Embed Size (px)
Citation preview

Vaccine 24 (2006) 5609–5614
Decreasing invasive pneumococcal disease in the elderly:A state-level analysis
A. Marshall McBean a,∗, Kyoungrae Jung a, Paul L. Hebert b
a Division of Health Services Research and Policy, University of Minnesota School of Public Health, MMC 97 A369 Mayo Memorial Building,420 Delaware St., S.E., Minneapolis, MN 55455, United States
b Department of Health Policy, Mount Sinai School of Medicine, New York, NY, United States
Received 18 November 2005; received in revised form 21 February 2006; accepted 17 April 2006Available online 6 May 2006
Abstract
Evidence has accumulated supporting the relationship between the use of 7-valent pneumococcal conjugate vaccine (PCV7) in childrenand a decline in invasive pneumococcal disease (IPD) in the elderly. We conducted a state-level analysis of vaccination coverage rates amongchildren 19–35 months of age and IPD hospitalization rates among elderly Medicare beneficiaries. Simple correlations were suggestive of anap©
K
1
ccIccccbtoIrmoa
0d
egative relationship. Multivariate analysis using a state fixed-effect model which helped control for the time invariant factors at the state levellso indicated a negative relationship, and it was statistically significant, p = 0.035. The relationship between the use of 23-valent pneumococcalolysaccharide vaccine (PPV23) and IPD hospitalizations was not statistically significant using either method.
2006 Elsevier Ltd. All rights reserved.
eywords: Invasive pneumococcal disease; Elderly; Pneumonia vaccine
. Introduction
In February 2000, 7-valent pneumococcal conjugate vac-ine (PCV7) was licensed for use among infants and younghildren, and in October 2000, the Advisory Committee onmmunization Practice (ACIP) recommended its use in allhildren ≤23 months of age, as well as among high riskhildren 24–59 months of age with certain conditions andhronic diseases for the prevention of invasive pneumococ-al disease (IPD) [1]. Subsequently, substantial declines haveeen reported in the rate of IPD in the elderly U.S. popula-ion [2–7]. Most information has come from the seven areasf the Active Bacterial Core Surveillance (ABCs)/Emergingnfections Program Network [2–6]. Initially, Whitney et al.eported an 18% decrease in isolates of Streptococcus pneu-oniae associated with IPD among persons 65 years of ager older, in 2001, compared with the 2 years prior to the avail-bility of the vaccine, 1998–1999 [2]. More recent informa-
∗ Corresponding author. Tel.: +1 612 625 6175.E-mail address: [email protected] (A.M. McBean).
tion from the ABCs group has shown further decreases in IPDrates in the elderly in 2002 and 2003, and they reported thatthe decreases were confined to the seven serotypes includedin the PCV7 vaccine [3–6]. No changes in IPD rates werefound for the 17 serotypes included only in the 23-valentpneumococcal polysaccharide vaccine (PPV23). In anotherstudy, we used Medicare administrative data, and comparednational IPD hospitalization rates in the elderly during the4 years preceding the availability of PCV7 with the first 3years of PCV7 use [7]. We found that IPD hospitalizationrates decreased by 22.6%, 30.2% and 40.6%, compared withthe 4-year baseline period. These ABCs area and nationalfindings are a remarkable and exciting example of herd, orindirect, immunity [4–8].
The purpose of this study is to augment this information bystudying the temporal relationship of PCV7 use and IPD ratesin the elderly at the state level. While PCV7 immunizationrates have rapidly increased since its introduction in 2000,each state shows different levels of coverage over time. Usingthis geographic variation, this study examines the relationshipof changes in state-specific IPD hospitalization rates during
264-410X/$ – see front matter © 2006 Elsevier Ltd. All rights reserved.oi:10.1016/j.vaccine.2006.04.055

5610 A.M. McBean et al. / Vaccine 24 (2006) 5609–5614
the influenza years 1998–1999, 2001–2002 and 2002–2003with the state-specific PCV7 coverage rates for these years.
2. Methods
2.1. Data and data sources
We used the National Immunization Survey (NIS) [9] andBehavioral Risk Factor Surveillance System (BRFSS) [10]of the National Center for Disease Control and Prevention(CDC) to obtain information about state-specific immuniza-tion rates for PCV7, PPV23 and influenza vaccine. The NISis an on-going survey of vaccination coverage used to moni-tor childhood immunizations. The website presents tables ofestimated coverage for recommended pediatric vaccines bystate and age for 12-month periods beginning with the firstand the third quarter of each year. Even though PCV7 vaccinewas licensed in February 2000, the first information on thepercent of fully immunized children 19–35 months of age;that is, those who received three or more doses of PCV7, isthat beginning with the third quarter of 2001. Because thisstudy focuses on influenza years, CDC reporting week 27 of200X through reporting week 26 of 200X + 1, we used theNIS estimates of PCV7 coverage for the 12 months beginningwith the third quarter of 2001 and 2002.
itwa
tvcyit1f2f“so
afiirpaabtI
(pneumococcus) together with either 038.9 (unspecified sep-ticemia) or 790.7 (bacteremia); Pneumococcal meningitis,ICD-9-CM code 320.1 (Pneumococcal meningitis) or 320.8(meningitis due to other specified bacteria) together witheither 041.2 or 038.2; or pneumococcal disease in anothernormally sterile site, ICD-9-CM code 041.2 together withany of the following codes: 711.0–711.09 (pyogenic arthri-tis), 727.0, 727.00 (synovitis and tenosynovitis), 510–510.9(empyema), 511–511.1, 511.9 (pleurisy), 513–513.1 (abscessof lung and mediastinum) were counted as IPD. If a recordhad diagnosis codes for a hospitalization that put it in morethan one group, it was counted only once. All hospitalizationswithin 30 days after discharge of a prior hospitalization forthe same diagnosis were excluded.
The denominator files contain Medicare enrollment anddemographic information, including state of residence. Asis the standard practice in analyses of Medicare data, ben-eficiaries who were enrolled in the Medicare managed careplans, between 12% and 14% during the study period, wereexcluded from the study because hospitalization informationis not consistently submitted by the plans about them. Alsoexcluded were those with end-stage renal disease.
2.2. Statistical analysis
taTe
Y
Yacts(to
ctofIttayavst
As we explained in our earlier publication [7], we usednfluenza years rather than calendar years because we wantedo minimize any effect of variations in the time period inhich the influenza season occurred, and we wanted to be
ble to compare our results from this study with those results.The BRFSS is a state-based continuous random-digit dial
elephone survey of persons 18 years of age and older. Inter-iewees are asked if they have ever received a PPV23 vac-ination or if they received influenza vaccine in the pastear. Because the BRFSS did not collect information regard-ng PPV23 and influenza immunization in 1998, we usedhe state-specific estimates of coverage in the elderly for999, and we averaged the estimates for 2001 and 2002, andor 2002 and 2003 to obtain values for the 2001–2002 and002–2003 influenza years, respectively. This may seem oddor influenza vaccine, but with the wording of the question,in the past 12 months”, rather than “the last influenza sea-on”, and the fact that the survey is conducted all 12 monthsf the year, this appears to be the best solution.
We used Medicare administrative data files: namely, thennual Medicare Provider and Analysis Review (MedPAR)les and Medicare Denominator files covering the same
nfluenza year periods to determine the IPD hospitalizationates by state. The MedPAR files contain one record per hos-italization and include information such as the admissionnd discharge dates, the principal diagnosis and up to ninedditional secondary diagnoses, the state of residence of theeneficiary, and each beneficiary’s unique identifier. Hospi-alizations with the diagnosis of Pneumococcal septicemia,CD-9-CM code 038.2 (Pneumococcal septicemia) or 041.2
The unit of analysis in this study was a state. Correla-ions between the changes in the rates of PCV7 coveragend changes in IPD hospitalization rates were explored first.hen, the following multiple regression model was used toxamine the effect of PCV7 vaccination rates on IPD rates.
st = β0 + β1(PCV7)st + β2(PPV23)st + β3(FLU)st
+ βs(S) + βt(T ) + εst
st is the IPD rate in the state s in the year t. PCV7, PPV23nd FLU are state-specific vaccination rates for PCV7 amonghildren, and PPV23 and influenza vaccination rates amonghe elderly. S and T represent indicator variables for eachtate S, and year T, respectively. The coefficient on PCV7β1) measures the estimated effect of our principal interest,he impact of PCV7 vaccination rates on the IPD rates basedn the change in each of these variables.
We used this state fixed-effect model to address potentialonfounding effects. In a state fixed-effect model, by takinghe difference in variable values of a state from the state’swn mean values, the estimates are obtained controllingor changes in the other variables over years for each state.n such a way, the model controls for all state-specificime invariant characteristics including unobserved factorshat may be related to both IPD rates and PCV7 rates. Welso included time fixed effects (T) to adjust for potentialear-specific effects on IPD hospitalization rates that are notssociated with immunization rates (e.g., low respiratoryiral activity in a specific year, either influenza or respiratoryyncytial virus [11]). PPV23 and FLU values were includedo account for potential associations between those vacci-

A.M. McBean et al. / Vaccine 24 (2006) 5609–5614 5611
Table 1State-specific invasive pneumococcal disease (IPD) hospitalization rates among the elderly, PCV7 immunization coverage among children, and PPV23 andinfluenza vaccine coverage among the elderly, 1998–1999 (or 1999), 2001–2002 and 2002–2003
State IPD hospitalizations/100,000elderly
PCV7 coverage/100 children19–35 months of age
PPV23 coverage/100elderly
Influenza vaccinecoverage/100 elderly
1998–99 2001–02 2002–03 2001–02 2002–03 1999 2001–02 2002–03 1999 2001–02 2002–03
Alabama 30.9 18.6 17.5 12.7 54.9 53.9 59.4 60.0 64.6 65.4 67.5Alaska 22.7 23.6 14.3 11.3 61.2 43.8 62.6 59.7 59.8 66.2 68.0Arizona 41.3 25.7 18.5 12.4 48.9 53.4 66.8 66.8 71.3 65.8 69.3Arkansas 36.1 29.5 30.8 10.7 36.7 50.2 58.9 60.3 67.3 66.1 70.0California 45.0 26.6 22.3 21.2 60.1 57.0 63.2 66.0 72.2 70.2 72.0Colorado 41.6 28.0 28.4 15.1 52.5 62.7 68.4 68.6 74.8 75.4 73.8Connecticut 37.1 25.7 27.1 24.3 73.5 49.0 63.9 59.6 64.8 70.3 72.9Delaware 23.2 21.9 17.2 24.6 58.3 66.5 66.6 65.9 67.7 69.6 70.8District of Columbia 41.2 22.2 18.5 17.4 55.6 35.3 48.5 49.1 55.8 57.1 60.9Florida 22.8 14.7 13.7 19.5 50.4 53.5 57.7 60.9 63.3 56.0 61.5Georgia 40.8 26.4 22.6 22.9 59.9 49.7 57.6 58.9 57.0 60.8 63.2Hawaii 13.0 13.6 8.9 34.4 71.0 55.8 61.6 64.4 74.1 76.5 72.8Idaho 31.1 16.9 29.5 10.7 54.1 55.2 58.9 62.4 69.0 65.1 67.7Illinois 41.2 32.6 27.2 16.4 55.5 47.4 56.7 56.7 67.5 61.7 62.2Indiana 46.7 29.0 25.0 19.7 58.2 51.6 60.7 61.4 66.2 66.0 66.2Iowa 41.2 32.9 22.0 22.1 62.5 61.2 66.1 68.8 69.6 73.2 75.5Kansas 35.0 29.7 30.0 20.8 58.2 55.1 62.5 61.2 67.0 68.6 69.7Kentucky 36.2 29.0 26.7 25.4 62.7 52.0 55.9 58.1 68.4 63.3 67.4Louisiana 48.2 27.8 23.5 11.6 44.8 40.4 52.9 60.3 60.3 56.7 62.8Maine 28.5 24.6 25.0 15.3 62.0 57.3 65.9 65.8 73.7 72.7 74.3Maryland 36.3 25.9 24.1 23.8 65.6 54.1 62.9 62.7 62.6 66.6 67.2Massachusetts 37.4 27.5 24.7 35.8 85.2 56.8 63.5 66.4 69.4 71.6 73.8Michigan 40.1 25.9 22.7 14.3 46.4 57.7 59.8 62.9 70.0 64.1 67.6Minnesota 35.1 27.3 21.9 23.5 67.9 51.9 66.7 71.7 64.0 73.4 78.5Mississippi 24.7 17.5 19.1 6.5 45.4 50.4 57.3 60.4 62.8 62.4 66.0Missouri 43.4 32.8 27.3 31.0 63.7 52.8 58.4 61.0 68.4 68.1 69.3Montana 29.1 27.8 29.8 23.0 56.8 61.2 67.6 68.2 72.9 70.4 70.2Nebraska 26.1 14.3 18.1 23.5 57.4 54.8 61.3 63.1 69.2 69.2 70.9Nevada 27.4 12.4 17.8 7.1 25.2 61.7 65.7 64.1 62.2 61.8 60.2New Hampshire 36.1 31.6 23.3 20.9 67.0 60.4 63.3 66.6 65.1 70.9 73.1New Jersey 49.4 29.8 22.7 35.4 68.5 55.1 61.0 62.8 65.3 66.8 68.2New Mexico 40.0 31.2 17.1 11.9 48.0 53.2 62.7 63.3 68.8 68.3 69.5New York 33.9 23.7 22.9 24.9 66.2 50.0 59.2 62.1 63.8 63.6 66.4North Carolina 35.5 21.3 17.1 16.0 68.8 58.5 64.4 64.8 64.2 67.1 68.5North Dakota 10.2 34.2 21.7 11.5 50.8 55.0 68.4 71.9 67.2 72.0 73.5Ohio 40.5 27.9 20.0 21.0 56.6 55.0 61.5 64.2 68.8 65.0 67.3Oklahoma 45.3 36.2 32.0 14.4 38.8 53.7 65.8 67.1 71.8 72.7 74.3Oregon 38.6 26.6 24.5 18.3 60.1 56.2 68.0 68.4 65.2 69.9 69.3Pennsylvania 49.2 31.3 27.0 31.5 75.9 52.2 61.5 64.8 63.1 67.2 69.9Rhode Island 46.4 35.9 24.7 37.1 83.4 56.9 67.3 68.5 75.8 73.2 75.0South Carolina 25.7 20.4 19.8 23.7 62.5 56.1 61.4 64.0 69.9 67.8 69.4South Dakota 26.7 23.1 23.1 7.4 23.1 50.4 58.0 60.2 73.6 74.2 76.1Tennessee 38.0 21.7 22.0 19.3 62.3 54.3 58.4 61.1 65.5 68.6 70.4Texas 29.9 26.6 20.5 11.6 53.6 55.9 57.5 59.5 69.8 61.4 64.4Utah 35.2 25.9 27.1 12.0 54.5 61.3 66.2 65.6 75.1 69.9 73.0Vermont 34.3 24.5 17.5 18.6 64.6 56.5 66.8 66.2 73.4 72.6 73.9Virginia 35.4 24.1 19.9 31.3 71.2 55.2 60.5 63.0 65.7 65.3 67.5Washington 38.6 27.8 21.7 8.9 51.3 55.8 64.9 65.8 68.9 68.8 69.3West Virginia 40.5 27.1 25.9 13.4 50.1 54.3 61.3 62.5 62.9 63.8 67.5Wisconsin 33.4 25.9 20.8 21.8 65.5 53.7 68.1 68.7 64.9 72.2 73.1Wyoming 19.0 12.6 10.5 12.8 46.3 61.5 68.3 69.3 73.8 70.1 71.6
U.S. mean 37.2 25.8 22.3 20.1 59.1 n.a. 60.9 n.a. n.a. 65.7 n.a.Value for median state 36.1 26.4 22.6 19.3 58.2 54.9 62.5 63.3 67.4 68.1 69.4Minimum state value 10.2 12.4 8.9 6.5 23.1 35.3 48.5 49.1 55.8 56.0 60.2Maximum state value 49.4 36.2 32.0 37.1 85.2 66.5 68.4 71.9 75.8 76.5 78.525% (Quartile 1) 29.5 22.7 18.8 12.6 51.1 52.1 59.0 60.9 64.4 65.1 67.475% (Quartile 3) 41.0 29.0 25.4 23.6 65.1 56.9 66.0 66.3 70.0 70.6 72.9
n.a., not available.

5612 A.M. McBean et al. / Vaccine 24 (2006) 5609–5614
nation rates and IPD rates. Stata statistical software (version9) was used for this analysis.
3. Results
State-specific and summary information for the vari-ables used are presented in Table 1. In 1998–1999, thenational rate of IPD hospitalizations in the elderly was37.2/100,000. It decreased to 25.8/100,000 in 2001–2002,and to 22.3/100,000 in 2002–2003; 30.7% and 40.2% lower,respectively, than in 1998–1999, p < 0.0001 for both com-parisons. The rates for the median states (36.1/100,000 in1998–1999; 26.4/100,000 in 2001–2002 and 22.6/100,000in 2002–2003) were very similar to the national means.
From a starting point of zero, the PCV7 coverage ratesin the median state for three or more doses of PCV7through 35 months of age reached 20.1/100 in 2001–2002and 59.1/100 in 2002–2003. There was substantial variationbetween states in both years with a difference of 30.6/100and 62.1/100 between the lowest and the highest states andinter-quartile ranges of 11.0/100 and 14.0/100 in 2001–2002and 2002–2003, respectively.
PPV23 coverage rates in the elderly also increased duringthe study period. The value for the median state increasedfrom 54.9/100 in 1999 to 63.3/100 in 2002–2003. The inter-qact
srtrr
chiN(
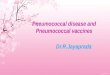
Fig. 1. Correlation between the change from 1998–1999 to 2002–2003 instate-specific PCV7 immunization rates/100 among children 19–35 monthsof age and the change in invasive pneumococcal disease (IPD) hospitalizationrates/100,000 among the elderly: (r = −0.223, p = 0.115).
The multiple regression analysis results (Table 2) indi-cate that the vaccination of children with PCV7 for childrenhad a significant negative effect on the IPD hospitalizationrates among the elderly (p = 0.035). A negative relationshipbetween the change in PPV23 and IPD hospitalization rateswas also found, but the association was not statistically sig-nificant (p = 0.313).
4. Discussion
Since the introduction of PCV7 for use in children, thesix studies described in Section 1 have provided increasinglystrong evidence for the indirect effect of PCV7 in prevent-ing IPD in the elderly. However, they largely have reportedinformation from one source, the ABCs project and haveall been similar in design. This study provides additionalevidence to this body of knowledge. We took advantage ofthe variation in PCV7 coverage rates between states to testthe impact of vaccine on IPD hospitalization rates in theelderly. Simple correlation between changes in the two mea-sures was only suggestive of a negative relationship betweenthem. However, the use of a regression model, specifically astate fixed-effect model, which helps us control for any time-invariant confounding effects allowed us to demonstrate a
TR
Natiosurveperio
Coef
P −0.15P −0.24F 0.22Y −4.25Y −1.28
S 23, 23-
uartile range was smaller than for PCV7, 4.8/100, 7.0/100nd 5.4/100 for the three study years. Influenza vaccinationoverage increased little during the study period, 2.0/100 forhe median state.
Simple correlations of the percentage point changes in thetate-specific PCV7 coverage rate and IPD hospitalizationates from 1998–1999 to 2001–2002 and from 1998–1999o 2002–2003 were negative, but they were not significant:= −0.113 (p = 0.426), and r = −0.223 (p = 0.115), Fig. 1,espectively.
For PPV23 the simple correlation of the percentage pointhange in the state-specific vaccination coverage and IPDospitalization rates from 1998–1999 to 2001–2002 was pos-tive, and from 1998–1999 to 2002–2003, it was negative.either was significant: r = 0.087 (p = 0.543), and r = −0.152
p = 0.287), respectively.
able 2esults of multiple regression modela
Full year
Coefficient S.E. p-value
CV7 rate among children −0.1535 0.0716 0.035PV23 rate among for the elderly −0.2208 0.2178 0.313LU rate among the elderly 0.2954 0.2272 0.197ear 1 −4.8841 2.4814 0.052ear 2 −2.4292 4.7407 0.610
.E., standard error; PCV7, 7-valent pneumococcal conjugate vaccine; PPVa Coefficients for each state are omitted.
nal influenza virusillance reportingd—CDC weeks 20–40
Period when national influenza virussurveillance not reported—CDCweeks 21–39
ficient S.E. p-value Coefficient S.E. p-value
27 0.0580 0.010 −0.0498 0.02104 0.02063 0.1763 0.166 −0.0846 0.05195 0.10774 0.1839 0.219 – – –42 2.0089 0.037 1.2828 0.9859 0.19655 3.8380 0.738 2.6582 1.5574 0.091
valent pneumococcal polysaccharide vaccine; FLU, influenza vaccination.

A.M. McBean et al. / Vaccine 24 (2006) 5609–5614 5613
significant impact of PCV7 utilization in IPD hospitaliza-tions in the elderly. The model was enhanced by the additionof information regarding state-specific PPV23 and influenzavaccine coverage among the elderly. Thus, adjusting for thepotential effect of these time-invariant factors and vaccines,the effect of PCV7 was clearly demonstrated.
We failed to find a significant negative effect of PPV23 onIPD. Possible explanations may include the small changes inthe PPV23 coverage rates by state during the study period.On the other hand, not all studies of the impact of PPV23on IPD have demonstrated vaccine efficacy. Domestic U.S.studies that support that position are largely case-control orretrospective cohort studies [12–15]. However, as recentlypresented by Melegaro and Edmunds [16], meta-analysis ofPPV23 using only randomized control trial information failedto show vaccine efficacy against IPD; that is, all confidenceintervals included zero.
We conducted additional separate analyses of the weeksduring which influenza virus isolates are reported for theUnited States (CDC weeks 40 of 200X through week 20 of200X + 1), called respiratory virus surveillance period, andCDC weeks 21–39, the non-respiratory virus surveillanceperiod. The results were similar to those found for the entireinfluenza year, and the regression model results are shown inTable 2.
We also examined how the model predicted decreaseit11cipftpwt0t61o
b2baoItvwtwT
estimates, which has been included as a weakness by theABCs authors in other studies of IPD [2,3].
In spite of these strengths, we were limited by the numberof years for which data were available. Further, the mea-sures of PCV7 coverage were only of those children whohad received three or more doses. We do not know what per-centage had received fewer doses, and there is evidence fromclinical trials that one dose may be effective in preventingdisease in 94% of children [17]. Because of issues of vaccineavailability through 2004 [4,18,19], there may have been asignificant number of children who were not fully immu-nized by the requirements of the immunization schedule, butwho were no longer carriers of the vaccine subtypes. As werecently pointed out, a potential major weakness of a studyof IPD using Medicare administrative data is the lack of cul-ture confirmation of the diagnosis of pneumococcal diseasein each person, and the passive nature of the case reportingcompared with the active surveillances of the ABCs. How-ever, the rates of IPD we reported in our earlier publicationwere still approximately 60% of the rates reported by theABCs in the period prior to the availability of PCV7 [7].Finally, this study’s methodology was different than that usedin other reports. This was an ecologic study which is subjectto aggregation bias [20,21]. While the state fixed-effect modeldoes not correct for this potential bias, nor for time-varyingcomponents that we could not measure in our database, itdw
A
c
R
n IPD hospitalizations due to PCV7 use compared withhe overall crude decrease of 40.1% we reported between998–1999 and 2002–2003 (Table 2: 37.2/100,000 in998–1999 and 22.3/100,000 in 2002–2003). The regressionoefficient of −0.1535 implies that for each percentage pointncrease in PCV7 use there would be a decrease in IPD hos-italizations of 0.1535/100,000, having controlled for otheractors in the model, including the time-invariant ones. Thus,he point-estimate and the 95% confidence interval of theredicted decrease in IPD hospitalizations in 2002–2003hen PCV7 coverage reached 59.1% for the nation using
he regression coefficient of −0.1535 and standard error of.0716 in Table 2 are 9.10/100,000, and from 0.61/100,000o 17.54/100,000, respectively. Thus, the point estimate is0.7% of the decrease we observed, and the range is from.6% to 47.2%, which includes the 40.1% decrease webserved.
The strengths of this study are the use of nation-wide dataased on the fee-for-service Medicare population of between2 and 25 million per year, which was available for the periodsefore and after the introduction of PCV7, and of a modelingpproach that allowed us to include information about the usef PPV23 and influenza vaccines in the elderly population.n addition, the secondary analysis in which we restrictedhe study to the non-respiratory virus period when influenzairus and RSV do not circulate, or circulate only minimally,hich eliminated their potential confounding effects found
he same results. Further, the Medicare administrative dataere the source of both the numerator and the denominator.hus, we avoided having to use Census Bureau population
oes account for those unavailable, or omitted, variables thatere state-specific and time-invariant.
cknowledgement
Financial support was provided by the Centers for Medi-are and Medicaid Services contract CMS 500-01-0043.
eferences
[1] Centers for Disease Control and Prevention. Preventing pneumococ-cal disease among infants and young children: recommendations ofthe Advisory Committee on Immunization Practices (ACIP). MMWR2000:49. #RR-9.
[2] Whitney CG, Farley MM, Hadler J, Harrison LH, Bennett NM, Lyn-field R, et al. Decline in invasive pneumococcal disease after theintroduction of protein–polysaccharide conjugate vaccine. N Eng JMed 2003;348:1737–46.
[3] Lexau C, Lynfield R, Pilisivili T, Facklam R, Farley MM, HarrisonLH, et al. Changes in the epidemiology of invasive pneumococcaldisease among older adults: evidence for indirect effects of pedi-atric pneumococcal conjugate vaccine presented at ICEID 2004. In:International Conference on Emerging Infectious Diseases. 2004.
[4] Flannery B, Schrag S, Bennett NM, Lynfield R, Harrison LH,Reingold A, et al. Impact of childhood vaccination on racial dis-parities in invasive Streptococcus pneumoniae infections. JAMA2004;291:2197–203.
[5] C.D.C. Direct and indirect effects of routine vaccination of chil-dren with 7-valent pneumococcal conjugate vaccine on incidence ofinvasive pneumococcal disease—United States, 1998–2003. MMWR2005;54:893–7.

5614 A.M. McBean et al. / Vaccine 24 (2006) 5609–5614
[6] Lexau CA, Lynfield R, Danila R, Pilishvili T, Facklam R, FarleyMM, et al. Changing epidemiology of invasive pneumococcal diseaseamong older adults in an era of pediatric pneumococcal conjugatevaccine. JAMA 2005;294:1043–51.
[7] McBean AM, Park Y-T, Caldwell D. Declining invasive pneumococ-cal disease in the U.S. Elderly. Vaccine 2005;23:5641–5.
[8] O’Brien KL, Dagan R. The potential indirect effect of conjugatepneumococcal vaccines. Vaccine 2003;21:1815–25.
[9] CDC. National Immunization Survey available at http://www.cdc.gov/nis/; last accessed February 20, 2006.
[10] CDC. Behavioral Risk Factor Surveillance System available at http://apps.nccd.cdc.gov/brfss/; last accessed November 7, 2005.
[11] Talbot TR, Poehling KA, Hartert TV, Arbogast PG, Halasa NB,Edwards KM, et al. Seasonality of invasive pneumococcal disease:temporal relationship to documented influenza and respiratory syn-cytial viral circulation. Am J Med 2005;118:285–91.
[12] Shapiro ED, Clemens JD. A controlled evaluation of the protectiveefficacy of pneumococcal vaccine for patients at high risk for seriouspneumococcal infections. Ann Int Med 1984;101:325–30.
[13] Shapiro ED, Berg AT, Austrian R, Schroeder D, Parcells V, MargolisA, et al. The protective efficacy of pneumococcal polysaccharidevaccine. N Engl J Med 1991;325:1453–60.
[14] Farr BM, Johnson BL, Cobb DK, Fisch MJ, Germanson TP, AdalKA, et al. Preventing pneumococcal bacterimia in patients at risk:results of a matched case-control study. Arch Int Med 1995;155:2336–40.
[15] Jackson LA, Neuzil KM, Yu O, Benson P, Barlow WE, Adams AL, etal. Vaccine safely datalink. Effectiveness of pneumococcal polysac-charide vaccine in older adults. N Engl J Med 2003;348:1747–55.
[16] Melegaro A, Edmunds J. The 23-valent pneumococcal polysaccha-ride vaccine. Part I. Efficacy of PPV in the elderly: a comparison ofmeta-analyses. Eur J Epidemiol 2004;19:353–63.
[17] Black S, Shinefield H, Fireman B, Lewis E, Ray P, Hansen JR, etal. Efficacy, safely and immunogenicity of heptavalent pneumococcalconjugate vaccine in children. Pediatr Infect Dis J 2000;19:187–95.
[18] Centers for Disease Control and Prevention. Limited supply of pneu-mococcal conjugate vaccine. MMWR 2003;52:1234.
[19] Centers for Disease Control and Prevention. Updated recommenda-tion on the use of pneumococcal conjugate vaccine: suspension ofrecommendation for third and fourth dose. MMWR 2003;53:177–78.
[20] Last JM. A dictionary of epidemiology. 3rd ed. New York, NY:Oxford University Press; 1995.
[21] Szklo M, Nieto FJ. Epidemiology: beyond the basics. Gaithersburg,MD: Aspen Publishers, Inc.; 2000.