Embed Size (px)
Citation preview

Cystic fibrosis gene therapy . William H Colledge
Wellcome/CRC Institute of Cancer and Developmental Biology and University of Cambridge, Cambridge, UK
A variety of cystic fibrosis gene therapy approaches based on viral (adenovirus, retrovirus, and adeno-associated virus) and non-viral (liposomes and receptor-mediated endocytosis) routes are currently being assessed for safety and efficacy. Of these, the trials involving liposomal and adenoviral vectors are the most advanced, as both have been shown to correct the cystic
fibrosis Cl- conductance defect in vivo.
Current Opinion in Genetics and Development 1994, 4:466-471
Introduction
Cystic fibrosis (CF) is a fatal autosomal recessive ge- netic disorder affecting approximately 4% of Caucasi- ans with over 50000 affected individuals world wide. The disorder is characterized by a variety of symp- toms, including hyper-accumulation of mucus in the lungs and gastrointestinal tract, reduced ability to di- gest and absorb duodenal contents because of pancre- atic enzyme insufficiency, male sterility and elevated salt levels in the sweat. The major cause of morbid- ity is gradual lung destruction, induced by severe in- flammatory reactions elicited in response to microbial colonization of the airway mucus. The current life ex- pectancy is about 27 years.
The gene responsible for CF, the cystic fibrosis trans- membrane conductance regulator gene (C~“7?)11,21, encodes an apical Cl- channel 13-51 that is regulated by cAhIP-dependent protein kinase phosphoxylation and nucleoside triphosphate binding [61. The CAMP- regulated Cl- conductors are absent or severely re- duced in epithelia from CF patients, contributing to increased fluid absorption 171 and excessive dehydra- tion of luminal mucus.
Current treatments are aimed at alleviating the symp- toms rather than correcting the genetic defect; these include daily physiotherapy to assist with airway clear- ance and antibiotic administration to combat respira- tory infections. Unfortunately, the emergence of resis- tant strains makes necessary the continuous develop- ment of new antimicrobial drugs. It is now possible, however, to attempt clinical improvement by a gene therapy route [Sl, that is, the delivery of a functional 07X gene and expression in somatic cells to correct the genetic defect and restore Cl- channel function.
Animal models
Animal models are crucial in the development of an ef- fective gene therapy treatment for CF, as they allow the feasibility, efficiency and safety of the various strategies to be evaluated. Several groups have now generated mutant mice that possess characteristics of CF [!J-151; these include the absence or reduction of a c&VIP-ac- tivated Cl- channel and hyper-accumulation of mucus in the gastrointestinal tract. The latter causes intestinal obstructions in newborn pups very similar to the fecal blockages (meconium ileus) found in some CF neo- nates. The CF mice that completely lack a functional cftr Cl- channel can be used as a sensitive electro- physiological indicator of the effectiveness of a gene therapy strategy.
Initially, none of the CF mice was reported to develop spontaneously the high incidence of lung pathology that is the hallmark of CF in humans. Recently, how- ever, one of the CF mouse models has been shown to have reduced mucociliary clearance of Stuplylococ- cw aureus following lung infection [l61 and to de- velop major lung pathology after chronic exposure to Pseudomonas aeroginosa or P. cepacia (J Dorm, personal communication). It will be interesting to see whether lung degeneration continues once exposure is stopped. If this is the case, then these mice will be invaluable for testing the effectiveness of a therapy in alleviating lung pathology.
In addition to the knockout animal models, a xenograft system has also been developed to study gene transfer based on epithelial recolonization of a denuded tra- chea implanted subcutaneously in the flank of a rat 1171. This system is particularly useful for studying the effect of epithelial cell proliferation on gene therapy delivery and expression.
466
Abbreviations MV-adeno-associated virus; Ad-adenovirus; CF+ystic fibrosis; CFTR-cystic fibrosis transmembrane conductance regulator gene.
0 Current Biology Ltd ISSN 0959-437X

Cystic fibrosis gene therapy Colledge 467
Gene therapy delivery routes
The demonstration that transfection of a CF77? cDNA could correct the cAMP-regulated Cl- channel defect in CF epithelial cells in culture suggested that similar expression in the airways and intestinal tract of CF pa- tients could represent a strategy for treatment. As lung deterioration is responsible for the major morbidity of the disease, it is the primary target of gene therapy. For- tunately, the lungs represent a relatively accessible site for gene delivery by either aerosol inhalation or lavage.
A variety of CF gene delivery systems are currently be- ing developed and tested. These are broadly based on either viral vector routes 1181 or a non-viral liposomal route 1191 (Fig. 1). For both adenovirus and liposomes, phase I clinical trials have been initiated to assess their safety and feasibility for gene delivery.
Adenovirus An adenovirus contains a 35 kb double-stranded DNA genome. Viral replication requires expression of sev- eral early genes, which are transcriptionally activated
by the ElA protein. Expression vectors typically delete this region (and sometimes the E3 region) and place the exogenous gene under the control of the ElA pro- moter, which is active immediately after viral infection. Consequently, recombinant viruses cannot replicate unless the ElA protein is supplied by a helper cell line, such as a human embryonic kidney line (293 cells).
Adenoviruses have many characteristics that make them suitable for gene therapy 120,211; they are trophic for the epithelium of the respiratory tree, can be pro- duced in high titres and will very efficiently infect non-replicating epithelial cells. They do not normally integrate (less than 1%) thus minimizing the risk of in- sertional mutagenesis. The risk exists, however, that a replication-competent infectious virus could be gen- erated by recombination either with the ElA region present in the helper line or with a ubiquitous wild- type virus. Either way, the introduction of wild-type adenovirus into the compromized lungs of CF patients could trigger pulmonary exacerbations that would be extremely undesirable.
Adenovectors are very efficient at infecting all major categories of airway epithelial cells. Mastrangeli et al.
Blood vessel endothelial cells
Putative epithelial stem cell
lumen delivery Bloodstream delivery
4J
/ I \ Receptor- I I Basement Nucleus Epithelial mediated Apical BasoL
membrane ccl I endocytosis face face
@ 1994 Current Opinion in Genetics and Development
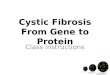
Fig. 1. Possible delivery routes for cystic fibrosis gene therapy. Schematic cross-section of a lung airway illustrating the inter-relationship between cell types and routes of virus- and liposorne-mediated gene therapy delivery. Direct access to the apical face of the airway epithelial cells can be achieved via the airway lumen, but the possibility exists that a bloodstream route could also deliver DNA into the epithelial cells if blood vessel endothelial cells and the basement membrane layer can be traversed. Specific receptor molecules located on the apical surface of epithelial cells can be used to improve the efficiency and specificity of liposome-mediated gene delivery.

468 Genetics of disease
1221 detected LacZ expression in 40% of ciliated and se- cretory epithelia and 3% of basal and undifferentiated cells after Ad(I.acZ) infection of cotton rat lungs. An adenovector has been used to express human CFTR in the lung epithelium of cotton rats 1231. Localized ap- plication of Ad(ClG?Q to the nasal epithelia of three CF patients corrected the defective cAMP-stimulated Cl- channel with no serious inflammatory reactions or evidence of viral replication 124”l. In this study, only a single dose of virus was administered. It is not yet known how often Ad(CKrZ?) would have to be applied to the airways of CF patients to give clini- cal benefit. Repeated treatments might elicit an adverse immune response and thus limit this gene therapy ap- proach. In a recent study, Zabner et al. 125’1 assessed the safety of repetitive Ad(CK?@ application to the air- ways of cotton rats and to the nasal epithelia of Rhesus monkeys and found no evidence of a local or systemic inflammatory response after repeat administration. It is possible that immune reactions are ameliorated by the adenovirus E3 region, which has been shown to sup- press the host immune response 1261.
Recently, Yoshimura et al. 1271 have shown that plas- mid DNA can be co-introduced into cells during aden- ovirus infection. This represents a novel route for the delivery of two different Cm expression vectors into the same epithelial cell and may improve gene delivery efficiencies.
Adeno-associated virus The adeno-associated virus (AAV) is a single-stranded DNA virus which requires co-infection with adenovirus to replicate. In the absence of replication, MV under- goes high frequency integration usually into a specific site on chromosome 19. The 4.7 kb AAV genome con- sists of two coding regions, rep and cap, flanked by inverted terminal repeats required for replication and packaging. The small size of AAV means that practically all of the coding region must be removed to accom- modate large genes, such as Cm. Fortunately, the inverted terminal repeat region has endogenous pro- moter activity allowing a recombinant G77? MV to be generated that can complement the CF defect in a human bronchial epithelial line 128*,291. Animal tri- als have now been initiated to assess the effectiveness of this vector in vim
One advantage of AAV is its natural tropism for epi- thelial cells of the respiratory and gastrointestinal tract; 6O-70% of airway epithelial cells can be stably trans- formed in vitro 1301. In addition, MV can be produced in high titres and the wild-type virus is non-pathogenic. Integration into a preferred chromosomal location low- ers the risk of insertional mutagenesis. The develop- ment of a packaging line will simplify propagation and reduce the risk of inadvertently introducing adenovirus with the recombinant MV.
Retrovirus Retroviruses contain a single-stranded RNA genome that is converted into proviral DNA by reverse transcriptase before integration into the host genome. The viral genome consists of three genes, gag, PO/ and env, sandwiched between two long terminal re- peat sequences. The viral genes can be replaced with a foreign gene, such as CFTR, expressed from either its own promoter or a promoter present in the long termi- nal repeat 1311. Infectious virions are produced using a packaging helper cell line that provides the gab, pal and env proteins in trans.
The advantage of using retroviruses is that their biol- ogy is well understood and they have already been approved and used in gene therapy trials for human adenosine deaminase deficiency 1321. Their ability to integrate into the host genome means that they might also be suitable for targeting epithelial stem cells to give long-term expression of CK?!? in daughter cells 133,341 (Fig. 1). A recombinant C’ retrovirus has been shown to restore the cAhW-regulated Cl- con- ductance after infection of a CF pancreatic adenocar- cinema cell line 131.
A major limitation of retroviral vectors is the require- ment for proliferating cells to allow proviral integra- tion and expression. As lung epithelial cells are ter- minally differentiated and predominantly post-mitotic, they represent an inappropriate target cell for retroviral infection. Using the tracheal xenograft animal system, Engelhardt et al. 1171 have shown that the efficiency of retroviral gene transfer of a LacZ reporter gene drops from 5-10% in a proliferating epithelium to 0% in a fully differentiated epithelial layer. Another problem with retroviral vectors is the relatively low titres, typically 105-107ml-1. This problem could be reduced by using retroviral vectors that carry enve- lope glycoproteins with a higher affinity for cell surface receptors than the usual amphotrophic envelope glyco- proteins. Bayle et al. [351 found that retroviruses with gibbon ape leukaemia virus envelope proteins infected primary monkey epithelial cells with lo-fold more ef- ficiency than murine amphotrophic retrovirus.
Liposomes Liposomes consist of a phospholipid bilayer arranged into a spherical micelle. The majority of liposomes used in CF gene therapy studies are cationic and therefore charge-interact with DNA and the cell surface. Follow- ing adsorption to the cell surface and membrane fu- sion, the DNA is delivered inside the cell. Liposomes can be administered into the lungs as an aerosol 1361, by direct lavage or following intravenous injection (Fig. 1). After intravenous injection, liposomes appear to be retained selectively in the organs of the reticuloendo- thelial system, so this route of administration is ideal for targeting the lungs 137.1. Indeed, several groups have delivered plasmid DNA to the lungs by intravenous in- jection of a liposome-DNA complex. In some cases,

Cystic fibrosis gene therapy Colledge 469
expression of a reporter gene, such as chloramphenicol acetyl transferase 1381 or human growth hormone 1391, was detected in the lungs, but no discrimination was made in these studies between expression in blood vessel endothelial cells and lung cells. Intuitively, one might not expect liposomes to transverse the blood vessel wall, but Zhu ef al. 137.1 detected chloram- phenicol acetyl transferase immunohistochemically in bronchiolar epithelia and alveolar cells after a single intravenous liposome injection.
The advantage of using liposomes is that DNA is de- livered through a non-viral vector and is thus inca- pable of propagation in animal cells. Liposomes can be formulated to contain hydrolyzable bonds to gen- erate biodegradable molecules after cell fusion. Exten- sive safety trials have been performed on pigs, rabbits and mice to demonstrate that liposomes are non-toxic 1401, non-immunogenic 1411 and do not deliver plasmid DNA to the gonads.
Liposomes are a relatively inefficient vehicle for gene delivery. Even under optimum conditions, only about 5% of primary epithelial cells are transfected. This is probably not a major concern for CF gene therapy, as it appears that as few as 6% of cells in an ep- ithelial sheet need express C’ to generate normal Cl- currents. Much of the DNA delivered by liposomes is degraded by lysosomal enzymes. Techniques to re- duce this, such as encapsulation of certain anti-lyso- somal viral proteins, might increase the efficiency of liposome-mediated gene delivery.
The feasibility of using liposomes for CF gene ther- apy has been clearly illustrated by two groups us- ing CF animal models. Hyde et al. 142”l delivered a liposome-Cm expression plasmid complex into the lungs of CF mice by direct tracheal instillation, whereas Alton ef al. 143’1 aerosolized the complex. In both cases, a cAMPregulated Cl- channel was re- stored to the upper airways, Alton et al. 143.1 also managed to partially correct the Cl- transport defect in the intestine following rectal delivery. Hyde ef al. 142a*l used in situ hybridization to demonstrate that the plasmid was delivered deep into the lungs, both to small airway epithelial cells and to type II alveolar cells.
Receptor-mediated endocytosis Several strategies are now being developed to intro- duce CF7R plasmid DNA into lung epithelial cells us- ing receptor-mediated endocytosis pathways. In this approach, the DNA is attached to a molecule that will bind to specific cellular receptors and be internal- ized by endocytosis or phagocytosis (Fig. 1). Targeting can be restricted to specific cells if they express the appropriate receptor molecule. Proposed delivery sys- tems include complexing the DNA with transferrin 1441, adenoviral coat protein 1451, or both 1461, bacterial pro- teins internalin and invasin 1471, or antibodies directed against cell surface markers 1481.
Conclusions
The past year has seen exciting and hopeful progress towards the development of an effective gene ther- apy treatment for CF. Liposomes have been used to demonstrate, using animal models, that the Cl- chan- nel defect can be repaired by gene therapy fn vim An adenoviral vector was shown to restore the C’ Cl- channel after infection of nasal epithelia in humans. In addition, a variety of other viral and non-viral deliv- ery systems are currently being tested and refined. Which of these approaches is finally adopted for use in CF patients will depend upon the results of ongoing clinical trials. Safety aspects, such as possible adverse immunological reactions and toxic side-effects, need to be assessed further, as well as the minimum frequency of treatment required to provide clinical benefit. Given the global research effort in this field, however, it is likely that within the next five years an effective CF gene therapy will be available to patients to comple- ment existing treatment.
References and recommended reading
Papers of particular interest, published within the annual period of review, have been highlighted as: . . .
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
of special interest of outstanding interest
Rommens JM, Iannuzzi MC, Kerem B-S, Drumm ML, Melmer G, Dean M, Rozmahel R, Cole JL, Kennedy D, Hid&a N, et al.: Identification of the Cystic Fibrosis Gene: Chromosome Walking and Jumping Scfence 1989, 245:105%1065. Riordan JR, Rommens JM, Kerem BS, Alon N, Rozmahel R, Grizelczak 2, Zieienski J, Lox S, Piavsic N, Chou J-L, et al.: Identification of the Cystic Fibrosis Gene; Cloning and Characterization of Complementary DNA. Sctence 1989, 24510661073. Drumm ML, Pope HA, Cliff WH, Rommens JM, Marvin SA, Tsui LC, Collins FS, Frizzell RA, Wilson JM: Correction of the Cystic Fibrosis Defect In Vihu by RetrovirusMediatcd Gene Transfer. Cell 1990, 62:1227-1233. Gregory RJ, Cheng SH, Rich DP, Marshall J, Paul S, Hehir K, Ostedgaard L, KRnger KW. Welsh MJ, Smith AE: Expression and Characterization of the Cystic Fibrosis Transmcmbranc Conductance Regulator. Natrrre 1990, 347:382-386. Tabcharani JA, Rommens JM, Hou Y-X, Chang X-B, Tsui L-C, Rio&n JR, Hanraham JW: Multi-Ion Pore Behaviour in the CFTR Chloride Channel. Natnre 1993, 366:79-82. Rio&n JR: The Cystic Fibrosis Transmembrane Conduc- tance Regulator. Annu Rev Pbysiol 1993, 55609-630. Jiang C, Finkbeiier WE, Widdicombe JH, McCtay PB, Miller SS: Altered Fluid Transport Across Airway EpitheRum in Cys tiwFibrosis. Science 1993, 262:424-427. Mulligan RC: The Basic Science of Gene Therapy. Science 1993, 260:926-932. Snouwaert JN, Brigman KK, Iatour AM, Malouf NN, Boucher RC, Smithies 0, Koller BH: An Animal Model for Cystic Fibrosis Made by Gene Targeting. Scfence 1992, 257:1083-1088. Clarke LL, Grubb BR, Gabriel SE, Smithies 0, KoEer BH, Boucher RC: Defective Epithcliai Chloride Transport in a Gene-Targeted Mouse Model of Cystic Fibrosis. Science 1992, 257:1125-1128.

470 Genetics of disease
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24. . .
Dorin JR, Dickinson P, AIton EWFW, Smith SN. Geddes DM, Stevenson BJ, Kimber WL. Fleming S, Clarke AR, Hoopcr ML er al.: Cystic Fibrosis in the Mouse by Targeted Inscr- tionai Mutagenesis. Narztre 1992, 359:211-214.
Colledge WI-I, Ratcliff R. Foster D, Williamson R, Evans MJ: Cystic Fibrosis Mouse with Intestinal Obstruction. Lancer 1992, 340680.
Ratcliff R, Evans MJ, Cuthben AW, MacVinish LJ, Foster D. Anderson JR, Colledge WH: Production of a Scvcrc Cystic Fibrosis Mut+tion in Mice by Gene Targeting. Nuhrre Gener 1993, 4:3%41.
VaIverde MA, O’Brien JA. Sepulveda FV, Rat&f R, Evans MJ, Colledge WH: Inactivation of the Murinc cftr Gene Abol- ishes cAMP-Mediated But Not Caz+-Mediated Sccrctagoguc- Induced Volume Dccrcasc in Small-Intestinal Crypts. Pfllrgets Arch 1993, 425:434-438.
O’NcaI WK, Hasty P, McCray PB Jr, Casey B, Rivera-Perez J, Welsh MJ, Beaudet AL., Bmdley A: A Scvcrc Phcnotypc in Mice with a Duplication of Exon 3 in the Cystic Fibrosis Locus. Hum Mol Gene1 1993, 2:1561-1569.
Porteous DJ: Cystic Fibrosis in the Mouse and Progtcss To wards Gene Therapy. In Clinfcal Ecology of C’ffc Ffbrosfs. Edited by Escobar H, Baquero CF, Suarez L. New York: Elsevier Science Publishers; 1993:27-31.
Engelhardt JF, Yankaskas JR, Wilson JM: In V&o Rctroviral Gene Transfer into Human Bronchial EpithcIia of Xenografts. J Clin Intk?st 1992, 90:259%2607.
Flotte TR: Prospects for Virus-Based Gene Therapy for Cystic Fibrosis. J Bionerg Biomembr 1993, 2537-42.
Hazinski TA: Gene Transfcction of Lung Cells In V&o and In Vfw. Anmc Rev Pbpiol 1993, 55:181-207.
Siegfried W: PrrspcctIvcs in Gene Therapy with Rccombi- nant Adcnoviruscs. Erp Clfn Endocrinol 1993, 101:7-11.
Kozarsky KF. Wilson JM: Gene Therapy: Adcnovirus Vectors. CWY Opin &net Lku 1993. 3~499-503.
Mastmngeli A, Dane1 C, Rosenfeld MA, Stratford-Perricaudet L, Penicaudet M, PavIrani A, Lccocq J-P, Crystai RG: Divcr- sky of Airway EpithcIiaI CcII Targets for In Vfw Rccombi- nant AdenovriusMcdiatcd Gcnc Transfer. J Clfn Invest 1993, 91:225234.
Roscnfeld MA, Yoshimura K. Trapnell BC, Yoneyama K. Rosenthal ER, Dalemans W, Fukayama M, Bargon J, Stier LE, Stratford-Perricaudet L. et al.: In VIw Transfer of the Hu- man Cystic Fibrosis Transmcmbranc Conductance Regulator Gcnc to the Airway EpithcIium. Cell 1992. 68:143-155.
Zabner J, Couture LA, Gregory RJ, Graham SM, Smith AE, Welsh JM: Adcnovirus-Mediated Gene Transfer Transiently Corrects the Chloride Transport Defect in Nasal Epithclia of Patients with Cystic Fibrosis. Cell 1993, 75:207-216.
A very encouraging first demonstration that gene therapy can be used to correct the Cl- transport defect in the nasal epitheha of CF pa- tients. Application of a recombinant Ad(CnR) vector improved the basal transepitheliai voltage across the nasal epithelia and restored the response to a CAMP agonist. No serious inflammatory responses were found or any evidence of viral replication.
25. Zabner J, Petersen DM, Puga AP, Graham SM, Couture LA, . Keyes LD, Lukason MJ, St George JA, Gregory RJ, Smith
AE, Welsh MJ: Safety and Emcacy of Repetitive Adcnovirus Mediated Transfer of CFTR cDNA to Airway Epithclia of Primates and Cotton Rats. Nature Genef 1994, 6:75-83.
A report on the safety of repetitive delivery of an Ad(Cm vector to the airway epitheha of cotton rats and Rhesus monkeys, showing no evidence of a local or systemic infIammatory responses.
26. Weld WS, Gooding LR: Region E3 of Adcnovirus a Gas- scttc of Gcncs Involved in Host Immunosurvcillancc and Vis-Ccl1 Interactions. Mro/ogy 1991, l&1:1-8.
27. Yoshirnura K, Rosenfeld MA, Seth P, Crystal RG: Adcnovirus- Mediated Augmentation of CcII Transfcction with Unrnodi- tied Plasmid Vectors. J Biol Chem 1993, 268:230&2303.
28. Flotte TR, Aftone SA, Solow R, Drumm ML, Markakis D, . Guggino WB, Zeitlin PL, Caner BJ: Expression of the Cys-
tic Fibrosis Transmcmbranc Conductance Regulator from a Novel AdcnoAssociatcd Virus Promoter. J Biol Chem 1993, 268:3781-3790.
Description of a recombinant CI7R adeno-associated virus (AAV) currently being assessed as a gene therdpy vehicle. The AAV(Cb7Rl vector can produce increased levels of CFTR protein imrnunofluo- rcscence and a cAMP-regulated Cl- efflux in infected cells.
29.
30.
31.
32.
33.
34.
35.
36.
37. .
Egan M. Flotte T, Afione S, Solow R, Zeitlin PL. Carter BJ, Guwion WB: Defective Regulation of Outwardly Rectifying Cl- Channels by Protein Kinasc A Corrected by Insertion of CITR. Narrtre 1992, 358581-584.
Flotte TR, Solow R, Owens RA, Aiione S, Zeitiin PL, Carter BJ: Gene Expression from AdcnoAssociated Virus Vectors in Airway Epithclial Cells. Am J Rap Cell Mol Biol 1992, 7:349-356.
Boris-Lawrie KA. Temin HM: Recent Advances in Retrovirus Vector Technology. Crcrr Opin Genef Dev 1993, 3:102-109.
FIcischman RA: Human Gene Therapy. Am J Med Sci 1991, 301:353363.
Olsen JC, Johnson LG, Stutts MJ. %Irkadi I~, Yankaskas JR, Swanstrom R. Boucher RC: Correction of the Apical Mcm- branc Chloride Pcrmcability Defect in Polarized Cystic Fi- brosis Airway Epithclia Following Rctrovirai-Mediated Gene Transfer. Hum Gene 77~ 1992, 3:253266.
Olsen JC, Johnson LG, Wong-Sun ML, Moore KL, Swanstrom R, Boucher RC: Rctrovirus~Mcdiatcd Gene Transfer to Cystic Fibrosis Airway Epithcliai Cells: Effect of Sclcctablc Marker Sequences on Long-Term Expression. Nrrclefc Acids Res 1993, 21663-669.
Bayle J-Y, Johnson LG, St George JA, Boucher RC, Olsen JC: High-Efficiency Gene Transfer to Primary Monkey Airway Ep ithclial CcUs with Rctrovints Vectors Using the Gibbon Apt Leukemia Virus Receptor. Hum Gene 7her 1993, 4:161-170. Stribling R, Brunette E, Liggit D, Gaensler K, Debs R: Aerosol Gene Dclivcry In Vfw. Proc Nut1 Acad Sci USA 1332, 89:11277-11281.
Zhu N. Liggit D, Liu Y, Debs 1~: Systemic Gene Expression After Intravenous DNA DcIivery into Adult Mice. Science 1993, 261:209-211.
An interesting paper describing liposome-mediated gene delivery and expression in the lungs of mice following intravenous injec- tion. This could represent an alternative delivery route for CF gene therapy.
38.
39.
40.
41.
42. . .
Brigham KL, Meyrick B, Christman B, Magnuson M, King G, Berry LC: In Vfw Transfcction of Murinc Lungs with a Functioning Prokaryotic Gene Using a Liposomc Vehicle. Am J Med Sci 1989. 298:278-281.
Brigham KL, Meyrick B, Christman B, Canary JT, King G, Berry LC. Magnuson MA: hprcssion of Human Growth Hormone Fusion Genes in Cultured Lung Endothelial Cells and in the Lungs of IMice. Am J Resp Cell Mol Biol 1993, 8:209-213.
Stewart MJ, Plautz GE, Buono LD, Yang ZY, Xu L, Gao X, Huang L, Nabel EG, Nabel GJ: Gene Transfer In Vfw with DNA-Liposomc Complexes: Safety and Acute Toxiciry in Mice. Hum Gene 7hr 1992, 3:267-275.
Nabcl EG, Gordon D, Yang Z-Y, Xu L, San H, Plautz GE, Wu B-Y, Gao X, .Huang L, Nabel GJ: Gene Transfer fn Vfw with DNA-Liposomc Complcxcs: Lack of Autoimmunity and Gonadal Localization. Hum Gene l&r 1992. 3:649-656.
Hyde SC. Gill DR, Higgins CF, Trezise AEO, MacViiish LJ, Cuthbert AW, Ratcliff R, Evans MJ, Colledge WH: Correction

Cystic fibrosis gene therapy Colledge 471
of the Ion Transport Dcfcct in Cystic Fibrosis Transgcnic Mice by Gcnc Therapy. Nafzrre 1993, 362:25&254.
The first demonstration that the CF Cl- transpon defect can be cor- rected In oiuo by gene therapy. Liposomes were used to deliver a UTR expression plasmid deep into the lungs of a CF mouse lead- ing to the correction of ion conductance defects in the trachea. In slfn hybridization detected pkismid in all five lobes of the lungs and both small airway epithelial cells and type II alveolar cells were trans- fected.
43. Alton EWFW, Middleton PG. Caplen NJ, Smith SN, Steel DM, . Munkonge FM, Jeffery PJ, Geddes DM, Hart SL, Wiiliamson
R. et al.: Non-Invasive Liposomc-Mediated Gene Dclivcry can Correct the Ion Transport Dcfcct in Cystic Fibrosis Mutant Mice. Nature Gene1 1993, 5:135-142.
Correction of the Cl- transport defect in the airways of a CF mouse following aerosol delivery of a liposomal C!77? expression plasmid. An aerosol delivery method would represent an ideal route for hu- man CF gene therdpy because it is non-invasive.
44. Curie1 DT, Agarwai S. Romer MU, Wagner E, Cotten M, Birn- stiel ML, Boucher RC: Gcnc Transfer to Respiratory Epithclial Cells via the Receptor-Mediated Endocytosis Pathway. Am / Resp Cell Mel Btol 1992, 6~247-252.
45. Curie1 DT, Wagner E, Cotten M, Birnstiel ML, Agarwal S, Li CM, Loechel S, Hu PC: High-Efficiency Gene Transfer Medi- ated by Adcnovirus Coupled to DNA-Polylysiie Complacs. Hum Gene 7&r 1992, 3:147-154.
46. Wagner E. Zatloukal K, Cotten M, Kirlappos H, Mechtler K, Curie1 DT. Bimstiel ML: Coupling of Adcnovirus to Transfcrrin-Polylysinc/DNA Complcxcs Greatly Enhances Receptor-Mediated Gcnc Dclivcry and Expression of Trans fccted Genes. Proc Nat1 Acad Scf USA 1992, 896099-6103.
47. Coutelle C, Caplen N, Hart S, Huxley C, Wiiliamson R: Gene Therapy for Cystic Fibrosis. Arch Dls Child 1993, 68:437443.
48. Wang C-Y, Huang L: pH-Sensitive lmmunoliposomcs Mediate TargetCell-Specific Dclivcry and Controlled Expression of a Foreign, Gene in Mouse. Proc Nat1 Acad Scf USA 1987, 84:7851-7855.
WH Colledge, Wellcome/CRC Institute of Cancer and Developmental Biology, and Department of Genetics, University of Cambridge, Tennis Court Road, Cambridge CB2 IQR, UK.