Embed Size (px)
Citation preview

Vaccine 23 (2005) 5641–5645
Declining invasive pneumococcal disease in the U.S. elderly
A. Marshall McBean∗, Young-Taek Park, Debra Caldwell, Xinhua YuDivision of Health Services Research and Policy, University of Minnesota School of Public Health, MMC 97,
D369 Mayo Memorial Building, 420 Delaware Street S.E., Minneapolis, MN 55455, USA
Received 4 February 2005; received in revised form 19 May 2005; accepted 25 May 2005Available online 27 July 2005
Abstract
In 2000, pneumococcal conjugate vaccine (PCV7) was recommended for young children. By 2002–2003, 48.6% had been fully immunized.Using Medicare administrative, we found that the rates of invasive pneumococcal disease (IPD) hospitalizations in the elderly in the 2000–2001,2001–2002 and 2002–2003, were 22.6, 30.2, and 40.6% lower, respectively, than during the baseline period, 1996–1997 through 1999–2000(range 35.1/100,000 to 38.3/100,000). Pneumococcal polysaccharide vaccine (PPV23) has been recommended for the elderly, since 1989.PPV23 vaccination rates in the elderly increased by 25.2% during the baseline period but by <5% during the period PCV7 has been available.Thus, during the period that PCV7 vaccine has been used in children, rates of IPD in the elderly have declined appreciably more comparedt©
K
1
ebd(mwiPmm[nrtot
eport
996ide
caretely
edi-d topital-sted.onsr theeu-mo-
0d
o the immediately prior period when PPV23 was the only vaccine available.2005 Elsevier Ltd. All rights reserved.
eywords: Pneumococcal conjugate vaccine; Invasive pneumococcal disease; Elderly
. Introduction
Rates of invasive pneumococcal disease (IPD) amonglderly Americans, those 65 years of age or older (65+), haveeen estimated to be 61.5/100,000, third in rank behind chil-ren 1–2 years of age (205.4/100,000) and <12 months of age162.7/100,000)[1]. In February 2000, a seven-valent pneu-ococcal polysaccharide–protein conjugate vaccine (PCV7)as licensed for use among infants and young children, and
n October 2000, the Advisory Committee on Immunizationractice (ACIP) recommended its use in all children≤23onths of age, as well as among high risk children 24–59onths of age with certain conditions and chronic diseases
2]. In spite of shortages of PCV7[3], Whitney et al.[4], Flan-ery et al.[5], and Lexau et al.[6] reported significantly lowerates of IPD in 2001 and 2002 compared with the 2 years prioro the availability of the vaccine, 1998–1999, among personsf all ages residing in the seven communities participating in
he Active Bacterial Core Surveillance (ABCs) project. Most
∗
relevant to this paper were the decreases of 24–34% ramong different age strata of the elderly in 2002[5,6].
We used Medicare administrative data for the years 1through 2003, to determine whether or not a nation-wimpact of PCV7 could be seen among the elderly Medifee-for-service population, which included approxima84–90% of elderly Americans during those years.
2. Methods
2.1. Data source and case identification
The annual 1996 through 2003 short-stay 100% Mcare Analysis and Review (MedPAR) files were useidentify cases. These files contain one record per hosization. Each record may have up to 10 diagnoses liHospitalizations with IPD were identified among pers65+ years of age residing in one of the 50 states oDistrict of Columbia if the record had a diagnosis of pnmococccal septicemia—ICD-9-CM code 038.2 (pneu
Corresponding author. Tel.: +1 612 625 6175; fax: +1 612 378 4866.E-mail address: [email protected] (A.M. McBean). coccal septicemia), or 041.2 (pneumococcus infection in
264-410X/$ – see front matter © 2005 Elsevier Ltd. All rights reserved.oi:10.1016/j.vaccine.2005.05.043

5642 A.M. McBean et al. / Vaccine 23 (2005) 5641–5645
conditions classified elsewhere) together with either 038.9(unspecified septicemia) or 790.7 (bacteremia); pneumo-coccal meningitis—ICD-9-CM code 320.1 (pneumococcalmeningitis) or 320.8 (meningitis due to other specified bac-teria) together with either 041.2 or 038.2; or pneumococcaldisease in another normally sterile site—ICD-9-CM code041.2 together with any of the following codes: 711.0–711.09(pyogenic arthritis), 727.0, 727.00 (synovitis and tenosyn-ovitis), 510–510.9 (empyema), 511–511.1, 511.9 (pleurisy),513–513.1 (abscess of lung and mediastinum).
Patient demographic information and the dates of hospitaladmission and discharge were obtained from the MedPARfiles, also. Because information about hospitalizations forMedicare beneficiaries who are in managed care are irreg-ularly submitted by managed care plans, we followed theconvention of researchers using Medicare administrative dataof excluding these beneficiaries from the analysis (10–16%of the Medicare elderly population during the study period),as well as those with end-stage renal disease. In order toavoid double counting cases, we excluded hospitalizationsthat occurred within 30 days of a prior hospitalization withthe same diagnosis. The annual 5% Medicare denominatorfiles for the same years were used to create the denominatorsused in the analysis.
2.2. Analysis
cal-c 997t 1997t 2001,2 s. Weu endary ffecto sono greatm zas ly halo ear-l aa en-d 00 (av s tos atesi a in1 2004s nt icanA g itsu n-di vac-c att cinei fort seen
in Section3, below, even in this year of abbreviated vaccineavailability, the IPD hospitalization rates among the elderlydecreased by 22.6% compared with the baseline period. Also,as mentioned earlier, vaccine shortages have occurred at var-ious times since licensure. Throughout most of 2001, vaccinefor the public sector, which includes the VFC program, wason back order[3], and in 2003 and 2004 vaccine supplieswere limited, also[10,11]. Thus, it is difficult to find a periodof full vaccine availability in any of the 12 months period wedesignated, 2000–2001, 2001–2002, or 2002–2003.
The 5% Medicare fee-for-service population was usedas the standard for age adjustment. We compared the aver-age annual rates of IPD hospitalizations in the baselineperiod with the annual rates in the vaccine availability periodusing thez-test. Analyses were conducted using SAS 8.2and Excel. Multivariate negative binomial regression mod-els were employed to examine the trends in the various IPDrates, using IPD rate as the dependent variable (SAS 9.1, ProcGenmod). This model accounts for possible overdispersionin the IPD incident rates. In our assessment of the trends, wecompared the trends between Blacks and Whites, betweenthe three age groups and between sexes.
3. Results
tionsw riodw nt 998,3 0,000w ,000,2 22.6,3 spec-t inep
pi-t 00,t ,
F (IPD)a 03 byt
Crude and age-adjusted rates of hospitalization wereulated for the July through June periods for 1996–1hrough 2002–2003. We considered the 4 years 1996–hrough 1999–2000 as the baseline period, and 2000–001–2002 and 2002–2003, as vaccine availability yearsed the July through June period rather than the calear for two reasons: first, we wanted to minimize any ef variations in the time period in which the influenza seaccurred. For example, 1999 was a year in which theajority of influenza activity for the 1998–1999 influen
eason was reported (the usual case), as well as roughf the activity for the 1999–2000 influenza season (an
ier season than usual)[7]. Thus, the impact of influenzctivity on IPD, if it occurred, would be greater in calar year 1999 (a baseline year) than calendar year 20accine availability year), potentially biasing the resulthow an effect of PCV7 reducing IPD hospitalization rn the elderly in 2000. The early occurrence of influenz999–2000 was not an isolated event, and the 2003–eason was another, more recent example[8]; secondly, evehough PCV7 was licensed in February 2000, the Amercademy of Pediatrics policy statement recommendinse was not issued until August[9], and the ACIP recommeation of its use was not published until October[2], which
s when the vaccine became widely available due to theines for children (VFC) program[5]. One could argue thhis would reduce the measured impact of the PCV7 vacn 2000–2001 because it was not “available” to all childrenhe entire 12 months of that period. However, as will be
f
The average annual age-adjusted rate of hospitalizaith IPD among the elderly in the 4-year baseline peas 36.8/100,000 (Table 1, Fig. 1). The difference betwee
he highest year during the baseline period 1997–18.3/100,000, and the lowest year 1999–2000, 35.1/10as 9.1%. In the next 3 years, the rates were 28.5/1005.7/100,000, and 21.8/100,000, respectively. These are0.2 and 40.6% lower than the baseline average, re
ively (p < 0.0001 for all comparisons with the baseleriod).
Elderly Blacks were 25.2% more likely to be hosalized with IPD in the pre-vaccine period, 45.5/100,0han elderly Whites, 36.3/100,000 (Fig. 1). By 2002–2003
ig. 1. Rates of hospitalization for invasive pneumococcal diseasemong elderly Medicare beneficiaries, 1996–1997 through 2002–20
otal and race.

A.M. McBean et al. / Vaccine 23 (2005) 5641–5645 5643
Table 1Invasive pneumococcal disease hospitalizations among elderly Medicare beneficiaries, 1996–1997 through 2002–2003
Baseline period PCV7a availability years
1996–1997 through1999–2000
2000–2001 2001–2002 2002–2003
Averageannualnumber
Averageannualrateb
Number Rate Change frombaselineperiodc
Number Rate Change frombaselineperiod
Number Rate Change frombaselineperiod
Age group65–74 3073 23.1 2326 18.0 −22.2% 2221 16.7 −28.0% 1947 14.3 −38.3%75–84 3737 40.0 2934 30.7 −23.1% 2718 27.6 −30.8% 2387 23.7 −40.7%85+ 2641 78.9 2129 61.3 −22.3% 1920 53.8 −31.8% 1645 45.0 −43.0%
GenderMale 3851 37.7 3077 29.4 −22.0% 2877 26.4 −29.8% 2567 22.8 −39.4%Female 5599 36.3 4312 27.9 −23.2% 3982 25.1 −30.7% 3412 21.1 −41.8%
RaceWhite 8239 36.3 6420 28.0 −22.9% 6012 25.5 −29.8% 5230 21.7 −40.2%Black 877 45.5 670 34.1 −25.0% 589 29.0 −36.2% 509 24.4 −46.3%Other 335 31.0 299 28.2 −9.0% 258 22.7 −26.6% 240 19.9 −35.7%
Total 9450 36.8 7389 28.5 −22.6% 6859 25.7 −30.2% 5979 21.8 −40.6%
Rates for gender and race groups and total were age-adjusted to the December 2000 Medicare fee-for-service population.a Seven-valent pneumococcal polysaccharide–protein conjugate vaccine.b All rates are per 100,000.c All changes in the rates between baseline period and each PCV7 vaccine availability year are significant at the levelp < 0.0001.
the third year of vaccine availability difference was cut inhalf to 12.4%, 24.4/100,000 in Blacks and 21.7/100,000 inWhites.
The multivariate analysis confirmed the statistical signifi-cance of the downward trend in the rate of IPD (p < 0.001) forthe entire population, as well as for each age group, genderand race stratum show inTable 1andFigs. 1 and 2, p < 0.001for each stratum. The downward trend among Blacks wasgreater than among Whites,p = 0.011. The decline in theyoungest age group was not statistically significantly differ-ent than the decline in either of the two older age groups(p = 0.4 for 65–74 versus 74–85, andp = 0.1 for 65–74 ver-sus 85+). The difference between the two oldest age groupswas not statistically significant, either,p = 0.36. There was nodifference in the decline between men and women,p = 0.66.
F IPD),1
4. Discussion
The remarkable decline in IPD rates among the elderlycould be due to the introduction and use of PCV7 amongchildren, the use of PPV23 among the elderly, or unrelated,unexplained secular trends. The most recent information fromthe ABCs group indicates that in 2002 the decline in cases ofIPD among the elderly was confined to the seven serotypesincluded in PCV7[5,6]. No changes in IPD rates among theelderly were reported for the 16 serotypes included only in the23-valent pneumococcal polysaccharide vaccine (PPV23).Thus, Flannery et al. suggested that the changes in diseaserates in the elderly were due to decreased transmission ofPCV7 serotypes from children to the elderly[5].
National information on PCV7 coverage among childrenis not available until the third quarter of 2001. For the 12months beginning with that quarter, which corresponds tothe 2001–2002 influenza year, the National ImmunizationSurvey reported the rate of children 19–35 months of agewho had received 3+ doses of PCV7 to be 20.1/100[12]. In2002–2003, it increased to 48.6/100[12]. This rapid, tempo-rally related increase in PCV7 use reinforces Flannery et al.’snotion that the decrease in the IPD hospitalization rate amongthe elderly is due to the immunization of children with PCV7mediated through a herd immunity effect of the decreasedpresence and circulation of the PCV7 serotypes.
V7o une2 alen-d e it.B t, we
ig. 2. Rates of hospitalization for invasive pneumococcal disease (996–1997 through 2002–2003, by age group.
Measuring the exact timing of the initial impact of PCn the elderly is difficult. We chose July 2000 through J001 and the authors representing the ABCs used car year 2001 as the first year in which to measurecause PCV7 could have had a more immediate effec

5644 A.M. McBean et al. / Vaccine 23 (2005) 5641–5645
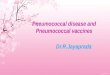
Fig. 3. Rates per 100 of self-reported PPV23 vaccination coverageamong U.S. elderly from the National Health Interview Survey (NHIS)(1997–2003), and the Medicare fee-for-service Consumer Assessment ofHealth Plans Survey (MFFS-CAHPS) (2000–2002).
also examined the differences in the IPD rate in the year1999–2000 compared with the prior year, 1998–1999, alone,as well as with the pooled rates for the three prior years,1996–1997 through 1998–1999 (data not shown). Each com-parison showed similar decreases of 5.6 and 5.9%, respec-tively, p < 0.0001. While the decrease in IPD in 1999–2000is much smaller than the 22.6% we found in 2000–2001, it ispossible that PCV7 was already exerting an influence in thecirculation ofStreptococcus pneumoniae in the communitybeginning soon after licensure in February 2000. The manu-facturer reports PCV7 revenues of $109,300,000 in the firstand second quarters of 2000[13]. The Harvard Focus of 24March 2000 reported a list price of $58 per dose[14], whichmeans that 1,884,483 doses of vaccine would have been avail-able during that time. Although no child would have receivedall of the recommended doses, many would have had a chanceto receive one, two, and possibly three doses, and the originalefficacy trials of PCV7 showed a 94% efficacy in children inpreventing IPD in those who had received one or more doses[15].
An alternative explanation to herd immunity that shouldbe considered is the direct effect of PCV23 use among theelderly. PCV23 has been available to Medicare beneficiariessince 1983 without payment of a co-payment or deductible,and it has been recommended for the elderly by the ACIPsince 1989[16]. These factors, as well as Medicare reim-b gin-n s toi e useo 3v sureda tion’s( 97t icaidS on-s PS)f ,i . By
2000, the year in which the PCV7 became available, vacci-nation coverage was 53.1/100, an increase of 25.2%. Theseyears correspond to our IPD baseline years, 1996–1997through 1999–2000, during which the age-adjusted rates ofIPD hospitalization were relatively stable: 36.5/100,000 in1996–1997; 38.3/100,000 in 1997–1998; 37.2/100,000 in1998–1999 and 35.1/100,000 in 1999–2000. The decreasebetween 1996–1997, and 1999–2000 was 3.8%. During thenext 3 years PPV23 coverage increased only 4.7%, fromthe previously mentioned 53.1/100 in 2000 to 55.6/100 in2003, yet the rate of IPD hospitalizations decreased by 40.6%(Table 1). According to the much larger MFFS-CAHPS sur-vey, PPV23 vaccination coverage in this population was verystable, also: 64/100, 65/100 and 66/100, in 2000 through2002, respectively. Based on these data PPV23 coverageincreased by only 3.1% during this period while the rate ofIPD hospitalizations decreased by 30.2% from the baselineperiod to 2001–2002 (Table 1).
Our observation of a greater decrease in the IPD hos-pitalization rate among Blacks than Whites in the vaccineavailability period is similar to the report by Flannery et al.[5], which found a greater decrease in IPD isolates amongyoung and elderly Blacks. Regarding children, they com-mented, “Surprisingly, declines in incidence were greateramong black children than among white children, despitesimilar vaccination coverage”. The observation in the elderlyi withP d farb 9,2 eil-l /100,5 prox-i 100,3 o theB mongW lacksi ase inI ulds thee
um-b able( canb n int ablef ct ab thisp ataw ator.T latione y theAd nualp ns int tionr
ursement for influenza vaccine and its administration being in 1993, and the implementation of many strategie
mprove coverage with both vaccines have increased thf PPV23[17–22]. We present inFig. 3, self-reported PPV2accine coverage among the elderly which has been meannually by the Centers for Disease Control and PrevenCDC) National Health Interview Survey (NHIS) for 19hrough 2003, and the Centers for Medicare and Medervices (CMS) sponsored Medicare fee-for-service Cumer Assessment of Health Plans Survey (MFFS-CAHor 2000 through 2002[18–20,23]. According to the NHISn 1997, 42.4/100 elderly were vaccinated with PPV23
s very interesting because the rates of vaccinationPV23 among elderly Blacks have consistently laggeehind Whites[5,17,20–22,24]. For example, in 1997, 199001 and 2002, the CDC’s behavioral risk factor surv
ance system (BRFSS) reported rates in Whites (47.26.8/100, 63.6/100, and 64.8/100, respectively) were ap
mately 50% greater than in Blacks (30.0/100, 36.4/9.4/100, and 44.5/100, respectively). Also, according tRFSS, between 1999 and 2002, the vaccination rate ahites increased by 8.0% points, and the rate among B
ncreased by 7.8% points. The reason for greater decrePD hospitalizations among Blacks is not clear, but woupport the idea that PCV7 is exerting its herd effect onntire community.
The strengths of this study includes the very large ner of elderly fee-for-service Medicare beneficiaries availbetween 22 and 25 million per year) and results thate generalized to all of this highly vulnerable populatio
he U.S. Also, Medicare administrative data were availor a sufficient number of years to allow us to construaseline period, which was similar to other studies ofhenomenon[4–6]. Further, the Medicare administrative dere the source of both the numerator and the denominhus, we avoided having to use census bureau popustimates, which has been included as a weakness bBCs authors in other studies of IPD[4,6,25]. Finally, asescribed earlier, by using July through June as our aneriod we have reduced the possible impact of variatio
he timing of the influenza season on IPD hospitalizaates.

A.M. McBean et al. / Vaccine 23 (2005) 5641–5645 5645
The major weakness of the study is the lack of culture con-firmation of the diagnosis of pneumococcal disease in eachperson. Another potential weakness is that our cumulativeannual baseline IPD hospitalization rate of 36.8/100,000 islower than that reported by Robinson et al., for 1995 through1998, 59.7/100,000 and Whitney et al. for 1998 and 1999,61.5/100,000, for IPD isolates in the elderly living in theABCs areas[1,25]. Robinson et al.[24] reported that 96% ofall isolates among the elderly were from hospitalized patients,the focus of our study. Thus, our estimates of IPD hospital-ization are about 60% of the rates they reported. The lowersensitivity of the administrative data is likely largely due tothe failure to correctly code cases of septicemia, meningitis,etc., that are caused byS. pneumoniae. Patients may be codedas having pneumococcal pneumonia, only, without coding forbacteremia or septicemia, or they may be incorrectly codedas streptococcal disease, or as “unspecified”, if the laboratoryresults are not closely examined. To our knowledge no studyof the accuracy (sensitivity, specificity, etc.) of the coding ofIPD diagnoses in administrative data has been carried out.Also contributing to our lower rates is the fact that the ABCsare conducting active surveillance, which will find morecases than passive systems such as ones using administrativedata.
In spite of these limitations, most of our findings regard-ing the impact of the PCV7 are very consistent with thoser es wef 5–74y 32%a to thed spec-t t thei
R
3
ococ-ns of
WR
enda-ccinetices.
n-r theng J
H,dis-
[6] Lexau C, Lynfield R, Pilisivili T, Facklam R, Farley MM, HarrisonLH, et al. Changes in the epidemiology of invasive pneumococcaldisease among older adults: evidence for indirect effects of pedi-atric pneumococcal conjugate vaccine presented at ICEID 2004. In:Proceedings of the International Conference on Emerging InfectiousDiseases. 2004.
[7] Brammer TL, Murray EL, Fukuda K, Hall HH, Kimlov A, Cox NJ.Surveillance for influenza—United States, 1997–1998, 1998–1999,and 1999–2000 seasons. MMWR 2002;51(SS07):1–10.
[8] Centers for Disease Control and Prevention, 2003–2004 U.S.Influenza season summary. http://www.cdc.gov/flu/weekly/weeklyarchives2003-2004/03-04summary.htm; last accessed 4January 2005.
[9] American Academy of Pediatrics. Policy statement: recommen-dations for the prevention of pneumococcal infections, includingthe use of pneumococcal conjugate vaccine (Prevnar), pneumococ-cal polysaccharide vaccine, and antibiotic prophylaxis. Pediatrics2000;106:362–6.
[10] Centers for Disease Control and Prevention. Limited supply of pneu-mococcal conjugate vaccine. MMWR 2003;52:1234.
[11] Centers for Disease Control and Prevention. Updated recommenda-tion on the use of pneumococcal conjugate vaccine: suspension ofrecommendation for third and fourth dose. MMWR 2003;53:177–78.
[12] Centers for Disease Control and Prevention. National ImmunizationSurvey available athttp://www.cdc.gov/nis/; last accessed 10 January2005;4:889–896.
[13] Doug Petkus, Vice President of Public Affairs, Wyeth, Madison, NJ,17 May 2005, Personal communication.
[14] http://focus.hms.harvard.edu/2000/Mar242000/ambulatorycare.html;last accessed 17 May 2005.
[15] Black S, Shinefield H, Fireman B, Lewis E, Ray P, Hansen JR, etoccal95.
[ ns ofccal
[ ccalArch
[ ealthis/
[ ealthc/
[ actor
[ umo-nited
[ umo-nited
[ mp-ne-
[ iza-nt of
[ ofs,
eported from the ABCs areas. For example, the decreasound in 2001–2002 by age group: 28% among those 6ears of age, 31% among those 75–84 years of age, andmong those 85 years of age and older, are very similarecreases found by the ABCs group: 31, 34 and 24%, re
ively [6]. Thus, we believe, our results accurately reflecmpact of the vaccine in the U.S. elderly population.
eferences
[1] Active Bacterial Core Surveillance website. Available athttp://www.cdc.gov/ncidod/dbmd/abcs/survreports/spneu99.pdf; last accessed 2July 2004.
[2] Centers for Disease Control and Prevention. Preventing pneumcal disease among infants and young children: recommendatiothe advisory committee on immunization practices (ACIP). MM2000;49:#RR-9.
[3] Centers for Disease Control and Prevention. Update recommtion on the use of pneumococcal conjugate in a setting of vashortage resolved—advisory committee on immunization pracMMWR 2001;50:1040–2.
[4] Whitney CG, Farley MM, Hadler J, Harrison LH, Bennett NM, Lyfield R, et al. Decline in invasive pneumococcal disease afteintroduction of protein-polysaccharide conjugate vaccine. N EMed 2003;348:1737–46.
[5] Flannery B, Schrag S, Bennett NM, Lynfield R, Harrison LReingold A, et al. Impact of childhood vaccination on racialparities in invasiveStreptococcus pneumoniae infections. JAMA2004;291:2197–203.
al. Efficacy, safety and immunogenicity of heptavalent pneumocconjugate vaccine in children. Pediatr Infect Dis 2000;19:187–
16] Centers for Disease Control and Prevention. Recommendatiothe Immunization Practices Advisory Committee: pneumocopolysaccharide vaccine. MMWR 1989;38(64–68):73–6.
17] McBean AM, Babish JD, Prihoda R. The utilization of pneumocopolysaccharide vaccine among elderly Medicare beneficiaries.Intern Med 1991;151:2009–16.
18] Centers for Disease Control and Prevention. National HInterview Survey available athttp://www.cdc.gov/nchs/data/nhearlyrelease/20040605.pdf; last accessed 19 October 2004.
19] Centers for Disease Control and Prevention. National HInterview Survey available athttp://www.cdc.gov/nchs/data/mishus2003excerpt.pdf; last accessed 19 October 2004.
20] Centers for Disease Control and Prevention. Behavioral Risk FSurveillance System available athttp://apps.nccd.cdc.gov/brfss/; lastaccessed 24 July 2004.
21] Centers for Disease Control and Prevention. Influenza and pnecoccal vaccination levels among persons aged >65 years—UStates, 2001. MMWR 2002;51:1019–24.
22] Centers for Disease Control and Prevention. Influenza and pnecoccal vaccination levels among persons aged >65 years—UStates, 2002. MMWR 2003;52:987–92.
23] Bonito AJ, Lenfestey NF, Eicheldinger C, Iannacchione VG, Cabell L. Disparities in immunizations among elderly Medicare beficiaries, 2000–2002. Am J Prev Med 2004;27:153–60.
24] Health Care Financing Administration. 1995 Influenza immuntions paid for by Medicare: state and county rates. DepartmeHealth and Human Services, October 1996.
25] Robinson K, Baughman W, Royhrock G, et al. Epidemiologyinvasive Streptococcus pneumoniae infection in the United State1995–1998. JAMA 2001;285:1729–35.