Embed Size (px)
Citation preview

© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
1
American Academy of Neurology American Geriatrics Society
American Medical Directors Association American Psychiatric Association
Physician Consortium for Performance Improvement® (PCPI™)
Dementia
Performance Measurement Set
PCPI Approved October 2011

© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
2
Table of Contents Executive Summary………………………………………………………………...……………………………………………….. 5
Purpose of Measurement Set………………………………………………………………...…………………………………… 9
Importance of Topic………………………………………………………………...……………………………………………… 9
Opportunity for Improvement………………………………………………………………...…………………………………. 10
Clinical Evidence Base………………………………………………………………...……………………………………………. 11
Dementia Outcomes………………………………………………………………...……………………………………………… 11
Intended Audience, Care Setting, and Patient Population………………………………………………………………...... 12
Dementia Work Group Recommendations………..………………………………………………………………................... 12
Other Potential Measures………………………………………………………………………………………………………….. 13
Measure Harmonization…………………………………………………………………………………………………………… 14
Technical Specifications Overview……………………………………………………………….............................................. 14
Testing and Implementation of the Measurement Set………………………………………………………………............ 14
Measure #1: Staging of Dementia………………………………………………………………............................................... 15
Measure #2: Cognitive Assessment………………………………………………………………............................................ 17
Measure #3: Functional Status Assessment………………………………………………………………............................. 19
Measure #4: Neuropsychiatric Symptom Assessment……………………………………………………………………… 21
Measure #5: Management of Neuropsychiatric Symptoms………………………………………………………………... 24
Measure #6: Screening for Depressive Symptoms……………………………………………………………….................. 27
Measure #7: Counseling Regarding Safety Concerns……………………………………………………………………….. 29
Measure #8: Counseling regarding Risks of Driving………………………………………………………………………... 31
Measure #9: Palliative Care Counseling and Advance Care Planning…………………………………………………… 33
Measure #10: Caregiver Education and Support…………………………………………………………………………….. 36
Evidence Classification/Rating Schemes……………………………………………………………………………………….. 38
Summary of Non-Material Interest Disclosures………………………………………………………………………………. 40
References………………………………………………………………………………………………………..…………………… 41
Dementia: Administrative Claims Specifications……………………………………………………………….................... Appendix A

© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
3
Physician Performance Measures (Measures) and related data specifications, developed by the Physician Consortium for Performance Improvement® (PCPI™), are intended to facilitate quality improvement activities by physicians. These Measures are intended to assist physicians in enhancing quality of care. Measures are designed for use by any physician who manages the care of a patient for a specific condition or for prevention. These performance Measures are not clinical guidelines and do not establish a standard of medical care. The PCPI has not tested its Measures for all potential applications. The PCPI encourages the testing and evaluation of its Measures. Measures are subject to review and may be revised or rescinded at any time by the PCPI. The Measures may not be altered without the prior written approval of the PCPI. Measures developed by the PCPI, while copyrighted, can be reproduced and distributed, without modification, for noncommercial purposes, e.g., use by health care providers in connection with their practices. Commercial use is defined as the sale, license, or distribution of the Measures for commercial gain, or incorporation of the Measures into a product or service that is sold, licensed or distributed for commercial gain. Commercial uses of the Measures require a license agreement between the user and American Medical Association, on behalf of the PCPI. Neither the PCPI nor its members shall be responsible for any use of these Measures. THE MEASURES AND SPECIFICATIONS ARE PROVIDED "AS IS" WITHOUT WARRANTY OF ANY KIND. © 2011 American Medical Association. All Rights Reserved Limited proprietary coding is contained in the Measure specifications for convenience. Users of the proprietary code sets should obtain all necessary licenses from the owners of these code sets. The AMA, the Consortium and its members disclaim all liability for use or accuracy of any Current Procedural Terminology (CPT®) or other coding contained in the specifications. CPT® contained in the Measures specifications is copyright 2009 American Medical Association. LOINC® copyright 2004 Regenstrief Institute, Inc. SNOMED CLINICAL TERMS (SNOMED CT®) copyright 2004 College of American Pathologists (CAP). All Rights Reserved. Use of SNOMED CT® is only authorized within the United States.

© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
4
Work Group Members Dementia
Work Group Members
Jerry C. Johnson, MD (Co-Chair) (geriatric medicine) Germaine Odenheimer, MD (Co-Chair) (neurology)
François Boller, MD, PhD, FAAN (neurology) Haydee Muse, MD (health plan representative) Soo Borson, MD (geriatric psychiatry) Bruce E. Robinson, MD, MPH (geriatric medicine) Charles A. Cefalu, MD, MS (geriatric medicine) Robert Paul Roca, MD, MPH, MBA (geriatric psychiatry) Mirean Coleman, MSW, LICSW, CT (social work) Amy E. Sanders, MD (geriatric neurology) Patricia C. Davis, MD, MBA, FACR (radiology) Jason E. Schillerstrom, MD (geriatric psychiatry) Mary Ann Forciea, MD (internal/geriatric medicine)
Joseph W. Shega, MD (geriatric medicine, hospice and palliative medicine)
Elizabeth M. Galik, PhD, CRNP (nursing) Eric G. Tangalos, MD, FACP, AGSF, CMD (internal/geriatric medicine)
Laura N. Gitlin, PhD (occupational therapy) Joan M. Teno, MD, MS (internal medicine) Helen H. Kyomen, MD, MS (geriatric and adult psychiatry)
Brian K. Unwin, MD, FAAFP (family medicine)
Katie Maslow, MSW (patient advocacy representative)
John Robert Absher, MD (neurology) -- Liaison to American Academy of Neurology’s Quality Measurement
and Reporting Subcommittee
Work Group Staff
American Academy of Neurology Gina K. Gjorvad Rebecca J. Swain-Eng, MS American Geriatrics Society Caitlin Connolly Susan Sherman
American Medical Directors Association Jill S. Epstein, MA Jacqueline Vance, RNC, CDONA/LTC American Psychiatric Association Robert M. Plovnick, MD, MS
American Medical Association (AMA) Mark Antman, DDS, MBA Christopher Carlucci, MBA Victoria Fils, EdD, MPH Kendra Hanley, MS Karen Kmetik, PhD Stephanie Moncada, MS Pamela O’Neil, MPH David Marc Small, MS, MPP Samantha Tierney, MPH

Executive Summary: Toward Improving Outcomes for Patients with Dementia
© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
5
The American Academy of Neurology (AAN), American Geriatrics Society (AGS), American Medical Directors Association (AMDA), American Psychiatric Association (APA), and Physician Consortium for Performance Improvement® (PCPI™) formed a Dementia Work Group to identify and define quality measures toward improving outcomes for patients with dementia (see diagram at the end of this section). The Work Group focused on measures that would be applicable to patients with an established diagnosis of dementia. As a result, the measures primarily target underemphasized aspects of the evaluation and management of dementia patients. Reasons for Prioritizing Improvement in Dementia High Impact Topic Area Dementia is a chronic condition that poses a major and growing threat to the public’s health. Improving the effectiveness of care and optimizing patient outcomes will become increasingly important as the population of the United States ages. Dementia affects approximately 5%–8% of individuals over age 65 years, 15%–20% of individuals over age 75
years, and 25%–50% of individuals over age 85 years.1 Currently, an estimated 5.3 million Americans of all ages have Alzheimer’s disease – the most common form
of dementia.2 More than 20 percent of women and approximately 17 percent of men reaching the age of 65 would
ultimately develop dementia (estimated lifetime risk).2 Alzheimer’s disease was the sixth-leading cause of death across all ages in the United States in 2007.3 It was
the fifth-leading cause of death for those aged 65 and older in 2006.2 People with Alzheimer’s disease and other dementias have more than three times as many hospital stays as
other older people.2 At any one time, about one-quarter of all hospital patients aged 65 and older are people with Alzheimer’s
and other dementias.1 In 2009, almost 11 million family members, friends and neighbors provided 12.5 billion hours of unpaid care
for a person with Alzheimer’s disease or other dementias. This number represents an average of 21.9 hours of care per caregiver per week, or 1,139 hours of care per caregiver per year.2
The total estimated worldwide costs of dementia are $604 billion in 2010, accounting for around 1% of the world’s gross domestic product.4
In 2005, the direct costs to Medicare and Medicaid for care for people with Alzheimer’s and other dementias and the estimated indirect costs to businesses for employees who were caregivers of people with Alzheimer’s and other dementias amounted to more than $148 billion.1
Demonstrated Opportunity for Improvement According to a study analyzing the quality of medical care provided to vulnerable community-dwelling older
patients, quality of care for geriatric conditions (eg, dementia, urinary incontinence) was found to be poorer than care for general medical conditions (eg, diabetes, heart failure). On average, patients with dementia received the recommended quality of care only about 35 percent of the time.5
Chodosh and colleagues found that current practice patterns indicate a significant opportunity for improvement in the quality of dementia care with a majority (11 of 18) of guideline-recommended dementia care processes having less than 40% adherence.6
Another study identified considerable variability across sites in the routine implementation of recommended practices for the assessment, management and treatment of patients with dementia.7
Disparities A recent systematic review and meta-analysis of the use of dementia treatment, care, and research identified
significant racial and ethnic disparities in western countries, particularly the United States. Overall, the authors found “consistent evidence, mostly from the United States, that [minority ethnic] people accessed diagnostic services later in their illness, and once they received a diagnosis, were less likely to access antidementia medication, research trials, and 24-hour care.”8
Rigorous Clinical Evidence Base Evidence-based clinical practice guidelines are available for the management of dementia. This measurement set is based on guidelines from: American Academy of Neurology American Medical Directors Association American Psychiatric Association

Executive Summary: Toward Improving Outcomes for Patients with Dementia
© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
6
California Workgroup on Guidelines for Alzheimer’s Disease Management Third Canadian Consensus Conference on the Diagnosis and Treatment of Dementia Dementia Outcomes Ideally, a set of performance measures would include both measures of outcomes as well as measures of processes that are known to positively influence desirable outcomes. The development of outcome measures for dementia proved particularly challenging given the frequently progressive nature of the syndrome and the paucity of interventions available to change its course. In light of these difficulties, the Work Group set out to develop performance measures based on processes that are associated with desired outcomes and reflect high quality care. Desired outcomes for dementia include:
1. Delay cognitive decline 2. Attain and maintain the highest practicable level of personal functioning 3. Decrease the severity and frequency of neuropsychiatric symptoms 4. Delay institutionalization of the patient 5. Promote caregiver and patient-centered decision-making 6. Reduce caregiver stress and burden 7. Enhance caregiver knowledge of and comfort with dementia care
Dementia Work Group Recommendations Process measures: Several processes of care, demonstrated to improve outcomes for dementia patients, are recommended:
Measures addressing underuse of effective services (evaluation and treatment strategies) Measure #1: Staging of Dementia Measure #2: Cognitive Assessment Measure #3: Functional Status Assessment Measure #4: Neuropsychiatric Symptom Assessment Measure #5: Management of Neuropsychiatric Symptoms Measure #6: Screening for Depressive Symptoms Measures addressing safety Measure #7: Counseling regarding Safety Concerns Measure #8: Counseling regarding Risks of Driving Measures addressing underuse of patient-centered care strategies Measure #9: Palliative Care Counseling and Advance Care Planning Measure #10: Caregiver Education and Support
These clinical performance measures are designed for practitioner level quality improvement to achieve better outcomes for patients with dementia. Unless otherwise indicated, the measures are also appropriate for accountability if the appropriate methodological, statistical, and implementation rules are achieved. Other Potential Measures The Work Group considered several other potential measures, though ultimately determined that they were not appropriate for inclusion in the measure set. Measure Harmonization When existing hospital-level or plan-level measures are available for the same measurement topics, the PCPI attempts to harmonize the measures to the extent feasible. Technical Specifications Overview There are several data sources available for collecting performance measures; generally different data sources require different sets of measure specifications, due to the structure of the systems storing the data. The PCPI recognizes that Electronic Health Records (EHRs) are the state of the art for clinical encounters and is focusing significant resources and expertise toward specifying and testing measures within EHRs, as they hold the

Executive Summary: Toward Improving Outcomes for Patients with Dementia
© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
7
promise of providing the relevant clinical data for measures and for providing feedback to physicians and other health care providers that is timely and actionable. The PCPI develops technical specifications for multiple data sources, including:
EHR Data Electronic Administrative Data (Claims)
o Prospective Claims-based reporting (using CPT Category II codes) o Retrospective Claims Analysis
Expanded (multiple-source) Administrative Data Paper Medical Record/Retrospective Data Collection Flow Sheet
Because administrative claims are currently available sources of data, specifications to collect and report on the Dementia measures for administrative claims are included in this document. In light of recent national initiatives to encourage physicians and other health care professionals to adopt EHRs in their practices, the PCPI advocates that performance measures be integrated into EHR systems so that data for measurement and improvement are part of the fabric of care. EHRs also may be the source for external reporting. One venue for advancing this work is the AMA/National Committee for Quality Assurance (NCQA)/Healthcare Information and Management Systems Society (HIMSS) Electronic Health Record Association (EHRA) Collaborative (see www.ama-assn.org/go/collaborative). Additional detailed information regarding PCPI Specifications Methodology, including measure exceptions, is included in the Technical Specifications section of this document. Testing and Implementation of the Measurement Set The measures in the set are being made available without any prior testing. The PCPI will welcome the opportunity to promote the initial testing of these measures and to ensure that any results available from testing are used to refine the measures before implementation.

Executive Summary: Toward Improving Outcomes for Patients with Dementia
8
Link to Outcomes:
The proposed measures focus on accurate and appropriate evaluation and monitoring of disease status and associated symptoms to guide treatment, effective therapeutic options in eligible patients, enhancing patient safety and the avoidance of adverse events, increasing patient and caregiver awareness of advance planning, and easing patient and caregiver burden by referring them to additional sources for support.

© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association 9
Purpose of Measurement Set:
The American Academy of Neurology (AAN), American Geriatrics Society (AGS), American Medical Directors Association (AMDA), American Psychiatric Association (APA), and Physician Consortium for Performance Improvement® (PCPI) formed a Dementia Work Group to identify and define quality measures toward improving outcomes for patients with dementia. The Work Group aimed to develop a comprehensive set of measures that support the efficient delivery of high quality health care in each of the Institute of Medicine’s (IOM) six aims for quality improvement (safe, effective, patient centered, timely, efficient, and equitable).9 The Work Group was tasked with developing measures that reflect the most rigorous clinical evidence and address areas most in need of performance improvement. The Work Group considered opportunities for outcome, process and structural measures as well as composite, bundled and group or system-level measures. The Work Group focused on measures that would be applicable to patients with an established diagnosis of dementia. As a result, the measures primarily target underemphasized aspects of the evaluation and management of dementia patients. Although the Work Group recognizes that diagnostic accuracy is the prerequisite for optimal therapy10, it is beyond the scope of the measure set and difficult to operationalize in performance measurement. The measures are developed and to be implemented based on the assumption that diagnosis of dementia is accurate and was established in accordance with evidence-based diagnostic criteria.
Importance of Topic
Prevalence and Incidence: Dementia affects approximately 5%–8% of individuals over age 65 years, 15%–20% of individuals over age 75
years, and 25%–50% of individuals over age 85 years.1 Alzheimer’s disease is the most common form of dementia, accounting for 60 to 80 percent of cases.1 One in eight persons aged 65 and older (13%) have Alzheimer’s disease.2 Currently, an estimated 5.3 million Americans of all ages have Alzheimer’s disease.2 The number of people aged 65 and older with Alzheimer’s disease is estimated to reach 7.7 million in 2030,
more than a 50 percent increase from current estimates. By 2050, the number of individuals aged 65 and older with Alzheimer’s is projected to number between 11 million and 16 million.1
In 2000, there were an estimated 411,000 incident cases of Alzheimer’s disease. By 2010, that number is
expected to increase to 454,000 new cases per year; and by 2050, to 959,000.2 Every 70 seconds, someone in America develops Alzheimer’s disease. By mid-century, someone will develop
Alzheimer’s every 33 seconds.2 More than 20 percent of women reaching the age of 65 would ultimately develop dementia (estimated
lifetime risk), compared to approximately 17 percent of men.1 For women, at age 65, the short-term risk for developing dementia over the next 10 years is approximately 1
percent. However, at age 75, for women, the risk of developing dementia over the next 10 years jumps more than sevenfold, and at 85, the risk skyrockets to 20-fold. The risk scenario for men follows a similar trajectory.1
Mortality: Alzheimer’s disease was the sixth-leading cause of death across all ages in the United States in 2007.3 It was
the fifth-leading cause of death for those aged 65 and older in 2006.2 While the total number of deaths attributed to other major causes of deaths has been decreasing, those due
to Alzheimer’s have continued to increase. Comparing changes in selected causes of death between 2000 and 2006, deaths attributed to Alzheimer’s disease increased 47.1 percent, while those attributed to the number one cause of death, heart disease, decreased 11.5 percent.1
A study of national death certificates for 2001 found that 66.9 percent of people aged 65 and older who
died of dementia did so in nursing homes. In contrast, 20.6 percent of patients dying from cancer died in nursing homes. Among those dying of other conditions, 28 percent died in nursing homes.1

© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
10
Median survival time for outpatients with Alzheimer’s disease has been found to be largely dependent on
age of onset with estimates ranging from 3.3 to 9.3 years.1 Use of Health Care Resources: People with Alzheimer’s disease and other dementias have more than three times as many hospital stays as
other older people.2 At any one time, about one-quarter of all hospital patients aged 65 and older are people with Alzheimer’s
and other dementias.1 In 2004, Medicare beneficiaries aged 65 and older with Alzheimer’s and other dementias were eight times
more likely than other Medicare beneficiaries in the same age group to have a Medicare-covered stay in a skilled nursing facility (SNF).12
In 2004, one-quarter of Medicare beneficiaries aged 65 and older who received Medicare-covered home
health care services were people with Alzheimer’s and other dementias, about twice as many as one would expect given the proportion of Medicare beneficiaries with Alzheimer’s and other dementias among all Medicare beneficiaries.12
Family Caregiving: The vast majority (87%) of individuals with Alzheimer’s disease are cared for at home by family members.1 In 2009, almost 11 million family members, friends and neighbors provided 12.5 billion hours of unpaid
care for a person with Alzheimer’s disease or other dementias. This number represents an average of 21.9 hours of care per caregiver per week, or 1,139 hours of care per caregiver per year.2
Cost: The total estimated worldwide costs of dementia are $604 billion in 2010, accounting for around 1% of the
world’s gross domestic product.4 - About 70% of the worldwide costs occur in Western Europe and North America.4 - Researchers tentatively estimated an 85% increase in worldwide costs by 2030 (exceeding $1 trillion),
based only on predicted increases in the numbers of people with dementia.4 In 2005, the direct costs to Medicare and Medicaid for care for people with Alzheimer’s and other dementias
and the estimated indirect costs to businesses for employees who were caregivers of people with Alzheimer’s and other dementias amounted to more than $148 billion, including: - $91 billion in Medicare costs for care of beneficiaries with Alzheimer’s and other dementias.1 - $21 billion in state and federal Medicaid costs for nursing home care for people with Alzheimer’s and
other dementias.1 - $36.5 billion in indirect costs to business for employees who are caregivers of people with Alzheimer’s
and other dementias, calculated for 2002 and projected to 2005.1 In 2009, the economic value of the care provided by family and other unpaid caregivers of people with
Alzheimer’s and other dementias was $144 billion.2
Opportunity for Improvement
According to a study analyzing the quality of medical care provided to vulnerable community-dwelling older patients, quality of care for geriatric conditions (eg, dementia, urinary incontinence) was found to be poorer than care for general medical conditions (eg, diabetes, heart failure). On average, patients with dementia received the recommended quality of care only about 35 percent of the time. Vulnerable elders, identified by a 13-item function-based screening survey, are community-dwelling persons 65 years of age and older who have 4 times the risk for functional decline or death over the next 2 years compared with individuals not identified as vulnerable. Quality of care was assessed by clinician performance on nine dementia quality indicators. Quality of care varied significantly by indicator with average rates of adherence ranging from 18% for an assessment of functional status upon admission to a hospital or a new visit to a physician practice (n=130) to 100% for the offering of appropriate stroke prophylaxis for a dementia patient who also has cerebrovascular disease (n=2).5
Chodosh and colleagues aimed to characterize contemporary care patterns for dementia within one U.S.
metropolitan area by analyzing medical records and caregiver surveys for 378 patients. To quantify quality of care, 18 dementia care processes drawn from existing guidelines were assessed. These care processes

© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
11
were aggregated within four care dimensions: assessment (6 processes), treatment (6 processes), education and support (3 processes), and safety (3 processes). Adherence to the 18 individual care processes ranged from 9% to 79%; notably 11 of 18 care processes had less than 40% adherence.6
A study surveying clinicians practicing in 6 VA medical centers aimed to asses the extent to which providers
are following dementia practice guidelines. The investigators identified considerable variability across sites in the routine implementation of recommended practices for the assessment, management and treatment of patients with dementia. Practices for which adherence to clinical practice guidelines was moderate to low included cognitive and depression screening, reporting of elder abuse, discussing care needs and decision-making issues with patients’ family and implementing caregiver support practices.7
Disparities A recent systematic review and meta-analysis of the use of dementia treatment, care, and research identified significant racial and ethnic disparities in western countries, particularly the United States. Overall, the authors found “consistent evidence, mostly from the United States, that [minority ethnic] people accessed diagnostic services later in their illness, and once they received a diagnosis, were less likely to access antidementia medication, research trials, and 24-hour care.”8 Non-Hispanic Blacks with dementia are more likely to be undiagnosed or misdiagnosed relative to non-
Hispanic Whites.”11,12 Anti-dementia medication use was approximately 30% higher among non-Hispanic Whites compared to other
racial/ethnic groups, after adjusting for demographics, socioeconomics, health care access and utilization, comorbidities, and service year.13
“Both non-Hispanic Blacks and Latinos transition to long-term care at more advanced stages of dementia.”14,15 Minority ethnic people with dementia were found to be 40% less likely to enter 24-hour care. This may be due
to choice, cultural preferences or barriers to access8 The PCPI believes that performance measure data should be stratified by race, ethnicity, and primary written and spoken language to assess disparities and initiate subsequent quality improvement activities addressing identified disparities. These categories are consistent with recent national efforts to standardize the collection of race and ethnicity data. A 2008 National Quality Forum (NQF) report endorsed 45 practices including stratification by the aforementioned variables.16 A 2009 Institute of Medicine (IOM) report “recommends collection of the existing Office of Management and Budget (OMB) race and Hispanic ethnicity categories as well as more fine-grained categories of ethnicity (referred to as granular ethnicity and based on one’s ancestry) and language need (a rating of spoken English language proficiency of less than very well and one’s preferred language for health-related encounters).”17
Clinical Evidence Base
Clinical practice guidelines serve as the foundation for the development of performance measures. A number of clinical practice guidelines have been developed for dementia and Alzheimer’s disease, offering a robust evidence base to guide clinical decision-making and performance measure development. Guidelines from the American Academy of Neurology18,19,20, American Psychiatric Association21, American Medical Directors Association22, Third Canadian Consensus Conference on the Diagnosis and Treatment of Dementia23, and a work group that included the Los Angeles chapter of the Alzheimer’s Association24 were reviewed during the measure development process. Additional recommendations from the American Geriatrics Society, American College of Physicians and other groups that focused on specific dimensions in the care of patients with dementia were also considered. Relevant guidelines met all of the required elements and many, if not all, of the preferred elements outlined in a PCPI position statement establishing a framework for consistent and objective selection of clinical practice guidelines from which PCPI Work Groups may derive clinical performance measures.25 Performance measures, however, are not clinical practice guidelines and cannot capture the full spectrum of care for all patients with dementia. The guideline principles with the strongest recommendations and often the highest level of evidence (well-designed randomized-controlled trials) served as the basis for measures in this set.
Dementia Outcomes
Ideally, a set of performance measures would include both measures of outcomes as well as measures of processes that are known to positively influence desirable outcomes. The development of outcome measures

© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
12
for dementia proved particularly challenging given the frequently progressive nature of the syndrome. Additionally, there are no existing interventions to halt progression with current pharmacologic and non-pharmacologic interventions showing only modest improvements, or a slower decline, in cognition and function in a substantial minority of patients.21 The goals of management, particularly for those patients with advanced cognitive impairment, are often focused on improving the quality of life for patients and caregivers, maintaining optimal function and providing maximum comfort.26 In light of these difficulties, the Work Group set out to identify the desired outcomes for dementia with a goal of developing performance measures based on processes that are associated with desired outcomes and reflect high quality care. Desired outcomes for dementia include:
1. Delay cognitive decline 2. Attain and maintain the highest practicable level of personal functioning 3. Decrease the severity and frequency of neuropsychiatric symptoms 4. Delay institutionalization of the patient 5. Promote caregiver and patient-centered decision-making 6. Reduce caregiver stress and burden 7. Enhance caregiver involvement and comfort with dementia care
Intended Audience, Care Setting, and Patient Population
The PCPI encourages use of these measures by physicians and other health care professionals, where appropriate, to manage the care for all patients with dementia, regardless of age.
Dementia Work Group Recommendations
The measurement set includes measures that focus on accurate and appropriate evaluation and monitoring of disease status and associated symptoms to guide treatment, effective therapeutic options in eligible patients, enhancing patient safety and the avoidance of adverse events, increasing patient and caregiver awareness of advance planning, and easing patient and caregiver burden by referring them to additional sources for support. The Dementia Work Group identified several desired outcomes for patients with dementia (see “Link to Outcomes” diagram in preceding section). Current quality gaps in dementia care emphasize the need to improve specific processes that have been demonstrated to improve dementia outcomes (ie, the assessment and monitoring of patients throughout the disease course, safety interventions, and the provision/referral of education and support for caregivers). As a result, many of the measures in the dementia set focus on the provision of effective and patient-centered care. These clinical performance measures are designed for practitioner level quality improvement to achieve better outcomes for patients with dementia. Unless otherwise indicated, the measures are also appropriate for accountability if the appropriate methodological, statistical, and implementation rules are achieved. The measures listed below may be used for quality improvement and accountability.
Measures addressing underuse of effective services (evaluation and treatment strategies) Measure #1: Staging of Dementia Measure #2: Cognitive Assessment Measure #3: Functional Status Assessment Measure #4: Neuropsychiatric Symptom Assessment Measure #5: Management of Neuropsychiatric Symptoms Measure #6: Screening for Depressive Symptoms Measures addressing safety Measure #7: Counseling regarding Safety Concerns Measure #8: Counseling regarding Risks of Driving Measures addressing underuse of patient-centered care strategies Measure #9: Palliative Care Counseling and Advance Care Planning Measure #10: Caregiver Education and Support
Given the continued and progressive impairment in cognition and function over time for dementia patients, family members and other individuals play a pivotal role in care management. We have used the following terms and corresponding definitions throughout the document to describe these individuals. The terms are not mutually exclusive.
Caregivers: “Persons who provide care to those who need supervision or assistance in illness or disability. They may provide the care in the home, in a hospital, or in an institution. Although caregivers include trained

© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
13
medical, nursing, and other health personnel, the concept also refers to parents, spouses, or other family members, friends, members of the clergy, teachers, social workers, fellow patients.”27
Knowledgeable Informants: Knowledgeable informants know and have frequent contact with the patient.28 These measures support the efficient delivery of high quality health care in many of the IOM’s six aims for quality improvement9 as described in the following table:
Effective IOM Domains of Health Care Quality Safe Underuse Overuse
Patient-centered
Timely Efficient Equitable
Measures 1 Staging of Dementia √ √ √ 2 Cognitive Assessment √ √ √ 3 Functional Status Assessment √ √ √ 4 Neuropsychiatric Symptom
Assessment √ √
5 Management of Neuropsychiatric Symptoms
√ √
6 Screening for Depressive Symptoms
√ √
7 Counseling Regarding Safety Concerns
√ √ √
8 Counseling regarding Risks of Driving
√ √ √
9 Palliative Care Counseling and Advance Care Planning √ √ √ √
10 Caregiver Education and Support √ √ √
Other Potential Measures
The Work Group considered several other important constructs in dementia care, though ultimately determined that they were not appropriate as the subject of performance measures. In particular, there was universal agreement among Work Group members that one of the largest problems in dementia care is the inadequate recognition of dementia in clinical practice. Research has shown that a small minority (anywhere between 12-35%) of patients with dementia, Alzheimer’s disease, or cognitive impairment had a diagnosis of the condition in their medical record.29,30,31,32,33 Another study concluded that only 41% of the subjects determined to have dementia by the researchers were recognized as having cognitive impairment by their primary care physician based on a notation in their medical record of any of three things (any cognitive diagnosis, prescription of an anti-dementia medication, and/or a notation that the physician had administered a mental status test and stated that the person’s score was abnormal).34 The identification and detection of dementia clearly represents a significant opportunity for improvement and is vital as the gateway to initiation and engagement in treatment. Despite its importance and the availability of several reliable and valid case detection tools, a number of national and international organizations have stopped short of recommending routine screening for dementia in older adults. However, many of these organizations “did recommend a diagnostic evaluation when memory problems or dementia were suspected.”35 Given the lack of evidence to support routine screening and the inherent difficulty in identifying the population of patients for whom dementia screening is recommended, the Work Group felt that it was premature to move forward with the development of a measure that could address this well documented gap in care. The Work Group considered including the use of cholinesterase inhibitors (CEIs) as a treatment-related performance measure for patients with Alzheimer’s disease or other dementias. While the use of these agents has demonstrated modest improvements in cognition and global assessments in a substantial minority of patients, “uncertainty persists about the clinical relevance of these outcomes (which are not used in routine clinical practice) and the duration of the apparent benefit (the randomized controlled trials reviewed were 12 to 52 weeks in duration, and all but one was 26 weeks or less).”36 Although clinical practice guidelines have appropriately recommended that cholinesterase inhibitors be considered for all patients with mild to moderate Alzheimer’s disease, they have also emphasized the need to base the decision to initiate pharmacotherapy with these agents on individualized assessment after a thorough discussion of their benefits and risks. As a result, the Work Group felt that it would be premature to establish the use of CEIs as a performance measure at this time.
© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
14
While each performance measure is intended to support quality improvement in one or more of the IOM domains (safe, effective, patient centered, timely, efficient, and equitable), the development of measures specifically designed to eliminate overuse of ineffective care and promote efficiency proved more challenging. One significant area of overuse in dementia care includes the use of aggressive and ineffective treatment at the end of life. Given the complexity of these issues and the importance of eliciting and adhering to patient preference, there is no generalizable way to identify patients who may be subject to this overuse. As a result, the direct assessment of these care processes was not feasible within the constructs of performance measurement. Nevertheless, measure #9 in this set may indirectly address these significant concerns in the care of patients with dementia.
Measure Harmonization
When existing hospital-level or plan-level measures are available for the same measurement topics, the PCPI attempts to harmonize the measures to the extent feasible. Apart from the 2001 work of RAND to identify quality indicators for dementia as part of the Assessing Care of Vulnerable Elderly (ACOVE) project37, there remains a paucity of measures to address the quality of dementia care. The ACOVE indicators were reviewed during the measure development process and harmonization was considered, where appropriate.
Technical Specifications Overview
There are several data sources available for collecting performance measures; generally different data sources require different sets of measure specifications, due to the structure of the systems storing the data. The PCPI recognizes that EHRs are the state of the art for clinical encounters and is focusing significant resources and expertise toward specifying and testing measures within EHRs, as they hold the promise of providing the relevant clinical data for measures and for providing feedback to physicians and other health care providers that is timely and actionable. The PCPI develops technical specifications for multiple data sources, including:
EHR Data Electronic Administrative Data (Claims)
o Prospective Claims-based reporting (using CPT Category II codes) o Retrospective Claims Analysis
Expanded (multiple-source) Administrative Data Paper Medical Record/Retrospective Data Collection Flow Sheet
Because administrative claims are currently available sources of data, specifications to collect and report on the Dementia measures for administrative claims are included in this document. In light of recent national initiatives to encourage physicians and other health care professionals to adopt EHRs in their practices, the PCPI advocates that performance measures be integrated into EHR systems so that data for measurement and improvement are part of the fabric of care. EHRs also may be the source for external reporting. One venue for advancing this work is the AMA/NCQA/HIMSS Electronic Health Record Association (EHRA) Collaborative (see www.ama-assn.org/go/collaborative). Additional detailed information regarding PCPI Specifications Methodology, including measure exceptions, is included in the Technical Specifications section of this document.
Testing and Implementation of the Measurement Set
The measures in the set are being made available without any prior testing. The PCPI recognizes the importance of testing all of its measures and encourages testing of the Dementia measurement set for feasibility and reliability by organizations or individuals positioned to do so. The Measure Testing Protocol for PCPI Measures was approved by the PCPI in 2007 and is available on the PCPI web site (see Position Papers at www.physicianconsortium.org); interested parties are encouraged to review this document and to contact PCPI staff. The PCPI will welcome the opportunity to promote the initial testing of these measures and to ensure that any results available from testing are used to refine the measures before implementation.
© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association 15
Measure #1: Staging of Dementia Dementia
Measure Description
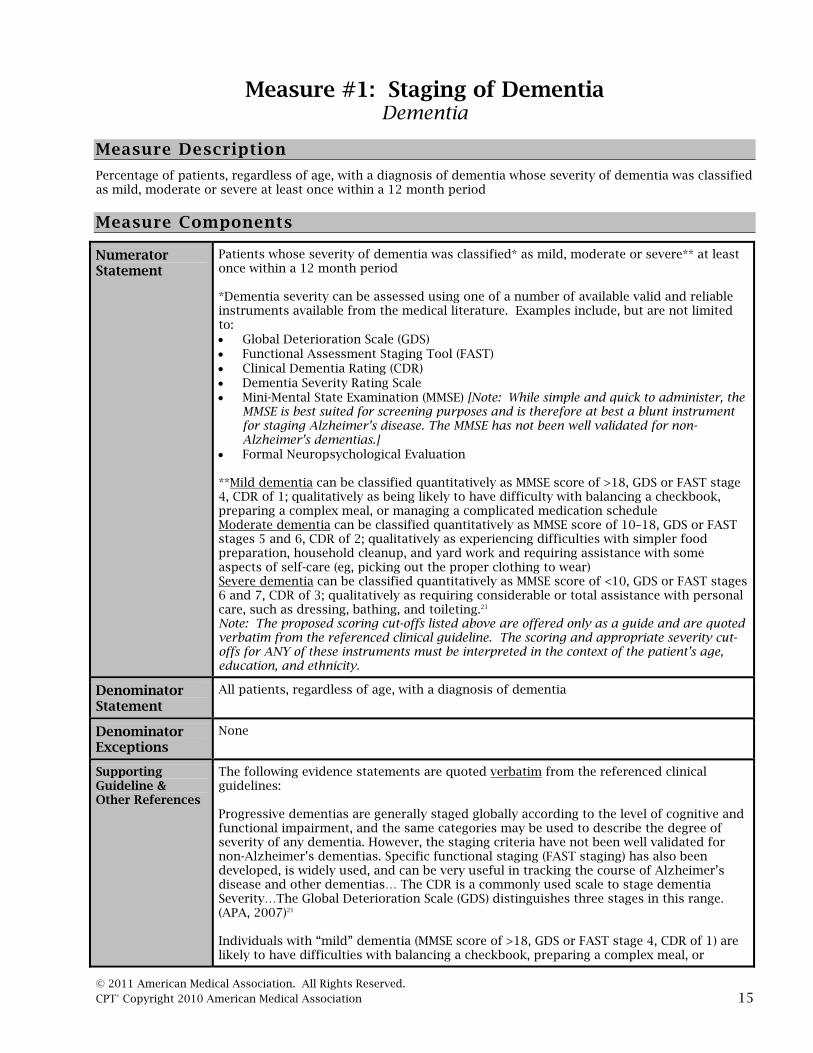
Percentage of patients, regardless of age, with a diagnosis of dementia whose severity of dementia was classified as mild, moderate or severe at least once within a 12 month period
Measure Components
Numerator Statement
Patients whose severity of dementia was classified* as mild, moderate or severe** at least once within a 12 month period *Dementia severity can be assessed using one of a number of available valid and reliable instruments available from the medical literature. Examples include, but are not limited to: Global Deterioration Scale (GDS) Functional Assessment Staging Tool (FAST) Clinical Dementia Rating (CDR) Dementia Severity Rating Scale Mini-Mental State Examination (MMSE) [Note: While simple and quick to administer, the
MMSE is best suited for screening purposes and is therefore at best a blunt instrument for staging Alzheimer’s disease. The MMSE has not been well validated for non-Alzheimer’s dementias.]
Formal Neuropsychological Evaluation **Mild dementia can be classified quantitatively as MMSE score of >18, GDS or FAST stage 4, CDR of 1; qualitatively as being likely to have difficulty with balancing a checkbook, preparing a complex meal, or managing a complicated medication schedule Moderate dementia can be classified quantitatively as MMSE score of 10–18, GDS or FAST stages 5 and 6, CDR of 2; qualitatively as experiencing difficulties with simpler food preparation, household cleanup, and yard work and requiring assistance with some aspects of self-care (eg, picking out the proper clothing to wear) Severe dementia can be classified quantitatively as MMSE score of <10, GDS or FAST stages 6 and 7, CDR of 3; qualitatively as requiring considerable or total assistance with personal care, such as dressing, bathing, and toileting.21 Note: The proposed scoring cut-offs listed above are offered only as a guide and are quoted verbatim from the referenced clinical guideline. The scoring and appropriate severity cut-offs for ANY of these instruments must be interpreted in the context of the patient’s age, education, and ethnicity.
Denominator Statement
All patients, regardless of age, with a diagnosis of dementia
Denominator Exceptions
None
Supporting Guideline & Other References
The following evidence statements are quoted verbatim from the referenced clinical guidelines: Progressive dementias are generally staged globally according to the level of cognitive and functional impairment, and the same categories may be used to describe the degree of severity of any dementia. However, the staging criteria have not been well validated for non-Alzheimer’s dementias. Specific functional staging (FAST staging) has also been developed, is widely used, and can be very useful in tracking the course of Alzheimer’s disease and other dementias… The CDR is a commonly used scale to stage dementia Severity…The Global Deterioration Scale (GDS) distinguishes three stages in this range. (APA, 2007)21 Individuals with “mild” dementia (MMSE score of >18, GDS or FAST stage 4, CDR of 1) are likely to have difficulties with balancing a checkbook, preparing a complex meal, or

© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
16
managing a difficult medication schedule. Those with “moderate” impairment (MMSE score of 10–18, GDS or FAST stages 5 and 6, CDR of 2) also have difficulties with simpler food preparation, household cleanup, and yard work and may require assistance with some aspects of self-care (e.g., picking out the proper clothing to wear). Those whose dementia is “severe” (MMSE score of <10, GDS or FAST stages 6 and 7, CDR of 3) require considerable or total assistance with personal care, such as dressing, bathing, and toileting. Research has shown that measurable cognitive abilities remain throughout the course of severe dementia. In the terminal phase, patients become bed bound, develop contractures, require constant care, and may be susceptible to accidents and infectious diseases, which ultimately prove fatal. (APA, 2007)21
Measure Importance
Relationship to desired outcome
Dementia is characterized by continued and progressive impairment in cognition and function including the evolution of symptoms over time.21 The treatment varies throughout the disease course.21 Patients with dementia, therefore, require assessment of disease severity and subsequent treatment specific and appropriate to their current stage of disease.21 Early stage patients, for example, have special needs and can and should be involved in care planning and referred to community resources.24 Care for late stage patients may focus on improving the quality of life for patients and caregivers, maintaining optimal function and providing maximum comfort.26
Opportunity for Improvement
Assessing a patient’s stage of dementia involves an evaluation of their cognitive and functional status. A 2007 analysis of medical records and caregiver surveys for 378 patients with dementia found that 50% of patients received an assessment of their cognitive status and only 9.5% received an assessment of their activities of daily living in the previous 12 months.6 Similar results were reported in a study analyzing the quality of health care provided to a broader population of vulnerable community-dwelling older patients. Of vulnerable elders admitted to a hospital or new to a physician practice, 52% had documentation of a multidimensional assessment of cognitive ability while only 18% received an assessment of their functional status.5 Another study surveying clinicians practicing in VA medical centers found that only two thirds of clinicians reported regularly performing a standardized assessment of cognitive functioning.7
IOM Domains of Health Care Quality Addressed
Effective Patient-centered
Equitable
Exception Justification
This measure has no exceptions.
Harmonization with Existing Measures
Harmonization with existing measures was not applicable to this measure.
Measure Designation
Measure purpose Quality improvement Accountability
Type of measure Process
Level of Measurement
Individual practitioner
Care setting Ambulatory care Residential (ie, nursing facility, domiciliary, home care)
Data source Electronic health record (EHR) data Administrative Data/Claims (outpatient claims) Administrative Data/Claims Expanded (multiple-source) Paper medical record

© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
17
Measure #2: Cognitive Assessment Dementia
Measure Description
Percentage of patients, regardless of age, with a diagnosis of dementia for whom an assessment of cognition is performed and the results reviewed at least within a 12 month period
Measure Components
Numerator Statement
Patients for whom an assessment of cognition is performed and the results reviewed at least once within a 12 month period *Cognition can be assessed by direct examination of the patient using one of a number of instruments, including several originally developed and validated for screening purposes. This can also include, where appropriate, administration to a knowledgeable informant. Examples include, but are not limited to: Blessed Orientation-Memory-Concentration Test (BOMC) Mini-Cog Montreal Cognitive Assessment (MoCA) Cognitive Abilities Screening Instrument (CASI) St. Louis University Mental Status Examination (SLUMS) Mini-Mental State Examination (MMSE) [Note: The MMSE has not been well validated for
non-Alzheimer’s dementias. Short Informant Questionnaire on Cognitive Decline in the Elderly (IQCODE) Ascertain Dementia 8 (AD8) Questionnaire Minimum Data Set (MDS) Brief Interview of Mental Status (BIMS) [Note: Validated for
use with nursing home patients only] Formal neuropsychological evaluation
Denominator Statement
All patients, regardless of age, with a diagnosis of dementia
Denominator Exceptions
Documentation of medical reason(s) for not assessing cognition (eg, patient with very advanced stage dementia, other medical reason) Documentation of patient reason(s) for not assessing cognition
Supporting Guideline & Other References
The following evidence statements are quoted verbatim from the referenced clinical guidelines: Ongoing assessment includes periodic monitoring of the development and evolution of cognitive and noncognitive psychiatric symptoms and their response to intervention (Category I). Both cognitive and noncognitive neuropsychiatric and behavioral symptoms of dementia tend to evolve over time, so regular monitoring allows detection of new symptoms and adaptation of treatment strategies to current needs…Cognitive symptoms that almost always require assessment include impairments in memory, executive function, language, judgment, and spatial abilities. It is often helpful to track cognitive status with a structured simple examination. (APA, 2007)21 Conduct and document an assessment and monitor changes in cognitive status using a reliable and valid instrument. Cognitive status should be reassessed periodically to identify sudden changes, as well as to monitor the potential beneficial or harmful effects of environmental changes, specific medications, or other interventions. Proper assessment requires the use of a standardized, objective instrument that is relatively easy to use, reliable (with less variability between different assessors), and valid (results that would be similar to gold-standard evaluations). (California Workgroup on Guidelines for Alzheimer’s Disease Management, 2008)24

© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
18
Measure Importance
Relationship to desired outcome
Dementia is often characterized by the gradual onset and continuing cognitive decline in one or more domains including memory, executive function, language, judgment, and spatial abilities.21 Cognitive deterioration represents a major source of morbidity and mortality and poses a significant burden on affected individuals and their caregivers.38 Although cognitive deterioration follows a different course depending on the type of dementia, significant rates of decline have been reported. For example, one study found that the annual rate of decline for Alzheimer’s disease patients was more than four times that of older adults with no cognitive impairment.39 Nevertheless, measurable cognitive abilities remain throughout the course of dementia.21 Initial and ongoing assessments of cognition are fundamental to the proper management of patients with dementia. These assessments serve as the basis for identifying treatment goals, developing a treatment plan, monitoring the effects of treatment, and modifying treatment as appropriate.
Opportunity for Improvement
A 2007 analysis of medical records and caregiver surveys for 378 patients with dementia found that only 50% of patients received an assessment of their cognitive status in the previous 12 months.6 Another study surveying clinicians practicing in VA medical centers found that only two thirds of clinicians reported regularly performing a standardized assessment of cognitive functioning.7
IOM Domains of Health Care Quality Addressed
Effective Patient-centered
Equitable
Exception Justification
A medical reason exception has been included so that clinicians can exclude patients for whom a cognitive assessment may not be appropriate (eg, patients at the end of life). A patient reason exception has been included for patients who might be unwilling to participate in the assessment.
Harmonization with Existing Measures
Harmonization with existing measures was not applicable to this measure.
Measure Designation
Measure purpose Quality improvement Accountability
Type of measure Process
Level of Measurement
Individual practitioner
Care setting Ambulatory care Residential (ie, nursing facility, domiciliary, home care)
Data source Electronic health record (EHR) data Administrative Data/Claims (outpatient claims) Administrative Data/Claims Expanded (multiple-source) Paper medical record

© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association 19
Measure #3: Functional Status Assessment
Dementia
Measure Description
Percentage of patients, regardless of age, with a diagnosis of dementia for whom an assessment of functional status is performed and the results reviewed at least once within a 12 month period
Measure Components
Numerator Statement
Patients for whom an assessment of functional status* is performed and the results reviewed at least once within a 12 month period * Functional status can be assessed by direct examination of the patient or knowledgeable informant. An assessment of functional status should include, at a minimum, an evaluation of the patient’s ability to perform instrumental activities of daily living (IADL) and basic activities of daily living (ADL). Functional status can also be assessed using one of a number of available valid and reliable instruments available from the medical literature. Examples include, but are not limited to: Lawton IADL Scale Barthel ADL Index Katz Index of Independence in ADL
Denominator Statement
All patients, regardless of age, with a diagnosis of dementia
Denominator Exceptions
Documentation of medical reason(s) for not assessing functional status (eg, patient is severely impaired and caregiver knowledge is limited, other medical reason)
Supporting Guideline & Other References
The following evidence statements are quoted verbatim from the referenced clinical guidelines: A detailed assessment of functional status may also aid the clinician in documenting and tracking changes over time as well as providing guidance to the patient and caregivers. Functional status is typically described in terms of the patient’s ability to perform instrumental activities of daily living such as shopping, writing checks, basic housework, and activities of daily living such as dressing, bathing, feeding, transferring, and maintaining continence. These regular assessments of recent cognitive and functional status provide a baseline for assessing the effect of any intervention, and they improve the recognition and treatment of acute problems, such as delirium. (APA, 2007)21 Conduct and document an assessment and monitor changes in daily functioning, including feeding, bathing, dressing, mobility, toileting, continence, and ability to manage finances and medications…Functional assessment includes evaluation of physical, psychological, and socioeconomic domains. Physical functioning may focus on basic activities of daily living (ADLs) that include feeding, bathing, dressing, mobility, and toileting. Assessment of instrumental (or intermediate) activities of daily living (IADLs) addresses more advanced self-care activities, such as shopping, cooking, and managing finances and medications. Standardized assessment instruments such as the Barthel or Katz indices can provide information on the patient’s capacity for self-care and independent living. Proxies or patient surrogates can complete a number of these instruments when necessary. The initial assessment of functional abilities is important to determine a baseline to which future functional deficits may be compared. (California Workgroup on Guidelines for Alzheimer’s Disease Management, 2008)24

© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
20
Measure Importance
Relationship to desired outcome
Dementia is characterized by cognitive deficits that cause functional impairment compromising basic and instrumental activities of daily living. Functional decline for dementia patients is progressive and continuous and typically marked by decline in instrumental activities of daily living followed by a slower decline in basic activities of daily living.40 Functional impairment is the main factor negatively impacting quality of life in patients with dementia including reported links to the development of apathy and depression.41,42,43 In addition, decline in basic activities of daily living is an important risk factor for institutionalization and a strong predictor of decreased survival in dementia patients.44,45 Initial and ongoing assessments of functional status should be conducted to determine baseline level of functioning, monitor changes over time, and to identify strategies to maximize patient’s independence.
Opportunity for Improvement
A 2007 analysis of medical records and caregiver surveys for 378 patients with dementia found that only 9.5% of patients received an assessment of their activities of daily living in the previous 12 months.6 Similar results were reported in a study analyzing the quality of health care provided to a broader population of vulnerable community-dwelling older patients. Only 18% of vulnerable elders admitted to a hospital or new to a physician practice received an assessment of their functional status.5
IOM Domains of Health Care Quality Addressed
Effective Patient-centered
Equitable
Exception Justification
A medical reason exception has been included so that clinicians can exclude patients for whom a functional assessment may not be feasible (eg, severely impaired patients whose caregiver knowledge is limited).
Harmonization with Existing Measures
Harmonization with existing measures was not applicable to this measure.
Measure Designation
Measure purpose Quality improvement Accountability
Type of measure Process
Level of Measurement
Individual practitioner
Care setting Ambulatory care Residential (ie, nursing facility, domiciliary, home care)
Data source Electronic health record (EHR) data Administrative Data/Claims (outpatient claims) Administrative Data/Claims Expanded (multiple-source) Paper medical record

© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
21
Measure #4: Neuropsychiatric Symptom Assessment Dementia
This measure is paired with Measure #5 – Management of Neuropsychiatric Symptoms
Implementers of this measure should not use Measure #4 without Measure #5.
Measure Description
Percentage of patients, regardless of age, with a diagnosis of dementia and for whom an assessment of neuropsychiatric symptoms is performed and results reviewed at least once in a 12 month period
Measure Components
Numerator Statement
Patients for whom an assessment of neuropsychiatric symptoms** is performed and results reviewed at least once in a 12 month period ** Neuropsychiatric symptoms can be assessed by direct examination of the patient or knowledgeable informant. The following is a non-exhaustive list of dimensions (based on items included in available validated instruments) that may be evaluated during an assessment of neuropsychiatric symptoms: Activity disturbances:
o agitation o wandering o purposeless hyperactivity o verbal or physical aggressiveness o resistiveness with care o apathy o impulsiveness o socially inappropriate behaviors o appetite o eating disturbances o sleep problems o diurnal/sleep-wake cycle disturbances o repetitive behavior
Mood disturbances: o anxiety o dysphoria o euphoria o irritability o mood lability/fluctuations
Thought and perceptual disturbances: o having fixed false beliefs (delusions) o hearing or seeing non-present entities (hallucinations) o paranoia
Examples of reliable and valid instruments that are commonly used in research settings and that can be used to assess behavior include, but are not limited to: Dementia Signs and Symptoms (DSS) Scale46 Neuropsychiatric Inventory47 (NPI) The assessment of behavioral status may include the assessment of Behavioral and Psychological Symptoms of Dementia (BPSD)48. For patients residing in nursing homes, it may include an assessment of the behavioral symptom items from the Minimum Data Set (MDS).
Denominator Statement
All patients, regardless of age, with a diagnosis of dementia
Denominator None

© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
22
Exceptions
Supporting Guideline & Other References
The following evidence statements are quoted verbatim from the referenced clinical guidelines: It is important for the [clinician] treating a patient with dementia to regularly assess cognitive deficits or behavioral difficulties that potentially pose a danger to the patient or others. (APA, 2007)21 Conduct and document an assessment and monitor changes in behavioral symptoms, psychotic symptoms, or depression. (California Workgroup on Guidelines for Alzheimer’s Disease Management, 2008)24 For mild to moderate Alzheimer's disease Assessment of patients with mild to moderate AD [Alzheimer’s Disease] should include measures of behavior and other neuropsychiatric symptoms. (Grade B, Level 3) (Third Canadian Consensus Conference on the Diagnosis and Treatment of Dementia, 2008)36 For severe Alzheimer's disease Assessment should include cognition (e.g., MMSE), function, behaviour, medical status, nutrition, safety and caregiver health. (Grade B, Level 3) (Third Canadian Consensus Conference on the Diagnosis and Treatment of Dementia, 2008)26
Measure Importance
Relationship to desired outcome
Neuropsychiatric symptoms appear to be common for patients with dementia. In community samples of dementia patients, the prevalence of neuropsychiatric symptoms range from 40-88%.49,50,51 Neuropsychiatric symptoms are also common in long-term care facilities, with prevalence ranges from 80-85%.52,53 Neuropsychiatric symptoms of dementia have been associated with accelerated cognitive decline;54 increased functional impairment;55 decreased mean survival time;47 increased co-morbid conditions;56 increased danger to self;48 increased danger to others;57 increased health care service utilization;48, 58, 59 higher risk for institutionalization;60, 61 and greater caregiver stress and burden.62, 63, 64 An assessment of neuropsychiatric symptoms, therefore, is an important step in the development of a management plan for those with dementia.
Opportunity for Improvement
In one analysis of medical records and caregiver surveys for 378 patients with dementia, it was found that within a 12 month period only 73% of patients received an assessment of behavioral problems or depression.6
IOM Domains of Health Care Quality Addressed
Efficient
Equitable
Exception Justification
This measure has no exceptions.
Harmonization with Existing Measures
Harmonization with existing measures was not applicable to this measure.
Measure Designation
Measure purpose Quality Improvement Accountability
Type of measure Process
Level of Measurement
Individual practitioner
Care setting Ambulatory care Residential (ie, nursing facility, domiciliary, home care)
Data source Electronic health record (EHR) data Administrative Data/Claims (outpatient claims)

© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
23
Administrative Data/Claims Expanded (multiple-source) Paper medical record
Additional Information
Measure #4 is paired with Measure #5 (Management of Neuropsychiatric Symptoms). The pairing of these measures is not intended to suggest the use of any particular scoring methodology (ie, a composite score), nor does it imply either equality of or difference in the relative “weights” of the two measures. A performance score for each measure should be reported individually to provide actionable information upon which to focus quality improvement efforts. The NQF provides definitions of paired and composite measures65: Paired measures are individual measures that should be measured concurrently in the same population;
however, the results are not combined into a single score (eg, measuring mortality and readmission and displaying them together—but not calculating a joint score)
A composite measure is a combination of two or more individual measures in a single measure that results in a single score.
© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
24
Measure #5: Management of Neuropsychiatric Symptoms
Dementia
This measure is paired with Measure #4 – Neuropsychiatric Symptom Assessment. Implementers of this measure should not use Measure #5 without Measure #4.
Measure Description
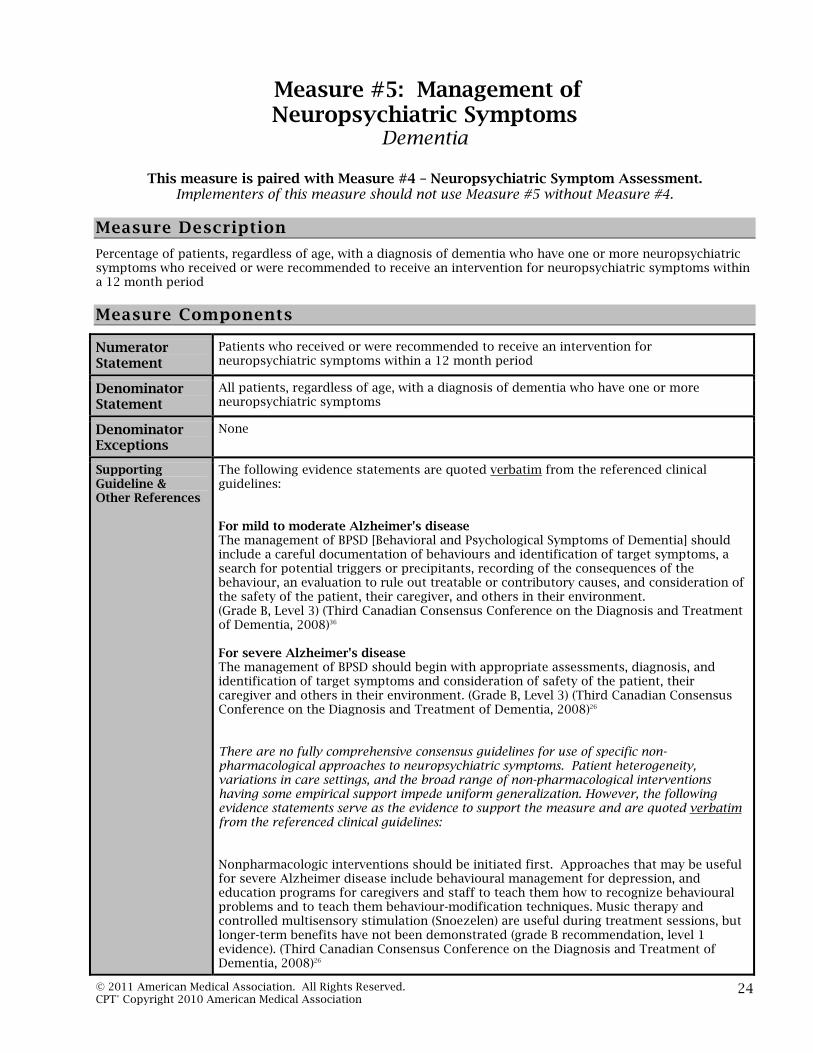
Percentage of patients, regardless of age, with a diagnosis of dementia who have one or more neuropsychiatric symptoms who received or were recommended to receive an intervention for neuropsychiatric symptoms within a 12 month period
Measure Components
Numerator Statement
Patients who received or were recommended to receive an intervention for neuropsychiatric symptoms within a 12 month period
Denominator Statement
All patients, regardless of age, with a diagnosis of dementia who have one or more neuropsychiatric symptoms
Denominator Exceptions
None
Supporting Guideline & Other References
The following evidence statements are quoted verbatim from the referenced clinical guidelines: For mild to moderate Alzheimer's disease The management of BPSD [Behavioral and Psychological Symptoms of Dementia] should include a careful documentation of behaviours and identification of target symptoms, a search for potential triggers or precipitants, recording of the consequences of the behaviour, an evaluation to rule out treatable or contributory causes, and consideration of the safety of the patient, their caregiver, and others in their environment. (Grade B, Level 3) (Third Canadian Consensus Conference on the Diagnosis and Treatment of Dementia, 2008)36 For severe Alzheimer's disease The management of BPSD should begin with appropriate assessments, diagnosis, and identification of target symptoms and consideration of safety of the patient, their caregiver and others in their environment. (Grade B, Level 3) (Third Canadian Consensus Conference on the Diagnosis and Treatment of Dementia, 2008)26 There are no fully comprehensive consensus guidelines for use of specific non-pharmacological approaches to neuropsychiatric symptoms. Patient heterogeneity, variations in care settings, and the broad range of non-pharmacological interventions having some empirical support impede uniform generalization. However, the following evidence statements serve as the evidence to support the measure and are quoted verbatim from the referenced clinical guidelines: Nonpharmacologic interventions should be initiated first. Approaches that may be useful for severe Alzheimer disease include behavioural management for depression, and education programs for caregivers and staff to teach them how to recognize behavioural problems and to teach them behaviour-modification techniques. Music therapy and controlled multisensory stimulation (Snoezelen) are useful during treatment sessions, but longer-term benefits have not been demonstrated (grade B recommendation, level 1 evidence). (Third Canadian Consensus Conference on the Diagnosis and Treatment of Dementia, 2008)26

© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
25
Except for emergency situations, non-pharmacological strategies are the preferred first-line treatment approach for behavioral problems. Medications should be used only as a last resort, if non-pharmacological approaches prove unsuccessful and they are clinically indicated. (California Workgroup on Guidelines for Alzheimer’s Disease Management, 2008)24 Pharmacologic therapies should be initiated concurrently with nonpharmacologic interventions in the presence of severe depression, psychosis or aggression that puts the patient or others at risk of harm (grade B recommendation, level 3 evidence). (Third Canadian Consensus Conference on the Diagnosis and Treatment of Dementia, 2008)26
Measure Importance
Relationship to desired outcome
Neuropsychiatric symptoms are common in patients with dementia. In community samples of dementia patients, the prevalence of neuropsychiatric symptoms ranges from 40-88%.49,50,51 Neuropsychiatric symptoms are also common in long-term care facilities, with prevalence ranges from 80-85%.52,53 Neuropsychiatric symptoms of dementia have been associated with accelerated cognitive decline;54 increased functional impairment;55 decreased mean survival time;47 increased co-morbid conditions;56 increased danger to self;48 increased danger to others;57 increased health care service utilization;48,58,59 higher risk for institutionalization;60,61 and greater caregiver stress and burden.62, 63, 64 Nonpharmacologic interventions should be considered in all cases and in some will be the mainstay of management. Examples of approaches that may be useful include behavioural management for depression, education programs for caregivers and staff to teach them how to recognize, manage, and sometimes prevent behavioral problems, stress reduction for caregivers, and, for patients living at home, enrollment in adult day programs offering structured activities and social stimulation. The evidence evaluating non-pharmacological interventions varies considerably in quality and amount, but broadly supports an individualized approach that includes one or more such interventions. A management plan that assesses the severity and intrusiveness of problematic behaviors can assist clinicians in determining what pharmacologic or non-pharmacologic interventions might be appropriate.66 Mild forms of neuropsychiatric symptoms may be alleviated with psychosocial or environmental interventions. For aggressiveness, presentations of psychosis, or agitation, pharmacologic approaches may be more appropriate.67 If pharmacologic approaches are necessary, they should be administered at the lowest effective dose and their use should be reevaluated and their benefit documented on an ongoing basis.21
Opportunity for Improvement
A 2007 analysis of medical records and caregiver surveys for 378 patients with dementia found that only 33.7% of patients were recommended two or more nonpharmacologic approaches for behavior problems in the previous 12 months.6 Another study surveying clinicians practicing in VA medical centers found that clinicians reported prescribing medications for behavior problems for a median of 22% of their patients.7
IOM Domains of Health Care Quality Addressed
Effective Equitable
Exception Justification
This measure has no exceptions.
Harmonization with Existing Measures
Harmonization with existing measures was not applicable to this measure.
Measure Designation
Measure purpose Quality improvement Accountability
Type of measure Process

© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
26
Level of Measurement
Individual practitioner
Care setting Ambulatory care Residential (ie, nursing facility, domiciliary, home care)
Data source Electronic health record (EHR) data Administrative Data/Claims (outpatient claims) Administrative Data/Claims Expanded (multiple-source) Paper medical record
Additional Information
Measure #5 is paired with Measure #4 (Neuropsychiatric Symptom Assessment). The pairing of these measures is not intended to suggest the use of any particular scoring methodology (ie, a composite score), nor does it imply either equality of or difference in the relative “weights” of the two measures. A performance score for each measure should be reported individually to provide actionable information upon which to focus quality improvement efforts. The NQF provides definitions of paired and composite measures65: Paired measures are individual measures that should be measured concurrently in the same population;
however, the results are not combined into a single score (eg, measuring mortality and readmission and displaying them together—but not calculating a joint score)
A composite measure is a combination of two or more individual measures in a single measure that results in a single score.

© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
27
Measure #6: Screening for Depressive Symptoms Dementia
Measure Description
Percentage of patients, regardless of age, with a diagnosis of dementia who were screened for depressive symptoms within a 12 month period
Measure Components
Numerator Statement
Patients who were screened for depressive symptoms* within a 12 month period *Depressive symptoms in a patient with dementia can include: anxiety, sadness, lack of reactivity to pleasant events, irritability, agitation, retardation, multiple physical complaints, acute loss of interest, appetite loss, lack of energy, diurnal variation of mood, difficulty falling asleep, multiple awakenings, during sleep, early morning awakenings, suicide, self-depreciation, pessimism, mood congruent delusions.68 Since patients may be unable to describe their symptoms, caregiver report of depressive symptoms should be reviewed and included in the screen for depressive symptoms. In addition to clinical qualitative approaches, dementia patients can be screened for depressive symptoms using one of a number of valid, reliable instruments available from the medical literature. Examples include, but are not limited to:
- Cornell Scale for Depression in Dementia - Geriatric Depression Scale [Note: a short form is also available.] - PHQ-9
Denominator Statement
All patients, regardless of age, with a diagnosis of dementia
Denominator Exceptions
None
Supporting Guideline & Other References
The following evidence statements are quoted verbatim from the referenced clinical guidelines: Depression is a common, treatable comorbidity in patients with dementia and should be screened for (Guideline). (AAN, 2001)18 Ongoing assessment includes periodic monitoring of the development and evolution of cognitive and noncognitive psychiatric symptoms and their response to intervention (Category I)…Among the neuropsychiatric symptoms that require ongoing assessment are depression (including major depression and other depressive syndromes), suicidal ideation or behavior, hallucinations, delusions, agitation, aggressive behavior, disinhibition, sexually inappropriate behavior, anxiety, apathy, and disturbances of appetite and sleep. (APA, 2007)21 Conduct and document an assessment and monitor changes in behavioral symptoms, psychotic symptoms, or depression…It is important for health care professionals to be sensitive to symptoms of affective disorders associated with Alzheimer’s Disease and to facilitate early intervention…Since administering assessment tests for depression to Alzheimer’s Disease patients is often challenging and patients may be unable to describe their symptoms to the [primary care practitioner], gathering data from family members becomes especially important…The Cornell Scale for Depression in Dementia is a useful tool for providers because it captures both patient and caregiver input. (California Workgroup on Guidelines for Alzheimer’s Disease Management, 2008)24 In patients with serious illness at the end of life, clinicians should regularly assess patients for pain, dyspnea, and depression. (Grade: strong recommendation, moderate

© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
28
quality of evidence.) (ACP, 2008)69
Measure Importance
Relationship to desired outcome
Depression is one of the most common co-occurring psychiatric conditions in dementia patients, affecting over 50% of patients with Alzheimer’s disease.42 Depression can be reliably detected and quantified, and can be differentiated from the other neuropsychiatric symptoms of dementia.70 The impact of depression is significant with even mild levels of depression in dementia patients associated with higher rates of disability, impaired quality of life, and greater mortality.21 In particular, Alzheimer’s disease patients with depression have demonstrated “significantly more severe apathy, delusions, anxiety, pathological affective crying, irritability, deficits in activities of daily living, impairments in social functioning, and parkinsonism than Alzheimer’s disease patients without depression.”42 Furthermore, with increasing severity of depression, the severity of psychopathological and neurological impairments in dementia patients increases.42 Identifying depression in patients with dementia is therefore essential for early intervention and proper management.
Opportunity for Improvement
A recent study examining the variability between clinical subspecialties in the outpatient evaluation and treatment of dementia reviewed medical records of 1,401 patients with dementia. They found that 63.4% of patients were given formal instruments for depression screening.71 Similar results were reported in a 2007 analysis of medical records and caregiver surveys for 378 patients with dementia with 73% of patients receiving an assessment of behavioral problems or depression in the previous 12 months.6
IOM Domains of Health Care Quality Addressed
Effective Equitable
Exception Justification
This measure has no exceptions.
Harmonization with Existing Measures
Harmonization with existing measures was not applicable to this measure.
Measure Designation
Measure purpose Quality improvement Accountability
Type of measure Process
Level of Measurement
Individual practitioner
Care setting Ambulatory care Residential (ie, nursing facility, domiciliary, home care)
Data source Electronic health record (EHR) data Administrative Data/Claims (inpatient or outpatient claims) Administrative Data/Claims Expanded (multiple-source) Paper medical record

© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
29
Measure #7: Counseling Regarding Safety Concerns Dementia
Measure Description
Percentage of patients, regardless of age, with a diagnosis of dementia or their caregiver(s) who were counseled or referred for counseling regarding safety concerns within in a 12 month period
Measure Components
Numerator Statement
Patients or their caregiver(s) who were counseled* or referred for counseling regarding safety concerns within a 12 month period *Counseling should include a discussion with the patient and their caregiver(s) regarding one or more of the following common safety concerns and potential risks to the patient. When appropriate, it should also include a recommendation or referral for a home safety evaluation. Safety concerns include, but are not limited to: Fall risk Gait/balance Medication management Financial management Home safety risks that could arise from cooking or smoking Physical aggression posing threat to self, family caregiver, or others Wandering Access to firearms or other weapons Access to potentially dangerous materials Being left alone in home or locked in room Inability to respond rapidly to crisis/household emergencies Driving Operation of hazardous equipment Suicidality Abuse or neglect Note: for nursing home patients, different safety concerns might apply. A number of organizations have developed educational materials that are recommended to aid implementation of the measure. These materials/tools include: Alzheimer’s Association Safety Topics. Available at:
http://www.alz.org/alzheimers_disease_publications_safety.asp Alzheimer’s Disease Education and Referral Center’s Home Safety for the Alzheimer’s
Patient. Available at: http://www.nia.nih.gov/Alzheimers/
Denominator Statement
All patients, regardless of age, with a diagnosis of dementia
Denominator Exceptions
Documentation of medical reason(s) for not counseling regarding safety concerns (eg, patient at end of life, other medical reason)
Supporting Guideline & Other References
The following evidence statements are quoted verbatim from the referenced clinical guidelines: Recommended assessments include evaluation of suicidality, dangerousness to self and others, and the potential for aggression, as well as evaluation of living conditions, safety of the environment, adequacy of supervision, and evidence of neglect or abuse (Category I). [I]mportant safety issues in the management of patients with dementia include interventions to decrease the hazards of wandering and recommendations concerning activities such as cooking, driving, hunting, and the operation of hazardous equipment.

© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
30
Caregivers should be referred to available books [and other materials] that provide advice and guidance about maximizing the safety of the environment for patients with dementia…As patients become more impaired, they are likely to require more supervision to remain safe, and safety issues should be addressed as part of every evaluation. Families should be advised about the possibility of accidents due to forgetfulness (e.g., fires while cooking), of difficulties coping with household emergencies, and of the possibility of wandering. Family members should also be advised to determine whether the patient is handling finances appropriately and to consider taking over the paying of bills and other responsibilities. At this stage of the disease [ie, moderately impaired patients], nearly all patients should not drive. (APA, 2007)21 Safety issues such as driving, fall risk, medication management, environmental hazards, wandering, and access to firearms need to be discussed periodically with the patient and caregiver. Safety concerns typically focus on three risks in particular: falling, wandering, and driving. (California Workgroup on Guidelines for Alzheimer’s Disease Management, 2008)24 For mild to moderate Alzheimer's disease Assess for safety risks (e.g., driving, financial management, medication management, home safety risks that could arise from cooking or smoking, potentially dangerous behaviours such as wandering) (Canadian Consensus Conference on Diagnosis and Treatment of Dementia, 2008)36
Measure Importance
Relationship to desired outcome
The vast majority (87%) of individuals with Alzheimer’s disease are cared for at home by family members.1 “As the disease progresses however, physical features of the home environment may present as a safety hazard or barrier to performing activities of daily living, particularly at the moderate stage of the disease process.”72 Safety concerns should be addressed with patients and their caregivers throughout the course of the disease.
Opportunity for Improvement
For only 26% of patients with dementia, did the physician discuss or refer for discussion about patient safety, provide education on how to deal with conflicts at home, and inform them about community resources for dementia in a study analyzing the quality of health care provided to a vulnerable community-dwelling older patients.5 A 2007 analysis of medical records and caregiver surveys for 378 patients with dementia found that only 20.6% of patients received recommended safety care processes.6
IOM Domains of Health Care Quality Addressed
Safe
Patient-centered Equitable
Exception Justification
This measure has no exceptions.
Harmonization with Existing Measures
Harmonization with existing measures was not applicable to this measure.
Measure Designation
Measure purpose Quality improvement Accountability
Type of measure Process
Level of Measurement
Individual practitioner
Care setting Ambulatory care Residential (ie, nursing facility, domiciliary, home care)
Data source Electronic health record (EHR) data Administrative Data/Claims (outpatient claims) Administrative Data/Claims Expanded (multiple-source) Paper medical record

© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
31
Measure #8: Counseling regarding Risks of Driving
Dementia
Measure Description
Percentage of patients, regardless of age, with a diagnosis of dementia or their caregiver(s) who were counseled regarding the risks of driving and the alternatives to driving at least once within a 12 month period
Measure Components
Numerator Statement
Patients or their caregiver(s) who were counseled regarding the risks of driving and the alternatives to driving at least once within a 12 month period One resource that includes patient and caregiver educational materials that can be used to aid implementation of the measure is the Physician's Guide to Assessing and Counseling Older Drivers, developed by the American Medical Association in cooperation with the National Highway Traffic Safety Administration,. This document is available at: http://www.ama-assn.org/ama/pub/physician-resources/public-health/promoting-healthy-lifestyles/geriatric-health/older-driver-safety/assessing-counseling-older-drivers.shtml.
Denominator Statement
All patients, regardless of age, with a diagnosis of dementia
Denominator Exceptions
Documentation of medical reason(s) for not counseling regarding the risks of driving (eg, patient is no longer driving, other medical reason)
Supporting Guideline & Other References
The following evidence statements are quoted verbatim from the referenced clinical guidelines: A diagnosis of Alzheimer’s disease is not, on its own, a sufficient reason to withdraw driving privileges. The determining factor in withdrawing driving privileges should be an individual’s driving ability. (Alzheimer’s Association, 2001)73 All patients and families should be informed that even mild dementia increases the risk of vehicular accidents (Category I). Mildly impaired patients should be advised to limit their driving to safer situations or to stop driving (Category I), and moderately impaired patients should be instructed not to drive (Category I). Advice about driving cessation should also be communicated to family members, as the implementation of the recommendation often falls on them (Category I). Relevant state laws regarding notification should be followed (Category I). (APA, 2007)21 For patients with dementia, consider the following characteristics useful for identifying patients at increased risk for unsafe driving: the Clinical Dementia Rating scale (Level A), a caregiver’s rating of a patient’s driving ability as marginal or unsafe (Level B), a history of crashes or traffic citations (Level C), reduced driving mileage or self-reported situational avoidance (Level C), Mini-Mental State Examination scores of 24 or less (Level C), and aggressive or impulsive personality characteristics (Level C). Consider the following characteristics not useful for identifying patients at increased risk for unsafe driving: a patient’s self-rating of safe driving ability (Level A) and lack of situational avoidance (Level C). There is insufficient evidence to support or refute the benefit of neuropsychological testing, after controlling for the presence and severity of dementia, or interventional strategies for drivers with dementia (Level U). Clinicians may present patients and their caregivers with the data showing that, as a group, patients with mild dementia (CDR of 1) are at a substantially higher risk for unsafe driving and thus should strongly consider discontinuing driving. At the very least, patients and their caregivers should prepare for the eventuality of driving cessation as dementia severity increases. (AAN, 2010)20
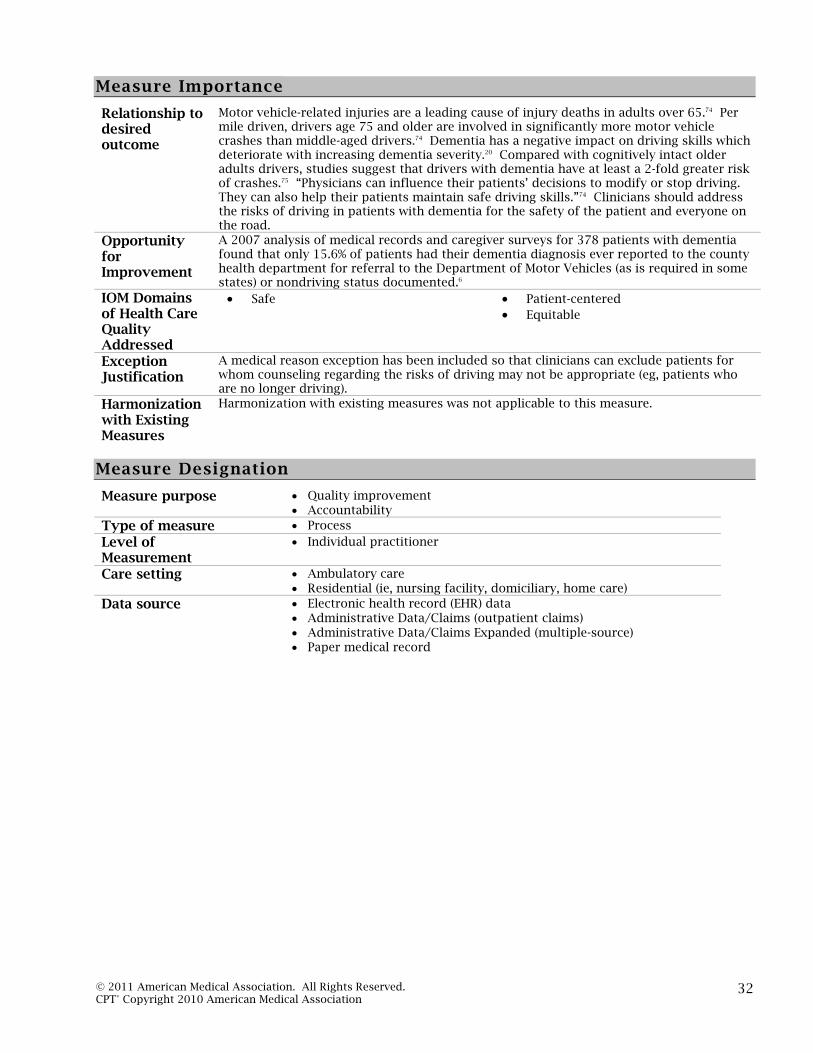
© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
32
Measure Importance
Relationship to desired outcome
Motor vehicle-related injuries are a leading cause of injury deaths in adults over 65.74 Per mile driven, drivers age 75 and older are involved in significantly more motor vehicle crashes than middle-aged drivers.74 Dementia has a negative impact on driving skills which deteriorate with increasing dementia severity.20 Compared with cognitively intact older adults drivers, studies suggest that drivers with dementia have at least a 2-fold greater risk of crashes.75 “Physicians can influence their patients’ decisions to modify or stop driving. They can also help their patients maintain safe driving skills.”74 Clinicians should address the risks of driving in patients with dementia for the safety of the patient and everyone on the road.
Opportunity for Improvement
A 2007 analysis of medical records and caregiver surveys for 378 patients with dementia found that only 15.6% of patients had their dementia diagnosis ever reported to the county health department for referral to the Department of Motor Vehicles (as is required in some states) or nondriving status documented.6
IOM Domains of Health Care Quality Addressed
Safe
Patient-centered Equitable
Exception Justification
A medical reason exception has been included so that clinicians can exclude patients for whom counseling regarding the risks of driving may not be appropriate (eg, patients who are no longer driving).
Harmonization with Existing Measures
Harmonization with existing measures was not applicable to this measure.
Measure Designation
Measure purpose Quality improvement Accountability
Type of measure Process
Level of Measurement
Individual practitioner
Care setting Ambulatory care Residential (ie, nursing facility, domiciliary, home care)
Data source Electronic health record (EHR) data Administrative Data/Claims (outpatient claims) Administrative Data/Claims Expanded (multiple-source) Paper medical record

© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
33
Measure #9: Palliative Care Counseling and Advance Care
Planning Dementia
Measure Description
Percentage of patients, regardless of age, with a diagnosis of dementia or their caregiver(s) who received 1) comprehensive counseling regarding ongoing palliation and symptom management and end of life decisions AND 2) have an advance care plan or surrogate decisions maker in the medical record or documentation in the medical record that the patient did not wish or was not able to name a surrogate decision maker or provide an advance care plan within two years of initial diagnosis or assumption of care
Measure Components
Numerator Statement
Patients or their caregiver(s) who received 1) comprehensive counseling regarding ongoing palliation and symptom management and end of life decisions* AND 2) have an advance care plan or surrogate decisions maker in the medical record or documentation in the medical record that the patient did not wish or was not able to name a surrogate decision maker or provide an advance care plan** within two years of initial diagnosis or assumption of care *Comprehensive counseling regarding end of life decisions includes a discussion of the risks and benefits of the following medical interventions to address the major clinical issues associated with advanced dementia: Hospitalization Treatment for infections Surgery Artificial nutrition and hydration Cardiopulmonary resuscitation Mechanical ventilation Comfort care Timing of a natural death Hospice referral **Definition: Documentation in the medical record that an advance care plan was discussed but patient did not wish or was not able to name a surrogate decision maker or provide an advance care plan. This documentation in the medical record could also include as appropriate that the patient's cultural and/or spiritual beliefs preclude a discussion of advance care planning as it would be viewed as harmful to the patient's beliefs and thus harmful to the physician-patient relationship.
Denominator Statement
All patients, regardless of age, with a diagnosis of dementia
Denominator Exceptions
None
Supporting Guideline & Other References
The following evidence statements are quoted verbatim from the referenced clinical guidelines: At this stage [ie, severely and profoundly impaired patients]…the treatment team should help the family prepare for the patient’s death. Ideally, discussions about feeding tube placement, treatment of infection, cardiopulmonary resuscitation, and intubation will have taken place when the patient could participate, but if they have not, it is important to raise these issues with the family before a decision about one of these options is urgently required. (APA, 2007)21 Advance directives and designation of healthcare surrogates should be put in place early,

© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
34
while the patient can still have input. The PCP should also discuss values, preferences, and goals related to death and dying with patients in early stages of Alzheimer’s Disease, including do not-resuscitate orders, artificial nutrition plans, and healthcare proxies. Expert opinion and Workgroup consensus suggest that PCPs should initiate conversations with patients and their families about late-stage care and appointing a proxy. Proxies should have extensive conversations with the patient about his or her wishes with respect to a variety of circumstances and situations. (California Workgroup on Guidelines for Alzheimer’s Disease Management, 2008)24 A crucial component of [care for nursing home residents] is providing information about the benefits and burdens of [medical] interventions to the resident’s surrogate decision maker, supporting development of a care plan that takes into consideration previous wishes of the resident, if any, and his or her best interest as interpreted by the decision maker. The care plan should consider the goals of care and priority order of the three possible goals – survival, maintenance of function, and comfort. (Volicer L. for Alzheimer’s Association, 2005)76 The National Hospice and Palliative Care Organization provides the Caring Connection web site (www.caringinfo.org). This web site provides resources and information on end-of-life care, including a national repository of state by state advance directives. [Advance directives are d]esigned to respect patient's autonomy and determine his/her wishes about future life-sustaining medical treatment if unable to indicate wishes… Key interventions, treatment decisions to include in advance directives [are]: resuscitation procedures, mechanical respiration, chemotherapy, radiation therapy, dialysis, simple diagnostic tests, pain control, blood products, transfusions, intentional deep sedation. (AGS, 2010)77
Measure Importance
Relationship to desired outcome
Unlike other diseases that cause death, dementia follows a “gradual downhill course punctuated by declines caused by acute illness that often are accompanied by delirium and decrements in mental and functional status.”78 As a result, there are a number of end of life considerations unique to dementia patients.79 An analysis of the clinical course of advanced dementia found that a number of distressing symptoms and burdensome interventions are pervasive at this stage of the disease. Dyspnea, pain, pressure ulcers and aspiration were prevalent and were more likely to occur as the end of life approached. Among nursing home residents who died, 40.7% underwent any one of several burdensome interventions (ie, received parenteral therapy, were hospitalized, were taken to the emergency room, underwent tube feeding) prior to death.80 “Aggressive medical treatment for [nursing home] residents with advanced dementia is often inappropriate for medical reasons, has a low rate of success, and can have negative outcomes that hasten functional decline and death.”76 A thorough, often ongoing, discussion with patients and caregivers of the common clinical complications of advanced dementia and corresponding medical interventions is critical to eliciting the patient’s preferences and can help ease the decision making burden on caregivers during more critical times.
Opportunity for Improvement
Despite its critical importance for dementia patients, research indicates that physician involvement in advance care counseling and planning is poor. Survey data has indicated that while a majority of physicians reported counseling their patients with mild to moderate Alzheimer’s disease regarding advance planning issues, only 47% discussed end of life care.81 Among health care proxies of nursing home residents with advanced dementia, only 32.5% stated that a physician had counseled them about clinical complications to expect in advanced dementia and an even smaller proportion (18%) stated that they had received prognostic information from a physician.80
IOM Domains of Health Care Quality Addressed
Safe Effective
Patient-centered Equitable
Exception Justification
This measure has no exceptions.

© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
35
Harmonization with Existing Measures
Harmonization with existing measures was not applicable to this measure.
Measure Designation
Measure purpose Quality improvement Accountability
Type of measure Process
Level of Measurement
Individual practitioner
Care setting Ambulatory care Residential (ie, nursing facility, domiciliary, home care)
Data source Electronic health record (EHR) data Administrative Data/Claims (outpatient claims) Administrative Data/Claims Expanded (multiple-source) Paper medical record

© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
36
Measure #10: Caregiver Education and Support Dementia
Measure Description
Percentage of patients, regardless of age, with a diagnosis of dementia whose caregiver(s) were provided with education on dementia disease management and health behavior changes AND referred to additional resources for support within a 12 month period
Measure Components
Numerator Statement
Patients whose caregiver(s) were provided with education* on dementia disease management and health behavior changes AND referred to additional resources for support within a 12 month period *Education should also include advising the caregiver that he or she is at “increased risk of serious illness (including circulatory and heart conditions and respiratory disease and hypertension), increased physician visits and use of prescription medications, emotional strain, anxiety, and depression.”24 There are a number of assessment tools available for the caregiver. These should be considered as an integral component of comprehensive caregiver education and support. The American Medical Association has developed a Caregiver Health Self-assessment Questionnaire to help caregivers analyze their own health-related behavior and health risks and, with their physician's help, make decisions that will benefit both the caregiver and the patient. This questionnaire is available at: http://www.ama-assn.org/ama/pub/physician-resources/public-health/promoting-healthy-lifestyles/geriatric-health/caregiver-health/caregiver-self-assessment.shtml
Denominator Statement
All patients, regardless of age, with a diagnosis of dementia
Denominator Exceptions
Documentation of medical reason(s) for not providing the caregiver with education on disease management and health behavior changes or referring to additional sources for support (eg, patient does not have a caregiver, other medical reason)
Supporting Guideline & Other References
The following evidence statements are quoted verbatim from the referenced clinical guidelines: Important aspects of psychiatric management include educating patients and families about the illness, its treatment, and sources of additional care and support (e.g., support groups, respite care, nursing homes, and other long-term-care facilities) and advising patients and their families of the need for financial and legal planning due to the patient’s eventual incapacity (e.g., power of attorney for medical and financial decisions, an up-to-date will, and the cost of long-term care) (Category I)… The family should be educated regarding basic principles of care, including 1) recognizing declines in capacity and adjusting expectations appropriately, 2) bringing sudden declines in function and the emergence of new symptoms to professional attention, 3) keeping requests and demands relatively simple, 4) deferring requests if the patient becomes overly upset or angered, 5) avoiding overly complex tasks that may lead to frustration, 6) not confronting patients about their deficits, 7) remaining calm, firm, and supportive and providing redirection if the patient becomes upset, 8) being consistent and avoiding unnecessary change, and 9) providing frequent reminders, explanations, and orientation cues… In addition to providing families with information on support groups, there are a number of benefits of referral to the local chapter or national office of the Alzheimer’s Association (1-800-272-3900; http://www.alz.org), the Alzheimer’s Disease Education and Referral Center (ADEAR) (1-800-438-4380; http://www.nia.nih.gov/Alzheimers/), and other support organizations. (APA, 2007)21 Studies have shown that education and support for caregivers increases the chances of adherence to treatment recommendations for patients. The PCP should provide information and education about the current stage of the disease process and talk with
© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
37
the patient and family to establish treatment goals. Based on the agreed-upon goals, a discussion regarding the expected effects (positive and negative) of interventions on cognition, mood, and behavior will ensure that the prescribed treatment strategy is appropriate to family values and culture. (California Workgroup on Guidelines for Alzheimer’s Disease Management, 2008)24 Seamless resource referral and access to critical services for both patients and caregivers are considered essential. The PCP should encourage the caregiver to participate in educational programs, support groups, respite services, and adult day service programs. The local Alzheimer’s Association chapter or other local agency support groups and community resources such as the Caregiver Resources Centers should be recommended. (California Workgroup on Guidelines for Alzheimer’s Disease Management, 2008)24
Measure Importance
Relationship to desired outcome
The vast majority (87%) of individuals with Alzheimer’s disease are cared for at home by family members.1 Chodosh et al. found that greater caregiver knowledge of dementia management was associated with higher care quality.6 Other studies have indicated that intensive caregiver support in the form of individual and family counseling and on-going telephone counseling results in improved patient health outcomes.82,83 Providing education to caregivers and referring them to additional sources for support is a critically important piece of comprehensive care for patients with dementia.
Opportunity for Improvement
A 2007 analysis of medical records and caregiver surveys for 378 patients with dementia found that only 51.6% of patients received recommended education or support services. In particular, caregiver support activities were recommended to only 24.6% of caregivers while referral to community agencies, including the Alzheimer’s Association or Caregiver’s Resource Center, was more frequent (78.6%).6 Another study surveying clinicians practicing in VA medical centers found that clinicians reported provision of patient and family education and support varied by activity. 74% of clinicians reported routinely telling the family about the disease course while 60% reported explaining the care needs to the family and even less (33%) reported referring the caregiver to the community.7
IOM Domains of Health Care Quality Addressed
Effective Patient-centered
Equitable
Exception Justification
Given the measure’s focus on patient’s caregivers, a medical reason exception has been included so that clinicians can exclude patients without a caregiver and to whom the measure does not apply.
Harmonization with Existing Measures
Harmonization with existing measures was not applicable to this measure.
Measure Designation
Measure purpose Quality improvement Accountability
Type of measure Process
Level of Measurement
Individual practitioner
Care setting Ambulatory care
Data source Electronic health record (EHR) data Administrative Data/Claims (inpatient or outpatient claims) Administrative Data/Claims Expanded (multiple-source) Paper medical record

© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
38
Evidence Classification and Rating Schemes Dementia
APA practice guideline for the treatment of patients With Alzheimer’s Disease and Other Dementias Each recommendation is identified as falling into one of three categories of endorsement, indicated by a bracketed Roman numeral following the statement. The three categories represent varying levels of clinical confidence: [Category I]: Recommended with substantial clinical confidence. [Category II]: Recommended with moderate clinical confidence. [Category III]: May be recommended on the basis of individual circumstances.
Third Canadian Consensus Conference on the Diagnosis and Treatment of Dementia Grades indicating the strength of recommendations A) There is good evidence to support this manoeuvre. B) There is fair evidence to support this manoeuvre. C) There is insufficient evidence to recommend for or against this manoeuvre but recommendations may be
made on other grounds. D) There is a fair evidence to recommend against this procedure. E) There is good evidence to recommend against this procedure. Levels of evidence 1. Evidence obtained from at least 1 properly randomized controlled trial. 2.1. Evidence obtained from well-designed controlled trials without randomization, or 2.2. Evidence obtained from well-designed cohort or case–control analytic studies preferably from more than 1 centre or research group, or 2.3. Evidence obtained from comparisons between times or places with or without the intervention. Dramatic results in uncontrolled experiments are included in this category. 3. Opinions of respected authorities based on clinical experience, descriptive studies or reports of expert committees. The American College of Physicians' Guideline: Evidence-based interventions to improve the palliative care of pain, dyspnea, and depression at the end of life
Strength of Recommendation
Quality of Evidence Benefits Clearly Outweigh Risks and Burden OR Risks and Burden Clearly
Outweigh Benefits
Benefits Finely Balanced with Risks and Burden
High Strong Weak Moderate Strong Weak
Low Strong Weak Insufficient evidence to
determine benefits or risks I - recommendation
AAN practice parameter for diagnosis of dementia Class Description I Evidence provided by a well designed prospective study in a broad spectrum of
persons with the suspected condition, using a “gold standard” for case definition, in which test is applied in a blinded evaluation, and enabling the assessment of appropriate tests of diagnostic accuracy.
II Evidence provided by a well designed prospective study of a narrow spectrum of persons with the suspected condition, or a well designed retrospective study of a broad spectrum of persons with an established condition (by “gold standard”) compared with a broad spectrum of controls, in which test is applied in blinded evaluation, and enabling the assessment of appropriate tests of diagnostic accuracy.
III Evidence provided by a retrospective study in which either persons with the established condition or controls are of a narrow spectrum, and in which test is applied in a blinded evaluation.
IV Any design in which test is not applied in blinded evaluation OR evidence provided by expert opinion alone or in descriptive case series (without controls).
Definitions for practice recommendations based on classification of evidence

© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
39
Recommendation Description Standard Principle for patient management that reflects a high degree of clinical
certainty (usually this requires Class I evidence that directly addresses the clinical question, or overwhelming Class II evidence when circumstances preclude randomized clinical trials).
Guideline Recommendation for patient management that reflects moderate clinical certainty (usually this requires Class II evidence or a strong consensus of Class III evidence).
Practice Option Strategy for patient management for which the clinical utility is uncertain (inconclusive or conflicting evidence or opinion).
Practice Advisory Practice recommendation for emerging and/or newly approved therapies or technologies based on evidence from at least one Class I study. The evidence may demonstrate only a modest statistical effect or limited (partial) clinical response, or significant cost-benefit questions may exist. Substantial (or potential) disagreement among practitioners or between payers and practitioners may exist.
AAN practice parameter for evaluation and management of driving risk in dementia Classification of recommendations A = Established as effective, ineffective or harmful (or established as useful/predictive or not
useful/predictive) for the given condition in the specified population. (Level A rating requires at least two consistent Class I studies.)
B = Probably effective, ineffective or harmful (or probably useful/predictive or not useful/predictive) for the given condition in the specified population. (Level B rating requires at least one Class I study or two consistent Class II studies.)
C = Possibly effective, ineffective or harmful (or possibly useful/predictive or not useful/predictive) for the given condition in the specified population. (Level C rating requires at least one Class II study or two consistent Class III studies.)
U = Data inadequate or conflicting; given current knowledge, treatment (test, predictor) is unproven. Classification of evidence for the rating of a diagnostic article Class I: A cohort study with prospective data collection of a broad spectrum of persons with the suspected
condition, using an acceptable reference standard for case definition. The diagnostic test is objective or performed and interpreted without knowledge of the patient’s clinical status. Study results allow calculation of measures of diagnostic accuracy.
Class II: A case control study of a broad spectrum of persons with the condition established by an acceptable reference standard compared to a broad spectrum of controls or a cohort study where a broad spectrum of persons with the suspected condition where the data was collected retrospectively. The diagnostic test is objective or performed and interpreted without knowledge of disease status. Study results allow calculation of measures of diagnostic accuracy.
Class III: A case control study or cohort study where either persons with the condition or controls are of a narrow spectrum. The condition is established by an acceptable reference standard. The reference standard and diagnostic test are objective or performed and interpreted by different observers. Study results allow calculation of measures of diagnostic accuracy.
Class IV: Studies not meeting Class I, II or III criteria including consensus, expert opinion or a case report.

© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association 40
Summary of Non-Material Interest Disclosures Dementia
None of the members of the Dementia Work Group had any disqualifying material interests under the PCPI Conflict of Interest Policy. The following is a summary of non-disqualifying interests disclosed on Work Group members' Material Interest Disclosure Statements. Completed Material Interest Disclosure Statements are available upon request.
Work Group Member
Disclosures
_Jerry C. Johnson_____ (Co-Chair) None _Germaine Odenheimer (Co-Chair) None _Francois Boller______ None _Soo Borson_________ None _Charles A. Cefalu____ None _Mirean Coleman___ None _Patricia C. Davis_____ None _Mary Ann Forciea____ None _Elizabeth M. Galik____ Payment for Consulting Services: Novartis – Development
of nurse practitioner education material on Dementia
_Laura N. Gitlin______ None _Helen H. Kyomen____ None Katie Maslow None Haydee Muse None Bruce E. Robinson None Robert Paul Roca None Amy E. Sanders None Jason E. Schillerstrom None Joseph W. Shega None Eric G. Tangalos Stock Ownership: Johnson & Johnson (family member)
Research or Other Grant Support: Baxter Payment for Consulting Services: Novartis Other Payments: Lilly – Participation on a data safety monitoring board
Joan M. Teno None Brian K. Unwin None

© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
41
References 1 Alzheimer’s Association. 2009 Alzheimer’s Disease Facts and Figures. Alzheimer’s Association ; 2009. http://www.alz.org/national/documents/report_alzfactsfigures2009.pdf. Accessed February 24, 2010. 2 Alzheimer’s Association. 2010 Alzheimer’s Disease Facts and Figures. Alzheimer’s Association; 2010. http://www.alz.org/documents_custom/report_alzfactsfigures2010.pdf. Accessed August 19, 2010. 3 Xu JQ, Kochanek KD, Murphy SL, Tejada-Vera B. Deaths: final data for 2007. Hyattsville, MD: US Department of Health and Human Services, CDC, National Center for Health Statistics; 2010. National Vital Statistics Report, vol. 58, no. 19. Available at http: //www.cdc.gov/nchs/data/nvsr/nvsr58/nvsr58_19.pdf. Accessed August 17, 2011. 4 Alzheimer’s Disease International. World Alzheimer Report 2010: The global economic impact of dementia. http://www.alz.org/documents/national/World_Alzheimer_Report_2010.pdf. Accessed September 28, 2010. 5 Wenger N, Solomon D, Roth C et al. The quality of medical care provided to vulnerable community-dwelling older patients. Ann Intern Med. 2003;139:740–747. 6 Chodosh J, Mittman BS, Connor KI. Caring for patients with dementia: How good is the quality of care? Results from three health systems. J Am Geriatr Soc. 2007 Aug;55(8):1260-8. 7 Rosen CS, Chow HC, Greenbaum MA, et al. How well are clinicians following dementia practice guidelines? Alzheimer Dis Assoc Disord. 2002;16(1): 15-23. 8 Cooper C, Tandy AR, Balamurali TB, Livingston G. A systematic review and meta-analysis of ethnic differences in use of dementia treatment, care, and research. Am J Geriatr Psychiatry. 2010 Mar;18(3):193-203. 9 Institute of Medicine. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academy Press; 2001. 10 Feldman HH, Jacova C, Robillard A, et al. Diagnosis and treatment of dementia: 2. Diagnosis. CMAJ 2008;178:825-36.[ 11 Clark PC, Kutner NG, Goldstein FC, et al. Impediments to timely diagnosis of Alzheimer’s disease in African Americans. J Am Geriatr Soc. 2005 Nov;53(11):2012-7. Cited by: Zuckerman IH, Ryder PT, Simoni-Wastila L, et al. Racial and ethnic disparities in the treatment of dementia among Medicare beneficiaries. J Gerontol B Psychol Sci Soc Sci. 2008 Sep;63(5):S328-33. 12 Leo RJ, Narayan DA, Sherry C. Geropsychiatric consultation for African American and Caucasian patients. Gen Hosp Psychiatry. 1997 May;19(3):216-22. Cited by: Zuckerman IH, Ryder PT, Simoni-Wastila L, et al. Racial and ethnic disparities in the treatment of dementia among Medicare beneficiaries. J Gerontol B Psychol Sci Soc Sci. 2008 Sep;63(5):S328-33. 13 Zuckerman IH, Ryder PT, Simoni-Wastila L, et al. Racial and ethnic disparities in the treatment of dementia among Medicare beneficiaries. J Gerontol B Psychol Sci Soc Sci. 2008 Sep;63(5):S328-33. 14 Stevens A, Owen J, Roth D, Clay O, Bartolucci A, Haley W. Predictors of time to nursing home placement in White and African American individuals with dementia. J Aging Health. 2004 Jun;16(3):375-97. Cited by: Zuckerman IH, Ryder PT, Simoni-Wastila L, et al. Racial and ethnic disparities in the treatment of dementia among Medicare beneficiaries. J Gerontol B Psychol Sci Soc Sci. 2008 Sep;63(5):S328-33. 15 Yaffe K, Fox P, Newcomer R, et al. Patient and caregiver characteristics and nursing home placement in patients with dementia. JAMA. 2002 Apr 24;287(16):2090-7. 16 National Quality Forum Issue Brief (No.10). Closing the Disparities Gap in Healthcare Quality with Performance Measurement and Public Reporting. Washington, DC: NQF, August 2008. 17 Agency for Healthcare Research and Quality. Race, Ethnicity, and Language Data: Standardization for Health Care Quality Improvement. March 2010. AHRQ Publication No. 10-0058-EF. http://www.ahrq.gov/research/iomracereport. Accessed May 25, 2010. 18 Knopman ST, DeKosky JL, Cummings H, et al. Practice parameter: Diagnosis of dementia (an evidence-based review): Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology. 2001;56;1143-1153. 19 Doody RS, Stevens JC, Beck C. Practice Parameter: Management of Dementia (An evidence-based review): Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology. 2001;56 :1154-1166. 20 Iverson DJ, Gronseth GS, Reger MA, Classen S, Dubinsky RM, Rizzo M. Practice Parameter update: Evaluation and management of driving risk in dementia: Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology. 2010;74:1316-1324. 21 American Psychiatric Association (APA). Practice guideline for the treatment of patients with Alzheimer's disease and other dementias. Arlington (VA): American Psychiatric Association (APA); 2007 Oct. 22 American Medical Directors Association. Dementia Clinical Practice Guideline. Columbia, MD: AMDA 2009. 23 Chertkow H. Diagnosis and treatment of dementia: introduction. Introducing a series based on the Third Canadian Consensus Conference on the Diagnosis and Treatment of Dementia. CMAJ. 2008;178:316-21. 24 California Workgroup on Guidelines for Alzheimer’s Disease Management. Guidelines for Alzheimer’s disease management. Los Angeles, CA: Alzheimer’s Disease and Related Disorders Association, Inc., Los Angeles Chapter. 2008.

© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
42
25 Physician Consortium for Performance Improvement (PCPI) Web site. PCPI position statement: the evidence base required for measure development. http://www.ama-assn.org/ama/pub/physician-resources/clinical-practice-improvement/clinical-quality/physician-consortium-performance-improvement/position-papers.shtml. Accessed June 25, 2010. 26 Herrmann N, Gauthier S. Diagnosis and treatment of dementia: 6. Management of severe Alzheimer disease. CMAJ. December 2, 2008; 179(12): 1279 - 1287. 27 National Library of Medicine. Medical Subject Headings Caregiver Descriptor Data. Available at: http://www.nlm.nih.gov/mesh/meshhome.html. Accessed August 17, 2011. 28 The Cornell Scale for Depression in Dementia Administration & Scoring. Available at: http://www.dementia-assessment.com.au/depression/Cornel_Scale_Guidelines.pdf. Accessed August 17, 2011. 29 Callahan CM, Hendrie HC, Tierney WM. Documentation and Evaluation of Cognitive Impairment in Elderly Primary Care Patients. Ann Intern Med. 1995;122:422-429. 30 Boise L, Neal MB, and Kaye J. Dementia assessment in primary care: Results from a study in three managed care systems. J Gerontol: Medical Sciences. 2004;59A(6):621-626. 31 Valcour VG, Masaki KH, Curb JD, Blanchette PL. The detection of dementia in the primary care setting. Arch Intern Med. 2000;160:2964-2968. 32 Ganguli M, Rodriguez E, Mulsant B, et al. Detection and Management of Cognitive Impairment in Primary Care: The Steel Valley Seniors Survey. J Am Geriatr Soc. 2004;52:1668-1675. 33 Boustani M, Callahan CM, Unverzagt FW, et al. Implementing a screening and diagnosis program for dementia in primary care. Journal of General Internal Medicine. 2005;20:572-577. 34 Borson S, Scanlan JM, Watanabe J, Tu S-P, and Lessig M. Improving identification of cognitive impairment in primary care. International Journal of Geriatric Psychiatry 2006;21(4):349-355. 35 Ashford JW, Borson S, O’Hara R, et al. Should older adults be screened for dementia? It is important to screen for evidence of dementia! Alzheimers Dement. 2007 Apr;3(2):75-80. 36 Hogan DB, Bailey P, Black S, et al. Diagnosis and treatment of dementia: 4. Approach to management of mild to moderate dementia. CMAJ. 2008;179:787-93. 37 Chow TW, MacLean CH. Quality indicators for dementia in vulnerable community-dwelling and hospitalized elders. Ann Intern Med. 2001 Oct 16;135(8 Pt 2):668-76. 38 National Institutes of Health (NIH). NIH State-of-the-Science Conference: Preventing Alzheimer’s Disease and Cognitive Decline. April 26–28, 2010. http://consensus.nih.gov/2010/docs/alz/alz_stmt.pdf. Accessed June 9, 2010. 39 Wilson RS, Aggarwal NT, Barnes LL, Mendes de Leon CF, Hebert LE, Evans DA. Cognitive decline in incident Alzheimer disease in a community population. Neurology. 2010 Mar 23;74(12):951-5. 40 Lechowski L, Van Pradelles S, Le Crane M, et al; and REAL Group. Patterns of loss of basic activities of daily living in Alzheimer patients: A cross-sectional study of the French REAL cohort. Dement Geriatr Cogn Disord. 2010;29(1):46-54. 41 Andersen CK, Wittrup-Jensen KU, Lolk A, Andersen K, Kragh-Sørensen P. Ability to perform activities of daily living is the main factor affecting quality of life in patients with dementia. Health Qual Life Outcomes. 2004, 2:52. 42 Starkstein SE, Jorge R, Mizrahi R, Robinson RG. The Construct of Minor and Major Depression in Alzheimer’s Disease. Am J Psychiatry. 2005;162:2086-2093. 43 Boyle PA, Malloy PF, Salloway S, Cahn-Weiner DA, Cohen R, Cummings JL. Executive dysfunction and apathy predict functional impairment in Alzheimer disease. Am J Geriatr Psychiatry. 2003 Mar-Apr;11(2):214-21. 44 Steeman E, Abraham IL, Godderis J. Risk profiles for institutionalization in a cohort of elderly people with dementia or depression. Arch Psychiatr Nurs. 1997;11, 295-303. 45 Bracco L, Gallato R, Grigoletto F, et al. Factors affecting course and survival in Alzheimer's disease. A 9-year longitudinal study. Arch Neurol. 1994 Dec;51(12):1213-9. 46 Loreck DJ, Bylsma FW, Folstein MF. A New Scale for Comprehensive Assessment of Psychopathology in Alzheimer's Disease. Am J Geriatr Psychiatry. 1994, 2:52-59. 47 Cummings JL, Mega M, Gray K, Rosenberg-Thompson S, Carusi DA, Gornbein J. The Neuropsychiatric Inventory: comprehensive assessment of psychopathology in dementia. Neurology. 1994, 44(12):2308-14. 48 International Psychogeriatric Association. Introduction to Behavioral and Psychological Symptoms of Dementia (Revised). http://www.ipa-online.org/ipaonlinev3/ipaprograms/bpsdarchives/bpsdrev/toc.asp. Accessed May 20, 2010. 49 Lyketsos CG, Lopez O, Jones B, Fitzpatrick AL, Breitner J, DeKosky S. Prevalence of neuropsychiatric symptoms in dementia and mild cognitive impairment: results from the Cardiovascular Health Study. JAMA. 2002; 288:1475-1483. 50 Ikeda M, Fukuhara R, Shigenobu K, et al. Dementia associated mental and behavioural disturbances in elderly people in the community: findings form the first Nakayama study. J Neurol Neurosurg Psychiatry. 2004; 75:146-148. 51 Liu CY, Wang PN, Lin KN, Liu HC. Behavioral and psychological symptoms in Taiwanese patients with Alzheimer’s disease. Int Psychogeriatr. 2007; 19:605-613.

© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
43
52 Zuidema SU, Derksen E, Verhey FR, Koopmans RT. Prevalence of neuropsychiatric symptoms in a large sample of Dutch nursing home patients with dementia. Int J Geriatr Psychiatry. 2007; 22:632-638. 53 Kverno KS, Black BS, Blass DM, Geiger-Brown J, Rabins PV. Neuropsychiatric symptom patterns in hospice-eligible nursing home residents with advanced dementia. J Am Med Dir Assoc. 2008; 7:509-15. 54 Chui HC, Lyness SA, Sobel E, Schneider LS. Extrapyramidal signs and psychiatric symptoms predict faster cognitive decline in Alzheimer's disease. Arch Neurol. 1994; 51:676–681. 55 Weiner MF, Hynan LS, Bret ME, White C,III. Early behavioral symptoms and course of Alzheimer’s disease. Acta Psychiatr Scand. 2005; 111:367-371. 56 Leger JM, Moulias R, Robert P, et al. Agitation and aggressiveness among the elderly population living in nursing or retirement homes in France. Int Psychogeriatr. 2002; 14:405-416. 57 Malone ML, Thompson L, Goodwin JS: Aggressive behaviors among the institutionalized elderly. J Am Geriatr Soc. 1993; 41:853-856. 58 Kunik ME, Snow AL, Molinari VA, et al. Health care utilization in dementia patients with psychiatric comorbidity. Gerontologist. 2003; 43:86-91. 59 Kunik ME, Cully JA, Snow L, Souchek J, Sullivan G, Ashton CM. Treatable comorbid conditions and use of VA health care services among patients with dementia. Psychiatr Serv. 2005; 56:70-75. 60 Steele C, Rovner B, Chase GA, Folstein M. Psychiatric symptoms and nursing home placement of patients with Alzheimer’s disease. Am J Psychiatry. 1990; 147:1049-1051. 61 Knopman DS, Berg JD, Thomas R, Grundman M, Thal LJ, Sano M, and for members of the Alzheimer’s Disease Cooperative Study. Nursing home placement is related to dementia progression: experience from a clinical trial. Neurology. 1999; 52:718-718. 62 Donaldson C, Tarrier N, Burns A. Determinants of carer stress in Alzheimer’s disease. Int J Geriatr Psychiatr. 1998; 13:248-256. 63 Miyamoto Y, Ito H, Otsuka T, Kurita H. Caregiver burden in mobile and non-mobile demented patients: a comparative study. Int J Geriatr Psychiatry. 2002; 17:765-773. 64 Snyder L, Jenkins C, Joosten L. Effectiveness of support groups for people with mild to moderate Alzheimer's disease: an evaluative survey. Am J Alzheimers Dis Other Demen. 2007; 22:14-19. 65 National Quality Forum (NQF). Composite Measure Evaluation Framework and National Voluntary Consensus Standards for Mortality and Safety—Composite Measures: A Consensus Report. Washington, DC: NQF;2009. 66 Lawlor B. Behavioral and psychological symptoms in dementia: the role of atypical antipsychotics. J Clin Psychiatry. 2004;65(Suppl 11):5–10. 67 Sink K, Holden K, Yaffe K. Pharmacological treatment of neuropsychiatric symptoms of dementia. JAMA. 2005;293:596–608. 68 Alexopoulos GS, Abrams RC, Young RC, Shamoian CA. Cornell scale for depression in dementia. Biol Psychiatry. 1988 Feb 1;23(3):271-84. 69 Qaseem A, Snow V, Cross JT. Current Pharmacologic Treatment of Dementia: A Clinical Practice Guideline from the American College of Physicians and the American Academy of Family Physicians. Ann Intern Med. 2008;148:370-378. 70 Lyketsos CG, Lee HB. Diagnosis and Treatment of Depression in Alzheimer's Disease A Practical Update for the Clinician. Dement Geriatr Cogn Disord. 2004;17:55-64. 71 Kalkonde YV, Pinto-Patarroyo GP, Goldman T, et al. Differences between clinical subspecialties in the outpatient evaluation and treatment of dementia in an academic medical center. Dement Geriatr Cogn Disord. 2010;29(1):28-36. 72 Gitlin LN, Schinfeld S, Winter L, Corcoran M, Boyce AA, Hauck W. Evaluating home environments of persons with dementia: interrater reliability and validity of the Home Environmental Assessment Protocol (HEAP). Disabil Rehabil. 2002, Vol. 24, No. 1-3, Pages 59-71. 73 Alzheimer’s Association. Position statement: Driving. Adopted by the Alzheimer’s Association Board of Directors, October 2001. Available at: http://www.alz.org/national/documents/statements_driving.pdf. Accessed February 16, 2011. 74 American Medical Association. Physician’s Guide to Assessing and Counseling Older Drivers. 2nd edition. 2010. http://www.ama-assn.org/ama/pub/physician-resources/public-health/promoting-healthy-lifestyles/geriatric-health/older-driver-safety.shtml. Accessed June 15, 2010. 75 Carr DB, Ott BR. The older adult driver With cognitive impairment. “It’s a frustrating life.” JAMA. 2010;303(16):1632-1641. 76 Volicer L. End-of-Life care for people with dementia in residential care settings. Alzheimer's Association; 2005. http://www.nccdp.org/resources/endoflifelitreview.pdf. Accessed August 31, 2010. 77 American Geriatrics Society (AGS). Geriatrics at your fingertips: Palliative and end-of-life care. In: Reuben DB, Herr KA, Pacala JT, et al., eds. Online edition: Geriatrics at your fingertips. 2010; 12th edition. http://www.geriatricsatyourfingertips.org. Accessed August 31, 2010. 78 Sachs GA, Shega JW, Cox-Haley D. Barriers to excellent end-of-life care for patients with dementia. J Gen Intern Med. 2004;19:1057e1063.

© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
44
79 Kim KY, Yeaman PA, Keene RL. End-of-life care for persons with Alzheimer's disease. Psychiatr Serv. 2005 Feb;56(2):139-41. 80 Mitchell SL, Teno JM, Kiely D, et al. The clinical course of advanced dementia. N Engl J Med. 2009 Oct 15 361 (16):1529-38. 81 Cavalieri TA, Latif W, Cieselski J, Ciervo CAJr, Forman LJ. How physicians approach advance care planning in patients with mild to moderate Alzheimer's disease. J Am Osteopath Assoc. 2002; 102(10):541-544. 82 Gaugler JE, Kane RL, Kane RA, Newcomer R. Unmet care needs and key outcomes in dementia. J Am Geriatr Soc. 2005;53:2098–2105. 83 Mittelman MS, Haley WE, Clay OJ, Roth DL. Improving caregiver well-being delays nursing home placement of patients with Alzheimer disease. Neurology. 2006;67:1592–1599.

© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
1
American Academy of Neurology American Geriatrics Society
American Medical Directors Association American Psychiatric Association
Physician Consortium for Performance Improvement® (PCPI™)
Dementia Administrative Claims Specifications
Appendix A
PCPI Approved October 2011
© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
2
Technical Specifications: Introduction
There are several data sources available for collecting performance measures, generally requiring different sets of measure specifications, due to the structure of the systems storing the data. The PCPI recognizes that electronic health records (EHRs) are the state of the art for clinical encounters and is focusing significant resources and expertise toward specifying and testing measures within EHRs, as they hold the promise of providing the relevant clinical data for measures and for providing feedback to physicians and other health care providers that is timely and actionable.
The following measure specifications include a listing of data elements required for collection of the measures in Electronic Health Records (EHRs).
The following measure specifications are divided into four distinct categories, based on the data source that is available to the provider or organization seeking to improve the quality of care delivered to their patients. The PCPI recognizes that such data are usually available only to health plans (public or private) or self-insured employers, but urges that, wherever possible, these data be shared with physician practices. The PCPI specifies the medications that apply to each medication-related measure. National Drug Code (NDC) lists for medication-related measures have been used in the past, however due to the movement nationally to use RxNorm within EHRs for medications, the PCPI has begun to use RxNorm in its quality measure specifications where EHR is the data source for medications.
Quality Reporting and Electronic Health Records: Overview
Specifications to collect and report on the Dementia measures are included in this document. In light of recent national initiatives to encourage physicians and other health care professionals to adopt and implement Electronic Health Records (EHRs) in their practices, we highlight here some of the current PCPI activities to promote use of these measures within EHRs. Integration with EHRs (HQMF and eMeasure) The Collaborative for Performance Measure Integration with EHRS--co-sponsored by the AMA, NCQA, and the HIMSS Electronic Health Record Association (EHRA)-- works with measure developers, EHR providers, and clinical users of EHRs to advance the use of measures within EHRs (see www.ama-assn.org/go/collaborative ). Among its work, the Collaborative developed a standard Health Quality Measure Format (available at HQMF.org) for use by EHRs and other IT providers to incorporate measure specifications within their systems. In Spring 2009, The National Quality Forum (NQF) funded an initiative to take the prototype HQMF XML, now referred to as an “eMeasure,” and align it with constructs previously defined by HL7 - including the HL7 Reference Information Model (RIM). The HQMF eMeasure was balloted and subsequently approved as an HL7 Draft Standard for Trial Use (DSTU) in February 2010.
Definition of Terms for Electronic Health Record (EHR) Specifications
The PCPI provides definitions for terms that are in use in the Health Information Technology and Quality Measure arenas to describe quality measure specifications. Electronic Specification (eSpecification) eSpecification, syn, EHR specification –a generic term used to describe a performance measure specification that includes information to facilitate the integration and interpretation of performance measures in electronic health records. eMeasure The translation of an eSpecification in computer readable format (XML) that has a specification in accordance with the HQMF (Health Quality Measure Format), an HL7 Draft Standard for Trial Use (DSTU). PCPI eSpecification A type of eSpecification developed by the PCPI that includes the following:
text description data elements (including constraints and attributes) visual representation of the measure logic mathematical expression to calculate the measure performance rates and exception
rates
© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
3
relevant value sets The PCPI eSpecification is “human readable” and useable by anyone wishing to understand how the data elements for a measure are constructed and combined to calculate quality measure performance and exception rates. It can also be used by a software developer to translate the quality measure specification into the HQMF eMeasure format. It is the PCPI’s objective that the PCPI eSpecifications will serve as the basis from which the HQMF eMeasure is developed. The development of the PCPI eSpecifications will ensure that the intent of the PCPI measure is preserved when it is translated into the eMeasure format.
Technical Specifications for Different Data Sources
The PCPI develops technical specifications for multiple data sources, including: Electronic Health Record (EHR) Data Electronic Administrative Data (Claims), which may include specifications for:
o Prospective Claims-based reporting (using CPT Category II codes) o Retrospective Claims Analysis
Expanded (multiple-source) Administrative Data Paper Medical Record Data/ Data Collection Flowsheet
We have included the recommended data source, given that not all measures are feasible for collection and reporting from all data sources. Electronic Health Record (EHR) Data Specification of the performance measure by the PCPI is critical to ensure that the intent of the measure is accurately represented prior to being integrated into an EHR. Complete PCPI eSpecifications will be developed once the Dementia measures have been finalized by the PCPI Measure Development Workgroup. It is anticipated that many meaningful, accurate and reliable performance measures can be computed relying on EHR data. Our measure specifications currently include relevant coding and logic to query an EHR for data and compute the measure provided in words and tables consistent with the National Quality Forum’s Quality Data Model, version 2.1 (QDM). We recognize that not all EHRs in use have the functionalities to support every data element required for these measures and, in some cases, such functionalities are available but are not being used. Our intent, therefore, is to prioritize measures for EHR integration in order to provide a roadmap for EHR developers and users of EHR systems Electronic Administrative Data (Claims) Electronic Administrative Data are typically used for reporting clinical services provided to the patient by the physician or physician group practice to third party payers, including diagnosis (ICD-9-CM) codes and service/procedure (CPT Category I) codes. In some cases, this information can be analyzed to provide quality of care information. Supplemental tracking codes (CPT Category II) are developed for performance measurement collection and reporting through a claims-based system. CPT Category II codes are optional tracking codes that can be included on the claim for quality measure reporting, but are not required in order to process the claim for reimbursement. The calculation of performance measure information is determined by the claim form composition. Some claims will solely include reimbursement codes and others will include a combination of reimbursement and supplemental tracking codes. Some performance measures may not require the supplemental tracking codes be present on the claim form in order for the measure to be calculated, but this is not the case for all measures. Until expanded and linked administrative databases or electronic health record systems are more widely available and utilized, various pay-for-performance and pay-for-reporting programs (including the Physician Quality Reporting System [PQRS] of the Centers for Medicare and Medicaid Services [CMS]) continue to rely on this type of claims data. Expanded (multiple-source) Administrative Data Expanded Administrative Data are routinely captured during the course of care delivery through either payment or care documentation purposes and accessible through the use of large electronic databases. Multiple organizations may gather such electronic data, including health plans (e.g., medical claims), health systems (e.g., patient registries), and large data aggregators or warehouses. In addition to physician claims data (as described above), these databases may aggregate data from multiple care settings (e.g. outpatient, inpatient, emergency department and other sites of care) and may include data elements not typically available on physician claims (e.g., pharmacy and laboratory data). While this data source enables the use of large data sets that can be joined and analyzed through complex, programmed algorithms, most data are currently confined to coded diagnosis and procedural claims and typically do not include more robust clinical detail.

© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
4
Paper Medical Record Data/ Data Collection Flowsheet Information from the paper medical record may be manually abstracted by prospective or retrospective manual review of clinical encounter information. Medical record data, despite being more expensive to acquire, can provide much richer clinical information usually not available in electronic transactional data, alongside typical administrative claims information from the patient encounter.
Data Elements for Electronic Health Record (EHR) Integration
PCPI Specifications Staff have identified the data elements required to collect and calculate the Dementia measures in an electronic health record. The identification of data elements is the first step in developing specifications for implementation in an Electronic Health Record (EHR). The data elements that follow are classified according to the National Quality Forum’s Quality Model, Version 2.1 (QDM). The QDM is a framework that can be used to clearly define concepts used in quality measures and clinical care. It provides a standardized method to describe data elements for electronic health record capture. Additional background information on the Quality Data Set can be found on the NQF Website at: http://www.qualityforum.org/Projects/h/QDS_Model/Quality_Data_Model.aspx Once the Dementia measures have completed the public comment process and are finalized by the Dementia Work Group, the PCPI eSpecifications (referenced above) will be developed. PCPI Staff welcomes comments on the representation of the data elements included here for public comment.
Measure Exceptions
For process measures, the PCPI provides three categories of reasons for which a patient may be excluded from the denominator of an individual measure:
Medical reasons Includes:
- not indicated (absence of organ/limb, already received/performed, other) - contraindicated (patient allergic history, potential adverse drug interaction, other)
Patient reasons
Includes: - patient declined - social or religious reasons - other patient reasons
System reasons
Includes: - resources to perform the services not available - insurance coverage/payor-related limitations - other reasons attributable to health care delivery system
These measure exception categories are not available uniformly across all measures; for each measure, there must be a clear rationale to permit an exception for a medical, patient, or system reason. Where possible, examples have been provided in the measure exception language of instances that would constitute an exception. Examples are intended to guide clinicians and are not all-inclusive lists of all possible reasons why a patient could be excluded from a measure. When using CPT Category II codes to report the measure, the exception of a patient should be reported by appending the appropriate modifier to the CPT Category II code designated for the measure:
Medical reasons: modifier 1P Patient reasons: modifier 2P System reasons: modifier 3P
Although this methodology does not require the external reporting of more detailed exception data, the PCPI recommends that clinicians document the specific reasons for exception in patients’ medical records for purposes of optimal patient management and audit-readiness. The PCPI also advocates the systematic review and analysis of each clinician’s exceptions data to identify practice patterns and opportunities for quality improvement. For example, it is possible for implementers to calculate the percentage of patients that clinicians have identified as meeting the criteria for exception.

© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
5
Please refer to documentation for each individual measure for information on the acceptable exception categories and the codes and modifiers to be used for reporting.

Administrative Claims Specifications PCPI APPROVED
Dementia
© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
6
Measure #1 – Staging of Dementia
Denominator (Eligible Population)
All patients, regardless of age, with a diagnosis of dementia ICD-9-CM Diagnosis Codes: Code Descriptor Neurosyphilis 094.1 Neurosyphilis, General paresis
Dementias 290.0 Senile dementia, uncomplicated
290.10 Presenile dementia, uncomplicated 290.11 Presenile dementia with delirium 290.12 Presenile dementia with delusional features 290.13 Presenile dementia with depressive features 290.20 Senile dementia with delusional features 290.21 Senile dementia with depressive features 290.3 Senile dementia with delirium
290.40 Vascular dementia, uncomplicated 290.41 Vascular dementia with delirium 290.42 Vascular dementia with delusions 290.43 Vascular dementia with depressed mood 290.8 Other specified senile psychotic conditions 290.9 Unspecified senile psychotic condition
Persistent Mental Disorders due to Conditions Classified Elsewhere 294.10 Dementia in conditions classified elsewhere without
behavioral disturbance 294.11 Dementia in conditions classified elsewhere with behavioral
disturbance 294.20 Dementia, unspecified, without behavioral disturbance 294.21 Dementia, unspecified, with behavioral disturbance 294.8 Other persistent mental disorders due to conditions classified
elsewhere Other cerebral degenerations 331.0 Alzheimer’s disease
331.11 Pick’s disease 331.19 Other frontotemporal dementia 331.82 Dementia with Lewy bodies
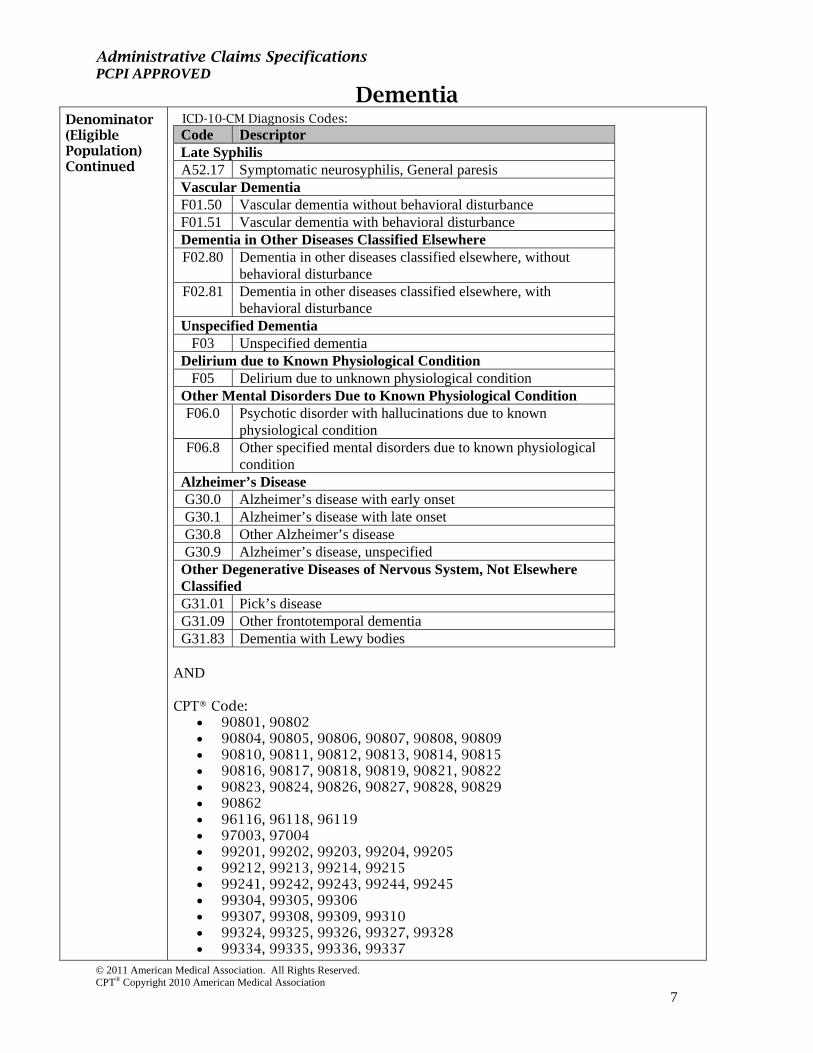
Administrative Claims Specifications PCPI APPROVED
Dementia
© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
7
Denominator (Eligible Population) Continued
ICD-10-CM Diagnosis Codes: Code Descriptor Late Syphilis A52.17 Symptomatic neurosyphilis, General paresis Vascular Dementia F01.50 Vascular dementia without behavioral disturbance F01.51 Vascular dementia with behavioral disturbance Dementia in Other Diseases Classified Elsewhere F02.80 Dementia in other diseases classified elsewhere, without
behavioral disturbance F02.81 Dementia in other diseases classified elsewhere, with
behavioral disturbance Unspecified Dementia
F03 Unspecified dementia Delirium due to Known Physiological Condition
F05 Delirium due to unknown physiological condition Other Mental Disorders Due to Known Physiological Condition F06.0 Psychotic disorder with hallucinations due to known
physiological condition F06.8 Other specified mental disorders due to known physiological
condition Alzheimer’s Disease G30.0 Alzheimer’s disease with early onset G30.1 Alzheimer’s disease with late onset G30.8 Other Alzheimer’s disease G30.9 Alzheimer’s disease, unspecified
Other Degenerative Diseases of Nervous System, Not Elsewhere Classified G31.01 Pick’s disease G31.09 Other frontotemporal dementia G31.83 Dementia with Lewy bodies
AND CPT® Code:
90801, 90802 90804, 90805, 90806, 90807, 90808, 90809 90810, 90811, 90812, 90813, 90814, 90815 90816, 90817, 90818, 90819, 90821, 90822 90823, 90824, 90826, 90827, 90828, 90829 90862 96116, 96118, 96119 97003, 97004 99201, 99202, 99203, 99204, 99205 99212, 99213, 99214, 99215 99241, 99242, 99243, 99244, 99245 99304, 99305, 99306 99307, 99308, 99309, 99310 99324, 99325, 99326, 99327, 99328 99334, 99335, 99336, 99337
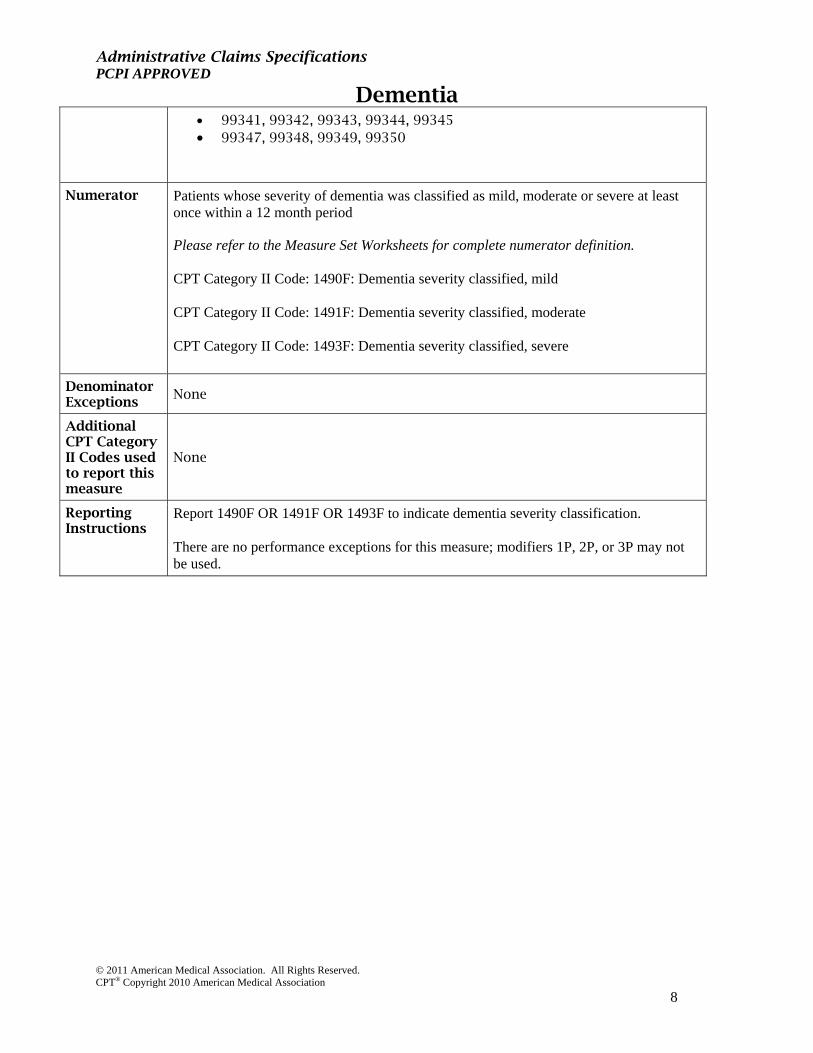
Administrative Claims Specifications PCPI APPROVED
Dementia
© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
8
99341, 99342, 99343, 99344, 99345 99347, 99348, 99349, 99350
Numerator Patients whose severity of dementia was classified as mild, moderate or severe at least once within a 12 month period Please refer to the Measure Set Worksheets for complete numerator definition. CPT Category II Code: 1490F: Dementia severity classified, mild CPT Category II Code: 1491F: Dementia severity classified, moderate CPT Category II Code: 1493F: Dementia severity classified, severe
Denominator Exceptions
None
Additional CPT Category II Codes used to report this measure
None
Reporting Instructions
Report 1490F OR 1491F OR 1493F to indicate dementia severity classification. There are no performance exceptions for this measure; modifiers 1P, 2P, or 3P may not be used.

Administrative Claims Specifications PCPI APPROVED
Dementia
© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
9
Measure #2 - Cognitive Assessment
Denominator (Eligible Population)
All patients, regardless of age, with a diagnosis of dementia ICD-9-CM Diagnosis Codes: Code Descriptor Neurosyphilis 094.1 Neurosyphilis, General paresis
Dementias 290.0 Senile dementia, uncomplicated
290.10 Presenile dementia, uncomplicated 290.11 Presenile dementia with delirium 290.12 Presenile dementia with delusional features 290.13 Presenile dementia with depressive features 290.20 Senile dementia with delusional features 290.21 Senile dementia with depressive features 290.3 Senile dementia with delirium
290.40 Vascular dementia, uncomplicated 290.41 Vascular dementia with delirium 290.42 Vascular dementia with delusions 290.43 Vascular dementia with depressed mood 290.8 Other specified senile psychotic conditions 290.9 Unspecified senile psychotic condition
Persistent Mental Disorders due to Conditions Classified Elsewhere 294.10 Dementia in conditions classified elsewhere without
behavioral disturbance 294.11 Dementia in conditions classified elsewhere with behavioral
disturbance 294.20 Dementia, unspecified, without behavioral disturbance 294.21 Dementia, unspecified, with behavioral disturbance 294.8 Other persistent mental disorders due to conditions classified
elsewhere Other cerebral degenerations 331.0 Alzheimer’s disease
331.11 Pick’s disease 331.19 Other frontotemporal dementia 331.82 Dementia with Lewy bodies

Administrative Claims Specifications PCPI APPROVED
Dementia
© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
10
Denominator (Eligible Population) Continued
ICD-10-CM Diagnosis Codes: Code Descriptor Late Syphilis A52.17 Symptomatic neurosyphilis, General paresis Vascular Dementia F01.50 Vascular dementia without behavioral disturbance F01.51 Vascular dementia with behavioral disturbance Dementia in Other Diseases Classified Elsewhere F02.80 Dementia in other diseases classified elsewhere, without
behavioral disturbance F02.81 Dementia in other diseases classified elsewhere, with
behavioral disturbance Unspecified Dementia
F03 Unspecified dementia Delirium due to Known Physiological Condition
F05 Delirium due to unknown physiological condition Other Mental Disorders Due to Known Physiological Condition F06.0 Psychotic disorder with hallucinations due to known
physiological condition F06.8 Other specified mental disorders due to known physiological
condition Alzheimer’s Disease G30.0 Alzheimer’s disease with early onset G30.1 Alzheimer’s disease with late onset G30.8 Other Alzheimer’s disease G30.9 Alzheimer’s disease, unspecified
Other Degenerative Diseases of Nervous System, Not Elsewhere Classified G31.01 Pick’s disease G31.09 Other frontotemporal dementia G31.83 Dementia with Lewy bodies
AND CPT® Code:
90801, 90802 90804, 90805, 90806, 90807, 90808, 90809 90810, 90811, 90812, 90813, 90814, 90815 90816, 90817, 90818, 90819, 90821, 90822 90823, 90824, 90826, 90827, 90828, 90829 90862 96116, 96118, 96119, 96120 97003, 97004 99201, 99202, 99203, 99204, 99205 99212, 99213, 99214, 99215 99241, 99242, 99243, 99244, 99245 99304, 99305, 99306 99307, 99308, 99309, 99310 99324, 99325, 99326, 99327, 99328

Administrative Claims Specifications PCPI APPROVED
Dementia
© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
11
99334, 99335, 99336, 99337 99341, 99342, 99343, 99344, 99345 99347, 99348, 99349, 99350
Numerator Patients for whom an assessment of cognition is performed and the results reviewed at least once within a 12 month period Please refer to the Measure Set Worksheets for complete numerator definition. CPT Category II Code: 1494F: Cognition assessed and reviewed
Denominator Exceptions
Documentation of medical reason(s) for not assessing cognition (eg, patient at end of life, other medical reason)
Append modifier to CPT II code 1494F-1P Documentation of patient reason(s) for not assessing cognition
Append modifier to CPT II code 1494F-2P
Additional CPT Category II Codes used to report this measure
None
Reporting Instructions
Report 1494F if assessment of cognition is performed and the results reviewed. For patient with appropriate exception criteria report 1494F with modifier -1P or -2P.

Administrative Claims Specifications PCPI APPROVED
Dementia
© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
12
Measure #3 – Functional Status Assessment
Denominator (Eligible Population)
All patients, regardless of age, with a diagnosis of dementia ICD-9-CM Diagnosis Codes: Code Descriptor Neurosyphilis 094.1 Neurosyphilis, General paresis
Dementias 290.0 Senile dementia, uncomplicated
290.10 Presenile dementia, uncomplicated 290.11 Presenile dementia with delirium 290.12 Presenile dementia with delusional features 290.13 Presenile dementia with depressive features 290.20 Senile dementia with delusional features 290.21 Senile dementia with depressive features 290.3 Senile dementia with delirium
290.40 Vascular dementia, uncomplicated 290.41 Vascular dementia with delirium 290.42 Vascular dementia with delusions 290.43 Vascular dementia with depressed mood 290.8 Other specified senile psychotic conditions 290.9 Unspecified senile psychotic condition
Persistent Mental Disorders due to Conditions Classified Elsewhere 294.10 Dementia in conditions classified elsewhere without
behavioral disturbance 294.11 Dementia in conditions classified elsewhere with behavioral
disturbance 294.20 Dementia, unspecified, without behavioral disturbance 294.21 Dementia, unspecified, with behavioral disturbance 294.8 Other persistent mental disorders due to conditions classified
elsewhere Other cerebral degenerations 331.0 Alzheimer’s disease
331.11 Pick’s disease 331.19 Other frontotemporal dementia 331.82 Dementia with Lewy bodies
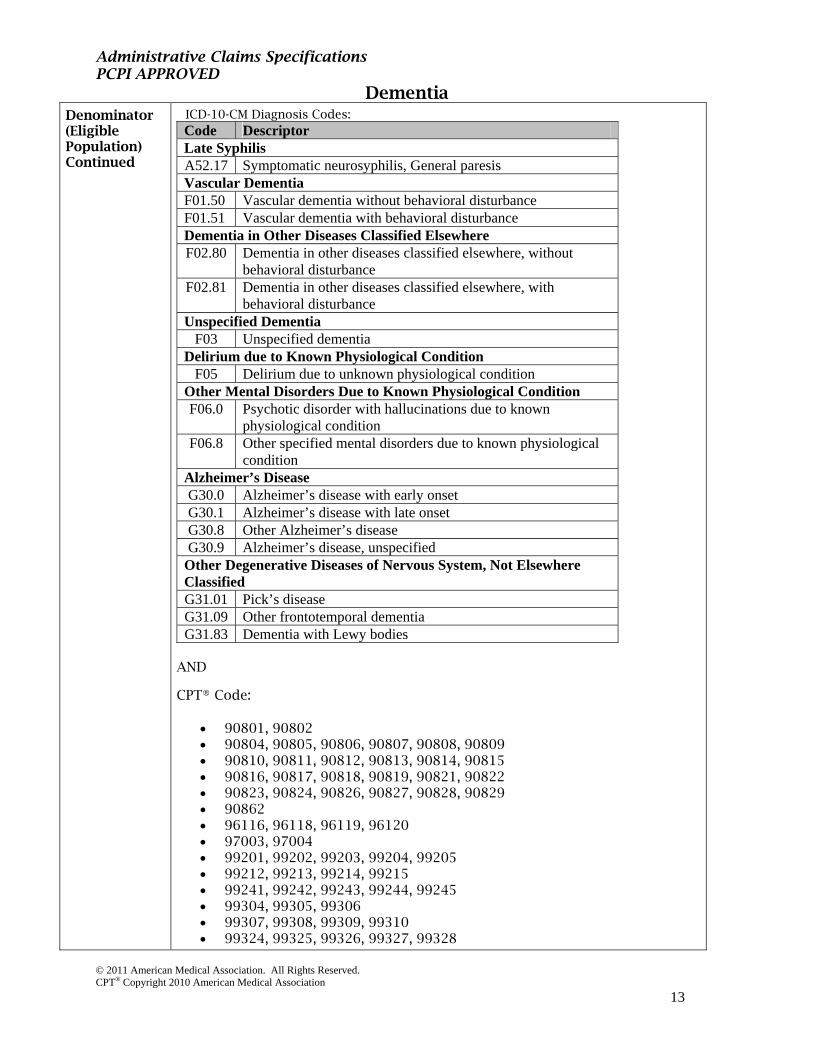
Administrative Claims Specifications PCPI APPROVED
Dementia
© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
13
Denominator (Eligible Population) Continued
ICD-10-CM Diagnosis Codes: Code Descriptor Late Syphilis A52.17 Symptomatic neurosyphilis, General paresis Vascular Dementia F01.50 Vascular dementia without behavioral disturbance F01.51 Vascular dementia with behavioral disturbance Dementia in Other Diseases Classified Elsewhere F02.80 Dementia in other diseases classified elsewhere, without
behavioral disturbance F02.81 Dementia in other diseases classified elsewhere, with
behavioral disturbance Unspecified Dementia
F03 Unspecified dementia Delirium due to Known Physiological Condition
F05 Delirium due to unknown physiological condition Other Mental Disorders Due to Known Physiological Condition F06.0 Psychotic disorder with hallucinations due to known
physiological condition F06.8 Other specified mental disorders due to known physiological
condition Alzheimer’s Disease G30.0 Alzheimer’s disease with early onset G30.1 Alzheimer’s disease with late onset G30.8 Other Alzheimer’s disease G30.9 Alzheimer’s disease, unspecified
Other Degenerative Diseases of Nervous System, Not Elsewhere Classified G31.01 Pick’s disease G31.09 Other frontotemporal dementia G31.83 Dementia with Lewy bodies
AND CPT® Code:
90801, 90802 90804, 90805, 90806, 90807, 90808, 90809 90810, 90811, 90812, 90813, 90814, 90815 90816, 90817, 90818, 90819, 90821, 90822 90823, 90824, 90826, 90827, 90828, 90829 90862 96116, 96118, 96119, 96120 97003, 97004 99201, 99202, 99203, 99204, 99205 99212, 99213, 99214, 99215 99241, 99242, 99243, 99244, 99245 99304, 99305, 99306 99307, 99308, 99309, 99310 99324, 99325, 99326, 99327, 99328

Administrative Claims Specifications PCPI APPROVED
Dementia
© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
14
99334, 99335, 99336, 99337 99341, 99342, 99343, 99344, 99345 99347, 99348, 99349, 99350
Numerator Patients for whom an assessment of functional status is performed and the results reviewed at least once within a 12 month period Please refer to the Measure Set Worksheets for complete numerator definition. CPT Category II Code: 1175F: Functional status for dementia assessed and results reviewed
Denominator Exceptions
Documentation of medical reason(s) for not assessing functional status (eg, patient is severely impaired and caregiver knowledge is limited, other medical reason)
Append modifier to CPT II code 1175F-1P
Additional CPT Category II Codes used to report this measure
None
Reporting Instructions
Report 1175F if assessment of functional status is performed and the results reviewed. For the patient with appropriate exception criteria, report 1175F with modifier -1P.

Administrative Claims Specifications PCPI APPROVED
Dementia
© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
15
Measure #4 – Neuropsychiatric Symptom Assessment
This measure is paired with Measure #5 – Management of Neuropsychiatric Symptoms Implementers of this measure should not use Measure #4 without Measure #5.
Denominator (Eligible Population)
All patients, regardless of age, with a diagnosis of dementia ICD-9-CM Diagnosis Codes: Code Descriptor Neurosyphilis 094.1 Neurosyphilis, General paresis
Dementias 290.0 Senile dementia, uncomplicated
290.10 Presenile dementia, uncomplicated 290.11 Presenile dementia with delirium 290.12 Presenile dementia with delusional features 290.13 Presenile dementia with depressive features 290.20 Senile dementia with delusional features 290.21 Senile dementia with depressive features 290.3 Senile dementia with delirium
290.40 Vascular dementia, uncomplicated 290.41 Vascular dementia with delirium 290.42 Vascular dementia with delusions 290.43 Vascular dementia with depressed mood 290.8 Other specified senile psychotic conditions 290.9 Unspecified senile psychotic condition
Persistent Mental Disorders due to Conditions Classified Elsewhere 294.10 Dementia in conditions classified elsewhere without
behavioral disturbance 294.11 Dementia in conditions classified elsewhere with behavioral
disturbance 294.20 Dementia, unspecified, without behavioral disturbance 294.21 Dementia, unspecified, with behavioral disturbance 294.8 Other persistent mental disorders due to conditions classified
elsewhere Other cerebral degenerations 331.0 Alzheimer’s disease
331.11 Pick’s disease 331.19 Other frontotemporal dementia 331.82 Dementia with Lewy bodies

Administrative Claims Specifications PCPI APPROVED
Dementia
© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
16
Denominator (Eligible Population) Continued
ICD-10-CM Diagnosis Codes: Code Descriptor Late Syphilis A52.17 Symptomatic neurosyphilis, General paresis Vascular Dementia F01.50 Vascular dementia without behavioral disturbance F01.51 Vascular dementia with behavioral disturbance Dementia in Other Diseases Classified Elsewhere F02.80 Dementia in other diseases classified elsewhere, without
behavioral disturbance F02.81 Dementia in other diseases classified elsewhere, with
behavioral disturbance Unspecified Dementia
F03 Unspecified dementia Delirium due to Known Physiological Condition
F05 Delirium due to unknown physiological condition Other Mental Disorders Due to Known Physiological Condition F06.0 Psychotic disorder with hallucinations due to known
physiological condition F06.8 Other specified mental disorders due to known physiological
condition Alzheimer’s Disease G30.0 Alzheimer’s disease with early onset G30.1 Alzheimer’s disease with late onset G30.8 Other Alzheimer’s disease G30.9 Alzheimer’s disease, unspecified
Other Degenerative Diseases of Nervous System, Not Elsewhere Classified G31.01 Pick’s disease G31.09 Other frontotemporal dementia G31.83 Dementia with Lewy bodies
AND CPT® Code:
90801, 90802 90804, 90805, 90806, 90807, 90808, 90809 90810, 90811, 90812, 90813, 90814, 90815 90816, 90817, 90818, 90819, 90821, 90822 90823, 90824, 90826, 90827, 90828, 90829 90862 96116, 96118, 96119 96150, 96151 97003, 97004 99201, 99202, 99203, 99204, 99205 99212, 99213, 99214, 99215 99241, 99242, 99243, 99244, 99245 99304, 99305, 99306 99307, 99308, 99309, 99310 99324, 99325, 99326, 99327, 99328

Administrative Claims Specifications PCPI APPROVED
Dementia
© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
17
99334, 99335, 99336, 99337 99341, 99342, 99343, 99344, 99345 99347, 99348, 99349, 99350
Numerator Patients for whom an assessment of neuropsychiatric symptoms is performed and results reviewed at least once in a 12 month period Please refer to the Measure Set Worksheets for complete numerator definition. CPT Category II Code 1181F: Neuropsychiatric symptoms assessed and results reviewed
Denominator Exceptions
None
Additional CPT Category II Codes used to report this measure
None
Reporting Instructions
This measure is paired with measure #5- Management of Neuropsychiatric Symptoms. Implementers of this measure should not use this Neuropsychiatric Symptom Assessment without the Management of Neuropsychiatric Symptoms measure. Report 1181F if assessment of neuropsychiatric symptoms performed and results reviewed. There are no performance exceptions for this measure; modifiers 1P, 2P, or 3P may not be used.

Administrative Claims Specifications PCPI APPROVED
Dementia
© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
18
Measure #5 – Management of Neuropsychiatric Symptoms
This measure is paired with Measure #4 – Neuropsychiatric Symptom Assessment. Implementers of this measure should not use Measure #5 without Measure #4.
Denominator (Eligible Population)
All patients, regardless of age, with a diagnosis of dementia ICD-9-CM Diagnosis Codes: Code Descriptor Neurosyphilis 094.1 Neurosyphilis, General paresis
Dementias 290.0 Senile dementia, uncomplicated
290.10 Presenile dementia, uncomplicated 290.11 Presenile dementia with delirium 290.12 Presenile dementia with delusional features 290.13 Presenile dementia with depressive features 290.20 Senile dementia with delusional features 290.21 Senile dementia with depressive features 290.3 Senile dementia with delirium
290.40 Vascular dementia, uncomplicated 290.41 Vascular dementia with delirium 290.42 Vascular dementia with delusions 290.43 Vascular dementia with depressed mood 290.8 Other specified senile psychotic conditions 290.9 Unspecified senile psychotic condition
Persistent Mental Disorders due to Conditions Classified Elsewhere 294.10 Dementia in conditions classified elsewhere without
behavioral disturbance 294.11 Dementia in conditions classified elsewhere with behavioral
disturbance 294.20 Dementia, unspecified, without behavioral disturbance 294.21 Dementia, unspecified, with behavioral disturbance 294.8 Other persistent mental disorders due to conditions classified
elsewhere Other cerebral degenerations 331.0 Alzheimer’s disease
331.11 Pick’s disease 331.19 Other frontotemporal dementia 331.82 Dementia with Lewy bodies

Administrative Claims Specifications PCPI APPROVED
Dementia
© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
19
Denominator (Eligible Population) Continued
ICD-10-CM Diagnosis Codes: Code Descriptor Late Syphilis A52.17 Symptomatic neurosyphilis, General paresis Vascular Dementia F01.50 Vascular dementia without behavioral disturbance F01.51 Vascular dementia with behavioral disturbance Dementia in Other Diseases Classified Elsewhere F02.80 Dementia in other diseases classified elsewhere, without
behavioral disturbance F02.81 Dementia in other diseases classified elsewhere, with
behavioral disturbance Unspecified Dementia
F03 Unspecified dementia Delirium due to Known Physiological Condition
F05 Delirium due to unknown physiological condition Other Mental Disorders Due to Known Physiological Condition F06.0 Psychotic disorder with hallucinations due to known
physiological condition F06.8 Other specified mental disorders due to known physiological
condition Alzheimer’s Disease G30.0 Alzheimer’s disease with early onset G30.1 Alzheimer’s disease with late onset G30.8 Other Alzheimer’s disease G30.9 Alzheimer’s disease, unspecified
Other Degenerative Diseases of Nervous System, Not Elsewhere Classified G31.01 Pick’s disease G31.09 Other frontotemporal dementia G31.83 Dementia with Lewy bodies
AND CPT® Code:
90801, 90802 90804, 90805, 90806, 90807, 90808, 90809 90810, 90811, 90812, 90813, 90814, 90815 90816, 90817, 90818, 90819, 90821, 90822 90823, 90824, 90826, 90827, 90828, 90829 90862 96150, 96151, 96152, 96154, 96155 97003, 97004 99201, 99202, 99203, 99204, 99205 99212, 99213, 99214, 99215 99241, 99242, 99243, 99244, 99245 99304, 99305, 99306 99307, 99308, 99309, 99310 99324, 99325, 99326, 99327, 99328

Administrative Claims Specifications PCPI APPROVED
Dementia
© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
20
99334, 99335, 99336, 99337 99341, 99342, 99343, 99344, 99345 99347, 99348, 99349, 99350
Numerator Patients who received or were recommended to receive an intervention for neuropsychiatric symptoms within a 12 month period Please refer to the Measure Set Worksheets for complete numerator definition. CPT Category II Code 4525F: Neuropsychiatric intervention ordered
CPT Category II Code 4526F: Neuropsychiatric intervention received
Denominator Exceptions
None
Additional CPT Category II Codes used to report this measure
1182F: Neuropsychiatric symptoms, one or more present
1183F: Neuropsychiatric symptoms, absent
Reporting Instructions
This measure is paired with Measure #4 – Neuropsychiatric Symptom Assessment. Implementers of this measure should not use this measure without the Neuropsychiatric Symptom Assessment measure.
Report 1182F OR 1183F to indicate the number of neuropsychiatric symptoms. If one or more neuropsychiatric symptoms is present (1182F), report 4525F if patient was recommended to receive or report 4526F if patient has received an intervention for neuropsychiatric symptoms. There are no performance exceptions for this measure; modifiers 1P, 2P, or 3P may not be used.

Administrative Claims Specifications PCPI APPROVED
Dementia
© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
21
Measure #6 – Screening for Depressive Symptoms
Denominator (Eligible Population)
All patients, regardless of age, with a diagnosis of dementia ICD-9-CM Diagnosis Codes: Code Descriptor Neurosyphilis 094.1 Neurosyphilis, General paresis
Dementias 290.0 Senile dementia, uncomplicated
290.10 Presenile dementia, uncomplicated 290.11 Presenile dementia with delirium 290.12 Presenile dementia with delusional features 290.13 Presenile dementia with depressive features 290.20 Senile dementia with delusional features 290.21 Senile dementia with depressive features 290.3 Senile dementia with delirium
290.40 Vascular dementia, uncomplicated 290.41 Vascular dementia with delirium 290.42 Vascular dementia with delusions 290.43 Vascular dementia with depressed mood 290.8 Other specified senile psychotic conditions 290.9 Unspecified senile psychotic condition
Persistent Mental Disorders due to Conditions Classified Elsewhere 294.10 Dementia in conditions classified elsewhere without
behavioral disturbance 294.11 Dementia in conditions classified elsewhere with behavioral
disturbance 294.20 Dementia, unspecified, without behavioral disturbance 294.21 Dementia, unspecified, with behavioral disturbance 294.8 Other persistent mental disorders due to conditions classified
elsewhere Other cerebral degenerations 331.0 Alzheimer’s disease
331.11 Pick’s disease 331.19 Other frontotemporal dementia 331.82 Dementia with Lewy bodies

Administrative Claims Specifications PCPI APPROVED
Dementia
© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
22
Denominator (Eligible Population) Continued
ICD-10-CM Diagnosis Codes: Code Descriptor Late Syphilis A52.17 Symptomatic neurosyphilis, General paresis Vascular Dementia F01.50 Vascular dementia without behavioral disturbance F01.51 Vascular dementia with behavioral disturbance Dementia in Other Diseases Classified Elsewhere F02.80 Dementia in other diseases classified elsewhere, without
behavioral disturbance F02.81 Dementia in other diseases classified elsewhere, with
behavioral disturbance Unspecified Dementia
F03 Unspecified dementia Delirium due to Known Physiological Condition
F05 Delirium due to unknown physiological condition Other Mental Disorders Due to Known Physiological Condition F06.0 Psychotic disorder with hallucinations due to known
physiological condition F06.8 Other specified mental disorders due to known physiological
condition Alzheimer’s Disease G30.0 Alzheimer’s disease with early onset G30.1 Alzheimer’s disease with late onset G30.8 Other Alzheimer’s disease G30.9 Alzheimer’s disease, unspecified
Other Degenerative Diseases of Nervous System, Not Elsewhere Classified G31.01 Pick’s disease G31.09 Other frontotemporal dementia G31.83 Dementia with Lewy bodies
AND CPT® Code:
90801, 90802 90804, 90805, 90806, 90807, 90808, 90809 90810, 90811, 90812, 90813, 90814, 90815 90816, 90817, 90818, 90819, 90821, 90822 90823, 90824, 90826, 90827, 90828, 90829 90862 96101, 96102, 96103 96116, 96118, 96119, 96120 96150, 96151 97003, 97004 99201, 99202, 99203, 99204, 99205 99212, 99213, 99214, 99215 99241, 99242, 99243, 99244, 99245 99304, 99305, 99306

Administrative Claims Specifications PCPI APPROVED
Dementia
© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
23
99307, 99308, 99309, 99310 99324, 99325, 99326, 99327, 99328 99334, 99335, 99336, 99337 99341, 99342, 99343, 99344, 99345 99347, 99348, 99349, 99350
Numerator Patients who were screened for depressive symptoms within a 12 month period Please refer to the Measure Set Worksheets for complete numerator definition. CPT Category II Code 3725F: Screening for depression performed
Denominator Exceptions
None
Additional CPT Category II Codes used to report this measure
None
Reporting Instructions
Report 3725F if patient was screened for depressive symptoms. There are no performance exceptions for this measure; modifiers 1P, 2P or 3P may not be used.

Administrative Claims Specifications PCPI APPROVED
Dementia
© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
24
Measure #7 – Counseling Regarding Safety Concerns
Denominator (Eligible Population)
All patients, regardless of age, with a diagnosis of dementia ICD-9-CM Diagnosis Codes: Code Descriptor Neurosyphilis 094.1 Neurosyphilis, General paresis
Dementias 290.0 Senile dementia, uncomplicated
290.10 Presenile dementia, uncomplicated 290.11 Presenile dementia with delirium 290.12 Presenile dementia with delusional features 290.13 Presenile dementia with depressive features 290.20 Senile dementia with delusional features 290.21 Senile dementia with depressive features 290.3 Senile dementia with delirium
290.40 Vascular dementia, uncomplicated 290.41 Vascular dementia with delirium 290.42 Vascular dementia with delusions 290.43 Vascular dementia with depressed mood 290.8 Other specified senile psychotic conditions 290.9 Unspecified senile psychotic condition
Persistent Mental Disorders due to Conditions Classified Elsewhere 294.10 Dementia in conditions classified elsewhere without
behavioral disturbance 294.11 Dementia in conditions classified elsewhere with behavioral
disturbance 294.20 Dementia, unspecified, without behavioral disturbance 294.21 Dementia, unspecified, with behavioral disturbance 294.8 Other persistent mental disorders due to conditions classified
elsewhere Other cerebral degenerations 331.0 Alzheimer’s disease
331.11 Pick’s disease 331.19 Other frontotemporal dementia 331.82 Dementia with Lewy bodies

Administrative Claims Specifications PCPI APPROVED
Dementia
© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
25
Denominator (Eligible Population) Continued
ICD-10-CM Diagnosis Codes: Code Descriptor Late Syphilis A52.17 Symptomatic neurosyphilis, General paresis Vascular Dementia F01.50 Vascular dementia without behavioral disturbance F01.51 Vascular dementia with behavioral disturbance Dementia in Other Diseases Classified Elsewhere F02.80 Dementia in other diseases classified elsewhere, without
behavioral disturbance F02.81 Dementia in other diseases classified elsewhere, with
behavioral disturbance Unspecified Dementia
F03 Unspecified dementia Delirium due to Known Physiological Condition
F05 Delirium due to unknown physiological condition Other Mental Disorders Due to Known Physiological Condition F06.0 Psychotic disorder with hallucinations due to known
physiological condition F06.8 Other specified mental disorders due to known physiological
condition Alzheimer’s Disease G30.0 Alzheimer’s disease with early onset G30.1 Alzheimer’s disease with late onset G30.8 Other Alzheimer’s disease G30.9 Alzheimer’s disease, unspecified
Other Degenerative Diseases of Nervous System, Not Elsewhere Classified G31.01 Pick’s disease G31.09 Other frontotemporal dementia G31.83 Dementia with Lewy bodies
AND CPT® Code:
90801, 90802 90804, 90805, 90806, 90807, 90808, 90809 90810, 90811, 90812, 90813, 90814, 90815 90816, 90817, 90818, 90819, 90821, 90822 90823, 90824, 90826, 90827, 90828, 90829 90846, 90847 90862 96152, 96154, 96155 97003, 97004 99201, 99202, 99203, 99204, 99205 99212, 99213, 99214, 99215 99241, 99242, 99243, 99244, 99245 99304, 99305, 99306 99307, 99308, 99309, 99310 99324, 99325, 99326, 99327, 99328

Administrative Claims Specifications PCPI APPROVED
Dementia
© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
26
99334, 99335, 99336, 99337 99341, 99342, 99343, 99344, 99345 99347, 99348, 99349, 99350
Numerator Patients or their caregiver(s) who were counseled or referred for counseling regarding safety concerns within a 12 month period Please refer to the Measure Set Worksheets for complete numerator definition. CPT Category II Code 6101F: Safety counseling for dementia provided CPT Category II Code 6102F: Safety counseling for dementia ordered
Denominator Exceptions
Documentation of medical reason(s) for not counseling regarding safety concerns (eg, patient at end of life, other medical reason)
Append modifier to CPT II Code 6102F-1P
Additional CPT Category II Codes used to report this measure
None
Reporting Instructions
Report 6101F if patient (or caregiver) counseled regarding safety concerns or report 6102F if patient (or caregiver) was referred for counseling regarding safety concerns. For the patient with appropriate exception criteria, report 6102F with modifier 1P; modifiers 2P and 3P may not be reported.

Administrative Claims Specifications PCPI APPROVED
Dementia
© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
27
Measure #8 – Counseling Regarding Risks of Driving
Denominator (Eligible Population)
All patients, regardless of age, with a diagnosis of dementia ICD-9-CM Diagnosis Codes: Code Descriptor Neurosyphilis 094.1 Neurosyphilis, General paresis
Dementias 290.0 Senile dementia, uncomplicated
290.10 Presenile dementia, uncomplicated 290.11 Presenile dementia with delirium 290.12 Presenile dementia with delusional features 290.13 Presenile dementia with depressive features 290.20 Senile dementia with delusional features 290.21 Senile dementia with depressive features 290.3 Senile dementia with delirium
290.40 Vascular dementia, uncomplicated 290.41 Vascular dementia with delirium 290.42 Vascular dementia with delusions 290.43 Vascular dementia with depressed mood 290.8 Other specified senile psychotic conditions 290.9 Unspecified senile psychotic condition
Persistent Mental Disorders due to Conditions Classified Elsewhere 294.10 Dementia in conditions classified elsewhere without
behavioral disturbance 294.11 Dementia in conditions classified elsewhere with behavioral
disturbance 294.20 Dementia, unspecified, without behavioral disturbance 294.21 Dementia, unspecified, with behavioral disturbance 294.8 Other persistent mental disorders due to conditions classified
elsewhere Other cerebral degenerations 331.0 Alzheimer’s disease
331.11 Pick’s disease 331.19 Other frontotemporal dementia 331.82 Dementia with Lewy bodies

Administrative Claims Specifications PCPI APPROVED
Dementia
© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
28
Denominator (Eligible Population) Continued
ICD-10-CM Diagnosis Codes: Code Descriptor Late Syphilis A52.17 Symptomatic neurosyphilis, General paresis Vascular Dementia F01.50 Vascular dementia without behavioral disturbance F01.51 Vascular dementia with behavioral disturbance Dementia in Other Diseases Classified Elsewhere F02.80 Dementia in other diseases classified elsewhere, without
behavioral disturbance F02.81 Dementia in other diseases classified elsewhere, with
behavioral disturbance Unspecified Dementia
F03 Unspecified dementia Delirium due to Known Physiological Condition
F05 Delirium due to unknown physiological condition Other Mental Disorders Due to Known Physiological Condition F06.0 Psychotic disorder with hallucinations due to known
physiological condition F06.8 Other specified mental disorders due to known physiological
condition Alzheimer’s Disease G30.0 Alzheimer’s disease with early onset G30.1 Alzheimer’s disease with late onset G30.8 Other Alzheimer’s disease G30.9 Alzheimer’s disease, unspecified
Other Degenerative Diseases of Nervous System, Not Elsewhere Classified G31.01 Pick’s disease G31.09 Other frontotemporal dementia G31.83 Dementia with Lewy bodies
AND CPT® Code:
90801, 90802 90804, 90805, 90806, 90807, 90808, 90809 90810, 90811, 90812, 90813, 90814, 90815 90816, 90817, 90818, 90819, 90821, 90822 90823, 90824, 90826, 90827, 90828, 90829 90846, 90847 90862 96152, 96154, 96155 97003, 97004 99201, 99202, 99203, 99204, 99205 99212, 99213, 99214, 99215 99241, 99242, 99243, 99244, 99245 99304, 99305, 99306 99307, 99308, 99309, 99310 99324, 99325, 99326, 99327, 99328

Administrative Claims Specifications PCPI APPROVED
Dementia
© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
29
99334, 99335, 99336, 99337 99341, 99342, 99343, 99344, 99345 99347, 99348, 99349, 99350
Numerator Patients or their caregiver(s) who were counseled regarding the risks of driving and the alternatives to driving at least once within a 12 month period Please refer to the Measure Set Worksheets for complete numerator definition. CPT Category II Code 6110F: Counseling provided regarding risks of driving and the alternatives to driving
Denominator Exceptions
Documentation of medical reason(s) for not counseling regarding the risks of driving (eg, patient is no longer driving, other medical reason)
Append modifier to CPT II Code 6110F-1P
Additional CPT Category II Codes used to report this measure
None
Reporting Instructions
Report 6110F if patient (or caregiver) was counseled regarding the risks of driving and alternatives to driving. For the patient with appropriate exception criteria, report 6110F with modifier 1P; modifiers 2P and 3P may not be reported.

Administrative Claims Specifications PCPI APPROVED
Dementia
© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
30
Measure #9 – Palliative Care Counseling and Advance Care Planning
Denominator (Eligible Population)
All patients, regardless of age, with a diagnosis of dementia ICD-9-CM Diagnosis Codes: Code Descriptor Neurosyphilis 094.1 Neurosyphilis, General paresis
Dementias 290.0 Senile dementia, uncomplicated
290.10 Presenile dementia, uncomplicated 290.11 Presenile dementia with delirium 290.12 Presenile dementia with delusional features 290.13 Presenile dementia with depressive features 290.20 Senile dementia with delusional features 290.21 Senile dementia with depressive features 290.3 Senile dementia with delirium
290.40 Vascular dementia, uncomplicated 290.41 Vascular dementia with delirium 290.42 Vascular dementia with delusions 290.43 Vascular dementia with depressed mood 290.8 Other specified senile psychotic conditions 290.9 Unspecified senile psychotic condition
Persistent Mental Disorders due to Conditions Classified Elsewhere 294.10 Dementia in conditions classified elsewhere without
behavioral disturbance 294.11 Dementia in conditions classified elsewhere with behavioral
disturbance 294.20 Dementia, unspecified, without behavioral disturbance 294.21 Dementia, unspecified, with behavioral disturbance 294.8 Other persistent mental disorders due to conditions classified
elsewhere Other cerebral degenerations 331.0 Alzheimer’s disease
331.11 Pick’s disease 331.19 Other frontotemporal dementia 331.82 Dementia with Lewy bodies

Administrative Claims Specifications PCPI APPROVED
Dementia
© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
31
Denominator (Eligible Population) Continued
ICD-10-CM Diagnosis Codes: Code Descriptor Late Syphilis A52.17 Symptomatic neurosyphilis, General paresis Vascular Dementia F01.50 Vascular dementia without behavioral disturbance F01.51 Vascular dementia with behavioral disturbance Dementia in Other Diseases Classified Elsewhere F02.80 Dementia in other diseases classified elsewhere, without
behavioral disturbance F02.81 Dementia in other diseases classified elsewhere, with
behavioral disturbance Unspecified Dementia
F03 Unspecified dementia Delirium due to Known Physiological Condition
F05 Delirium due to unknown physiological condition Other Mental Disorders Due to Known Physiological Condition F06.0 Psychotic disorder with hallucinations due to known
physiological condition F06.8 Other specified mental disorders due to known physiological
condition Alzheimer’s Disease G30.0 Alzheimer’s disease with early onset G30.1 Alzheimer’s disease with late onset G30.8 Other Alzheimer’s disease G30.9 Alzheimer’s disease, unspecified
Other Degenerative Diseases of Nervous System, Not Elsewhere Classified G31.01 Pick’s disease G31.09 Other frontotemporal dementia G31.83 Dementia with Lewy bodies
AND CPT® Code:
90801, 90802 90804, 90805, 90806, 90807, 90808, 90809 90810, 90811, 90812, 90813, 90814, 90815 90816, 90817, 90818, 90819, 90821, 90822 90823, 90824, 90826, 90827, 90828, 90829 90846, 90847 90862 96152, 96154, 96155 99201, 99202, 99203, 99204, 99205 99212, 99213, 99214, 99215 99241, 99242, 99243, 99244, 99245 99304, 99305, 99306 99307, 99308, 99309, 99310 99324, 99325, 99326, 99327, 99328

Administrative Claims Specifications PCPI APPROVED
Dementia
© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
32
99334, 99335, 99336, 99337 99341, 99342, 99343, 99344, 99345 99347, 99348, 99349, 99350
Numerator Patients or their caregiver(s) who received 1) comprehensive counseling regarding ongoing palliation and symptom management and end of life decisions AND 2) have an advance care plan or surrogate decisions maker in the medical record or documentation in the medical record that the patient did not wish or was not able to name a surrogate decision maker or provide an advance care plan within two years of initial diagnosis or assumption of care Please refer to the Measure Set Worksheets for complete numerator definition. CPT Category II Code 4350F: Counseling provided on symptom management, end of life decisions, and palliation CPT Category II Code 1123F: Advanced care planning discussed and documented advanced care plan or surrogate decision maker documented in the medical record CPT Category II Code 1124F: Advanced care planning discussed and documented in the medical record, patient did not wish or was not able to name a surrogate decision maker or provide an advanced care plan
Denominator Exceptions
None
Additional CPT Category II Codes used to report this measure
None
Reporting Instructions
Report 4350F if patient (or caregiver) received comprehensive counseling regarding ongoing palliation and symptom management and end of life decisions. In addition, report 1123F or 1124F, to indicate advance care planning discussion and decision regarding an advance care plan. There are no performance exceptions for this measure; modifiers 1P, 2P or 3P may not be used.

Administrative Claims Specifications PCPI APPROVED
Dementia
© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
33
Measure #10 – Caregiver Education and Support
Denominator (Eligible Population)
All patients, regardless of age, with a diagnosis of dementia ICD-9-CM Diagnosis Codes: Code Descriptor Neurosyphilis 094.1 Neurosyphilis, General paresis
Dementias 290.0 Senile dementia, uncomplicated
290.10 Presenile dementia, uncomplicated 290.11 Presenile dementia with delirium 290.12 Presenile dementia with delusional features 290.13 Presenile dementia with depressive features 290.20 Senile dementia with delusional features 290.21 Senile dementia with depressive features 290.3 Senile dementia with delirium
290.40 Vascular dementia, uncomplicated 290.41 Vascular dementia with delirium 290.42 Vascular dementia with delusions 290.43 Vascular dementia with depressed mood 290.8 Other specified senile psychotic conditions 290.9 Unspecified senile psychotic condition
Persistent Mental Disorders due to Conditions Classified Elsewhere 294.10 Dementia in conditions classified elsewhere without
behavioral disturbance 294.11 Dementia in conditions classified elsewhere with behavioral
disturbance 294.20 Dementia, unspecified, without behavioral disturbance 294.21 Dementia, unspecified, with behavioral disturbance 294.8 Other persistent mental disorders due to conditions classified
elsewhere Other cerebral degenerations 331.0 Alzheimer’s disease
331.11 Pick’s disease 331.19 Other frontotemporal dementia 331.82 Dementia with Lewy bodies

Administrative Claims Specifications PCPI APPROVED
Dementia
© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
34
Denominator (Eligible Population) Continued
ICD-10-CM Diagnosis Codes: Code Descriptor Late Syphilis A52.17 Symptomatic neurosyphilis, General paresis Vascular Dementia F01.50 Vascular dementia without behavioral disturbance F01.51 Vascular dementia with behavioral disturbance Dementia in Other Diseases Classified Elsewhere F02.80 Dementia in other diseases classified elsewhere, without
behavioral disturbance F02.81 Dementia in other diseases classified elsewhere, with
behavioral disturbance Unspecified Dementia
F03 Unspecified dementia Delirium due to Known Physiological Condition
F05 Delirium due to unknown physiological condition Other Mental Disorders Due to Known Physiological Condition F06.0 Psychotic disorder with hallucinations due to known
physiological condition F06.8 Other specified mental disorders due to known physiological
condition Alzheimer’s Disease G30.0 Alzheimer’s disease with early onset G30.1 Alzheimer’s disease with late onset G30.8 Other Alzheimer’s disease G30.9 Alzheimer’s disease, unspecified
Other Degenerative Diseases of Nervous System, Not Elsewhere Classified G31.01 Pick’s disease G31.09 Other frontotemporal dementia G31.83 Dementia with Lewy bodies
AND CPT® Code:
90801, 90802 90804, 90805, 90806, 90807, 90808, 90809 90810, 90811, 90812, 90813, 90814, 90815 90816, 90817, 90818, 90819, 90821, 90822 90823, 90824, 90826, 90827, 90828, 90829 90846, 90847 90862 96154, 96155 97003, 97004 99201, 99202, 99203, 99204, 99205 99212, 99213, 99214, 99215 99241, 99242, 99243, 99244, 99245
Numerator Patients whose caregiver(s) were provided with education on dementia disease management and health behavior changes AND referred to additional resources for

Administrative Claims Specifications PCPI APPROVED
Dementia
© 2011 American Medical Association. All Rights Reserved. CPT® Copyright 2010 American Medical Association
35
support within a 12 month period Please refer to the Measure Set Worksheets for complete numerator definition. CPT Category II Code 4322F: Caregiver provided with education and referred to additional resources for support
Denominator Exceptions
Documentation of medical reason(s) for not providing the caregiver with education on disease management and health behavior changes or referring to additional sources for support (eg, patient does not have a caregiver, other medical reason)
Append modifier to CPT II code 4322F-1P
Additional CPT Category II Codes used to report this measure
None
Reporting Instructions
Report 4322F if patient’s caregiver was provided education on disease management and health behavior changes performed AND referred to additional resources for support. For the patient with appropriate exception criteria, report 4322F with modifier 1P; modifiers 2P and 3P may not be reported.





























