Embed Size (px)
Citation preview

1
DENTAL TREATMENT FOR CHILDREN UNDER GENERAL
ANAESTHESIA AT KING HUSSEIN MEDICAL CENTRE IN
JORDAN
Corresponding author:
Basma K. ALSakarna BDS, MDentSci, JDB,*
Co-authors:
Othman Y. Ajlouni, DDS, MSc, Senior Consultant in Pediatric Dentistry
Hazem M. Khraisat, BDS, JDB
Gadeer E. Mukatash, BDS, MSc
* From the department of dentistry. Queen Alia Military Hospital, Amman
Correspondence should be addressed to:
Dr. Basma ALSakarna
Specialist Paediatric Dentist, Royal Medical Services
E-mail: [email protected]
Postal Address: P. O. Box: 6
Post code: 11710
Amman-Naur
Jordan
Mobile: 0777466439

2
DENTAL TREATMENT FOR CHILDREN UNDER GENERAL
ANAESTHESIA AT KING HUSSEIN MEDICAL CENTRE IN
JORDAN
ABSTRACT
Objectives: To determine the indications and to describe the types of dental treatment, which were
carried out for children under general anaesthesia at King Hussein medical centre in Jordan
Methods: A retrospective, descriptive and comparative study was designed. Data were collected
from patients who required full mouth rehabilitation under general anaesthesia over a one year period
(27-April-2007 to 27-April-2008). The information collected from the records included age, gender,
general health status, indications for general anaesthesia, type of procedure, attendance for review
appointment and treatment provided including the number of primary and permanent teeth extracted
and restored. The type of restoration was also recorded. Note was made of attendance at recall visit.
Results: A total of 92 patients, 56(60.9%) male and 36(39.1%) female received full mouth
rehabilitation under general anaesthesia at King Hussein Medical Centre in Jordan. The age of the
patients range from 2 to 14 years old with mean of 6.30±3.97 years. The main indications for general
anaesthesia were behaviour management problem (44.6%); special health care needs patients (27.2%),
and young children with extensive caries (26.1%). Complete oral rehabilitation including restorations
(fissure sealants, glass ionomer cement, composite filling, and amalgam restorations), dental extraction
of deciduous and permanent teeth and surgical procedures were performed under general anaesthesia
in a single visit. A total of 1030 dental treatments were recorded for 92 patients with a mean of
10.96±4.05. For lacking in cooperative ability children 412 procedures, 338 dental procedures for
special health care needs children and 278 dental procedures for young children with extensive caries
were recorded.

3
Conclusions: It was concluded that dental treatment can be carried out under general anaesthesia in a
hospital environment for certain paediatric patients who are very young with behaviour management
problems, and special health care needs patients. Complete oral rehabilitation under general
anaesthesia which was provided in a single visit proved to be effective and efficient.
Key words: behavior management, children, dental treatment, general anesthesia, medically
compromised.

4
DENTAL TREATMENT FOR CHILDREN UNDER GENERAL
ANAESTHESIA AT KING HUSSEIN MEDICAL CENTRE IN
JORDAN
Introduction
The treatment of young children is a challenging situation for the dental practitioner. “Children are
often anxious in the dental situation and their level of co-operation is limited and the establishment of
a good relationship between the child, his parents and the dentist is important” (1)
.
The majority of children accept dental treatment with the aid of behaviour management techniques in
the dental clinic, with or without local anaesthesia. However, there are some cases where children fail
to respond to dental treatment and the use of general anaesthesia (GA) becomes the only resource to
provide dental treatment for children in a safe and effective way (2)
. The situations that require dental
treatment under GA may include; children with behaviour management problems of extreme anxiety
or fear who refuse to accept treatment using local anaesthesia, very young children with rampant
caries, special health care needs children who have mental or physical disabilities and children
requiring oral surgical procedures (3-6)
. The administration of GA has both advantages and
disadvantages. Advantages include providing comprehensive oral rehabilitation which consists of
fissure sealants, composite/amalgam/glass ionomer restorations, pulpal treatment, stainless steel
crowns and extractions in a short period of time and at a single visit allowing immediate relief of pain
with little or no cooperation from the child (7, 8)
. Among the disadvantages, GA is a procedure which is
never without risk (9)
, an expensive alternative (10)
, and also the administration of GA is relatively safe,
even though mortality following GA in healthy children is unlikely (11)
, morbidity is common (2,12)
. It
has been stated that parents should be informed of the risk of GA and offered, where indicated, a range
of alternative treatments (13)
. Therefore, a greater obligation has now been placed on the dental
profession in respect to assessment, patient information and in obtaining informed consent (14)
.
Previous studies on caries activity levels among children in Jordan have demonstrated that caries
experience among 6 year-old children was 2.73 dmft and 6.09 dmfs; only 29.4% of the children were

5
caries free (15)
. Other studies from Jordan on preschool children aged 1-5 years found that overall 52%
of children were caries free (16)
. This represents a particular problem and a high need for dental
treatment. Until now there had been no previous study on dental treatment for children under GA in
the Royal Medical Services in Jordan. So we are in shortage of this necessary information. The aims of
our study were:
1- To obtain base line data about comprehensive dental treatment under GA for children at King
Hussein Medical Centre (KHMC), which will make it possible to compare future studies from other
sectors in Jordan with ours. 2- To determine the characteristics of children attending for treatment
under GA in relation to age, gender and medical status. 3- To investigate the different indications for
dental treatment of children under GA. 4-To study the mean numbers of different dental procedures
performed under GA at a single day care unit during one year with regard to age groups, indications
and medical condition. These procedures, as mentioned earlier, include operative procedures, pulpal
therapy, stainless steel crowns and extractions.

6
Methods
The Jordanian Royal Medical Services provide medical and dental treatment for free for military
personnel and their dependants. In Jordan there are three military hospitals, located in major cities of
the country which provide comprehensive dental treatment under GA for children. This study had been
undertaken at (KHMC) in Amman. KHMC is the main military hospital in Amman and is considered a
central referral hospital across Jordan. The paediatric dentistry clinic at the dental department at
KHMC provides all types of dental services for hundreds of children monthly, and whenever treatment
is needed under GA it is available. The study was carried out through an assessment of hospital
records of patients who received treatment under GA in the Dental Centre at KHMC in Jordan,
between 27-April-2007 to 27-April-2008. Permission to carry out the study was obtained from the
‘Medical Research Committee’ in the hospital. A total of 92 patients, 56 males and 36 females
received full mouth rehabilitation under GA. The mean age of the patients at the time of procedure was
6.3±3.97 and ranged from 2 to 14 years. 67 patients were healthy and 25 were special health care
needs. Data collected from the records included age at the time of treatment, gender, general health
status, the main indication for treatment under GA. Treatment provided including the number of
primary and permanent teeth extracted and restored. The type of restoration was also recorded.
Preoperative assessment
Forty-eight hours before the surgery, consultation form for paediatrition regarding any contra
indications for GA was required. When the decision was made to use GA to perform a necessary
treatment, the nurse arranged the appointment, explained all practical details and supplied printed
booklet with information about the procedures and instructions to the parents. Parents were given
telephone number to contact if they wanted addition information. The parents were instructed that
fasting should be 6 to 8 hours according to the age of the patient. Treatment was postponed for any
child presenting with acute respiratory infection or congestion. At the time of the study, 2-3 sessions
were held per month with 3-5 patients receiving treatment per session. Informed consent was obtained
by the parents. Priority for treatment was given for special health care needs patients and patients with

7
severe dental pain and abscesses. The oral examination was carried out by single examiner, using a
mouth mirror and dental probe and with appropriate dental lighting. Periapical radiographs, if needed,
were taken during GA since the operating theatre is equipped with periapical dental x-ray machine. A
provisional treatment plan was made with the knowledge that it will be adjusted as needed during
operative procedure. All treatments were carried out by consultant and two paediatric dentists in the
hospital (one of which was the principle investigator) in day care facilities.
Dental procedures in the operation theatre
The final treatment plan was made in the operating theatre, after proper intra-oral examination was
carried. Nasal and endotracheal intubations were the method commonly administered for GA. An oral
pack was placed in order to prevent possible aspiration of debris and pieces of materials during dental
procedures. In the operating theatre maximum dental procedures should be done within minimal time.
The sequence of procedures was as follows:
Start with pulp therapy then place stainless steel crowns if needed.
Restorative preparations which include: amalgam, composite and glass ionomer restorations.
Fissure sealants were placed, then oral cavity was rinsed to remove any debris.
Finally extractions were the last dental procedure.
Statistical analysis
The data were analyzed using computerized Statistical Package for Social Sciences (SPSS) 15 for
windows (SPSS Inc, Chicago, IL, USA). ANOVA test was used to compare the means of multiple
variables. An Independent-Samples T-test was used to compare the means of two variable, while
Chi-Square test was used when proportions were compared. The level of statistical significance was
chosen at p< 0.05

8
Results
Age
The total subjects of the study group were 92 patients. They were made up of 56 males (60.9%) and 36
females (39.1%). The relation between different age groups and gender is shown in Table I. Most of
the study population (54.3%) belonged to the youngest age group (2-5 years). The mean age of the
total study groups at the time of treatment was 6.30 ±3.97 with a range between 2 years and 14 years.
The mean age of males was 6.62±4.34 and that of females was 5.78 ± 3.27. The age of special health
care needs children was generally older than healthy children with a mean age of 7.96±6.35 and
5.63±2.16 respectively.
Indications
The indications for treatment under GA in relation to different age groups are summarized in Table II.
Behaviour management problem was the most common indication for treatment under GA (41
patients) with highest percent among 6-9 years age group (63.4%). Extensive caries was most common
among youngest age group (95.8%). Special health care needs patients were the second most common
reason for treatment under GA (25 cases). The relation between the indications and age groups was
statistically significant (p value < 0.001, Chi-Square test).
Special health care needs patients
36.0% of patients were physically handicapped; also 28.0% of patients were mentally handicapped.
Remaining subjects were having heart disease 12.0%, developmental defects (Sanjad-Sakati
syndrome) 12.0%, 8.0% of patients had bleeding disorders and 4.0% had autism (Table III).
Dental treatment and age groups
The sum of and mean numbers for different dental treatments provided under GA according to age
groups are summarized in Table IV.
The following is an account of the different treatments provided:
Restorations
The restorations provided included fissure sealants, composites, glass ionomer cements and amalgam
restorations. The sum of all restorations was 547 with a mean of 5.82±3.57 teeth restored per child.

9
There was statistically significant difference between restorations and different age groups (p=0.009,
ANOVA). Pulp therapy was more common in youngest age group with a mean of 1.20±1.28. Stainless
steel crowns were more in youngest age group with a mean of 0.74±1.07 with statistically significant
difference between different age groups (p=0.013, ANOVA).
Extractions
The mean of extractions for age group >9 years was less than other younger age groups (2.71 versus
3.65 and 3.96 respectively). The mean for all dental procedures for total subjects was 10.96±4.04. the
mean of all dental treatments per different age groups were 11.24 for 2-5 years 10.38 for 6-9 years and
12.00 for >9 years.
Dental treatments and indications
The sum of and mean numbers for different dental procedures provided for children under GA
according to different indications are summarized in Table V.
Restorations
For 41 children with behaviour management problems a total of 223 restorations with a mean of 5.44
±3.41were done. For the 24 young children with extensive caries the total restorations were 136 with a
mean of 5.67±3.12, while for the 25 special health care needs children the sum was 188 with a mean of
6.96±3.85. There were two children who had undergone surgical procedures for extraction of
supernumerary teeth. No statistically significant was difference observed between restorations and
different indications of GA for children (p=0.743, ANOVA).
Pulp therapy
A total of 88 pulp therapies were done with a mean of 0.94 ±1.20. More pulp therapy was performed
for special health care needs children than extensive caries or lacking in cooperative ability children.
This was not statistically significant (p=0.613, ANOVA).
Stainless steel crowns
46 stainless steel crowns were placed with a mean of 0.49±0.91 for the 92 children. The use of
stainless steel crowns was nearly the same for lacking in cooperative ability children and children with
extensive caries and special health care needs (mean of 0.51, 0.50 and 0.48 respectively).

11
Extraction
A total of 352 extractions were done with a mean of 3.74 for total subjects; 335 (95.2%) deciduous
teeth and 17 (4.8%) permanent teeth. The mean of deciduous and permanent teeth extractions was 3.56
and 0.18 respectively, with a mean of 3.24 for lacking in cooperative ability children, 4.46 for children
with extensive caries, 4.07 for special health care needs and 1.00 for surgical procedures.
Total treatments
A total of 1030 dental treatments were recorded for 92 patients with a mean of 10.96±4.05. For lacking
in cooperative ability children a total of 412 procedures, with a mean of 10.05±3.74 were recorded.
For young children with extensive caries a total of 278 procedures with a mean of 11.58±3.81 were
recorded. For special health care needs children a total of 338 dental procedures with a mean of
12.52±3.52 were recorded. Two children had surgical extraction of supernumerary teeth. There was a
statistically significant relation between total treatments and different indications for children under
GA (p<0.001, ANOVA).
Patterns of dental treatment and medical status
The mean number of different dental procedures for children according to medical status is shown in
(Table VI). The mean number for total procedures for special health care needs children was 12.52
while it was 10.33 for healthy group with significant difference between both groups (p=0.017). The
mean number for extractions for both groups was 4.07 and 3.61 respectively with no significant
difference between both groups (p=0.495). The relation between the sum of all dental procedures and
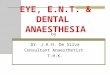
their frequency is shown in figure 1. Eleven children had a total of 10 dental procedures. There was a
range between 1 to 20 dental procedures under GA. Two children had a single dental procedure while
one child had a total of 20 procedures.

11
Discussion
The aims of this study were to determine the characteristics of children attending for treatment under
GA, to investigate the different indications for dental treatment of children under GA and to study the
mean numbers of dental procedures performed under GA with regard to age groups, different
indications and medical condition at KHMC in Jordan. This study demonstrates that the majority of
children undergoing dental treatment under GA were of the very young age group (2-5) years which
agreed with some studies (3, 17)
, but disagreed with others (4)
. The finding of more boys than girls in our
study is consistent with the findings in several other studies (18, 4)
but in contrast to findings of others (1,
12). Some studies have shown that in young age groups there is a male predominance and in the older
age groups there is a female predominance (4)
.
In our study the most common indication for dental treatment of children under GA was behaviour
management problem, which coincides with other studies from Jordan (19)
, or other countries (7,3)
while
in another study (6)
the most common reason for referral for GA was the need for multiple extraction.
Our findings demonstrated that (27.2%) of our patients were special health care needs children. A high
standard of care can be provided to mentally and physically disabled patients using GA, which is not
possible in the dental chair (20)
. The study showed that special health care needs children had
immediate priority to receiving dental care. As mentioned previously GA is never without a risk (9)
,
and in the United Kingdom National Guidelines in Paediatric Dentistry it has been stated that: Once a
decision has been made to use GA, it should be explained to the parents that the anaesthetic is not
administered by a dentist, but by an anaesthetic consultant who has undergone specialist training in
paediatric anaesthesia. It should also be explained that the procedure will take place in an operating
theatre, with a team trained in the care of children. The potentially serious nature of the procedure
should be clearly explained to the parents and, where appropriate, the patient (13)
. So alternative
methods for GA used to provide dental treatment, such as inhalation sedation (21)
, should be kept for
consideration in some cases particularly in older children.
Details of different dental procedures provided in this study with regard to age groups showed that

12
in all age groups more teeth were restored than extracted. In our study the mean number of teeth
restored per child was 5.82. This includes fissure sealants, composites, glass ionomer cements and
amalgam restorations. This number is higher than other studies (7, 8)
but lower than others (4)
. This may
reflect not only that parents are stimulated to seek care at an early stage to conserve teeth (many of
them expressed their desire for the avoidance of extraction), but may also indicate the importance of
prevention and behaviour shaping if further treatment is required that it may be accepted in the normal
way rather than necessitating GA. Extractions were more limited in number and carried out for a
smaller proportion of children than in the past. This may be a result of a more conservative approach
by professionals of the dental services at KHMC. In the present study extractions were carried out for
both primary and permanent teeth. The mean of deciduous and permanent teeth extractions was 3.56
and 0.18 respectively. This result is greater for the primary teeth but less for the permanent teeth in
other studies (12)
.
In this study, 25 (27.2%) patients were special health care needs, while 67 (72.8%) were healthy and
this finding agrees with other studies (7, 22)
. In comparing the means for different dental procedures
between special health care needs and healthy subjects it was found that, the operative procedures,
extractions and total dental treatments were more in special health care needs, with statistical
difference with regard to operative procedures and total treatments but not with regard to extractions.
These results agree with some studies (2,8)
but disagree with results found by Ibricevic et al in their
study in Kuwait, who reported more total dental procedures for normal group, whether intracoronal
restorations, pulpotomies, stainless steel crowns or even extractions than in special needs patients (23)
.
Instructions for home prevention and recall visit one week after GA were given to parents before
discharging the patient. A six month follow-up was also given after a one week review. The findings
of this study indicated a high percentage of children 76 (81%) returned for the post-operative dental
care after one week. However, for recall visits after 6 months the rates were 31(32.9%) only. This poor
attendance for patients for recall visits after GA has been reported in other studies (23, 24)
. A report by
Ibricevic et al, on recall after three years, a total of 10% of patients returned for recall visits once
treatment was completed (23)
. It may be that parents do not consider the need for dental visits after

13
treatment is completed since the child no longer suffers from pain (7)
. Preventive measures by
protecting the sound occlusal surfaces of both primary and permanent teeth with fissure sealants were
undertaken in the majority of cases. Beside its clinical advantages, an important advantage of dental
treatment using day stay GA is that all necessary treatment is carried out in one session, a factor that
may contribute to the acceptability to both parent and patients (2)
. The study showed sick children had
immediate priority to receive dental care. The present study revealed dental care received under GA
included both restorations as well as extractions. In the present study more teeth were restored than
extracted and that was true for both primary and permanent teeth. All non vital or abscessed teeth were
extracted since procedures with doubtful prognosis were avoided especially in special health care
needs patients. This policy indicates a radical approach to treatment planning in order to avoid the
need for further GA (25)
. Other methods to provide treatment would have been possible in some cases,
but this would have needed a large number of dental visits to complete the treatment; therefore GA
was an attractive option for some families to receive treatment in a single visit. This is in agreement
with other studies (2, 20)
. After treatment in day stay facilities, patients received regular appointments at
the outpatient dental clinic. Repeated oral hygiene is emphasized; the oral condition is examined
thoroughly. Empathy that must develop between dentist and child should prepare the patients to cope
with further treatment under local anaesthesia in a conventional office environment.

14
Conclusions
Although most children can be successfully treated in the dental office, there is a group of
paediatric patients, who require dental treatment in the hospital, under GA. It appears that dental
treatment under GA in day care facilities at KHMC proved to be an effective and efficient way of
providing dental treatment. Complete oral rehabilitation was provided under GA at a single visit, for
children who are too young with extreme fear of dental treatment, special health care needs patients,
and for those with extensive treatment need.

15
References
1. Vinckier F, Gizani S, Declerck D. Comprehensive dental care for children with rampant caries
under general anesthesia. Int J Paediatr Dent 2001; 11:25-32
2. Holt RD, Chidiac RH, Rule DC. Dental treatment for children under general anesthesia in day care
facilities at a London dental hospital. Br Dent J 1991; 170: 262-266.
3. Bello LL. A Retrospective study of pediatric dental patients treated under general anesthesia. Saudi
Dent J 2000; 12: 10-15.
4. Jamjoom MM, AL-Malik MI, HOLT RD, et al. Dental treatment under general anaesthesia at a
hospital in Jeddah, Saudi Arabia. Int J Paediatr Dent 2001; 11: 110-116.
5. Harrison MG, Roberts GJ. Comprehensive dental treatment of healthy and chronically sick
children under intubation general anaesthesia during a 5-year period. Br Dent J 1998; 184: 503 – 506.
6. Maccormac C, Kinirons M. Reasons for referral of children to a general anaesthetic
service in Northern Ireland. Int J Paediatr Dent 1998; 8: 191-196.
7. Al-Malik MI, Al-Sarheed MA. Comprehensive Dental Care of Pediatric Patients Treated Under
General Anesthesia in a Hospital Setting in Saudia Arabia. The J of Contemp Dent Pract 2006; 7: 1-9.
8. Holt RD, Rule DC, Davenport ES, et al. The use of general anesthesia for tooth extraction in
children in London: a multi-centre study. Br Dent J 1992; 173: 333-339.
9. Tyrer GL. Referrals for dental general anaesthetics—how many really need GA? Br Dent J 1999;
187(8): 440-443.
10. Jameson K, Averley PA,
Shackley P, et al. A comparison of the ‘cost per child treated’ at a
primary care-based sedation referral service, compared to a general anaesthetic in hospital. Br Dent J
2007; 203: 1-6.
11. Enever GR, Nunn JH, Sheehan JK. A comparison of postoperative morbidity following
outpatient dental care under general anaesthesia in paediatric patients with and without disabilities. Int
J Paediatr Dent 2000; 10:120-5.
12. Atan S, Ashley P, Gilthorpe MS, et al. Morbidity following dental treatment of children under
intubation general anaesthesia in a day-stay unit. Int J Paediatr Dent 2004; 14: 9–16.

16
13. Davies C, Harrison M, Roberts G. Guideline for the Use of General Anaesthesia (GA) in
Paediatric Dentistry. UK National Clinical Guidelines in Paediatric Dentistry 2008; May: 1-11.
14. Tochel C, Hosey M, Macpherson L, et al. Assessment of children prior to dental extractions
under general anaesthesia in Scotland. Br Dent J 2004; 196: 629-633.
15. Hamdan MA. Caries experience among 6 and 12 year-old school children in Jordan. Dirasat,
Medical and Biological Sciences 1997; 24 (2): 112-121.
16. Rajab LD, Hamdan MAM. Early childhood caries and risk factors in Jordan.
Com dent health 2002; 19: 224-229.
17. Jamieson LM, Thomson KF. Dental general anaesthetic trends among Australian children. BMC
Oral Health 2006; 6 (16): 1-7.
18.Vermeulen M, Vinckier F, Vandenbroucke J. Dental general anesthesia: clinical
characteristics of 933 patients. ASDC J Dent Child 1991; 58(1): 27-30.
19. Rajab LD. Paediatric dental general anaesthesia: Clinical Evaluation of Day-Stay Care Patients at
The Jordan University Hospital. Alexandria Dent J 1996; 21: 85-96.
20. Bohaty B, Spencer P. Trends in dental treatment rendered under general anesthesia, 1978 to
1990. J Clin Pediatr Dent 1992; 16: 222-4.
21. Averley PA, Girdler NM, Bond S et al. A randomised controlled trial of paediatric conscious
sedation for dental treatment using intravenous midazolam combined with inhaled nitrous oxide or
nitrous oxide⁄sevoflurane. Anaesthesia 2004; 59: 844–852.
22. Tsai CL, Tsai1 YL, Lin YT, et al. A Retrospective Study of Dental Treatment under General
Anesthesia of Children with or without a Chronic Illness and/or a Disability. Chang Gung Med J 2006;
29: 412-8.
23. Ibricevic H, Al-Jame Q, Honkala S. Pediatric dental procedures under general anesthesia at
the Amiri Hospital in Kuwait. J Clin Pediatr Dent 2001; 25: 337-42.
24. Berkowitz RJ, Billings RJ, Weinstein P. Clinical outcomes for nursing caries treated
under general anesthesia. J Dent Child 1997; 64: 210-211.
25. Mason C, Holt RD, Rule DC. The changing pattern of day-care treatment

17
for children in a London dental teaching hospital. Br Dent J 1995; 179(4): 136-140.

18
Table I. Frequency distributions and percentages of child dental patients treated under GA
according to age groups and gender.
Age group
Gender Total number (%)
Males (%) Females (%)
2-5 y 28 (30.4%) 22 (23.9%) 50 (54.3%)
6-9 y 26 (28.3%) 11 (11.9%) 37 (40.2%)
9-14 y 2 (2.2%) 3 (3.3%) 5 (5.4%)
Total 56 (60.9%) 36 (39.1%) 92 (100.0%)

19
Table II. Indications for treatment under GA for 92 patients and row percentages
according to different age groups.
Indications
Age group
Total (%) 2-5 years
N (row %)
6-9 years
N (row %)
9-14 years
N (row %)
Behavior management problem 13 (31.7%) 26 (63.4%) 2 (4.9%) 41 (44.6%)
Extensive caries and young child 23 (95.8%) 1 (4.2%) 0 (0.0%) 24 (26.1%)
Special health care needs patients 14 (56.0%) 8 (32.0%) 3 (12.0%) 25(27.2%)
Surgical procedures 0 (0.0%) 2 (100.0%) 0 (0.0%) 2 (2.2%)
Total 50 (54.3%) 37 (40.2%) 5 (5.4%) 92 (100.0%)

21
Table III. Diagnosis of special health care needs patients treated under GA
Types of Special health care needs patients N (%)
Physically handicapped 9 (36.0%)
Mentally handicapped 7 (28.0%)
Heart diseases 3 (12.0%)
Blood disorders 2 (8.0%)
Developmental defects 3 (12.0%)
Autism 1 (4.0%)
Total 25 (100.0%)

21
Table IV. Different dental procedures according to age groups
Frequency
Mean ±SD (a)
(a) Standard deviation
(b) One way analysis of variance
Variable
Age in years
p-value (b) 2-5
n=50
6-9
n=37
9-14
n=5
Total
N=92
Fissure
sealants
34
0.68±1.29
70
1.89±2.60
19
2.71±4.03
123
1.31±2.24
0.009
Composite
restorations
119
2.38±2.87
68
1.84±2.13
30
4.29±4.27
217
2.31±2.77
0.096
Glass
ionomer
cements
48
0.96±1.81
34
0.92±1.57
7
1.00±1.53
89
0.95±1.68
0.990
Amalgam
Restorations
67
1.34±1.66
43
1.16±1.57
8
1.14±1.46
118
1.26±1.60
0.863
Total
Restorations
268
5.36±3.19
215
5.81±3.64
64
9.14±4.45
547
5.82±3.57
0.009
Pulp
therapy
60
1.20±1.28
27
0.73±1.10
1
0.14±0.38
88
0.94±1.20
0.035
Stainless
steel crowns
37
0.74±1.07
9
0.24±0.64
0
0.00±0.00
46
0.49±0.91
0.013
Extractions
198
3.96±2.96
135
3.65±2.99
19
2.71±2.81
352
3.74±2.95
0.565
Total
treatments
562
11.24±3.83
384
10.38±4.39
84
12.00±3.83
1030
10.96±4.04
0.486

22
Table V. Different dental procedures according to indications of GA.
Frequency
Mean ±SD (a)
Procedures
Lacking in
cooperative
ability
children
n=41
Extensive
caries
n=24
Special health
care needs
n=25
Surgical
procedure
n=2
Total
N=92
P value
(b)
Fissure sealants
64
1.56±2.44
24
1.00±1.67
35
1.30±2.46
0
0.00±0.00
123
1.31±2.24
0.654
Composite
restorations
75
1.83±2.40
60
2.50±2.89
82
3.04±3.14
0
0.00±0.00
217
2.31±2.77
0.205
Glass ionomer
cements
35
0.85±1.28
29
1.21±2.19
25
0.93±1.80
0
.00±0.00
89
0.95±1.68
0.725
Amalgam
restorations
49
1.20±1.59
23
0.96±1.37
46
1.70±1.80
0
.00±0.00
118
1.26±1.60
0.238
Sum of restorations
(operative dentistry)
223
5.44±3.41
136
5.67±3.12
188
6.96±3.85
0
0.00±0.00
547
5.82±3.57
0.743
Pulp therapies
35
0.85±1.20
24
1.00±1.18
29
1.07±1.27
0
.00±0.00
88
0.94±1.20
0.613
Stainless steel
crowns
21
0.51±0.87
12
0.50±0.86
13
0.48±1.05
0
.00±0.00
46
0.49±0.91
0.898
Extractions
133
3.24±2.95
107
4.46±3.08
110
4.07±2.80
2
1.00±0.00
352
3.74±2.95
0.200
Total treatments 412
10.05±3.74
278
11.58±3.81
338
12.52±3.52
2
1.00±0.00
1030
10.96±4.05
0.000
(a) Standard deviation
(b) One way analysis of variance

23
Table VI. Different dental procedures according to medical status (mean ±SD (a)
)
Dental
Procedure
Special health care
needs group
N= 25
Healthy group
N= 67
P value (b)
Operative dentistry 6.96±3.85 5.36±3.37 0.048
Pulp therapy 1.07±1.27 0.88±1.18 0.482
Stainless steel crowns 0.48±1.05 0.49±0.86 0.958
Extractions 4.07±2.8 3.61±3.02 0.495
Total dental treatments 12.52±3.52 10.33±4.10 0.017
(a) Standard deviation
(b) Independent samples T-test

24
Figure1. A histogram comparing the total number of dental
procedures with their frequency.
Total number of restored and extracted teeth
25 20 15 10 5 0
Frequency
12
10
8
6
4
2
0
Mean =10.96 Std. Dev. =4.048
N =92