Embed Size (px)
Citation preview

THE JOU R N A L OF BO N E & JO I N T SU RG ER Y · JB JS .ORG
VO LUM E 89-A · NUM B ER 1 · JAN UA R Y 2007
DU P UY T RE N D I SE A S E : AN ATOMY, PA TH O LO G Y,
PRE S EN T A T I ON , A N D TRE A T M EN T
Dupuytren Disease: Anatomy, Pathology, Presentation, and Treatment
By Ghazi M. Rayan, MD
An Instructional Course Lecture, American Academy of Orthopaedic Surgeons
The disorder called Dupuytren disease has been recognized for approximately 400 years. Its presentation, although seemingly rather constant, is actually extremely variable, depending on which structures are involved. A thorough knowledge of palmar fascial anatomy is essential to the understanding of Du-puytren disease. There have been re-cent advances in the pathophysiology of Dupuytren disease, and these have added to our knowledge of this disorder but have not yet changed its treatment. There are two distinct clinical entities, classic Dupuytren disease and atypical, so-called non-Dupuytren palmar fas-cial disease1,2. These two types differ in presentation, etiology, treatment, and prognosis. Authors of future epidemio-logical and outcome studies should not confuse these two clinical entities. Sur-gical treatment is the conventional and most widely used method of managing Dupuytren disease.
The earliest published reference to the disorder that was later to be called Dupuytren disease was by Felix Platter, who in 1614 described a case, attributing the deformity to a flexor tendon contracture3. In 1777 Henry Cline recognized that the disorder in-
volved the palmar fascia, in 1822 Sir Astley Cooper advocated closed fasciot-omy as a treatment for the condition, and in 1831 Guillaume Dupuytren gave a detailed anatomic and pathologic de-scription of the disease and demon-strated a surgical case in Paris that earned him the disease eponym4. By 1900 there were at least 256 publica-tions related to Dupuytren disease and at least eight books on the subject2,5-11.
Age, gender, geography, and ethnicity influence the disease preva-lence, which has been reported to be as low as 2% and as high as 42%12-14. Men are more likely to have it than women (a ratio of nine to one), and the overall incidence increases with age, with the frequency in women catching up to that in men later in life15. The disease is common in Scandinavia, Great Brit-ain, Ireland, Australia, and North America. It is uncommon in southern Europe and South America and rare in Africa and China16,17.
Dupuytren disease is associated with diabetes18-20. Burge et al. reported a higher risk of Dupuytren disease in al-coholics, smokers, people with hyperc-holesterol, and patients infected with human immunodeficiency virus21-23.
There is controversy regarding a rela-tionship between Dupuytren disease and seizure disorders24,25. The etiology of Dupuytren disease remains controver-sial as well, but inflammation, trauma, neoplasia, and genetics have been im-plicated as factors26-31. The evidence is strongest for at least a genetic predispo-sition. There is a clearly increased inci-dence in relatives of patients with Dupuytren disease, and there has been at least one report of identical twins with the disease13,32. There seems to be an autosomal dominant transmission with variable penetrance.
Anatomy
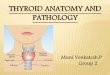
The radial, ulnar, and central apo-neuroses, palmodigital fascia, and digital fascia are all part of the palmar fascial complex (Fig. 1)33. These struc-tures are involved to varying degrees in Dupuytren disease. Each structure can be subdivided. The radial aponeu-rosis has four components: the thenar fascia (an extension of the central apo-neurosis), the thumb pretendinous band (small or absent), the distal com-missural ligament, and the proximal commissural ligament34. The ulnar apo-neurosis consists of the hypothenar
Disclosure: The author did not receive grants or outside funding in support of his research for or preparation of this manuscript. He did not receive
payments or other benefits or a commitment or agreement to provide such benefits from a commercial entity. No commercial entity paid or directed,
or agreed to pay or direct, any benefits to any research fund, foundation, educational institution, or other charitable or nonprofit organization with
which the author is affiliated or associated.

THE JOU R N A L OF BO N E & JO I N T SU RG ER Y · JB JS .ORG
VO LUM E 89-A · NUM B ER 1 · JAN UA R Y 2007
DU P UY T RE N D I SE A S E : AN ATOMY, PA TH O LO G Y,
PRE S EN T A T I ON , A N D TRE A T M EN T
muscle fascia (an extension of the cen-tral aponeurosis), the pretendinous band to the small finger (always present and very substantial), and the abductor digiti minimi confluence, which is enveloped by the fibers of the sagittal band35,36. The central aponeurosis is the core of Dupuytren disease activity. It is a triangular fascial layer with its apex proximal. Its fibers are oriented longi-tudinally, transversely, and vertically. The longitudinal fibers fan out as pre-tendinous bands in the three central digits, and each bifurcates distally. Each bifurcation has three layers37. A superficial layer inserts into the dermis, a middle layer continues to the digit as the spiral band, and a deep layer passes almost vertically and dorsally. The transverse fibers make up the natatory ligament located in the distal part of the palm and the transverse ligament of the palmar aponeurosis. The transverse lig-
ament of the palmar aponeurosis is proximal and parallel to the natatory ligament and deep to the pretendinous bands. Its distal, radial extent is the proximal commissural ligament. The transverse ligament of the palmar apo-neurosis gives origin to the septa of Legueu and Juvara, which protect the neurovascular structures and provide an additional proximal pulley to the flexor tendons. The vertical fibers of the central aponeurosis are the minute ver-tical bands of Grapow and the septa of Legueu and Juvara. The vertical bands are numerous, small, strong, and scat-tered along the palmar fascial complex and are most abundant in the central aponeurosis38. The vertical septa of Legueu and Juvara are deep to the pal-mar fascia and form fibro-osseous compartments33,39,40. There are eight septa, one radial and one ulnar for each finger41. They form seven compart-
ments of two types: four flexor septal canals that contain the flexor tendons and three web space canals that contain the common digital nerves and arteries and the lumbrical muscles (Fig. 2). These septa are inserted in a soft-tissue confluence that consists of five struc-tures: the A1 pulley, the palmar plate, the sagittal band, the interpalmar plate ligament, and the septa of Legueu and Juvara (Fig. 3). The fascial structures in the palmodigital region are complex. The middle layer of the bifurcated pre-tendinous band spirals on its axis nearly 90°, and the peripheral fibers run verti-cally adjacent to the metacarpopha-langeal joint capsule40. They continue distally deep to the neurovascular bun-dle and natatory ligaments and emerge distal to the natatory ligaments to con-tinue as the lateral digital sheet. This spiral band therefore is the connection between the palmar and digital fascial structures. The proximal fibers of the natatory ligaments run in a transverse plane, but the distal fibers form a “u” and continue longitudinally along both sides of the digit, forming the lateral digital sheet. The lateral digital sheet therefore has deep and superficial con-tributions from the spiral band and the natatory ligament. The neurovascular bundle in the digit is surrounded by four fascial structures: the Grayson liga-ment (palmar), the Cleland ligament (dorsal), the Gosset lateral digital sheet laterally, and the Thomine retrovascular fascia medially and dorsally42.
Pathophysiology
The myofibroblast is the offending cell in Dupuytren disease. It was described originally by Gabbiani and Majno43 and further studied by Tomasek et al.44. The myofibroblast has morphologic charac-teristics of both a fibroblast and a smooth muscle cell, and it can actively contract45. The myofibroblast of Du-puytren disease expresses alpha-smooth muscle actin that plays a role in contrac-tion46. The Dupuytren myofibroblast synthesizes fibronectin, an extracellular glycoprotein, which connects myofibro-blastic cells together and connects myo-fibroblastic cells to the extracellular stromal matrix with an integrin47,48.
Fig. 1
Palmar fascial complex with its five components: the radial aponeurosis (RA), ulnar aponeurosis
(UA), central aponeurosis, palmodigital fascia, and digital fascia. NL = natatory ligament, PA =
palmar aponeurosis, and TLPA = transverse ligament of the palmar aponeurosis. (Reprinted,
with permission, from: Rayan GM. Palmar fascial complex anatomy and pathology in Dupuytren’s
disease. Hand Clin. 1999;15:75.)

THE JOU R N A L OF BO N E & JO I N T SU RG ER Y · JB JS .ORG
VO LUM E 89-A · NUM B ER 1 · JAN UA R Y 2007
DU P UY T RE N D I SE A S E : AN ATOMY, PA TH O LO G Y,
PRE S EN T A T I ON , A N D TRE A T M EN T
Myofibroblast contractility can be influenced by prostaglandins, which are found in nodules and active stages of the disease49-51. Fibroblast growth factor (FGF), transforming growth factor-alpha (TGF-α), epidermal growth factor, interleukin-1 (IL-1), and platelet-derived growth factor (PDGF) have been found to be ex-pressed more in Dupuytren disease52.
In Dupuytren disease, normal fascial bands become diseased cords53. Dupuytren nodules and cords are pathognomonic of Dupuytren disease54. A nodule usually appears first, but sometimes a cord develops without a nodule. Typically, the cords progres-sively shorten, leading to joint and soft-tissue contracture. The cords involve the palmar, palmodigital, or digital re-gions. Shortened cords cause joint de-formity, and long-standing flexion deformity leads to contracture of the capsuloligamentous tissue and flexion contractures of the metacarpopha-langeal and proximal interphalangeal joints.
Grapow vertical bands become microcords leading to skin-thickening, which is one of the earliest manifesta-
Fig. 2
Interpalmar plate ligament (IPPL) and septa of Legueu and Juvara. PA = palmar
aponeurosis. (Reprinted, with permission, from: Rayan GM. Palmar fascial complex
anatomy and pathology in Dupuytren’s disease. Hand Clin. 1999;15:79.)
Fig. 3
Soft-tissue confluence and septa of Legueu and Juvara. IPPL = interpalmar plate ligament and PA = palmar
aponeurosis. (Reprinted, with permission, from: Rayan GM. Palmar fascial complex anatomy and pathology in
Dupuytren’s disease. Hand Clin. 1999;15:80.)

THE JOU R N A L OF BO N E & JO I N T SU RG ER Y · JB JS .ORG
VO LUM E 89-A · NUM B ER 1 · JAN UA R Y 2007
DU P UY T RE N D I SE A S E : AN ATOMY, PA TH O LO G Y,
PRE S EN T A T I ON , A N D TRE A T M EN T
tions of Dupuytren disease. Skin pits develop from the first layer of the split pretendinous band and are usually dis-tal to the distal palmar crease.
The pretendinous cord develops from the pretendinous band and is the cord most frequently seen in Du-puytren disease. It is responsible for flexion deformity of the metacarpopha-langeal joint and often extends distally to continue with digital cords. Occa-sionally, the pretendinous cord bifur-cates distally, with each branch extending into a different digit and forming a commissural “Y” cord. The vertical cord is less common and is con-nected to the pretendinous cord55. The vertical cord is short thick diseased tis-sue departing from the pretendinous cord and extending deeply in between the neurovascular bundle and the flexor tendon fibrous sheath. This cord is the diseased septa of Legueu and Juvara. Extensive palmar fascial disease is en-countered in severe conditions and af-fects a large area of the palm, leading to diffuse thickening of many compo-nents of the palmar fascial complex in-cluding the transverse ligament of the palmar aponeurosis.
The spiral cord has four origins; the pretendinous band, the spiral band, the lateral digital sheet, and the Grayson ligament56. This cord is encountered most often in the small finger, but it may affect the ring finger. In the palm it is located superficial to the neurovascu-lar bundle, just distal to the metacar-pophalangeal joint; it passes deep to the neurovascular bundle; and in the digit it runs lateral to the neurovascular bundle as it involves the lateral digital sheet. Distally in the digit it is again superficial to the neurovascular bundle as it in-volves the Grayson ligament. Initially, the cord spirals around the neurovascu-lar bundle, but as it contracts the cord straightens and the neurovascular bun-dle spirals around the cord. The dis-torted anatomy of the neurovascular bundle, which displaces medially and centrally, renders it at risk of injury during surgery57,58. The natatory cord develops from the natatory ligament, converting the u-shaped web-space fi-bers into a v shape and producing a
contracture of the second, third, and fourth web spaces. The cord extends along the dorsal-lateral aspect of the adjacent digits and can be best detected by passively abducting the digits and at the same time flexing one digit and extending the other at the metacar-pophalangeal joints. This maneuver al-lows the natatory cord to become more prominent.
The most frequently encountered digital cords are the central, spiral, and lateral cords. They are responsible for flexion deformity of the proximal inter-phalangeal joints. The central cord is an extension of the pretendinous cord in the palm. It courses in the midline and attaches into the flexor tendon sheath near the proximal interphalangeal joint or the periosteum of the middle pha-lanx on one side of the digit. The cen-tral cord usually does not displace the neurovascular bundle. The lateral cord originates from the lateral digital sheet and attaches to the skin or to the flexor tendon sheath near the Grayson liga-ment. The lateral cord leads to contrac-ture of the proximal interphalangeal joint but can cause a flexion contracture of the distal interphalangeal joint. This cord can displace the digital neurovas-cular bundle toward the midline by its volume. The abductor digiti minimi cord is also known as the isolated digital cord. It originates from the abductor digiti minimi tendon, but it may also arise from the nearby muscle fascia or base of the proximal phalanx. It courses superficial to the neurovascular bundle and infrequently entraps and displaces it toward the midline. It frequently in-serts on the ulnar side of the base of the middle phalanx, but it may attach on the radial side or have an additional in-sertion in the base of the distal phalanx, causing a contracture of the distal inter-phalangeal joint. The retrovascular cord is a poorly defined structure but is thought to develop from the retrovas-cular band of Thomine and is located deep to the neurovascular bundle58. It is different from the checkrein ligament. The retrovascular diseased tissue does not cause contracture of the proximal interphalangeal joint, but if the tissue is not removed, the proximal interpha-
langeal joint contracture may not be completely corrected.
The distal commissural cord is the diseased distal commissural liga-ment, which is the radial extension of the natatory ligament, whereas the proximal commissural cord originates from the proximal commissural liga-ment, which is the radial extension of the transverse ligament of the palmar aponeurosis. Both of these cords cause contracture of the first web space. The thumb pretendinous cord originates from the thumb pretendinous band and causes flexion deformity of the thumb metacarpophalangeal joint59, which is uncommon.
Diagnosis and Classification
In its early stages, Dupuytren disease can be difficult to diagnose60-62. Skin changes are the earliest manifestation. Changes on the dorsum of the hand consist of either Garrod nodes, which are rare, or knuckle pads, which are more common. Garrod nodes are firm nodules at the proximal interpha-langeal joints63,64. Knuckle pads are fi-brosing lesions over the proximal interphalangeal joints. They are preva-lent in patients with bilateral disease and in those with ectopic disease, such as in the feet and genitals63. Knuckle pads include loss of wrinkles, thicken-ing, tethering, or hyperkeratosis. They are found in just fewer than half of pa-tients with Dupuytren disease, and the index finger is the most common digit involved65,66.
The changes in the palm begin with the formation of microcords from the Grapow fibers, which connect the dermis to the palmar fascia. This pro-duces a pseudocallus or thickening of the skin and underlying subcutaneous tissue. These vertical bands are proba-bly the first anatomic structures to be-come affected by Dupuytren disease. The deep subcutaneous fat becomes fibrotic near the distal palmar crease67. As a result, the skin becomes tethered and adherent to the underlying fascial structures and loses its normal mobility. Skin-thickening is often associated with surface rippling and dimpling. A skin pit is rarely confused or associated with

THE JOU R N A L OF BO N E & JO I N T SU RG ER Y · JB JS .ORG
VO LUM E 89-A · NUM B ER 1 · JAN UA R Y 2007
DU P UY T RE N D I SE A S E : AN ATOMY, PA TH O LO G Y,
PRE S EN T A T I ON , A N D TRE A T M EN T
other conditions and therefore it is a re-liable sign of early Dupuytren disease. Skin pits are caused by deep full-thickness skin retraction into the subcutaneous tissue. The diseased superficial fibers of the split pretendinous band form a der-mal cord that pulls the dermal side of the skin inward. The apex of the cone-shaped skin pit is often buried deep within the subcutaneous space and cannot be seen by the examiner.
A Dupuytren nodule is a firm soft-tissue mass that is fixed to both the skin and the deep fascia. The nodule seems to originate in the superficial components of the palmar or digital fascia. It is usually well defined, local-ized, and raised above the surface, but it can be only a diffuse thickening of the deeper fascia. Nodules occur in the palm or digits. Palmar nodules are adja-cent to the distal palmar crease, often in line with the ring and small fingers and sometimes proximal to the base of the thumb and small finger. Digital nodules are usually near the proximal interpha-langeal joint or at the base of the digit. Nodules are often painless, but they can enlarge and become troublesome, caus-ing pain when they are associated with stenosing tenosynovitis as a result of di-rect pressure on the flexor tendons and A1 pulley or from a vertical cord. Nod-ules have an abundance of myofibro-blasts and a rich vascular supply.
Nodules tend to regress sponta-neously and are replaced by a cord, but a cord can develop and mature without nodule regression. The normal bands discussed previously are the precursors of pathologic cords54. Early cords can adhere to the skin and blend with the nodule, making it difficult to ascertain where a nodule ends and a cord begins. The cord later becomes prominent and acquires the appearance and consis-tency of a tendon. Cords are located in the palm, the palmodigital area, or the digits. A mature cord has only sparse myofibroblasts but abundant collagen.
The disease has early, intermedi-ate, and late phases. Skin changes with loss of normal architecture and for-mation of skin pits is the early phase. Nodules and cords form during the intermediate phase, and contractures
mark the late phase. The late phase tends to go through four stages of con-tracture, with contracture of the meta-carpophalangeal joint of the ring finger in stage I; contractures of the metacar-pophalangeal and proximal interpha-langeal joints of the ring finger and the metacarpophalangeal joint of the small finger in stage II; contractures of the metacarpophalangeal and proximal in-terphalangeal joints of the ring finger, the metacarpophalangeal and proximal interphalangeal joints of the small fin-ger, and the metacarpophalangeal joint of the long finger in stage III; and stage-III contractures as well as distal inter-phalangeal joint hyperextension of the ring or small finger in stage IV. This progression is not immutable. In many cases, palmar fascial disease or contrac-ture remains confined to the palm and does not progress enough to cause digi-tal flexion deformity. Palmar involve-ment usually precedes extension of the disease into the digits; however, the dis-ease may also begin and remain in the digits. The ring finger is the most com-monly involved digit, followed in order of frequency by the small, long, and in-dex fingers and lastly by the thumb. The anatomy of the neurovascular bundle can be distorted as the spiral cord con-tracts. A palpable interdigital soft-tissue mass is an indication that the neurovas-cular bundle is involved, but it is not a reliable indicator57,68.
Dupuytren disease may affect locations other than the hand, and patients with Dupuytren disease should be examined for ectopic sites of involvement. Ectopic disease can be either regional in the upper extremity or distant in other parts of the body. Garrod nodes or knuckle pads occur on the dorsum of the hand and are al-most always limited to the fingers. Three reports have noted disease ex-tension into the wrist area69-71.
Dupuytren contractures have been reported in more proximal loca-tions in the upper extremity72,73. Distant ectopic disease occurs occasionally, and patients with knuckle pads are more likely to have distant involvement66. The most common distant ectopic disease is fibromatosis restricted to the plantar
fascia. This is usually asymptomatic and rarely causes flexion contracture of the toes74,75. Wheeler and Meals76 reported on a patient with Dupuytren disease who had bilateral palmar contracture, bilateral plantar nodules, and nodular fasciitis of the popliteal space.
There is a clinical condition that is similar to Dupuytren disease but should not be confused with it. It is termed non-Dupuytren disease1,2. Classic Dupuytren disease occurs mostly in white people, whereas non-Dupuytren disease occurs mostly in a diverse ethnic group. Non-Dupuytren disease is unilateral, usually involving a single digit, and it is not in-frequently associated with trauma, in-cluding surgery. Patients with this disease rarely need surgical treatment, and the condition can spontaneously improve. Confusing these two condi-tions can produce contrasting epidemio-logical data.
In addition to non-Dupuytren dis-ease, there are other soft-tissue changes that can mimic early Dupuytren disease, and certain pathologic processes can be mistaken for established Dupuytren dis-ease. Epithelioid sarcoma has masquer-aded as Dupuytren disease77,78. Also, skin changes and nodules in Dupuytren dis-ease should be distinguished from occu-pational thickening, hyperkeratosis, and callus formation that are caused by chronic friction and pressure on a work-ing person’s hand61. McGrouther de-scribed changes in the edematous hand that cause bulging of the subcutaneous adipose tissue between fibrous bands with exaggeration of normal anchorage of the fascia to the skin, giving the ap-pearance of early Dupuytren disease62. Large Dupuytren nodules should be differentiated from palmar soft-tissue subcutaneous lesions such as localized pigmented villonodular synovitis (soft-tissue giant-cell tumor), palmar gangli-ons, and inclusion cysts. Stenosing tenosynovitis without triggering can be associated with thickening and adher-ence of the skin to the underlying flexor tendon sheath. Prominence of flexor ten-dons due to attenuation of anular pul-leys, as is found in rheumatoid arthritis, can be confused with pretendinous cords79. Digital joint flexion deformity

THE JOU R N A L OF BO N E & JO I N T SU RG ER Y · JB JS .ORG
VO LUM E 89-A · NUM B ER 1 · JAN UA R Y 2007
DU P UY T RE N D I SE A S E : AN ATOMY, PA TH O LO G Y,
PRE S EN T A T I ON , A N D TRE A T M EN T
such as that seen following ulnar nerve lesions and posttraumatic contracture also should be differentiated from long-standing Dupuytren disease. The pres-ence of other manifestations in the typi-cal disease can reinforce its diagnosis. Accurate diagnosis and differentiation between the types of palmar fascial con-tracture are necessary to gain insight into the disease prognosis and to achieve a satisfactory treatment outcome.
Treatment
Observation is indicated for a patient who has static Dupuytren disease with minimal contracture and without com-promise of function. Recent basic-science research has shown the potential of cer-tain local agents in the treatment of Dupuytren disease. These include the calcium channel blockers nifedipine and verapamil45 for early stages of the disease and collagenase80 for advanced stages. Enzymatic fasciotomy with trypsin and hyaluronidase followed by forced extension of the digit has been reported81. Steroid injection into nodules has been used to suppress the disease82. Intrale-sional injections of gamma-interferon83 decrease the symptoms and the size of the lesions in both Dupuytren disease and hypertrophic scars, probably by de-creasing expression of alpha-smooth muscle actin and production of col-lagen. There is no consensus regarding local injection for the treatment of Du-puytren disease.
Surgery is the most widely used treatment for advanced Dupuytren dis-ease. Flexion contracture of the meta-carpophalangeal joint of >30° and flexion contracture of the proximal in-terphalangeal joint of 15° interfere with function and, in the presence of a well-developed cord, are indications for sur-gical treatment. Treatment of metacar-pophalangeal joint contractures is more successful than that of proximal inter-phalangeal joint contractures.
Percutaneous fasciotomy was first used by Astley Cooper and has been advocated for palmar cords in older patients84,85. In severe cases, this technique may be useful as a prelimi-nary procedure86. There is a risk to the flexor tendons and the nerves, and re-
flex sympathetic dystrophy has been re-ported after percutaneous releases87. The technique of percutaneous release utilizes a stab wound adjacent to the cord and a number-11 blade to cut the cord while the digit is extended.
Fasciectomy is associated with a lower recurrence rate than is fasciot-omy (15% compared with 43%). Par-tial, regional, or limited fasciectomy remains the most conventional and widely used technique among hand surgeons today88,89. Partial fasciectomy is the excision of the diseased tissue only and was first described by Goyrand in 1834. Freehafer and Strong recom-mended that treatment with use of multiple small longitudinal incisions88.
In segmental aponeurectomy, multiple small incisions are created in the palm and digits, and segments of diseased tissue are excised without re-moval of all tissue. Russ first described this minimally invasive technique, and the results are comparable with those of other methods of treatment, with a re-currence rate of 21%89,90. The procedure is done through a series of c-shaped in-cisions, and 1-cm segments of diseased tissue are excised.
McIndoe and Beare performed a total fasciectomy through a transverse palmar incision and digital z-plasties without excising the skin, which they reported on in 195891. Zachariae com-pared this procedure with a limited fasciectomy and found nearly equal functional results, but other authors reported a higher incidence of compli-cations with total fasciectomy92.
Dermofasciectomy involves si-multaneous excision of skin and dis-eased tissue10,93. The recurrence rate after this procedure is lower than that after other surgical techniques. When it was combined with skin-grafting, there were no recurrences beneath the graft even when the method was used to treat recurrent disease93-95. A midterm review revealed recurrent nodule formation limited to graft insets in 10% of pa-tients, without recurrence of cords. There were few other complications, but an increase in disease extension was found between three and thirteen years after dermofasciectomy94,96. This tech-
nique is best suited for recurrent and severe primary disease, when the skin is adherent to the underlying Dupuytren disease tissue, but it is not indicated for all recurrent and severe cases. Roush and Stern reported the total range of motion after operative treatment of re-current Dupuytren disease to be better after fasciectomy and flap coverage than after skin-grafting or arthrodesis97. An attempt should always be made to dis-sect the skin from Dupuytren disease tissue, but skin that cannot be saved should be excised and skin graft should be used if necessary.
Severe flexion deformity of the proximal interphalangeal joint can re-sult in a residual contracture after exci-sion of the offending digital cord. This contracture may be due to attenuation of the central slip of the extensor ten-don, which is placed at risk by a pro-longed contracture of the proximal interphalangeal joint, especially when the deformity exceeds 60°. If the proxi-mal interphalangeal joint remains con-tracted after a digital fasciectomy, extension splinting for several weeks can help to restore the tone of the cen-tral slip95,96,98-100. Surgical release of a proximal interphalangeal joint contrac-ture after fasciectomy is indicated if the residual deformity is >40°.
Preoperative and postoperative skeletal traction with an external fixa-tion device has been utilized to im-prove correction of severe contractures of the proximal interphalangeal joint. In severe cases, a continuous-elongation technique prior to fasciectomy has been shown to decrease the deformity, facilitate surgery, minimize the need for amputation, and alter the collagen ori-entation and even the metabolism of the fascia101,102. Although this technique is an additional option for treating diffi-cult cases, it is associated with a high rate of complications such as infection, pin-loosening, recurrence, and even amputation.
Salvage procedures may be neces-sary for severe digital deformities (for example, a flexion contracture of the proximal interphalangeal joint in ex-cess of 70°) and especially for recurrent cases with an exuberant amount of

THE JOU R N A L OF BO N E & JO I N T SU RG ER Y · JB JS .ORG
VO LUM E 89-A · NUM B ER 1 · JAN UA R Y 2007
DU P UY T RE N D I SE A S E : AN ATOMY, PA TH O LO G Y,
PRE S EN T A T I ON , A N D TRE A T M EN T
scarring. Dorsal wedge osteotomy of the proximal phalanx is a method to prevent amputation103. Another option is arthrodesis of the proximal interpha-langeal joint combined with resection of a portion of the proximal phalanx to shorten the digit, allowing extension without tension on the neurovascular structures. Arthroplasty of the proxi-mal interphalangeal joint with a silicone implant can correct some of the defor-mity and retain motion but is associ-ated with the risk of further flexion deformity of the joint. Amputation at the proximal interphalangeal joint or through the proximal phalanx may be necessary when nerve and vascular damage results in loss of sensory func-tion and cold intolerance.
Primary closure should be used whenever possible. McGrouther illus-trated about sixty diagrams in the liter-ature of surgical incisions used for the treatment of Dupuytren disease62. How-ever, the most commonly used are the Bruner zigzag incision and the midline longitudinal incision that is closed with multiple z-plasties.
When primary closure is not possible, the wounds can be left open. Dupuytren was the first to leave wounds open after making a transverse palmar incision. McCash used the same method with minor modifications104. The palmar incision is left open to heal by secondary intention. Reports of satis-factory results of this method, with less pain, better motion, and low compli-cation rates, continue to appear in the literature105-108.
A full-thickness skin graft from the wrist, the ulnar side of the hand, or the antecubital area is most useful for recurrent or severe cases when primary closure is not possible. A distally based dorsal hand flap, rotation flaps from the side of the fourth and fifth digits, and a cross-finger flap from an adja-cent digit can be used. A butterfly flap is useful for coverage after excision of a natatory cord from a digital web space in order to minimize web-space con-tracture formation. Simple and four-flap z-plasties can be used for the first web space.
Complications of surgery for
Dupuytren disease are either technique-related, such as neurovascular injury, hematoma, and infection, or related to patient physiology, such as stiffness and reflex symptomatic dystrophy. Boyer and Gelberman classified complications temporally as intraoperative, early post-operative, and late postoperative109. The risk of digital nerve injury is asso-ciated with severe contractures of the metacarpophalangeal and proximal in-terphalangeal joints, with altered nerve anatomy by a spiral cord, and, espe-cially in recurrent cases, with exuber-ant amounts of scar tissue. Preventive measures include isolation of the neu-rovascular bundle by careful dissection, with use of loop magnification and on the basis of knowledge of the patho-logic anatomy. The dissection is carried out in a proximal-to-distal direction, sometimes in combination with a distal-to-proximal approach, prior to re-moval of the diseased cord. If the nerve is transected, a primary repair should be done.
A vascular injury can be an arte-rial laceration, arterial spasm, intimal hemorrhage, or vessel rupture result-ing from vigorous correction of a se-vere digital joint contracture. Arterial laceration that results in vascular com-promise requires immediate repair or placement of an interposition vein graft. Arterial spasm and intimal hemorrhage are treated first by re-positioning the digit in flexion, then irrigating with warm saline solution, applying topical lidocaine, and even administering intravenous heparin. If all else fails, vascular reconstruction should be done.
Separating diseased tissue from adherent skin is difficult, especially in recurrent cases. To reduce the risk of buttonholing the skin, the use of a number-15C scalpel and the back of the knife as a dissector allows separation of diseased tissue from normal skin. In ad-dition, using an operating room light to transilluminate from the epidermal side of the skin allows visualization of the thickness of the flap and can alert the surgeon when the dissection is becom-ing too superficial.
Hematoma is prevented by tour-
niquet deflation and then achieve-ment of adequate hemostasis prior to wound closure. Deflating the tourni-quet and assessing the skin vascularity prior to closure to ensure adequate cir-culation is the best way to prevent skin necrosis. Closure under tension should be avoided, and skin-grafting or use of the open palm method should be considered if a primary closure is too tight. If skin necrosis develops, exci-sion of necrotic tissue and skin-grafting or flap coverage are performed.
Reflex sympathetic dystrophy, also referred to as a “flare” reaction and “complex regional pain syndrome,” may occur after surgery. The patient has swelling, hyperemia, dysesthesias, and pain out of proportion to that expected. Direct trauma to the nerves and exces-sive dissection are thought to be pre-disposing factors. The simultaneous performance of a carpal tunnel release with the surgery for Dupuytren disease is a predisposing factor, especially in women. An atraumatic surgical tech-nique and gentle handling of nerves and other tissues during surgery should minimize the development of this com-plication. If a specific cause cannot be identified, the treatment is therapy for pain control. In recalcitrant cases, a se-ries of stellate sympathetic ganglion blocks can be helpful.
Inclusion cysts can occur near the scar as a result of entrapment of dermal tissue in the subcutaneous space and can be prevented by careful attention to skin approximation dur-ing wound closure. Hypertrophic scar formation is lessened by careful attention to the placement of the skin incisions.
The recurrence rate ranges be-tween 2% and 60%, with an average of 33%104-108,110. This may represent true recurrence (disease at the operative site) or disease extension (disease out-side of the area of the prior surgery). Recurrence is more common in pa-tients with proximal interphalangeal joint involvement, a diseased small fin-ger, and more than one digit affected as well as in those who present a longer time after surgery or after a secondary fasciectomy.

THE JOU R N A L OF BO N E & JO I N T SU RG ER Y · JB JS .ORG
VO LUM E 89-A · NUM B ER 1 · JAN UA R Y 2007
DU P UY T RE N D I SE A S E : AN ATOMY, PA TH O LO G Y,
PRE S EN T A T I ON , A N D TRE A T M EN T
Ghazi M. Rayan, MDUpper Extremity, Hand and Microsurgery Center, Baptist Physicians Building D, 3366 N.W. Expressway, Suite 700, Oklahoma City, OK 73112
Printed with permission of the American Academy of Orthopaedic Surgeons. This arti-cle, as well as other lectures presented at the Academy’s Annual Meeting, will be available in February 2007 in Instructional Course Lec-
tures, Volume 56. The complete volume can be ordered online at www.aaos.org, or by calling 800-626-6726 (8 A.M.-5 P.M., Central time).
References
1. Rayan G, Moore J. Non-Dupuytren’s disease
of the palmar fascia. J Hand Surg [Br]. 2005;
30:551-6.
2. Rayan GM. Clinical presentation and types of Du-
puytren’s disease. Hand Clin. 1999;15:87-96.
3. Elliot D. The early history of Dupuytren’s disease.
Hand Clin. 1999;15:1-19, v.
4. Dupuytren G. De la retraction des doigts par suite
d’une affection de l’aponevrose palmaire – descrip-
tion de la maladie – operation Chirugicale qui con-
vient dens de cas. J Univ Hebd Med Chir Prat Inst
Med. 1831;5:349-65.
5. Stack HG. The palmar fascia. Edinburgh: Churchill
Livingstone; 1973.
6. Hueston JT, Tubiana R, editors. Dupuytren’s
disease. 2nd ed. New York: Churchill Livingstone;
1985.
7. McFarlane RM, McGrouther DA, Flint MH, edi-
tors. Dupuytren’s disease: biology and treatment.
New York: Churchill Livingstone; 1990.
8. Berger A, Delbruck A, Brenner P, Hinzmann R,
editors. Dupuytren’s disease pathobiochemistry
and clinical management. New York: Springer;
1994.
9. Hueston JT, Seyfer AE. Some medicolegal as-
pects of Dupuytren's contracture. Hand Clin. 1991;
7:617-32.
10. Tubiana R, Leclercq C, Hurst LC, Badalamente
MA, Mackin EJ, editors. Dupuytren’s disease. Lon-
don: Martin Dunitz; 2000.
11. Brenner P, Rayan GM. Dupuytren’s disease: a
concept of surgical treatment. Vienna: Springer;
2003.
12. Ross DC. Epidemiology of Dupuytren’s disease.
Hand Clin. 1999;15:53-62, vi.
13. Ling RSM. The genetic factor in Dupuytren’s dis-
ease. J Bone Joint Surg Br. 1963;45:709-18.
14. Mikkelsen O. Epidemiology in a Norwegian pop-
ulation. In: McFarlane RM, McGrouther DA, Flint
MH, editors. Dupuytren’s disease: biology and
treatment. New York: Churchill Livingstone; 1990.
p 199-200.
15. Early PF. Population studies in Dupuytren’s con-
tracture. J Bone Joint Surg Br. 1962;44:602-13.
16. Hueston JT. Dupuytren’s diathesis. In: Hueston
JT, editor. Dupuytren’s contracture. Edinburgh: Liv-
ingstone; 1963. p 51-63,E45.
17. McFarlane R. On the origin and spread of Dupuy-
tren’s disease. J Hand Surg [Am]. 2002;27:385-90.
18. McFarlane R, Ross D. Dupuytren’s disease. In:
Weinzweig J, editor. Plastic surgery secrets. Phila-
delphia: Hanley and Belfus; 1998. p 554-9.
19. Arkkila PE, Kantola IM, Viikari JS. Dupuytren’s
disease: association with chronic diabetic complica-
tions. J Rheumatol. 1997;24:153-9.
20. Chammas M, Bousquet P, Renard E, Poirier JL,
Jaffiol C, Allieu Y. Dupuytren’s disease, carpal tunnel
syndrome, trigger finger and diabetes mellitus. J
Hand Surg [Am]. 1995;20:109-14.
21. Burge P, Hoy G, Regan P, Milne R. Smoking, alco-
hol and the risk of Dupuytren’s contracture. J Bone
Joint Surg Br. 1997;79:206-10.
22. Noble J, Arafa M, Royle SG, McGeorge G,
Crank S. The association between alcohol, hepatic
pathology and Dupuytren’s disease. J Hand Surg
[Br]. 1992;17:71-4.
23. An HS, Southworth SR, Jackson WT, Russ B.
Cigarette smoking and Dupuytren’s contracture of
the hand. J Hand Surg [Am]. 1988;13:872-4.
24. Critchley EM, Vakil SD, Hayward HW, Owen VM.
Dupuytren’s disease in epilepsy: result of prolonged
administration of anticonvulsants. J Neurol Neuro-
surg Psychiatry. 1976;39:498-503.
25. Arafa M, Noble J, Royle SG, Trail IA, Allen J.
Dupuytren's and epilepsy revisited. J Hand Surg
[Br]. 1992;17:221-4.
26. Chansky HA, Trumble TE, Conrad EU 3rd, Wolff
JF, Murray LW, Raskind WH. Evidence for a poly-
clonal etiology of palmar fibromatosis. J Hand Surg
[Am]. 1999;24:339-44.
27. Zachariae L. Dupuytren’s contracture: the aetio-
logical role of trauma. Scand J Plast Reconstr Surg.
1971;5:116-9.
28. Meagher S. Manual work and industrial injury:
a personal commentary. In: McFarlane RM,
McGrouther DA, Flint MH, editors. Dupuytren’s
disease: biology and treatment. New York:
Churchill Livingstone; 1990. p 261-3.
29. Hueston JT, Seyfer AE. Some medicolegal as-
pects of Dupuytren’s contracture. Hand Clin.
1991;7:617-34.
30. McFarlane R, Botz J, Cheung H. Epidemiology of
surgical patients. In: McFarlane RM, McGrouther
DA, Flint MH, editors. Dupuytren’s disease: biology
and treatment. New York: Churchill Livingstone;
1990. p 201-13.
31. Liss GM, Stock SR. Can Dupuytren’s contracture
be work related?: review of the evidence. Am J Ind
Med. 1996;29:521-32.
32. Couch H. Identical Dupuytren’s contracture
in identical twins. Can Med Assoc J. 1938;
39:225-6.
33. Rayan GM. Palmar fascial complex anatomy
and pathology in Dupuytren’s disease. Hand Clin.
1999;15:73-86.
34. Tubiana R, Simmons BP, DeFrenne HA. Location
of Dupuytren’s disease on the radial aspect of the
hand. Clin Orthop Relat Res. 1982;168:222-9.
35. White S. Anatomy of the palmar fascia on the
ulnar border of the hand. J Hand Surg [Br]. 1984;
9:50-6.
36. Rayan GM, Murray D, Chung KW, Rohrer M. The
extensor retinacular system at the metacarpopha-
langeal joint. Anatomical and histological study. J
Hand Surg [Br]. 1997;22:585-90.
37. McGrouther DA. The microanatomy of Du-
puytren’s contracture. Hand. 1982;14:215-36.
38. Grapow M. Die anatomie und physiologische
bedeutung der palmaraponourose. Archiv fur
Anatomie Und Physiologie Leipzig. Anatomicsche
Abtheilung. 1887;143:2-3.
39. Legueu F, Juvara E. Des aponévroses de
la paume de la main. Bull Soc Anat Paris. 1892;
6:383.
40. Gosset J. Dupuytren’s disease and the anatomy
of the palmodigital aponeurosis. In: Hueston JT,
Tubiana R, editors. Dupuytren’s disease. 2nd ed.
New York: Churchill Livingstone; 1985. p 75-81.
41. Bilderback KK, Rayan GM. The septa of Legueu
and Juvara: an anatomic study. J Hand Surg [Am].
2004;29:494-9.
42. Thomine JM. The development and anatomy of
the digital fascia. In: Hueston JT, Tubiana R, edi-
tors. Dupuytren’s disease. 2nd ed. New York:
Churchill Livingstone; 1985. p 3-12.
43. Gabbiani G, Majno G. Dupuytren’s contracture:
fibroblast contraction? An ultrastructural study. Am J
Pathol. 1972;66:131-46.
44. Tomasek JJ, Gabbiani G, Hinz B, Chaponnier C,
Brown RA. Myofibroblasts and mechano-regulation
of connective tissue remodelling. Nat Rev Mol Cell
Biol. 2002;3:349-63.
45. Rayan GM, Parizi M, Tomasek JJ. Pharmaco-
logic regulation of Dupuytren’s fibroblast contrac-
tion in vitro. J Hand Surg [Am]. 1996;21:1065-70.
46. Tomasek JJ, Rayan GM. Correlation of alpha-
smooth muscle actin expression and contraction in
Dupuytren’s disease fibroblasts. J Hand Surg [Am].
1995;20:450-5.
47. Tomasek JJ, Haaksma CJ. Fibronectin filaments
and actin microfilaments are organized into a fibro-
nexus in Dupuytren’s diseased tissue. Anat Rec.
1991;230:175-82.
48. Halliday NL, Rayan GM, Zardi L, Tomasek JJ.
Distribution of ED-A and ED-B containing fibronectin
isoforms in Dupuytren’s disease. J Hand Surg [Am].
1994;19:428-34.
49. Hurst LC, Badalamente MA, Makowski J. The
pathobiology of Dupuytren’s contracture: effects of
prostaglandins on myofibroblasts. J Hand Surg
[Am]. 1986;11:18-23.
50. Chiu HF, McFarlane RM. Pathogenesis of
Dupuytren’s contracture: a correlative clinical-
pathological study. J Hand Surg [Am]. 1978;3:1-10.
51. Magro G, Fraggetta F, Colombatti A, Lanzafame
S. Myofibroblasts and extracellular matrix glycopro-
teins in palmar fibromatosis. Gen Diagn Pathol.
1997; 142:185-90.
52. Badalamente MA, Hurst LC. The biochemistry of
Dupuytren’s disease. Hand Clin. 1999;15:35-42.
53. Luck JV. Dupuytren’s contracture; a new concept
of the pathogenesis correlated with surgical man-
agement. J Bone Joint Surg Am. 1959;41:635-64.
54. McFarlane RM. Patterns of the diseased fascia
in the fingers in Dupuytren’s contracture. Displace-
ment of the neurovascular bundle. Plast Reconstr
Surg. 1974;54:31-44.
55. Bilderback KK, Rayan GM. Dupuytren’s cord in-
volving the septa of Legueu and Juvara: a case re-
port. J Hand Surg [Am]. 2002;27:344-6.
56. McFarlane R. The finger. In: McFarlane RM, Mc-
Grouther DA, Flint MH, editors. Dupuytren’s disease:

THE JOU R N A L OF BO N E & JO I N T SU RG ER Y · JB JS .ORG
VO LUM E 89-A · NUM B ER 1 · JAN UA R Y 2007
DU P UY T RE N D I SE A S E : AN ATOMY, PA TH O LO G Y,
PRE S EN T A T I ON , A N D TRE A T M EN T
biology and treatment. New York: Churchill Living-
stone; 1990. p 155-67.
57. Umlas ME, Bischoff RJ, Gelberman RH. Predic-
tors of neurovascular displacement in hands with
Dupuytren’s contracture. J Hand Surg [Br]. 1994;
19:664-6.
58. McFarlane R. The anatomy of Dupuytren’s
disease. In: Hueston JT, Tubiana R, editors. Du-
puytren’s disease. 2nd ed. New York: Churchill Liv-
ingstone; 1985. p 54-71.
59. Rayan GM. Dupuytren’s disease. American Acad-
emy of Orthopaedic Surgeons (AAOS) Orthopaedic
Knowledge Online. http://www5.aaos.org/oko
60. Hueston JT. Dupuytren’s contracture. Edin-
burgh: Livingstone; 1963.
61. McFarlane RM. Dupuytren’s disease: relation to
work and injury. J Hand Surg [Am]. 1991;16:775-9.
62. McGrouther D. The extensor mechanism and
knuckle changes. An overview of operative treat-
ment. In: McFarlane RM, McGrouther DA, Flint MH,
editors. Dupuytren’s disease: biology and treat-
ment. New York: Churchill Livingstone; 1990.
p 295-310.
63. Garrod AE. On an unusual form of nodule upon
the joints of the fingers. St. Bartholomew’s Hosp
Rep. 1893;29:157-61.
64. Hueston JT. Dorsal Dupuytren’s disease. J Hand
Surg [Am]. 1982;7:384-7.
65. Skoog T. Dupuytren’s contracture with special
reference to etiology and improved surgical treat-
ment, its occurrence in epileptics. Acta Chir Scandi-
nav. 1948;96(Suppl 139):1.
66. Caroli A, Zanasi S, Marcuzzi A, Guerra D,
Cristiani G, Ronchetti IP. Epidemiological and
structural findings supporting the fibromatous
origin of dorsal knuckle pads. J Hand Surg [Br].
1991;16:258-62.
67. Flint M. The genesis of the palmar lesion. In:
McFarlane RM, McGrouther DA, Flint MH, editors.
Dupuytren’s disease: biology and treatment. New
York: Churchill Livingstone; 1990. p 282-70.
68. Short WH, Watson HK. Prediction of the spiral
nerve in Dupuytren’s contracture. J Hand Surg [Am].
1982;7:84-6.
69. Boyes JH, Jones FE. Dupuytren’s disease involv-
ing the volar aspect of the wrist. Plast Reconstr
Surg. 1968;41:204-7.
70. Simons AW, Srivastava S, Nancarrow JD. Du-
puytren’s disease affecting the wrist. J Hand Surg
[Br]. 1996;21:367-8.
71. Sinha A. Dupuytren’s disease may extend be-
yond the wrist crease in continuity. J Bone Joint Surg
Br. 1997;79:211-2.
72. Okano M. Dupuytren’s contracture (palmar fibro-
matosis) extending over the arm. Acta Derm Ve-
nereol. 1992;72:381-2.
73. Bunnell S. Surgery of the hand. Philadelphia:
J.B. Lippincott; 1944. p 613.
74. Classen DA, Hurst LN. Plantar fibromatosis and
bilateral flexion contractures: a review of the litera-
ture. Ann Plast Surg. 1992;28:475-8.
75. Donato RR, Morrison WA. Dupuytren’s disease
in feet causing flexion contracture in the toes. J
Hand Surg [Br]. 1996;21:364-6.
76. Wheeler ES, Meals RA. Dupuytren’s diathesis: a
broad spectrum disease. Plast Reconstr Surg.
1981;68:781-3.
77. Erdmann MW, Quaba AA, Sommerlad BC. Epi-
thelioid sarcoma masquerading as Dupuytren’s dis-
ease. Br J Plast Surg. 1995;48:39-42.
78. Yacoe ME, Bergman AG, Ladd AL, Hellman BH.
Dupuytren’s contracture: MR imaging findings and cor-
relation between MR signal intensity and cellularity of
lesions. AJR Am J Roentgenol. 1993;160:813-7.
79. Elliot D, Khan J. Palmar bands in rheumatoid ar-
thritis and other chronic conditions of the upper
limb. J Hand Surg [Br]. 1996;21:369-74.
80. Badalamente MA, Hurst LC. Enzyme injection
as nonsurgical treatment of Dupuytren’s disease.
J Hand Surg [Am]. 2000;25:629-36.
81. McCarthy DM. The long-term results of enzymic
fasciotomy. J Hand Surg [Br]. 1992;17:356.
82. Ketchum LD, Donahue TK. The injection of nod-
ules of Dupuytren’s disease with triamcinolone ace-
tonide. J Hand Surg [Am]. 2000;25:1157-62.
83. Pittet B, Rubbia-Brandt L, Desmouliere A,
Sappino AP, Roggero P, Guerret S, Grimaud JA,
Lacher R, Montandon D, Gabbiani G. Effect of
gamma-interferon on the clinical and biologic
evolution of hypertrophic scars and Dupuytren’s
disease: an open pilot study. Plast Reconstr Surg.
1994;93:1224-35.
84. Colville J. Dupuytren’s contracture—the role of
fasciotomy. Hand. 1983;15:162-6.
85. Rowley DI, Couch M, Chesney RB, Norris SH. As-
sessment of percutaneous fasciotomy in the man-
agement of Dupuytren’s contracture. J Hand Surg
[Br]. 1984;9:163-4.
86. Bryan AS, Ghorbal MS. The long-term results
of closed palmar fasciotomy in the management of
Dupuytren’s contracture. J Hand Surg [Br]. 1988;
13:254-6.
87. Leclercq C Hurst L, Badalamente M. Nonsurgi-
cal treatment. In: Tubiana R, Leclercq C, Hurst LC,
Badalamente MA, Mackin EJ, editors. Dupuytren’s
disease. London: Martin Dunitz; 2000. p 121-31.
88. Freehafer AA, Strong JM. The treatment of Du-
puytren’s contracture by partial fasciectomy. J Bone
Joint Surg Am. 1963;45:1207-16.
89. Russ R. The surgical aspects of Dupuytren’s
contraction. Am J Med Sci. 1908;135:856.
90. Moermans JP. Segmental aponeurectomy in Du-
puytren’s disease. J Hand Surg [Br]. 1991;16:243-54.
91. McIndoe A, Beare R. The surgical management
of Dupuytren’s contracture. Am J Surg.
1958;95:197-203.
92. Zachariae L. Extensive versus limited fasciec-
tomy for Dupuytren’s contracture. Scand J Plast Re-
constr Surg. 1967;1:150-3.
93. Hueston JT. The control of recurrent Dupuytren’s
contracture by skin replacement. Br J Plast Surg.
1969;22:152-6.
94. Searle AE, Logan AM. A mid-term review of the re-
sults of dermofasciectomy for Dupuytren’s disease.
Ann Chir Main Memb Super. 1992;11:375-80.
95. Ketchum LD, Hixson FD. Dermofasciectomy and
full-thickness grafts in the treatment of Dupuytren’s
contracture. J Hand Surg [Am]. 1987;12:659-64.
96. Kelly C, Varian J. Dermofasciectomy: a long
term review. Ann Chir Main Memb Super. 1992;
11:381-2.
97. Roush TF, Stern PJ. Results following surgery for
recurrent Dupuytren’s disease. J Hand Surg [Am].
2000;25:291-6.
98. Smith P, Breed C. Central slip attenuation in Du-
puytren’s contracture: a cause of persistent flexion
of the proximal interphalangeal joint. J Hand Surg
[Am]. 1994;19:840-3.
99. Weinzweig N, Culver JE, Fleegler EJ. Severe con-
tractures of the proximal interphalangeal joint in Du-
puytren's disease: combined fasciectomy with
capsuloligamentous release versus fasciectomy
alone. Plast Reconstr Surg. 1996;97:560-6.
100. Rives K, Gelberman R, Smith B, Carney K.
Severe contractures of the proximal interpha-
langeal joint in Dupuytren’s disease: results of
a prospective trial of operative correction and
dynamic extension splinting. J Hand Surg [Am].
1992;17:1153-9.
101. Messina A, Messina J. The continuous elonga-
tion treatment by the TEC device for severe Du-
puytren’s contracture of the fingers. Plast Reconstr
Surg. 1993;92:84-90.
102. Bailey AJ, Tarlton JF, Van der Stappen J,
Sims TJ, Messina A. The continuous elongation
technique for severe Dupuytren's disease. A bio-
chemical mechanism. J Hand Surg [Br]. 1994;
19:522-7.
103. Moberg E. Three useful ways to avoid amputa-
tion in advanced Dupuytren’s contracture. Orthop
Clin North Am. 1973;4:1001-5.
104. McCash CR. The open palm technique in
Dupuytren’s contracture. Br J Plast Surg. 1964;
17:271-80.
105. Gelberman RH, Panagis JS, Hergenroeder
PT, Zakaib GS. Wound complications in the surgi-
cal management of Dupuytren’s contracture: a
comparison of operative incisions. Hand. 1982;
14:248-54.
106. Zachariae L. Operation for Dupuytren’s con-
tracture by the method of McCash. Acta Orthop
Scand. 1970;41:433-8.
107. Lubahn JD. Open-palm technique and soft-
tissue coverage in Dupuytren’s disease. Hand Clin.
1999;15:127-36.
108. Schneider LH, Hankin FM, Eisenberg T. Surgery
of Dupuytren’s disease: a review of the open palm
method. J Hand Surg [Am]. 1986;11:23-7.
109. Boyer MI, Gelberman RH. Complications of the
operative treatment of Dupuytren’s disease. Hand
Clin. 1999;15:161-6, viii.
110. Foucher G, Cornil C, Lenoble E. Open palm tech-
nique for Dupuytren’s disease. A five-year follow-up.
Ann Chir Main Memb Super. 1992;11:362-6.