Embed Size (px)
Citation preview

1
DECLARATION
I, Dr. Sai Satish Kandraju, hereby declare that this project was undertaken by me
under the supervision of the faculty, Department of Neurology, Sree Chitra
Tirunal Institute for Medical Sciences and Technology.
Thiruvananthapuram Dr. Sai Satish.Kandraju
Date:

2
Forwarded
The candidate, Dr Sai Satish.Kandraju, has completed the project under my guidance.
He has carried out the minimum required project.
Thiruvananthapuram Dr.Muralidharan Nair,
Date: Professor and Head,
Department of Neurology
SCTIMST.

3
ACKNOWLEDGEMENT
I take this opportunity to express my sincere gratitude to Dr Dr.Muralidharan Nair, Professor of
Neurology and Head, Department of Neurology, SCTIMST, my guide for the study, for his expert
guidance, constant review, kind help and keen interest at each and every step of the study
I am thankful to Mr Anees & Mr.Kenaz, Neurotechnologists for helping me with the technical
guidance while performing the study.
I express my sincere thanks to Dr. Sankara Sarma, Professor, AchuthaMenon Centre for Health
Science Studies for helping me with the statistical analysis of this study.
I am extremely thankful to the nursing staff, technicians and my colleagues in the Department
of Neurology for their valuable input and assistance to the study.
Last but not the least, I extend my gratitude to all my patients and their primary caregivers who
willingly participated in this study.
Dr Sai Satish Kandraju
Senior Resident
Department of Neurology
SCTIMST, Trivandrum, Kerala

4
INDEX
i. Introduction 1
ii. Review of Literature 3
iii. Hypothesis and objectives of the study 23
iv. Subjects and Methods 24
v. Results 27
vi. Discussion 56
vii. Conclusions and summary 63
viii. Limitations 65
ix. References 66
x. Annexure 76

5
INTRODUCTION:
Standard diagnostic nerve conduction tests evaluate integrity of large nerve fibers which
explain numbness and tingling, but not pain and dysesthesias which are common in Carpal
tunnel syndrome (CTS). Cutaneous silent period (Cu.SP) is an electrodiagnostic method to
evaluate small nerve fibers1.This study looks at the variables of Cu.SP in CTS as compared to
normal individuals.

6
REVIEW OF LITERATURE
Electrophysiology is an integral part of the physician’s diagnostic armamentarium. It is
considered as an extension of the physical examination to determine the neuro-anatomical
localization and underlying pathophysiology. Nerve conduction studies and electromyography
are widely used to evaluate the integrity and various disorders affecting the peripheral nervous
system.
Classification of Peripheral Nerves: A brief note.
Peripheral nerve fibers were classified by Erlanger and Gasser into A (α,ß,γ,δ),B and C
fibers based on their diameter and conduction velocities2.While the thickly myelinated Aα, Aß
fibers designated as “large fibers”, sub serve motor efferents to extrafusal fibers in addition to
touch, vibration and joint position sense, thinly myelinated Aδ and unmyelinated C fibers are
segregated as “small fibers” which sub serve pain and temperature sensation in addition to
autonomic functions. Figure 1 shows a Classification of peripheral nerve fibers3.

7
1
Routine nerve conduction studies do not evaluate small nerve fibers: Simple tool to evaluate
function of small nerve fibers-Unmet need.
Most of the parameters in various nerve conduction tests done routinely, like distal
latency, compound muscle action potential and conduction velocity in the motor conduction
studies evaluate the functioning of large nerve fibers, and similarly peak latency of sensory
nerve action potential in the sensory conduction studies also evaluate large nerve fiber’s
integrity. Thus, these parameters are unperturbed in disorders affecting small nerve fibers
selectively. In another view, the above modalities of investigations are also insensitive to
Figure 1:-Classification of peripheral nerve fibers3

8
implicate the involvement of small nerve fibers in patients complaining of pain in disorders such
as in Carpal tunnel syndrome.
There are few semi quantitative electrophysiological methods by which small nerve
fibers are evaluated. These include Quantitative cold, warm and pain threshold tests. However,
these tests need sophisticated equipment like neodymium Laser (Nd: YAP) stimulator to elicit
pinprick (pain) sensation and Thermal Sensory Analyzer for determining warm and cold sensory
threshold4. In addition, these tests rely on response of the individual, thereby hindered because
of subjective bias. Quantitative sudomotor axon reflex test (QSART) and Thermoregulatory
sweat tests evaluates autonomic nervous system.5 The definitive diagnostic test for small fiber
neuropathy is Intraepidermal nerve fiber density estimation, which needs minimally invasive
skin biopsy and immunostaining with protein gene product of 9.5 which is available, mainly in
research or referral lab settings6. In this context, there is a need for a simple, readily available,
cost effective and technically feasible test for evaluating small nerve fibers.
Cutaneous silent period (Cu.SP) is a brief period of cessation of muscle contraction that
occurs after stimulation of the cutaneous nerves close to or distant from the muscle that is
contracting.1 Stimulation of small nerve fibers, especially Aδ fibers, is needed to elicit this
response, which can be done with standard electromyography equipment using simple settings.
Hence, Cu.SP is a simple non invasive approach to study small nerve fibers, which needs
standardization of method.

9
Cutaneous Silent Period for evaluation of small nerve fiber’s dysfunction. What is it?
The Cu.SP is protective painful withdrawal reflex as it is obtained by electrical stimuli
that are felt as painful1. It is a spinal inhibitory reflex sub served essentially primarily by small-
diameter Aδ fibers, which enter the spinal cord’s dorsal horn and inhibits activity in spinal
motor nuclei in neighboring myotomes. This motor neuron inhibition may be mediated by
Renshaw cells which are presumed to be directly activated by high threshold cutaneous
afferents i.e small fibers14.
Thinly myelinated afferents fibers are the important component of the afferent arc of
the Cu.SP in limb muscles. Even though the electrical stimulus needed to elicit the Cu.SP
stimulates both large- as well as small-diameter fibers, the long latency of the CSP, seen in
muscles of distal upper extremity, 50 –80 ms after stimulation of the finger, is more consistent
with a spinal reflex mediated by afferent fibers with slow conduction velocities.Conduction
velocity of the afferents fibers were derived by stimulating two points of a cutaneous nerve,
which yielded approximate values of 9 –18 m/s, within the range of conduction velocities of A-
delta fibers7.The high intensity of stimuli required to elicit the Cu.SP are beyond that required
for eliciting a maximal Sensory Nerve Action Potential8. In addition, when afferents with large
diameter blocked are blocked by ischemia Cu.SP was still elicitable 9. Above observations
support the hypothesis that the afferent pathway of the Cu.SP is composed by fibers which are
small and have thin myelination. Moreover, preserved Cu.SPs were observed in patients with
peripheral neuropathy affecting large diameter sensory fibers, who had unelicitable Sensory
Nerve Action Potentials or somato sensory evoked potentials (SSEPs), which strengthens the

10
argument against an important role for fibers with large diameter in the CSP10. However, large-
diameter afferent fibers contributed for Cu.SP, albeit this contribution may not be important11.
Figure 2 depicts Cutaneous silent period elicited in hand and leg in a normal subject.
Different variables in Cutaneous Silent Period:
As depicted in Figure 2 (red colored lines), different variables of Cu.SP can be
determined from the averaged surface electromyography traces. The beginning and endpoint
latencies of Cu.SPs can be identified through visual inspection at the start of a sudden cessation
and at the time of return of surface electromyographic activity, respectively. The “latency” of
the Cu.SP can be derived by measuring the time between the stimulation and the sudden
beginning of the silent period. The latency of the Cu.SP increases with height of the subject. The
“duration” of the CuSP can be derived by measuring the time from the beginning to endpoint of
the silent period, which denotes intensity of suppression. In contrast to averaged EMG traces,
rectified EMG traces allows to calculate Cu.SP area which can also be used to express the
intensity of suppression11.
Cutaneous silent period: from bench to bedside.
The clinical significance of this inhibition might be to ‘‘prime’’ the extremity (Eg. upper
extremity) for a prompt withdrawal away from a noxious stimulus, by selectively inhibiting
muscles that are responsible for approaching and grasping (triceps and intrinsic hand
muscles).At the same time, allowing the activation of the muscles that sub serve withdrawal
(biceps & deltoid muscles). From a practical viewpoint, it is pertinent that reflex inhibition of
continuing motor activity might be a part of reflex withdrawal. For instance, in case of a hand

11
unknowingly approaching and grasping a hot object, it is safe and beneficial to drop the object
before withdrawing the extremity12.If he doesn’t leave, he will burn himself.

12

13
Sites where Cutaneous silent period can be elicited:
In upper limbs, Cu.SP elicited by stimulation of the fingers is marked in the intrinsic
muscles of hand. In one study, stimulation of the finger elicited Cu.SPs lasting from 50 - 100 ms
in the abductor pollicis brevis muscle13. In another study which looked at the distribution of the
Cu.SP elicited after stimulating the index finger, revealed incrementally longer latency of Cu.SP
in distal muscles and the greater magnitude of inhibition in thenar and hypothenar hand
muscles. Finger stimulation elicited relatively briefer periods of Cu.SP in muscles of the forearm
and masseter, while Cu.SP was unelicitable in the orbicularis oculi muscles14. It is also observed
that the same stimulus facilitated the ongoing contraction the biceps and deltoid muscles15.
In lower limbs, Cu.SPs is elicited in soleus and tibialis anterior muscles after stimulating
either plantar or sural nerves innervating the foot13. Latency and duration of Cu.SP was 80–100
ms and 40-80ms respectively in both muscles after stimulating sural nerve. Plantar stimulation
elicited Cu.SPs with a latency about 20 ms longer relatively.
In cranial musculature (Masseter and Temporalis) stimulating Trigeminal stimulation
over face, gums or teeth elicits Silent Periods16. The Masseter Inhibitory Reflex is elicited after
stimulating the mental nerve during maximal steady bite by the subject. In contrast to Cu.SPs
elicited in upper limbs, Silent periods elicited in cranial musculature has two discrete periods of
silence analogous to oligosynaptic and polysynaptic components of the blink reflex (R1 & R2
components respectively).

14
Though silent period can be elicited from cranial, upper and lower limb musculature,
major advantage in utilizing the upper limb depends on the fact that particularly strong reflex
changes can be evoked by stimulating fingers and thumb17.
Cutaneous silent period in various disorders:
Central nervous system disorders:
Parkinson’s Disease & Dystonia:
While CuSP duration was prolonged in Parkinson’s disease18 and dystonia19, its latency,
magnitude of suppression and intensity of post inhibition facilitation was not different from
controls. Dopa replacement rectified prolonged CuSP in Parkinson’s disease but not in atypical
Parkinsonism.
Syringomyelia:
CuSP abnormalities range from shortened duration to unelicitable CuSP depending on
the severity of the cavitation involving the posterior horn of spinal cord20,21.
Peripheral nervous system disorders:
Radiculopathies:
As stimulated impulse needs to traverse the proximal sensory radicles to reach the
spinal cord, one of the suggested uses of Cu.SP was to assess the integrity of the sensory
radicles especially following traumatic brachial plexopathy22. The muscle selected for recording
must be innervated from different radicle as compared to the sensory level being assessed. By

15
this approach, the absence of the CSP could point the discontinuity of the sensory root at the
level corresponding to the stimulated finger.
Peripheral neuropathies:
The application of Cu.SPs to diagnose generalized neuropathy has been overall
ineffective.
Cu.SPs were normal in neuropathies with large fiber involvement like in idiopathic
sensory neuronopathy10, abetalipoproteinemia23 Friedreich’s ataxia14.
Considerable interest has been directed at determining whether the Cu.SP can be
utilized for evaluating small-fiber neuropathies, as small diameter fibers are not well evaluated
by standard nerve conduction tests. Even though all evidence suggest an important
contribution from small myelinated fibers to the Cu.SP, unequivocal abnormalities in the Cu.SP
have been identified only in subjects with severe small-fiber dysfunction as in Fabry disease and
Hereditary sensory and autonomic neuropathy. Cu.SP in patients with Fabry disease was of
shorter duration and intensity of suppression was also abnormal as compared to controls.24
Cu.SP in patient with Hereditary sensory and autonomic neuropathy was unelicitable upon
stimulation of one digit, while it was delayed and shorter upon stimulating 2 digits25.
Carpal tunnel syndrome:
Yong Seo Koo et al reported longer mean Cu.SP latencies in CTS when compared to
control group, although there was no difference in duration of Cu.SP. The duration and latency
of Cu.SP correlated with the severity of CTS.26

16
M.J. Pablo et al reported no responses in a small percentage of severe CTS. In the rest of
the severe CTS, and the moderate/severe cases, the latency was increased and the duration
was decreased. No alterations were found in the Cu.SP in mild and moderate cases.27
S.K. Aurora et al reported absent Cu.SP in severe cases and prolonged duration in mild to
moderately severe CTS cases.28
Although there have been studies on variables of Cutaneous silent period in patients
with Carpal tunnel syndrome, results were variable. Hence we attempted to systematically
examine Cu.SP in CTS of variable severity which would help us to validate changes of Cu.SP in
CTS.
Carpal tunnel syndrome:
Carpal tunnel syndrome is defined as “a constellation of clinical symptoms and signs
resulting as a consequence of compression of median nerve at the level of wrist and ensuing
slowed conduction.”29
There are no epidemiological data from India. Studies from western population report
an incidence of 1-3 cases per 1000 persons per year30,31,32.Study from Sweden reports
prevalence of clinical and electrophysiologically proven carpal tunnel syndrome to at 2.7%
(CI,2.1%-3.4%)33.Females are 3-10 times more commonly diagnosed with CTS as compared to
males30.The peak age range susceptible for CTS is 45-60yrs.Only 10% of CTS patients are
younger than 31 years30.

17
The features that highly suggest CTS are (1) Pain or paresthesias during driving, holding
a phone,book or news paper. (2)Above symptoms involving 1st, 2nd, 3rd along with radial aspect
of 4th digit. (3)Nocturnal arousal from sleep due to sensory symptoms. (4)Shaking or wringing
the hand to relieve the symptoms. (5)Weakness or wasting of thenar group of muscles.
(6)Phalen’s maneuver precipitating the symptoms34.
Boston Carpal Tunnel Questionnaire (BQ)35:
Also known as Levine scale, BQ is a patient- derived outcome measure that was
structured particularly for patients with CTS.
It includes 2 discrete scales, the Symptom Severity Scale (SSS) which consists 11
questions with a 5 point rating scale and the Functional Status Scale (FSS) with 8 items which
needs to be rated for extent of difficulty on a 5 point scale. Each scale gives an ultimate score
calculated as sum of individual scores divided by number of items. The final score ranges from 1
to 5, with an increasing score score signifying increasing disability 35. The BQ has been adopted
as an outcome measure in several studies, and also withstood considerable testing in terms of
validity, reliability and responsiveness. The evidence indicates that the BQ is a valid, reliable,
responsive and satisfactory tool that should be considered as a primary outcome variable in CTS
trials36.
Diagnosis of clinically suspected CTS is confirmed electrophysiologically by
demonstrating focal conduction slowing of median nerve at the level of the carpal tunnel.
When the standard motor as well as sensory median nerve conduction tests are normal, CTS is
diagnosed based on internal comparison studies between median and ulnar or radial nerves.

18
Sensitivity and specificity of these internal comparison test are depicted in the Table 137,38.
Accordingly, severity of CTS can be graded based on electrophysiological data according to
Canterbury neurophysiological grading as described in Table 239.
Table .1.Characteristics of internal comparison studies in CTS37,37.
Test Sensitivity(%) Specificity (%) Distance Significant
difference
Median – Ulnar digit IV
sensory latency
74 97 12-14cm >0.5 msec
Median-Radial digit I
sensory latency
76 97 8-10cm >0.5msec
Median-Ulnar palm-
wrist latency study
70 97 8cm >0.4msec

19
Table.2.Canterbury Neurophysiological grading of CTS39.
Severity
grade
Sensory
conduction
velocity
SNAP Motor
conduction
velocity
Motor
potential
amplitude
0 Normal No neurophysiological abnormality
1 Very mild Above tests are normal
Detected by sensitive tests (Internal comparision studies)
2 Mild Slowing Preserved Normal Preserved
3 Moderate Slowing Preserved >4.5 - <6.5ms Preserved
4 Severe Absent >4.5 - <6.5ms Preserved
5 Very severe Absent >6.5ms Preserved
6 Extremely
severe
Sensory and motor potentials effectively unrecordable (surface
motor potential from APB <0.2mV amplitude)

20
HYPOTHESIS AND OBJECTIVES OF THE STUDY
HYPOTHESIS:
There is involvement of small sensory fibers causing pain in Carpal Tunnel Syndrome,
which is responsible for abnormal Cu.SP. Depending on the severity of small sensory fibers
involvement there will be corresponding changes in CuSP.
We propose following pathophysiological mechanisms underlying the abnormalities of
Cu.SP in CTS.
In CTS, pain carrying fibers in the median nerve gets compressed as they traverse the
carpal tunnel and become dysfunctional, there by delaying their conduction velocity, which
should reasonably prolong the latency of Cu.SP.
Normal pain carrying fibers decrease in number as disease progress, thereby decreasing
the magnitude of inhibition of motor neurons, which can be conceivably reflected in NCS as
decrease in duration of Cu.SP.
In case of severe CTS where all pain fibers are dysfunctional and there is no conduction
possible and motor fibers are not inhibited, it is plausible that Cu.SP will be absent.
OBJECTIVES OF THE STUDY:
1. To systematically study the characteristics of Cu.SP in the sample.
2. To attempt a correlation between clinical and electrophysiological severity of the CTS and the
characteristics of Cu.SP.

21
SUBJECTS AND METHODS
Study design and setting:
This study was a hospital based cross-sectional descriptive study. The subjects were
selected among the patients attending the Electromyography lab of Department of Neurology,
Sree Chitra Tirunal Institute of Medical Sciences and Technology, Thiruvananthapuram.
Study period:
The study was conducted over a period of 18 months from 4th March 2014 to September
2015.
Methodology:
Consecutive patients attending the Electromyography lab in the Sree Chitra Tirunal
Institute of Medical Sciences and Technology were screened for eligibility for the study.
Those fulfilling the inclusion criteria were explained the procedure and those willing to give
informed consent were recruited into the study. The subjects were interviewed using a detailed
questionnaire to note the demographic data, duration of symptoms, symptom severity and
functional severity score. The subjects were then evaluated by nerve conduction studies and
surface electromyography.

22
Ethical considerations:
The study was approved by the Institute Ethical Committee. Written informed consent
was obtained from all the subjects participating in the study. The informed consent procedure
was done according to the guidelines provided in the Declaration of Helsinki and the ICH E6
Guideline for Good Clinical Practice.
Inclusion criteria:
1. Consecutive patients evaluated in EMG laboratory for CTS and those consenting for the
study.
2. Patients referred to EMG laboratory for evaluation of their primary condition, but with
normal conduction studies and consenting for the study were included as Controls.
3. Patients referred to EMG laboratory for diagnosis other than CTS with abnormal nerve
conduction studies and those consenting for the study were included as Disease controls.
Exclusion criteria:
1. Subjects not tolerating the discomfort and not co-operating for the study.
2. Patients with history of surgery for cervical spondylosis or herniated intervertebral discs
(nucleus pulposus) were excluded.
Symptom Evaluation:
Details of symptoms regarding the duration, severity of the symptomps and consequent
functional disability were noted based on Boston Questionnaire (See Appendix i). The
questionnaire consists of 11 questions on the severity of symptoms i.e Symptom Severity Scale

23
(SSS) and 8 on functional disability i.e Functional Severity Scale (FSS). SSS and FSS scores were
obtained after calculating the means of responses to the individual questions. Answers to the
first 5 questions of the SSS were used to assess pain severity [Pain Severity Score (PSS)].
Neurophysiological evaluation:
I. Diagnosis and electrophysiological grading of CTS
CTS: Diagnosed based on nerve conduction studies, and the severity graded according to
the Canterbury neurophysiological grading of CTS (See Table 2).
II. Method to elicit CuSP
• Surface electromyographic activity was recorded from the abductor pollicis brevis (APB ).
• During a maximal voluntary contraction, a single painful stimulus was given to ipsilateral 2nd
finger until a complete silent period of reproducible latency and duration was acquired.
• To obtain a maximum and steady contraction, the subject was asked to contract against
resistance, and muscle contraction was monitored with help of auditory output from EMG
machine.
• A stimulus of 0.2 ms duration was given and gradually intensity of stimulus was increased
up to values above 40 mA, until a constant response was obtained. The latency, duration
and end point of CuSP was determined.
• 5 recordings showing Cutaneous silent period with shorter latency in addition to longer
duration were selected for analysis. The average of latencies, durations and endpoints of
Cu.SPs (the average values of the 5 recordings) were used in the final analysis.

24
Statistics:
Data analysis was performed using SPSS ver.22.0.Quantitative variables were described
by mean and standard deviation. Qualitative variables were described by frequency
distribution.
Comparison of Quantitative variables between two groups was done by independent
sample t-test. Comparison of averages among more than two groups was analyzed by ANOVA,
while multiple comparisons among the group were analyzed by post hoc test.
Variables which were found to be significant during univariate analysis were subjected
to multivariate analysis of binary logistic regression.
A p value of <0.05 was taken as level of significance.

25
Results:
50 patients satisfyied the inclusion criteria for CTS cases and lab controls. However, 6
patients, each from CTS group and control group did not co-operate to elicit Cu.SP because of
discomfort associated with stimulus. Hence, they were not included in the analysis. Among
remaining 44 patients in each group, 3 patients from CTS group and 6 patients from control
group co-operated to elicit Cu.SP in one hand only. Hence, data of 85 hands from 44 CTS cases
and 82 hands from control cases were available for analysis. As Cu.SP was absent in 4 out of 85
CTS hands, finally 81 CTS hands were considered for analyzing the Cu.SP variables and various
clinical and electrophysiological characteristics.
50 CTS patients
44 CTS patients (88
hands)
3 CTS patients allowed
examination of only one hand
85 hands were
analyzed
6 didn't tolerate
procedure
50 lab controls
44 CTS lab controls (88
hands)
6 subjects allowed only
one hand examination
82 hands were
analyzed
6 didn't tolerate
procedure

26
Demographic characteristics:
CTS group was significantly elder than the control group. Mean age of CTS group being
49.1 +11.04 yrs as compared to mean age of control group (35.2+13.71yrs) which was
statistically significant (p<0.001). The gender distribution and height were not statistically
different between the two groups (p 0.647 and 0.106 respectively). 29.5% (n=13) of CTS group
and 34.1% (n=15) of control group were males. 70.5% (n=31) among CTS group and 65.9%
(n=29) among control group were females. Mean height of CTS group was 159.0 +9.4 cm as
compared to 162+8.3 cm in control group.
49.1
35.2
0
10
20
30
40
50
60
70
CTS Control
Age in years(p<0.001)

27
159 162.1
0
20
40
60
80
100
120
140
160
180
CTS Controls
Height in cm(p =0.106 )
29.5 34.1
70.5 65.9
0%
20%
40%
60%
80%
100%
CTS Controls
Gender distribution(p =0.647 )
Male Female

28
Characteristics of CTS group:
Among the CTS group, mean Symptom Severity Score (SSS) was 1.95 + 0.67, mean Pain
Severity Score (PSS) was 1.94 + 0.97 and Functional Severity Score (FSS) was 2.03 + 0.89. All the
severity scores were positively correlated with each other, which was statistically significant as
depicted in the table.
Correlation between scores of Boston Questionnaire
Symptom Score
Severity
Pain Severity
Score
Pain Severity Score .840** 1
Functional Severity
Score
.694** .662**
** Correlation is significant at .001 level
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
0 1 2 3 4 5
Sym
pto
m a
nd
Pai
n s
eve
rity
sco
re
Functional severity score
Correlation between FSS,SSS & PSS
Pain severity score
Symptom severity score
Linear (Pain severity score)
Linear (Symptom severity score)

29
Duration of symptoms ranged from 0.5 months to 84 months with median duration of
12 months (IQR 6-24 months).Duration of symptoms was significantly positively correlated with
SSS (r 0.22,p 0.01) and FSS (r 0.27,p 0.01), but not with PSS (r 0.11,p >0.05).
Based on the Canterbury scale, among 85 hands with CTS, 4 hands were grade1, 26
were grade2, 39 were grade 3, 6 were grade 4, 9 were grade 5 and one hand was grade 6.
Subgroups based on Canterbury scale were not different in terms of age, gender
distribution and height (p=0.93, p=0.57 & p=0.39 respectively). Similarly, duration of symptoms,
symptom severity score, pain severity score and functional severity scores were not different
among the subgroups divided by Canterbury scale (p=0.17, p=0.07, p=0.46 & p=0.32
respectively).
5%
31%
46%
7%
10%
1%
Percentage of hands in each Grade of CTS (n=85)
Grade 1 (very mild, n=4)
Grade 2 (mild,n=26)
Grade 3 (moderate,n=39)
Grade 4 (severe,n=6)
Grade 5 (very severe,n=9)
Grade 6 (extremely severe,n=1)

30
Comparison of mean age between CTS subgroups
Neurophysiological
grading
N Age in years F p
Mean sd
1.0 4 52.25 14.77
.273
.927
2.0 26 49.19 12.56
3.0 39 49.13 10.70
4.0 6 48.60 13.59
5.0 9 45.90 7.77
6.0 1 55.00
Total 85 48.95 11.13
Comparison of mean height between CTS subgroups
Neurophysiological
grading
N Height in cm F p
Mean sd
1.0 4 150.75 6.65
1.062
.388
2.0 26 159.35 9.40
3.0 39 158.73 8.37
4.0 6 160.00 8.03
5.0 9 163.15 12.90
6.0 1 160.00
Total 85 159.15 9.27

31
Comparison of Gender distribution between CTS subgroups
Neurophysiological
grading
Male Female
N % N %
1.0 2 8.0 2 3.3
2.0 9 36.0 17 28.3
3.0 8 32.0 31 51.7
4.0 2 8.0 4 5.0
5.0 4 16.0 5 10.0
6.0 0 0.0 1 1.7
Total 25 100.0 60 100.0
χ2 =3.870 df =4 p=0.568
Comparison of Mean Symptom severity score between CTS subgroups
Neurophysiological
grading
N symptom severity F p
Mean sd
1.0 4 1.40 0.33
2.153
.068
2.0 26 1.88 0.69
3.0 39 1.94 0.66
4.0 6 1.82 0.16
5.0 9 2.35 0.71
6.0 1 3.18
Total 85 1.95 0.67
Comparison of Mean Pain severity score between CTS subgroups
Neurophysiological
grading
N Pain severity score F p
Mean sd
1.0 4 1.20 0.40
2.0 26 1.99 1.02

32
3.0 39 1.94 0.91
.941
.459
4.0 6 1.72 0.82
5.0 9 2.12 1.23
6.0 1 3.20
Total 85 1.94 0.97
Comparison of Mean Functional severity score between CTS subgroups
Neurophysiological
grading
N Functional severity
score
F p
Mean sd
1.0 4 1.97 1.13
1.194
.320
2.0 26 1.94 1.00
3.0 39 1.93 0.72
4.0 6 2.13 0.85
5.0 9 2.56 1.11
6.0 1 3.13
Total 85 2.03 0.90
Comparison of Mean duration of symptoms between CTS subgroups
Neurophysiological
grading
N Duration of symptom in
months
F p
Mean sd
1.0 4 19.88 27.96
1.616
.166
2.0 26 18.23 14.89
3.0 39 15.48 18.88
4.0 6 9.00 2.83
5.0 9 31.26 24.48
6.0 1 36.00
Total 85 18.24 18.77

33
Characteristics of Cu.SP.
Considering both CTS and control groups together (n=177), among the demographic
factors, Age had significant positive correlation with latency (r 0.29, p<0.001) and endpoint (r
0.37,p <0.001).Height had significant correlation with latency alone (r 0.32 p <0.001).On linear
regression analysis both age and height predicted Cu.SP latency and endpoint.
Correlation of Latency
Pearson
correlation - r
p
Age .293** <0.001
height .324** <0.001
Correlation of End point
Pearson
correlation - r
p
Age .373** .000
height .132 .094
Correlation of Duration
Pearson
correlation - r
p
Age .153 .052
height -.111 .157

34
Linear regression analysis was performed on all hands (n=177)
Dependent Variable: latency
Predictors: (Constant), height, Age
Unstandardized
Coefficients
t p
B Std. Error
(Constant) -8.614 13.324 -.646 .519
Age .221 .048 4.564 .000
height .459 .081 5.673 .000
Linear regression analysis was performed on all hands (n=177)
Dependent Variable: Duration
Predictors: (Constant), height, Age
Unstandardized
Coefficients
t p
B Std. Error
(Constant) 76.065 27.097 2.807 .006
Age .184 .099 1.865 .064
height -.208 .165 -1.263 .208
Linear regression analysis was performed on all hands (n=177)
Dependent Variable: Endpoint
Predictors: (Constant), height, Age
Unstandardized
Coefficients
t p
B Std. Error
(Constant) 38.893 24.579 1.582 .115
Age .470 .089 5.258 .000
height .404 .149 2.708 .007

35
When latency, duration and endpoint of Cu.SP were analyzed, latency had significant
negative correlation with duration (r -0.341,p 0.01) as depicted in scatter diagram below and
positive correlation with endpoint (r 0.271, p=0.01). Endpoint had significant positive
correlation with duration (r 0.741, p=0.01).
Correlation between Cu.SP variables
Latency Duration End point
Latency 1.000 -.341** .271**
Duration -.341** 1.000 .741**
**. Correlation is significant at the 0.01 level (2-tailed).
0
20
40
60
80
100
120
140
0 20 40 60 80 100 120
Latency
Duration
Correlation of latency & duration

36
0
50
100
150
200
250
0 20 40 60 80 100 120
Endpoint
Latency
Correlation between latency & endpoint
0
20
40
60
80
100
120
140
160
180
0 20 40 60 80 100 120
E
n
d
p
o
i
n
t
Duration
end point in ms

37
Cu.SP in CARPAL TUNNEL SYNDROME Group:
Of all CTS hands (n=85), Cu.SP could be elicited in 81 hands (95.3%) and Cu.SP was
absent in 4 hands (4.7%).Cu.SP was absent in very severe (n=3) and extremely severe (n=1) CTS
hands and none in less severe grades of CTS.
Mean latency, duration and endpoint of Cu.SP among CTS hands were 78.07 + 12.35ms,
50.56 + 20.36 ms and 127.61 +15.0ms respectively.
When variables of Cu.SP and severity scores were analyzed, only functional severity
score had significant positive correlation with duration (r=0.28, p 0.01) and endpoint (r=0.29, p
0.001) of Cu.SP. Latency of Cu.SP didn’t have any significant correlation with any of the clinical
severity scores (SSS, PSS or FSS).
Correlation between Cu.SP variables and score on Boston Questionnaire
Latency Duration End point
Symptom severity score -.100 .163 .129
Pain severity score -.138 .090 .018
Functional severity
score
-.113 .281* .289**
**. Correlation is significant at the 0.001 level.
*. Correlation is significant at the 0.01 level.

38
In addition, among the Cu.SP variables, endpoint (r 0.25, p=0.01) alone was positively
correlated with duration of symptoms.
Cu.SP latency increased as neurophysiological grade of CTS increased. Mean Cu.SP
latency in very severe CTS (grade 5) was longest (86.12+3.16ms), followed by severe (grade 4,
82.57+16.83ms), moderate (grade 3, 78.35+12.49ms, p=0.067), mild (grade 2, 76.83+11.1ms,
p0.034) and very mild CTS (grade 1, 64.65+11.89ms, p=0.001).Mean Cu.SP latency of all severe
CTS hands (severe + very severe hands, 84.34+11.69 ms) was significantly greater than that of
very mild CTS (p=0.005) but not significantly longer than that of mild and moderate CTS (p=0.75
& p=0.13, respectively)
64.6576.83 78.35 82.57 86.12
0
20
40
60
80
100
120
1 2 3 4 5
Late
ncy
in m
s
Neurophysiological grade
Cu.SP latency in different grades of CTS

39
Mean Cu.SP duration was not significantly different among different grades of CTS.
Similar to Cu.SP latency, endpoint also increased as neurophysiological grade of CTS
increased. Mean Cu.SP endpoint of Very Severe CTS (grade 5, 142 +11.83ms) was longest
followed by severe (grade 4, 136.1 + 14.88ms), moderate (grade 3,124.15 + 14.66ms), mild
(grade 2, 127.9 + 13ms) and very mild (grade 1,124 + 22ms). Mean Cu.SP endpoint of very
severe CTS was statistically longer than that of very mild, mild and moderate CTS (p=0.048,
p=0.03, p=0.004 respectively), but was not statistically longer than severe CTS (p=0.43).
59.3551.127 47.879
53.55 56.617
0
10
20
30
40
50
60
70
1 2 3 4 5
Duration in ms
Neurophysiological grade
Cu.SP Duration in different grades of CTS

40
When variables of Cu.SP and nerve conduction parameters (distal latency of CMAP and
SNAP latency) were analyzed, Cu.SP latency and endpoint but not duration, were positively
correlated with CMAP latency and SNAP latency which was statistically significant.
Correlation between Cu.SP variables and distal motor latency and sensory latency
CMAP_latency SNAP_latency
latency_in_ms .372** .312**
duration_in_ms .097 .026
end_point_in_ms .272** .181*
**. Correlation is significant at the 0.01 level (2-tailed).
*. Correlation is significant at the 0.05 level (2-tailed).
124 127.93 124.15 136.12 142.65
0
20
40
60
80
100
120
140
160
180
1 2 3 4 5
End point in ms
Neurophysiological Grade
Cu.SP Endpoint in different grades of CTS

41
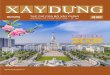
Samples of Cu.SP traces elicited from a moderately severe CTS case. Individual traces (above)
and superimposed traces.

42
CONTROL group:
Mean Cu.SP latency among controls was 70.10 ms +6.61 ms, which was significantly
shorter as compared to CTS group (p <0.001).Age adjusted mean Cu.SP latency of controls was
also significantly shorter (p <0.001). As compared with control group, Mean Cu.SP latency was
significantly prolonged in all grades of CTS except for very mild CTS (grade 1).
Mean Cu.SP duration among controls was 50.05 +20.15ms, which was slightly shorter
than that of CTS group (50.6+20.36ms, p=0.87), but was not statistically significant.
Mean Cu.SP endpoint among controls was 118.80 +22.06ms, which was significantly
shorter as compared to that of CTS hands (P=0.003).However, this significance was lost when
age adjusted mean Cu.SP endpoints were compared (p=0.65).

43
78.0770.1
0
10
20
30
40
50
60
70
80
90
100
CTS Controls
Late
ncy
in m
s
64.6576.83 78.35 82.57 86.12
70.1
0
20
40
60
80
100
120
1 2 3 4 5 Control
Late
ncy
in m
s
Neurophysiological Grade
Cu.SP latency in different grades of CTS & controls

44
50.56 50.05
0
10
20
30
40
50
60
70
80
CTS Control I
Du
rati
on
in m
s
59.3551.13 47.88 53.55 56.62
50.05
0
10
20
30
40
50
60
70
80
90
100
1 2 3 4 5 Control
Du
rati
on
in m
s
Neurophysiological Grade
Cu.SP Duration in different grades of CTS & controls

45
127.61 118.8
0
20
40
60
80
100
120
140
160
CTS Control I
End
po
int
in m
s
124 127.93 124.15 136.12 142.65118.8
0
20
40
60
80
100
120
140
160
180
1 2 3 4 5 Control
End
po
int
in m
s
Neurophysiological Grade
Cu.SP Endpoint in different grades of CTS & controls

46
Cu.SP traces elicited from a control. Individual traces (above) and superimposed traces.

47
Disease control group (Peripheral Neuropathy)
1 4 hands from 7 patients of peripheral neuropathy were analyzed. Mean Cu.SP latency
was 82.65 ms + 8.52ms which was significantly prolonged as compared to controls but not
significantly prolonged as compared to CTS group.
Category N Latency
p mean sd
CTS 81 78.07 12.34 <0.001
Controls 82 70.10 6.61
Disease
Controls 14 82.65 8.52
78.0770.1
82.65
0
10
20
30
40
50
60
70
80
90
100
CTS Controls Disease controls
Latency in ms
Comparison of mean Cu.SP latencies of different groups
Comparison Mean
difrerene se p
CTS and Disease Controls -4.5759 2.8329 .108
Controls and Disease Controls -12.5537* 2.8304 <0.001

48
Mean Cu.SP duration in the disease control group (49.69+7.09ms) was neither different from
that of the control nor the CTS group.
Category N Duration in ms
p mean sd
CTS 81 50.56 20.36 .980
Controls 82 50.05 20.15
Disease Controls 14 49.69 7.09
Comparison Mean
difference se p
CTS and Disease Controls .8698 5.6661 .878
Controls and Disease Controls .3606 5.6611 .949
50.56 50.05 49.69
0
10
20
30
40
50
60
70
80
CTS Controls Disease controls
Duration in ms
Comparison of mean Cu.SP Duration of different groups

49
Mean Cu.SP endpoint in the disease control group (132.11+12.25ms) was significantly
delayed as compared to Control group but was not statistically different from CTS group.
Category N End point in ms
p mean sd
CTS 81 127.61 15.00 .003
Control I 82 118.80 22.06
Control II 14 132.11 12.25
Comparison Mean difrerene se p
CTS and Control I 8.8148* 2.8943 .003
CTS and Control II -4.5007 5.3475 .401
Control I and Control II -13.3155* 5.3427 .014
127.61 118.8132.11
0
20
40
60
80
100
120
140
160
CTS Control Disease controls
End point in ms
Comparison of mean Cu.SP Endpoint of different groups

50
Discussion
The Cu.SP mean latency of patients with CTS was significantly prolonged in patients with
CTS as compared to that of controls. In addition, the prolonged mean latencies correlated with
the neurophysiological severity grading of CTS according to the Canterbury scale. There was
significant direct correlation between CuSP latencies and nerve conduction (CMAP distal
latency and SNAP latency) data. There was no correlation between latency and scores from
Boston questionnaire (SSS, PSS or FSS). Based on the proposed hypothesis that the Cu.SP
reflects the function of Aδ fibers, the prolongation of mean Cu.SP latencies might be related to
slowed conduction and dysfunction of the fastest-conducting fibers among the Aδ fibers40. This
observation is similar to those from previous studies26,40. Svilpauskaite et al40 in their study
involving forty CTS patients reported prolonged Cu.SP latencies in clinically severe CTS.
Similarly, Yong Seo Koo et al26 also reported prolonged distal latency in severe CTS group.
However, Aurora et al28, had observed that mean latency of CuSP in CTS group did not differ
significantly as compared to that of control group. Disparity in the results of this study might
have emerged because of methodological differences in eliciting the CuSP or incomplete
control of factors that plausibly affect CuSP, such as age, gender and height, as well as a fewer
number of subjects (n=19).This is important because age and gender has complex influence on
Cu.SP41, with age changes being more pronounced in males but not in females, especially when
younger than 35 years of age. In addition in our study and previous study by Yong Seo Koo et al
observed that age and height predicted Cu.SP latency.

51
We observed that Cu.SP latency of very mild group was prolonged than that of control
group, though it was not statistically significant. However, rest of all the severe grades of CTS
had Cu.SP latency which was significantly greater than the control group. Hence, Cu.SP latency
may not be sensitive enough to delineate very mild CTS grade from normal hands.
In our study, duration of Cu.SP was little longer in CTS group than that of control group,
though it was not statistically significant. However, duration in severe CTS was shorter as
compared to very mild CTS. The above finding indicate that as the number of normally
functional Aδ fibers decreases, the intensity of motor neuron inhibition decreases, thereby
decreasing the duration of Cu.SP. Shorter duration of Cu.SP in CTS group was also reported by
Yong Seo Koo et al26. On the contrary, Aurora et al28 reported increased Cu.SP duration in CTS
group and proposed that oversensitization of remaining polymodal C fibers as the mechanism
to explain their observation. Similar to the finding in study by Svilpauskaite et al40 , we observed
prolonged duration of Cu.SP in very mild and mild cases as compared to controls. This may be
secondary to following factors: (1) In order to attain maximal contraction of APB, thumb is
contracted against a resistance. In mild CTS groups, voluntary contraction of APB can be slightly
decreased because of decreased perception of the resistance applied to the thumb caused by
the dysfunctional sensory fibers. This might increase duration of Cu.SP. Two studies have shown
that CuSP duration increases as strength of contraction decreases.42,9 (2) Partial dysfunction of
median motor fibers compressed within the carpal tunnel (caused by axonotmesis or
neurapraxia) can also lead to reduction in the voluntary activity, and thereby increasing Cu.SP
duration.

52
The Endpoint of Cu.SP was found to be significantly delayed in CTS hands as compared
to that of controls. Given the positive correlation we found between endpoint and latency
(which is prolonged in CTS) and duration being similar in both the study groups, it is plausible
that endpoint may be prolonged as a function of latency in CTS cases. Leis AA et al7, studied
silent period produced by electrical stimulation of mixed peripheral nerves and reported that
endpoint of Cu.SP was determined by Cutaneous afferents. On the contrary, Yong Seo Koo et al
reported no difference in Cu.SP endpoints between study groups and suggested that endpoint
was not influenced by peripheral nerve lesions but a function of supraspinal control. This
discrepancy needs to be sorted out in future studies.
In addition as Cu.SP Endpoint increased, Cu.SP duration was expected to increase, as
both showed a positive correlation. However, though CuSP endpoint was significantly
prolonged in the CTS group as that of control group, duration was not significantly increased
nor decreased as we hypothesised. This finding would suggest that, after spinal motor neurons
gets inhibited by afferent volley of impulses from small nerve fibers, duration after which they
recover may depend on other influences on motor neurons like supraspinal mechanisms. This
was exemplified in a study by Serrao et al18 where Cu.SP duration was prolonged in Parkinson’s
disease patients in “off” state that decreased in “on” state following L-dopa treatment,
implicating supraspinal dopaminergic pathways influencing duration of Cu.SP. In another study
by Logigian et al43, reported decreased intensity of spinal motor inhibition in complete cervical
spinal cord injury patients as compared to normal suggesting the influence of supraspinal
mechanisms on Cu.SP.

53
Following table gives an overview of studies on Cu.SP in CTS.
Overview of studies of Cutaneous Silent Period in Carpal tunnel syndrome
Study
(CTS=n)
(controls=n)
Latency in ms
Duration in ms
Endpoint in ms
/
CTS
Control
P value
CTS
Control
P
value
CTS
Control
P
value
Aurora et.al28
1996 (CTS = 19)
(Controls=20)
NA
NA
NS
51.8
36.9
0.001
127.3
113.4
0.005
Svilpauskait et
al40
2006 (CTS = 40)
(Controls=40)
Mild
77.91+4.34
75.47+5.81
NS
Mild
55.1+8.4
43.19
<0.01
NA
NA
NA
Moderate
81.66+6.56
<0.01
Moderate
57.11+10.28
<0.01
NA
Severe
85.02+6.45
<0.01
Severe
39.74+8.68
NS
NA
Y. S. Koo et al26
2010 (CTS = 114)
(Controls=30)
72.4+16.1
64.6+13.4
0.014
58.9+21.4
65.1+15
0.133
129.7+16.2
131.3+17.6
0.519
Current study
2015 (CTS = 44)
(Controls=44)
78.07+12.35
70.1+6.61
<0.001
50.56+20.36
50.05+20.15
0.87
127.61+
118.8+22
0.003
NA – Not available, NS-Not significant

54
Cu.SP was absent in 4.71% of CTS hands (n=4/85) and none in the control group. All the
hands in which Cu.SP was absent were of very severe (n=3) or extremely severe (n=1) grade of
CTS, but none of the CTS hands with lower severity Cu.SP was absent. This in agreement with
our hypothesis that when all pain carrying fibers become dysfunctional as in hands of severe of
CTS, there will be no motor neuron inhibition and as a result Cu.SP will be absent. Similarly,
Cu.SP was absent in few of severe CTS hands in previous two studies28,40.
When we looked at the utility of the Cu.SP in assessing the severity of pain, we found
that there was no statistically significant correlation between Cu.SP parameters and clinical
questionnaires quantifying symptom and pain severity.Only functional severity score were
positively correlated with prolonged endpoint. Conceivably, more impaired the Cutaneous
sensations, more difficult it would be to fine tune the skilled hand movements, hence more
functional disability.In a previous study by Inghilleri et al who investigated changes in the Cu.SP
in healthy subjects following administration of opioids, observed that there were no changes in
Cu.SP parameters following administration of opiods, even though there was significant
decrease in painful sensation with electrical stimulation. These findings convey that the Cu.SP,
which reflects Aδ fiber function, may be not a dependable tool for assessing severity of pain.
One explanation may be because painful sensations from periphery are carried by both C fibres
and Aδ fibres and, C fibers being unmyelinated and smallest in diameter are least susceptible to
compression effects or are affected last44.

55
As a sub test, we looked at variables of Cu.SP in 7 cases (14 hands) of peripheral
neuropathy and observed that only latency was significantly prolonged as compared to
controls. This was similar to observations made by Yaman et al in diabetic peripheral
neuropathy, wherein Cu.SP latency was longer as compared to controls45. When compared to
CTS group none of the variables were significantly different.
To conclude, Cutaneous Silent Period is a simple, less cumbersome and easily performed
electrophysiological tool to evaluate patients with carpal tunnel syndrome especially of mild or
greater severity. This was similar to studies done in other painful conditions like Fabry’s disease,
where in there was no significant change in variables of Cu.SP in mild to moderate
cases24.There is a need to improve the methodology to improve the sensitivity of Cu.SP to
pickup even the subtle small fiber dysfunction.

56
CONCLUSION
1. Cutaneous silent period is a simple, non cumbersome and easily available test that can be
done with standard electromyography equipment.
2. Cu.SP latency was prolonged in Carpal tunnel syndrome especially of mild or greater
severity.
3. Cu.SP duration and endpoint changes are variable in CTS as they are also influenced not
only by peripheral but also by supraspinal mechanisms, which are yet to be clearly
delineated.
4. Cu.SP variables were not affected by symptom severity or duration of symptoms.
5. Age and height of the individuals affect variables of Cu.SP.
6. The utility of Cu.SP is to assess the integrity of peripheral nerves in severe peripheral
neuropathies, where Cu.SP can be elicited in spite of unexcitable peripheral nerves during
standard conduction studies.

57
SUMMARY
Cutaneous silent period is a temporary cessation of voluntary muscle activity following a
painful stimulus. It evaluates small nerve fibers which form the afferent arc of this nociceptive
reflex. Cutaneous silent period is abnormal in Carpal tunnel syndrome, which is characterized
by pain, in addition to paresthesias. It should be included in protocols evaluating the peripheral
nervous system disorders as a complimentary to standard nerve conduction studies which
reflect large fiber dysfunction.
Based on the observations in previous studies18,40,43 and current study the beginning of
the Cu.SP may be mostly influenced by small fibers in the peripheral nerves, while its duration
and endpoint may be regulated by both peripheral mechanisms and supraspinal mechanisms in
the central nervous system.
Cutaneous silent period needs to be studied in greater detail in other peripheral and
central nervous system disorders to understand the anatomic elements and physiological
principles sub serving it and various pathologies affecting it. Further studies are needed to see
how well it fares in comparison with skin biopsy in diagnosing small nerve fiber neuropathy. If
validated and standardized it will be an invaluable tool to alleviate the ‘pain’ in diagnosing
conditions with small fiber dysfunction.

58
LIMITATIONS OF THE STUDY
1. Small number of subjects in each subgroup of CTS segregated based on Canterbury
neurophysiological grading.
2. Intensity of APB contraction was gauged by auditory output from EMG machine, which
can have subjective bias.

59
References
1 Shefner et al. Relationship between stimulus strength and the Cutaneous silent period. Muscle
& Nerve. 1993;16:278-282 .
2 Gilberto M. Manzano et al. A brief historical note on the classification of nerve fibers. Arq
Neuropsiquiatr 2008;66(1):117-119.
3 Vinik AI, Mehrabyan A. Diabetic Neuropathies. Med Clin North Am. 2004;88:947-999.
4 Grazia Devigili et al. The diagnostic criteria for small fiber neuropathy: from symptoms to
neuropathology. Brain. 2008;131: 1912-1925.
5 John D. Stewart et al. Distal small fiber neuropathy: results of tests of sweating and autonomic
cardiovascular reflexes. Muscle & Nerve. 1992;15:661-665
6 Jinny Tavee et al. Small fiber neuropathy: A burning problem. Cleveland Clinic Journal Of
Medicine.2009;76:297-305.
7 Leis AA et al. The silent period produced by electrical stimulation of mixed peripheral nerves.
Muscle Nerve 1991;14:1202–1208.
8 Inghilleri M et al. Silent period in upper limb muscles after noxious Cutaneous stimulation in
man. Electroencephalogr Clin Neurophysiol 1997;105:109–115.
9 Serrao M et al. Cutaneous afferents mediating the cutaneous silent period in the upper limbs:
evidences for a role of low-threshold sensory fibres. Clin Neurophysiol.2001;112:2007–2014.
10 Leis AA et al. The silent period in pure sensory neuronopathy. Muscle Nerve.1992;15:1345–
1348.
11 Mary Kay Floeter et al. Cutaneous silent periods. Muscle Nerve. 2003; 28: 391–401.
12 Leis AA.Cutaneous silent period. Muscle Nerve. 1998; 21: 1243–1245.

60
13
Shahani BT et al. Studies of the normal human silent period.New developments in
electromyography and clinical neurophysiology. Basel: Karger; 1973. p 589–602.
14 Uncini A et al. Silent period induced by cutaneous stimulation. Electroencephalogr Clin
Neurophysiol 1991;81:344–352
15 Leis AA et al. Nociceptive fingertip stimulation inhibits synergistic motoneuron pools in the
human upper limb. Neurology 2000;55:1305–1309.
16 Aramideh M et al. Brainstem reflexes: electrodiagnostic techniques, physiology, normative
data, and clinical applications. Muscle Nerve.2002;26:14–30.
17 Caccia M et al.Cutaneous reflexes in small muscles of the hand. J Neruol Neurosurg Psy.
1973;36:960-977.
18 Serrao M et al. L-Dopa decreases cutaneous nociceptive inhibition of motor activity in
Parkinson’s disease. Acta Neurol Scand 2002;105:196–201.
19 Pullman SL et al.Cutaneous electromyographic silent period findings in brachial dystonia.
Neurology 1996;46:503–508.
20 Stetkarova I et al. Cutaneous and mixed nerve silent periods in syringomyelia. Clin
Neurophysiol.2001;112:78–85.
21 Kaneko K et al. Cutaneous silent period in syringomyelia. Muscle Nerve.1997;20: 884–886.
22 Leis AA. Silent period studies and long latency reflexes.Comprehensive clinical
neurophysiology. Philadelphia: W. B. Saunders; 2000. p 295–306.
23 Sandbrink F et al. Cutaneous silent periods in abetalipoproteinemia.
MuscleNerve.1999;22:1324.
24 Nadir Ali Syed et al. Cutaneous silent periods in patients with fabry disease. Muscle Nerve.
2000; 23: 1179–1186.

61
25
Corsi FM et al. Electromyographic mixed nerve and cutaneous silent period in evaluating the
A-delta fibres in a patient with hereditary sensory-autonomic neuropathy. Funct
Neurol.2002;17:31–34.
26 Yong Seo Koo et al. Utility of the cutaneous silent period in the evaluation of carpal tunnel
syndrome.Clin Neurophysiol. 2010 Sep;121(9):1584-8.
27 M.J. Pablo et al. Function of A-delta fibres in carpal tunnel syndrome: A study using the
cutaneous silent period. Clinical Neurophysiology.2010 Oct:121(S1): S284
28 S.K. Aurora et al.Cutaneous silent period abnormalities in the carpal tunnel syndrome. Muscle
Nerve.1998; 21: 1213–1215.
29 Phalen GS.The carpal tunnel syndrome.Seventeen years experience in diagnosing and
treatment of six forty four hands.J Bone Joint Surg.1996;48:211-28.
30 Bongers FJ et al. Carpal tunnel syndrome in general practice (1987 and 2001): incidence and
the role of occupational and non-occupational factors. Br J Gen Pract. 2007:36–39.
31 Ashworth N. Carpal Tunnel Syndrome. http://www.medicine.com/pmr/topic21.htm.
32 . Keith MW et al. American Academy of Orthopaedic Surgeons Clinical Practice Guideline on
diagnosis of carpal tunnel syndrome. J Bone Joint Surg Am. 2009;91(10):2478–2479.
33 Isam Atroshi MD et al.Prevalence of Carpal tunnel syndrome in a general population.
JAMA.1999;282:153-158.
34 Padua L et al.Neurophysiological classification and sensitivity in 500 carpal tunnel syndrome
hands.Acta Neruol Scand.1997;96:211-17.
35 Levine DW et al. A self-administered questionnaire for the assessment of severity of
symptoms and functional status in carpal tunnel syndrome. Journal of Bone & Joint Surgery -
American Volume 1993, 75:1585-1592.

62
36
Jose C de Carvalho Leite et al. A systematic review of the psychometric properties of the
Boston Carpal Tunnel Questionnaire. BMC Musculoskeletal Disorders 2006, 7:78.
37 Uncini A et al.Sensitivity of three median to ulnar comparative tests in diagnosis of mild
carpal tunnel syndrome.Muscle Nerve.1993;16:1366-73.
38 American Association of Electrodiagnostic Medicine,American Academy of
Neurology,American Academy of Physical Medicine and Rehabilitation,Practice Parameter for
electrodiagnostic studies in carpal tunnel syndrome:Summar statement.Muscle
Nerve.2002;25:918-22.
39 Bland JDP. A neurophysiological grading scale for carpal tunnel syndrome. Muscle Nerve
2000;23:1280–3.
40 Svilpauskaite J, Truffert A, Vaiciene N, Magistris MR. Cutaneous silent period in carpal
tunnel syndrome. Muscle Nerve 2006a;33:487–93.
41 de Leonni Stanonik et al.The influence of age and sex on cutaneous silent periods. Clin
Neurophysiol.2010;121:S(1): S272.
42 Shefner JM, Logigian EL. Factors affecting mixed nerve and
cutaneous silent periods. Electroencephalogr Clin Neurophysiol 1996;98:10P.
43Eric L. Logigian et al. The cutaneous silent period is mediated by spinal
inhibitory reflex. Muscle Nerve.1999; 22: 467–472.
44 Fowler TJ, Danta G, Gilliatt RW. Recovery of nerve conduction after a pneumatic tourniquet:
observations on the hindlimb of the baboon. J Neurol Neurosurg Psychiatry.1972;35:638–647.
45 Yaman M, Uluduz D, Solak O, Pay G, Kiziltan ME. The cutaneous silent period in carpal
tunnel syndrome. Electromyogr Clin Neurophysiol.2007a;47:215–20.

63
ANNEXURE i
Proforma of Thesis
1. Identification information
1.1 Serial number -------------------------
1.2 Hospital number -------------------------
1.3 Age --------------------------
1.4. Gender -------------------------
1.5.Height (in cm.) --------------------------
2. Details of Carpal tunnel syndrome
2.1.Right or Left hand.
2.2.Duration of symptoms
2.3.Boston Questionnaire
2.3.1. Symptom severity scale
The following questions refer to your symptoms for a typical 24 hour period during the past
two weeks (circle one answer to each question)
i. How severe is the hand or wrist pain that you have at night?
1. I do not have hand or wrist pain that you have at night
2. Mild pain

64
3. Moderate pain
4. Severe pain
5. Very severe pain
ii. How often did hand or wrist pain wake you up during a typical night in the past two
weeks?
1. Never
2. Once
3. Two or three times
4. Four or five times
5. More than five times.
iii. Do you typically have pain in your hand or wrist during daytime?
1. I never had pain during the day.
2. I have mild pain during the day.
3. I have moderate pain during the day.
4. I have severe pain during the day.
5. I have very severe pain during the day.
iv. How often do you have hand or wrist pain during the daytime?
1. Never
2. Once or twice a day
3. Three to five times a day
4. More than five times a day.
5. The pain is constant

65
v. How long on average, does as episode of pain last during the daytime?
1. I never get pain during the day.
2. Less than 10 minutes
3. 10 to 60 minutes
4. Greater than 60 minutes
5. The pain is constant throughout the day.
vi. Do you have numbness (loss of sensation) in your hand?
1. No
2. I have mild numbness.
3. I have moderate numbness.
4. I have severe numbness.
5. I have very severe numbness.
vii. Do you have weakness in your hand or wrist?
1. No weakness
2. Mild weakness
3. Moderate weakness
4. Severe weakness
5. Very severe weakness

66
viii. Do you have tingling sensations in your hand?
1. No tingling
2. Mild tingling
3. Moderate tingling
4. Severe tingling
5. Very severe tingling
ix. How severe is numbness (loss of sensation) or tingling at night?
1. I have no numbness or tingling at night.
2. Mild
3. Moderate
4. Severe
5. Very severe
x. How often did numbness or tingling sensation wake you up during a
typical night during the last two weeks?
1- Never
2- Once
3- Twice to three times
4- Four to five times
5- More than five times

67
xi. Do you have difficulty with the grasping and use of small objects such as keys or pens?
1- No difficulty
2- Mild difficulty
3- Moderately difficulty
4- Severe difficulty
5- Very severe difficulty

68
2.3.2..Functional status scale
On a typical day during the past two weeks have hand and wrist symptoms caused you to have
any difficulty doing the activities listed below? Please encircle one number that best describes
your ability to do the activity.
Activity No
difficulty
Mild
difficulty
Moderate
difficulty
Severe
difficulty
Cannot do at all due to hand or
wrist symptoms
Writing 1 2 3 4 5
Buttoning
of clothes
1 2 3 4 5
Holding a
book
while
reading
1
2
3
4
5
Gripping a
telephone
handle
1
2
3
4
5
Opening
of jars
1 2 3 4 5
Household
chores
1 2 3 4 5
Carrying
of grocery
bags
1
2
3
4
5
Bathing
and
dressing
1
2
3
4
5

69
3.1.Neurophysiological grading of Carpal tunnel syndrome.
Severity
grade
Sensory
conduction
velocity
SNAP Motor
conduction
velocity
Motor
potential
amplitude
0 Normal No neurophysiological abnormality
1 Very mild Above tests are normal
Detected by sensitive tests (Internal comparision studies)
2 Mild Slowing Preserved Normal Preserved
3 Moderate Slowing Preserved >4.5 - <6.5ms Preserved
4 Severe Absent >4.5 - <6.5ms Preserved
5 Very severe Absent >6.5ms Preserved
6 Extremely
severe
Sensory and motor potentials effectively unrecordable (surface
motor potential from APB <0.2mV amplitude)
3.2.Cutaneous silent period
1. Elicitable
a. Yes
b. No
2. If Yes
a. Latency
b. Duration
c. Endpoint

70