Embed Size (px)
Citation preview
Dentin bonding agents. Relevance of in vitro investigations
Werner J. Finger, DDS, Dr Med Dent
University of Aachen, and Bayer AG, Donnagen, Federal Republic of Gennany.
Finger WJ: Dentin bonding agents. Relevance of in vitro investigations. Am J Dent 1: 184-188, Special Issue, 1988.
Abstract: Composite resin restorations placed into intradental cavities often show incomplete marginal adaptation due to the effects of polymerization contraction stresses and due to mechanical and/or thermal stress generated at the restoration/cavity interface. Bonding of restorative resins by micromechanical retention to acid-etched enamel and by chemical coupling with dentin and root cementum has a potential of reducing or eliminating marginal gap formation. Dentin bonding agents are usually evaluated by in vitro testing procedures. The determination of bond strength to dentin is the most commonly used method. Bond strength figures should be considered relative to the influence of experimental variables and relative to their reliability as parameters for prediction of cavity adaptation. The efficacy of dentin bonding agents is not conclusively described by in vitro testing. Bond strength figures are only roughly discriminating parameters and not very predictive for the long term clinical performance of a bonded resin restoration.
Key words: Bond strength; dentin bonding agents; restorative dentistry.
Reprint requests: Dr. W J . Finger, Department of Prosthetic Dentistry and Dental Materials, School of Dentistry, University of Aachen, Pauwelstrasse, D - 5100 Aachen, Federal Republic of Germany.
INTRODUCTION The restoration with composite resin of lesions which
are not totally surrounded by enamel is a particular challenge to restorative dentistry. Defects of this type are often CI II, sometimes extensive CI III cavities and almost regularly cervical tooth lesions. The treatment needs for such lesions, either cervical erosions or root caries, is steadily increasing as documented by Katz et al.1
Until recently, restoration of this type of defect with restorative resins and cements has relied on a cavity design giving mechanical retention by undercuts. Consequently, a considerable amount of sound tooth substance had to be sacrificed resulting in a weakening of the tooth. A fum adaptation, however, between restoration and cavity wall was not obtained.
The development of glass ionomer cements has led to some improvements in the restoration of these lesions. The advantages of glass ionomer cements are that they form adhesive bonds to calcified tissues and release fluoride which is readily taken up by mineralized dental tissues. The disadvantages are their brittleness, opacity, rather large water sorption and surface roughness.
The introduction of dentin bonding agents, which by a chemical coupling mechanism mediate a bond between the dental hard tissue; either to the inorganic or to the organic part of dentin, and the restorative resin, has been announced as a real breakthrough in dentistry. After several years of experience with some of these compounds, it became obvious that the high initial ex-
184
pectations, which were mainly based on the results of laboratory studies, were not being fulfilled. New dentinal bonding agents have become available to the profession recently. The manufacturers compete for a share of their products in the market; however, as before, the claims for efficacy are almost exclusively based on the results of laboratory investigations. Sometimes it seems that the manufacturers are competing in a world championship in bond strength figures, where it is implied that the effectiveness of a product is coupled with the magnitude of the bond strength. Similarly, microleakage studies in extracted teeth are often cited as the ultimate proof of a product's benefit.
The purpose of this paper is to discuss the clinical significance of in vitro evaluation parameters, particularly of bond strength figures.
Bond strength to dentin has been and is still the most commonly reported parameter for the evaluation of dentin bonding systems. There is a wide variation in the preparation and design of test specimens. However, basically a flat dentin surface is prepared by grinding and a composite resin rod is polymerized on the dentin following pretreatment and bonding agent application. Then shear or tensile bond strengths are determined. The bonding interface is only moderately loaded by polymerization contraction stresses parallel to the flat dentin surface while shrinkage in a perpendicular direction can occur almost freely and without generation of stresses at the bonding site. This stress pattern is very different from the one developed in a cavity where con-
www.amjdent.com
American JOunull oC Dentist!)" Vol. 1, Speciallssuc, September, 1988
siderable stresses are generated which often result in debonding.
The wide range of bond strength figures reported for identical material systems2 indicate that the test is very complex. Possible variables introduced during bond strength testing are as follow:
Age of the extracted teeth
The age of the extracted teeth, i.e. the duration of storage prior to specimen preparation seems to be of minor significance to bond strength.3 No differences were found in our investigations when extracted teeth were used either immediately after extraction or following storage of up to three months.
Storage condition of the extracted teeth
In contrast, the storage condition of the teeth may be a relevant variable4
• It is, for example, known that preservation in a thymol solution can have an adverse effect on the degree of polymerization of resins. Hansen & Asmussen5 demonstrated that dentin which had been exposed to eugenol-containing temporary restorations contained free eugenol even after refinishing the surface. Eugenol inhibits the polymerization of resins and will thus have an adverse effect on the bond strength to dentin.
In a recent publication,6 very low bond strength figures have been reported for the Glumaa bonding system. In this study the extracted teeth had been stored first in 10% NaOCI solution for 24 hours and then in a 5% NaOCI solution for non-specified time periods. NaOCI effectively removes connective tissue and collagen to which Glumaa is suggested to bond chemically. Therefore, it is not surprising that low bond strengths were reported.
Physiologic saline is suitable when teeth are stored for a few days only, while a 1% Chloramine solution according to Jorgensen et at is an adequate preservative storage medium.
Human or bovine teeth
Due to difficulties experienced in obtaining extracted human teeth, bovine dentin is often used as an alternative. The strength figures obtained on bovine teeth, however, are not comparable and are commonly lower than the ones recorded on human dentin.
Site of dentin used for bonding
Another major variable in bond strength tests is the site of dentin as reported by Causton7 and Mitchem & Gronas.3 Suzuki & Finger8 found a linear relationship between the remaining dentin thickness to the pulp and the shear bond strength mediated by the Glumaj Lumifora system, by Clearftl New BondjClearftl RaY' and by Scotchbond l.c.jSiluxC when determined 15 minutes after light activation of the restorative resin. The relationship between the remaining dentin thickness and the percentage area of solid dentin, that is the area
Relevance of dentin bonding studies 185
of dentin minus the percentage area of dentinal tubules, was described by a logarithmic regression line. The bond strength on dentin close to the pulp was only 30-40% of the bond strength recorded on peripheral dentin. These results may to some extent explain the high coefficients of variation often associated with mean bond strength figures. For clinical dentistry, however, the fmdings may have very limited, if any, significance. When the rules of adhesive cavity preparation are followed, the area of exposed dentinal tubules constitutes a small part only of the dentin surface covered by the restorative. This holds for both smooth surface cervical erosion lesions and for dentin underneath an area of dental caries. In these instances, the lumina of the dentinal tubules are very narrow or may even be obliterated by the apposition of irregular dentin.
In an additional investigation, it was demonstrated that the bond strengths obtained on non-carious extracted third molars were considerably less than the strengths recorded on a random sample of extracted teeth. Th~ reason for this fmding is not fully understood. However, it is hypothesized that non-carious third molars are usually extracted from young individuals soon after eruption. These teeth may have wider dentinal tubules and thus a decrease in the effective bonding area and may be less mineralized than teeth which have been exposed to the oral environment for longer time periods.
Roughness of the dentin surface
Mowery et at studied the effect of the surface roughness of dentin samples on the shear bond strength of light cure Scotchbondc combined with Prism a Fil.d They reported that a rough dentin surface prepared on 60 grit abrasive yielded 4.7 MPa in bond strength after 24 hours. On less roughened dentin abraded 260, 600 and 1200 grit abrasives significantly lower strengths were found. The lowest bond strength figure (2.7 MPa) was reported for dentin prepared on grit 600 abrasive. These observations may be of clinical significance in selecting the cutting instruments for cavity preparation.
Manabe & FingerlO evaluated the effect of dentin roughness on bond strength for the following systems: Clearftl n.b.jClearftl-RaY' (CL), GlumajLumifora (GL), Scotchbond 2jValuxc (SV), ScotchbondjSiluxC (SS), and Tenuree jSiluxC (TS). The tensile bond strengths were determined five minutes after the initiation of light activation of the restorative resins on dentin surfaces ground in one direction on silicone carbide paper with grits of 180, 240, 320, 400, 600 and 4000, respectively. With each of the five systems tested, the bond strengths were independent of the surface roughness of the underlying dentin. Testing by ANOV A showed no statistically significant differences (P > 0.05). The effective bonding surfaces produced by grinding of the dentin on each of the six grits were determined from the surface roughness proftles. The maximum effective dentin surface enlargement due to roughness was approximately 10%. This moderate increase in area may explain why
www.amjdent.com

186 Finger
no significant differences in bond strength were found in spite of the tremendous differences in surface roughness recorded in terms of R or R figures. The average pooled tensile bond str~ngth ftgures in MPa from 60 determinations each were: CL 9.1, GL 15.5, SV 12.9, SS 4.2, and TS 10.1. From this investigation it was concluded that the roughness of prepared dentin surfaces might not be a variable of clinical significance for bonding of resins.
Time of application of the load on the bonded specimen
The time of the application of the load on the bonded test specimen is a critical factor. Bond strengths are usually determined after 24 hours' storage in water or saline at body or room temperature. The crucial time for measuring bond strength is, however, the early time when the stresses arising from polymerization contraction are established, since this is the time interval when debonding may occur between cavity wall and restorative material. It is suggested, therefore, that bond strengths should be determined immediately after the initial curing.lI,12 Additionally, it is certainly necessary for a long term evaluation of the bonding efficacy to determine the bond strengths after prolonged storage time intervals to investigate whether the bond strengths are subject to changes, for example, by hydrolysis. Finger & Ohsawal2 reported that the bond strength of Clearfu New Bond/Clearfil-Ra/ 2 to 3 minutes after light activation of the composite resin was more than twice the bond strength recorded after 24 hours' storage in water.
Fasbinder et 0113 reported that the bond strengths to dentin of Universal Bond/Prismafil,d Bondlite/ Command/ and Scotchbond/Silw( were significantly reduced by storage in water for six months. In contrast, Tenure/Ultrabonde was not affected. The tensile bond bond strengths of this system after 24 hours and 6 months were 2.46 and 2.97 MPa, respectively. Munksgaard & Asmussenl4 reported that the tensile bond strength of Glumaa bonded specimens stored in water was consistently maintained at 17.5 MPa throughout an observation period of six months.
ThennocyC/ing prior to testing
The recent ADA guidelines for dentinal bonding agentsl5
propose that bond strength should be deter~ined both after storage in water and after thermocycling of the specimens. Chan et 01,16 O'Brien et 01,17 and Marchman et 0/
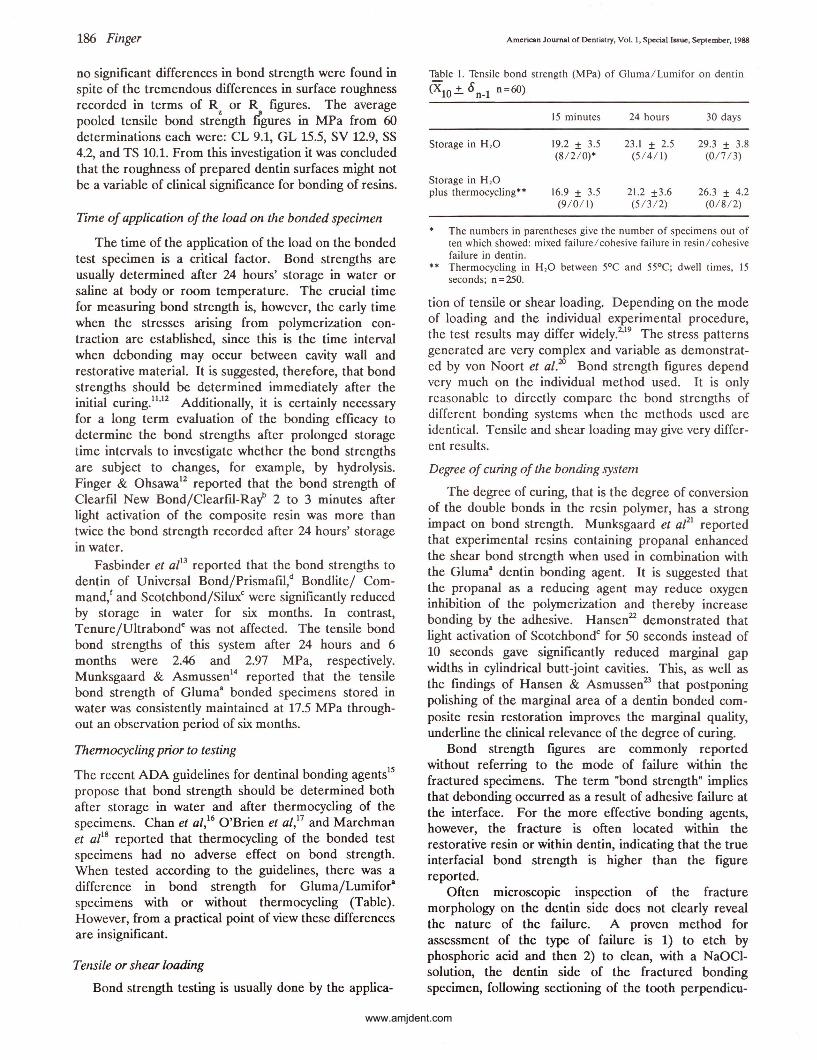
18 reported that thermocycling of the bonded test specimens had no adverse effect on bond strength. When tested according to the guidelines, there was a difference in bond strength for Gluma/Lumifora
specimens with or without thermocycling. (Table). However, from a practical point of view these differences are insignificant.
Tensile or shear loading
Bond strength testing is usually done by the applica-
American Journal of OcntiJ;try, Vol. I , Spcciallssuc, September, 1988
Table I. Tensile bond strength (MPa) of Gluma/ Lumifor on dentin
(XlO'±' 0 n-l n =60)
15 minutes 24 hours 30 days
Storage in H 2O 19.2 ± 3.5 23 .1 ± 2.5 29.3 ± 3.8 (8/2 / 0)* (5 14/ 1) (0 /7 13)
Storage in H 2O plus thermocycling** 16.9 ± 3.5 21.2 ±3 .6 26.3 ± 4.2
(9 / 0/1) (5/ 3/2) (0/ 8/ 2)
The numbers in parentheses give the number of specimens out of ten which showed: mixed failurel cohesive failure in resin l cohesive failure in dentin.
** Thermocycling in H 20 between 5°C and 55°C; dwell times, 15 seconds; n=250.
tion of tensile or shear loading. Depending on the mode of loading and the individual experimental procedure, the test results may differ widely.2,19 The stress patterns generated are very complex and variable as demonstrated by von Noort et al.1JJ Bond strength figures depend very much on the individual method used. It is only reasonable to directly compare the bond strengths of different bonding systems when the methods used are identical. Tensile and shear loading may give very different results.
Degree of curing of the bonding system
The degree of curing, that is the degree of conversion of the double bonds in the resin polymer, has a strong impact on bond strength. Munksgaard et 0121 reported that experimental resins containing propanal enhanced the shear bond strength when used in combination with the Glumaa dentin bonding agent. It is suggested that the propanal as a reducing agent may reduce oxygen inhibition of the polymerization and thereby increase bonding by the adhesive. Hansen22 demonstrated that light activation of Scotchbondc for 50 seconds instead of 10 seconds gave significantly reduced marginal gap widths in cylindrical butt-joint cavities. This, as well as the fmdings of Hansen & Asmussen23 that postponing polishing of the marginal area of a dentin bonded composite resin restoration improves the marginal q~ality, underline the clinical relevance of the degree of curmg.
Bond strength figures are commonly reported without referring to the mode of failure within the fractured specimens. The term "bond strength" implies that debonding occurred as a result of adhesive failure at the interface. For the more effective bonding agents, however, the fracture is often located within the restorative resin or within dentin, indicating that the true interfacial bond strength is higher than the figure reported.
Often microscopic inspection of the fracture morphology on the dentin side does not clearly reveal the nature of the failure. A proven method for assessment of the type of failure is 1) to etch by phosphoric acid and then 2) to clean, with a NaOClsolution, the dentin side of the fractured bonding specimen, following sectioning of the tooth perpendicu-
www.amjdent.com
186 Finger
no significant differences in bond strength were found in spite of the tremendous differences in surface roughness recorded in terms of R or R figures. The average pooled tensile bond str~ngth figures in MPa from 60 determinations each were: CL 9.1, GL 15.5, SV 12.9, SS 4.2, and TS 10.1. From this investigation it was concluded that the roughness of prepared dentin surfaces might not be a variable of clinical significance for bonding of resins.
Time of application of the load on the bonded specimen
The time of the application of the load on the bonded test specimen is a critical factor. Bond strengths are usually determined after 24 hours' storage in water or saline at body or room temperature. The crucial time for measuring bond strength is, however, the early time when the stresses arising from polymerization contraction are established, since this is the time interval when debonding may occur between cavity wall and restorative material. It is suggested, therefore, that bond strengths should be determined immediately after the initial curing.11
•12 Additionally, it is certainly necessary
for a long term evaluation of the bonding efficacy to determine the bond strengths after prolonged storage time intervals to investigate whether the bond strengths are subject to changes, for example, by hydrolysis. Finger & Ohsawal2 reported that the bond strength of Clearfll New Bond/Clearfll-RaY' 2 to 3 minutes after light activation of the composite resin was more than twice the bond strength recorded after 24 hours' storage in water.
Fasbinder et 0113 reported that the bond strengths to
dentin of Universal Bond/Prismafu,d Bondlite/ Command/ and Scotchbond/Siluxc were significantly reduced by storage in water for six months. In contrast, Tenure/Ultrabonde was not affected. The tensile bond bond strengths of this system after 24 hours and 6 months were 2.46 and 2.97 MPa, respectively. Munksgaard & Asmussenl4 reported that the tensile bond strength of Glumaa bonded specimens stored in water was consistently maintained at 17.5 MPa throughout an observation period of six months.
ThennocyC/ing prior to testing
The recent ADA guidelines for dentinal bonding agentslS
propose that bond strength should be deter~ined both after storage in water and after thermocycling of the specimens. Chan et 01,16 O'Brien et 01,17 and Marchman et 0/
18 reported that thermocycling of the bonded test specimens had no adverse effect on bond strength. When tested according to the guidelines, there was a difference in bond strength for Gluma/Lumifora
specimens with or without thermocycling. (Table). However, from a practical point of view these differences are insignificant.
Tensile or shear loading
Bond strength testing is usually done by the applica-
American Journal of Dentistry. Vol. I. Speciall .. ue. September. 1988
Table I. Tensile bond strength (MPa) of Gluma/ Lumifor on dentin (XlO .±. 8n_1 n=60)
15 minutes 24 hours 30 days
Storage in H 2O 19.2 ± 3.5 23.1 ± 2.5 29.3 ± 3.8 (8/2 / 0)* (5 14/ 1) (017 / 3)
Storage in H 2O plus thermocycling** 16.9 ± 3.5 21.2 ±3.6 26.3 ± 4.2
(9 / 0/1) (5 / 3/2) (0 / 8/2)
* The numbers in parentheses give the number of specimens out of ten which showed: mixed failure / cohesive failure in resin / cohesive failure in dentin.
** Thermocycling in H 20 between 5°C and 55°C; dwell times, 15 seconds; n=250.
tion of tensile or shear loading. Depending on the mode of loading and the individual experimental procedure, the test results may differ widely.2.19 The stress patterns generated are very complex and variable as demonstrated by von Noort et al.w Bond strength figures depend very much on the individual method used. It is only reasonable to directly compare the bond strengths of different bonding systems when the methods used are identical. Tensile and shear loading may give very different results.
Degree of curing of the bonding system
The degree of curing, that is the degree of conversion of the double bonds in the resin polymer, has a strong impact on bond strength. Munksgaard et aPI reported that experimental resins containing propanal enhanced the shear bond strength when used in combination with the Gluma8 dentin bonding agent. It is suggested that the propanal as a reducing agent may reduce oxygen inhibition of the polymerization and thereby increase bonding by the adhesive. Hansen22 demonstrated that light activation of Scotchbondc for 50 seconds instead of 10 seconds gave significantly reduced marginal gap widths in cylindrical butt-joint cavities. This, as well as the fmdings of Hansen & Asmussen23 that postponing polishing of the marginal area of a dentin bonded composite resin restoration improves the marginal q~ality, underline the clinical relevance of the degree of curmg.
Bond strength figures are commonly reported without referring to the mode of failure within the fractured specimens. The term "bond strength" implies that debonding occurred as a result of adhesive failure at the interface. For the more effective bonding agents, however, the fracture is often located within the restorative resin or within dentin, indicating that the true interfacial bond strength is higher than the figure reported.
Often microscopic inspection of the fracture morphology on the dentin side does not clearly reveal the nature of the failure. A proven method for assessment of the type of failure is 1) to etch by phosphoric acid and then 2) to clean, with a NaO~Isolution the dentin side of the fractured bondmg , . specimen, following sectioning of the tooth perpendlcu-
www.amjdent.com

American Journal of Dent istry, Vol. I, Special Issue, September, 1988
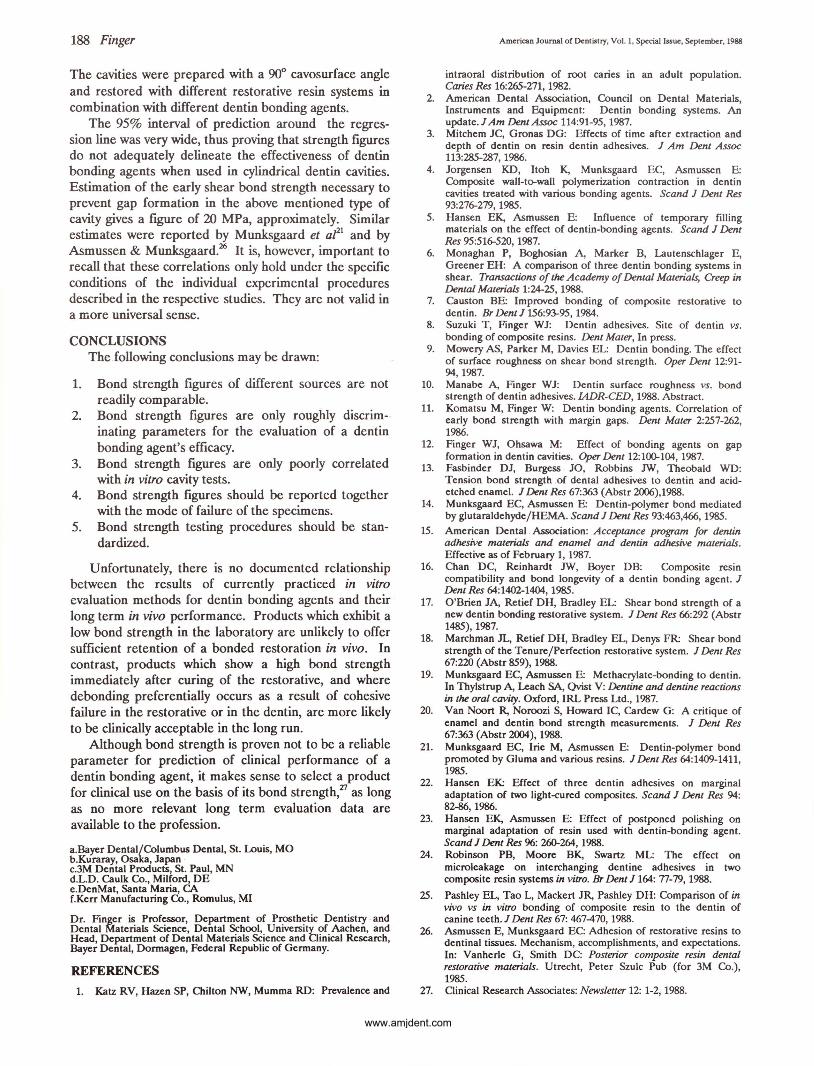
lar to and through the center of the debonded area. Fig. 1 shows an adhesive failure resulting from debonding of a Scotch bond l.c.jSilux" specimen. There is almost no resin left on the bonding surface. The corresponding SEM picture for Clearftl New Bond/Clearftl-RaY' (Fig. 2) shows a mixed type of failure partially cohesive, but mainly adhesive debonding. In contrast, Figs. 3, 4 and 5, the SEM photographs for Gluma/ Lumifor: Scotchbond 2/V alux, C and Tenured / Silux" respectively, show consistently cohesive failure in the resin. The SEM pictures demonstrate that bond strength figures have to be considered very critically, since generally they do not properly describe the quality of the bond. Thus, they may sometimes only reflect strength characteristics of the restorative resin system. It is also well-known that combination of one dentin bonding agent with different restorative resin systems may give different bond strength figures. ll
,24
It has been questioned whether in vitro bond strength testing will reflect the bond strength to dentin in vivo. Due to the hydrostatic pressure of the dentinal fluid in the tubules, a freshly cut dentin surface will be wet. This wetness may impair bonding. Pashley et al'15 reported that no significant differences were observed between
Fig. 1. This and the following SEM photographs Figs 2 through 5, show the dentin side of fractured tensile bond strength specimens (lower half) and a dentin surface produced by sectioning of the specimens perpendicular to the bond 109 interface. The specimen was treated witb a 37% phosphoric acid solution for 60 seconds, then rinsed and dried, and additionally treated with a 10% NaOCI solution for 60 seconds. Scotchbond, light-cured/Silux. Adhesive failure.
Fig. 2. As Fig. 1. Clearfil New Bond/Clearfil-Ray. Mixed failure.
Relevance of dentin bonding studies 187
Fig. 3. As Fig. 1. Gluma Dentin Bond/Lumifor. Cohesive failure.
Fig. 4As Fig. 1. Scotchbond 2/Valux. Cohesive fa ilure.
Fig. 5. As Fig. 1. Tenure/Silux. Cohesive failure.
bonds made in vivo on dog teeth and those made in vitro on the same teeth 30 minutes, one day, one week and one month · post -extraction. In spite of the similarity of the in vivo and in vitro bond strength results, the clinical significance of bond strength figures remains questionable.
Komatsu & Fingerll reported a logarithmic relationship between the maximum widths of marginal contraction gaps in cylindrical butt -joint dentin cavities (cp 3.0 mm, h = l.5mm) and ·the early shear bond strength of a series of material combinations (r = -0.88).
www.amjdent.com
188 Finger
The cavities were prepared with a 900 cavosurface angle and restored with different restorative resin systems in combination with different dentin bonding agents.
The 95% interval of prediction around the regression line was very wide, thus proving that strength figures do not adequately delineate the effectiveness of dentin bonding agents when used in cylindrical dentin cavities. Estimation of the early shear bond strength necessary to prevent gap formation in the above mentioned type of cavity gives a figure of 20 MPa, approximately. Similar estimates were reported by Munksgaard et aPl and by Asmussen & Munksgaard.26 It is, however, important to recall that these correlations only hold under the specific conditions of the individual experimental procedures described in the respective studies. They are not valid in a more universal sense.
CONCLUSIONS The following conclusions may be drawn:
1. Bond strength figures of different sources are not readily comparable.
2. Bond strength figures are only roughly discriminating parameters for the evaluation of a dentin bonding agent's efficacy.
3. Bond strength figures are only poorly correlated with in vitro cavity tests.
4. Bond strength figures should be reported together with the mode of failure of the specimens.
5. Bond strength testing procedures should be standardized.
Unfortunately, there is no documented relationship between the results of currently practiced in vitro evaluation methods for dentin bonding agents and their long term in vivo performance. Products which exhibit a low bond strength in the laboratory are unlikely to offer sufficient retention of a bonded restoration in vivo. In contrast, products which show a high bond strength immediately after curing of the restorative, and where debonding preferentially occurs as a result of cohesive failure in the restorative or in the dentin, are more likely to be clinically acceptable in the long run.
Although bond strength is proven not to be a reliable parameter for prediction of clinical performance of a dentin bonding agent, it makes sense to select a product for clinical use on the basis of its bond strength,27 as long as no more relevant long term evaluation data are available to the profession.
a.Bayer Dental/Columbus Dental, St. Louis, MO b.Kuraray, Osaka, Japan · c.3M Dental Products, St. Paul, MN d.L.D. Caulk Co., Milford, DE e.DenMat, Santa Maria, CA f.Kerr Manufacturing Co., Romulus, MI
Dr. Finger is Professor, Department of Prosthetic Dentistry · and Dental Materials Science, Dental School, University of Aachen, and Head, Department of Dental Materials Science and Clinical Research, Bayer Dental, Dormagen, Federal Republic of Germany.
REFERENCES
1. Katz RV, Hazen SP, Chilton NW, Mumma RD: Prevalence and
American Journal of Dentistry, Vol. 1, Special Issue, September. 1988
intraoral distribution of root caries in an adult population. Caries Res 16:265-271, 1982.
2. American Dental Association, Council on Dental Materials, Instruments and Equipment: Dentin bonding systems. An update. JAm Dent Assoc 114:91-95, 1987.
3. Mitchem JC, Gronas DG: Effects of time after extraction and depth of dentin on resin dentin adhesives. J Am Dent Assoc 113:285-287, 1986.
4. Jorgensen KD, Itoh K, Munksgaard EC, Asmussen E: Composite wall-to-wall polymerization contraction in dentin cavities treated with various bonding agents. Scand J Dent Res 93:276-279, 1985.
5. Hansen EK, Asmussen E: Influence of temporary filling materials on the effect of dentin-bonding agents. Scand J Dent Res 95:516-520, 1987.
6. Monaghan P, Boghosian A, Marker B, Lautenschlager E, Greener EH: A comparison of three dentin bonding systems in shear. Transactions of the Academy of Dental Materials, Creep in Dental Materials 1:24-25, 1988.
7. Causton BE: Improved bonding of composite restorative to dentin. Br Dent J 156:93-95, 1984.
8. Suzuki T, Finger WJ: Dentin adhesives. Site of dentin vs. bonding of composite resins. Dent Mater, In press.
9. Mowery AS, Parker M, Davies EL: Dentin bonding. The effect of surface roughness on shear bond strength. Oper Dent 12:91-94,1987.
10. Manabe A, Finger WJ: Dentin surface roughness vs. bond strength of dentin adhesives. IADR-CED, 1988. Abstract.
11. Komatsu M, Finger W: Dentin bonding agents. Correlation of early bond strength with margin gaps. Dent Mater 2:257-262, 1986.
12. Finger WJ, Ohsawa M: Effect of bonding agents on gap formation in dentin cavities. Oper Dent 12:100-104, 1987.
13. Fasbinder DJ, Burgess JO, Robbins JW, Theobald WD: Tension bond strength of dental adhesives to dentin and acidetched enamel. J Dent Res 67:363 (Abstr 2006),1988.
14. Munksgaard EC, Asmussen E: Dentin-polymer bond mediated by glutaraldehyde/HEMA. Scand J Dent Res 93:463,466, 1985.
15. American Dental Association: Acceptance program for dentin adhesive materials and enamel and dentin adhesive materials. Effective as of February 1, 1987.
16. Chan DC, Reinhardt JW, Boyer DB: Composite resin compatibility and bond longevity of a dentin bonding agent. J Dent Res 64:1402-1404, 1985.
17. O'Brien JA, Retief DH, Bradley EL: Shear bond strength of a new dentin bonding restorative system. J Dent Res 66:292 (Abstr 1485), 1987.
18. Marchman JL, Retief DH, Bradley EL, Denys FR: Shear bond strength of the Tenure/Perfection restorative system. J Dent Res 67:220 (Abstr 859), 1988.
19. Munksgaard EC, Asmussen E: Methacrylate-bonding to dentin. In Thylstrup A, Leach SA, Qvist V: Dentine and dentine reactions in the oral cavity. Oxford, IRL Press Ltd., 1987.
20. Van Noort R, Noroozi S, Howard IC, Cardew G: A critique of enamel and dentin bond strength measurements. J Dent Res 67:363 (Abstr 2004), 1988.
21. Munksgaard EC, Irie M, Asmussen E: Dentin-polymer bond promoted by Gluma and various resins. J Dent Res 64:1409-1411, 1985.
22. Hansen EK: Effect of three dentin adhesives on marginal adaptation of two light-cured composites. Scand J Dent Res 94: 82-86,1986.
23. Hansen EK, Asmussen E: Effect of postponed polishing on marginal adaptation of resin used with dentin-bonding agent. Scand J Dent Res 96: 260-264, 1988.
24. Robinson PB, Moore BK, Swartz ML: The effect on microleakage on interchanging dentine adhesives in two composite resin systems in vitro. Br Dent J 164: n-79, 1988.
25. Pashley EL, Tao L, Mackert JR, Pashley DH: Comparison of in vivo vs in vitro bonding of composite resin to the dentin of canine teeth. J Dent Res 67: 467-470, 1988.
26. Asmussen E, Munksgaard EC: Adhesion of restorative resins to dentinal tissues. Mechanism, accomplishments; and expectations. In: Vanherle G, Smith DC: Posterior composite resin dental restorative materials. Utrecht, Peter Szuic Pub (for 3M Co.), 1985.
27. Clinical Research Associates: Newsletter 12: 1-2,1988.
www.amjdent.com





























