Embed Size (px)
Citation preview

ORIGINAL ARTICLE
Day One Talk: parent preferences when learningthat their child has cancer
Rachel M. Kessel & Michael Roth & Karen Moody &
Adam Levy
Received: 27 November 2012 /Accepted: 30 May 2013# Springer-Verlag Berlin Heidelberg 2013
AbstractPurpose The discussion that occurs between a pediatriconcologist and a family when they first learn about theirchild’s new diagnosis of cancer is known as the “Day OneTalk.” Few studies have addressed parent preferences whenlearning that their child has been diagnosed with cancer. Theobjective of this study is to assess what information parentsof children with newly diagnosed cancer believe is importantto learn during the Day One Talk.Methods In this cross-sectional study, a survey tool based onexpert opinion was created to assess parents’ views of com-ponents of the Day One Talk including its content, length,and setting, as well as whether the child should be present forthe initial talk and which staff should be present for the talk.Results Sixty-two parents of children with newly diagnosedcancer participated. Ninety-seven percent believed that theDay One Talk is extremely important. Ninety percent believedthat the word “cancer” should be used during the Day OneTalk. Seventy-seven percent believed that the pediatric oncol-ogist should provide specific numbers regarding cure rates forthe patient’s diagnosis. Eighty-four percent of parents do notbelieve that children younger than 14 should be present.Conclusions These results suggest that parents of childrenwith cancer have certain preferences regarding the Day OneTalk. When conducting the Day One Talk, providers shouldelicit parent preferences regarding these issues in order tobest meet families’ needs.
Keywords Day One Talk . Cancer diagnosis .Newdiagnosis .
Pediatric cancer . Delivering bad news
Background
Every year more than 17,000 children in the USA are diag-nosed with cancer [1]. Pediatric oncologists have the difficultduty to discuss these life-changing diagnoses with theirpatients and families. The initial communications in whicha child and family learns about the child’s new diagnosis ofcancer is known as the Day One Talk.
The time when families first learn that their child has beendiagnosed with cancer is often described as devastating andoverwhelming [2, 3]. In addition to delivering vital newsabout the patient’s diagnosis, the Day One Talk sets the stagefor the relationship between the physician, the patient, andthe family. Higher patient satisfaction with the initial talk canlead to improved trust as well as an easier adjustment to-wards accepting the diagnosis and treatment [4, 5].
Studies and reviews in the pediatric literature and adultoncology literature highlight the importance of a number ofcomponents of the initial talk including the setting of thetalk, the content of the talk, and the amount of supportoffered by the physician [6–25]. However, evidence-basedliterature on the delivery of bad news is significantly lackingin quality and number [11, 17]. In addition, there is currentlyvery limited data in the pediatric oncology literature address-ing how parents prefer to learn of their child’s diagnosis ofcancer. One prior study 25 years ago showed that parents andpediatric oncologists viewed similar information, such as thediagnosis, prognosis, and therapy, as critical to discuss dur-ing the initial discussion of a new diagnosis of leukemia [12].However, there are no studies assessing the importance of thevarious components of the Day One Talk for parents ofpediatric patients with different malignancies. In addition,the treatment and prognosis of many childhood cancers havechanged significantly in the last few decades, and the contentof the Day One Talk may be very different in this era of newtherapeutics and improved survival rates for many childhood
R. M. Kessel (*) :M. Roth :K. Moody :A. LevyDepartment of Pediatrics, Division of Hematology/Oncology,The Children’s Hospital at Montefiore, 3415 Bainbridge Ave.,Bronx, NY 10467, USAe-mail: [email protected]
Support Care CancerDOI 10.1007/s00520-013-1874-8

cancers. We conducted this study to determine parent pref-erences when learning that their child is diagnosed withcancer.
Methods
Design
This is a cross-sectional survey. It was approved by expedit-ed review by the Internal Review Board and signed consentwas waived.
Population and recruitment
Parents of children from birth to 21 years who were diag-nosed with cancer within the past 6 months and requiredchemotherapy for at least 3 months were invited in toparticipate in the study. The study was conducted in anurban children’s hospital in Bronx, NY, USA from 2009to 2010. Parents of children who did not require at least3 months of chemotherapy were excluded from the studybecause it is likely that the Day One Talk with these fam-ilies is conducted differently than the Day One Talk forpatients who require more intensive treatment. Parents ofchildren with low-grade CNS tumors were excluded fromthe study.
Eligible participants were approached in the outpatientpediatric oncology clinic and were offered to participate inthe study. Participants must have been English- or Spanish-speaking as the survey tool was available in these twolanguages. Two parents declined participation in the study.
Questionnaire
Participants were asked to complete a questionnaire regard-ing their preferences when learning that their child wasdiagnosed with cancer. The questionnaire was designedby an expert panel consisting of two pediatric oncologists,a pediatric palliative care specialist, and a pediatric psy-chologist after performing an extensive literature review onthe delivery of bad news in the adult and pediatric popula-tions [2–31]. The questionnaire elicited demographic infor-mation and focused on parents’ views of various compo-nents of the Day One Talk including its content, length, andsetting, as well as whether the child should be present forthe initial talk and which staff should be present for the talk.The questionnaire consisted of 41 questions using amultiple-choice format or Likert Scale response and oneopen-ended question requiring write-in responses. TheFlesch Reading Ease score was 79.8, and the Flesch–Kincaid reading level was 4.7. The questionnaire was avail-able in English and Spanish.
Statistical analysis
Qualitative and quantitative data were collected. Descrip-tive statistics were generated for demographic characteris-tics and all variables. Means, medians, standard deviations,and ranges were computed for continuous variables andfrequencies for categorical variables. Qualitative data wereexpressed descriptively.
Results
A total of 62 parents of children with newly diagnosed cancercompleted the study, with two parents refusing participation(Table 1). This includes surveys for 56 individual patients; forsix patients, both parents completed the survey. The meantime from diagnosis until questionnaire completion was 2-months. Diagnoses included leukemia (57.6 %), sarcoma(25 %), lymphoma (10 %), CNS tumor (6.7 %), and germcell tumor (1.7%). Two parents omitted their child’s diagnosisfrom the questionnaire. Participants represented the patientpopulation of an urban children’s hospital in Bronx, NY,USA. Participants described themselves as Hispanic (64.5 %)or Black (21 %) and 49.2 % described their highest level ofeducation as high school. Over 50 % of parents stated that theywere told that their child was likely to be cured with treatment.Approximately 5 % of parents stated that they were told thattheir child was not likely to be cured with treatment.
Importance of the talk and satisfaction with the talk
Nearly all parents (97 %) believed that the Day One Talk isextremely important. Parents were asked to consider the DayOne Talk when they were told of their child’s cancer diag-nosis and to rate their satisfaction with the talk on a five-point Likert Scale, ranging from extremely satisfied to notsatisfied. A chi-square test was used to test the associationbetween satisfaction with the talk and prognosis. No associ-ation was found. Fifty-six percent of parents were extremelysatisfied with the talk.
Logistics of the talk
Eighty-seven percent of parents want to be told in advancewhen the first talk will take place. Parents were asked howlong the first talk should be, with responses from less than10 min to more than 2 h. Sixty-seven percent of parentsindicated that it should last between 30 min and 1.5 h and30 % state that it should last less than 30 min. Parents didnot have a preference for the location of the talk, as long asprivacy was ensured (Table 2).
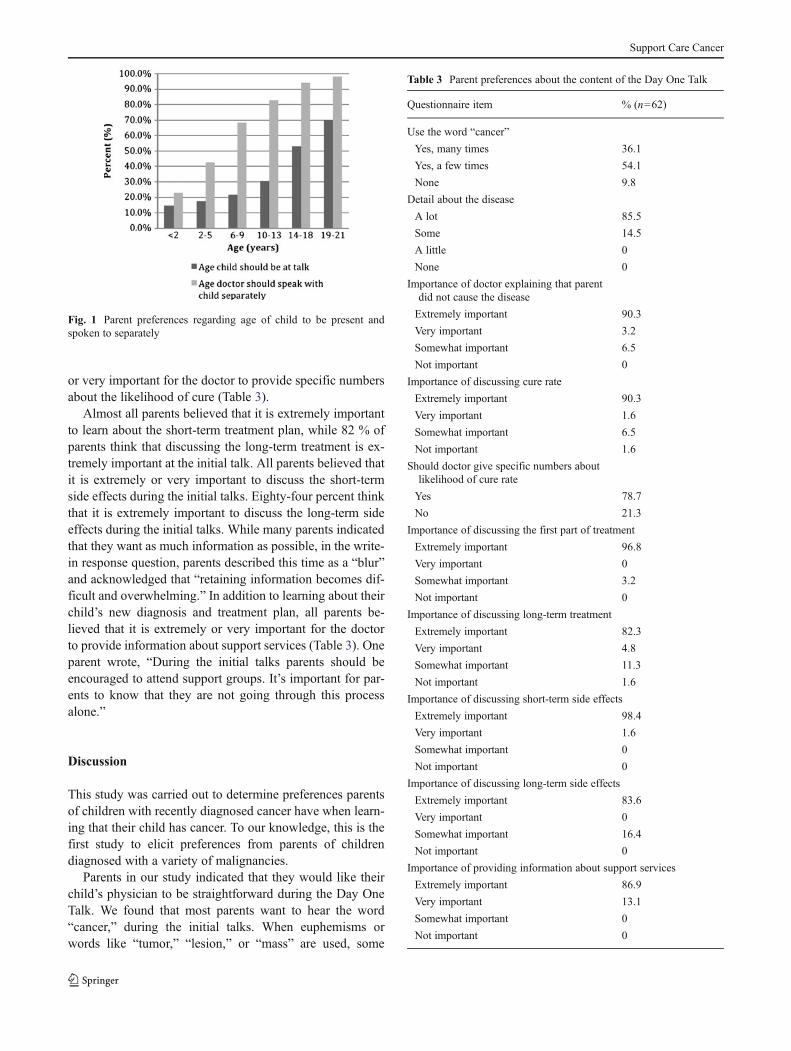
Eighty-four percent of parents do not believe that childrenyounger than 14 should be at the Day One Talk. However,
Support Care Cancer

the majority of parents believed that the oncologist shouldspeak with children older than 5 shortly after (Fig. 1). Parentswere evenly split on their preference for whether close fam-ily members should be at the talk. Seventy-five percent ofparents indicated that the social worker should be present.One parent suggested that physicians “introduce the fullteam if possible so parents aren’t left confused by differentdoctors giving different information.”
Eighty-four percent of parents believed that it is extremelyor very important to write down what the doctor says duringthe talk. Ninety percent of parents believed that it is extreme-ly or very important for the doctor to provide written infor-mation on their child’s diagnosis. All parents believed that itis extremely or very important for the doctor to provideenough time for questions to be answered (Table 2). Oneparent emphasized that “doctors need to be accessible toaddress questions and concerns.”
Content of the talk
Ninety percent of parents believed that the word “cancer”should be used during the Day One Talk and 86 % of parentswant to hear a lot of details about their child’s disease.Almost all parents responded that it is important for thedoctor to explain that the parents did nothing to cause thedisease. Ninety-two percent think that it is extremely or veryimportant for the doctor to discuss the cure rate and morethan three-quarters of respondents think that it is extremely
Table 1 Baseline characteristics of participants
Characteristic % (n=62)
Age (mean, range) 5.5 (2–20)
Ethnicity
Hispanic 64.5
Black 21
Caucasian 9.7
Asian 1.6
Other 1.6
Education level
Elementary school 1.7
Middle school 6.8
High school 49.2
College 27.1
Graduate school 15.3
Religious
Extremely religious 43.5
Very religious 11.3
Somewhat religious 38.7
A little religious 0
Not religious 6.5
Type of cancer
Leukemia 56.7
Sarcoma 25
Lymphoma 10
CNS tumor 6.7
Germ cell tumor 1.7
Chance of cure
Told likely to be cured 55.7
Told may be cured 36.1
Told not likely to be cured 4.9
Did not discuss chance of cure 3.3
Table 2 Parent preferences about logistics of the Day One Talk
Questionnaire item % (n=62)
Advanced notice about talk
Yes 86.7
No 13.3
Location within hospital for talk
Conference room 46.8
Patient room 3.2
Either, as long as private 50
Location within clinic for talk
Clinic room 8.1
Doctor’s office 35.5
Either, as long as private 56.5
Length of initial talk
<10 min 6.7
10–30 min 23.3
30 min–1 h 46.7
1–1.5 h 20
1.5–2 h 1.7
>2 h 1.7
Close family to be present
Yes 49.2
No 50.8
Support staff to be present
Social worker 75
Psychologist 54.7
Child life 51.5
Nurse 40.2
Importance of writing what doctor says
Extremely important 80.6
Very important 3.2
Somewhat important 14.5
Not important 1.6
Importance of doctor providing written information on diagnosis
Extremely important 88.5
Very important 1.6
Somewhat important 4.9
Not important 4.9
Support Care Cancer
or very important for the doctor to provide specific numbersabout the likelihood of cure (Table 3).
Almost all parents believed that it is extremely importantto learn about the short-term treatment plan, while 82 % ofparents think that discussing the long-term treatment is ex-tremely important at the initial talk. All parents believed thatit is extremely or very important to discuss the short-termside effects during the initial talks. Eighty-four percent thinkthat it is extremely important to discuss the long-term sideeffects during the initial talks. While many parents indicatedthat they want as much information as possible, in the write-in response question, parents described this time as a “blur”and acknowledged that “retaining information becomes dif-ficult and overwhelming.” In addition to learning about theirchild’s new diagnosis and treatment plan, all parents be-lieved that it is extremely or very important for the doctorto provide information about support services (Table 3). Oneparent wrote, “During the initial talks parents should beencouraged to attend support groups. It’s important for par-ents to know that they are not going through this processalone.”
Discussion
This study was carried out to determine preferences parentsof children with recently diagnosed cancer have when learn-ing that their child has cancer. To our knowledge, this is thefirst study to elicit preferences from parents of childrendiagnosed with a variety of malignancies.
Parents in our study indicated that they would like theirchild’s physician to be straightforward during the Day OneTalk. We found that most parents want to hear the word“cancer,” during the initial talks. When euphemisms orwords like “tumor,” “lesion,” or “mass” are used, some
Fig. 1 Parent preferences regarding age of child to be present andspoken to separately
Table 3 Parent preferences about the content of the Day One Talk
Questionnaire item % (n=62)
Use the word “cancer”
Yes, many times 36.1
Yes, a few times 54.1
None 9.8
Detail about the disease
A lot 85.5
Some 14.5
A little 0
None 0
Importance of doctor explaining that parentdid not cause the disease
Extremely important 90.3
Very important 3.2
Somewhat important 6.5
Not important 0
Importance of discussing cure rate
Extremely important 90.3
Very important 1.6
Somewhat important 6.5
Not important 1.6
Should doctor give specific numbers aboutlikelihood of cure rate
Yes 78.7
No 21.3
Importance of discussing the first part of treatment
Extremely important 96.8
Very important 0
Somewhat important 3.2
Not important 0
Importance of discussing long-term treatment
Extremely important 82.3
Very important 4.8
Somewhat important 11.3
Not important 1.6
Importance of discussing short-term side effects
Extremely important 98.4
Very important 1.6
Somewhat important 0
Not important 0
Importance of discussing long-term side effects
Extremely important 83.6
Very important 0
Somewhat important 16.4
Not important 0
Importance of providing information about support services
Extremely important 86.9
Very important 13.1
Somewhat important 0
Not important 0
Support Care Cancer

families may fail to understand that these words mean cancer[2]. In addition, the word cancer may have different mean-ings to different families, so it is important for physicians toascertain what families understand about the diagnosis andwhat this diagnosis means for their child [2].
When learning of a new diagnosis, families may irratio-nally blame themselves for something they did or did not dowhich they believe may have caused the illness [21]. Manyfamilies experience guilt for not addressing their child’ssymptoms at an earlier time point. It is important for thedoctor to communicate to families that there is nothing theydid or did not do to cause their child to become sick.
Almost all parents wanted their doctor to provide specificnumbers regarding the likelihood of cure. This is consistentwith findings in previous studies. In a cross-sectional studyeliciting preference for prognostic information from parentsof cancer patients, Mack et al. found that the majority ofparents (87 %) desired as much information as possibleabout prognosis and 85 % preferred numerical expression.Even while approximately one-third of parents found theinformation about prognosis to be extremely or very upset-ting, those parents were even more likely to want additionalinformation about prognosis [15]. In a systematic review ofadult oncology literature, researchers concluded that patientsrate being given prognostic information as both importantand necessary [27]. However, many patients preferred for thephysician to inquire if they actually want to hear prognosticinformation and what type of information they prefer, such asprobabilities of cure, survival rates, and general expectedoutcome of the disease [29, 31]. In a study by Kaplowitzet al., 352 patients were asked whether they would like to begiven a “qualitative prognosis” or a “quantitative prognosis”and found that 80 % preferred a qualitative prognosis butonly half wanted a quantitative estimate [29]. Similarly,Mack et al. suggested asking parents if they are “numberpeople” to tailor the information provided; other familiesmay be satisfied with words that convey a sense of likelihoodof cure [2, 28]. Additionally, the language of written infor-mation should be carefully chosen. One study found thatpatients preferred for the written prognostic information tobe presented using positively framed language in terms ofsurvival probabilities as opposed to chances of mortality[26]. We recommend eliciting from parents their preferencefor receiving information regarding the likelihood of cure.
In our survey, parents indicated that they want to learn a lotabout their child’s diagnosis, treatment, and side effects in thefirst few talks. Similarly, Mack et al. found that 91 % ofparents wanted as much information as possible about theirchild’s diagnosis and treatment [15]. However, in the write-inresponse question of our survey, parents also acknowledgedtheir limitation in retaining too much information at once. Oneparent indicated that “it is hard to soak in all of the informationin the first few talks,” and another parent described this time as
“a blur.” A third parent advised physicians to expect to repeatinformation to the family “since a level of shock occurs andretaining information becomes difficult and overwhelming.”This phenomenon resonates with the literature on the deliveryof bad news within cancer as well as in other fields. Eden et al.conducted parental interviews 3 months after a child’s cancerdiagnosis and found that the emotional state of the parentdetermines his or her ability to hear and comprehend infor-mation given [32]. The authors emphasized the need forrepetition and clarification until parents are emotionally ableto hear, accept, and comprehend the news. They suggestedwritten material, taped interviews, and videos to assist in theprocess. In another study, one-third of parents of children withnewly diagnosed cystic fibrosis felt that they had understoodand retained less than half of what the doctor told theminitially about the diagnosis [13]. Furthermore, in a surveyof parents of newly diagnosed cancer patients and oncologists,Greenberg et al. found that oncologists considered it “essen-tial” to acknowledge to parents that they will retain littleinformation from the initial talk [12]. Since another findingin our survey was that most families wanted to write downwhat physicians say, perhaps providing the family with paperand a pen would be appropriate and help with retention.
In coordinating the Day One Talk, physicians often have todecide who should be present. Given that preferences varyamong families, physicians should elicit each family’s prefer-ences prior to the talk so as to respect their wishes. In oursurvey, half of parents thought that other family membersshould be present and varied amongwhich support staff shouldbe present. Most parents thought that children younger than14 years should not be present during the talk and preferred forthe physician to speak with the child separately. When childrenare not included initially, our practice is to discuss their diag-nosis at a developmentally appropriate level soon after withtheir parents present. Interestingly, in our survey, only half ofparents thought that children aged 14–18 and 70 % of parentsthought that children aged 19–21 should be present for the talk.It must be acknowledged that local laws regarding children’slegal rights should be adhered to. For example, in the USA,patients ≥18 years have a legal right to their medical informa-tion, while in other countries, the age of legal consent isyounger. Patients’ consentmust be obtained in order to excludethem from the discussions. Excluding adolescents in the dis-cussion leads them to assume that the information they laterreceive is not completely honest and that the actual news aboutdiagnosis and treatment is worse than what they were told. Inaddition, including teenagers from the start will help to engagethem in their own care [2]. Physicians must balance familialrequests with legal obligations and the understanding that it istypically not in the best interest of adolescents to shield themfrom learning of their diagnosis.
A potential limitation of our survey is recall bias. Whilethe mean time of survey completion was 2 months following
Support Care Cancer

diagnosis, some parents were surveyed up to 6 months fol-lowing their child’s diagnosis. They were asked to considerretrospectively what they thought was essential to know attime of diagnosis. Their responses were potentially influencedby their child’s specific experiences during the course of theillness to date. While recognizing this limitation, it may bechallenging to survey families immediately after the talk atsuch an emotionally stressful time. Another potential limita-tion is that we conducted our study at a single institution in apoor urban environment and it is unclear to what extentparental preferences differ by socioeconomic backgrounds,education levels, and support networks.
Conclusions
The Day One Talk establishes the relationship between thephysician and family and often sets the tone for the course tofollow. Eliciting and understanding families’ preferences willenable physicians to tailor the Day One Talk specifically foreach family and likely increase their satisfaction with the talk.
Conflict of interest Authors have no financial relationships to de-clare. Authors have full control of all primary data and agree to allowthe journal to review their data if requested.
References
1. Jemal A, Siegel R, Ward E, Murray T, Xu J, Thun MJ (2007)Cancer statistics. CA Cancer J Clin 57:43–66
2. Mack JW, Grier HE (2004) The Day One Talk. J Clin Oncol22:563–566
3. Oshea J, Smith O, O’Marcaigh A, McMahon C, Geoghegan R,Cotter M (2007) Breaking bad news—parents’ experience of learn-ing that their child has leukaemia. Ir Med J 100:588
4. Ptacek JT, Ptacek JJ (2001) Patients’ perceptions of receiving badnews about cancer. J Clin Oncol 19:4160–4164
5. Wooley H, Stein A, Forrest GC, Baum JD (1989) Imparting thediagnosis of life threatening illness in children. BMJ 298:1623–1626
6. Ablon J (2000) Parents’ responses to their child’s diagnosis ofneurofibromatosis. Am J Med Genet 93:136–142
7. Byrnes AL, Berk NW, Cooper ME, Marazita ML (2003) Parentalevaluation of informing interviews for cleft lip and/or palate.Pediatrics 112:308–313
8. Chanock S (2001) Reflections on events surrounding the time ofdiagnosis in pediatric oncology. J Pediatr Hematol Oncol 23:211–212
9. Fallowfield L, Jenkins V (2004) Communicating sad, bad, anddifficult news in medicine. Lancet 363:312–319
10. Garwick AW, Patterson J, Bennett FC, Blum RW (1995) Breakingthe news. How families first learn about their child’s chroniccondition. Arch Pediatr Adolesc Med 149:991–997
11. Girgis A, Sanson-Fisher RW (1995) Breaking bad news: consensusguidelines for medical practitioners. J Clin Oncol 13:2449–2456
12. Greenberg LW, Jewett LS, Gluck RS, Champion LA, Leikin SL,Altieri MF, Lipnick RN (1984) Giving information for a life-threatening diagnosis. Parents’ and oncologists’ perceptions. AmJ Dis Child 138:649–653
13. Jedlicka-Kohler I, Gotz M, Eichler I (1996) Parents’ recollection ofthe initial communication of the diagnosis of cystic fibrosis.Pediatrics 97:204–209
14. Levetown M (2008) Communicating with children and families:from everyday interactions to skill in conveying distressing infor-mation. Pediatrics 121:e1441–e1460
15. Mack JW, Wolfe J, Grier HE, Cleary PD, Weeks JC (2006)Communication about prognosis between parents and physiciansof children with cancer: parent preferences and the impact ofprognostic information. J Clin Oncol 24:5265–5270
16. Parker PA, Baile WF, de Moor C, Lenzi R, Kudelka AP, Cohen L(2001) Breaking bad news about cancer: patients’ preferences forcommunication. J Clin Oncol 19:2049–2056
17. Ptacek JT, Eberhardt TL (1996) Breaking bad news. A review of theliterature. JAMA 276:496–502
18. Pueschel SM, Murphy A (1977) Assessment of counseling prac-tices at the birth of a child with Down’s syndrome. Am J MentDefic 81:325–330
19. Sharp MC, Strauss RP, Lorch SC (1992) Communicating medicalbad news: parents’ experiences and preferences. J Pediatr 121:539–546
20. Sloper P, Turner S (1993) Determinants of parental satisfaction withdisclosure of disability. Dev Med Child Neurol 35:816–825
21. Strauss RP, Sharp MC, Lorch SC, Kachalia B (1995) Physiciansand the communication of “bad news”: parent experiences of beinginformed of their child’s cleft lip and/or palate. Pediatrics 96:82–89
22. Vaidya VU, Greenberg LW, Patel KM, Strauss LH, Pollack MM(1999) Teaching physicians how to break bad news: a 1-day work-shop using standardized parents. Arch Pediatr Adolesc Med153:419–422
23. Buckman R (1992) How to break bad news: a guide for health careprofessionals. Johns Hopkins University Press, Baltimore
24. Serwint JRL (2000) Sharing bad news with patients. ContempPediatr 17:45–66
25. Miller KS, Vannatta K, Vasey M, Yeager N, Compas BE, GerhardtCA (2012) Health literacy variables related to parents’ understand-ing of their child’s cancer prognosis. Pediatr Blood Cancer 59:914–918
26. Davey HM, Butow PN, Armstrong BK (2003) Cancer patients’preferences for written prognostic information provided outside theclinical context. Br J Cancer 89:1450–1456
27. Hagerty RG, Butow PN, Ellis PM, Dimitry S, Tattersall MH (2005)Communicating prognosis in cancer care: a systematic review ofthe literature. Ann Oncol 16:1005–1053
28. Groopman J (2001) Dying words. The New Yorker29. Kaplowitz SA, Campo S, Chiu WT (2002) Cancer patients’ desires
for communication of prognosis information. Health Commun14:221–241
30. Kim MK, Alvi A (1999) Breaking the bad news of cancer: thepatient’s perspective. Laryngoscope 109:1064–1067
31. Lobb EA, Butow PN, Kenny DT, Tattersall MH (1999)Communicating prognosis in early breast cancer: do women under-stand the language used? Med J Aust 171:290–294
32. Eden O, Black I, MacKinlay G, Emery A (1994) Communicationwith parents of children with cancer. Palliat Med 8:105–114
Support Care Cancer





























