Embed Size (px)
Citation preview
990
DR BEHAN AND OTHERS: REFERENCES
1. Prineas, J. W. in Handbook of Clinical Neurology (edited P. J. Vincken andG. W. Bruyn); vol. IX. Amsterdam, 1970.
2. Mackay, I. R., Carnegie, P. R., Coates, A. S. Clin. exp. Immun. 1973, 15,471.
3. Lancet, 1976, i, 459.4. Oldstone, M. B. A., Dixon, F. J. in Progress in Immunology. First Interna-
tional Congress of Immunology (edited by B. Amos); p. 763. New York,1971.
5 Adams, J., Imagawa, D. Proc. Soc exp. Biol. Med. 1962, 111, 562.6. Caspary, E. A., Chambers, M. E., Field, E. J. Neurology, Minneap. 1969,
19, 1038.7. Ross, C. A. C., Lenman, J. A. R., Melville, I. D. Br. med. J. 1969, iii, 512.8. Lancet, 1974, i, 247.9. Utermohlen, V., Zabriskie, J. B. J. exp. Med. 1973, 138, 1591.
10. Ciongoli, A. K., Platz, P., Dupont, B., Svejgaard, A., Fog, T., Jersild, C.Lancet, 1973, ii, 1147.
11. Utermohlen, V., Zabriskie, J. B. ibid. p. 1147.12. Moulias, R., Goust, J. M., Remert, P., Fournal, J. T., Reville-Chabrolle, A.,
Duong, N., Muller-Berat, C. N., Berthaux, P. Nouv. Presse. méd. 1973,2, 1341.
13. Levin, A. S., Spitler, L. E., Wybran, J., Fudenberg, H. H., Hellstian, I.,Hellstian, K. E. Clin. Res. 1972, 20, 568.
14. Behan, P. O. Unpublished.15. Nelson, J. D., Sandusky, G., Peck, B. F. J. Am. med. Ass. 1966, 198, 185.16. Lennon, R. G., Isacson, P., Rosales, T., Elsea, W. R., Karzon, D. T., Win-
kelstein, W. Jr. ibid. 1967, 200, 99.17. Lawrence, H. S., Al-Askari, S. in In Vitro Methods of Cell-Mediated Im-
munity (edited by B. R. Blook and P. Glade); p. 531. New York, 1971.18. Brown, P., Cathala, F., Gajdusek, D. C., Gibbs, Jr C. J. Proc. Soc. exp. Biol.
Med. 1971, 137, 956.19. ter Meulen, V., Koprowski, H., Iwasaki, Y., Kackell, Y. M., Muller, D. Lan-
cet, 1972, ii, 1.20. Prineas, J. Science, 1972, 178, 760.21. Jersild, C., Fog, T., Hansen, G. S., Thomsen, M., Svejgaard, A., Dupont,
B. Lancet, 1973, ii, 1221.22. Schumacher, G. A. Neurology, Minneap. 1974, 24, 1010.23. Arnason, B. G. W. in Multiple Sclerosis Research: Proceedings of a Joint
Conference held by the Medical Research Council and the MultipleSclerosis Society of Great Britain and Northern Ireland (edited by A. N.Davidson, J. H. Humphrey, L. A. Liversedge, W. I. McDonald, and J. S.Porterfield). H. M. Stationery Office, 1976.
24. Lawrence, H. S. Harvey Lect. 1974, series 68.25. Vandvik, B., Froland, S. S., Hoyeraal, H. M., Stein, R., Degre, M. Scand.
J. Immun. 1973, 2, 367.26. Hughes, D., Caspary, E. A., Field, E. J. Lancet, 1968, ii, 1205.
CYSTIC FIBROSIS HETEROZYGOSITY IN THEPATHOGENESIS OF ALLERGY
J. O. WARNER A. P. NORMANJ. F. SOOTHILL
Departments of Respiratory Medicine and Immunology,Hospital for Sick Children, Great Ormond Street, and
Institute of Child Health, London WC1
Summary 47% of cystic fibrosis (C.F.) heterozy-gotes had positive prick skin tests to 1 or
more of 9 antigens and 53% had histories of allergic dis-ease, both occurring significantly more often than in acontrol group. Since 1 in 20 of the population are C.F.carriers, this would contribute considerably to allergy inthe community.
Introduction
IT has been suggested that allergy may result fromdefective antigen handling at mucous surfaces. Allergyis also associated with transient IgA deficiency,’ andhomozygosity for the cystic fibrosis (c.F.) gene.2-’ Wetherefore studied allergy in c.F. heterozygotes, identifiedas parents of c.F. patients; the calculated gene frequencyfor c.F. is 1 in 20 of the population.
Methods
47 parents of c.F. patients (22 couples and 3 mothers) andappropriate controls (friends of the parents--11 couples and3 individuals) were studied. An allergy history was obtained by
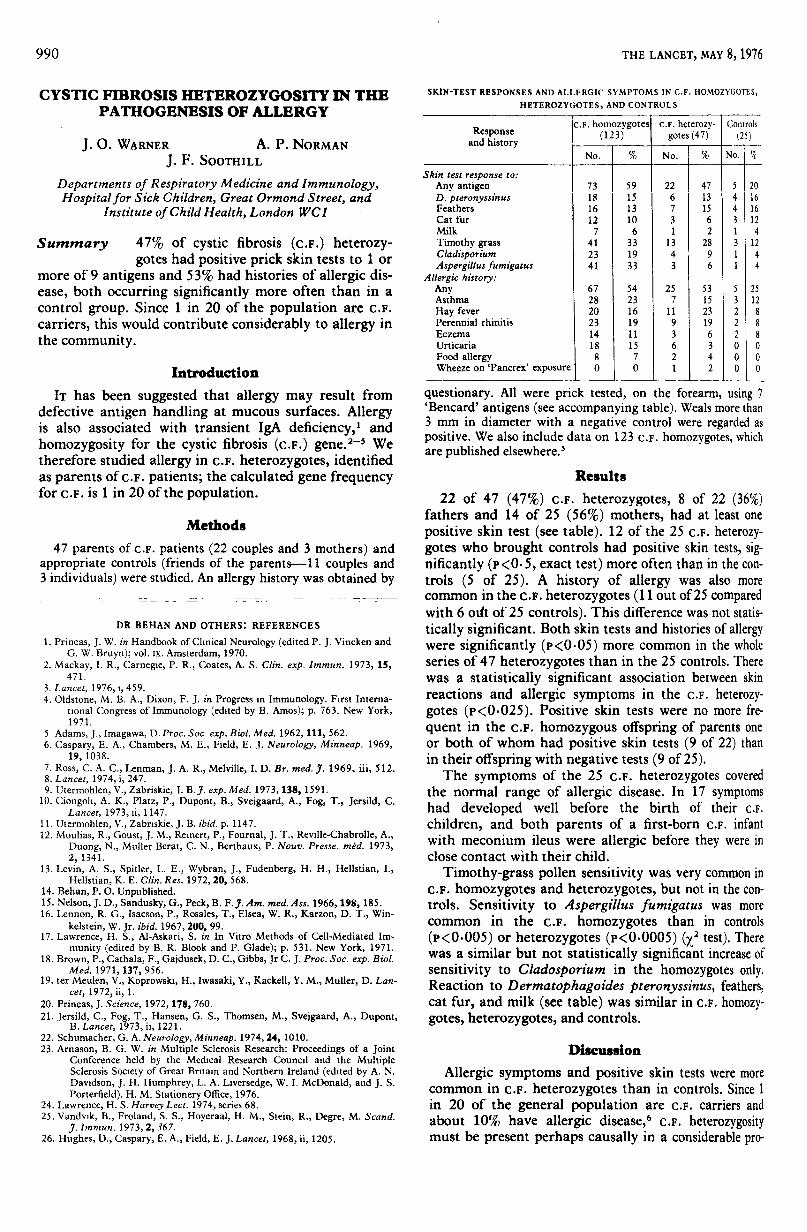
SKIN-TEST RESPONSES AND ALLERGIC SYMPTOMS IN C.F. HOMOZYGOTES,HETEROZYGOTES, AND CONTROLS
r I
questionary. All were prick tested, on the forearm, using 7’Bencard’ antigens (see accompanying table). Weals more than3 mm in diameter with a negative control were regarded aspositive. We also include data on 123 c.F. homozygotes, whichare published elsewhere.’
Results
22 of 47 (47%) c.F. heterozygotes, 8 of 22 (36%)fathers and 14 of 25 (56%) mothers, had at least onepositive skin test (see table). 12 of the 25 c.F. heterozy-gotes who brought controls had positive skin tests, sig-nificantly (P<0.5, exact test) more often than in the con-trols (5 of 25). A history of allergy was also morecommon in the c.F. heterozygotes (11 out of 25 comparedwith 6 out of 25 controls). This difference was not statis-tically significant. Both skin tests and histories of allergywere significantly (P<0.05) more common in the wholeseries of 47 heterozygotes than in the 25 controls. Therewas a statistically significant association between skinreactions and allergic symptoms in the c.F. heterozy-gotes (P<0.025). Positive skin tests were no more fre-
quent in the c.F. homozygous offspring of parents oneor both of whom had positive skin tests (9 of 22) thanin their offspring with negative tests (9 of 25).The symptoms of the 25 c.F. heterozygotes covered
the normal range of allergic disease. In 17 symptomshad developed well before the birth of their c.F.
children, and both parents of a first-born c.F. infantwith meconium ileus were allergic before they were inclose contact with their child.
Timothy-grass pollen sensitivity was very common inc.F. homozygotes and heterozygotes, but not in the con-trols. Sensitivity to Aspergillus fumigatus was morecommon in the c.F. homozygotes than in controls
(P<0.003) or heterozygotes (p<0.0005) (X2 test). Therewas a similar but not statistically significant increase ofsensitivity to Cladosporium in the homozygotes only.Reaction to Dermatophagoides pteronyssinus, feathers,cat fur, and milk (see table) was similar in c.F. homozy-gotes, heterozygotes, and controls.
Discussion
Allergic symptoms and positive skin tests were morecommon in c.F. heterozygotes than in controls. Since 1in 20 of the general population are c.F. carriers andabout 10% have allergic disease,6 c.F. heterozygositymust be present perhaps causally in a considerable pro-

991
portion of allergic patients. Counahan and Mearns’ 7found no increase in skin sensitivity in 53 relatives ofc.F. patients, but they included sibs who may not havebeen c.F. heterozygotes and they did not test with grasspollen.Contact with the c.F. homozygote was probably not
the cause of the allergy in the heterozygotes, becausesymptoms occurred in most before their c.F. childrenwere born. The c.F. heterozygotes were sensitive to asimilar range of antigens as the controls, and differedfrom the homozygotes in whom mould allergy was pre-dominant, so the predisposition is apparently not
antigen specific. Though allergy is familial," allergy wasno more common in parents of allergic c.F. patients thanin those with non-allergic c.F. children, so the associ-ation is probably not due to a simple genetic link.Most c.F. heterozygotes have serum factors which in-
hibit cilial activity, II 1U though to a lesser extent than inmost homozygotes. Such a defect could result in inade-quate antigen clearance from mucous surfaces, leadingto allergy if the appropriate environmental exposureoccurs, as suggested for IgA deficiency. 1
Allergy tests could be of some use in screening for c.F.carriers, allergic people having more detailed tests forc.F. heterozygosity. This suggestion is supported by thestudy of Caplin and Haynes" who found that 14 of 27aspirin-sensitive asthmatics had a se,rum cilial inhibitoryfactor, and all 27 had a salivary inhibitory factor whichwas also found in c.F. patients and their parents.We thank the Joint Research Board of this Hospital and Institute
for support for J.0. W.
Requests for reprints should be addressed to J.O.W.
REFERENCES
1.Taylor, B., Norman, A. P., Orgel, H. A., Stokes, C. R., Turner, M. W.,Soothill, J. F. Lancet, 1973, ii, 111.
2. Mearns, M., Longbottom, J. L, Batten, J. ibid. 1967, i, 538.3. Warren, C. P. W., Tai, E., Batten, J C., Hutchcroft, B. J., Pepys, J. Clin.
Allergy, 1975, 5, i.4. Allan, J. D., Moss, A. D., Wallwork, J. C., McFarlane, H. ibid. P. 255.5. Warner, J. O., Taylor, B , Norman, A. P., Soothill, J. F Archs Dis. Childh.
(in the press).6 Blair, H. Clin. Allergy, 1974, 4, 389.7. Counahan, R., Mearns, M. B Archs Dis. Childh. 1975, 50, 477.8. Smith, J. M. Med. Clins N. Am 1974, 48, 3.9. Spock, A., Heick, H. M C., Cress, H., Logan, W. S. Pediat. Res. 1967, 1,
173
10. Besley, G.T. N., Patrick, A. D., Norman, A. P. J. med. Genet. 1969, 6, 278.11 Caplin, I., Haynes, J. T. Ann. Allergy, 1973, 31, 320.
POSSIBLE DUAL ROLE FOR VASOACTIVEINTESTINAL PEPTIDE AS
GASTROINTESTINAL HORMONE ANDNEUROTRANSMITTER SUBSTANCE
M. G. BRYANT S. R. BLOOMJ. M. POLAR R. H. ALBUQUERQUEI. MODLIN A. G. E. PEARSE
Departments of Medicine, Surgery, and Histochemistry, RoyalPostgraduate Medical School, Hammersmith Hospital,
London W12
Summary Vasoactive intestinal peptide (V.I.P.) hasbeen found in high concentrations both
in the gastrointestinal tract and, unexpectedly, in thecentral nervous system. Immunocytochemical studieshave demonstrated V.I.P. in nerve-fibres. These findingschallenge the concept of V.I.P. as a simple gastrointes-
tinal hormone and suggest a possible neurotransmitterfunction.
Introduction
VASOACTIVE intestinal peptide (v.i.p.), isolated frompig small intestine,’ has been included in a list of candi-date hormones of the gut by Grossman.2 v.i.p. has asimilar aminoacid sequence3 and pharmacology4 to twoclassical hormones, secretin and glucagon. Its numerouspowerful actions include systemic vasodilation, stimula-tion of myocardial contractility,’ glycogenolysis,5 lipo-lysis, stimulation of insulin secretion, inhibition of gas-tric-acid production, stimulation of alkaline pancreaticjuice now/ and stimulation of small intestinal cyclicadenosine monophosphate and juice secretion.7We have previously reported the development of a
specific radioimmunoassay for v.i.p.,8 and have shown itto be widely distributed throughout the gastrointestinaltract of all species studied, occurring in high concentra-tions from oesophagus to rectum.1I A parallel distributionof v.i.p.-producing cells in the gut mucosa was alsoobserved. 10 High levels of circulating plasma-v.i.p. havebeen found in patients with ganglioneuroblastomas.11This finding and reports of possible neurotransmitterfunction of endocrine peptides from cells of the AminePrecursor Uptake and Decarboxylation (APUD)series,12 including substance P 13 and somatostatin, 14suggested the need for a full survey of the quantity anddistribution of v .I.P. in human and animal tissues, anda precise morphological definition of its localisation.
Materials and Methods
Tissue from mice, rats, and pigs was removed immediatelyafter death. Human brain tissue was obtained 8 h after deathand samples of normal human bowel, adrenals, pancreas, andsalivary glands were collected during surgery. Four neuraltumours, removed surgically from patients with the waterydiarrhoea syndrome, were also examined. All tissues were keptdeep-frozen until the time of extraction. For immunoassay,each region was boiled for 10 min in water (5 mVg wet tissue),centrifuged, and the sediment homogenised in 5 ml/g of 0- lAfformic acid and allowed to extract for half an hour. The celldebris was removed by centrifugation and, to ensure full recov-ery, further extracted with 4 ml/g O.lM formic acid. Thesupernatants were pooled before the assay. For immunocyto-chemistry, tissues were immediately quenched in ’Arcton’
(freon 22) at -156°C and then freeze-dried in a thermoelectricfreeze-drier and vapour-fixed.15
Antisera to pure porcine v.i.p. were raised in rabbits by con-ventional immunisation procedures. Two antisera were used forassay, one reacting preferentially with the C-terminal and theother with the N-terminal end of v.i.p. Both were used at afinal dilution of 1/240 000. Radioactive label was prepared byenzymatic iodination, with lactoperoxidase and iodine-125,and was purified by high-resolution ion-exchange chromato-graphy to yield pure monoiodinated v .I.P .16 The assay coulddetect 5 pg v.i.p. per tube using pure porcine v.i.p. as stan-dards. There was no cross-reactivity with secretin, glucagon,gastric inhibitory peptide (G.I.P.), motilin, gastrin, or cholecys-tokinin. All extracts were assayed in ten-fold serial dilutions.
Immunocytochemistry was carried out by an indirectmethod.17 Numerous controls were performed including priorabsorption of the antibodies with pure natural v.i.p.
Column ChromatographyExtracts (1 - 5 ml) were chromatographed on a 1 x 90 cm gel-
column by means of ’Sephadex G50 superfine’ eluted with0-IM formic acid at 7.5 ml/h. The column was precalibrated





























