Embed Size (px)
Citation preview
Delta Dental of Massachusetts
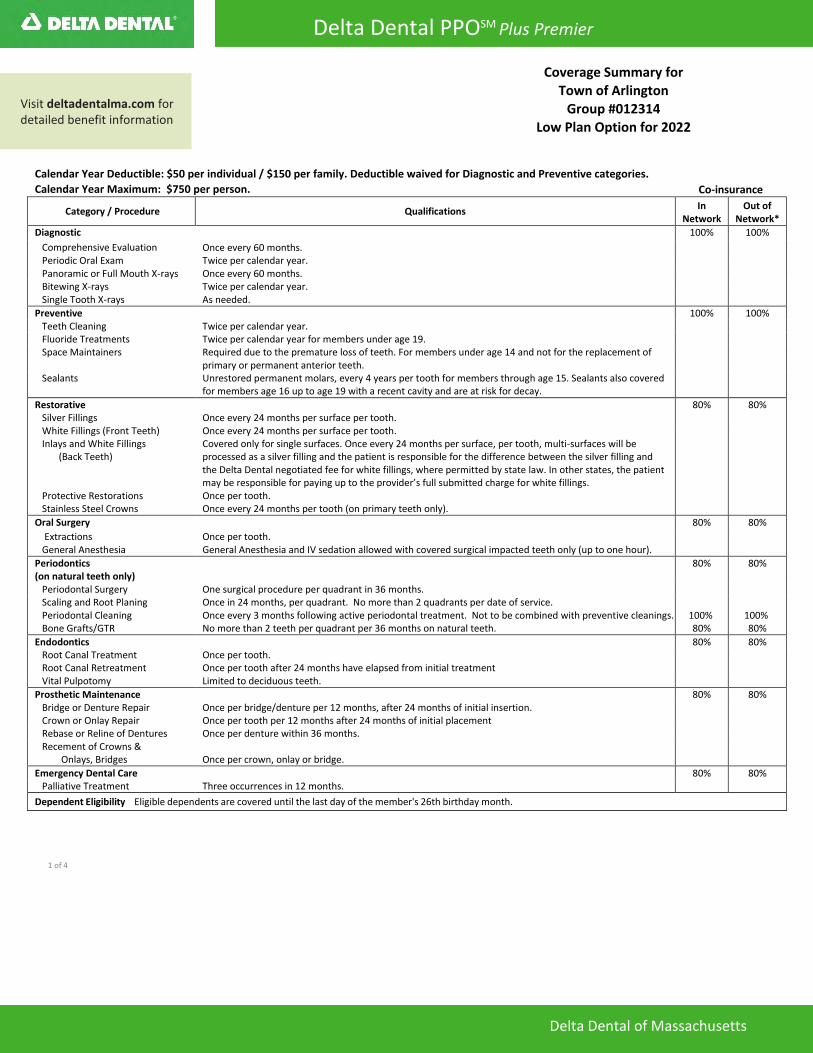
Calendar Year Deductible: $50 per individual / $150 per family. Deductible waived for Diagnostic and Preventive categories.
Calendar Year Maximum: $750 per person. Co-insurance
Category / Procedure Qualifications In
Network Out of
Network*
Diagnostic 100% 100%
Comprehensive Evaluation Once every 60 months. Periodic Oral Exam Twice per calendar year. Panoramic or Full Mouth X-rays Once every 60 months. Bitewing X-rays Twice per calendar year. Single Tooth X-rays As needed.
Preventive 100% 100% Teeth Cleaning Twice per calendar year. Fluoride Treatments Twice per calendar year for members under age 19. Space Maintainers Required due to the premature loss of teeth. For members under age 14 and not for the replacement of
primary or permanent anterior teeth. Sealants Unrestored permanent molars, every 4 years per tooth for members through age 15. Sealants also covered
for members age 16 up to age 19 with a recent cavity and are at risk for decay.
Restorative 80% 80% Silver Fillings Once every 24 months per surface per tooth. White Fillings (Front Teeth) Once every 24 months per surface per tooth. Inlays and White Fillings
(Back Teeth) Covered only for single surfaces. Once every 24 months per surface, per tooth, multi-surfaces will be processed as a silver filling and the patient is responsible for the difference between the silver filling and the Delta Dental negotiated fee for white fillings, where permitted by state law. In other states, the patient may be responsible for paying up to the provider’s full submitted charge for white fillings.
Protective Restorations Once per tooth. Stainless Steel Crowns Once every 24 months per tooth (on primary teeth only).
Oral Surgery 80% 80%
Extractions Once per tooth. General Anesthesia General Anesthesia and IV sedation allowed with covered surgical impacted teeth only (up to one hour).
Periodontics (on natural teeth only)
80% 80%
Periodontal Surgery One surgical procedure per quadrant in 36 months. Scaling and Root Planing Periodontal Cleaning Bone Grafts/GTR
Once in 24 months, per quadrant. No more than 2 quadrants per date of service. Once every 3 months following active periodontal treatment. Not to be combined with preventive cleanings. No more than 2 teeth per quadrant per 36 months on natural teeth.
100% 80%
100% 80%
Endodontics 80% 80% Root Canal Treatment Root Canal Retreatment
Once per tooth. Once per tooth after 24 months have elapsed from initial treatment
Vital Pulpotomy Limited to deciduous teeth.
Prosthetic Maintenance 80% 80% Bridge or Denture Repair Crown or Onlay Repair
Once per bridge/denture per 12 months, after 24 months of initial insertion. Once per tooth per 12 months after 24 months of initial placement
Rebase or Reline of Dentures Once per denture within 36 months. Recement of Crowns &
Onlays, Bridges Once per crown, onlay or bridge.
Emergency Dental Care 80% 80% Palliative Treatment Three occurrences in 12 months.
Dependent Eligibility Eligible dependents are covered until the last day of the member's 26th birthday month.
1 of 4
Coverage Summary for Town of Arlington
Group #012314 Low Plan Option for 2022
Visit deltadentalma.com for detailed benefit information
Delta Dental PPOSM Plus Premier

Additional Benefit Information Deductible waived for periodontal cleanings.
Ask your dentist to submit a pre-treatment estimate to Delta Dental for any procedure that exceeds $300. This will help you estimate any out-of-pocket expenses you may incur and will confirm that the services are covered under your dental coverage.
Easy Access and Great Value – Your Delta Dental Networks As a Delta Dental PPO Plus Premier subscriber, you have access to two of Delta Dental’s extensive national networks- Delta Dental PPO, with more than 283,000 participating dentist locations and Delta Dental Premier, the largest dental network in the country with more than 358,000 dentist locations. Three out of four dentists nationwide participate in one or both of these networks.
You will enjoy great benefits when you receive your dental care from a participating dentist in either the Delta Dental PPO or Delta Dental Premier networks.
• Both networks offer discounted fees and a no balancebilling policy.
• You will receive good value from Delta Dental Premiernetwork dentists who generally accept discounted fees.
• You will enjoy the greatest savings when visiting Delta DentalPPO network dentists due to even deeper discounts.
• If you choose to receive services from a non-participatingdentist, you will have higher out-of-pocket costs as the DeltaDental contract rates and the no balance billing policy donot apply.
Delta Dental members can also take advantage of expanded discounts on many covered services, even after they have used up their benefit dollars, visit limits and other situations. Get the details at http://www.deltadentalma.com/members/discounts- on-covered-services/
Simply visit www.deltadentalma.com to find a participating dentist in your area.
Learn more at deltadentalma.com
Visit the member area of www.deltadentalma.com to find plan information, review eligibility status, check on claim status, or find a dentist. If you have any questions or need additional information, you can call customer service at 1-800-872-0500.
You can also find more information about your plan in the Delta Dental Member Guide, available from your benefits administrator or online at www.deltadentalma.com. In the guide, you can learn how to use your benefits, how to find a dentist or specialist, how to access online resources, and more about keeping a healthy mouth for life.
Dental Services of Massachusetts, Inc. is an independent licensee of the Delta Dental Plans Association. ®Registered marks of the Delta Dental Plans Association. ©2017 DSM. 2 of 4
Your Plan is Administered by: Delta Dental of Massachusetts 1-800-872-0500www.deltadentalma.com
465 Medford Street
Boston, MA 02129
The information on this coverage summary should be used only as a guideline for your dental benefits plan. For detailed information on your group’s plan, riders, terms and conditions, or limitations and exclusions, refer to your plan’s Subscriber Certificate, which is available through your benefits administrator.
SP5
62
(5.
17
) P
assi
ve
Delta Dental PPOSM Plus Premier
*Non-participating dentists may balance bill. Subscribers are responsible for the difference between the non-participating maximum plan allowance and the full fee charged by the dentist.

Delta Dental of Massachusetts
Calendar Year Deductible: $50 per individual / $150 per family. Deductible waived for Diagnostic and Preventive categories.
Calendar Year Maximum: $1,500 per person. Co-insurance
Category / Procedure Qualifications In
Network Out of
Network*
Diagnostic 100% 100%
Comprehensive Evaluation Once every 60 months. Periodic Oral Exam Twice per calendar year. Panoramic or Full Mouth X-rays Once every 60 months. Bitewing X-rays Twice per calendar year. Single Tooth X-rays As needed.
Preventive 100% 100% Teeth Cleaning Twice per calendar year. Fluoride Treatments Twice per calendar year for members under age 19. Space Maintainers Required due to the premature loss of teeth. For members under age 14 and not for the replacement of
primary or permanent anterior teeth. Sealants Unrestored permanent molars, every 4 years per tooth for members through age 15. Sealants also covered
for members age 16 up to age 19 with a recent cavity and are at risk for decay.
Restorative 80% 80% Silver Fillings Once every 24 months per surface per tooth. White Fillings (Front Teeth) Once every 24 months per surface per tooth. Inlays and White Fillings
(Back Teeth) Covered only for single surfaces. Once every 24 months per surface, per tooth, multi-surfaces will be processed as a silver filling and the patient is responsible for the difference between the silver filling and the Delta Dental negotiated fee for white fillings, where permitted by state law. In other states, the patient may be responsible for paying up to the provider’s full submitted charge for white fillings.
Protective Restorations Once per tooth. Stainless Steel Crowns Once every 24 months per tooth (on primary teeth only).
Oral Surgery 80% 80%
Extractions Once per tooth. General Anesthesia General Anesthesia and IV sedation allowed with covered surgical impacted teeth only (up to one hour).
Periodontics (on natural teeth only)
80% 80%
Periodontal Surgery One surgical procedure per quadrant in 36 months. Scaling and Root Planing Periodontal Cleaning Bone Grafts/GTR
Once in 24 months, per quadrant. No more than 2 quadrants per date of service. Once every 3 months following active periodontal treatment. Not to be combined with preventive cleanings. No more than 2 teeth per quadrant per 36 months on natural teeth.
100% 80%
100% 80%
Endodontics 80% 80% Root Canal Treatment Root Canal Retreatment
Once per tooth. Once per tooth after 24 months have elapsed from initial treatment
Vital Pulpotomy Limited to deciduous teeth.
Prosthetic Maintenance 80% 80% Bridge or Denture Repair Crown or Onlay Repair
Once per bridge/denture per 12 months, after 24 months of initial insertion. Once per tooth per 12 months after 24 months of initial placement
Rebase or Reline of Dentures Once per denture within 36 months. Recement of Crowns &
Onlays, Bridges Once per crown, onlay or bridge.
Emergency Dental Care 80% 80% Palliative Treatment Three occurrences in 12 months.
Prosthodontics 50% 50%
Dentures Once within 60 months (age 16 and older).
Fixed Bridges Once within 60 months (age 16 and older).
Implants (only in lieu of a 3-unit bridge)
Implant Abutments
Endosteal Implant: Only when replacing one missing tooth and when adjacent teeth are healthy and do not require crowns. Once per 60 months per Implant. (Pre-estimate recommended). Once per implant only when surgical implant is benefitted.
Major Restorative 50% 50%
Crowns or Onlay Cast Posts/Buildups
When teeth cannot be restored with regular fillings. Once within 60 months per tooth (age 12 and older). Once per tooth per 60 months only benefitted to retain a crown.
Orthodontics: Covered at 100% of Maximum Plan Allowance charges up to age 19. $1,000 separate LIFETIME maximum. Orthodontic treatment must be administered/supervised by a licensed dentist
Dependent Eligibility Eligible dependents are covered until the last day of the member's 26th birthday month.
1 of 4
Coverage Summary for
Town of Arlington
Group #012314
High Plan Option for 2022
Visit deltadentalma.com for detailed benefit information
Delta Dental PPOSM Plus Premier

Additional Benefit Information Deductible waived for periodontal cleanings.
Ask your dentist to submit a pre-treatment estimate to Delta Dental for any procedure that exceeds $300. This will help you estimate any out-of-pocket expenses you may incur and will confirm that the services are covered under your dental coverage.
This plan is eligible for Rollover Maximum: Rollover Max dollars do not apply to orthodontic services. To qualify for Rollover Max, you must receive at least one cleaning or oral exam in the calendar year. You must be enrolled for dental coverage before the 4th quarter of the plan year (10/1-12/31) and your paid claims must not exceed the maximum “threshold” amount.
Your calendar year maximum benefit
amount.
If your total yearly claims don’t exceed this threshold
amount…
Then you can roll over this amount to use next year, and
beyond.
Your accumulated rollover total is capped at this
amount.
$1,500 $700 $500 $1,250
Easy Access and Great Value – Your Delta Dental Networks As a Delta Dental PPO Plus Premier subscriber, you have access to two of Delta Dental’s extensive national networks- Delta Dental PPO, with more than 283,000 participating dentist locations and Delta Dental Premier, the largest dental network in the country with more than 358,000 dentist locations. Three out of four dentists nationwide participate in one or both of these networks.
You will enjoy great benefits when you receive your dental care from a participating dentist in either the Delta Dental PPO or Delta Dental Premier networks.
• Both networks offer discounted fees and a no balancebilling policy.
• You will receive good value from Delta Dental Premiernetwork dentists who generally accept discounted fees.
• You will enjoy the greatest savings when visiting Delta DentalPPO network dentists due to even deeper discounts.
• If you choose to receive services from a non-participatingdentist, you will have higher out-of-pocket costs as the DeltaDental contract rates and the no balance billing policy donot apply.
Delta Dental members can also take advantage of expanded discounts on many covered services, even after they have used up their benefit dollars, visit limits and other situations. Get the details at http://www.deltadentalma.com/members/discounts- on-covered-services/
Simply visit www.deltadentalma.com to find a participating dentist in your area.
Learn more at deltadentalma.com
Visit the member area of www.deltadentalma.com to find plan information, review eligibility status, check on claim status, or find a dentist. If you have any questions or need additional information, you can call customer service at 1-800-872-0500.
You can also find more information about your plan in the Delta Dental Member Guide, available from your benefits administrator or online at www.deltadentalma.com. In the guide, you can learn how to use your benefits, how to find a dentist or specialist, how to access online resources, and more about keeping a healthy mouth for life.
Dental Services of Massachusetts, Inc. is an independent licensee of the Delta Dental Plans Association. ®Registered marks of the Delta Dental Plans Association. ©2017 DSM. 2 of 4
Your Plan is Administered by: Delta Dental of Massachusetts 1-800-872-0500www.deltadentalma.com
465 Medford Street
Boston, MA 02129
The information on this coverage summary should be used only as a guideline for your dental benefits plan. For detailed information on your group’s plan, riders, terms and conditions, or limitations and exclusions, refer to your plan’s Subscriber Certificate, which is available through your benefits administrator.
SP5
62
(5.
17
) P
assi
ve
*Non-participating dentists may balance bill. Subscribers are responsible for the difference between the non-participating maximum plan allowance and the full fee charged by the dentist.
Delta Dental PPOSM Plus Premier

Delta Dental PPO Plus Premier
An independent licensee of the Delta Dental Plans Association. ® Registered marks of the Delta Dental Plans Association. ©2017 DSM. 3 of 4 SP562 (5.17) Passive
NONDISCRIMINATION NOTICE
Delta Dental of Massachusetts complies with applicable Federal civil rights laws and does not discriminate on the basis of race, color, national origin, age, disability, or sex. Delta Dental of Massachusetts does not exclude people or treat them differently because of race, color, national origin, age, disability, or sex.
Delta Dental of Massachusetts: • Provides free aids and services to people with disabilities to communicate effectively with us, such as:
o Qualified sign language interpreterso Written information in other formats (large print, audio, and accessible electronic formats)
• Provides free language services to people whose primary language is not English, such as:o Qualified interpreterso Information written in other languages
If you need these services, visit: http://www.deltadentalma.com or call the number on your member ID card.
If you believe that Delta Dental of Massachusetts has failed to provide these services or discriminated in another way on the basis of race, color, national origin, age, disability, or sex, you can file a grievance with:
Ugonna Onyekwu Civil Rights Coordinator Compliance Department
465 Medford Street Boston, MA 02129 Fax: 617-886-1390
Phone: 617-886-1683 Email: [email protected]
TTY: 711
You can file a grievance in person or by mail, fax, or email. If you need help filing a grievance, Ugonna Onyekwu is available to help you.
You can also file a civil rights complaint with the U.S. Department of Health and Human Services, Office for Civil Rights. Complaint forms are available at http://www.hhs.gov/ocr/office/file/index.html. You can file a complaint electronically through the Office for Civil Rights Complaint Portal, available at https://ocrportal.hhs.gov/ocr/portal/lobby.jsf, or by mail or phone at:
U.S. Department of Health and Human Services 200 Independence Avenue, SW
Room 509F, HHH Building Washington, D.C. 20201
1-800-368-1019, 800-537-7697 (TDD)
Delta Dental of Massachusetts PPO and Premier insurance products are offered by Dental Service of Massachusetts, Inc. Delta Dental of Massachusetts
EPO and DeltaCare insurance products are offered DSM Massachusetts Insurance Company, Inc.

Delta Dental PPO Plus Premier
An independent licensee of the Delta Dental Plans Association. ® Registered marks of the Delta Dental Plans Association. ©2017 DSM. 4 of 4 SP562 (5.17) Passive
ATENCIÓN: si habla español, tiene a su disposición servicios gratuitos de asistencia lingüística. Llame al 1-800-872-0500.
ATENÇÃO: Se fala português, encontram-se disponíveis serviços linguísticos, grátis. Ligue para 1-800-872-0500.
注意:如果您使用繁體中文,您可以免費獲得語言援助服務。請致電 1-800-872-0500。
ATANSYON: Si w pale Kreyòl Ayisyen, gen sèvis èd pou lang ki disponib gratis pou ou. Rele 1-800-872-0500.
CHÚ Ý: Nếu bạn nói Tiếng Việt, có các dịch vụ hỗ trợ ngôn ngữ miễn phí dành cho bạn. Gọi số 1-800-872-0500.
ВНИМАНИЕ: Если вы говорите на русском языке, то вам доступны бесплатные услуги перевода. Звоните 1-800-872-0500.
لال ركذا ثدحتت تنك اذإ :ةظوحلم .1-800-872-0500 ال تامدخ نإف ،ة الب كل رفاوتت ةيولال ةدعاس مقرب لصتا .ناج
ប្រយ័ត្ន៖ បរើសិនជាអ្នកនិយាយ ភាសាខ្មែរ, បសវាជំនួយខ្ននកភាសា បោយមិនគិត្ឈ្ន លួ គឺអាចមានសំរារ់រំបរ ើអ្នក។ ចូរ ទូរស័ព្ទ 1-800-872-0500.។ ATTENTION : Si vous
parlez français, des services d’aide linguistique vous sont proposés gratuitement. Appelez le 1-800-872-0500.
ATTENZIONE: In caso la lingua parlata sia l’italiano, sono disponibili servizi di assistenza linguistica gratuiti. Chiamare il numero 1-800-872-0500.
주의: 한국어를 사용하시는 경우, 언어 지원 서비스를 무료로 이용하실 수 있습니다. 1-800-872-0500.번으로 전화해 주십시오.
ΠΡΟΣΟΧΗ: Αν μιλάτε ελληνικά, στη διάθεσή σας βρίσκονται υπηρεσίες γλωσσικής υποστήριξης, οι οποίες παρέχονται δωρεάν. Καλέστε 1-800-872-0500.
UWAGA: Jeżeli mówisz po polsku, możesz skorzystać z bezpłatnej pomocy językowej. Zadzwoń pod numer 1-800-872-0500.
ध्यान दें : यदद आप द िंदी बोलते ैं तो आपके दलए मुफ्त में भाषा स ायता सेवाएिं उपलब्ध ैं। 1-800-872-0500. पर कॉल करें ।
સચુના: જો તમે ગજુરાતી બોલતા હો, તો નન:શલુ્ક ભાષા સહાય સેવાઓ તમારા માટે ઉપલબ્ધ છે. ફોન કરો 1-800-872-0500.
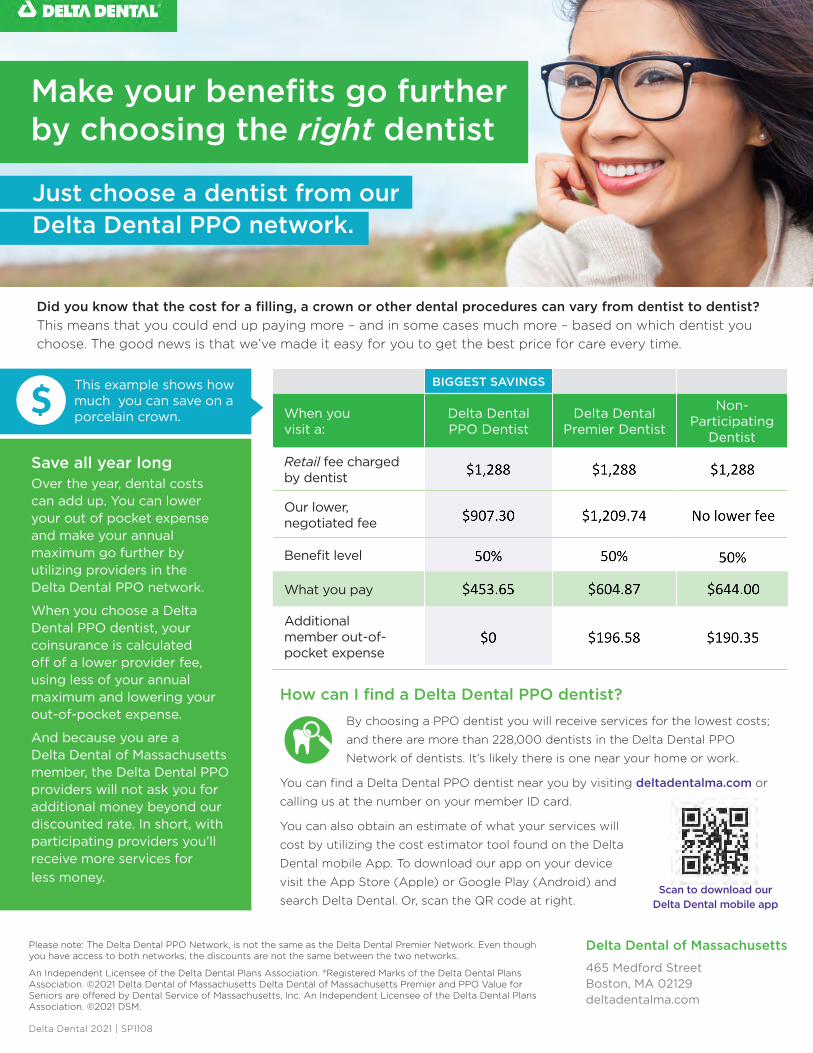
Did you know that the cost for a filling, a crown or other dental procedures can vary from dentist to dentist? This means that you could end up paying more – and in some cases much more – based on which dentist you choose. The good news is that we’ve made it easy for you to get the best price for care every time.
Make your benefits go further by choosing the right dentist
Delta Dental 2021 | SP1108
Just choose a dentist from our Delta Dental PPO network.
BIGGEST SAVINGS
When you visit a:
Delta Dental PPO Dentist
Delta Dental Premier Dentist
Non- Participating
Dentist
Retail fee charged by dentist
Our lower, negotiated fee
Benefit level
What you pay
Additional member out-of-pocket expense
This example shows how much you can save on a porcelain crown.
Save all year longOver the year, dental costs can add up. You can lower your out of pocket expense and make your annual maximum go further by utilizing providers in the Delta Dental PPO network.
When you choose a Delta Dental PPO dentist, your coinsurance is calculated off of a lower provider fee, using less of your annual maximum and lowering your out-of-pocket expense.
And because you are a Delta Dental of Massachusetts member, the Delta Dental PPO providers will not ask you for additional money beyond our discounted rate. In short, with participating providers you’ll receive more services for less money.
How can I find a Delta Dental PPO dentist?By choosing a PPO dentist you will receive services for the lowest costs;
and there are more than 228,000 dentists in the Delta Dental PPO
Network of dentists. It’s likely there is one near your home or work.
You can find a Delta Dental PPO dentist near you by visiting deltadentalma.com or
calling us at the number on your member ID card.
You can also obtain an estimate of what your services will
cost by utilizing the cost estimator tool found on the Delta
Dental mobile App. To download our app on your device
visit the App Store (Apple) or Google Play (Android) and
search Delta Dental. Or, scan the QR code at right.
Please note: The Delta Dental PPO Network, is not the same as the Delta Dental Premier Network. Even though you have access to both networks, the discounts are not the same between the two networks.
An Independent Licensee of the Delta Dental Plans Association. ®Registered Marks of the Delta Dental Plans Association. ©2021 Delta Dental of Massachusetts Delta Dental of Massachusetts Premier and PPO Value for Seniors are offered by Dental Service of Massachusetts, Inc. An Independent Licensee of the Delta Dental Plans Association. ©2021 DSM.
Delta Dental of Massachusetts
465 Medford StreetBoston, MA 02129deltadentalma.com
Scan to download ourDelta Dental mobile app

Rollover Maximum Benefit Summary
Delta Dental of Massachusetts An Independent Licensee of the Delta Dental Plans Association. ®Registered Marks of the Delta Dental Plans Association. ©2021 DSM.
Your Plan Year Maximum benefit amount.
If your total yearly claims don’t exceed this threshold amount.
Then you can roll over this amount to use next year, and beyond.
Your accumulated rollover total will not exceed this amount.
How to check your Rollover Max balance online:• Log on to your account at deltadentalma.com
(You’ll need to register if this will be your first visit.)• Click on Benefit Maximums.• The rollover amount for each member will be listed under Rollover Maximum.
Rollover Max increases your dental benefit value.You get more flexibility in planning and paying for your dental care, as well as the peace of mind knowing you have more benefits—if you need them, when you need them. Best of all, Rollover Max comes as part of your Delta Dental coverage.
SP955 (9.21)
With Rollover Max from Delta Dental, you won’t lose what you don’t use.Thanks to the Rollover Max benefit from Delta Dental, you can save some of your unused benefit dollars to be applied to future services that would otherwise exceed your plan maximum.
Rollover Max is easy and automatic.• To qualify for Rollover Max, you must receive at
least one cleaning or oral exam in the plan year. Ifyou don’t receive a cleaning or exam, you won’t beeligible to rollover any of your benefit dollarsto the following year.
• In addition, your paid claims must not exceed thePlan Year Maximum “threshold” amounts outlinedin the chart below.
• Once you qualify, some of your unused annual PlanYear maximum benefit dollars will automaticallyrollover for use in your next plan year and beyond.The amounts are outlined in the chart below.
• Annual Plan Year Maximum dollars are usedfirst. Rollover Max dollars are used after theannual maximum amount for your plan hasbeen exhausted.
• Rollover Max dollars cannot be applied toorthodontic treatment or other lifetime benefits.
• You must be enrolled for dental coverage beforethe 4th quarter of the plan (10/1-12/31) to qualifyfor the rollover that year.
How Rollover Max works.The chart below shows how Rollover Max is calculated based on your plan’s annual Plan Year Maximum level.

UNDERSTANDING YOUR ORTHODONTIC BENEFITS-High Plan Coverage Your dental plan provides the following coverage for orthodontic services:
• Your coverage is based on the maximum allowable fee for orthodontic services.• Coverage is subject to a lifetime maximum of $1,000 per member.• Members up to age 19 years of age are eligible for coverage.• A maximum of 24 months of active treatment.
Paying for orthodontic care In most cases, Delta Dental issues reimbursements for orthodontic care in automatic monthly payments not to exceed 12 installments. The first payment is based on the date of banding/placement of appliances. Additional payments will be issued automatically on a monthly basis assuming you are still eligible for orthodontic benefits.
If you begin orthodontic treatment after your effective date of coverage and you receive care from a network dentist, Delta Dental will reimburse your dentist directly and send you and your dentist an Explanation of Benefits (EOB). The EOB will detail any payments made to the dentist. It is up to you and your dentist to develop a payment plan for the balance minus any Delta Dental adjustments.
If you’ve already started your orthodontic treatment We provide pro-rated orthodontic benefits for members who are in active treatment and banded within 24 months of DDMA effective date. Coverage will be based on the maximum allowable fee, determined by the lower of the dentists submitted fee or contracted fee, and the time remaining in your treatment plan once your coverage with Delta Dental begins.
To determine your coverage, we exclude the banding allowance, which we estimate to be 30% of total cost of treatment. Since that cost was incurred before your coverage began with Delta Dental, it is not covered.
We process your benefit on the remaining 70% of the maximum allowable fee. Payment will vary based on banding date and effective date with Delta Dental. If banded less than 5 months from DDMA effective date, benefit is issued in automatic monthly payments. If banded more than 5 months from effective date with DDMA, benefit is issued in one lump payment. All payments are issued provided patient is in active treatment and covered by Delta Dental.
Termination of Coverage In the event your coverage terminates before you complete your orthodontic treatment the automatic monthly payments will cease.
Delta Dental of Massachusetts, 465 Medford Street, Boston, MA 02129 • www.deltadentalma.com An Independent Licensee of the Delta Dental Plans Association. ®Registered Marks of the Delta Dental Plans Association. ©2017 DSM.
SP1276 (10.17)
Delta Dental of Massachusetts

Coordination of BenefitsSometimes family members are covered by more than one health care plan. This happens, for example, when a husband and wife both work and choose to have family coverage through both employers. When you are covered by more than one plan, Delta Dental of Massachusetts follows a legal procedure called coordination of benefits to establish which dental plan is primary and how much the secondary plan should pay. The goal is to pay the maximum allowable benefit without exceeding the actual cost approved for your care.
Determining the Primary PlanThe guidelines below will help determine which plan is primary.
• If a health plan does not have a coordination of benefits provision, that plan is primary.
• The plan that covers the patient as the employee (member or subscriber) is primary over a plan covering the patient as a dependent, retiree, or COBRA-qualified beneficiary.
• If a child is covered under both parents’ plans, the plan of the parent (or legal guardian) whose birthday is earlier in the year is the primary plan.
• For children of divorced or separated parents, benefits are determined in the following order unless a court order places financial responsibility on one parent: • plan of the custodial parent;• plan of the custodial parent’s new spouse (if remarried);• plan of the noncustodial parent;• plan of the noncustodial parent’s new spouse (if remarried).
Delta Dental as Primary PlanWhen Delta Dental is the primary plan, we pay the claim to the full extent of the patient’s coverage.
Delta Dental as Secondary PlanPayment is calculated on the total approved amount for the services billed. The primary payment amount is deducted from the total approved amount, and Delta Dental makes payment based on the balance. Delta Dental’s limitations and exclusions apply to COB claims.
Some plans have a non-duplication of benefits clause. This means if the primary plan’s payment is less than what Delta Dental would have paid as primary, Delta Dental pays the difference between the actual primary payment and the amount Delta Dental would have paid as primary. If the primary plan’s payment is more than Delta Dental would have paid as primary, Delta Dental’s payment is zero.
Coordination of benefits covers a variety of circumstances. This is only an overview of the most common ones. If you have questions, email us at [email protected] or call Customer Service at 1-800-872-0500.
Delta Dental of Massachusetts
SP1274 (9.17)

Where your dental benefit information is always at your fingertips. At www.deltadentalma.com, you can:
Welcome todeltadentalma.com
• Check your eligibility
• Verify your deductible and annualmaximum
• Check your Rollover Max Balance
• Check the date of your last cleaning
• View your benefit plan design
• Check the status of your claims
• Request a replacement ID card
• Download the Delta Dental mobile app
You can also search for a dentist on our site using our Find a Dentist feature. Just enter your plan name, area preference, dentist name or specialty, and you’ll get a list of participating dentists who may be perfect for you.
Visit www.deltadentalma.com today and start taking advantage of our user-friendly services. Follow the instructions on the back of this card. It has never been easier to get the dental benefit information you need to keep a healthy smile.
www.deltadentalma.com

Step 1: Go to www.deltadentalma.com.
Step 2: Click on Members from the right-hand login box.
Step 3: Click on Members click here to registerunder "Forgot Password?" link.
Step 4: Please read and review our Terms andConditions and click Yes to agree and continue.
Step 5: Complete the Register Member PersonalInformation section, and continue on tocomplete the Account Information section.
Step 6: Begin accessing your dental benefitsinformation right away.
How To Check Your Rollover Max Balance
• Select “Members” from the login box atwww.deltadentalma.com. Log in to youraccount by using your user name andpassword.
• Click on Benefit Maximums.• The rollover amount will be listed under the
section“Benefit Maximums and Deductibles”as Rollover Maximum.
• This is the amount available once your plan’sannual maximum has been satisfied.
Delta Dental of Massachusetts465 Medford Street, Boston, MA 02129
Dental Service of Massachusetts, Inc. is an Independent Licensee of the Delta Dental Plans Association.
®Registered Marks of the Delta Dental Plans Association. ©2016 DSM.
SP670 (7/16)
Register Now!
Managing your dental benefits has never been easier.

Getting startedDelta Dental’s mobile app is optimized for iOS (Apple) and Android devices. To download our app on your device, visit the App Store (Apple) or Google Play (Android) and search for Delta Dental. Or, scan the QR code at the left. You will need an internet connection in order to download and use most features of our free app.
Logging in to view benefitsDelta Dental subscribers can log in using the username and password they use to log in to our website. If you haven’t registered for an account yet, you can do that within the app.
Forgot your username or password?You can easily also retrieve your username or password via the Delta Dental mobile app.
deltadentalMA.com Delta Dental 2021 | SP1234
Delta Dental mobile app
Manage your benefits
anytime, anywhere
Your oral health is important to Delta Dental — and to your overall health! We’ve designed our mobile app to make it easy for you to make the most of your dental benefits. Maximize your health, wherever you are! Search for a dentist near you, check claims and coverage, view ID cards and more, right on your mobile device.
SCAN TO DOWNLOADDELTA DENTAL MOBILE

Mobile ID cardNo need for a paper card. View and share your ID card from your phone, and easily save it to your device for quick access, including Apple Passbook and Google Wallet.
My coverage and my claimsView information on your plan and coverage details, and check the status of claims for you and your family. Easily add your dependents to your account so you can access the whole family’s coverage in one spot.
Find a dentistIt’s easy to find a dentist near you. Search and compare dental offices to find one that suits your needs. Save your family’s preferred dentists to your account for easy access.
ENHANCED Dental Care Cost Estimator*You can easily estimate your costs and coverage before you to to the dentist with our Dental Care Cost Estimator. Our easy to use tool combines your benefits with your deductible and information from your dentist to give you the best estimate possible.
LifeSmile™ ScoreDo you know how your smile scores? Learn more about your personal oral health risk profile by taking our simple risk assessment survey.
* The cost estimator tool only generates estimated costs and cannot be relied upon for the
actual costs. The members should carefully review their benefit terms and speak with their
dentists before the dental procedures are undertaken.
Log in to access the full range of tools and resources
Secure access to your benefits
You must log in each time you access the secure portion of the mobile app. No personal health information is ever stored on your device. For more details on security, our Privacy Policy can be viewed by clicking the lock icon on the main menu.
Delta Dental mobile app features
deltadentalMA.com Delta Dental 2021 | SP1234

A healthy smile for life!
What is gum disease?• Periodontal disease is an infection of your gums
and jawbone.
• Gingivitis is an infection in your gums.
Gum disease• Gets worse if not properly treated.• Can be passed on to other family members.• Can appear without symptoms so people may
not know they have it.• May affect the outcomes of other diseases,
such as diabetes and heart disease.• May lead to premature birth in pregnant women.
How is gum disease treated?• A deep cleaning by your dentist to remove the
bacteria that is damaging your gums.• Prescription mouth rinse or fluoride toothpaste,
or other medicine to use at home.• Some people may need gum surgery.
Stay healthy after treatment for gum disease• Floss daily.
• Brush twice a day.
• Visit your dentist twice per calendar year for oral exams and cleanings.
• Use at-home products your dentist recommends.
• Do not chew or smoke tobacco.
you can prevent
oral health problems
What causes cavities?• Bacteria in your mouth.
• Frequent snacking and sippingsugary drinks.
• Not cleaning your teeth well.
Reduce your risk for cavities• Brush for two minutes, twice a day,
with fluoride toothpaste.
• Brush your teeth after eating sugaryor starchy foods.
• Floss daily to remove food trappedbetween teeth.
• Chew Xylitol gum.
Protect your teeth with sealants• A dental sealant is a thin, plastic
coating painted on the chewingsurfaces of teeth -- usually the backmolars – to prevent tooth decay
• Takes only a few minutes to apply asealant to a tooth.
• Last for 5 years or longer.
Who should get sealants?• Children when their first molars
(ages 6-7) and second molars(ages 12-13) emerge.
SP1324 (9.21)

Keep up your oral hygiene at homeKeeping up with your home oral health care is more important than ever! With proper care, you can decrease your risk for tooth decay and gum disease, which can weaken your immune system.
Take care of your teeth and gums with a thorough, at-home oral care routine that includes regular brushing, flossing and healthy eating.
For tips on keeping your oral health in check, visit the Delta Dental of Massachusetts web site at: www.deltadentalma.com/Your-Oral-Health. You’ll get age-based tips so you and your family get the right preventive care at the right time, and an oral heath library with articles on an extensive list of mouth health topics. Take a few minutes to read our quarterly = Grin! magazine. You can even take a quiz to assess your oral health.
We’re still here for youAnd no matter what is happening, Delta Dental of Massachusetts is here for you. You can give us a call at 800.872.0500 with your questions and our Customer Service team will be there to help. Our hours are:
Monday–Thursday, 8:30 a.m.–8 p.m. and Friday, 8:30 a.m.–4:30 p.m.
If your questions are about your plan, an ID card (or replacement card) or finding a dentist, log into our secure member portal or download and use the Delta Dental mobile app. Just visit deltadentalma.com to get connected. These resources are available 24/7. And if you haven’t yet registered for the member portal or downloaded the app, now is a great time to do so.
During this critical time, our customer service team is focusing their efforts on answering questions that cannot be answered via our automated technology tools.
Tips to Prevent the Spread of COVID-19
Wash your hands with soap and water for at
least 20 seconds.
Avoid close contact with people and shaking hands. Use other
noncontact methods of greeting.
Stay home if you are sick except to get
medical care.
Cover coughs and sneezes with a tissue or the inside of your elbow.
Clean and disinfect frequently touched
surfaces daily.
Don’t share a toothbrush or mouthwash and replace your toothbrush after you are sick.
Source: Centers for Disease Control and Prevention
Things You Can Do
Here’s how to orderOnline• Go to: myzsonic.com/DDMA• Add products to your cart• Enter payment information
By Phone• Call 1-888-228-7706• Be sure to mention that
you are a Delta Dental ofMassachusetts member
As a member of Delta Dental, you can now take advantage of significant discounts on two kinds of Z Sonic toothbrushes, as well as replacement heads.
With your member discount, you can get the premier Z Sonic toothbrush for $59.95, $140 off the Manufacturer’s Suggested Retail Price (MSRP). The offer also includes 2 brush heads & 1 charging base. And as a member you also get discounts on replacement heads.
The Z Sonic pulses 31,000 – 48,000 times a minute and features 5 brushing modes (Clean, Whiten, Polish, Massage, and Sensitive) to customize your tooth cleaning experience.
Take Your Sonic Cleaning on the Road
If you travel and want to keep your mouth healthy on the road, you can also pick up a Z Sonic travel toothbrush for $14.50. This portable, battery powered, toothbrush gives you the benefits of sonic brushing in a size that can fit in your carry on, in the glove compartment or in your desk drawer.
Save On Replacement Heads Too
You can also get replacement heads for both the Z Sonic or Z Sonic Mini at 50% off retail costs. And if you buy replacement heads and the toothbrush together, you can get FREE shipping.
Delta Dental of Massachusetts is an Independent Licensee of the Delta Dental Plans Association. ®Registered Marks of the Delta Dental Plans Association. Delta Dental of Massachusetts and Z Sonic are independent, unaffiliated companies.
The plan is not insurance coverage and does not meet the minimum creditable coverage requirements under the Affordable Care Act or Massachusetts M.G.L. c. 111M and 956 CMR 5.00. SP1328 (8.21)
Discount Codes:
• Z Sonic$59.95 (MSRP: $199.95)
• 4 Regular Brush Heads$21.88 (MSRP: $43.76)
• 4 Premium Brush Heads$25.88 (MSRP: $51.76)
• Z Sonic Mini Travel Toothbrush$14.50 (MSRP: $19.95)Promo Code: DDMA4
• 4 Z Sonic Mini Brush Heads$14.00 (MSRP: $28.00)
Keeping your teeth clean is easier and less expensive than ever

ADDITIONAL MONEY-SAVING OFFER!*
CALLTODAY:1-888-402-1394 *Savings on top of our already discounted pricing.
Please bring this offer with you to your appointment.
$50 off one
hearing aid
$125 off two
hearing aids
Hearing Health Care ™
YOUR HEARING HEALTH CARE PROGRAM FOR LIFE Delta Dental of Massachusetts
CUSTOM HEARING SOLUTIONS
We find the solution that best fits your lifestyle and your budget from one of
our 10 brands.
RISK-FREE 60-DAY TRIAL
100% money-back guarantee if not
completely satisfied. No restocking or return
fees.
CONTINUOUS CARE
1-year free follow-up care, 2 years free batteries, and a
3-year warranty.*
GREAT PRICES ON HEARING AIDS
The average discount you get on hearing aid
prices is 62 percent.
ACCESSING YOUR DISCOUNT IS AS EASY AS...
Call Amplifon at 1-888-402-1394 and we’ll find a provider near you
We’ll explain the Amplifon process and help you schedule an
appointment
www.amplifonusa.com/ddma
We’ll send information to you and the provider, ensuring your
discount is activated
*Some exclusions apply. Limited to one-time claim for loss and damage. Deductibles may apply.
Hearing services are administered by Amplifon Hearing Health Care, Corp. Amplifon Hearing Health Care is solely responsible for the administration of hearing health care services, and its own financial and contractual obligations. Delta Dental of Massachusetts and Amplifon are independent, unaffiliated companies.
Delta Dental of Massachusetts is an Independent Licensee of the Delta Dental Plans Association. ®Registered Marks of the Delta Dental Plans Association.
The plan is not insurance coverage and does not meet the minimum creditable coverage requirements under the Affordable Care Act or Massachusetts M.G.L. c. 111M and 956 CMR 5.00.©2019 Amplifon Hearing Health Care, Corp. | 3264MISC/ DDMA
3 2 1





























