Embed Size (px)
Citation preview

Journal of Plastic, Reconstructive & Aesthetic Surgery (2010) 63, 1223e1226
CASE REPORT
Deep superior epigastric artery perforator‘propeller’ flap for abdominal wall reconstruction: Acase report
Kyong-Je Woo, Jai-Kyong Pyon*, So-Young Lim, Goo-Hyun Mun, Sa-Ik Bang,Kap-Sung Oh
Department of Plastic Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, 50 Ilwon-dong,Gangnam-gu, Seoul, 135-710, Korea
Received 30 November 2009; accepted 1 December 2009
KEYWORDSPerforator pedicledpropeller flap;Superior epigastric;Upper abdomen
* Corresponding author. Tel.: þ82 20036.
E-mail address: pspriest.pyon@sam
1748-6815/$-seefrontmatterª2009Britdoi:10.1016/j.bjps.2009.12.004
Summary As the concept of ‘free style perforator’ flap and the ‘propeller’ flap is widelyaccepted, any region of the body can be used as a possible donor site for a perforator flap.A ‘propeller’ flap is a local flap that is rotated to different extents (up to 180�) about a reliableperforator to cover adjacent defects. Rectus abdominis perforators (epigastric artery perfora-tors) are the main perforators in the abdominal region from the deep inferior epigastric arteryor the deep superior epigastric artery. Traditionally, deep inferior epigastric artery perforatorshave been often used in the abdominal region because they provide a dominant blood supply toabdominal skin. In the described case, a large abdominal wall defect (20.5� 19 cm) caused bytumour resection was covered successfully using a superior epigastric artery perforator‘propeller’ flap.ª 2009 British Association of Plastic, Reconstructive and Aesthetic Surgeons. Published byElsevier Ltd. All rights reserved.
Background
The perforator pedicled ‘propeller flap’ is a type of a localflap that is rotated to various extents about a reliable
3410 2235; fax: þ82 2 3410
sung.com (J.-K. Pyon).
ishAssociationofPlastic,Reconstruc
dominant perforator to cover adjacent defects. The flapdoesnot include muscles and the need for perforator dissection isminimal, which minimises donor-site morbidities andreduces operation times. ‘Propeller’ flaps have often beenused for extremity reconstruction and scar contracturerelease.1 In the described case, we used the ‘propeller’ flapconcept to reconstruct a large abdominal wall defect.
Deep inferior epigastric artery perforators (DIEPs) arethe main perforators in the abdominal region, especially in
tiveandAestheticSurgeons.PublishedbyElsevierLtd.All rightsreserved.

Figure 2 20.5� 19 cm sized abdominal defect remainedafter wide local excision. A deep superior epigastric arteryperforator ‘propeller’ flap, measuring 20� 10 cm, wasdesigned such that the long axis of flap lay in the transversedirection.
1224 K.-J. Woo et al.
the area below the umbilicus. Over decades, DIEP flapshave proven to be reliable and useful option for either freeflap or pedicled local flap reconstruction. However, supe-rior epigastric artery perforator flaps were introducedcomparatively recently and are not used as frequently asDIEP flaps. The first case report on a superior epigastricperforator flap was published in 2005 by Hallock, and sincethen a small number of cases have been reported.2e5
However, all of these cases involved the reconstruction ofsternal defects and the ‘propeller’ flap was not used.
The reconstruction of a large defect in the supra-umbilical abdomen is challenging. The vertical rectusabdominis myocutaneous (VRAM) flap is one option, but ithas shortcomings, because the use of rectus muscle cancause donor-site morbidities, such as hernia and motorweakness, and the flap has an indirect blood supply. Thelatissimuss dorsi myocutaneous flap is another option, but italso involves muscle sacrifice and more time to change thepatient’s position. In this report, a large abdominal defectwas successfully covered with a deep superior epigastricartery perforator ‘propeller’ flap and donor-site morbiditywas minimal.
Clinical case
A 40-year-old man with a dermatofibrosarcoma protuber-ance on his left upper abdomen underwent wide excisionincluding skin, subcutaneous fat and deep fascia. A 5-cmsafety margin was obtained in all directions, which lefta 20.5� 19-cm-sized defect (Figures 1 and 2).
A deep superior epigastric artery perforator ‘propellerflap’ was harvested using the ‘free style perforator flap’concept.6 One dominant skin perforator over the rightupper abdomen in the area below the xiphysternum wasfound by computed tomography (CT) angiography andhand-held Doppler (Figure 2). A ‘propeller’ flap of20� 10 cm, based on the expected perforator, was
Figure 1 (left) 40-year-old man with a dermatofibrosarcoma protdeep superior epigastric artery by CT angiography indicated a pateperforator was predicted. The white arrow indicates the deep sup
designed such that its long axis lay in the transversedirection (Figure 2).
Exploratory skin incision and careful suprafascialdissection under loop magnification were performed fromthe medial side of the flap, until a dominant perforatoremerging from the rectus abdominis was visualised. Theperforator was freed from connective tissue to gain therequired mobility and rotational arc. No intramuscular
uberance measuring 10.5� 9 cm (center). An evaluation of thent deep superior epigastric artery (right), and thus, a reliableerior epigastric artery perforator.
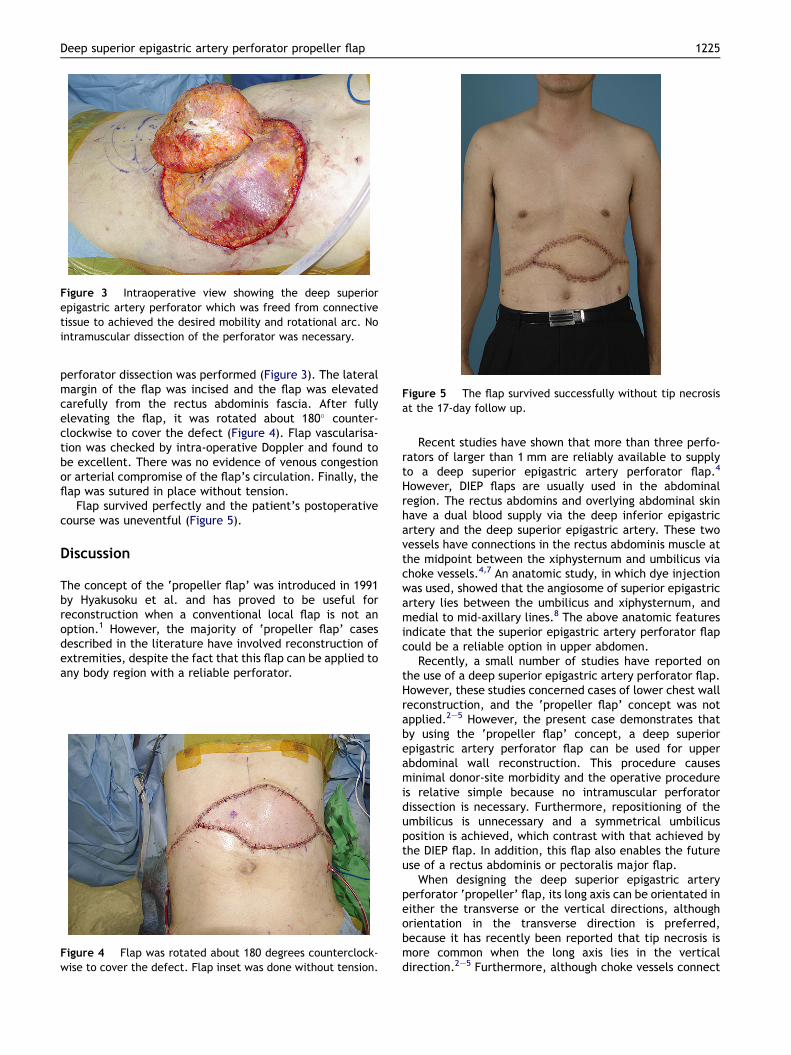
Figure 3 Intraoperative view showing the deep superiorepigastric artery perforator which was freed from connectivetissue to achieved the desired mobility and rotational arc. Nointramuscular dissection of the perforator was necessary.
Figure 5 The flap survived successfully without tip necrosisat the 17-day follow up.
Deep superior epigastric artery perforator propeller flap 1225
perforator dissection was performed (Figure 3). The lateralmargin of the flap was incised and the flap was elevatedcarefully from the rectus abdominis fascia. After fullyelevating the flap, it was rotated about 180� counter-clockwise to cover the defect (Figure 4). Flap vascularisa-tion was checked by intra-operative Doppler and found tobe excellent. There was no evidence of venous congestionor arterial compromise of the flap’s circulation. Finally, theflap was sutured in place without tension.
Flap survived perfectly and the patient’s postoperativecourse was uneventful (Figure 5).
Discussion
The concept of the ‘propeller flap’ was introduced in 1991by Hyakusoku et al. and has proved to be useful forreconstruction when a conventional local flap is not anoption.1 However, the majority of ‘propeller flap’ casesdescribed in the literature have involved reconstruction ofextremities, despite the fact that this flap can be applied toany body region with a reliable perforator.
Figure 4 Flap was rotated about 180 degrees counterclock-wise to cover the defect. Flap inset was done without tension.
Recent studies have shown that more than three perfo-rators of larger than 1 mm are reliably available to supplyto a deep superior epigastric artery perforator flap.4
However, DIEP flaps are usually used in the abdominalregion. The rectus abdomins and overlying abdominal skinhave a dual blood supply via the deep inferior epigastricartery and the deep superior epigastric artery. These twovessels have connections in the rectus abdominis muscle atthe midpoint between the xiphysternum and umbilicus viachoke vessels.4,7 An anatomic study, in which dye injectionwas used, showed that the angiosome of superior epigastricartery lies between the umbilicus and xiphysternum, andmedial to mid-axillary lines.8 The above anatomic featuresindicate that the superior epigastric artery perforator flapcould be a reliable option in upper abdomen.
Recently, a small number of studies have reported onthe use of a deep superior epigastric artery perforator flap.However, these studies concerned cases of lower chest wallreconstruction, and the ‘propeller flap’ concept was notapplied.2e5 However, the present case demonstrates thatby using the ‘propeller flap’ concept, a deep superiorepigastric artery perforator flap can be used for upperabdominal wall reconstruction. This procedure causesminimal donor-site morbidity and the operative procedureis relative simple because no intramuscular perforatordissection is necessary. Furthermore, repositioning of theumbilicus is unnecessary and a symmetrical umbilicusposition is achieved, which contrast with that achieved bythe DIEP flap. In addition, this flap also enables the futureuse of a rectus abdominis or pectoralis major flap.
When designing the deep superior epigastric arteryperforator ‘propeller’ flap, its long axis can be orientated ineither the transverse or the vertical directions, althoughorientation in the transverse direction is preferred,because it has recently been reported that tip necrosis ismore common when the long axis lies in the verticaldirection.2e5 Furthermore, although choke vessels connect

1226 K.-J. Woo et al.
the superior epigastric artery and the deep inferiorepigastric artery, the skin below the umbilicus is suppliedprimarily by the deep inferior epigastric artery.8 Preoper-ative evaluation of the superior epigastric artery perfora-tors could be done for the flap design. The deep superiorepigastric artery perforator is reliable, but its position is notas constant as those of DIEPs,4 which is why a preoperativeevaluation of perforators by audible hand-held Doppler orCT angiography is essential prior to designing the flap.
In our case, a large abdominal defect was reconstructedwith no tip necrosis. By combining the ‘propeller’ flapconcept with the ‘perforator’ flap, the deep superiorepigastric artery perforator ‘propeller’ flap offers a goodalternative means of abdominal wall reconstruction, espe-cially above the umbilical region.
Acknowledgements
Disclosure: None of the authors has any financial interest inany products and devices mentioned in this article.
References
1. Hyakusoku H, Yamamoto T, Fumiiri M. The propeller flapmethod. Br J Plast Surg 1991;44:53e4.
2. Hallock GG. The superior epigastric(RECTUS ABDOMINIS) muscleperforator flap. Ann Plast Surg 2005;55:430e2.
3. Uemura T. Superior epigastric artery perforator flap: prelimi-nary report. Plast Reconstr Surg 2007;120:1ee5e.
4. Mah E, Rozen WM, Ashton MW, et al. Deep superior epigastricartery perforators: anatomical study and clinical application insternal reconstruction. Plast Reconstr Surg 2009;123:1719e23.
5. Hamdi M, Van Landuyt K, Ulens S, et al. Clinical applications ofthe superior epigastric artery perforator (SEAP) flap: anatomicalstudies and preoperative perforator mapping with multidetectorCT. J Plast Reconstr Aesthet Surg 2009;62:1127e34.
6. Wei FC, Mardini S. Free-style free flaps. Plast Reconstr Surg2004;114:910e6.
7. Daegu Son, Byungju Park, Jinhan Kim, et al. Cadaver dissectionand dynamic CT for vascular anatomy of rectus abdominismuscle. J Korean Soc Plast Reconstr Surg 2008;35:663e8.
8. Boyd JB, Taylor GI, Corlett R. The vascular territories of thesuperior epigastric and the deep inferior epigastric systems.Plast Reconstr Surg 1984;73:1e16.







![Deep Inferior Epigastric Perforator Flap (DIEP) Post …...Printed on 6/4/2020 at 4:55 PM from SUP Page 1 of 29 Deep Inferior Epigastric Perforator Flap (DIEP) Post-Op [1706] General](https://img.dokumen.tips/doc/110x75/5f593ba906ef9d19e75cb6db/deep-inferior-epigastric-perforator-flap-diep-post-printed-on-642020-at.jpg)










![The keystone-design perforator-based flap for leg defects ... · reconstruction.[2] A modification is proposed, which combines the philosophies of perforator‑based flaps and the](https://img.dokumen.tips/doc/110x75/5f03de807e708231d40b2adb/the-keystone-design-perforator-based-flap-for-leg-defects-reconstruction2.jpg)










