Embed Size (px)
Citation preview

Trzeszcz M1,2, Mazurec M2, Jelen M3, Barcikowski P2, Bielicki K2, Kotkowska-Szeps I2, Maslak M2, Zabielska A2, Kos-Polozynska A2, Mazurec K2
1Department of Pathology and Clinical Cytology, University Hospital in Wroclaw, Poland2Woman’s Health Center Corfamed Ltd, Wroclaw, Poland3Department of Pathology and Oncological Cytology, Wroclaw Medical University, Poland

Current cervical cancer screening systems:
clinical algorithms have limitations in detecting precancerouslesions
developing an efficient management for women with abnormalscreening tests results is challenging
ICC p16/Ki67 test profile:
a simultaneous co-expression of proliferative and anti-proliferative proteins
a biomarker for the high-grade intraepithelial lesion developmentwith high specificity and high sensitivity
a morphology-independent reducing the evaluation subjectivity
a promising role for triaging of HPV-positive women and/or withabnormal cytology results
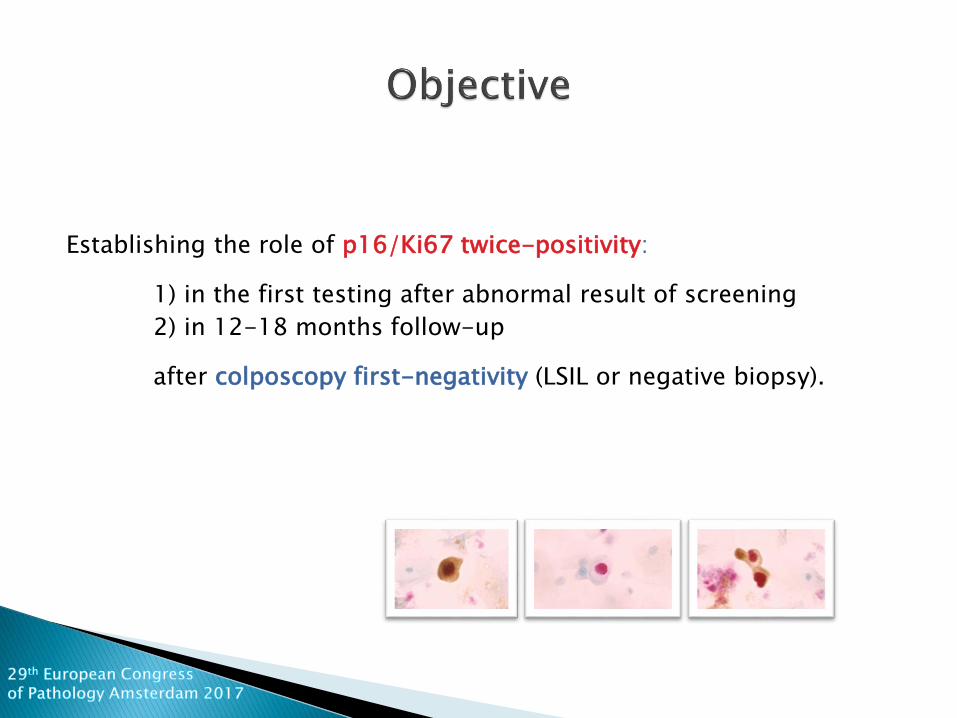
Establishing the role of p16/Ki67 twice-positivity:
1) in the first testing after abnormal result of screening
2) in 12-18 months follow-up
after colposcopy first-negativity (LSIL or negative biopsy).

Fig.1. Study group.
8350 cases (cytology alone/reflex HPV/cotesting)
6398 cases (no HPV results)
1952 cases (reflex HPV/cotesting)
182 cases (declined to participate)
1247 cases (NILM HRHPV14 negative)
3 cases (NILM HRHPV14 positive)
520 cases (ASC-US+ and HRHPV14 positive)
176 cases (no p16/Ki67 test results)
344 cases (ASC-US+ and HRHPV14 positive and test p16/Ki67 results)
163 cases (declined to continue)
181 cases (biopsy results)
157 cases (other results)
24 cases (first-p16/Ki67-positivity & first-biopsy-negativity cases were followed-up with cotest & p16/Ki67)

COTESTING PLUS (HRHPV14 + LBC + P16/Ki67 TEST) for all cotesting ASC-US/LSIL HRHPV14-positive and ASC-H+
COLPO + BIOPSY (random + ECC + directed) for all cotesting ASC-US/LSIL HRHPV14-positive and ASC-H+
FOLLOW-UP (AFTER 12-18 MONTHS) COTESTING PLUS (HRHPV14 + LBC + P16/Ki67 TEST) for all LSIL or NEGATIVE biopsy results
COLPO + BIOPSY (random + ECC + directed) for all cotesting ASC-US/LSIL HRHPV14-positive and ASC-H+
Fig.2. The study protocol and management in group with p16/Ki67 testing.344 women had performed cytology, HPV and first p16/Ki67 testing in one screening round.24 patients with histological LSIL or less (biopsy first-negativity), reached follow-upcotesting with the second p16/Ki67 testing and biopsy in 12-18 months. A random biopsyand endocervical curettage were sampled in all women referred for colposcopy. Ifcolposcopically abnormal lesions were observed, directed biopsy was taken.

Tab. 1. Overview of histologic diagnoses in the second biopsy after12-18 months follow-up with cotesting and p16/Ki67 double-staining.All women who had LSIL or negative histologic results in the first biopsy werereferred for the second colpobiopsy due to ASC-US+ and HRHPV+ in cotesting.
HISTOLOGY
ICC
HSIL n (%) LSIL/NEG n (%) TOTAL n (%)
11 (45,8) 13 (54,2) 24 (100,0)
p16/Ki67+ve 10 (90,9) 2 (15,4) 12 (50,0)
p16/Ki67-ve 1 (9,1) 11 (84,6) 12 (50,0)
Sensitivity % (95% CI)
Specificity % (95% CI)
PPV % (95% CI)
NPV % (95% CI)
p16/Ki67 twice-positivity
89 (52-99) 86 (59-98) 80 (44-97) 93 (66-99)
Tab. 2. Clinical performance of twice-positive p16/Ki67 test for hHSILafter LSIL or negative first biopsy.

Twice-positive p16/Ki67 double-staining test can be a precisebiomarker in triaging patients for the identification of histologicHSIL-risk groups.
p16/Ki67 test result might be decisive in referring to 12-18-months follow-up colposcopy in women with positive first DS testand histologic LSIL or negative result in the first biopsy. Usingp16/Ki 67 test in these cases could be reliable without performingfollow-up cytology or HPV testing.
Authors have declared no conflicts of interest.

1. Huh WK, Ault KA, Chelmow D, Davey DD, Goulart RA, Garcia FA, Kinney WK, Massad LS, Mayeaux EJ, Saslow D, Schiffman M,Wentzensen N, Lawson HW, Einstein MH. Use of primary high-risk human papillomavirus testing for cervical cancerscreening: interim clinical guidance. Gynecol Oncol. 2015 Feb;136(2):178-82. doi: 10.1016/j.ygyno.2014.12.022. Epub 2015Jan 8.
2. Ikenberg H, Bergeron C, Schmidt D, Griesser H, Alameda F, Angeloni C, Bogers J, Dachez R, Denton K, Hariri J, Keller T, vonKnebel Doeberitz M, Neumann HH, Puig-Tintore LM, Sideri M, Rehm S, Ridder R; PALMS Study Group. Screening for cervicalcancer precursors with p16/Ki-67 dual-stained cytology: results of the PALMS study. J Natl Cancer Inst. 2013 Oct16;105(20):1550-7.
3. Lorincz A, Castanon A, Wey Lim AW, Sasieni P. New strategies for human papillomavirus-based cervical screening. WomensHealth (Lond). 2013 Sep;9(5):443-52. doi: 10.2217/whe.13.48.
4. Luttmer R, Dijkstra MG, Snijders PJ, Berkhof J, van Kemenade FJ, Rozendaal L, Helmerhorst TJ, Verheijen RH, Ter HarmselWA, van Baal WM, Graziosi PG, Quint WG, Spruijt JW, van Dijken DK, Heideman DA, Meijer CJ. p16/Ki-67 dual-stained cytologyfor detecting cervical (pre)cancer in a HPV-positive gynecologic outpatient population. Mod Pathol. 2016 Aug;29(8):870-8.
5. Schmidt D, Bergeron C, Denton KJ, Ridder R; European CINtec Cytology Study Group. p16/ki-67 dual-stain cytology in thetriage of ASCUS and LSIL papanicolaou cytology: results from the European equivocal or mildly abnormal Papanicolaoucytology study. Cancer Cytopathol. 2011 Jun 25;119(3):158-66.
6. Wentzensen N, Silver M. Biomarkers for Cervical Cancer Prevention Programs: The Long and Winding Road From Discoveryto Clinical Use. J Low Genit Tract Dis. 2016 Jul;20(3):191-4.
7. Wright TC Jr, Behrens CM, Ranger-Moore J, Rehm S, Sharma A, Stoler MH, Ridder R. Triaging HPV-positive women withp16/Ki-67 dual-stained cytology: Results from a sub-study nested into the ATHENA trial. Gynecol Oncol. 2017Jan;144(1):51-56. doi: 10.1016/j.ygyno.2016.10.031. Epub 2016 Oct 27.
8. Wright TC, Stoler MH, Behrens CM, Sharma A, Zhang G, Wright TL. Primary cervical cancer screening with humanpapillomavirus: end of study results from the ATHENA study using HPV as the first-line screening test. Gynecol Oncol. 2015Feb;136(2):189-97. doi: 10.1016/j.ygyno.2014.11.076. Epub 2015 Jan 8.





























