometrioid Endometrial Cancer

Endometrial Ca:
Molecular vs Pathological Diagnostics
• Endometrial cancer Classification :
• Histopathological Classification
• Molecular Classification
• The impact of molecular classification on
routine practice:
• The role of the Pathologist-Molecular Tx

After TCGA: Pathology Correlations
• TCGA + Age + LVSI + DOI incorportaion
• POLE mutant: HGEEC:
• Superficial broad inv, TILs, (ambiguous)
• MSI : MLH1, PMS2, MSH2 and MSH6 partly Lynch synd
• Challenges to overcome :
• Multiple classifyers
• additional (Er, PgR, LCAM, b-catenin..)

Integrated TCGA Molecular & Clinicopathologic

TCGA : Molecular Classes of Endometrial Ca

TCGA : Molecular Classes of Endometrial Ca

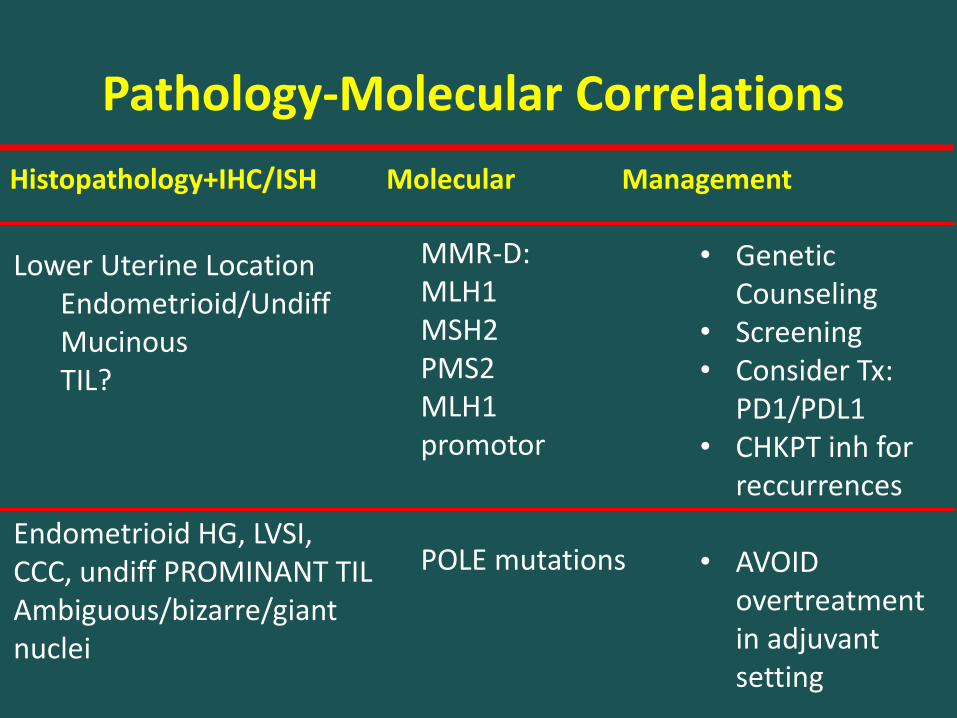
Pathology-Molecular Correlations
Histopathology+IHC/ISH Molecular Management
Lower Uterine LocationEndometrioid/UndiffMucinousTIL?
Endometrioid HG, LVSI,CCC, undiff PROMINANT TILAmbiguous/bizarre/giantnuclei
MMR-D:MLH1MSH2PMS2MLH1 promotor
POLE mutations
• Genetic Counseling
• Screening• Consider Tx:
PD1/PDL1• CHKPT inh for
reccurrences
• AVOID overtreatment in adjuvant setting

Immune-Editing, Immune-Escape, Immune Checkpoint Regulation
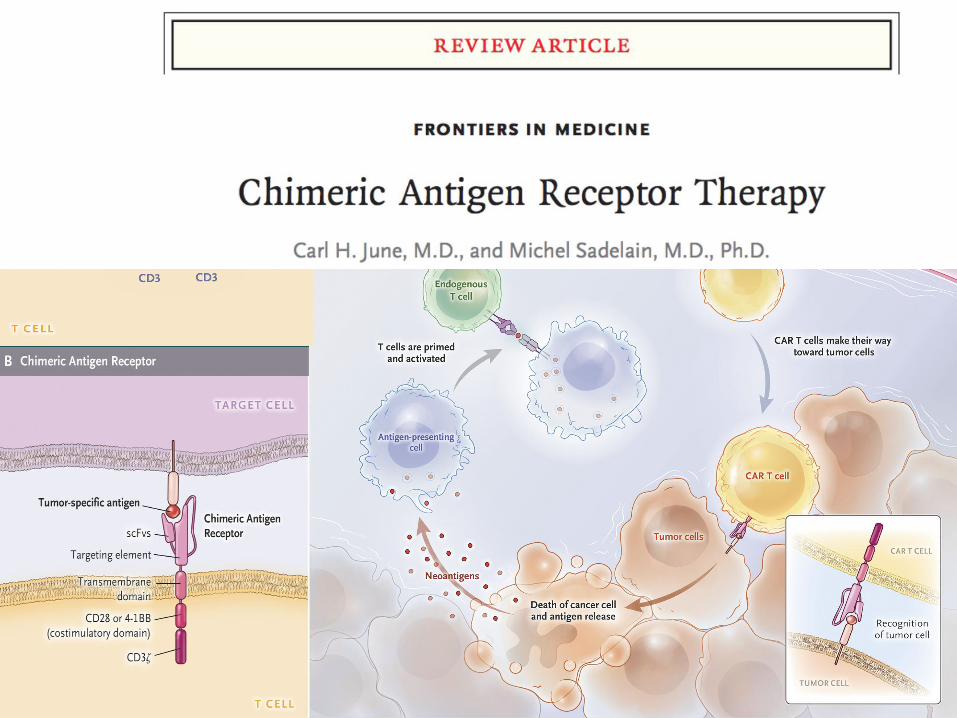

• Currently, the single approved marker-driven treatment :
pembrolizumab (immune checkpoint inhibitor) for tumors
with defective MMR (abnormal IHC findings).
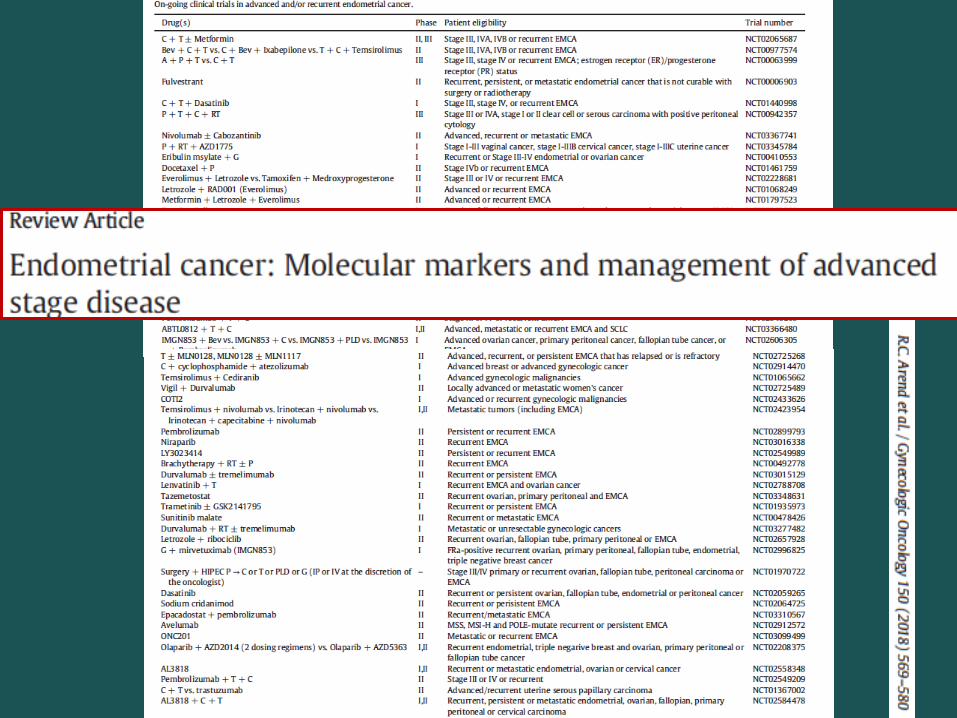
• There is promise for targetting specific mutations/defects for
advanced stage endometrial cancers:
• PIK3CA pathway (PIK3CA or mTOR inhibitors),
• ER/PR (hormonal therapy),
• PTEN mutations (mTOR inhibitors or PARP inhibitors),
• ARIDIA mutations (EZH2 inhibitors, or PARP inhibitors)
• VEGF inhibitor(??) for recurrent ?
• Trials in recurrent Emca (GOG-86P and MITO END-2 trials)

• Bevacizumab (VEGF inhibitor) or temsirolimus (mTOR
inhibitor) with chemotherapy (stage III, Stage IVA, Stage IVB or
recurrent).
• PFS :19.6 months in patients with p53 loss of function (null) for
bevacizumab+paclitaxel+carboplatin compared to 12.2 months
PFS in the p53 wild-type group
• The group treated with temsirolimus did not show any effect
P53 MUTANTS??
A.R.Mallen, V.L. Filiaci, D.A. Levine, K. Thiel, C.A. Aghajanian, X.Meng, E. Devor,
K.N. Moore, M.A. Powell, A.A. Secord, K.S. Tewari, D.P. Bender, A.R. Stuckey, J.M.
Fowler, S.B. Dewdney, K.K. Leslie, Evidence for synthetic lethality between
bevacizumab and chemotherapy in advanced, p53 null endometrial cancers, 49th
Annual Meeting of the Society of Gynecologic Oncology. New Orleans, LA, 2018.

What do new techniques bring us?
Euphoria
Disappointment
Reality
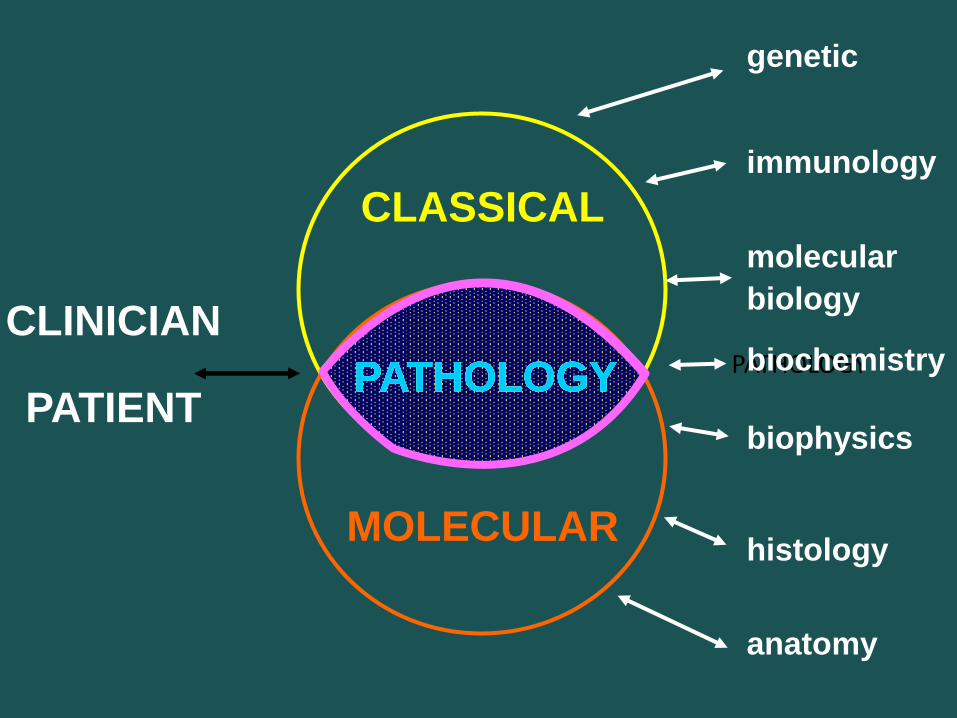
PATHOLOGY
CLASSICAL
MOLECULAR
CLINICIAN
PATIENT
genetic
immunology
molecular
biology
biochemistry
biophysics
histology
anatomy
PATHOLOGYPATHOLOGYPATHOLOGYPATHOLOGYPATHOLOGY

Tesekkurler………………[email protected]

mutation
deletion
amplification
translocation
Genomic studies will offer pathologistsan unprecedented opportunity to bridgebasic research and clinical science
Application of genomic data and incorporate those to pathology practice will re-define the roles of pathologists in the patient care
Pathology will be the critical profession that advances future translational genomic research and providing new information beyond morphology

Nanopore sequencing-Towards the 15-minute genomeGenetics: Pulling strands of DNA through nanopores could dramatically speed up the sequencing of human genomes
Nanopore
(a-hemolysin)
Mar 10th 2011
… It is now possible to sequence
a human genome in about eight
days, at a cost of around $10,000.
But researchers dream of being
able to complete the process in a
matter of hours, or even minutes,
for less than $1,000.

Thank You…[email protected]
DISEASES
Congenital
have genetic basis
• Pathologic presence:infectious diseases
• Abnormal gene expression
• Aberrant gene creation
Acquired

Normal endometriumARID 1A expression
Low-grade Endometrioid Endometrial Carcinoma:ARID 1A loss
Serous endometrial CarcinomaNo ARID 1A loss
AJSP 35:625, 2011
Low-grade Endometrioid Endometrial Carcinoma:ARID 1A loss
Serous endometrial CarcinomaNo ARID 1A loss
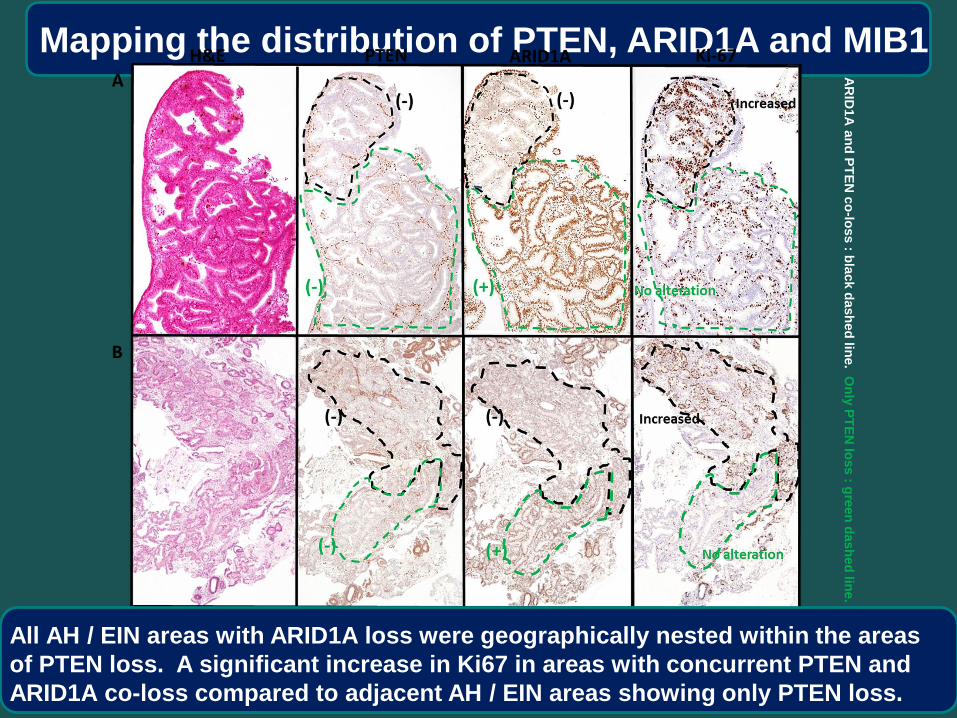
Mapping the distribution of PTEN, ARID1A and MIB1
All AH / EIN areas with ARID1A loss were geographically nested within the areas
of PTEN loss. A significant increase in Ki67 in areas with concurrent PTEN and
ARID1A co-loss compared to adjacent AH / EIN areas showing only PTEN loss.
AR
ID1
A a
nd
PT
EN
co
-loss : b
lack d
ash
ed
line. O
nly
PT
EN
loss : g
reen
dash
ed
line.

PPP2R1A mutations occur frequently in
uterine serous but not endometrioid CA

Fadare & Zheng, 2009
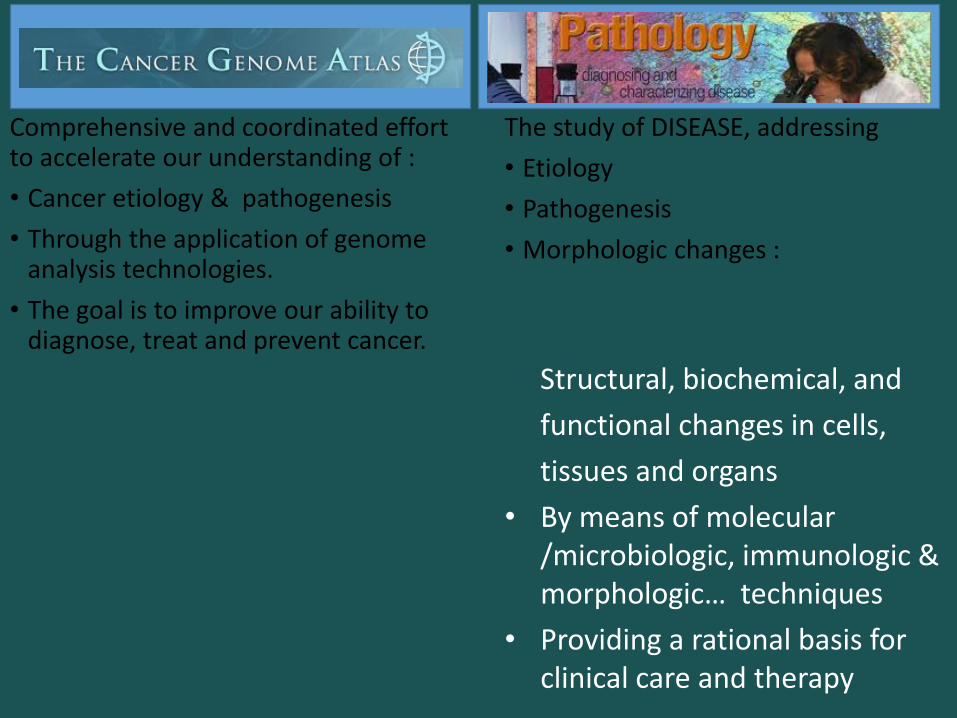
Comprehensive and coordinated effort to accelerate our understanding of :
• Cancer etiology & pathogenesis
• Through the application of genome analysis technologies.
• The goal is to improve our ability to diagnose, treat and prevent cancer.
The study of DISEASE, addressing
• Etiology
• Pathogenesis
• Morphologic changes :
Structural, biochemical, and
functional changes in cells,
tissues and organs
• By means of molecular /microbiologic, immunologic & morphologic… techniques
• Providing a rational basis for clinical care and therapy