Embed Size (px)
Citation preview
1
Delivering Vocational Rehabilitation As
An Enhanced Service Within The
Occupational Therapy Rheumatology
Service:
A Practice Analysis
Authors
Justine Griffin Alison Leiper
Katie McAlarey
March 2011

2
Acknowledgements
In undertaking this pilot Glasgow Rheumatology Occupational Therapy Service would like to thank
the following people who participated and contributed their time and support; rheumatology
medical and nursing staff at Southern General Hospital; clinical effectiveness team and public health
team for their support in designing the pilot and in undertaking the statistical analysis; Maureen
Grove for her support in undertaking the telephone questionnaires; The rheumatology occupational
therapy team for their support in data collecting and ongoing input and to Janet Harkess, Head
Occupational Therapy Rheumatology Service, Fife. The final thank you is reserved for patients who
gave their time and support to the pilot.
3
Contents
Acknowledgements 2
Executive Summary 4
Introduction 10
Methodology 12
Results 20
Discussion 38
Conclusion 41
The Way Forward 43
References 44
Appendices 45

4
Executive Summary
Background/Aims An increasing evidence base indicates that Vocational Rehabilitation (VR) can be effective in helping
people stay in or return to work. VR can be defined as “whatever helps someone with a health
problem to stay at, return to and remain in work” (Waddell et al, 2008).
Rheumatology Occupational Therapists (OT) work as part of a multi-disciplinary team treating people
with a wide variety of long term conditions such as rheumatoid arthritis and routinely explore any
work issues as part of the assessment process. Research literature shows that even at early diagnosis
individuals can experience works difficulties and this increases with time (NRAS, 2010). There are
barriers and challenges to remaining in employment, such as pain and fatigue, physical demands of
work, travel, lack of adaptations and modifications, lack of family support, time off sick and
problems with colleagues (Hammond, 2008).
The aims of this practice analysis are as follows:
To provide timely intervention to meet the needs of clients in relation to their work issues.
To provide information and resources to support clients in the workplace.
To make recommendations that would support the client return to the workplace and
sustain employment.
Methodology
As well as demographic information, a range of outcome measures were used at initial assessment
and at discharge from the service. This included, details of the OT intervention undertaken;
outcomes from workplace assessments; and qualitative telephone interviews with patients. The
outcome measures that were selected were SF-36, Euro QoL 5D, Pain and Fatigue Visual Analogue
Scales, Early Morning Joint Stiffness, Number of Days incurring sick absence and/or reduced
productivity and perceptions of Future Work ability. The pilot ran from January 2010 to January
2011. The pilot was based on one hospital site in Glasgow.
Results
A summary of the results are as follows;
46 patients were referred to the VR service during this period.
Complete data was collected on 21 patients during that period.

5
Demographic Information of Patients ____________________________________________________________________________ Gender n=46 Female 37 Male 9 Age n=46 Average 46 years Range 20-67 years Length of Time Since Diagnosis n=29 Average 8.25 years Range 1-40 years Employment n=29 Average length of Time 12.2 years Range 3-40 years Work Status n=21 In Work at Initial Assessment 16 In Work at Discharge 19 ____________________________________________________________________________ Employment Status The graph below shows patients work status at initial assessment versus work status at discharge.
This graph represents only patients who completed intervention, n=21 in order to determine the pre
and post responses.
Graph 1: Work Status at Initial Assessment versus Work Status, n=21
6
Employer Awareness Patients were asked if their employer was aware of their condition. The responses of completed,
withdrawn patients and not appropriate referrals n=29, was taken into account. The findings showed
that n=14 reported that their employers were not aware of their condition and n=15 reported that
their employers were aware.
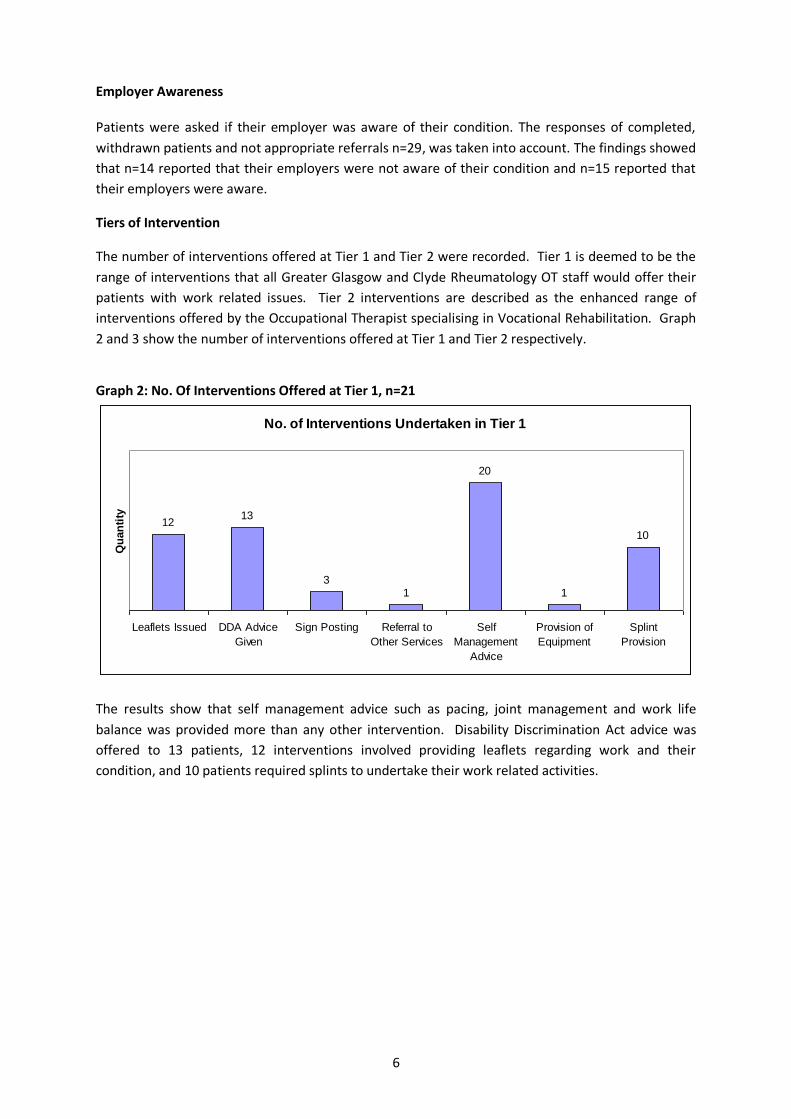
Tiers of Intervention
The number of interventions offered at Tier 1 and Tier 2 were recorded. Tier 1 is deemed to be the
range of interventions that all Greater Glasgow and Clyde Rheumatology OT staff would offer their
patients with work related issues. Tier 2 interventions are described as the enhanced range of
interventions offered by the Occupational Therapist specialising in Vocational Rehabilitation. Graph
2 and 3 show the number of interventions offered at Tier 1 and Tier 2 respectively.
Graph 2: No. Of Interventions Offered at Tier 1, n=21
No. of Interventions Undertaken in Tier 1
1213
31
20
1
10
Leaflets Issued DDA Advice
Given
Sign Posting Referral to
Other Services
Self
Management
Advice
Provision of
Equipment
Splint
Provision
Qu
an
tity
The results show that self management advice such as pacing, joint management and work life
balance was provided more than any other intervention. Disability Discrimination Act advice was
offered to 13 patients, 12 interventions involved providing leaflets regarding work and their
condition, and 10 patients required splints to undertake their work related activities.

7
Graph 3: No. Of Interventions Offered at Tier 2, n=21
The range of interventions at Tier 2 shows that workplace assessments, written reports and liaising
with employers and other services dominated the type of interventions offered. A total of 5 patients
were offered return to work programmes; a further 4 were offered job demands analysis in relation
to their work; 4 patients received self help advice using CBT principles, for example managing low
mood and anxiety, and 2 patients were provided with a letter for their employer recommending and
supporting equipment provision.
Workplace Assessment
Workplace assessments were offered as part of the range of vocational rehabilitation Tier 2
interventions. In total 8 workplace assessments was undertaken and 52% of the workplace
assessment recommendations were undertaken or implemented by the patient or line manager.
Table 2 highlights the reasons why recommendations were not implemented.
Table 2 – Workplace Assessment Recommendation Outcome
No. of
Recommendations
No.
Implemented
Comments
7 6 Support worker requested and funded through Access to
Work
6 0 Unable to self fund recommendations initially, in spite of
grant being awarded from Access to Work.
3 2 Work was supportive in applying changes but pt
struggling to adapt to these changes
8 6 Waiting on IT equipment. Ongoing dispute of core tasks
within the role
8
5 1 Parking was paid for by Access to Work, employer did not
support other recommendations
4 4 Employer also facilitated a graded return to work
programmed
2 1 Employer is looking for ways to move the pt closer to
home for work to minimise travelling time
5 1 Access to Work provided chair, employer refused to
support any other recommendations
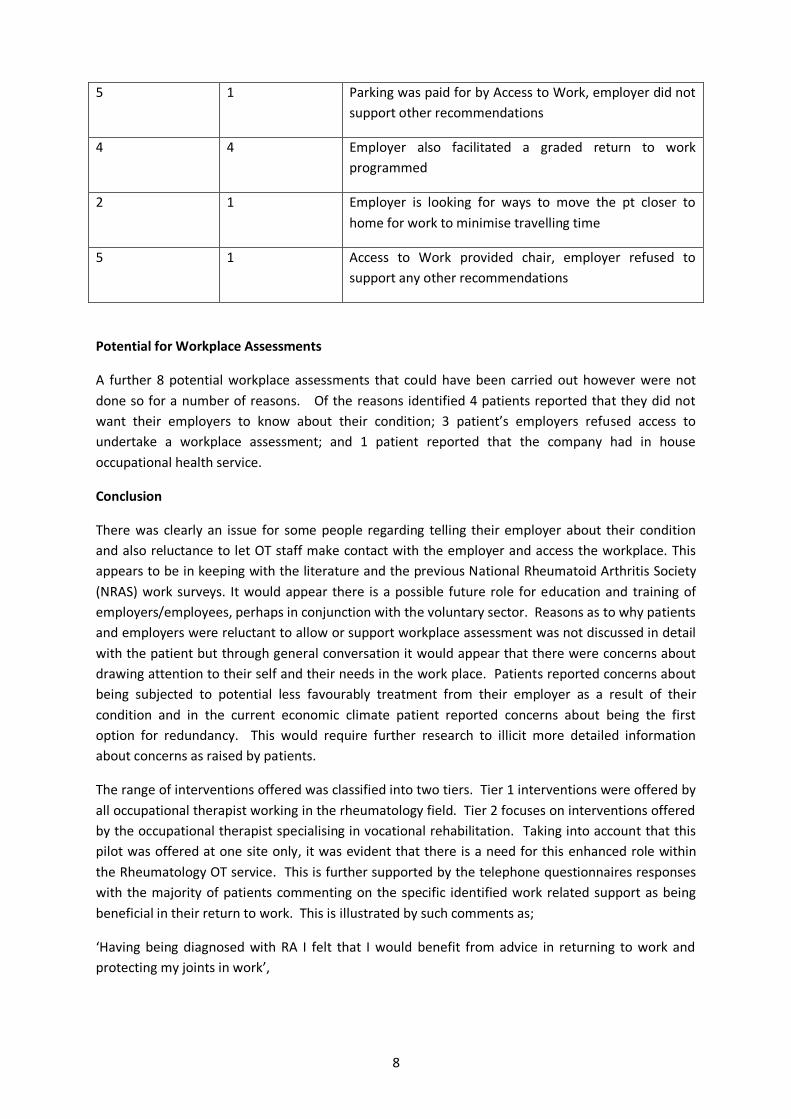
Potential for Workplace Assessments
A further 8 potential workplace assessments that could have been carried out however were not
done so for a number of reasons. Of the reasons identified 4 patients reported that they did not
want their employers to know about their condition; 3 patient’s employers refused access to
undertake a workplace assessment; and 1 patient reported that the company had in house
occupational health service.
Conclusion
There was clearly an issue for some people regarding telling their employer about their condition
and also reluctance to let OT staff make contact with the employer and access the workplace. This
appears to be in keeping with the literature and the previous National Rheumatoid Arthritis Society
(NRAS) work surveys. It would appear there is a possible future role for education and training of
employers/employees, perhaps in conjunction with the voluntary sector. Reasons as to why patients
and employers were reluctant to allow or support workplace assessment was not discussed in detail
with the patient but through general conversation it would appear that there were concerns about
drawing attention to their self and their needs in the work place. Patients reported concerns about
being subjected to potential less favourably treatment from their employer as a result of their
condition and in the current economic climate patient reported concerns about being the first
option for redundancy. This would require further research to illicit more detailed information
about concerns as raised by patients.
The range of interventions offered was classified into two tiers. Tier 1 interventions were offered by
all occupational therapist working in the rheumatology field. Tier 2 focuses on interventions offered
by the occupational therapist specialising in vocational rehabilitation. Taking into account that this
pilot was offered at one site only, it was evident that there is a need for this enhanced role within
the Rheumatology OT service. This is further supported by the telephone questionnaires responses
with the majority of patients commenting on the specific identified work related support as being
beneficial in their return to work. This is illustrated by such comments as;
‘Having being diagnosed with RA I felt that I would benefit from advice in returning to work and
protecting my joints in work’,
9
‘OT carried out a detailed interview about background, general health, to identify any problems
/issues, especially at work, to enable me to stay in work’
‘Yes, I don’t think that I would be able to remain in work without the service. I have been able to
park nearer’ and so forth.
‘I had been working full time, but off work, this helped me return to work’
These comments give weight to the benefits of a targeted approach of enhanced OT interventions to
support the patient to remain in work. The range of interventions offered at Tier 2 is specifically
work related and offered a higher level support and work based assessment/intervention than
would be offered at Tier 1.
The Way Forward
The pilot was available on only one site in order to make best use of the staff resource and
since there was an existing facility on that site. Assessment equipment and resources were
gathered over the period of the pilot from some limited funding. To deliver a VR service on
other sites will require development of resources and tools to be used in the assessment
process.
Equity of service, accessing resources and future development needs of OT staff need to be
examined in relation to offering the various enhanced aspects of VR within the service.
Exploring service delivery in this context will require further discussions with OT staff to
explore ways of providing and developing the service. This may include such aspects as
using the existing expertise within the team to offer job shadowing opportunities, having VR
clinics on different sites and development of a VR training plan to up skill all OT staff where
necessary.
The use of appropriate screening tools or referral criteria would perhaps ensure that those
patients who required support accessed the service when they require it. Increasing
awareness of the Rheumatology team about the role of VR and how to refer would also be
required. Also copying any workplace assessments to our Rheumatology consultants would
facilitate good communication relating to work.
Development of an information pack for patients and employers may also be useful.
Future considerations should perhaps also include developing functional capacity
assessments and sharing and developing skills with other specialties in the context of the
policy drivers that support the vocational rehabilitation agenda.
10
Introduction
Work/Employment plays an important part in maintaining, promoting and improving physical and
mental health. In recent years there has been growing evidence that assisting and supporting people
to remain and return to work has not only individual benefits but also benefits the economy and
society as a whole, (Armstrong & Wilkie 2010).
The demographics of society are changing. As a population we are living longer, having to manage
long term conditions and co-morbidities.
In Dame Carol Black’s report, Working for a Healthier Tomorrow (2008), she highlights the need for
healthcare professionals to consider the individual’s work status in their interventions. Figures
estimate in the report that 175 million working days were lost to illness in 2006, and that common
health problems such as musculoskeletal and mental health disorders are the major cause of
sickness absence and worklessness in the United Kingdom, (Black 2008).
This report has already led to changes including the introduction of the Fit Note and pilots looking at
improving access to Occupational Health services.
There are various current political, health and social drivers highlighting the importance of
supporting individuals to manage their health with work being an aspect of self care. The Co-
ordinated, Integrated and Fit for Purpose, A Delivery Framework for Rehabilitation in Scotland
(2007) indicates the need for vocational rehabilitation (VR) to be delivered in order to support those
with long term conditions to remain in or return to work, (Scottish Executive 2007).
Work abilities can be affected by a range of factors including changes in physical and mental health,
psychological pressures, organisational issues, environmental and social issues.
There is an evidence base indicating that VR can be effective in helping people stay in or return to
work. Waddell et al (2008) define VR as “whatever helps someone with a health problem to stay at,
return to and remain in work”. The report synthesizes the evidence and concludes that there is a
strong case for various aspects of VR and that healthcare has a role to play.
Occupation and productivity is fundamental to Occupational Therapy. Therefore, work is seen as
important to the individual and their well- being. In the College of Occupational Therapists
Vocational Rehabilitation strategy document ,Work Matters, they state “OTs help people to
maximize employment opportunities by developing strategies to prevent injury or illness in the
workplace, ensuring health and safety at work, and carrying out workplace assessments, task
analysis, capacity and motivation building and absence management”.
Rheumatology Occupational Therapists work as part of a multi-disciplinary team treating people
with a wide variety of long term conditions such as inflammatory arthritis, connective tissues
diseases and degenerative conditions, such as osteoarthritis. Literature research identifies two key
points in relation to rheumatoid arthritis and work; firstly that even at early diagnosis individuals
experience works difficulties and this increases with time; and secondly that there are barriers and
challenges to remaining in employment such as pain and fatigue, physical demands of work, travel,
lack of adaptations and modifications, lack of family support, time off sick and problems with
colleagues, (Hammonnd, 2008, Allaire et al 2003).

11
In day to day practice it has become increasingly apparent that work issues are being identified
within the OT assessment especially with regards to work retention. This observation was further
supported by a local audit carried out in 2005. It was identified that work issues experienced by our
patients mirrored those concerns and issues raised in the research of literature. The main common
factors influencing work disability in RA, as described by Frank and Chamberlin 2001, included;
Employment factors, e.g. the nature of the job, the physical activity needed, the degree of
autonomy at work, the work environment and transport.
Employee factors, e.g. age of onset of rheumatoid arthritis, marital status, education and
motivation for work.
Disease factors e.g. time since onset, level of disability and symptoms affecting disability
(early morning stiffness, loss of limb function, recurrent flare-ups and general disability.
Other factors included visits to the G.P. or hospital and in-patient care.
A randomized control trial undertaken by Macedo et al (2009) focused on the benefits of OT and
demonstrates that both functional and work outcomes improved following specific interventions
such as ergonomic reviews, liaison with employers and self management education. It was
speculated that a more coordinated OT approach to support working patients with health needs stay
in work or return from sick leave was required. In light of current literature research, the
rheumatology occupational therapy service agreed there was an increasing need to explore
vocational rehabilitation interventions. In structuring the pilot the following aims were agreed;
To provided a robust and timely intervention to meet the needs of clients in relation to their work issues.
To provide information and resources to support clients in the workplace.
To make recommendations that will support the client return to the workplace and sustain employment.
The pilot was based on a resource of 0.5 WTE Band 6 OT post running for 18 months to include staff
induction and training, project set up, patient recruitment and following evaluation.

12
Methodology
The development of the VR pilot was divided into three key phases of development; information
gathering and consultation with others offering similar services; creating a paperwork and referral
pathway for use with patients accessing the service and; developing an audit structure in which to
evaluate the outcomes of the pilot.
Phase 1
Information Gathering
A period of consultation and liaison with OT in other areas that were providing a similar service was
undertaken. This included visits to Edinburgh Astley Ainslie Hospital who deliver an OT led
occupational health service for NHS employees. Information gathered on this visit included
paperwork pathways; use of assessment and outcome measures; referral criteria for access to the
service; range of interventions offered to patients and resources and equipment used. In
development of this VR pilot the OT also visited a specialist rheumatology OT service that offered a
VR service to their patients in Fife. From this visit information was gathered in regards to
interventions and use of resources that were used in delivering a VR service specifically for the
rheumatology patient.
A literature search was also undertaken to identify similar projects and pilots within this field of
practice. In undertaking the literature search focus was given to the outcome measures used, range
of interventions offered and findings of pilots and studies undertaken as well as focusing on
condition specific approaches within the VR field.
Early in the consultation process it was decided that this VR pilot would only be offered to patients
who were in employment but were experiencing difficulty with requirements of their job due to
their health condition. The patient could either be at work or on sick leave in order to access the
service. During the consultation process it was decided that the needs of rheumatology patients,
who were not working, was being meet through employability initiatives such as those offered by
the Department of Work and Pensions and other employability partners.

13
Phase 2
Developing the Vocational Rehabilitation Service
In developing the VR service within the Rheumatology OT service a number of aspects needed to be
considered to ensure optimum and seamless approach in offering a range of interventions to the
patient. The following aspects were implemented;
Pilot Base
Due to original funding sources and capacity of the occupational therapist it was agreed that the
pilot should be based solely with the Southern General Hospital. This approach allowed for a
contained approach in delivering services within one area and making best use of OT’s time.
Referral Pathway
Using information gathered from the consultation period and reflecting on the needs of the patient
group, the pathway to access the vocational rehabilitation service was developed. The point of
entry into the service was via referral from medical staff, Rheumatology OT staff and clinical nurse
specialist. Screening was carried out by the vocational rehabilitation OT and if any additional
identified needs i.e. difficulties with ADL tasks, then patient could be cross referred to mainstream
OT Rheumatology service.
Developing the Paperwork Pathway
Consent
At first session with VR OT the patient was consented for interventions, see appendix 1 for consent
form. The consent form was discussed with the patient and any queries answered. The patient was
informed verbally and in writing that should they consent the information gathered will be used in
the evaluation of the pilot. The consent form also sought agreement from the patient to contact
their employer should this be necessary to address and resolve any health related issues in the
workplace.
Initial Assessment
The initial interview encompassed the following aspects of the patient’s health and the workplace;
Background History
Current Employment
Job Tasks

14
Work Environment
Prevocational Skills
Summary and Goals Agreed
(See appendix 2 for copy of initial vocational rehabilitation assessment)
Range of Interventions Offered
To decide which interventions to offer as part of the VR, meetings were held with rheumatology
occupational therapists, health improvement practitioners and line managers. It was decided by the
group that the tiered aspect would allow for a more timely approach of the range of interventions
offered, thus allowing more appropriate access to VR.
Adopting a tiered approach allowed access at various points of the service for all patients referred.
This approach also allowed patients to re-access the service at another tier should their condition
change or engaging in work becomes difficult/ challenging again. The tiered approach was classed
into three main areas are described as follows;
First Tier – Undertaken by all OTs within the Rheumatology Service
Leaflet Issued
Providing information or increasing awareness of Disability Discrimination Act
Sign Posting to other services
Referrals to other services
Providing self management advice
Provision of Equipment
Splint provision
If it was considered that further input and/ or advice was required, the patient could be referred to
the vocational rehabilitation service at the second tier, that is patients who required more specific
information, advice, assessment or adaptation to support them return to the workplace or consider
their work options.
15
Second Tier – Undertaken by the Vocational Rehabilitation Occupational
This second tier of VR was undertaken by the vocational rehabilitation OT. The second tier offered a
wider, more specialised range of interventions to enable a client to remain at work or return to
work. The interventions were goal specific and work orientated and included the following;
Job task analysis
Joint protection in the workplace
Ergonomics assessment
Workplace assessment
Liaising with the employer
Job modification
Work hardening
Sign posting and referral to other services
Accessing for work related equipment and adaptation
Psychological intervention i.e. fatigue management
Working with clients to address the boundaries that limit returning to work
Third Tier – For Patients Who Have Previously Accessed the VR Service
The vision for this third tier was based on long term development of the service. This aspect of the
service would be a point of access and further intervention to manage flare-ups in condition and
where possible sustain a client at work during this time. The range of interventions available at this
point may have included;
Ongoing support
Further job modification
Recommendation for increased specialised equipment
Lifestyle and work-life balance programmes
Flare up management
Return to work programmes
Access and referral to services
Management of condition in workplace
Liaising and joint working with other AHPs with specialist interest in Rheumatology.

16
With the limitations of this pilot it has not been possible to evaluate this tier of the service and
would require further extended study.
Patient Information
During the consultation period it was agreed that a leaflet providing information about the VR
service would be beneficial. This leaflet, see appendix 3, explained the role of VR; the reason why
the patient had been referred; what to bring to the initial appointment; what to expect from the
appointment; informing that the vocational rehabilitation service was being piloted and contact
details.
Increasing Awareness of Vocational Rehabilitation Pilot
To increase awareness of the VR pilot a series of presentations was undertaken. A presentation
outlining the VR pilot was given to medical staff, nursing staff and allied health profession staff.
These sessions provided information about referral criteria; assessment process; range of
interventions offered; and an overview of the pilot evaluation. OTs contact details were also
provided for further information.
Phase 3
Phase three focused on developing the framework for evaluating the pilot. It was important from
the outset to build a robust process that allowed for seamless gathering of information from a
number of perspectives. The structure of the evaluation is illustrated in the following table 1a and
1b with table 1a outlining the tools used to gather information and table 1b describing the outcome
measures;

17
Table 1a –Informational Gather Tools
Information Gathering Tool Outcome
Initial Interview Demographic Information
Access to other services
Diagnosis
Job Type/ Descriptions
Achieved goal
See Appendix 2
Workplace Assessment Work Modifications recommended and
implemented.
Telephone Questionnaire – Patient Stories Undertaken by OT (not connected to the pilot)
to gather information about patient’s
perceptions of the vocational rehabilitation
service and any thoughts of future changes for
the service.
See appendix 6
Audit of Vocational Rehabilitation Issues on
other Sites
Rheumatology OTs based at the Gartnavel
General Infirmary, Glasgow Royal Infirmary and
New Victoria Hospital undertook an audit
focusing on potential for tier 2 VR interventions
for patients accessing their service.
See appendix 7
Summary Outcome Sheet Information gathered from the Initial Interview
and Outcome Measures were summarised on
one outcome sheet. This was to facilitate better
organisation of information gathered.
See appendix 8

18
In conjunction with the clinical effectiveness team a data base using the Microsoft Excel computer
software programme was devised. Information data gathered was recorded on the database and
used in the analysis.
Determining Outcome Measures
The advice and opinion of the range of outcome measures used in VR and rheumatology was sought
from a number of stake holders, this included, Rheumatology Consultants, OTs, vocational
rehabilitation peers and colleagues. The following criteria were used in selecting the outcome
measures;
Could be applied to all Rheumatologic conditions
Self reporting and easy to use
Encompassed health and well being
An indicator of work productivity
A measureable outcome of pain, fatigue and early morning joint stiffness
Table 1b further describes the reasons for selecting the outcome measure used in this pilot.
19
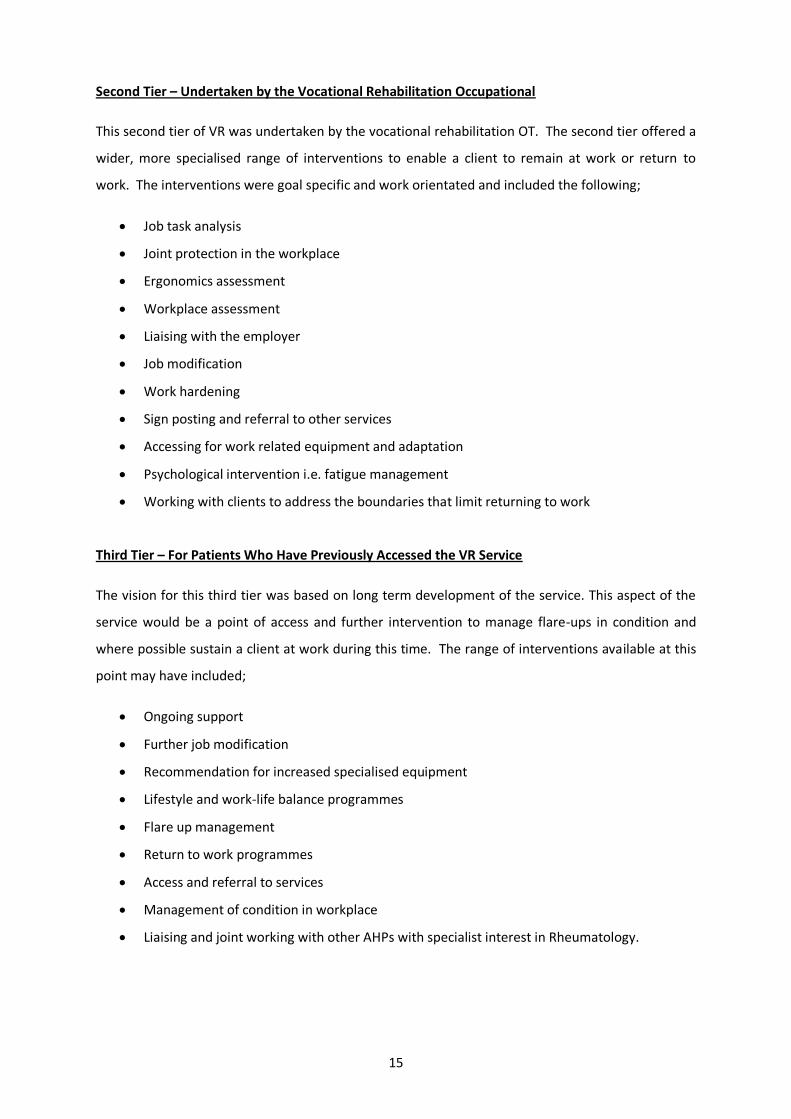
Table 1b – Outcome Measures
Outcome Measure Description Reason for Including in Pilot
Pain Visual Analogue
Scale
A visual pain scale of 0-10 was used. The
score of 0 indicated no pain, 5 - moderate
pain and 10-severe pain. Patient was ask to
consider their pain level over the last 7
days and rate their pain on the scale
Self administering
Quick to use
An indicator of a barrier to work
Fatigue Scale A scale of 1-5 describing fatigue was used.
1 – Indicated no fatigue through to 5 -
indicating very fatigued. Patient was asked
to consider their fatigue level over the last
7 days and rate this on the scale.
Self administering
Quick to use
An indicator of a barrier to work
Sick Absence and
Productivity
Patients are asked to consider how many
days that have been off work due to their
health condition.
Self administering.
Future work ability Patients are asked to consider if they are
likely to be working in one year, responses
are Yes, No and Don’t Know
Self administering. This question
reflects patient’s perception of their
likely hood of being in work in 1
year.
Euro QoL 5D This self reporting questionnaire consists of
2 sections but for the purpose of this study
the visual analogue scale is only used. The
patient rates their health by drawing a line
at the appropriate point that best indicates
their health on that day.
Self administering. Provides an
indication of the patient’s perceived
health state.
Quality of Life Measure
SF-36 This is a multi purposeful health survey.
Questions cover functional health and well
being. Well evidence reliability and validity.
Self administering, non condition
specific, comparing the relative
burden of diseases, and in
differentiating the health benefits
produced by a wide range of
different treatments.
20
Results
Analysis of Data
The data gathered from the initial interviews and outcome measures were entered onto a database.
This database was developed using the excel software programme and was utilised in the analysis of
the information.
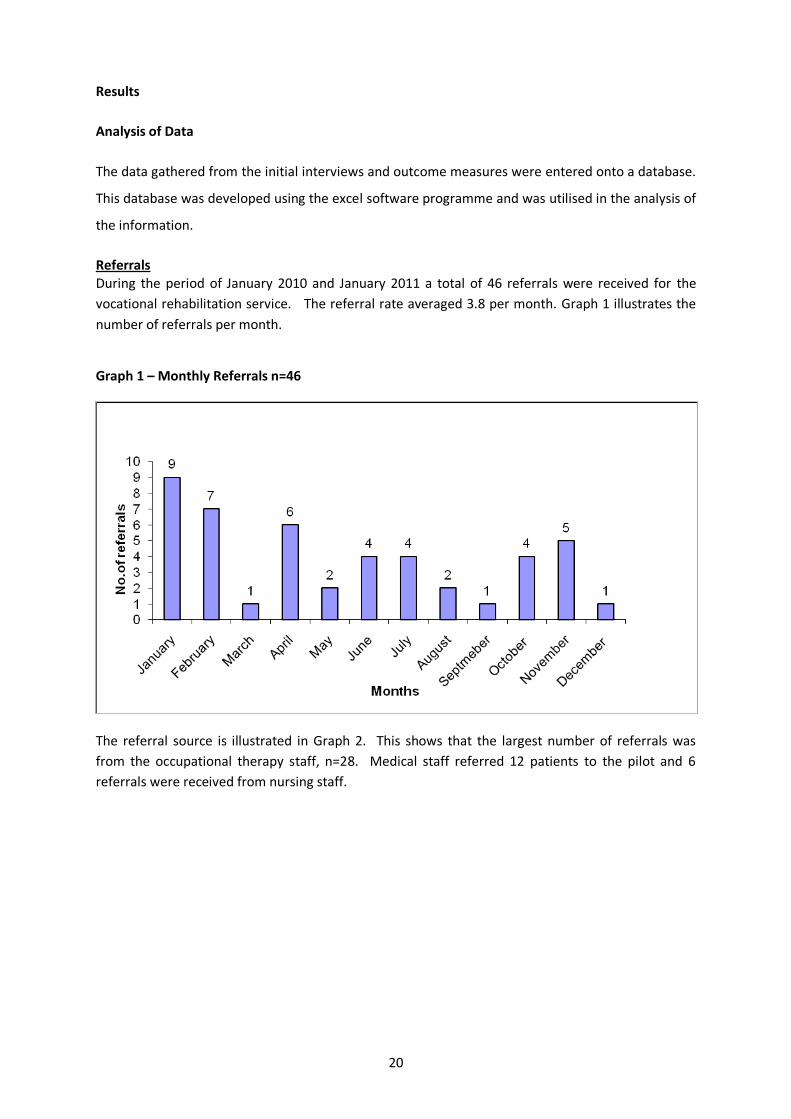
Referrals During the period of January 2010 and January 2011 a total of 46 referrals were received for the
vocational rehabilitation service. The referral rate averaged 3.8 per month. Graph 1 illustrates the
number of referrals per month.
Graph 1 – Monthly Referrals n=46
The referral source is illustrated in Graph 2. This shows that the largest number of referrals was
from the occupational therapy staff, n=28. Medical staff referred 12 patients to the pilot and 6
referrals were received from nursing staff.

21
Graph 2 – Referral Source n=46
The breakdown of the 46 referrals is as follows;
21 patients attended VR, completed the process and were discharged from the pilot.
8 patients attended for initial assessment, however did not return for further appointments
and were therefore deemed to have withdrawn from the pilot.
9 patients did not attend any initial assessment offered and therefore classed as did not
attend
8 patients were considered not appropriate referrals.
The 8 patients were not considered appropriate for the VR for the following the reasons;
4 referrals were for patients who were NHS Employees and were therefore referred onto
NHS OHSxtra.
3 referrals were for patients who were not in employment and therefore did not meet the
criteria.
1 referral was for a patient who was retired.
Patients who withdrew or did not attend the VR were sent a three week opt in letter after their first
missed appointment and were offered one further opportunity to attend.

22
Demographics Table 2 – Demographic Information of Patients _________________________________________________________________________ Gender n=46 Female 37 Male 9 Age n=46 Average 46 years Range 20-67 years Length of Time Since Diagnosis n=29 Average 8.25 years Range 1-40 years Employment n=29 Average length of Time 12.2 years Range 3-40 years Work Status n=21 In Work at Initial Assessment 16 In Work at Discharge 19 _________________________________________________________________________ Age Range of Patients Referred
Graph 3 illustrates the age range of patients referred for VR. The largest group was 46-55 years old
which is indicative of this patient group who have Rheumatology conditions and may reflect age of
onset for some inflammatory conditions.
Graph 3: Referred Patients to VR Pilot, n=46
23
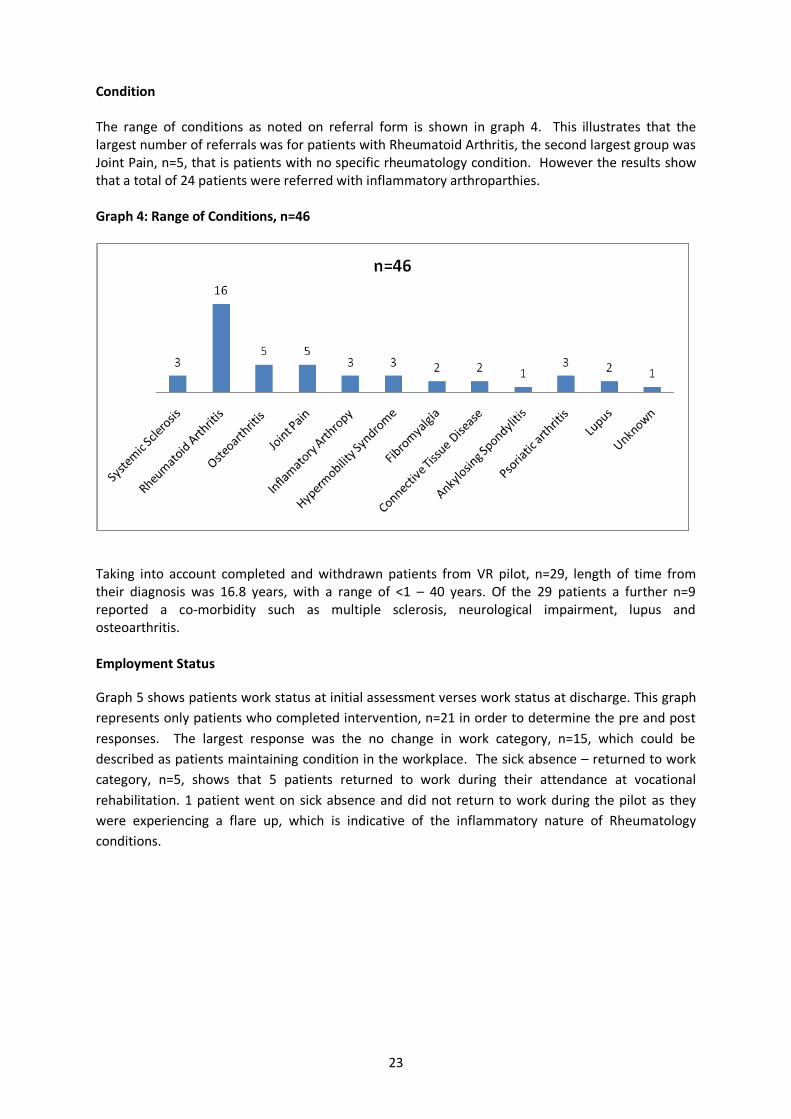
Condition The range of conditions as noted on referral form is shown in graph 4. This illustrates that the largest number of referrals was for patients with Rheumatoid Arthritis, the second largest group was Joint Pain, n=5, that is patients with no specific rheumatology condition. However the results show that a total of 24 patients were referred with inflammatory arthroparthies. Graph 4: Range of Conditions, n=46
Taking into account completed and withdrawn patients from VR pilot, n=29, length of time from their diagnosis was 16.8 years, with a range of <1 – 40 years. Of the 29 patients a further n=9 reported a co-morbidity such as multiple sclerosis, neurological impairment, lupus and osteoarthritis. Employment Status
Graph 5 shows patients work status at initial assessment verses work status at discharge. This graph
represents only patients who completed intervention, n=21 in order to determine the pre and post
responses. The largest response was the no change in work category, n=15, which could be
described as patients maintaining condition in the workplace. The sick absence – returned to work
category, n=5, shows that 5 patients returned to work during their attendance at vocational
rehabilitation. 1 patient went on sick absence and did not return to work during the pilot as they
were experiencing a flare up, which is indicative of the inflammatory nature of Rheumatology
conditions.

24
Graph 5: Work Status at Initial Assessment vs. Work Status at Discharge, n=21.
Employer Awareness
Patients were asked if their employer was aware of their condition. The responses of completed,
withdrawn patients and not appropriate referrals n=29, was taken into account. The findings showed
that n=14 reported that their employers were not aware of their condition and n=15 reported that
their employers were aware.
Job Type
Patients were asked how they rated their job in terms of level of physical activity required. Patients
had the option of five choices. Table 3 illustrates patient’s responses. Those job types highlighted in
red, post office assistant and post mistress, where perceived by author to be similar roles however
classed differently by the patients.

25
Table 3 - How Patients Perceived their Job Type: Completed & Withdrawn n=29
Job Types
Sedentary Light Moderate Physical Heavy
Warranty Officer
Business Manager
Bank Teller x 2
Administration x 3
Cashier (Shop)
Voluntary Sector
Worker
Book Maker
NHS Employee
G.P. Receptionist
Senior Care Worker
Post Office Assistant
Health Visitor
Teacher
Social Care
Worker
Mechanic
Landscape Gardiner
Bar Manager
Classroom Assistant x 2
(Special Needs)
Cleaner x 2
Catering Assistant
Chef
Nurse A&E
Shop Assistant
Store Assistant
Dentist
Post Mistress
Hours At initial assessment and discharge the number of hours the patient worked was recorded. The purpose of this measurement was to identify any changes in hours worked at pre and post interventions. The average number of hours worked at initial assessment was 26 hours and at discharge 30 hours, the range of hours worked was 0-50 hours. Graph 6 – The Change in the Number of Hours Work at Initial Assessment vs. Discharge, n=21.

26
Sick Absence and Productivity Sick absence and productivity was recorded at initial assessment and discharge. Patients were asked to record the numbers of days that they were absent from their work due to their Rheumatology condition. Graph 7 illustrates the changes in recorded sick absence from initial assessment and discharge. Graph 7 – Changes in Sick Absence from Initial Assessment to Discharge, n=21
Patients were also asked to consider how many days they experienced reduced productivity, that is
not achieving all that they needed to do in work, asking colleagues to undertake or finish tasks for
them or leaving work early due to their health condition, in the last six months. Patients were asked
this question at initial assessment and discharge. Graph 8 shows the changes in work productivity
from initial assessment and discharge.
Graph 8 – Changes in Productivity Level Initial Assessment vs. Discharge, n=21.
Outcome Measures Patients were asked to complete a series of outcome measures at pre initial assessment and at discharge. The outcome measures were chosen to reflect disease impact and quality of life. The results are described according to each outcome measure.
20
1
Increased Productivity Levels Reduced Productivity Levels
27
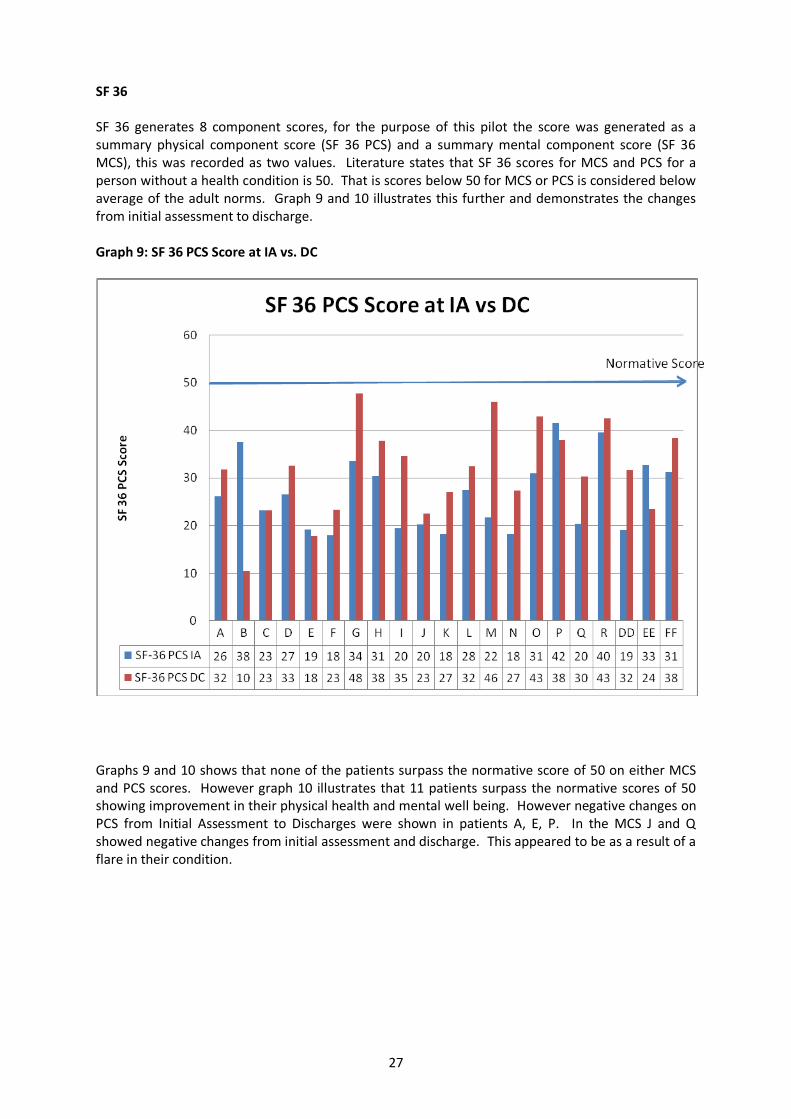
SF 36 SF 36 generates 8 component scores, for the purpose of this pilot the score was generated as a summary physical component score (SF 36 PCS) and a summary mental component score (SF 36 MCS), this was recorded as two values. Literature states that SF 36 scores for MCS and PCS for a person without a health condition is 50. That is scores below 50 for MCS or PCS is considered below average of the adult norms. Graph 9 and 10 illustrates this further and demonstrates the changes from initial assessment to discharge. Graph 9: SF 36 PCS Score at IA vs. DC
Graphs 9 and 10 shows that none of the patients surpass the normative score of 50 on either MCS and PCS scores. However graph 10 illustrates that 11 patients surpass the normative scores of 50 showing improvement in their physical health and mental well being. However negative changes on PCS from Initial Assessment to Discharges were shown in patients A, E, P. In the MCS J and Q showed negative changes from initial assessment and discharge. This appeared to be as a result of a flare in their condition.

28
Graph 10: SF 36 MCS Score at IA vs. DC
EuroQoL The EuroQol is a quality of life outcome measure. The patient was asked to rate their health on a scale of 0-100 with 0 being worst possible health state and 100 indicating their best possible health state. These scores were taken at pre and post vocational rehabilitation intervention, n=21. Graph 11 illustrates this further and shows the changes in EuroQoL score between initial assessment and discharge. Graph 11 – Changes in EuroQoL Score Initial Assessment vs. Discharge, n=21
1
16
4
No Change Increased EuroQoL Score Decreased EuroQoL Score

29
Pain Visual Analogue Scale Patients were asked to record their pain scores on a scale of 0-10 pre and post intervention. The
average pain score at initial assessment was 7.2 and an average pain score 5.25 was recorded at
discharge. Graphs 12 shows changes in pain scores at pre and post intervention and illustrates that
90% reported a decrease in pain and 10% noted an increase in pain levels.
Graph 12 – Changes in Pain Levels Initial Assessment vs. Discharge, n=21
Fatigue Scores
Patients were asked to record their fatigue levels on a scale of 1-5 pre and post intervention. The
average fatigue score of 4.1 was recorded at initial assessment and fatigue score of 3.25 at
discharge. Graph 13 illustrates changes in pain score at pre and post interventions. Overall graph 13
illustrates that 57% reported a decrease in fatigue levels and 14% noted an increase in fatigue levels
and 29% recorded no change between pre and post intervention.
Graph 13 – Changes in Fatigue Levels Initial Assessment vs. Discharge, n=21
Early Morning Joint Stiffness Patients were asked to record their Early Morning Joint Stiffness, in intervals of 0, ½ , 1, 1 ½ , 2 hours pre and post intervention (although this information was converted to minutes). Graphs 14
30
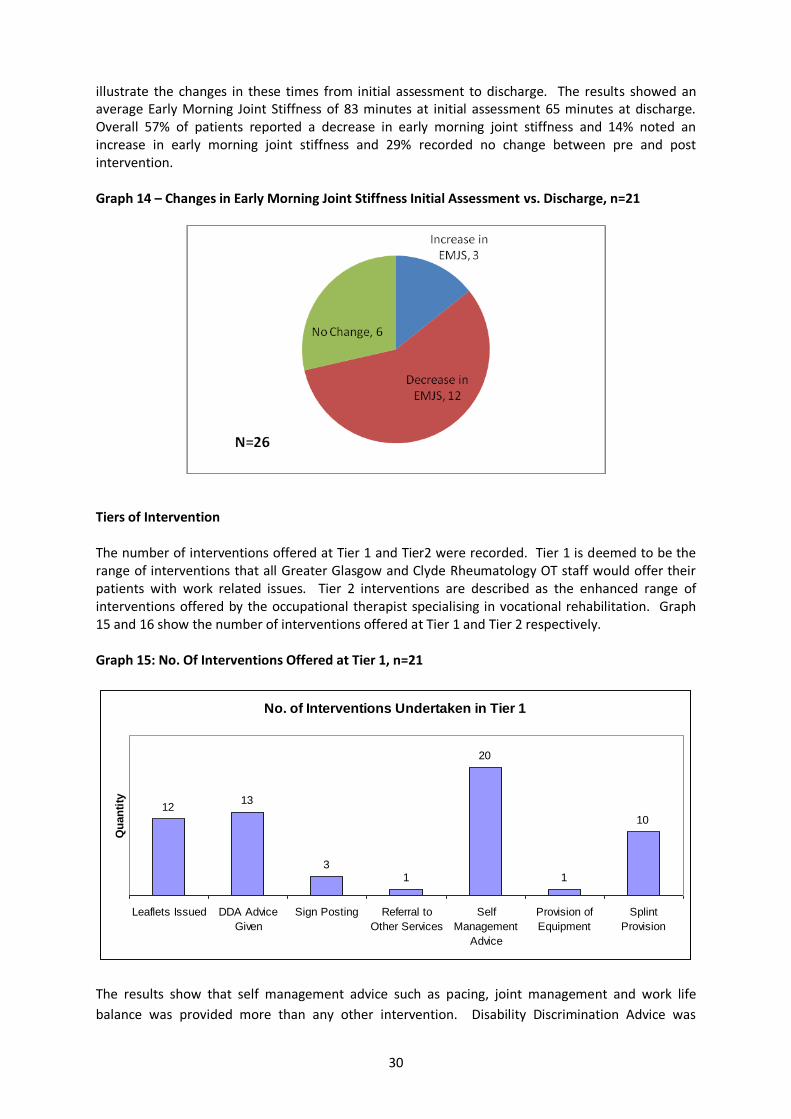
illustrate the changes in these times from initial assessment to discharge. The results showed an average Early Morning Joint Stiffness of 83 minutes at initial assessment 65 minutes at discharge. Overall 57% of patients reported a decrease in early morning joint stiffness and 14% noted an increase in early morning joint stiffness and 29% recorded no change between pre and post intervention. Graph 14 – Changes in Early Morning Joint Stiffness Initial Assessment vs. Discharge, n=21
Tiers of Intervention The number of interventions offered at Tier 1 and Tier2 were recorded. Tier 1 is deemed to be the range of interventions that all Greater Glasgow and Clyde Rheumatology OT staff would offer their patients with work related issues. Tier 2 interventions are described as the enhanced range of interventions offered by the occupational therapist specialising in vocational rehabilitation. Graph 15 and 16 show the number of interventions offered at Tier 1 and Tier 2 respectively. Graph 15: No. Of Interventions Offered at Tier 1, n=21
No. of Interventions Undertaken in Tier 1
1213
31
20
1
10
Leaflets Issued DDA Advice
Given
Sign Posting Referral to
Other Services
Self
Management
Advice
Provision of
Equipment
Splint
Provision
Qu
an
tity
The results show that self management advice such as pacing, joint management and work life
balance was provided more than any other intervention. Disability Discrimination Advice was

31
offered to 13 patients, 12 interventions involved providing leaflets regarding work and their
condition and 10 patients required splints to undertake their work related activities.
Graph 16: No. Of Interventions Offered at Tier 2, n=21
The range of interventions at Tier 2 shows that workplace assessments, written reports and liaising
with employers and other services dominated the type of interventions offered. A total of 5 patients
were offered return to work programmes; a further 4 were offered job demands analysis in relation
to their work; 4 patients receiving self help advice using CBT principles, for example managing low
mood, managing anxiety etc; and 2 patients were provided with a letter for their employer
recommending and supporting equipment provision.
Patients Perception of Remaining in Work at Initial Assessment and Discharge
Patients were asked at initial assessment and discharge their perceptions of being in work 6 months
time. Patients were provided with the responses of Yes, No and Do Not Know as response. Table 4
illustrates these results;
Table 4: Patients Perception of Remaining in Work at Initial Assessment and Discharge, n=21.
Yes No Do Not Know
Initial Assessment 9 3 9
Discharge 16 2 3
Difference 7 1 6
% 77% more patients thought that they would remain in work in 6 months at discharge
33% less patients thought that they would not be in work in 6 months at discharge
66% less patients remain unsure that they would be in work in 6 months at discharge
32
Telephone Questionnaire
Patients who completed and were discharged from the vocational rehabilitation pilot were contacted by telephone and asked a series of questions in relation to
experience of the vocational rehabilitation. A data collector unconnected to vocational rehabilitation pilot undertook the telephone questionnaires to maintain
objectivity. The table 5 below highlights the trend in responses to each question, see appendix for further information.
Table 5 Samples of Telephone Questionnaire Responses
• I have poly arthritis and I have difficulty using a keyboard at work, I am a bank teller. My shoulders, neck, wrist and fingers are also affected
• My referral was suggested by OT in out patients. The decision to make referral was due to my increased symptoms that was affecting by employment status.
• Having being diagnosed with RA I felt I would benefit from advice in returning to work and protecting my joints while in work
Q.1 Firstly, can you tell me why you were referred to the service?
• OT carried out a detailed interview about background, general health to identify any problems/ issues, especially at work, to enable me to stay in work
• OT carried out a workplace assessment and was able to give weight to an office desk being moved to a more suitable position. OT also provided me with information on looking after your joints and made splints for me. She also organised for other splints to be sent.
Q. 2 What happened when you attended?

33
34
35
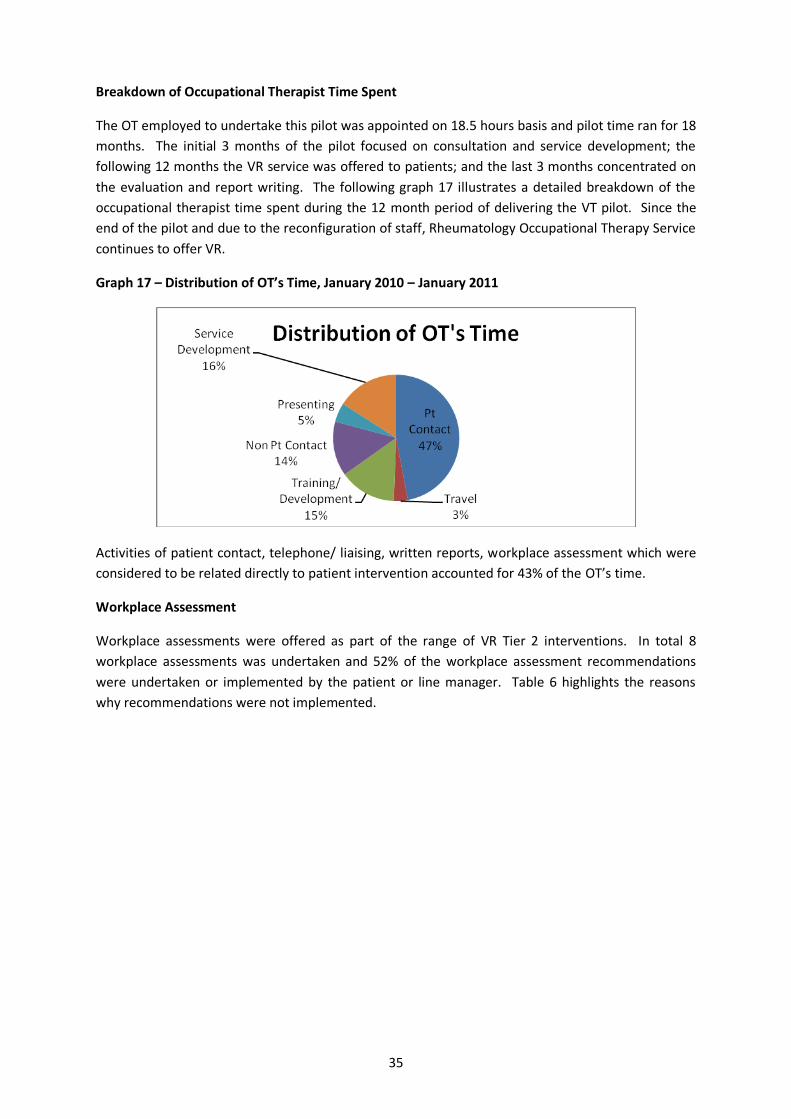
Breakdown of Occupational Therapist Time Spent
The OT employed to undertake this pilot was appointed on 18.5 hours basis and pilot time ran for 18
months. The initial 3 months of the pilot focused on consultation and service development; the
following 12 months the VR service was offered to patients; and the last 3 months concentrated on
the evaluation and report writing. The following graph 17 illustrates a detailed breakdown of the
occupational therapist time spent during the 12 month period of delivering the VT pilot. Since the
end of the pilot and due to the reconfiguration of staff, Rheumatology Occupational Therapy Service
continues to offer VR.
Graph 17 – Distribution of OT’s Time, January 2010 – January 2011
Activities of patient contact, telephone/ liaising, written reports, workplace assessment which were
considered to be related directly to patient intervention accounted for 43% of the OT’s time.
Workplace Assessment
Workplace assessments were offered as part of the range of VR Tier 2 interventions. In total 8
workplace assessments was undertaken and 52% of the workplace assessment recommendations
were undertaken or implemented by the patient or line manager. Table 6 highlights the reasons
why recommendations were not implemented.

36
Table 6 – Workplace Assessment Recommendation Outcome
No. of
Recommendations
No.
Implemented
Comments
7 6 Support worker requested and funded through Access to
Work
6 0 Unable to self fund recommendations initially, in spite of
grant being awarded from Access to Work.
3 2 Work was supportive in applying changes but pt
struggling to adapt to these changes
8 6 Waiting on IT equipment. Ongoing dispute of core tasks
within the role
5 1 Parking was paid for by Access to Work, employer did not
support other recommendations
4 4 Employer also facilitated a graded return to work
programme
2 1 Employer is looking for ways to move the pt closer to
home for work to minimise travelling time
5 1 Access to Work provided chair, employer refused to
support any other recommendations
Potential for Workplace Assessments
A further 8 potential workplace assessments that could have been carried out however were not
done so for a number of reasons. These reasons are describes further in table 7. Of the reasons
identified 4 patients reported that they did not want their employers to know about their condition;
3 patient’s employers refused access to undertake a workplace assessment; and 1 patient reported
that the company had in house occupational health service.

37
Table 7 - Potential Workplace Assessments
Reasons why Work Place Assessment was not Carried Out
Line Manager refused, stating that they had in house support
Employer refused, patient did not ‘want to push it’
In house OH, no workplace assessment carried out, in spite of OT liaising with OH Nurse
Patient refused, did not want employees to know about her condition
Refused, did not want employer to know about condition
Refused, did not want employer to know about condition
Refused, did not want employer to know about condition
Employer refused did not respond to OT’s letter

38
Discussion
Anyone who did not attend or failed to attend follow up appointments was sent a letter
offering a further appointment if they contacted the service to arrange one. This ensured
that patients were given a further opportunity to access the service but did not tie up
further clinical time. It was not possible to contact these individuals to explore why they had
not attended due to the limitations of staffing resources and possible ethical issues.
However from information provided by patients during telephone calls it would appear that
there were issues about getting time off work to attend appointments or patients often had
a number of appointments to attend and were therefore prioritising their appointments.
The monthly referral rate to the pilot was variable. However the majority were from the
Rheumatology OTs and while this is not surprising it does raise the question regarding why
there were limited referrals from the rest of the Rheumatology team. It may be that in the
initial stages of the pilot more time was needed to make the wider Rheumatology team
aware of the service. Another possible reason could be lack of clarity around who should be
referred to the service and this may indicate a need to consider a clearer screening process
out or referral criteria. While in the initial stages of the pilot, awareness sessions were
carried for staff, however due to the limited nature of the pilot the service was not routinely
advertised in clinics /patients areas. Work is also a relatively new concept in the health
assessment process and therefore may be marginalised in the overall assessment process.
There may be more opportunity for clarity about how to refer if a screening process was
introduced to capture all potential patients.
There was clearly an issue for some people regarding telling their employer about their
condition and also reluctance to let OT staff make contact with the employer and access the
workplace. This appears to be in keeping with the literature and the previous National
Rheumatoid Arthritis Society work surveys. It would appear there is a possible future role for
education and training of employers/employees, perhaps in conjunction with the voluntary
sector. Reasons as to why patients and employers were reluctant to allow or support
workplace assessment was not discussed in detail with the patient but through general
conversation it would appear that there were concerns about drawing attention to their self
and their needs in the work place. Patients reported concerns about being subjected to
potential less favourable treatment from their employer as a result of their condition and in
the current economic climate patients reported concerns about being the first option for
redundancy. This would require further research to illicit more detailed information about
concerns as raised by patients.
While not everyone required a workplace assessment it is apparent that completion of these
assessments are time consuming since they require travel time, the assessment process,
liaison with relevant parties and production of a detailed report to highlight
recommendations. While this is a valid resource concern, many patients found the
workplace assessment process to be beneficial in addressing their health needs in the
workplace. From the telephone questionnaire, patients responded that they considered the
workplace assessment to be beneficial in identifying and addressing workplace issues and
also in raising awareness of their condition to their employer.

39
The choice of appropriate outcome measures was discussed at an early stage. Self reporting
measures were selected to try to capture disease activity, quality of life factors and the
quality of the service from the patient’s perspective. From the results it was evident that
there was some improvement shown in the symptom progress scores, i.e. early morning
joint stiffness, fatigue and pain visual analogue scores, however due to the structure of the
pilot it remains uncertain if these changes are a result of medication and flares resolving.
When the quality of life scores, EuroQoL and SF 36 MCS were analysed improvements were
shown in the majority of patients’ outcome measures. Improvement in the wellbeing aspect
of the scores may be as a result of improved coping strategies experienced by the patient as
a result of interventions. There was also an improvement of patients’ perception of whether
or not they would still be in work in 6 months time, at point of discharge. This response
maybe indicative of patients’ improved confidence in their abilities to manage their needs in
the workplace and increase awareness and assertiveness in regard to their rights. Patient
outcomes also reported an improvement in sick absence and work productivity and may also
contribute to the evidence that providing support to patients to manage their health
condition in the workplace may also increase their confidence and sense of increased
contribution to the workplace.
Information on productivity and sickness absence levels was gathered in terms of patient
reported sick days in the past year, as a result of their health condition. The results showed
76% of patients experienced no further sick days in the last six months at point of discharge.
When considering work productivity all but 1 patient recorded improved productivity levels
at their work. These results are significant as they may be interpreted in the financial
perspective of supporting patients to return to work and stay in work and the benefits this
has for the patient financially and to the wider economy. Research has been undertaken
into the cost benefits of VR and it shows that undertaking interventions and specific
targeted approach to health and work is cost effective to wider community and to the
individual, Geuskens A. et al Lacaille, D 2008.
The previous point is further supported by the results of work status recorded in terms of
returning to work from sick leave and retaining work. There appears to have been a positive
impact on both work retention and return to work. Whilst it cannot be argued in its purest
terms that this pilot was entirely responsible to facilitating this return to work and work
retention, however from an adjunct intervention approach VR appears to strongly support
the patients’ return to work.
The range of interventions offered was classified into two tiers. Tier 1 interventions were
offered by all occupational therapist working in the rheumatology field. Tier 2 focuses on
interventions offered by the occupational therapist specialising in VR. Taking into account
that this pilot was offered at one site only it was evident that there is a need for the
enhanced role of an OT with VR with these additional skills. This is further supported by the
telephone questionnaire responses with the majority of patients commenting on the specific
identified work related support as being beneficial in their return to work. This is illustrated
by such comments as ‘having being diagnosed with RA I felt that I would benefit from advice
in returning to work and protecting my joints in work’, ‘OT carried out a detailed interview

40
about background, general health, to identify any problems /issues, especially at work, to
enable me to stay in work’ ‘yes, I don’t think that I would be able to remain in work without
the service. I have been able to park nearer’ and so forth. These comments give weight to
the benefits of a targeted approach of enhanced OT interventions to support the patient to
remain in work. However what was clearly evident was the role of the self management
approach and the bio-psychosocial approach to supporting the patient manage to their
health appeared to have an impact in supporting patients return to work or stay in work.
The range of interventions offered at tier 2 is specifically work related and offered a higher
level of skills and support than what would be offered at tier 1.
When asking patients if they thought that they would be in work in 6 months time at point
of initial assessment and discharge there was marked changes in their responses. There was
a significant increase in patients responding ‘yes’ at discharge which indicated improved
confidence from the patient that they would be in work in 6 months time. This may be
attributed to better control of the disease symptoms; however it can be implied that an
increase in coping strategies, improved management of workplace activities, adaptation to
the workplace environment and overall increased assertiveness and management of their
condition may also significantly have improved patient’s perception of remaining in work.
Workplace assessment carried out as part of the pilot appeared to have some impact on the
patient’s ability to remain at work. There were a number of recommendations implemented
as a result of the workplace assessment carried out. These recommendations ranged from
minor changes in workplace activities to provision of equipment to support patients to
manage their health condition in the workplace. Patients’ feedback to the occupational
therapist that these changes to the workplace had an impact in their overall management of
their condition in the workplace. Telephone questionnaires further support this point as
patients’ feedback included ‘yes, I missed work and I was keen to get back to work. Now I
am due to return to work next week and adjustments have been made’ and ‘OT carried out a
workplace assessment and advised on protecting my joints while at work .... discussed what
tasks I could and couldn’t do through a traffic light system’. Patients’ also reported to the
OT that having a supportive backup from the VR service provided as one patient stated
‘information on your rights as an employee was helpful at a particularly worrying time’.
The telephone questionnaires undertaken by a third party gathered a depth of details in
regards to patients’ perceptions of the VR service that they attended. The responses were
overwhelming positive in regards to the service that they received. Patients’ commented on
the benefits of receiving this service in relation to returning to work with such comments as
‘I had been working full time, but off work, this helped me return to work’, ‘I would
definitely have dropped another day if I hadn’t accessed the service’ and ‘I feel that I
managed to stay in a job I loved’

41
Conclusion
The employment needs of the Rheumatology patient is well established in literature and there is a
growing popular trend of incorporating patients’ work issues in their health care journey. The
Glasgow Rheumatology OT service recognised the increasing health and work needs of this patient
group.
An audit undertaken in 2005, by the occupational therapy department, began to explore the work
related needs of this patient group and the range of interventions required to meet their needs.
From the 2005 audit the aims of this pilot was established.
This pilot aimed to deliver a robust and timely intervention to meet the needs of the patients and
this was addressed through the tiered approach of the VR service. This tiered approach allowed all
OTs to deliver the baseline of VR interventions. Patients who were considered to require further
support accessed the OT with specialist VR skills, ensuring that the more complex cases were offered
the right level of service at the most appropriate time. A toolbox of health and work resources and
information was developed to support the patient. This information was provided by all OTs at tier
1, however more specific and detailed information was also provided by the VR OT. The most
surprising aspect of the pilot was the majority of patients accessed self management and self help
advice in regards to managing their condition in the workplace. A number of patients required more
specific interventions such as self management approaches to address low mood, lack of confidence
and self esteem as well as managing pain and fatigue. Whilst it cannot be argued that that the pilot
solely prevented work loss in this patient group, from the results there was emerging evidence of
improved pain management, reduction in fatigue and improvements in overall wellbeing. These
factors contribute to patients improving their coping strategies and this subsequently appeared to
have an impact on their ability to remain in work for longer. Macedo et al 2009 study concludes that
a timely comprehensive occupational therapy intervention significantly improves functional and
work-related outcomes in employed patients with RA who are at risk of work loss.
Other aspects, such as increasing work productivity and reducing patients’ sick absence days of
those completed the process can also be considered as positive outcomes for both the patient and
society as a whole. However, other outcomes that could be perceived as positive, such as the
majority of patients reported an increased of belief that they will be in work in six months time.
The bio-psychosocial approach to delivering VR addresses the needs of the patient from a holistic
perspective. When a patient is initially diagnosed with a chronic health condition their initial
concerns tend to focus on symptoms control and regaining health and function. However it is also
important to address the patient’s employment needs as this outcome can be vital to the overall
health outcome. For the patient not to be in work or off work because of their health needs can
lead to concerns relating to finances, retaining work, maintaining social support and networks,
decreasing empowerment and confidence as well as a decrease on overall wellbeing.
Occupational therapists are well placed to deliver services to meet the VR agenda. As well as being
experts in the bio-psychosocial approach to delivering interventions and treatments the
occupational therapist also has a wide range of skills that pertain directly to VR. These skills include
expert knowledge of human occupation, purposeful activity including occupational analysis, graded
return to work/activity, modification and adaptation as well as the impact of using fatigue and pain
coping strategies in the workplace. Occupational Therapists can contribute significantly to enable

42
the patient to remain in work or return to work through extending the services offered to the
patient within the current Rheumatology services. Research and government drivers support and
build the case for offering a vocational rehabilitation service to minimise work loss with all patient
groups and occupational therapist come equipped with the skills and resources to offer this service.
Research also strongly argues the benefits to the patient, to economy and to healthcare as a whole
of supporting patient to remain in work or return to work. The cost benefit of delivering a VR service
outweighs the costs of running the service. Therefore, it is increasingly important as therapists and
health care providers that we continue to develop and extend our services to meet the needs of our
patients. It is also important for our working age patient group to continue working and contributing
to the wider society and economy. During the most vulnerable time of the patient’s journey it is
important to support the patient to consider their future aims and aspirations of returning to work
and retaining work in spite of their health needs. Meeting the patients’ work and health needs is
ideally placed at the heart of their overall health care journey to provide continuity of care with a
holistic approach to their needs.

43
The Way Forward
The pilot was available on only one site in order to make best use of the staff resource and
since there was an existing facility on that site. Assessment equipment and resources were
gathered over the period of the pilot from some limited funding. To deliver VR service on
other sites will require development of resources and tools to be used in the assessment
process.
Equity of service, accessing resources and future development needs of OT staff need to be
examined in relation to offering the various enhanced aspects of VR within the service.
Exploring service delivery in this context will require further discussions with OT staff to
explore ways of providing and developing the service. This may include such aspects as
using the existing expertise within the team to offer job shadowing opportunities, having VR
clinics on different sites and development of a VR training plan to up skill all OT staff where
necessary.
The use of appropriate screening tools or referral criteria would perhaps ensure that those
patients who required support accessed the service at the most appropriate time to meet
their needs. Increasing awareness of the Rheumatology team about the role of VR and how
to refer would also be required. Also copying any workplace assessments to our
Rheumatology consultants would facilitate good communication relating to work.
Development of an information pack for patients and employers may also be useful.
Future considerations should perhaps also include developing functional capacity
assessments and sharing and developing skills with other specialties in the context of the
policy drivers that support the VR agenda.

44
References
Allaire, S.H. 2004, "What work changes do people with arthritis make to preserve employment, and are such changes effective?", Arthritis & Rheumatism, vol. 51, no. 6, pp. 871-873.
Allaire, S.H., Li, W. & LaValley, M.P. 2003, "Reduction of job loss in persons with rheumatic diseases receiving vocational rehabilitation: a randomized controlled trial.", Arthritis & Rheumatism, vol. 48, no. 11, pp. 3212-3218.
Black, C.,Dame. 2008, Working for a healthier tomorrow, Department for Work and Pensions, London.
Cooper, N.J. 2000, "Economic burden of rheumatoid arthritis: a systematic review", Rheumatology, vol. 39, no. 1, pp. 28-33.
de Buck, P.D., le Cessie, S., van den Hout, W.B., Peeters, A.J., Ronday, H.K., Westedt, M.L., Breedveld, F.C. & Vliet Vlieland, T.P. 2005, "Randomized comparison of a multidisciplinary job-retention vocational rehabilitation program with usual outpatient care in patients with chronic arthritis at risk for job loss", Arthritis and Rheumatism, vol. 53, no. 5, pp. 682-690.
Frank, A.O. & Chamberlain, M.A. 2001, "Keeping our patients at work: implications for the management of those with rheumatoid arthritis and musculoskeletal conditions", Rheumatology, vol. 40, no. 11, pp. 1201-1205.
Geuskens, G.A., Hazes, J.M., Barendregt, P.J. & Burdorf, A. 2008, "Work and sick leave among patients with early inflammatory joint conditions.", Arthritis & Rheumatism, vol. 59, no. 10, pp. 1458-1466.
Lacaille, D., Sheps, S., Spinelli, J.J., Chalmers, A. & Esdaile, J.M. 2004, "Identification of modifiable work-related factors that influence the risk of work disability in rheumatoid arthritis.", Arthritis & Rheumatism, vol. 51, no. 5, pp. 843-852.
Long-Term Conditions Alliance Scotland. 2011, , Long-Term Conditions Alliance Scotland: people not patients. [Homepage of Long-Term Conditions Alliance Scotland], [Online]. Available: http://www.ltcas.org.uk [2011, May/27].
Macedo, A.M., Oakley, S.P., Panayi, G.S. & Kirkham, B.W. 2009, "Functional and work outcomes improve in patients with rheumatoid arthritis who receive targeted, comprehensive occupational therapy", Arthritis and Rheumatism, vol. 61, no. 11, pp. 1522-1530.
National Rheumatoid Arthritis Society. 2010, RA and work: employment and rheumatoid arthritis in Scotland. A national picture., National Rheumatoid Arthritis Society, Berkshire.
Talamo, J., Frater, A., Gallivan, S. & Young, A. 1997, "Use of the short form 36 (SF36) for health status measurement in rheumatoid arthritis", British journal of rheumatology, vol. 36, no. 4, pp. 463-469.
The College of Occupational Therapy. 2008, Work Matters, The College of Occupational Therapy, London.
The Scottish Executive. 2007, Co-ordinated, integrated and fit for purpose: a delivery framework for adult rehabilitation in Scotland., The Scottish Executive, Edinburgh.
G. Waddell, K. Burton &N. Kendall (2008) Vocational Rehabilitation: What works, for whom, and
when? The Stationary Office, London, www.tso.co.uk

45
Appendices
Appendix Page
1 Patient Consent 46
2 Vocational Rehabilitation Initial Assessment 48
3 Patient Information Leaflet 55
4 Outcome Measures 57
5 Outcome Measure SF 36 59
6 Telephone Questionnaire 65
7 Audit of Vocational Rehabilitation on other sites 66
8 Summary Outcome Sheet 67
9 Telephone Results 69
10 Case Study 73
46
Appendix 1
Patient Consent
Greater Glasgow and Clyde NHS Acute Trust
Rheumatology Occupational Therapy Department
Vocational Rehabilitation Department
Consent Form
Your have been referred to the Rheumatology Vocational Rehabilitation Department. This
department aims to support you return to work or stay in work. Working with you, to help you
manage your health condition in the workplace.
In order for us to provide this service we need to collect information about you and from time to
time to speak other relevant people who may be involved in your health care or assisting you return
to work.
All staff within the Vocational Rehabilitation Department is bound by the NHS Code of Practice on
Protecting Patient Confidentiality (Scottish Executive, 2003). In processing any data or personal
information we hold about you we will comply with the requirements of the Data Protection Act
1998. That means we will take all reasonable steps to ensure that your information will be
processed fairly, kept securely, protected against loss or damage and will only be disclosed (unless
required by law or legal process) on a need to know basis and in consultation with your self.
On occasion we may also need to speak with or visit your employer or place of work. This will be
undertaken with your full consent and knowledge. On these occasions no information will be given
in regards to your health condition, medication or medical condition unless in agreement with
yourself.
It is also important to be aware that under the Data Protection Act 1998, you are entitled to ask us in
writing to provide copies of certain data that we may hold about you, upon payment of appropriate
fee. We may provide the information without charge. In the first instance speak with your therapist
for further information in regards to the process of accessing these files.
Please Turn Over
47
Consent form Continued
Please note that this service is currently being piloted to ensure good practice, future development
and increasing the knowledge base in this field. Therefore certain information will be collated as
part of this pilot. This information will not be identifiable to you personally. However an important
aspect of the pilot will be finding out more about your perceptions of the service and this is
undertaken by patient satisfaction questionnaires. You may be contacted after you are discharged
from the service and asked to complete a questionnaire about your experiences of the service you
received. If you do not wish to participate in this questionnaire please tick the box below.
The content of the above has been explained to me by and I give consent for the following:
To participate in the Vocational Rehabilitation Service
Contact my employer regarding work practices
Patient’s Signature: _______________________________________
PRINT Name: ________________________________________
Date: ________________________________________
Therapist Signature: ________________________________________
PRINT Name: _______________________________
Date: ________________

48
Appendix 2
Rheumatology Occupational Therapy Department
Vocational Rehabilitation
Initial Assessment
Patient Name
Date of Assessment
Present at Assessment
Company and Line Management Information
Are you currently involved with any other services i.e. Agencies, Private Contractors or Occupational Health
Are you involved in any other healthcare services i.e. physiotherapy, podiatry etc.
Has an Occupational Therapy Initial Work Assessment been Undertaken?
Brief History of Diagnosis. Including; Date and Onset Symptoms Drug Treatment Other Treatments i.e. Splints, surgery etc.
49
Job Information
Current Job Title and overview of job. Also included grade and staffing levels.
How would you describes the role
Heavy Manual i.e. Construction Moderate Manual i.e. Nursing, Factory Work, Delivery Driver Light Sedentary i.e. Office, Driving
Hours of Work and Shift Pattern
Breaks Is the Client taking these breaks? How frequent are they?
Pattern of Work How is the day sectioned? Are there key tasks that require to be done at a certain time?
Are there targets to be met? If so what are they?
Description of Duties
Essential Duties Skills/ Training Required
Equipment/ Tools/ Machinery used
Pain Score 0-10

50
Occasional Duties Skills/ Training Required
Equipment/ Tools/ Machinery used
Pain Score 0-10
Physical Activities
Activity Constantly up to 2/3
Frequently up to 2/3
Occasionally up to 1/3
Never Equipment Used
Pain Levels Rate your pain on a score of 0-10 when undertaking these activities
Sitting
Standing
Crouching
Walking
Kneeling
Stooping
Climbing
Crawling
Balancing
Twisting
Carrying Unilateral
Carrying Bilateral
Pulling
Lifting (heaviest)
Lowering
Reaching - above shoulder
Reaching – below waist
Reaching –shoulder/waist
Manipulation R/H
Manipulation of L/H
Grip Pinch/ Fine
Grip Power / Gross
Fine Dexterity
51
Fine Detailed Focus
Specific Hearing
Other Physical Demands Required
Work Travel
How do you access your work? Bus/ car/ lift/ train other
Do you use transport within your post i.e. bus, van, car Do you have any difficulties doing so?
Do you have a Blue badge?
Other
Work Access
Access to building Ramped/ steps
Car Park Distance? Designated Space Level of difficulty
Security access Keys Number Pads Swipe Card Intercom Level of Difficulty Used
Internal Stairs Wide /Narrow Steep Treads Are they Busy used for the public Stair Rails
52
How Many times a day would you climb stairs?
Lifts Goods/ Public/ Staff Can you Use the lift? Buttons Pressed Distance from Access Distance fro place of work
Internal Navigation Distance from front entrance Canteen Car Park WC Distance Covered Distance between tasks
Work Environment
Lighting What type of lighting, any difficulties Ability to turn lighting on/off Natural Sunlight
Temperature Hot Cold Uncomfortable Within your control to increase or decrease
Noise Levels
53
Clutter/ Obstructions
Level of Cleanliness
Do you work from a car or Van Any difficulties with steering, gear stick, viewing blind spots, using clutch and accelerator
Work Station –Diagram of Workstation Prevocational Skills
Yes No Further Information
Reading
Writing
Maths
Clerical
Visual
Hearing
Drivers License
Vehicle Use
Cognitive Demands
Yes No Further Information
Short term Memory
Long term Memory
Organisational Skills
Planning Skills
Sequencing of Tasks
Reasoning
Problem Solving
Safety Awareness
Spatial Awareness

54
Temperaments
Yes No Further Information
Directing
Repetitive
Influencing
Variety
Expressing feeling
Working Alone
Stress
Specific
Deal with people
Make Judgements
Aptitude to Work
Are you enjoying your job at present?
Are you receiving support from your line management?
Do you receive support from colleagues?
Are there any other barriers to work?
Other
55
Appendix 3
Vocational Rehabilitation Pilot
Occupational Therapy
Therapy Centre
Southern General Hospital
1345 Govan Road
Glasgow G51 4TF
Telephone 0141 201 1507
What is Vocational Rehabilitation?
As part of the Occupational Therapy service we are running Vocational Rehabilitation (VR) Pilot that
aims to support people with health conditions return to work manage their condition in work. We
know from research the majority of people want to remain in work and stay at work regardless of
their health needs, but this can be difficult if you are not receiving the right advice and support. The
VR pilot offers a confidential, non judgemental and free service to support you with all your work
needs. You can be assured that you can discuss your work needs in confidence and we will never
contact your employer unless you give us your permission.
Why have I been referred?
As part of your therapy you have been referred to the VR pilot by an occupational therapist or your
consultant. The reason for your referral is that you have expressed difficulties in your workplace or
returning to work because of your condition.
The VR pilot is led by occupational therapists that are specialised in supporting people to return to
work or remain in work. We offer a range of services including;
Assessment of your needs within the workplace
Ergonomic assessment of your workstation
Workplace assessment looking at areas/ duties in work that you may find difficult
We also offer
Advice and resources regarding your rights in the workplace
Advice on managing your day, managing your health condition, developing coping strategies
Advice on managing fatigue and pain
Information on your condition and how to manage it
Should a flare up occur, advice can be provided on how best to manage this in the workplace.

56
When required we can also offer
With your permission we can communicate with your employers to support you in your workplace
Return to work programmes
Job modification programmes
Referral to other services, where appropriate
What to bring with you
Accompanying this letter you will find a sheet with questions that ask you to;
Rate your pain and fatigue levels (how tired you are) on a scale of 0-10
Record morning joint stiffness
Record sick days off work and reduced productivity levels due to your condition
Your thoughts on your future health in the workplace
This should only require 10 minutes approximately to complete
What to expect on your visit
The VR pilot is based within the occupational therapy department at the Therapy Centre at Southern
General Hospital. You will be seen within the out patients department. On your first visit a full
assessment will be carried out focusing on your work and work tasks. Following on from the
assessment the occupational therapist will devised a plan with you that will focus on your needs in
the workplace. Everyone is different and one person may require 2-3 sessions and others more. The
number of sessions required will be discussed at your first appointment.
What you can expect from VR pilot
We aim to see everyone at the time of their appointment, however very occasionally there may be
delays. We will not contact your employer unless expressly consented by you and fully discussed
with you. We will provide a full, robust and comprehensive service to meet the needs that you
identify that will try to help you return to work or remain at work.
What if I need to change my appointment?
It is important to contact us if you need to change your appointment as this allows us to offer the
appointment to someone else. If you have any further queries please do not hesitate to contact us
on 0141 201 1507.
57
Appendix 4
Outcome Measures
Vocational Rehabilitation Pilot
Occupational Therapy Department
Southern General Hospital
You are being asked to complete the following questions before your first appointment at the
Vocational Rehabilitation Department, please see accompanying leaflet entitled ‘Vocational
Rehabilitation’. The following questions allow us to find a start point of your health needs relation
to your workplace. All responses are treated with the strictest of confidence and will be held in
your medical notes and not share with anyone else without your consent.
Pain
Thinking back over the last 7 days on a scale of 0-10 indicate your pain levels with 0 being no pain
and 10 being most severe pain experienced.
Fatigue
Thinking back over the last 7 days on a scale of 1-5, please indicate your fatigue (how tired you are)
levels.
1 2 3
Not at all Fatigues Slightly fatigued Moderately Fatigued
4 5 Much Fatigued Very Fatigued
Early Morning Joint Stiffness
Thinking back over the last 7 days how long, on average, for how long did you experience early
morning joint stiffness, circle approximate time which is noted in hours.
_________________________________________________
0 ½ 1 1½ 2 or more
58
Sick Absence and Productivity
Over the last 6 months
a. How many days off have you taken due to your health condition?
__________ days
b. How many days have you worked at reduced productivity i.e. someone undertaking your duties to
help, leaving early from work, not getting completed what you have done, due to your health
condition?
__________ days
c. Do you feel now or in the near future (within the next year) that your condition will affect your
ability to stay in work? Please Circle
Yes No Do Not Know
59
Appendix 5
SF – 36 Questionnaire Name:________________________________ Date:________________
This survey asks for your views about your health. This information will help keep track of how
you feel and how well you are able to do your usual activities. Please answer all questions as best
you can.
Mark an X next to response that best describes your answer.
Q1 In general, would you say your health is:
Excellent
Very good
Good
Fair
Poor
Q2 COMPARED TO ONE WEEK AGO, how would you rate your health in general NOW?
Much better now than one week ago
Somewhat better now than one week ago
About the same as one week ago
Somewhat worse now than one week ago
Much worse now than one week ago
Q3 The following questions are about activities you might do during a typical day.
Does YOUR HEALTH NOW LIMIT YOU in these activities? If so, how much?
Q3a VIGOROUS ACTIVITIES, such as running, lifting heavy objects, participating in
strenuous sports
Yes, limited a lot
Yes, limited a little
No, not limited at all
Q3b MODERATE ACTIVITIES, such as moving a table, pushing a vacuum cleaner,
bowling, or
playing golf
Yes, limited a lot
Yes, limited a little
No, not limited at all
Q3c Lifting or carrying groceries
Yes, limited a lot
Yes, limited a little
No, not limited at all
Q3d Climbing SEVERAL flights of stairs
Yes, limited a lot
Yes, limited a little
No, not limited at all

60
Q3e Climbing ONE flight of stairs Yes, limited a lot
Yes, limited a little
No, not limited at all
Q3f Bending, kneeling, or stooping
Yes, limited a lot
Yes, limited a little
No, not limited at all
Q3g Walking MORE THAN A MILE
Yes, limited a lot
Yes, limited a little
No, not limited at all
Q3h Walking SEVERAL HUNDRED YARDS
Yes, limited a lot
Yes, limited a little
No, not limited at all
Q3i Walking ONE HUNDRED YARDS
Yes, limited a lot
Yes, limited a little No, not limited at all
Q3j Bathing or dressing yourself
Yes, limited a lot
Yes, limited a little
No, not limited at all
Q4 During the PAST WEEK, how much of the time have you had any of the following problems
with
your work or other regular daily activities AS A RESULT OF YOUR PHYSICAL HEALTH?
Q4a Cut down on the AMOUNT OF TIME you spent on work or other activities
All of the time
Most of the time
Some of the time
A little of the time
None of the time
Q4b ACCOMPLISHED LESS than you would like
All of the time
Most of the time
Some of the time
A little of the time
None of the time
61
Q4c Were limited in the KIND of work or other activities
All of the time
Most of the time
Some of the time
A little of the time
None of the time
Q4d Had DIFFICULTY performing the work or other activities (for example, it took extra
effort)
All of the time
Most of the time
Some of the time
A little of the time
None of the time
Q5 During the PAST WEEK, how much of the time have you had any of the following problems
with your work or other regular daily activities AS A RESULT OF ANY EMOTIONAL
PROBLEMS
(such as feeling depressed or anxious)?
Q5a Cut down on the AMOUNT OF TIME you spent on work or other activities
All of the time
Most of the time
Some of the time
A little of the time
None of the time
Q5b ACCOMPLISHED LESS than you would like
All of the time
Most of the time
Some of the time
A little of the time
None of the time
Q5c Did work or other activities LESS CAREFULLY THAN USUAL
All of the time
Most of the time
Some of the time
A little of the time
None of the time
Q6 During the PAST WEEK, to what extent has your physical health or emotional problems
interfered
with your normal social activities with family, friends, neighbors, or groups?
Not at all
Slightly
Moderately
Quite a bit
Extremely

62
Q7 How much BODILY pain have you had during the PAST WEEK?
None
Very mild
Mild
Moderate
Severe
Very severe
Q8 During the PAST WEEK, how much did PAIN interfere with your normal work (including both
work outside the home and housework)?
Not at all
A little bit
Moderately
Quite a bit
Extremely
Q9 These questions are about how you feel and how things have been with you DURING THE
PAST
WEEK. For each question, please give the one answer that comes closest to the way you have been feeling. How much of the time during the PAST WEEK --
Q9a Did you feel full of life?
All of the time
Most of the time
Some of the time
A little of the time
None of the time
Q9b Have you been very nervous?
All of the time
Most of the time
Some of the time
A little of the time
None of the time
Q9c Have you felt so down in the dumps that nothing could cheer you up?
All of the time
Most of the time
Some of the time
A little of the time
None of the time
Q9d Have you felt calm and peaceful?
All of the time
Most of the time
Some of the time
A little of the time
None of the time

63
Q9e Did you have a lot of energy?
All of the time
Most of the time
Some of the time
A little of the time
None of the time
Q9f Have you felt downhearted and depressed?
All of the time
Most of the time
Some of the time
A little of the time
None of the time
Q9g Did you feel worn out?
All of the time
Most of the time Some of the time
A little of the time
None of the time
Q9h Have you been happy?
All of the time
Most of the time
Some of the time
A little of the time
None of the time
Q9i Did you feel tired?
All of the time
Most of the time
Some of the time
A little of the time
None of the time
Q10 During the PAST WEEK, how much of the time has your PHYSICAL HEALTH OR EMOTIONAL
PROBLEMS interfered with your social activities (like visiting friends, relatives, etc.)?
All of the time
Most of the time
Some of the time
A little of the time
None of the time
Q11 How TRUE or FALSE is EACH of the following statements for you?
Q11a I seem to get sick a little easier than other people
Definitely true
Mostly true
Don't know
Mostly false
Definitely false

64
Q11b I am as healthy as anybody I know
Definitely true
Mostly true
Don't know
Mostly false
Definitely false
Q11c I expect my health to get worse
Definitely true Mostly true
Don't know
Mostly false Definitely false
Q11d My health is excellent
Definitely true
Mostly true
Don't know
Mostly false
Definitely false
THANK YOU FOR COMPLETING THESE QUESTIONS !
65
Appendix 6
Telephone Questionnaire
Firstly, can you tell me why you were referred to the service?
What happened when you attended?
Did the service help you? Yes/ No
Comment – If yes why/ if not why not?
What were your expectations of the service?
How could the service be improved in the future?
An aim on this service is to encourage patient to return to work or stay in work. Did the
service help you do this?

66
Appendix 7
Audit of Vocational Rehabilitation Needs on Other Sites
Occupational Therapy
Audit of Work/ Interventions
Patients Name CHI
DOB Unit No.
Initial Assessment
Date Hospital Site (please circle) GGH NVH GRI
Occupation Diagnosis
Hours Worked Date of Diagnosis
Shift Pattern Date of Discharge
On Sick Leave YES / NO
Type of work issues identified
Code Interventions Tier 1 Tick if provided
T1/01 Leaflets Issued
T1/02 DDA Advice Given
T1/03 Sign Posting
T1/04 Referral to other services
T1/05 Self management advice ie. JP
T1/06 Loan of Equipment
T1/07 Splint Provision
Other, please give details:
Would Patient have benefited from
V.R. OT Input
YES / NO
Left work due to Rheumatic
Condition? YES / NO When

67
Appendix 8
Summary Patient Sheet
Patient Summary Sheet
Outcome Measure IA DC Outcome Measures
IA DC
EuroQol
SF-36
Fatigue Scale Early Morning Joint Stiffness
Pain Scale Other:
Code Interventions Tier 1 Tick
T1/01 Leaflets Issued
T1/02 DDA Advice Given
T1/03 Sign Posting
T1/04 Referral to other Services
T1/05 Self Management Advice i.e JP, WLB, PM
T1/06 Provision of Equipment
Patients name: Primary condition: Date of initial Assessment:
DOB: Duration: Date of Discharge:
Occupation: Work Status: IA Discharge 3 Month Follow-up
Postcode: Other Services:
IA Hours DC Hours No. Sessions
Gender: M F Job Type (Coding)
Case Outcome:
Refused VR Withdrew from VR
DNA VR Completed VR

68
T1/07 Loan of Equipment
T1/07 Splint Provision
Code Intervention Tier 2 Tick
T2/08 Job Demands Analysis
T2/09 Workplace Assessment
T2/10 Ergonomics Assessment
T2/11 Work Simulation Assessment
T2/12 Liaising with Employers
T2/13 Job Modification
T2/14 Workplace Adaptation
T2/15 Return to Work programme
T2/16 Liaising with other services i.e AtW, OH
T2/17 Written Reports
T2/18 Other- please specify
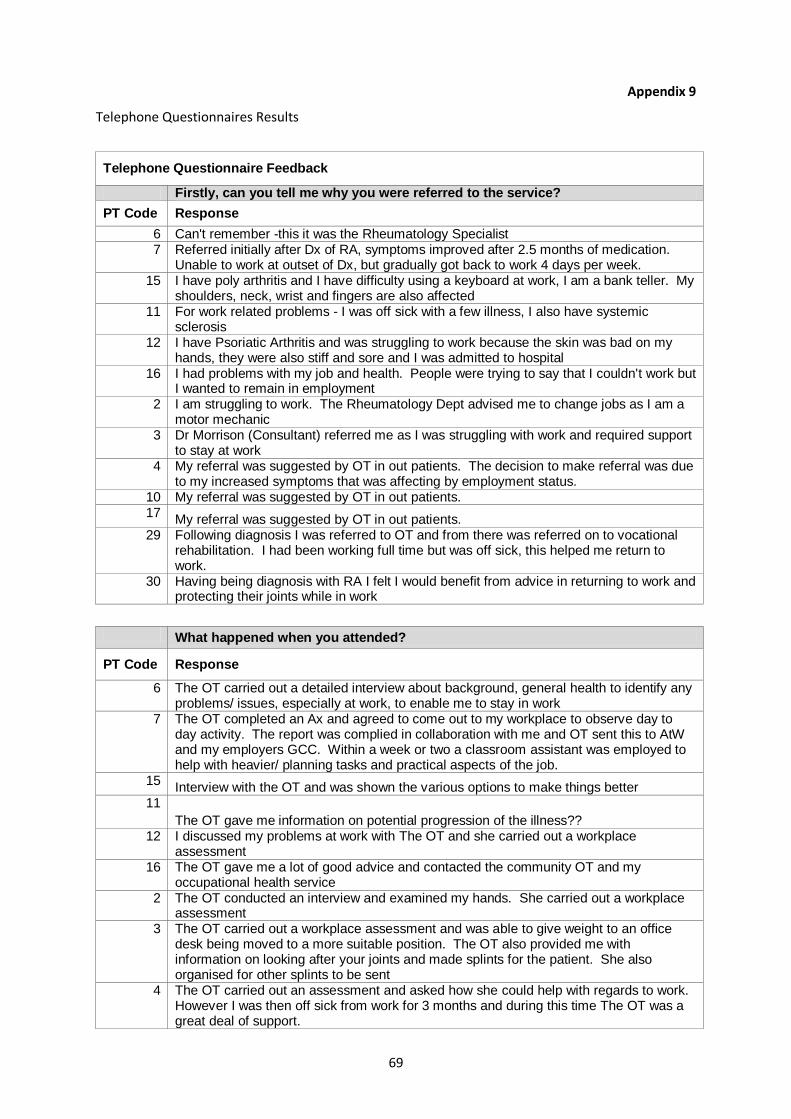
69
Appendix 9
Telephone Questionnaires Results
Telephone Questionnaire Feedback
Firstly, can you tell me why you were referred to the service?
PT Code Response
6 Can't remember -this it was the Rheumatology Specialist 7 Referred initially after Dx of RA, symptoms improved after 2.5 months of medication.
Unable to work at outset of Dx, but gradually got back to work 4 days per week. 15 I have poly arthritis and I have difficulty using a keyboard at work, I am a bank teller. My
shoulders, neck, wrist and fingers are also affected 11 For work related problems - I was off sick with a few illness, I also have systemic
sclerosis 12 I have Psoriatic Arthritis and was struggling to work because the skin was bad on my
hands, they were also stiff and sore and I was admitted to hospital 16 I had problems with my job and health. People were trying to say that I couldn't work but
I wanted to remain in employment 2 I am struggling to work. The Rheumatology Dept advised me to change jobs as I am a
motor mechanic 3 Dr Morrison (Consultant) referred me as I was struggling with work and required support
to stay at work 4 My referral was suggested by OT in out patients. The decision to make referral was due
to my increased symptoms that was affecting by employment status. 10 My referral was suggested by OT in out patients. 17
My referral was suggested by OT in out patients. 29 Following diagnosis I was referred to OT and from there was referred on to vocational
rehabilitation. I had been working full time but was off sick, this helped me return to work.
30 Having being diagnosis with RA I felt I would benefit from advice in returning to work and protecting their joints while in work
What happened when you attended?
PT Code Response
6 The OT carried out a detailed interview about background, general health to identify any problems/ issues, especially at work, to enable me to stay in work
7 The OT completed an Ax and agreed to come out to my workplace to observe day to day activity. The report was complied in collaboration with me and OT sent this to AtW and my employers GCC. Within a week or two a classroom assistant was employed to help with heavier/ planning tasks and practical aspects of the job.
15 Interview with the OT and was shown the various options to make things better
11
The OT gave me information on potential progression of the illness?? 12 I discussed my problems at work with The OT and she carried out a workplace
assessment 16 The OT gave me a lot of good advice and contacted the community OT and my
occupational health service 2 The OT conducted an interview and examined my hands. She carried out a workplace
assessment 3 The OT carried out a workplace assessment and was able to give weight to an office
desk being moved to a more suitable position. The OT also provided me with information on looking after your joints and made splints for the patient. She also organised for other splints to be sent
4 The OT carried out an assessment and asked how she could help with regards to work. However I was then off sick from work for 3 months and during this time The OT was a great deal of support.

70
10 When I attended I was able to discuss areas I was having difficulty in and receive valuable advice such as how to look after your joints at work, aids and adaptations. Information on your rights as an employee was helpful at a particularly worrying time.
17 The OT interviewed me and discussed issues relating to work and home
29 The OT met with me and my range of abilities was assessed. The OT also carried out a workplace assessment and advised on protecting the joints while at work. I also discussed what work related task I could and couldn't do through a traffic light system,
30 I felt I was able to talk about her difficulties in relation to work and was able to ask questions at a very worrying time.
Did the service help you? Y/N (Why)
PT Code Response
6 Yes, no question. The OT provided ample back up and support 7 Yes - without The OT's involvement I feel that I would have been unable to work. The
OT gave all practical information and everything happened very quickly after this initial contact. All departments in SGH appear to communicate efficiently and well, according to pt.
15 Yes 11
Yes, although it was a bit short term contact but helpful 12 Yes, definitely. Parking facilities were arranged closer to the workplace for me 16 Definitely, I would not have know about the options available to me if The OT hadn't 2 Very difficulty to quantify whether or not it has help. Because of the environment in
which I work in it is hard to change what I do 3 Yes, I felt that The OT's involvement helped my company to be more open to change.
My company previously demonstrated some resistance but OT involvement improved the situation.
4 Yes, being able to speak to someone who is knowledge not only in terms of the condition but in work aspects also. The service was helpful as it was able to offer solutions and give practical advice.
10 Yes, I don't think that I would have been able to remain in work without the service. I am now able to park nearer the entrance which has been helpful. I also received helpful information on speaking with the boss about my condition and how I am managing. Also the fact that the service will plan to contact me after the summer as my class may change and bring new challenges.
17 Yes, I don't think that I would have been able to remain in work without the service. I am now able to park nearer the entrance which has been helpful. I also received helpful information on speaking with the boss about my condition and how I am managing. Also the fact that the service will plan to contact me after the summer as my class may change and bring new challenges.
29 Yes, the service was very supporting and informative. I was perhaps too eager to return to work and received good advice from The OT on taking time to protect joints and allow medication to work.
30 yes, I felt that The OT was able to give good practical advice and inform me of my rights. However the issue has been from her employers who are yet to make any reasonable adjustment to the place of work.
What were your expectations of the service?
PT Code Response
6 No idea what to expect, thought it would be more tests 7 I was unsure what the service would provide to begin with - didn't realise that The OT
would come to the workplace 15 I thought that I got only get help at home not at work, it was a nice surprise. The extra
help was no expected 11 I was advised by other OTs about Voc Rehab pilot but was not sure what to expect
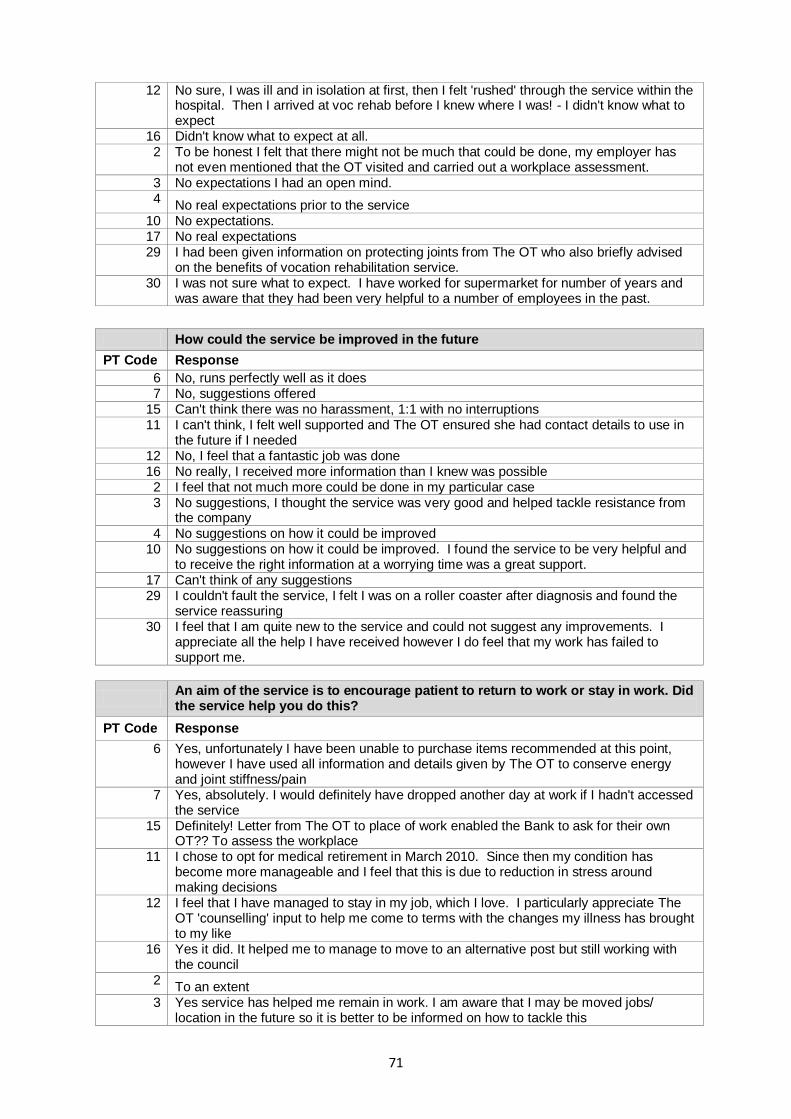
71
12 No sure, I was ill and in isolation at first, then I felt 'rushed' through the service within the hospital. Then I arrived at voc rehab before I knew where I was! - I didn't know what to expect
16 Didn't know what to expect at all. 2 To be honest I felt that there might not be much that could be done, my employer has
not even mentioned that the OT visited and carried out a workplace assessment. 3 No expectations I had an open mind. 4
No real expectations prior to the service 10 No expectations. 17 No real expectations 29 I had been given information on protecting joints from The OT who also briefly advised
on the benefits of vocation rehabilitation service. 30 I was not sure what to expect. I have worked for supermarket for number of years and
was aware that they had been very helpful to a number of employees in the past.
How could the service be improved in the future
PT Code Response
6 No, runs perfectly well as it does 7 No, suggestions offered
15 Can't think there was no harassment, 1:1 with no interruptions 11 I can't think, I felt well supported and The OT ensured she had contact details to use in
the future if I needed 12 No, I feel that a fantastic job was done 16 No really, I received more information than I knew was possible 2 I feel that not much more could be done in my particular case 3 No suggestions, I thought the service was very good and helped tackle resistance from
the company 4 No suggestions on how it could be improved
10 No suggestions on how it could be improved. I found the service to be very helpful and to receive the right information at a worrying time was a great support.
17 Can't think of any suggestions 29 I couldn't fault the service, I felt I was on a roller coaster after diagnosis and found the
service reassuring 30 I feel that I am quite new to the service and could not suggest any improvements. I
appreciate all the help I have received however I do feel that my work has failed to support me.
An aim of the service is to encourage patient to return to work or stay in work. Did the service help you do this?
PT Code Response
6 Yes, unfortunately I have been unable to purchase items recommended at this point, however I have used all information and details given by The OT to conserve energy and joint stiffness/pain
7 Yes, absolutely. I would definitely have dropped another day at work if I hadn't accessed the service
15 Definitely! Letter from The OT to place of work enabled the Bank to ask for their own OT?? To assess the workplace
11 I chose to opt for medical retirement in March 2010. Since then my condition has become more manageable and I feel that this is due to reduction in stress around making decisions
12 I feel that I have managed to stay in my job, which I love. I particularly appreciate The OT 'counselling' input to help me come to terms with the changes my illness has brought to my like
16 Yes it did. It helped me to manage to move to an alternative post but still working with the council
2 To an extent
3 Yes service has helped me remain in work. I am aware that I may be moved jobs/ location in the future so it is better to be informed on how to tackle this
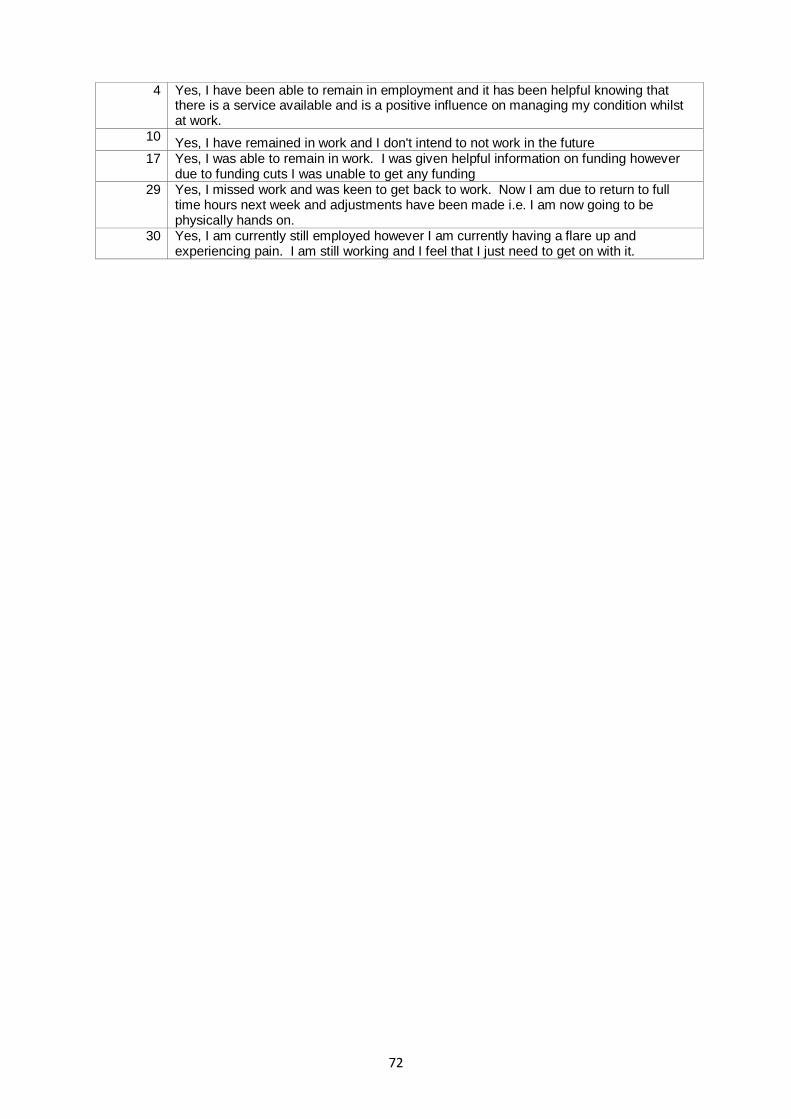
72
4 Yes, I have been able to remain in employment and it has been helpful knowing that there is a service available and is a positive influence on managing my condition whilst at work.
10 Yes, I have remained in work and I don't intend to not work in the future
17 Yes, I was able to remain in work. I was given helpful information on funding however due to funding cuts I was unable to get any funding
29 Yes, I missed work and was keen to get back to work. Now I am due to return to full time hours next week and adjustments have been made i.e. I am now going to be physically hands on.
30 Yes, I am currently still employed however I am currently having a flare up and experiencing pain. I am still working and I feel that I just need to get on with it.

73
Appendix 10
Case Study
Patient’s Name: Mrs T
Age: 51 years old
Diagnosis: Rheumatoid Arthritis, February 2009
Drug therapy: Sulphasalazine and Methotrexate
Co-codomol and Naproxen
Presenting Symptoms:
Early morning joint stiffness lasting approximately 1 hour.
Hot stiff joints of the right hand affecting range of movement, grip and hand function.
Painful ankle and heel of right foot, affecting mobility, uses a walking stick to mobiles.
Fatigue
Overall muscle pain, particularly affecting the legs and shoulders, tends to worsen throughout the day and week.
Background History
Mrs T has worked as a primary school teacher for 20 years and for the last 4 years in her current
school. Mrs T also a farmers wife and therefore undertakes a role on the farm to support her
husband, these tasks include feeding and caring for the cattle, tending to the land and assisting her
husband. Mrs T also reports that she looks after her mother who has increased care needs due to
CVA.
Patient’s OT journey
Mrs T was seen by the Rheumatology OT and an occupational therapy assessment was carried out
encompassing the areas of ADL, function, lifestyle and work activities.
Mrs T was provided with a thumb spika for the right hand to manage pain at the CMC joint.
Information on joint protection to identify coping strategies for reducing stress on joints when carrying out day to day activities.
Referral for vocational rehabilitation assessment
Vocational Rehabilitation: Occupational Therapy Input
Mrs T was seen by the OT specialising in work related issues due to health needs. An initial
assessment focusing on work and health was carried out. Outcome measures were undertaken at
assessment and discharge and are as follows;

74
Initial Assessment Discharge Assessment
Pain VAS 4 Pain VAS 2
Fatigue VAS 4 Fatigue VAS 2
Early Morning Joint
Stiffness
30 minutes Early Morning Joint
Stiffness
30 minutes
EuroQuol 90 EuroQuol 30
Days Taken off 5 Days Taken off 0
Reduced Productivity 0 Reduced Productivity 0
Health Condition
Affecting Ability to
Stay in Work
Yes Health Condition
Affecting Ability to
Stay in Work
No
Work Environment
Mrs T works in a purpose built primary school, constructed 4 years ago. The building has level access
with good clear internal pathways. The building has been constructed in a ‘T’ shape with classes and
pupil areas situated at the top end of the building and the staff entrance, administration offices and
staff canteen based in the centre of the building. There was also adequate accessible toileting at
various points about the building.
Access to the school is through a secured controlled entrance, ramped access on approaching the
building. The car park is situated a short distance from the school. The school is bright and Mrs T has
noted no concerns with eyesight or visually negotiating her way around the school.
Patients Role
Mrs T’s role within the school is referred to as ‘McCrone Teacher’. This role involves Mrs T having no
permanent class and therefore she teaches all classes from Primary 1 to 7 at various times
throughout the week. This system is to allow other teachers to have approximately 3x50 minutes
sessions, without classes, to focus on class preparation. Mrs T has 2 x 50 minutes session for her
own class preparation time; however tends to use this time to attend hospital appointments.
Work Shift Patterns
Mrs T works 9am to 3.30pm Tuesday to Friday, dropping a day due to fatigue and pain.
Works until 5.15pm on a Tuesday
15 minute break in the morning
45 minute lunch break
The working day is structured with little flexibility due to the timetable
75
A work place assessment was carried out by the OT and the following areas of difficulty were
identified;
Mobility
Mrs T reports bilateral pain in the ankles and heels which appears to affect her mobility and uses a
stick to mobilise. Mrs T identifies internal navigation of her workplace as being significantly difficult.
One of her core tasks is to oversee her pupils coming in and out of the school at the start of each
day, at first break, lunch time and end of school. During these times Mrs T will escort her class to
the changing area and support them with their shoes and jackets. Mrs T reports that she finds this
increasingly difficult to manage due to the accumulative distances that she is required to walk and
the limited time that she has to complete the task. Mrs T reports that she feels increased time
constraints to undertake these tasks, therefore quickening her speed and adding increased pressure
to her joints and therefore exacerbating pain and fatigue levels. Mrs T states that on occasion she
will receive support from colleagues to carry out the task but this is infrequent.
Carrying Objects
Mrs T reports that her classroom remains static for the majority of the time; she will also use the art
room to teach. Mrs T describes her main challenge as being able to lift the guillotine, as this is not
always in the class. She also reports difficulties with lifting objects such as paper, paints and craft
supplies due to the weight.
Pushing and Pulling
Mrs T teaches Information and Communication Technology to various classes. The laptops for pupils
are held in the computer trolley which is a large heavy metal case on wheels which has an electric
source. This trolley holds and charges all laptops for the pupils in the class. Mrs T reports that this
trolley is too heavy for her too push or pull from one area to another and relies upon older children
to assist her or another passing staff member.
Hand Function
Mrs T is right handed dominant, however reports reduced grip strength in both hands. She reports
difficulty in holding and using pens, pencils, pencil sharpener, hole punch, stapler, cups and using
scissors. Mrs T reports that she would use these items on a daily basis and presents with a
significant amount of pain when doing so. Mrs T has developed her own method of record keeping
which has reduced her need to write, however she also reports that this is only possible in the
McCrone class. Mrs T also uses a laptop and smart board for teaching and this appears to present
her with no difficulties in doing so.
Identified Issues and Recommendations
Mobility
Mrs T identifies this issue as her main challenge within this role. The accumulative walking and time
limitations to undertake the tasks exacerbate Mrs T pain and fatigue levels. Mrs T reported that to
accommodate this she would often not go to the staffroom for lunch or tea as this would make her
feel isolated at times.
76
Recommended
Assigning a classroom assistant to undertake this task allowing Mrs T to focus her time and energies
on other aspects of her work.
Outcome
Classroom assistant assigned to undertake this task.
Hand Function
Difficulty cutting paper, retrieving guillotine when moved, using hole punch and sharpening pencils
Recommendations
Guillotine to remain in art room or staff to be informed that it is to be returned when moved.
Provision of an electric pencil sharpener
Provision of and electric punch
Support to carry and cut paper – classroom assistant to undertake
Outcome
The above recommendations were met and subsequently reduce the pain experienced by Mrs T in
hands. The above recommendations were facilitating joint protection in the workplace.
Pushing and Pulling
Mrs T’s was unable to transferring the computer trolley to the classroom for ICT and this would
cause her increased stress finding someone to assist her.
Recommendations
Classroom assistant to carryout this task.
Outcome
Classroom assistant undertake this role and subsequently Mrs T reports reduced stress in finding
someone to support her.
Role within the School
Mrs T states that her role as a McCrone teacher has been beneficial to her in managing her condition
as it has allowed her to undertake minimal writing, she is not required to participate in gym sessions
with pupils and reduces her overall work load. Therefore remaining in this post for another
academic year would continue to benefit Mrs T further and allow her increased time and
opportunity for her condition to stabilise and medications to be effective.
Outcome
Mrs T works 2 days per week in the role of McCrone Teacher and 2 days a week as a Primary 6
teacher.

77
Summary
Mrs T has worked as a teacher for 20 years and enjoys her role. However since being diagnosed with
Rheumatoid Arthritis she has reduced to 4 working days and was very concerned that she would
need to reduce this further due to address her pain and fatigue levels.
Since the implementation of the above recommendations Mrs T reports that she is no longer
concerned about reducing her hours further, she has more time and energy to undertake activities
out with work and her stress levels of managing health in the workplace has significantly reduced,
improving her overall sense of wellbeing.





























