Embed Size (px)
Citation preview

T b i t S tT b i t S tTabagisme et SportTabagisme et Sport
Daniel THOMASInstitut de Cardiologie Pitié Salpêtrière ParisPitié-Salpêtrière, Paris
DU Cardiologie du sport Pitié SalpêtrièreDU Cardiologie du sport Pitié Salpêtrière

Le tabagisme est il compatible g pavec le sport?
OUI !
…pour l’industrie du tabac !

« Propos de « sportifs » »« Propos de « sportifs » »« Oui, Docteur, je fume mais je fais du sport »Oui, Docteur, je fume mais je fais du sport« J’élimine les effets du tabac par le sport »« Je fume si peu que cela n’a pas d’importance »Je fume si peu que cela n a pas d importance« Je fume mais cela ne limite pas mes performances »« Une cigarette après le match, c’est si bon! »U e c ga e e ap ès e a c , c es s bo« Il y a des sportifs de haut niveau qui fument! »
What knowledge do we need?What knowledge do we need?What knowledge do we need?What knowledge do we need?
11-- Cardiovascular riskCardiovascular riskattributable to smokingattributable to smoking
22-- Mechanisms involvedMechanisms involved in the in the CV t i it f kiCV t i it f kiCV toxicity of smokingCV toxicity of smoking
33 BenefitsBenefits resulting fromresulting from33-- Benefits Benefits resulting fromresulting fromsmoking cessationsmoking cessationsmoking cessationsmoking cessation

What knowledge do we need?What knowledge do we need?What knowledge do we need?What knowledge do we need?
Cardiovascular riskCardiovascular riskCardiovascular riskCardiovascular riskattributable to smokingattributable to smokingattributable to smokingattributable to smoking

: a: a few numbersfew numbers: a : a few numbersfew numbers●● 4 833 0004 833 000 deaths/yeardeaths/year●● 4 833 000 4 833 000 deaths/yeardeaths/year
attributable to smoking in the worldattributable to smoking in the world19 % of deaths for men19 % of deaths for men < 70 years< 70 years19 % of deaths for men19 % of deaths for men < 70 years< 70 years5% of deaths for women5% of deaths for women < 70 years< 70 years
First cause of avoidable mortalityFirst cause of avoidable mortalityFirst cause of avoidable mortalityFirst cause of avoidable mortality●● Cardiovascular deathsCardiovascular deaths due to smoking due to smoking = 1 690 000= 1 690 000
24 % f di l d th24 % f di l d th
ggDeaths by Deaths by lung cancerlung cancer due to smoking = due to smoking = 848 000848 000
●● 24 % of cardiovascular deaths24 % of cardiovascular deathsof men between 30 and 69 years of men between 30 and 69 years are exclusively linked to smokingare exclusively linked to smoking
Ezzati M, Lopez AD. Lancet 2003: 362: 847Ezzati M, Lopez AD. Lancet 2003: 362: 847--5252
are exclusively linked to smokingare exclusively linked to smoking

S ki dS ki dSmoking and Smoking and myocardial infarctionmyocardial infarctionmyocardial infarctionmyocardial infarction
Lancet 2006; 368: 647Lancet 2006; 368: 647––5858

Risk of MI associated withRisk of MI associated with any type of tobacco usedany type of tobacco usedRisk of MI associated with Risk of MI associated with any type of tobacco usedany type of tobacco used
OR for current smokers = 2.95 (95% CI 2.77–3.14)OR
(95%CI)
2.952.95
Filter Non filter Beedies Pipes,Cigares
ChewChew
+Smoke
Never
Teo KK, Ounpuu S, Hawken S. Lancet 2006; 368: 647–58
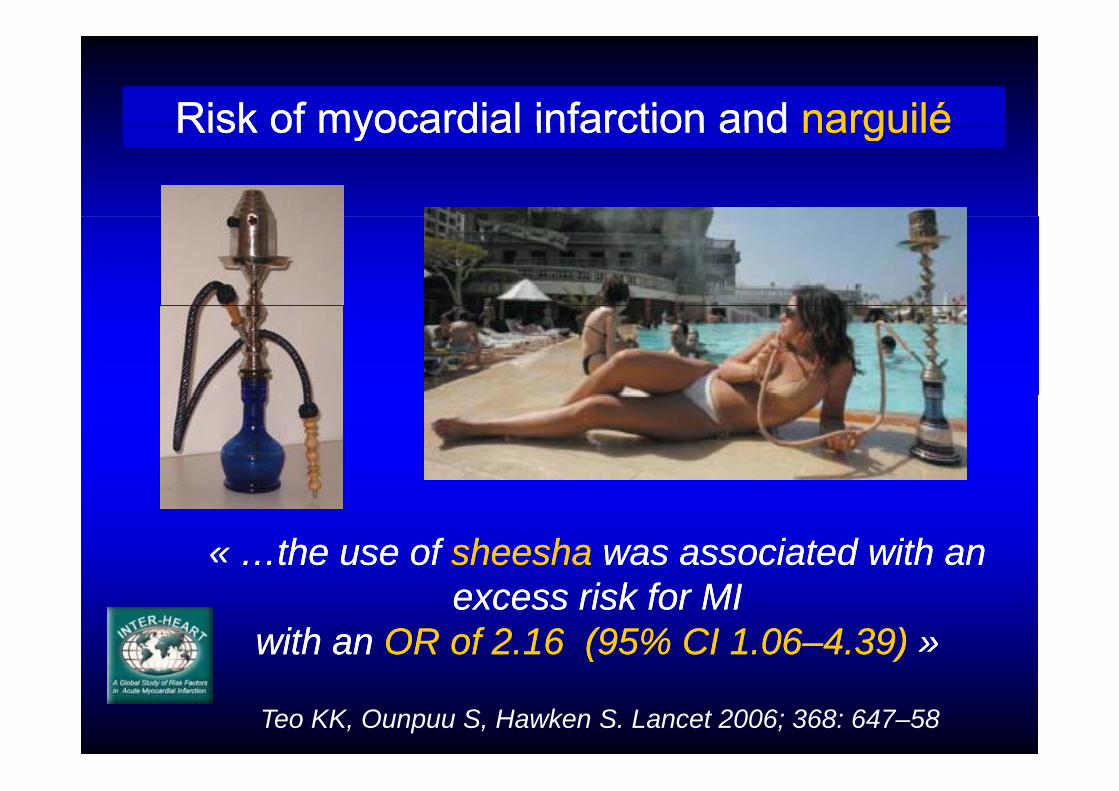
Risk of myocardial infarction andRisk of myocardial infarction and narguilénarguiléRisk of myocardial infarction and Risk of myocardial infarction and narguilénarguilé
«« …the use of …the use of sheeshasheesha was associated with an was associated with an excess risk for MI excess risk for MI
with an with an OR of 2.16 (95% CI 1.06OR of 2.16 (95% CI 1.06––4.39)4.39) »»
Teo KK, Ounpuu S, Hawken S. Lancet 2006; 368: 647–58
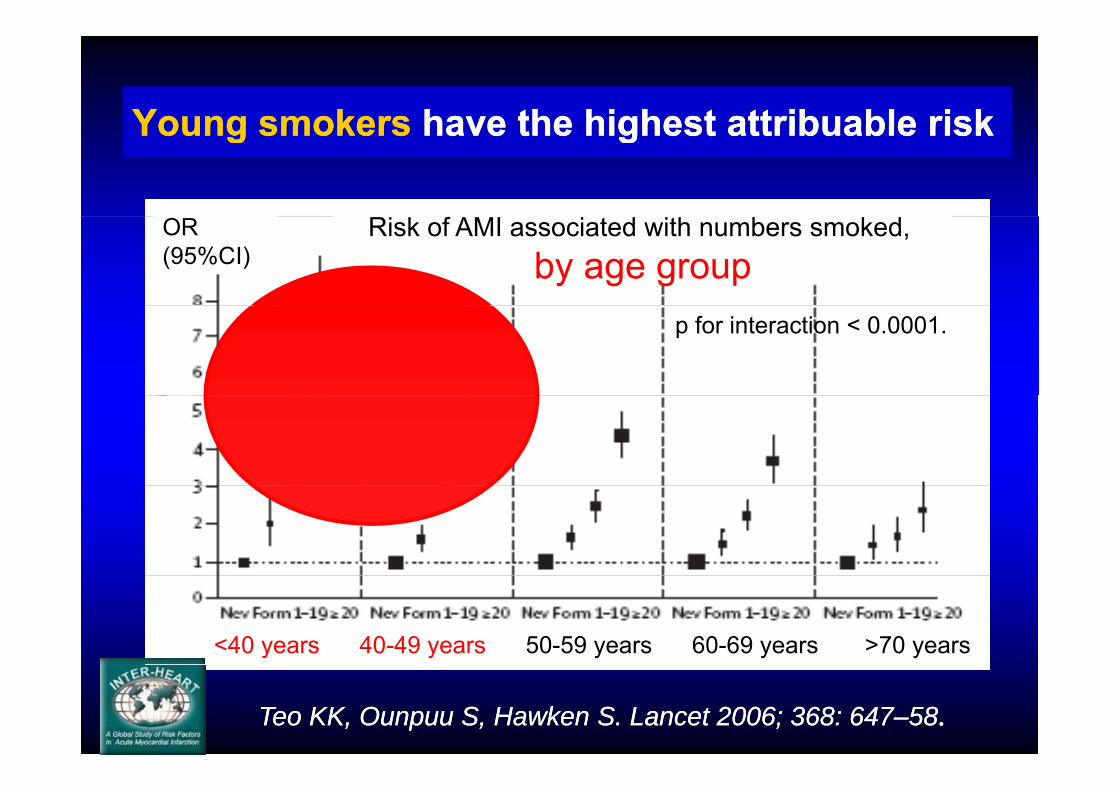
Young smokersYoung smokers have the highest attribuable riskhave the highest attribuable riskYoung smokersYoung smokers have the highest attribuable riskhave the highest attribuable risk
Risk of AMI associated with numbers smoked, by age group
OR(95%CI)
p for interaction < 0.0001.
<40 years 40-49 years 50-59 years 60-69 years >70 years
Teo KK, Ounpuu S, Hawken S. Lancet 2006; 368: 647Teo KK, Ounpuu S, Hawken S. Lancet 2006; 368: 647––5858..
Under 45 years,Under 45 years,80% of80% of
the victims of the victims of myocardial myocardial infarction infarction infarction infarction
are smokersare smokers

6448 patients with ST+ AMI6448 patients with ST+ AMIwith information on smoking statuswith information on smoking statuswith information on smoking statuswith information on smoking status
% of smokers regarding age and sex(Woman/Man prevalence)74
80
7078
8090
3848
62
404650
6070
Men n = 4753Women n = 1695
16
28
38
1721
40
203040
7810214
11
01020
<45 45 49 50 54 55 59 60 64 65 69 70 74 75 79 80 84 >= 85<45 45-49 50-54 55-59 60-64 65-69 70-74 75-79 80-84 >= 850,97 0,94 0,74 0,55 0,60 0,180,83 0,250,68 0,40Global Woman/Man prevalence = 0,38
Thomas D et al. Étude ALLIANCE Journées Européennes de la SFC Janvier 2007

% of smokers among ST+ AMI patients % of smokers among ST+ AMI patients ith l i k f tith l i k f t % of smokers regarding age and sex
with only one risk factorwith only one risk factor
in patients with only one risk factor(Woman/Man prevalence)
75
84
7680
90
50
62 6168
50
60
70 Men n = 1674Women n = 551
23
36
22
40
30
40
50
865
16
214
141822
0
10
20
0<45 45-49 50-54 55-59 60-64 65-69 70-74 75-79 80-84 >= 85
0,90 0,90 0,98 0,80 0,61 0,78 0,87 0,80 0,16 0,20Global Woman/Man prevalence = 0 38Global Woman/Man prevalence = 0,38
Thomas D et al. Journées Européennes SFC Janvier 2007

Number of cigarettesNumber of cigarettes smokedsmokedand risk of MIand risk of MI
8 ≥21 cigarettes smoked per dayrepresents about 1.5 pack of cigarettes per day, associated with OR 6.00–7.00.
OR(95%CI)
8
associated with OR 6.00 7.00.4
2
1
For 1 to 9 cigarettes/d OR=1,63 (95% CI 1,45 -1,82, p<0,0001)
Number of cigarettes smoked per day
0.75
Teo KK, Ounpuu S, Hawken S. Lancet 2006; 368: 647Teo KK, Ounpuu S, Hawken S. Lancet 2006; 368: 647––58.58.
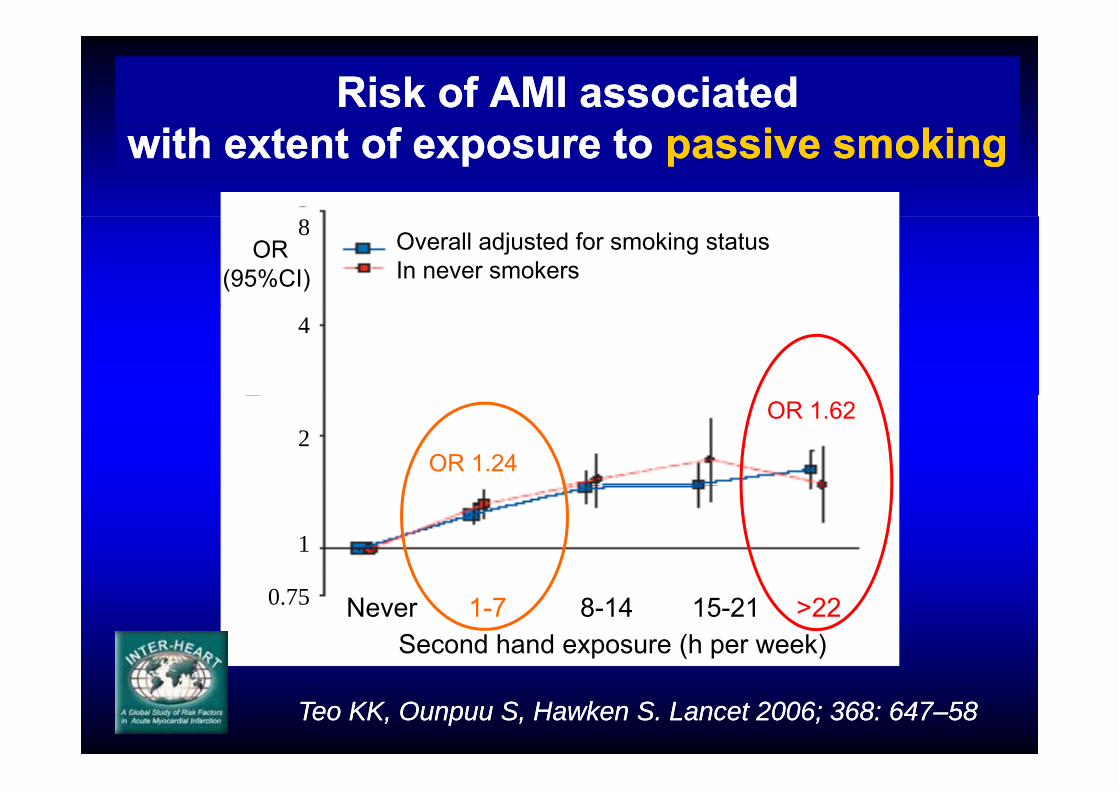
Risk of AMI associated Risk of AMI associated with extent of exposure to with extent of exposure to passive smokingpassive smoking
OR(95%CI)
8 Overall adjusted for smoking statusIn never smokers
4
2OR 1.24
OR 1.62
1
Second hand exposure (h per week)
0.75 Never 1-7 8-14 15-21 >22
Teo KK, Ounpuu S, Hawken S. Lancet 2006; 368: 647Teo KK, Ounpuu S, Hawken S. Lancet 2006; 368: 647––5858

Smoking intervenes Smoking intervenes without threshold without threshold ith f i t itith f i t itneither of intensity, neither of intensity,
nor length of consumptionnor length of consumptionev
ent
dise
ase
eic
hea
rt d
P i ki t diP i ki t di
isch
aem
i Passive smoking studiesPassive smoking studies
No exposureNo exposure
Number of cigarettes smoked a dayRR
of i
D’après Law MR et Wald NJ. Prog Cardiovasc Dis 2003; 46:31-8

Tabagisme et maladies vasculairesTabagisme et maladies vasculairesTabagisme et maladies vasculairesTabagisme et maladies vasculairesne se résume pas à l’infarctus du myocardene se résume pas à l’infarctus du myocarde
What knowledge do we need?What knowledge do we need?What knowledge do we need?What knowledge do we need?
Mechanisms involvedMechanisms involved ininthe cardiovascular toxicity of smokingthe cardiovascular toxicity of smokingthe cardiovascular toxicity of smokingthe cardiovascular toxicity of smoking
Th b iTh b iEndothelial dysfunctionEndothelial dysfunction ThrombosisThrombosis

Biological effects of smoking on cardiovascular system
Plateletactivation
Endothelium
Oxydativestress
Vascular inflammation
Smoke Acute
Coronary
Endothelium dysfunctionCarbon
monoxide
exposureCoronarysyndromeAutonomic
dysfunction Negativemyocardial
Adrenergic stimulation
yoxygen balance
Adapted from Raupach T et al. Eur Heart J 2006; 27: 386–392
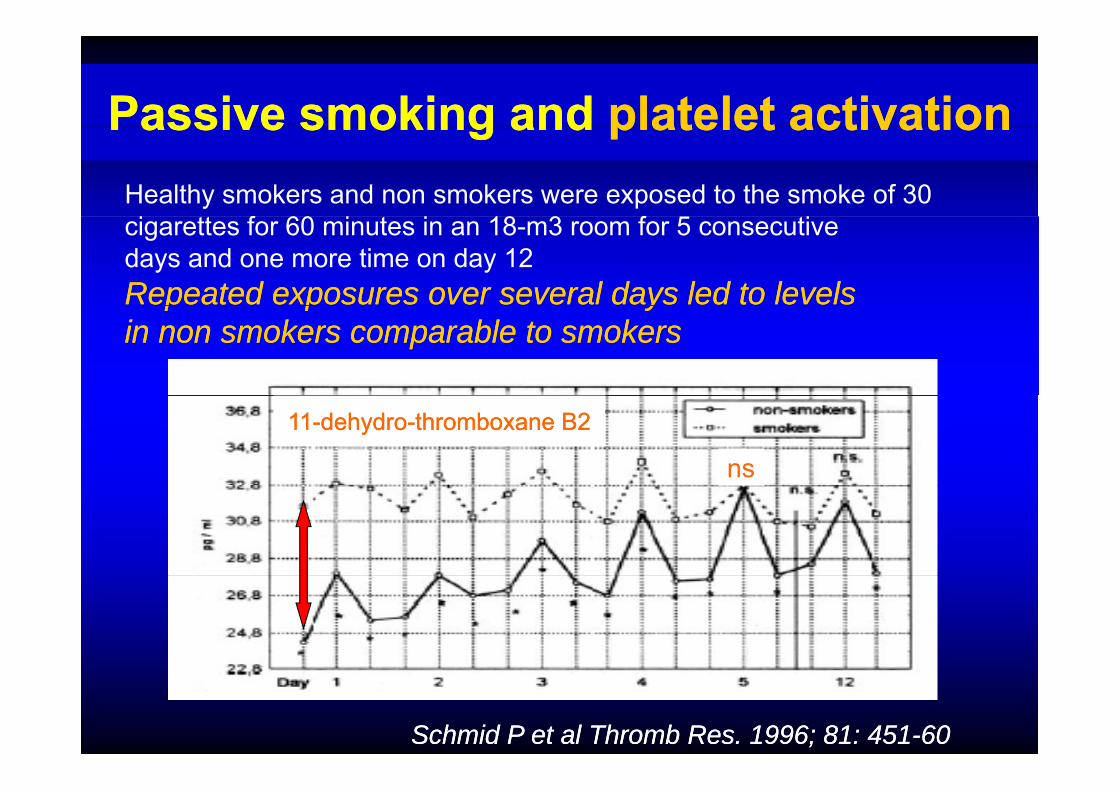
Passive smokingPassive smoking andand plateletplatelet activationactivationPassive smoking Passive smoking and and plateletplatelet activationactivationHealthy smokers and non smokers were exposed to the smoke of 30
f fcigarettes for 60 minutes in an 18-m3 room for 5 consecutivedays and one more time on day 12Repeated exposures over several days led to levelsRepeated exposures over several days led to levelsp p yp p yin non smokers comparable to smokersin non smokers comparable to smokers
1111--dehydrodehydro--thromboxane B2thromboxane B2
ns
Schmid P et al Thromb Res. 1996; 81: 451Schmid P et al Thromb Res. 1996; 81: 451--6060

Active and passive smokingActive and passive smokingandand coronary endothelial dysfunctioncoronary endothelial dysfunction
% change in lumen diameters of % change in lumen diameters of th i fl tth i fl tthe circumflex arterythe circumflex arteryin in responseresponseto intracoronary injection ofto intracoronary injection ofto intracoronary injection of to intracoronary injection of acetylcholine (100 acetylcholine (100 μμgg)in patients:in patients:pp-- non smokers non smokers -- passive smokers passive smokers
ti kti k-- active smokersactive smokers
H Sumida et al. J. Am. Coll. Cardiol. 1998;31;811H Sumida et al. J. Am. Coll. Cardiol. 1998;31;811--815815
Nicotine and cardiovascular diseasesNicotine and cardiovascular diseasesNicotine and cardiovascular diseasesNicotine and cardiovascular diseases
Ni ti ff tNi ti ff t (( ) *) *Nicotine effectsNicotine effects (when «(when « smokedsmoked ») *») *
Heart rate +10%Heart rate +10%Heart rate +10%Heart rate +10%Blood pressure + 5 mmHgBlood pressure + 5 mmHgduring about 15 minutes for 1 cigaretteduring about 15 minutes for 1 cigaretteduring about 15 minutes for 1 cigaretteduring about 15 minutes for 1 cigarettemyocardial work and O2 consumptionmyocardial work and O2 consumption
* these effects are absent for the concentration of * these effects are absent for the concentration of nicotine released by nicotine replacement therapy +++nicotine released by nicotine replacement therapy +++
Nicotine is responsible for tobacco addictionNicotine is responsible for tobacco addictionbut has a small if any effectbut has a small if any effectbut has a small, if any, effect but has a small, if any, effect in cardiovascular events in cardiovascular events
NNicotine icotine RReplacement eplacement TTreatment reatment in CHD patientsin CHD patients
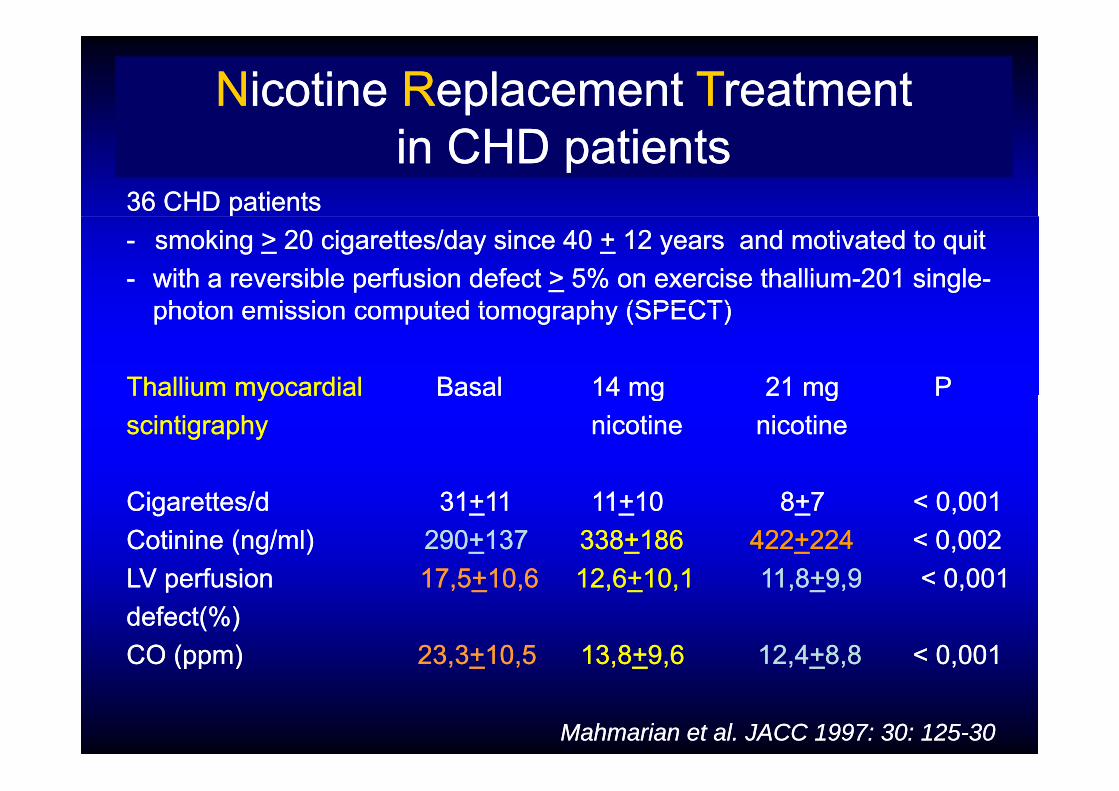
3636 CHD patientsCHD patients-- smoking smoking >> 20 cigarettes/20 cigarettes/dayday sincesince 40 40 ++ 12 12 yearsyears and motivatedand motivated to to quitquit-- withwith a a reversiblereversible perfusion perfusion defectdefect >> 5% on 5% on exercise thalliumexercise thallium--201 single201 single--
photon emission computed tomography (SPECT)photon emission computed tomography (SPECT)photon emission computed tomography (SPECT) photon emission computed tomography (SPECT)
ThalliumThallium myocardialmyocardial BasalBasal 14 mg14 mg 21 mg P21 mg PThallium Thallium myocardialmyocardial BasalBasal 14 mg14 mg 21 mg P21 mg Pscintigraphyscintigraphy nicotine nicotine nicotinenicotine
Cigarettes/dCigarettes/d 3131++1111 1111++1010 88++7 < 0,0017 < 0,001CotinineCotinine ((ngng/ml)/ml) 290290++137 137 338338++186 186 422422++224 224 < 0,002< 0,002LV perfusionLV perfusion 17 517 5++10 610 6 12 612 6++10 110 1 11 811 8++9 99 9 < 0 001< 0 001LV perfusionLV perfusion 17,517,5++10,6 10,6 12,612,6++10,1 10,1 11,811,8++9,99,9 < 0,001< 0,001defectdefect(%)(%)CO (ppm)CO (ppm) 23,323,3++10,510,5 13,813,8++9,6 9,6 12,412,4++8,8 8,8 < 0,001< 0,001(pp )(pp ) ,, ,, ,, ,, ,, ,, ,,
Mahmarian et al. JACC 1997: 30: 125Mahmarian et al. JACC 1997: 30: 125--3030
FRENCH RECOMMENDATIONS OF GOOD PRACTICEFRENCH RECOMMENDATIONS OF GOOD PRACTICE
DrugDrug and non drug therapeutic strategies to assist smoking cessationand non drug therapeutic strategies to assist smoking cessation
•• Nicotine replacement therapy (NRT) Nicotine replacement therapy (NRT) i ll t l t d CHD ti ti ll t l t d CHD ti tis well tolerated among CHD patients is well tolerated among CHD patients and do not cause aggravation of CHD or arrhythmiasand do not cause aggravation of CHD or arrhythmias
•• NRT is recommended for CHD patients who are smokersNRT is recommended for CHD patients who are smokerspp
•• NRT b ib d t th it f th itNRT b ib d t th it f th it•• NRT can be prescribed at the exit of the coronary care unit, NRT can be prescribed at the exit of the coronary care unit, immediatelyimmediately after a myocardial infarctionafter a myocardial infarction
AFSSAPS Mai 2003AFSSAPS Mai 2003
What knowledge do we need?What knowledge do we need?What knowledge do we need?What knowledge do we need?
Benefits resulting Benefits resulting fromfrom smoking cessationsmoking cessationfromfrom smoking cessationsmoking cessation

Carbon monoxideCarbon monoxide levels drop levels drop within hourswithin hours
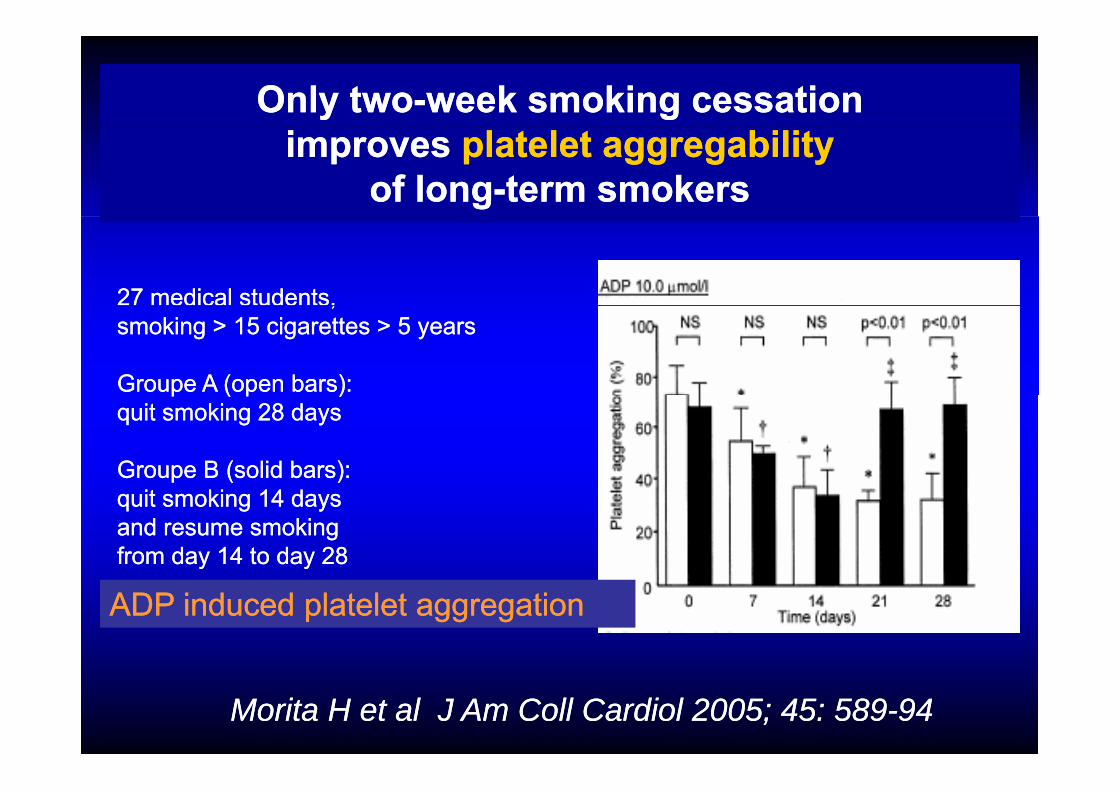
Only twoOnly two--week smoking cessationweek smoking cessationimprovesimproves platelet aggregabilityplatelet aggregability
of longof long--term smokersterm smokers
27 medical students, 27 medical students, ,,smoking > 15 cigarettes > 5 yearssmoking > 15 cigarettes > 5 years
Groupe A (open bars): Groupe A (open bars): p ( p )p ( p )quit smoking 28 daysquit smoking 28 days
Groupe B (solid bars): Groupe B (solid bars): quit smoking 14 daysquit smoking 14 daysand resume smoking and resume smoking from day 14 to day 28from day 14 to day 28
ADP induced platelet aggregationADP induced platelet aggregation
Morita HMorita H et al et al J Am Coll Cardiol 2005; 45: 589J Am Coll Cardiol 2005; 45: 589--9494

Smoking and Smoking and life expectancylife expectancygg p yp y1711 Finnish men 40 to 59 year old Follow up: 35 years1711 Finnish men 40 to 59 year old Follow up: 35 years
Age at death according to smoking statusAge at death according to smoking status(at the beginning)(at the beginning)
Total mortality Total mortality Coronary deathsCoronary deathsNb of cig/day Nb of cig/day n = 1219n = 1219 n = 388n = 388
NEVER SMOKERSNEVER SMOKERS 73,673,6 73,473,4
SMOKERSSMOKERS 68 968 9 (( 4 7 yrs)4 7 yrs) 68 368 3 (( 5 1 yrs)5 1 yrs)SMOKERSSMOKERS 68,968,9 ((--4,7 yrs)4,7 yrs) 68,368,3 ((--5,1 yrs)5,1 yrs)>> 2020 67,867,8 ((--5,8 yrs)5,8 yrs) 67,867,8 ((--5,6 yrs)5,6 yrs)
EX SMOKERSEX SMOKERS 70 770 7 (( 2 9 )2 9 ) 71 771 7 (( 1 7 )1 7 )EX SMOKERSEX SMOKERS 70,770,7 ((--2,9 yrs)2,9 yrs) 71,771,7 ((--1,7 yrs)1,7 yrs)
Qiao Q et al. Eur Heart J 2000; 21: 1621Qiao Q et al. Eur Heart J 2000; 21: 1621--66

Effects on Effects on survivalsurvival of smoking cessationof smoking cessationgg
CESSATION AT AGE 35CESSATION AT AGE 35--4444 CESSATION AT AGE 55CESSATION AT AGE 55--6464
Stopped smoking Stopped smoking
ars
ars
Cigarette smokersCigarette smokers
Non smokersNon smokers
m a
ge 4
0 ye
age
60 y
ea
60%
80%
urvi
val f
rom
urvi
val f
rom
% s
u
% s
u
70 70yearsyears
Smoking cessationSmoking cessation is is alwaysalways associated with a benefit…associated with a benefit……but, stopping…but, stopping earlier earlier is associated is associated withwith greater benefit !greater benefit !
Doll R, Peto R et al. BMJ2004; 328: 1519-28
Effects of smoking cessation Effects of smoking cessation i d tii d tiin secondary preventionin secondary prevention
• • After acute myocardial infarction After acute myocardial infarction (observational studies)(observational studies)50% deaths in patients who quit smoking50% deaths in patients who quit smoking
Aberg A et al. Br Heart J 1983; 49:416Aberg A et al. Br Heart J 1983; 49:416--2222
Risk of Risk of rhythmic deathrhythmic death for non quittersfor non quittersPeters W et al Peters W et al J Am Coll Cardiol 1995; 26:1287-92
• • After CABGAfter CABGRisk ofRisk of reintervention X 2,5reintervention X 2,5 at 1 year at 1 year for non quitters for non quitters Voors AA et al Voors AA et al Circulation 1996; 93: 42Circulation 1996; 93: 42--77
•• After angioplastyAfter angioplastyRisk of Risk of acute MI and death X 1,4acute MI and death X 1,4 at 4,5 years at 4,5 years for non quitters for non quitters Hasdai D et alHasdai D et al N Engl J Med 1997; 336: 755N Engl J Med 1997; 336: 755--6161
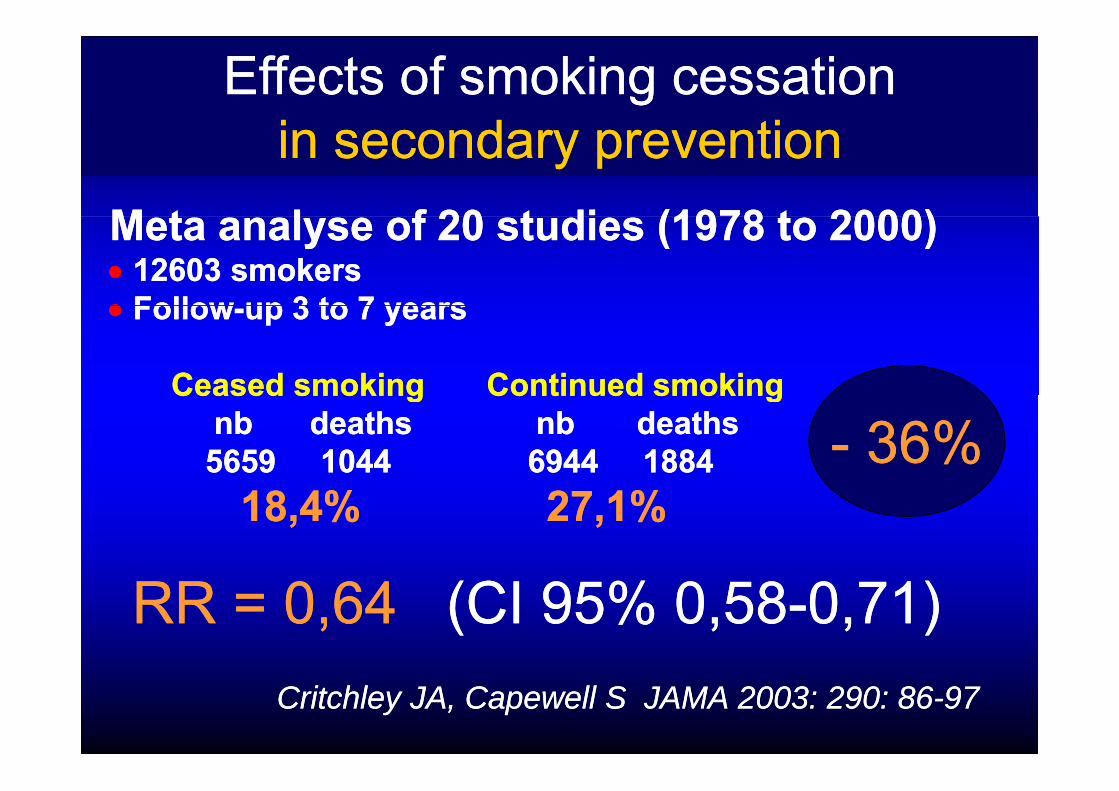
Effects of smoking cessation Effects of smoking cessation i d tii d ti
M t l f 20 t di (1978 t 2000)M t l f 20 t di (1978 t 2000)
in secondary preventionin secondary preventionMeta analyse of 20 studies (1978 to 2000)Meta analyse of 20 studies (1978 to 2000)•• 12603 smokers12603 smokers•• FollowFollow up 3 to 7 yearsup 3 to 7 years•• FollowFollow--up 3 to 7 yearsup 3 to 7 years
Ceased smokingCeased smoking Continued smokingContinued smokingCeased smokingCeased smoking Continued smokingContinued smokingnbnb deaths nb deathsdeaths nb deaths5659 10445659 1044 6944 18846944 1884 -- 36%36%
18,4%18,4% 27,1%27,1%
RR = 0,64RR = 0,64 (CI 95% 0,58(CI 95% 0,58--0,71)0,71)Critchley JA, Capewell S JAMA 2003: 290: 86Critchley JA, Capewell S JAMA 2003: 290: 86--9797
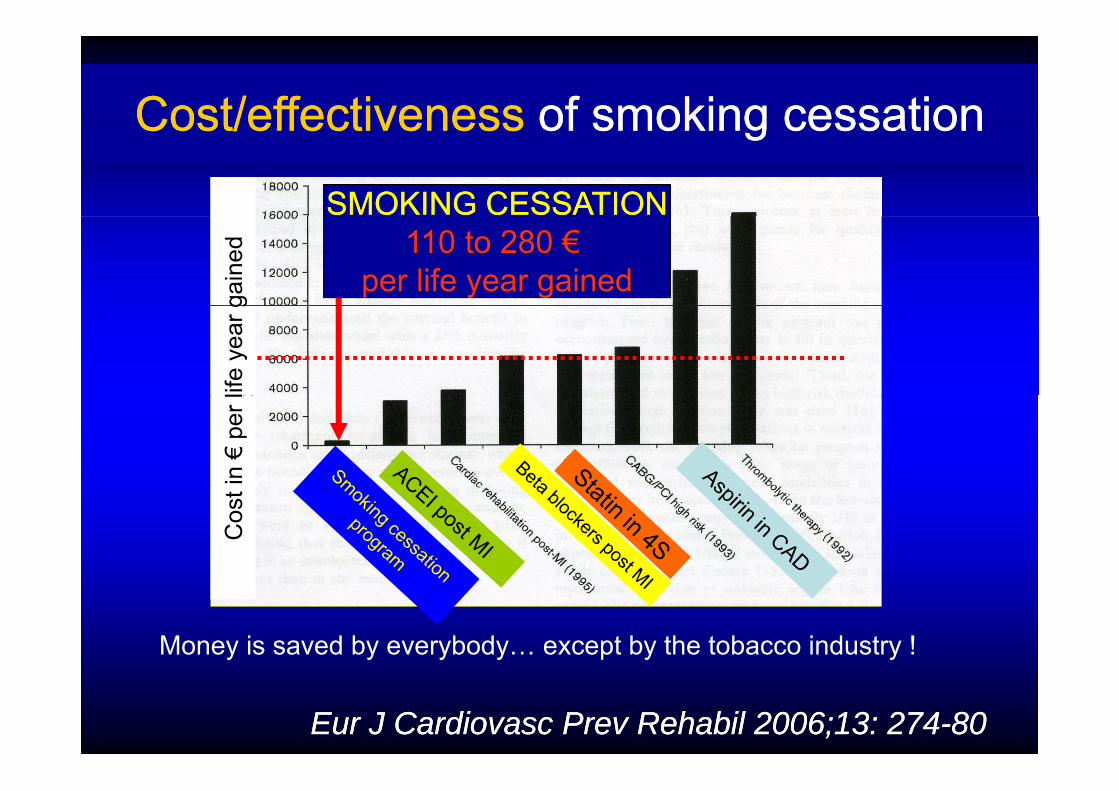
Cost/effectivenessCost/effectiveness of smoking cessationof smoking cessation
SMOKING CESSATIONSMOKING CESSATION
Cost/effectivenessCost/effectiveness of smoking cessationof smoking cessation
110 to 280 €per life year gained
gain
edlif
e ye
ar g
in €
per l
Cos
t
Money is saved by everybody… except by the tobacco industry !
Eur J Cardiovasc Prev Rehabil 2006;13: 274Eur J Cardiovasc Prev Rehabil 2006;13: 274--8080
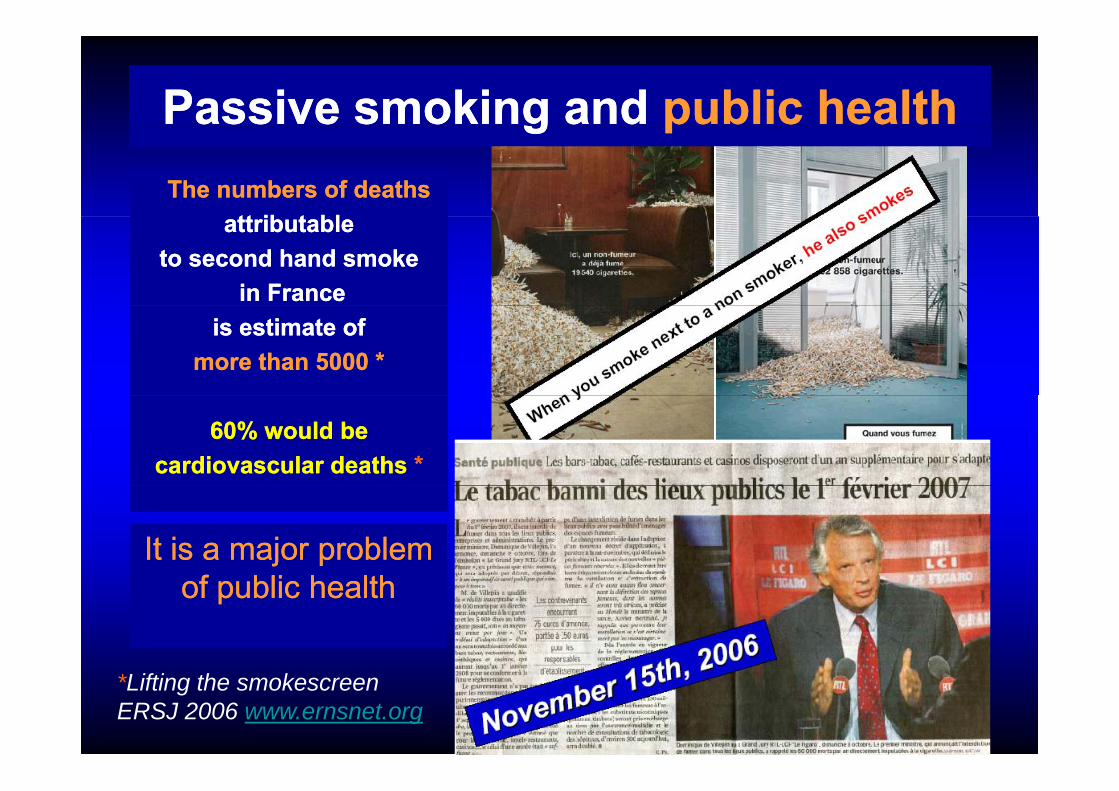
Passive smoking andPassive smoking and public healthpublic healthgg ppThe numbers of deathsThe numbers of deaths
tt ib t bltt ib t blattributable attributable to second hand smoke to second hand smoke
in France in France is estimate ofis estimate of
more than 5000 *more than 5000 *
60% would be 60% would be cardiovascular deaths cardiovascular deaths **
It is a major problem It is a major problem f bli h l hf bli h l hof public healthof public health
*Lifting the smokescreen ERSJ 2006 www.ernsnet.org

A national law banning smoking A national law banning smoking in public on 10 January 2005in public on 10 January 2005in public on 10 January 2005in public on 10 January 2005
ShortShort--term reduction in hospital admissions term reduction in hospital admissions for acute myocardial infarction for acute myocardial infarction among persons aged under 60among persons aged under 60 - 11%among persons aged under 60 among persons aged under 60
Results waited for France:Results waited for France: A reduction ofA reduction ofResults waited for France: Results waited for France: A reduction of A reduction of 5000 to 7000 myocardial infarction per year ?5000 to 7000 myocardial infarction per year ?
BaroneBarone--Adesi F et al. Eur Heart J 2006; 27Adesi F et al. Eur Heart J 2006; 27: : 24682468––7272
For many patients, smoking cessation For many patients, smoking cessation needs medical assistanceneeds medical assistance
The US Public Health Service ‘‘treating tobacco use The US Public Health Service ‘‘treating tobacco use and dependence clinical practice guidelines’’ as aand dependence clinical practice guidelines’’ as aand dependence clinical practice guidelines as a and dependence clinical practice guidelines as a legal standard of carelegal standard of care
Randy M Torrijos, Stanton A GlantzRandy M Torrijos, Stanton A Glantz
“…a judicial standard of care that could be used in cases of malpractice brought against healthcare
id h d t t t ti t h k ”
T b C t l 2006 15 447 451
providers who do not treat patients who smoke.”
Tobacco Control 2006;15:447–451.
« D’accord Docteur« D’accord Docteur,je veux bienje veux bien,
mais je fais comment? »mais je fais comment? »

So why do people smoke?So why do people smoke?So why do people smoke?So why do people smoke?Smoking leads to a double dependenceSmoking leads to a double dependence
physiological dependencepsychological dependencepsychological dependence
Nicotine is one of thestrongest gaddictive drug
Produces multiple effects of reinforcement
Leads to withdrawal symptoms and craving when its level decrease
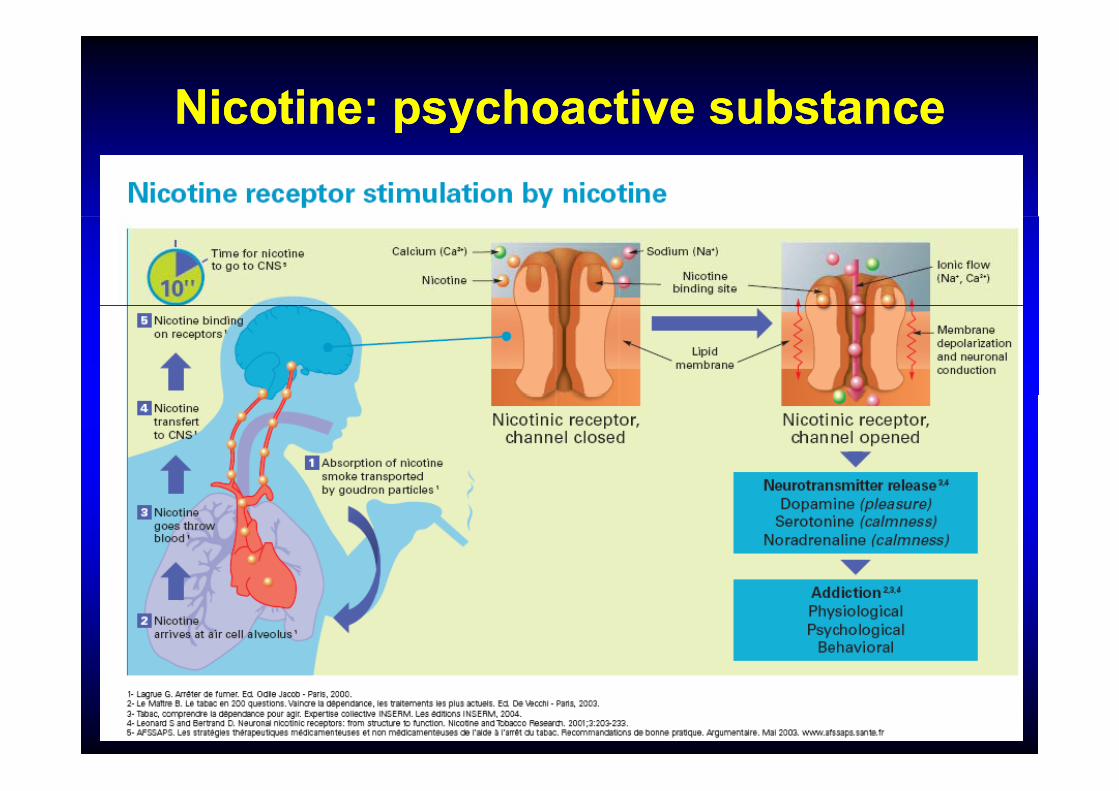
Nicotine: psychoactive substanceNicotine: psychoactive substancep yp y

Withdrawal SyndromeWithdrawal Syndromeyy

Treatment for Smoking Cessation: Treatment for Smoking Cessation: ggGuidelinesGuidelines
– The minimal counseling
– Nicotine replacement therapy (OTC):• patches / gums / sublingual tablets / inhalerp g g
– Prescription Treatment: Bupropion, Vareniclinep p p ,
Behavioral and cognitive therapies must be– Behavioral and cognitive therapies must be associated
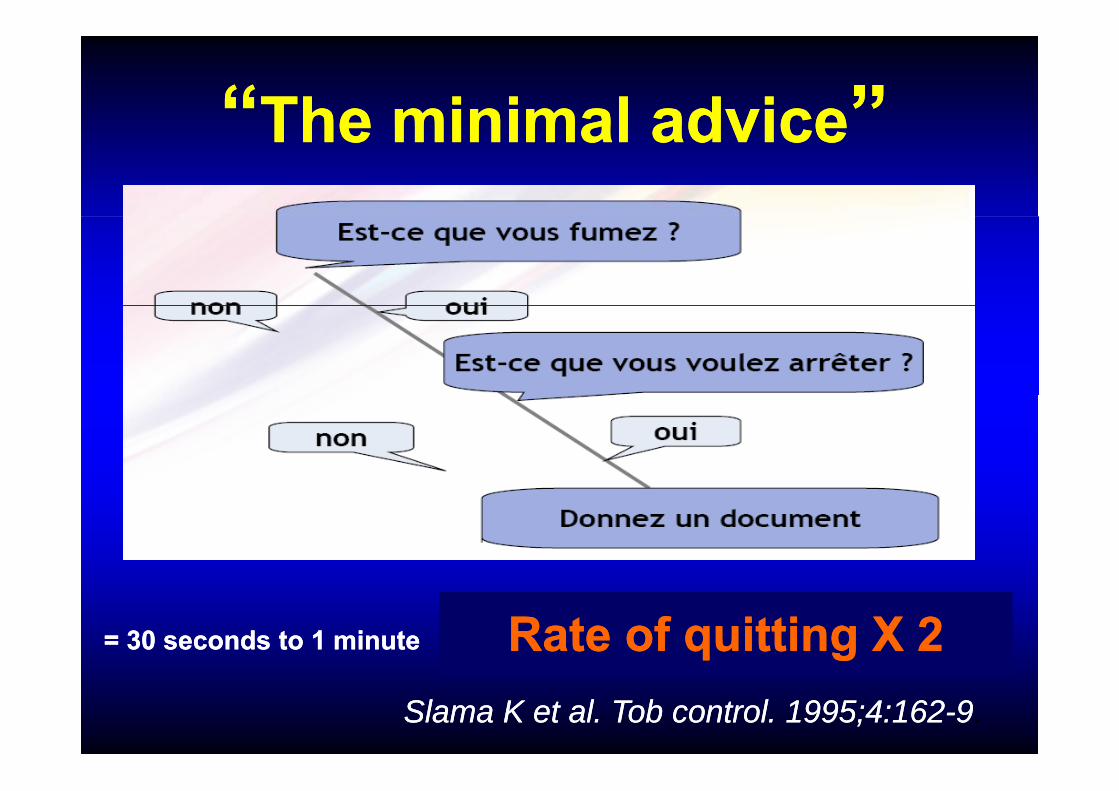
““The minimal adviceThe minimal advice””The minimal adviceThe minimal advice
Rate of quitting X 2Rate of quitting X 2= 30 seconds to 1 minute= 30 seconds to 1 minute
Slama K et al. Tob control. 1995;4:162Slama K et al. Tob control. 1995;4:162--99.
ÉÉléments de motivationde motivation
Éléments de motivation

Éléments de motivation
Smoking and Smoking and ggSkin Aging in Skin Aging in IdenticalIdenticalIdentical Identical TwinsTwins
Doshi, D. N. et al. Doshi, D. N. et al. Arch Dermatol Arch Dermatol 2007;143:15432007;143:1543 154615462007;143:15432007;143:1543--15461546.

Nicotine replacement therapyNicotine replacement therapyNicotine replacement therapyNicotine replacement therapy
PatchsPatchs GumsGums InhalerInhalerPatchsPatchs GumsGums InhalerInhaler
TabletsTabletsTabletsTablets
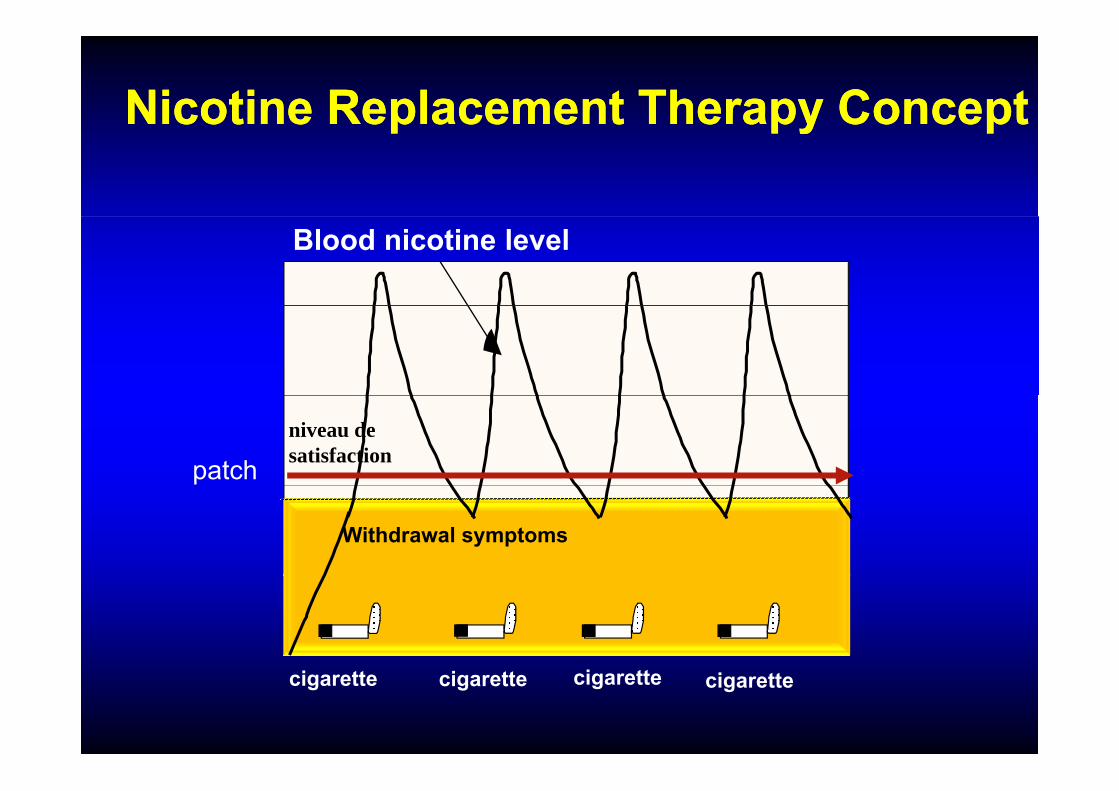
Nicotine Replacement Therapy ConceptNicotine Replacement Therapy Conceptp py pp py p
Blood nicotine level
niveau de satisfactionpatch
Withdrawal symptoms
cigarette cigarettecigarette cigarette

Nicotine KineticNicotine KineticPlasmatic Nicotine
/ l
Nicotine KineticNicotine Kineticng/ml
Cigarette
25
Spray NasalGum 4 mg
Patch 21 mgGum 4 mg
Inhaler
Gum 2 mg0
0 30 60 min
Gum 2 mg
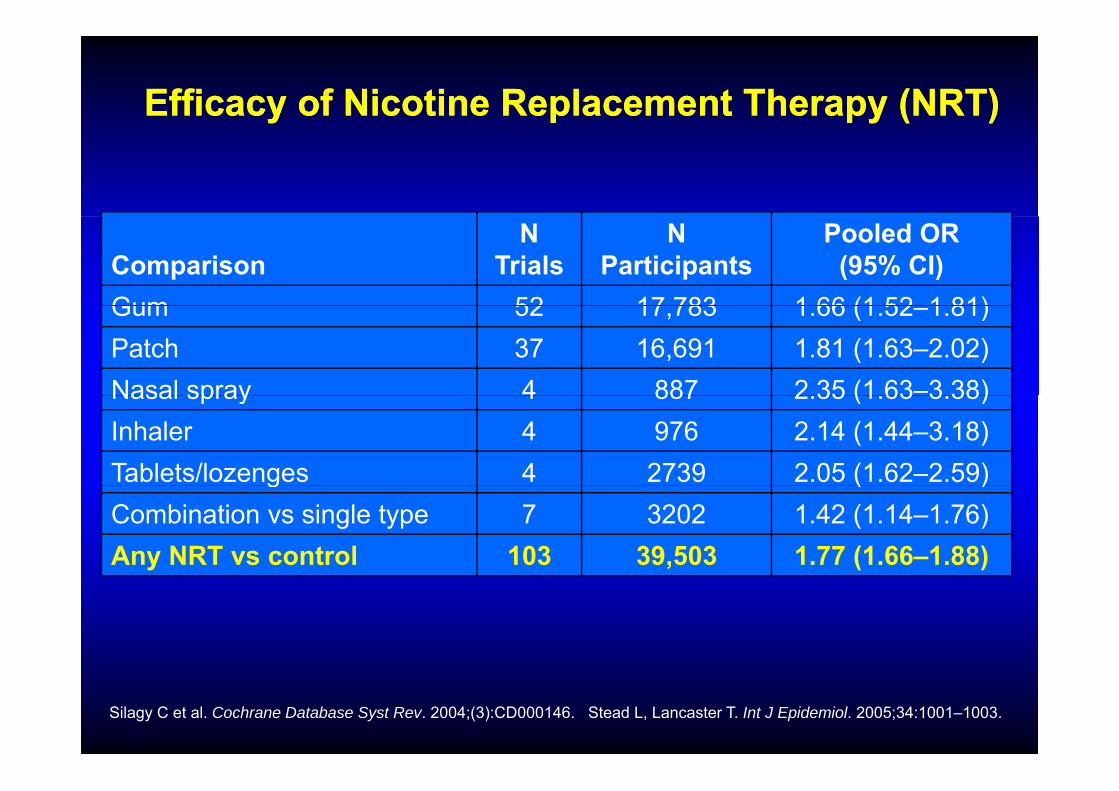
Efficacy of Nicotine Replacement Therapy (NRT)Efficacy of Nicotine Replacement Therapy (NRT)
ComparisonN
TrialsN
ParticipantsPooled OR
(95% CI)Gum 52 17 783 1 66 (1 52 1 81)Gum 52 17,783 1.66 (1.52–1.81)Patch 37 16,691 1.81 (1.63–2.02)Nasal spray 4 887 2 35 (1 63–3 38)Nasal spray 4 887 2.35 (1.63 3.38)Inhaler 4 976 2.14 (1.44–3.18)Tablets/lozenges 4 2739 2.05 (1.62–2.59)g ( )Combination vs single type 7 3202 1.42 (1.14–1.76)Any NRT vs control 103 39,503 1.77 (1.66–1.88)
Silagy C et al. Cochrane Database Syst Rev. 2004;(3):CD000146. Stead L, Lancaster T. Int J Epidemiol. 2005;34:1001–1003.

Bupropion SRBupropion SR
Blocks reuptake of dopamine
Must respect contraindications and precautions of use
Side effects:Side effects:Mouth drynessInsomniaHeadacheAllergic reactions
2 months treatment « on prescription »
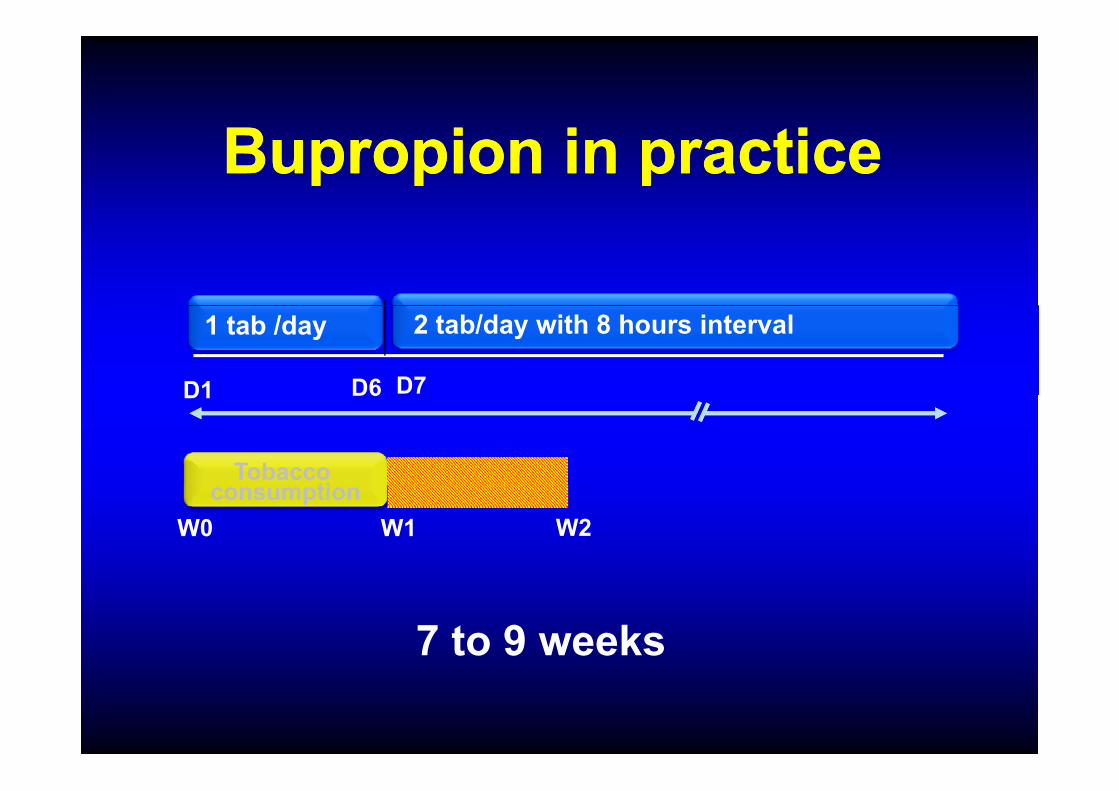
Bupropion in practiceBupropion in practice
1 tab /day
D7
2 tab/day with 8 hours interval
D1 D6D1 D6
Tobacco ti
W2W0 W1consumption
7 to 9 weeks
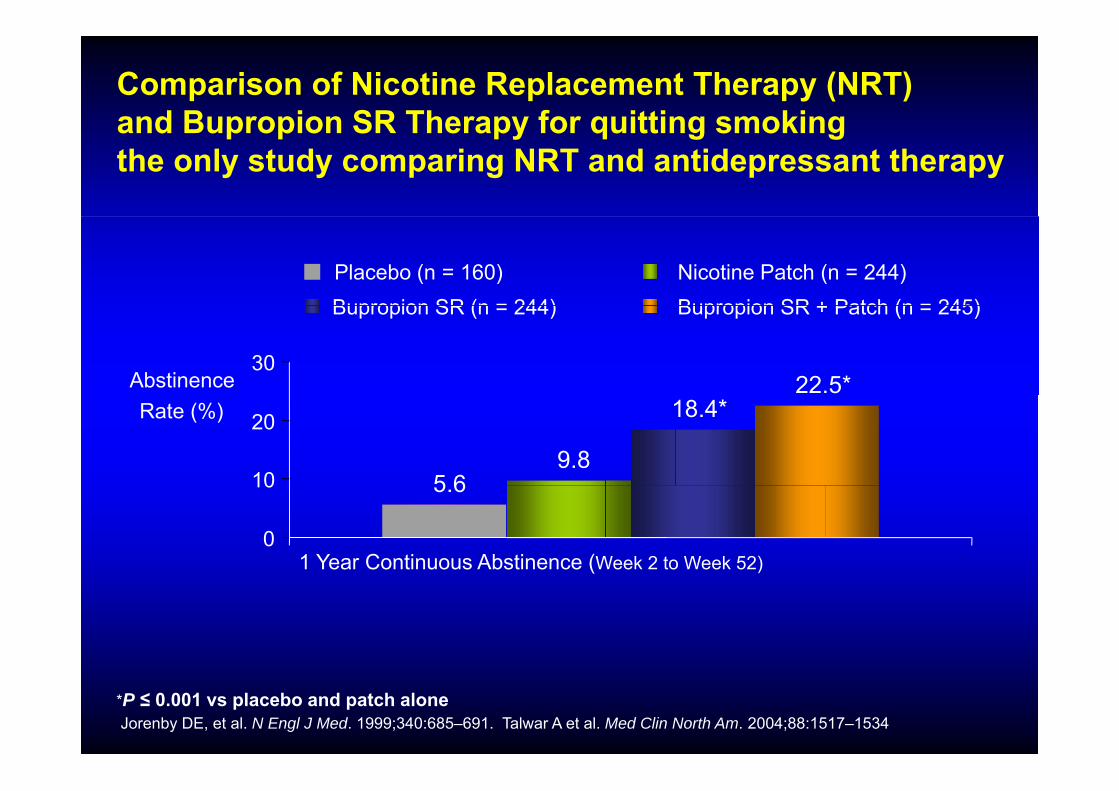
Comparison of Nicotine Replacement Therapy (NRT) and Bupropion SR Therapy for quitting smokingand Bupropion SR Therapy for quitting smokingthe only study comparing NRT and antidepressant therapy
Placebo (n = 160) Nicotine Patch (n = 244)Bupropion SR (n = 244) Bupropion SR + Patch (n = 245)
22.5*30
Abstinence
Bupropion SR (n = 244) Bupropion SR + Patch (n = 245)
5 69.8
18.4*
10
20Rate (%)
5.6
0
10
1 Year Continuous Abstinence (Week 2 to Week 52)
*P ≤ 0.001 vs placebo and patch aloneJorenby DE, et al. N Engl J Med. 1999;340:685–691. Talwar A et al. Med Clin North Am. 2004;88:1517–1534.
Varenicline Mechanism of ActionVarenicline Mechanism of ActionVarenicline Mechanism of ActionVarenicline Mechanism of Action
• Specifically developed for tobacco dependencedependence
A d bl h i f ti• A double mechanism of action– partial agonist activity: reduces craving and p g y g
withdrawal symptoms – antagonist activity: produces a reduction of theantagonist activity: produces a reduction of the
rewarding and reinforcing effects of smoking
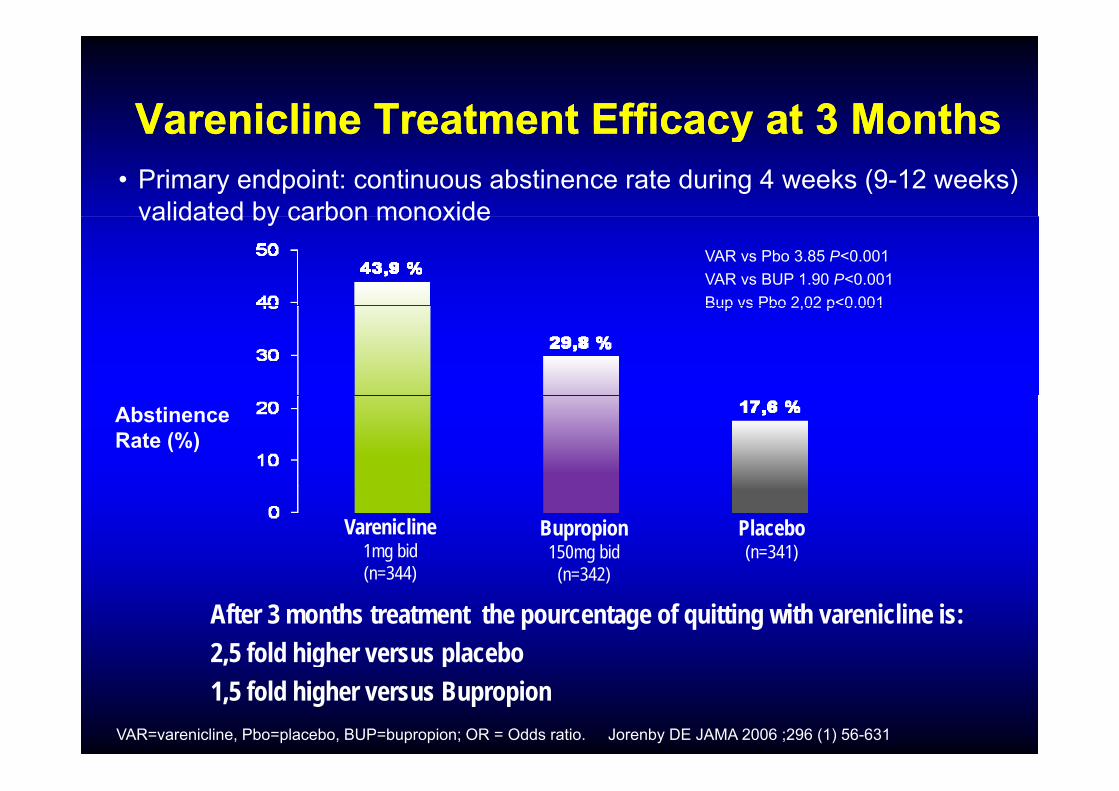
VareniclineVarenicline Treatment Efficacy atTreatment Efficacy at 33 MonthsMonthsVareniclineVarenicline Treatment Efficacy at Treatment Efficacy at 3 3 MonthsMonths• Primary endpoint: continuous abstinence rate during 4 weeks (9-12 weeks)
validated by carbon monoxideVAR vs Pbo 3.85 P<0.001VAR vs BUP 1.90 P<0.001Bup vs Pbo 2 02 p<0 001
validated by carbon monoxide
Bup vs Pbo 2,02 p<0.001
AbstinenceRate (%)
Varenicline1mg bid (n=344)
Bupropion150mg bid
(n=342)
Placebo(n=341)
After 3 months treatment the pourcentage of quitting with varenicline is:2,5 fold higher versus placebo
(n=344) (n=342)
VAR=varenicline, Pbo=placebo, BUP=bupropion; OR = Odds ratio. Jorenby DE JAMA 2006 ;296 (1) 56-631
, g p1,5 fold higher versus Bupropion

VVarenicline Treatment Efficacy at arenicline Treatment Efficacy at One YearOne Year• Secondary endpoint: continuous abstinence rate 9 - 52 weeks
validated by carbon monoxide
VAR vs Pbo 3.85 P<0.001VAR vs BUP 1.90 P<0.001B Pb 2 02 0 001
validated by carbon monoxide
Bup vs Pbo 2,02 p<0.001
Ab tiAbstinenceRate (%)
Varenicline1mg bid ( 344)
Bupropion150mg bid
( 342)
Placebo(n=341)
After 1 year treatment the pourcentage of quitting with varenicline is: 2,2 fold higher versus placebo
(n=344) (n=342)
VAR=varenicline, Pbo=placebo, BUP=bupropion; Jorenby DE JAMA 2006 , 296 (1) 56-63
, g p1,6 fold higher versus Bupropion
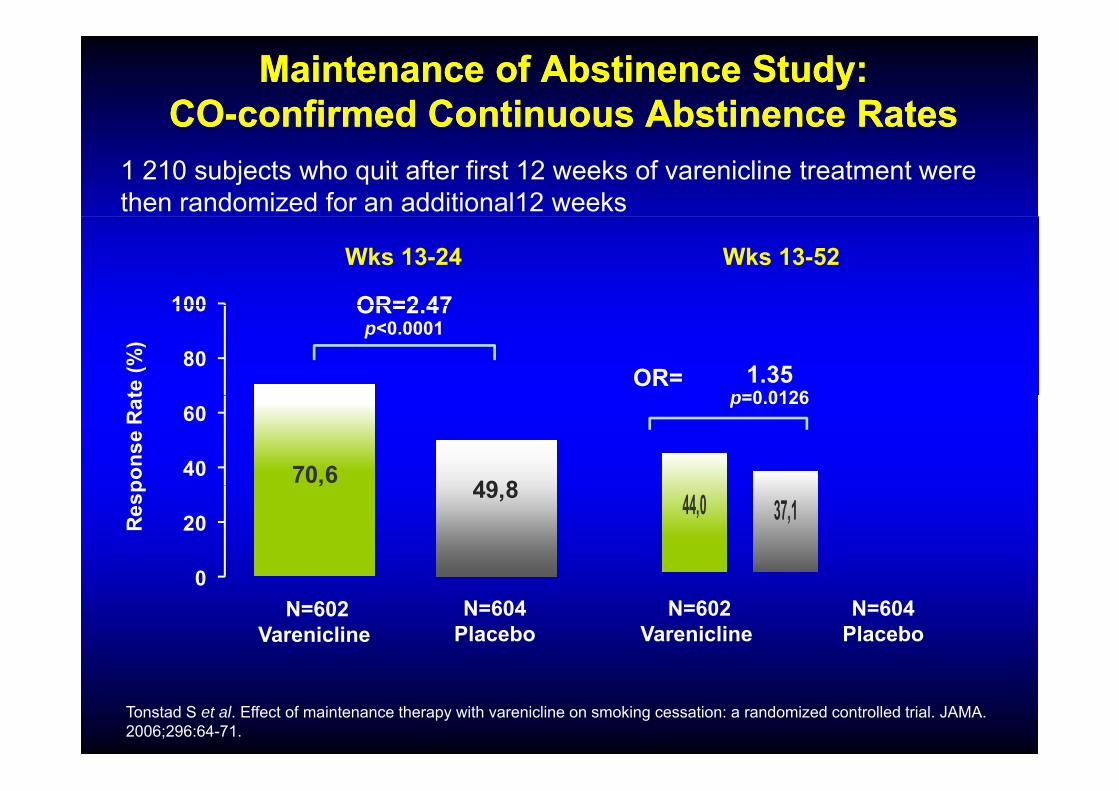
Maintenance of Abstinence Study:Maintenance of Abstinence Study:COCO--confirmed Continuous Abstinence Ratesconfirmed Continuous Abstinence RatesCOCO confirmed Continuous Abstinence Ratesconfirmed Continuous Abstinence Rates
1 210 subjects who quit after first 12 weeks of varenicline treatment were then randomized for an additional12 weeks
100
Wks 13-24
OR=2 47
Wks 13-52
80
100
te (%
)
OR=2.47p<0.0001
1.35p=0 0126
OR=
70,6 49 840
60
pons
e R
at p=0.0126
, 49,8
0
20Res
p
44,0 37,1
0N=604
PlaceboN=602
VareniclineN=604
PlaceboN=602
Varenicline
Tonstad S et al. Effect of maintenance therapy with varenicline on smoking cessation: a randomized controlled trial. JAMA. 2006;296:64-71.
Varenicline: A Good Tolerance Profile
Clinical trials included approximately 4 000 patientsClinical trials included approximately 4 000 patientsClinical trials included approximately 4,000 patients Clinical trials included approximately 4,000 patients treated with varenicline for up to 1 year (average treated with varenicline for up to 1 year (average exposure 84 days)exposure 84 days)p y )p y )
In general, when adverse reactions oocured, onset was In general, when adverse reactions oocured, onset was in the first week of therapy; severity was generaly mild to in the first week of therapy; severity was generaly mild to moderatemoderate
-- nauseas (28 6%)nauseas (28 6%)
Side events reported with a frequency Side events reported with a frequency ≥ ≥ 10% were:10% were:-- nauseas (28.6%)nauseas (28.6%)-- headachesheadaches-- abnormal dreamsabnormal dreams
i ii i-- insomniainsomnia
How Prescribe Varenicline In PracticeHow Prescribe Varenicline In PracticeHow Prescribe Varenicline In PracticeHow Prescribe Varenicline In Practice
• Recommended dosage: 1 mg bid• Recommended dosage: 1 mg bid
• Posology and method of administration• Posology and method of administration- D1 - D3: 0,5mg od
D4 D7 0 5 bid- D4 - D7: 0,5 mg bid- D8 - end of treatment: 1 mg bid
• 12 weeks treatment
• For patients who have successfully stopped smoking at the d f 12 k dditi l f 12 kend of 12 weeks, an additional course of 12 weeks
treatment with varenicline at 1mg bid may be considered

Varenicline (CHAMPIX)® 12 Weeks Treatment
W k 1 W k 2 W k 3 t 12
Varenicline (CHAMPIX)® 12 Weeks Treatment
Week 1 Week 2 Week 3 to 12
TitrationD1 to D3: 0 5 mg 1/day 1 mg 2/day 1 2/dD1 to D3: 0,5 mg 1/dayD4 to D7: 0,5 mg 2/day
1 mg 2/day 1 mg 2/day
Two maintenance packs: 1 h- 1 month
(56 x 1mg tablets
- 2 weeks- 2 weeks(28 x 1mg tablets
Also available: 56 x 0,5 mg tablets
Some Smokers May Need More Help to Quit
– Higher level of dependence• Cigarettes per day• Cigarettes per day• Time to first cigarette upon awakening
– Living with a current smoker– Fewer educational qualificationsq– Lower socioeconomic class– Comorbid psychiatric disorders
1. Hyland A et al. Nicotine Tob Res. 2004;6(Suppl 3):S363-S369.2. Chandola T et al. Addiction. 2004;99:770-777.3. Kalman D et al. Am J Addict. 2005;14:106–123.
Au totalAu totalAu totalAu totalT b i t t tT b i t t t•• Tabagisme et sport sont Tabagisme et sport sont incompatibles = incompatibles = «« association dangereuseassociation dangereuse »»«« association dangereuseassociation dangereuse »»
•• Sujet devant être Sujet devant être systématiquement abordé systématiquement abordé yyavec un sportifavec un sportif
•• Il faut proposer une aide au Il faut proposer une aide au sevrage chez tous lessevrage chez tous lessevrage chez tous les sevrage chez tous les fumeursfumeurs
•• Il faut apprendre à gérer leIl faut apprendre à gérer le•• Il faut apprendre à gérer le Il faut apprendre à gérer le sevrage tabagique au sevrage tabagique au quotidienquotidien

![HÔPITAL PITIÉ-SALPÊTRIÈRE - Coma Science … update April 2017 [1] ATHENA DEMERTZI INSTITUT DU CERVEAU ET DE LA MOELLE ÉPINIÈRE - ICM 4ÈME ÉTAGE- PIÈCE 4.029 HÔPITAL PITIÉ-SALPÊTRIÈRE](https://img.dokumen.tips/doc/110x75/5b9b455d09d3f22d2a8ce5f2/hopital-pitie-salpetriere-coma-science-update-april-2017-1-athena-demertzi.jpg)



























