Embed Size (px)
Citation preview

VOL 3 No 9 SEPTEMBER 2016
Page �1
“DOCENDO DECIMUS”
DCMC Emergency Department Radiology Case of the MonthThese cases have been removed of identifying information. These cases are intended for peer review and educational purposes only.
Welcome to the DCMC Emergency Department Radiology Case of the Month!
In conjunction with our pediatric radiology specialists from ARA, we hope you enjoy these monthly radiological highlights from the case files of the Emergency Department at DCMC. These cases are meant to highlight important chief complaints, cases, and radiology findings that we all encounter every day.
If you enjoy these reviews, we invite you to check out Pediatric Emergency Medicine Fellowship Radiology rounds, which are offered quarterly and are held with the outstanding support of the pediatric radiology specialists at Austin Radiologic Association.
If you have and questions or feedback regarding the Case of the Month format, feel free to email Robert Vezzetti, MD at [email protected].
This Month: We’ve covered foreign body ingestions before, but batteries and coins are not the only objects that can pose a health hazard to children. In this issue, we look at a few cases that demonstrate non radio-opaque ingestions.
Conference Schedule: September 2016
6th - Conflict Resolution………..…..Drs Vezzetti and Friesen
7th 9:15 - The IRB……………….……………………….Dr Allen 10:15 - Rheumatologic Emerg..…Drs Rencher and Irwin 11:15 - Musculoskeletal Disorders 12:15 - Fellowship Feedback……………..…PEM Fellows
9th - PEM Fellow Interview Day!
14th 9:15 - Patient Safety…………..……………………Dr Iyer 10:15 - Vaccines/Wound Prophylaxis..……Dr Whitaker 11:15 - Empiric Antibiotics…………………..…..Dr Allen
16th - PEM fellow Interview Day!
21st 9:15 - Toxicology:Heavy Metals..Drs Earp and Schwartz 10:15 - EKG’s…………………..……Drs Gorn and Friesen 11:15 - EMS Part 1…………….………………….Dr Remick 12:00 - ED Staff Meeting
23rd - PEM Fellow Interview Day!
27th - Journal Club
28th 9:15 - M&M………………..……Drs Schwartz and Salinas 10:15 - Board Review………………….…………….Dr Earp 12:15 - Research Update…………………..…Dr Wilkinson
Simulations are held at the CEC at UMC Brackenridge.Lectures are held at DCMC Command Rooms 3&4.
Locations subject to change. All are welcome!

VOL 3 No 8 SEPTEMBER 2016
Page �2
Case 1: Kind of a slow summer in the ED this year, which is a nice change of pace. The relative quiet is interrupted by spikes of activity and today is no exception, as EMS brings you a child who was found playing with lighter fluid just prior to arrival. The EMS providers tell you that the mother saw the child drink the fluid (a quick sip, per the mother) and then he had a gagging episode, which his mother described as choking and gagging (hmm..). EMS further says that he has been fine the entire time during transport and in fact, has been extremely active. As they depart, you look at the Triage sheet and go to examine the patient. You find an very active child, who is running around laughing and yelling. He did stop long enough for the ED nurse to get vital signs: Temp 97.5 HR 110 RR 24 Sats 99% (Room Air). You can’t get a blood pressure because he won’t sit still long enough and, in fact, keeps ripping off the BP cuff. His exam is entirely unremarkable. His oropharyngeal examination is unremarkable, which moist membranes and no sign of erythema. He is in no respiratory distress and his lung fields are all clear. He has no abdominal tenderness and his neurologic exam is normal. Now what? Lighter fluid. This child has a normal examination and is asymptomatic. Does he need anything done? Will imaging help you determine if any harm has occurred with his encounter with the lighter fluid? What potentially can happen with lighter fluid ingestion? When will this kiddo stop running around the Emergency Department?
Case 2: Now you have a headache and go to find some Ibuprofen when the PEM Fellow comes to you with a Emergency Medicine Resident with another case. This one’s easy, you think, because it is a 12 month old male that swallowed a plastic coin. His mother saw the child with a coin in his mouth; she went to attempt to sweep the coin out of the child’s mouth without success, as he promptly swallowed it. He gagged per his mother, but seemed fine at first, but his mother noticed he was fussy and, when offered drink, he refused to take it. He was seen at an outside Free Standing Emergency Department where plain radiographs of his neck and chest, which did not demonstrate an obvious foreign body. Again, a drink was offered to the child and he refused to take it. This prompted his transfer to the Emergency Department. On arrival, you find a nontoxic child in no respiratory distress. He is slightly fussy, and wants nothing to do with you, but is not in respiratory distress. He is afebrile, HR 133 RR 30 BP 119/85 Sats 100 % on Room Air (he is crying during those vital signs). His oropharynx is clear but he does appear to be a little more droopy than normal per his mother. His lungs are clear. The rest of his exam is unremarkable. Your friendly DCMC Pediatric Radiologist reviewed the outside plain films, all normal. Does this child have a foreign body. What are the odds that a plastic coin will be visible on a radiograph? Do you offer oral fluids? Call surgery for endoscopy? Is there another imaging test that might help you?
Band-Aids were invented in the month of September.
George Eastman got his patent for the roll-film camera, in September of 1888 and the Eastman-Kodak company soon was off to becoming one of America's major corporations.
VOL 3 No 8 SEPTEMBER 2016
Page �3
Remember Mr Yuck? I sure do! Mr Yuck was conceived in 1971 and introduced in Pittsburg that year by Dr Richard Moriarty, a pediatrician and professor of Pediatrics at the University of Pittsburg School of Medicine. Dr Moriarty also founded the Pittsburg Poison Center and the National Poison Center Network. Traditional poison markings had a skull and crossbones (we’ve all seen that) and were felt by Dr Moriarty not to be appropriate for children, and some even suggested that the skull and crossbones conjured up images of adventurous pirates, as well as the mascot for sports teams (Pittsburg Pirates) and seen on cereal boxes of the day. During development there were pediatric focus groups who thought the green color was yucky, hence the name!
Some studies have suggested that Mr Yuck does not keep children away and in fact is appealing to them (Fergusson 1982 and Vernberg 1984). In daycare testing, though, Mr Yuck was rated as least appealing when compared to the skull and crossbones, as well as other symbols.
What’s the point? Well, for one thing, this is interesting trivia. More practically, though, is the national number for Poison Center advice is: 1-800-222-1222. This number will route a caller to the nearest regional Poison Control Center, 24 hours a day, 7 days a week. All parents should know this number, and physicians too! In addition to advice, the center can provide a medical provider with a Toxicologist if needed for management advice of the complex poisoned patient. This is a very valuable resource!
Mr Yuck is copyrighted by and property of Children’s Hospital of Pittsburg of UPMC.
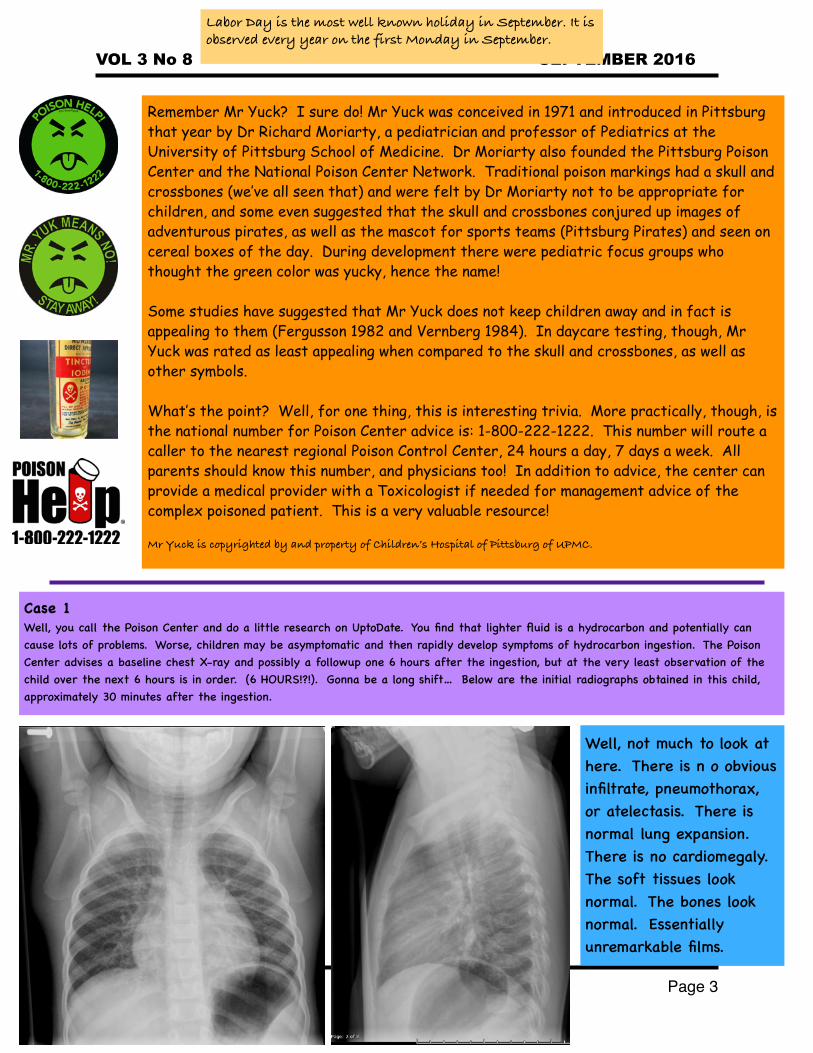
Case 1Well, you call the Poison Center and do a little research on UptoDate. You find that lighter fluid is a hydrocarbon and potentially can cause lots of problems. Worse, children may be asymptomatic and then rapidly develop symptoms of hydrocarbon ingestion. The Poison Center advises a baseline chest X-ray and possibly a followup one 6 hours after the ingestion, but at the very least observation of the child over the next 6 hours is in order. (6 HOURS!?!). Gonna be a long shift… Below are the initial radiographs obtained in this child, approximately 30 minutes after the ingestion.
Well, not much to look at here. There is n o obvious infiltrate, pneumothorax, or atelectasis. There is normal lung expansion. There is no cardiomegaly. The soft tissues look normal. The bones look normal. Essentially unremarkable films.
Labor Day is the most well known holiday in September. It is observed every year on the first Monday in September.

VOL 3 No 8 SEPTEMBER 2016
Page �4
Six hours have passed since you evaluated the rambunctious child who may or may not have drank some lighter fluid. He remains asymptomatic and he has tolerated oral fluids. You write his discharge order and that’s that..until the nurse comes to you and tells you that the child now has a fever of 101.5 and he seems a little tachypneic. Sure enough, you evaluate him and he is definitely tachypneic, with a respiratory rate of 50. Is this from the fever? And why does he have fever now?
You obtain a repeat films, which are on the right and below. Notice anything? The left lower lobe now has what appears to be airspace density (red arrows). What? Yep.
Given the history of this child’s drinking lighter fluid and then have a gagging/choking episode this is most likely aspiration pneumonitis. Additionally, the new tachypnea and fever highly suggest that is the case. Well, so much for the discharge plans. Now what?
There’s a very real concern that the child can decompensate quickly, and in fact has begun to decompensate right in front of your eyes in the emergency department. He needs to be admitted and observed for progression of symptoms. While he is maintaining his airway at this time, this could change and you certainly don’t want him at home if that happens.
So what’s in lighter fluid? Butane. Butane is a hydrocarbon, which, as people in health care know (especially the Emergency Department and Intensive Care Unit) can be really, really bad if ingested and/or aspirated. Remember organic chemistry? I don’t.But here is Butane for all you chemistry buffs out there.
What happened? See below.
Ancient Romans believed that September was watched over by Vulcan, the god of fire and volcanos; they believed this month was associated with earthquakes, fires, and volcanic eruptions!
Traditionally people did not wear white or seersucker clothes after Labor Day as it unofficially marked the end of summer.
VOL 3 No 8 SEPTEMBER 2016
Page �5
Case 2Well, oral fluids were offered to the child, who immediately tried to drink but could not, spitting up the fluid and looking uncomfortable when he tried to swallow. It’s pretty suspicious that this child has a foreign object in his esophagus. It’s not surprising that the plain films do not show the object..it’s plastic, which is pretty hard to see on a plain film. There are several courses of action that can be taken at this time.
1. Consult Pediatric Surgery: definitive diagnosis and treatment would be Esophagogastroduodenoscopy, which would visualize and remove the FB. But this requires anesthesia and it would be great to know if this procedure is necessary.
2. Non-contrast CT Scan of the Neck: this would definitely see a foreign body, but requires radiation. Still, it could be valuable imaging.
3. Esophagram: not as much radiation as a CT, but requires po contrast and the child may not tolerate drinking it well. Also, it might miss a foreign body. If he drinks the contrast material without difficulty and the study is normal, then the likelihood of a foreign body is pretty low.
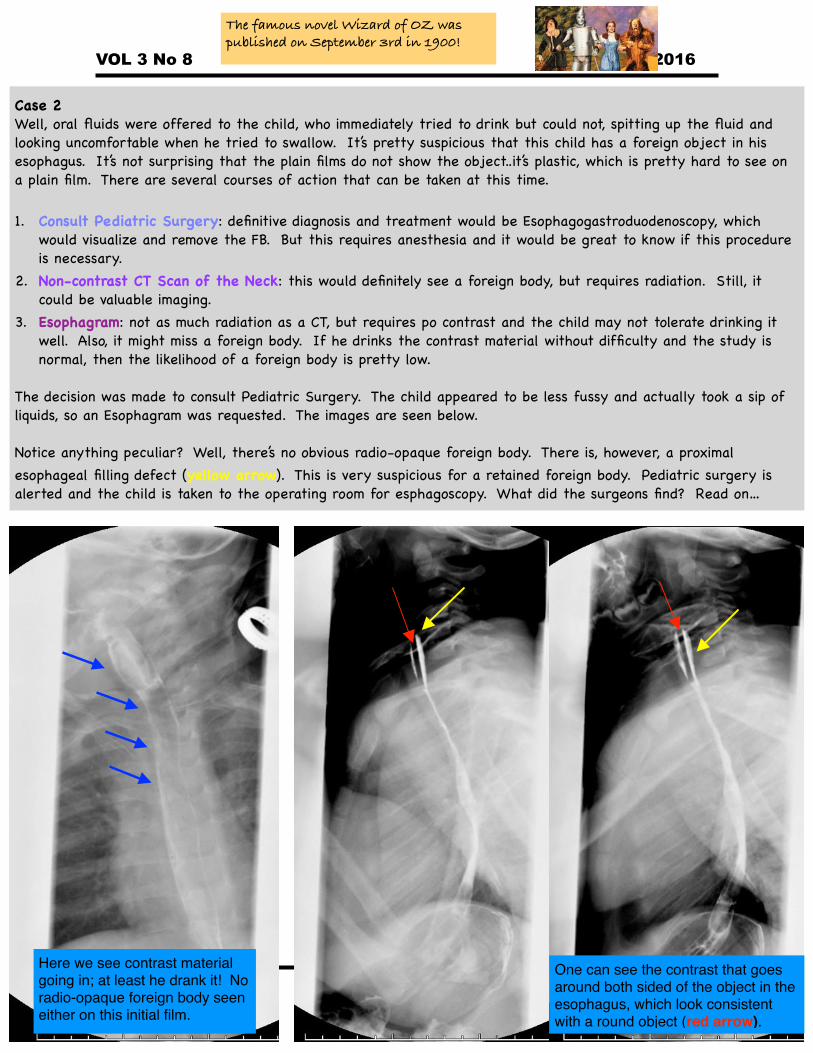
The decision was made to consult Pediatric Surgery. The child appeared to be less fussy and actually took a sip of liquids, so an Esophagram was requested. The images are seen below.
Notice anything peculiar? Well, there’s no obvious radio-opaque foreign body. There is, however, a proximal esophageal filling defect (yellow arrow). This is very suspicious for a retained foreign body. Pediatric surgery is alerted and the child is taken to the operating room for esphagoscopy. What did the surgeons find? Read on…
One can see the contrast that goes around both sided of the object in the esophagus, which look consistent with a round object (red arrow).
Here we see contrast material going in; at least he drank it! No radio-opaque foreign body seen either on this initial film.
The famous novel Wizard of OZ was published on September 3rd in 1900!

VOL 3 No 8 SEPTEMBER 2016
Page �6
Hydrocarbon IngestionThese substances account for a small percentage of exposures in children (roughly 2%), but their effects can be devastating. Children are often accidentally exposed to theses substances, which are often improperly stored. Adolescents are often exposed intentionally, though inhalation activities. Aspiration hazard is determined by:1. Volatility (the greater, the more likelihood of aspiration).2. Surface Tension (the lesser, the more likelihood of aspiration).3. Viscosity (lower viscosity allows the substance to go deeper
into the bronchial tree).
Systemic ToxicityThe effects of hydrocarbon toxicity is primarily determined by the amount of the substance absorbed.
PathophysiologyAspiration of hydrocarbons affects the respiratory system and CNS. The pulmonary injury seen with aspiration occurs by direct impact, causing chemical pneumonitis. One can see necrotizing pneumonia in severe exposures. Fever is commonly seen in these patients due to the systemic inflammatory response (as was seen in our patient). This temperature elevation can be seen within hours of aspiration (also s seen in our case). Hydrocarbons are very laid soluable, so they can penetrate the CNS quite readily.
Clinical EffectsRespiratory - initially may be asymptomatic but rapid progression to respiratory failure is not uncommon.CNS - Somnolence, lethargy, seizure, headache, ataxia.Cardiovascular - arrhythmias and myocardial dysfunction.GI - due to direct irritation of the upper and lower GI tract; extreme exposures can cause ulceration.Hematologic - leukocytosis is not uncommon. In extreme exposures, coagulopathies can occur.
ManagementThis depends on the degree of exposure and symptomatology of the patient. ABC’s first, always, so a child in severe respiratory distress should undergo immediate intubation. Asymptomatic - monitoring for 6 hours with pulse oximetry; a chest X-ray should be obtained between 4-6 hours after exposure. Discharge is appropriate for these patients.Mild - Moderate Symptoms - these children should undergo very careful monitoring and are at high risk for clinical decompensation. A chest X-ray should be obtained and followed (especially if there are pulmonary symptoms) with serial films.Severe Symptoms - Advanced airway management, IV fluids, seizure management, admission to the PICU for close monitoring.
Types of HydrocarbonsAromatic - benzene, used in solvents, glues, paint.Aliphatic - petroleum, used in gas, kerosene, lighter fluid.Halogenated - industrial solvents (chlorides).Terpene - turpentine and pine oil.Aspiration risk is highest with Aliphatic and Terpene hydrocarbons.
Decontamination - remember to decontaminate externally with vigorous irrigation. Don’t forget to protect your team with universal precautions! There are no effective GI decontamination techniques; do NOT induce emesis. Activated charcoal is NOT effective, unless there is very large amounts of aliphatic compounds. Gastric lavage with nasogastric tube as a decontamination technique is NOT recommended, as this may increase the risk for aspiration, unless the amount ingested is exceedingly large. Consultation with a toxicologist is always helpful!
This person was siphoning diesel.
This 9 month old ingested kerosene. Note the bilateral lower airspace disease; the pattern looks very similar to edema.
Learningradiology.com
“My favorite poem is the one that starts ‘Thirty days hath September’ because it actually tells you something” (Groucho Marx)

VOL 3 No 8 SEPTEMBER 2016
Page �7
Swallowed foreign bodies that get stuck in the esophagus are nothing new and will continue to be seen in children from now until forever. In past issues, we have discussed coins and button batteries (among other objects). Removal is accomplished using:1. Flexible Endoscopy 2. Rigid Endoscopy - mist useful for sharp objects or objects
located in the proximal esophagus.
Here’s a fish bone that’s stuck.radiopaedia.org
Richard Saunders, the 17th century English astrologer and physician, said it was good to eat pomegranates and goats’ milk in September.
Chicken Bone!
Pen!radiopaedia.org
Most foreign bodies that children swallow as radio-opaque (some studies quote 65% or greater). But, there are times where this may not be the case. Plain films are always a good idea, and you can attempt decubitus views as well if you suspect an airway foreign body. CT or esophagram are also options, as is consulting pediatric surgery (See above). Some studies suggest that decubitus films do not add much to the evaluation of a child with possible foreign body aspiration.The image below shows lateral decubitus film. Note the left side remains well-aerated despite the child laying on that side. This is indicative of air trapping and the raises concerns of a foreign body.

VOL 3 No 8 SEPTEMBER 2016
Page �8
References 1. Vernberg K, Culver-Dickinson P, Spyker DA. The deterrent effect of poison-warning stickers. American Journal of Diseases of Children. 1984. 138: 1018. 2. Fergusson DM, Horwood LJ, Beautrais AL, Shannon FT. A controlled field trial of a poisoning prevention method. Pediatrics 1982. 69: 515. 3. Joliff HA, Fletcher E, Roberts JK, et al. Pediatric hydrocarbon-related injuries in the United States: 2000-2009. Pediatrics. 2013. 131:1139. 4. Tormoehlen LM, Tekulve KJ, Manages KA. Hydrocarbon toxicity: A review. Clin Toxicol (Phila). 2014. 52:479. 5. Gummin DD, Hryozuk DO. Hydrocarbons. In: Goldfrank’s Toxicologic Emergencies, 8th Edition, Flomenbaum NE, Goldfrank LR, Hoffman RS, et al. (Eds). McGraw-Hill. New York. 2006. 1429. 6. Venkatnarayan K, Madan K, Walia R, et al. Diesel siphon’s lung: Exogenous lipoid pneumonia following hydrocarbon aspiration. Lung India. 2014. 31:63. 7. Das D, May G. Best evidence topic report. Is CT effective in cases of upper oesophageal fish bone ingestion?. Emerg Med J. 2007;24 (1): 48-9. 8. Kramer RE, Lerner DG, Lin T, et al. Management of ingested foreign bodies in children: a clinical report of the NASPGHAN Endoscopy Committee. J Pediatric Gastroenterol Nutr. 2015. 60:562. 9. Assefa D, Amin N, Stringel G, Dozor AJ. Use of decubitus radiographs in the diagnosis of foreign body aspiration in young children. Pediatric Emerg Care. 2007;23(3):154.
Teaching Points1. Hydrocarbon ingestions/aspiration are rare, but clinically important. They are very diverse and
found in a variety of household chemicals, including paint, gas, glues, lighter fluid, and turpentine (painters beware).
2. Toxicity depends on the type of hydrocarbon ingested. Signs of systemic toxicity include CNS and cardiac symptoms.
3. Gastric emptying procedures are generally not recommended in hydrocarbon ingestions. Vomiting should not be induced and activated charcoal is generally not recommended or effective, unless there is co-ingestion of a compound that is absorbed by activated charcoal.
4. Pulmonary status with hydrocarbon aspiration can vary widely and patients should be observed for 6 hours following exposure. A baseline chest X-ray should be obtained, and if a child is asymptomatic, then a chest X-ray prior to discharge is recommended.
5. Treatment is supportive and fever is common; antibiotics and steroids are not indicated. Don’t forget the Poison Center Number: 1-800-222-1222.
6. Suspected non-radio-opaque foreign bodies can be identified often by non contrast CT or esophagram. Lateral decubitus views may be helpful as well for airway foreign bodies. Consultation with Pediatric Surgery is recommended in any patient suspected of harboring a non-radio-opaque foreign body.
Case ResolutionsCase 1: This child was exhibiting signs of a hydrocarbon toxidrome and was admitted for overnight observation. Symptomatic care was initiated for his fever, and he did not require prolonged supplemental oxygen. He did not progress further and after a little more than 24 hours in the hospital, he was afebrile, in no respiratory distress, and exhibited no other signs of intoxication. He was discharged home and hopefully will avoid further hydrocarbon encounters in the future. Of note, his mother was given information regarding safety measure shoe could take in her home as well as the number to the Poison Center.Case 2: This child was taken to the operating room for esophagoscopy. At that time, a plastic coin was visualized in the proximal esophagus and easily removed. There did not appear to be any further foreign bodies and no obvious injury to the esophagus. He was discharged and his parents were given tips on making their home as child safe as possible.
When the British changed from the Julian calendar to the Gregorian calendar in 1752, they needed to adjust some days to get the seasons aligned with the months. They took 11 days from the month of September jumping directly from September 3rd to the 14th. Now it's as if the days between September 3 and 13 during 1752 never happened!





























