Embed Size (px)
Citation preview

Journal ofNeurology, Neurosurgery, and Psychiatry, 1976, 39, 829-834
Dacrystic epilepsyM. L. OFFEN, R. A. DAVIDOFF1, B. T. TROOST, AND E. T. RICHEY
From the Department ofNeurology, University ofMiami School of Medicine and NeurologyService, Veterans Administration Hospital, Miami, Florida, USA
SYNOPSIS We observed a 69 year old patient who had spontaneous paroxysmal attacks ofweeping with lacrimation, contorted facies, and (usually) head-turning to the right. These episodeswere followed by confusion and amnesia. During a pentylenetetrazol-evoked attack the EEG showeda right temporal delta rhythm. Atrophy, particularly of the right temporal regions, was noted on
pneumoencephalography. We propose the term 'dacrystic epilepsy' for this rare type of seizuredisorder.
No one today would dispute that laughter canbe a manifestation of epileptic activity. Thephenomenon has been documented for ovei 100years since Trousseau (1873) observed laughterduring an ictal episode. Since then there havebeen upwards of 120 similar case reports (Rey-Pias, 1972; Chen and Forster, 1973). But crying-which might be looked upon as the expressiveantithesis of laughter-is curiously absent frommost descriptions of epilepsy. Indeed, anextensive search in the literature revealed onlyfive case reports in which weeping might beconstrued as epileptiform (Ziligien, 1906; Purves-Stewart, 1927; Davison and Kelman, 1939;Efron, 1961; Stutte, 1963).
Recently, we had the opportunity to study apatient with a seizure disorder in which episodesof paroxysmal crying were prominent. Thephenomena were unusual and intriguing. Becauseof the rarity of this type of seizure, we feel that itwarrants reporting. We propose that the term'dacrystic epilepsy' [Greek dakrvon, tear] beused to describe this type of seizure disorder.
CASE HISTORY
In January 1975 a 60 year old, right-handed man washospitalized because he suffered from seizures which
1 Address for correspondence: Robert A. Davidoff, MD, NeurologyService (127), Veterans Administration Hospital, 1201 NW 16th Street,Miami, Fla., 33125, USA.(Accepted 6 May 1976.)
were nearly continuous despite the administration ofdiphenylhydantoin and phenobarbitone. His mentalstate precluded us from obtaining a thorough medicalhistory, but the following is known about his past:
In 1954 the patient was treated for syphilis of thecentral nervous system. The diagnosis was supportedby cerebrospinal fluid that showed a positive sero-logical test and a first zone colloidal gold curve. Atthat time he received penicillin for 20 days. Some timeafter this he developed epilepsy. Initially the seizureswere grand mal in type, but in subsequent years thepattern changed, so that on separate occasions hewould experience one or more of the following:grand mal convulsions, focal motor seizures involvingthe left-sided limbs, laughing spells, and episodes ofcrying. In recent years, most episodes were left-sidedfocal motor in type.
In 1958 he was seen by a physician for a complaintof generalized convulsions which occurred once ortwice a month. These were sometimes preceded by a'bad taste' in his mouth. Examination revealed onlya left superior incongruous quadrantanopsia; nofurther investigations were carried out at that time.Three years later, however, re-examination of thevisual field revealed that the visual loss had progressedand that he now had a complete left homonymoushemianopsia. Although the EEG demonstrated spikedischarges in the right parietal region, right carotidarteriography was normal. An examination in 1964disclosed a mild hemiparesis, the first focal deficitother than hemianopsia to be noted. This is the lastrecord we have for the patient until the hospitaliza-tion described below.At the time of the present admission there was
almost constant twitching of the left lower facialmusculature. We observed that the patient had a
829
Protected by copyright.
on 23 May 2018 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.39.9.829 on 1 Septem
ber 1976. Dow
nloaded from

M. L. Offen, R. A. Davidoff, B. T. Troost, and E. T. Richey
severe organic mental syndrome, and this was subse-quently confirmed by psychometric testing. Thefollowing deficits were noted: a dense left hemianop-sia; a mild left hemiparesis which involved the face,tongue, arm, and leg, and which was accompaniedby slightly increased tone, hyperreflexia, and anextensor plantar response; moderate lefthypaesthesia.At times, without any apparent provoking stimuli,
he would begin to weep. These episodes seemed to belike normal crying because they were accompaniedby lacrimation, contorted, mournful facies, andsobbing sounds, and because they were capable ofevoking an emotional response in observers. Theweeping usually lasted about 30 seconds and wasoften, but not always, followed by head-turning tothe right side. During the attacks the patient wasinattentive to his environment and unresponsive tocommand; afterwards he was slightly confused for afew seconds. The patient was amnestic for eventsoccurring during these episodes. At other times heexperienced periods of giggling which lasted a few
seconds. Except for these paroxysmal disturbances,the patient was pleasant and co-operative. His be-haviour was not grossly inappropriate nor was hisaffect otherwise labile.
Skull radiographs were normal. Four vessel cere-bral angiography revealed diffuse intracranial athero-sclerotic changes and evidence of lateral ventricularenlargement. While pneumoencephalography demon-strated enlargement of both lateral ventricles, theright frontal and temporal horns were considerablylarger than those on the left. The cerebrospinalfluid VDRL test was reactive, although the fluid wasacellular and had a protein concentration of 0.57 g/l.When the dosage of anticonvulsant medication
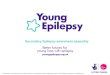
was increased, this patient's seizures eventuallystopped. The focal motor episodes proved easiest tocontrol; the laughing and crying spells were morerefractory to treatment. However, in order to docu-ment the ictal nature of our patient's crying and toverify that his emotional lability did not just reflectbihemispheric disease, we performed a pentylene-tetrazol test. The baseline EEG (Fig. 1) had shown a
CA- F8
T3-P3
T4- P4
T3-01
T, -02
59 M S- 7 5 50V I 1 s 1-35 Hz
FIG. 1 Bipolar EEG recording shows disorganization ofbasic pattern on right side with absence ofalpha rhythm.The pattern consists of theta with some delta activity. The left side shows alpha rhythm with occasional thetaactivity. Eye blink artefact present in first two channels.
830
Protected by copyright.
on 23 May 2018 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.39.9.829 on 1 Septem
ber 1976. Dow
nloaded from

Dacrystic epilepsy
diffusely abnormal record with asymmetry of theintrinsic pattern of electrical activity over the twohemispheres. The most organized tracings wererecorded from the posterior region of the left side andconsisted of alpha, theta, and beta waves. The homo-logous area on the right side was dominated by thetaand delta components; alpha activity was notpresent.With continuous 16 channel EEG and cinemato-
graphic monitoring, we administered pentylenetet-razol intravenously at a rate of 50 mg/min. When100 mg of the drug had been infused, a low voltage(50 /V) rhythmic 2.0 Hz delta rhythm developed inthe right posterior temporal-parietal-occipital regionand subsequently rose in amplitude to 150 ,tV.Concurrent with the inception of the delta activity,the patient's eyelids began to quiver. Fifteen secondslater this was followed by a left-beating horizontalnystagmus. When 175 mg of the convulsant drug
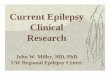
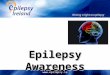
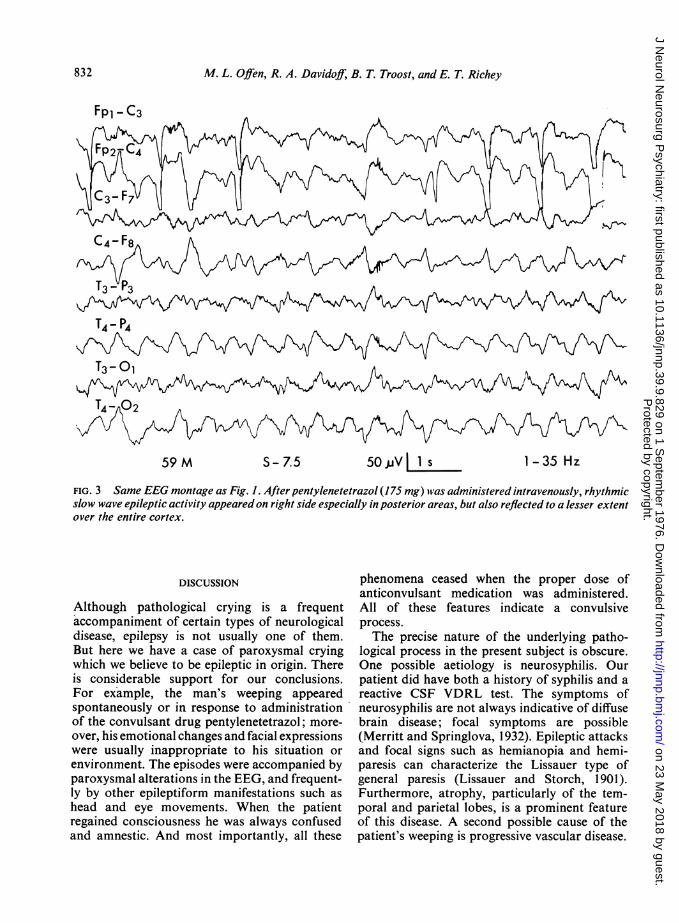
had been administered (and the injection terminated)the patient began to cry (Fig. 2). This was accom-panied by lacrimation and appeared to be identicalwith the spontaneous episodes observed previously.At the same time we observed in the EEG an electricalseizure characterized by diffuse rhythmic high voltage(50-100 4V) slow (1.5-2.0 Hz) discharges (Fig. 3).The patient continued to weep for 40 seconds, thenthe eyes deviated to the right, the left facial muscula-ture contracted tonically, and the left-beating nystag-mus returned. The seizure seemed to end when thefacial musculature relaxed and the patient salivated;but there was a second episode characterized byrightward ocular deviation, sustained tonic contrac-tion of the left face followed by deviation of the headto the left and clonic activity of the left arm. At thispoint we terminated the episode with 10 mg intra-venous diazepam. The patient was completelyamnestic for the event.
...n..
C:.:..
FlIJ. 2 Serial photographs of patient during pentylenetetrazol-induced seizure (times indicated are after startof infusion). (1) Control; (2) Two minutes, 15 seconds. (3) Three minuttes, 30 seconds. Crying began. (4) Threeminutes, 50 seconds. (5) Four minutes. Crying accompanied by sobbing and tears.
831
Protected by copyright.
on 23 May 2018 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.39.9.829 on 1 Septem
ber 1976. Dow
nloaded from
M. L. Offen, R. A. Davidoff, B. T. Troost, and E. T. Richey
Fpl - C3
C4-F8
AS*P S
59 M S- 7.5 50V I 1 S
FIG. 3 Same EEG montage as Fig. 1. After pentylenetetrazol (175 mg) was administered intravenously, rhythmicslow wave epileptic activity appeared on right side especially in posterior areas, but also reflected to a lesser extentover the entire cortex.
DISCUSSION
Although pathological crying is a frequentaccompaniment of certain types of neurologicaldisease, epilepsy is not usually one of them.But here we have a case of paroxysmal cryingwhich we believe to be epileptic in origin. Thereis considerable support for our conclusions.For example, the man's weeping appearedspontaneously or in response to administrationof the convulsant drug pentylenetetrazol; more-over, his emotional changes and facial expressionswere usually inappropriate to his situation or
environment. The episodes were accompanied byparoxysmal alterations in the EEG, and frequent-ly by other epileptiform manifestations such ashead and eye movements. When the patientregained consciousness he was always confusedand amnestic. And most importantly, all these
phenomena ceased when the proper dose ofanticonvulsant medication was administered.All of these features indicate a convulsiveprocess.The precise nature of the underlying patho-
logical process in the present subject is obscure.One possible aetiology is neurosyphilis. Ourpatient did have both a history of syphilis and areactive CSF VDRL test. The symptoms ofneurosyphilis are not always indicative of diffusebrain disease; focal symptoms are possible(Merritt and Springlova, 1932). Epileptic attacksand focal signs such as hemianopia and hemi-paresis can characterize the Lissauer type ofgeneral paresis (Lissauer and Storch, 1901).Furthermore, atrophy, particularly of the tem-poral and parietal lobes, is a prominent featureof this disease. A second possible cause of thepatient's weeping is progressive vascular disease.
1-35 Hz
832
Protected by copyright.
on 23 May 2018 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.39.9.829 on 1 Septem
ber 1976. Dow
nloaded from

Dacrystic epilepsy
The angiogram performed on the present ad-mission did show evidence of diffuse vascularpathology, but one performed 14 years previouslywas normal. Finally, trauma could produce a
similar clinical picture, but the lack of a definitivehistory makes this most speculative.
Involuntary and irresistible crying-so-calledforced crying-after organic brain disease iswidely recognized as a symptom of severalneurological states. One is pseudobulbar palsy,whether it results from amyotrophic lateralsclerosis or is an effect of bilateral cerebraldamage from vascular disease (Wilson, 1924;Davison and Kelman, 1939). The syndrome hasalso been observed in advanced multiple sclerosis,mesencephalic (Wilson, 1924) and hypothalmictumours (Davison and Kelman, 1939); on
occasion unilateral hemispheric tumours, in-farcts, or Wilson's disease have been implicatedas causative factors. In addition, although it hasbeen often denied, pathological crying frequentlyaccompanies bulbar palsy.
Forced crying may resemble our patient's
condition to some extent in that such periods ofcrying are involuntary, stereotyped, and uncon-
trollable. But in contrast with our patient'sepisodes, forced crying is usually, but not always,precipitated by events or objects in the externalenvironment (even though the precipitating causemay be inappropriate or non-specific). Further-more, the patients are neither unresponsiveduring attacks, nor amnestic for them afterward;they do not respond to anticonvulsant medica-tion. Thus, despite certain similarities, it shouldbe possible to differentiate between forced cryingand epileptic crying.Common sense may dictate that laughter and
weeping are closely related-'they laughed untilthey cried'-but gelastic seizures crop upfrequently, while ifwe are to judge from publishedaccounts, dacrystic seizures must be rare or atleast infrequently recognized. Before the presentcase there have been descriptions of five cases
in which pathological crying appeared to have an
epileptic basis (Table). Of these five, all butStutte's (1963) lack sufficient detail. None
TABLE
PATIENTS WITH CRYING SEIZURES
Reference
Ziligiesi(1906)
Purves-Stewart(1927)
Davison and Kelman(1939)
Efron(1961)
Stutte(1963)
Present
Age, sex
(y)
52 M
Clinical leatures
Aura: 'dizziness'; then production of whistlingsound, fluttering oflids, opening and shutting ofmouth, contraction of L face, turning of headto L; finally violent sobbing after which patientbrought L hand to mouth and then wiped eyeswith handkerchief
11 F No aura; uncontrollable attacks of seepingculminating in loss ofconsciousness and falling
51 M Aura: dimming of vision and vertigo; then tonicdeviation of eyes to R; pupil fixed and dilated;then uncontrollable weeping lasting 2-15 min;postictal R-sided dysaesthesias; no loss ofconsciousness
28 M Aura: 'dizziness'; 'throbbing sensation in head';loss of consciousness and weeping. Later:complex seizures including at various timesauditory, olfactory, and formed visual hallu-cinations: sensory Jacksonian march, crying,crawling on hands and knees
12 M No aura; deviation of head to R; flexion ofextremities; rotation of body to R, crying
60 M No aura; weeping and lacrimation followed byhead turning to R; inattention to environment,amnesia
Pathology or
clinicalfindings
Luetic pachymeningitis; soft-ening ofR parietotemporalcortex
Glioma of interpeduncularspace infiltrating upperpons, third nerve, and opticchiasm
Encephalomalacia L parietalcortex and medial nucleusof R thalamus
R cerebral arteriovenous mal-formation
Neonatal asphyxia; mentalretardation
Ventricular enlargement es-
pecially of R frontal andtemporal horns
L: left. R: right.
833
Protected by copyright.
on 23 May 2018 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.39.9.829 on 1 Septem
ber 1976. Dow
nloaded from
M. L. Offen, R. A. Davidoff, B. T. Troost, and E. T. Riclhey
provide EEG tracings taken during a weepingepisode.
In the absence of more adequate data, anygeneralizations based on clinical observationshave to be offered with obvious reservations.But it is of interest that four of six patients hadhead and/or eye deviation preceding the episodesof weeping. In most cases, there was amnesia forthe crying. Davison and Kelman's case (1939) isan obvious exception because the patient ap-parently maintained consciousness during hisseizures; a postictal affective component was notdescribed.The dacrystic seizures that are documented
vary from simple (Purves-Stewart, 1927; Stutte,1963) to very complex automatisms (Ziligien,1906; Efron, 1961). In some instances a definitepathological localization is available; even so,the data do not permit identification of a specificlocus responsible for weeping itself. However, aswith gelastic seizures, it seems probable that apathological substrate for dacrystic phenomenawill ultimately be demonstrated.At present, the neurophysiological basis of
'normal' crying is still unknown. It is a complexneurophysiological event which involves theassociation of affective changes, facial andrespiratory movements, and vasomoter andsecretory alterations. Clearly many neural struc-tures must participate. But as yet, there is noevidence either for an accurate localization orrepresentation of this complex pattern within thebrain. To our knowledge, experimental stimula-tion of brain structures has not evoked weeping.Lacrimation by itself has been produced,reportedly as part ofdiffuse autonomic dischargescaused by lesions which involved the structuressurrounding the third ventricle (Penfield, 1930;Haymaker 1958). Stimulation of the amygdalaand other parts of the limbic system (Anand andDug, 1955) is another source of tearing. The facialpatterns associated with crying can probably beelicited by brain stem stimulation (Weinsteinand Bender, 1943). However, the most obviousdifficulty in understanding crying is the lack of
a suitable experimental model, as humans areapparently unique in this regard. It is notunreasonable to expect that further clinicalinvestigations ofpatients with crying epilepsy mayproduce information concerning the underlyingmechanisms of crying.
REFERENCES
Anand, B. K., and Dug, S. (1955). Stimulation of limbicsystem of brain in waking animals. Science, 122, 1139.
Chen, R. C., and Forster, F. M. (1973). Cursive epilepsyand gelastic epilepsy. Neurology (Minneap.), 23,1019-1029.
Davison, C., and Kelman, H. (1939). Pathologic laughingand crying. Archives of Neurology and Psychiatry(Chic.), 42, 595-643.
Efron, R. (1961). Post-epileptic paralysis: theoreticalcritique and report of a case. Brain, 84, 381-394.
Haymaker, W. (1958). Colloid cysts of the third ventricle:A clinical study of 54 cases in the light of previouspublications. Acta Neurologica, 17, 211-277.
Lissauer, H., and Storch, E. (1901). Cter einige Falleatypischer progressiver Paralyse. Monatsschrift furPsychiatrie und Neurologie, 9, 401-420.
Merritt, H. H., and Springlova, M. (1932). Lissauer'sdementia par4lytica. Archives ofNeurology andPsychia-try (Chic.), 27, 987-1030.
Penfield, W. G. (1930). Diencephalic autonomic epilepsy.Research Publications of the Association for Researchin Nervous and Mental Disease, 9, 645-663.
Purves-Stewart, J. (1927). Intracranial Tumnours, p. 105.Oxford University Press: London.
Rey-Pias, J. M. (1972). Gelastic epilepsy (laughingseizures). Schweizer Archiv fur Neurologie, Neuro-chirurgie uindPsychiatrie, 111, 29-35.
Stutte, H. (1963). Zwangsaffekte und paroxysmal Lachund Weinaus brtiche als Epilepsie-Symptom, Nerven-artz, 34, 290-295.
Trousseau, A. (1873). Clinique Medicale de l'HOtel-Dieude Paris, 4th edn, p. 409. Balliere: Paris.
Weinstein, E., and Bender, M. B. (1943). Integrated facialpatterns elicited by stimulation of the brain stem.Archives ofNeutrology andPsychiatry (Chic.), 50, 34-42.
Wilson, S. A. K. (1924). Pathological laughing and crying.Journal ofNeurology and Psychopathology, 4, 229-333.
Ziligien, H. (1906). Rire et pleurer spasmodique. RevueMedicale de l'Est, 38, 1-12.
834
Protected by copyright.
on 23 May 2018 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.39.9.829 on 1 Septem
ber 1976. Dow
nloaded from






![RESEARCHARTICLE TwoDimensionalYau-HausdorffDistance ... · 2020. 11. 26. · Wepropose heretheYau-Hausdorff distance in termsofthe minimumone-dimensional Hausdorff distance [11].TheminimumHausdorff](https://img.dokumen.tips/doc/110x75/60b2e15de50b16271d5090e5/researcharticle-twodimensionalyau-hausdorffdistance-2020-11-26-wepropose.jpg)