Embed Size (px)
DESCRIPTION
cvs imaging
Citation preview
CARDIOVASCULAR
IMAGING
LEVEL V MBCHB
BY DR ONYAMBU
LECTURER DDIRM

Objectives
Know the different imaging modalities
used in imaging the CVS
Understand the clinical application of
each modality
Understand the best imaging modality for
each clinical indication

IMAGING MODALITIES
Plain CXR-PA,LAT
Echocardiography
Isotope scanning
Cardiac catheterisation
Angiocardiography
CT
MRI

PLAIN X-RAYS
Plain radiographs are important as the first imaging investigation in cases of heart disease. It gives vital information concerning:
Size of the heart
Enlargement of individual chambers
Pulmonary vasculature
Condition of the lung fields
Presence or absence of pleural effusion

SIZE OF THE HEART
Measured by the cardio-thoracic ratio
(CTR)
The maximum transverse diameter of the
heart is compared to the maximum
transverse diameter of the chest.
In normal adults this is <_ 50%
In children it is <_ 60%



CT OF THE HEART

Chamber orientation
RA-lies on the right and forms the RT heart
border
RV-lies to the LT and anterior to RA forms
anterior heart border
LA-lies posteriorly and forms the
posterior heart border
LV-forms the bulk of the left heart border




THE SHAPE OF THE HEART
The cardiac contour has characteristic
appearance in specific conditions
depending on the chambers mainly
enlarged.
LV enlargement is seen in HTN, and
aortic valve disease
The apex enlarges downward and to the left

LV ENLARGEMENT

THE LEFT ATRIUM
LA enlargement is seen in mitral valve
disease,
Enlarges backwards and to the right
Double density of the heart
Projects backwards and slightly upwards in
the lateral film .
Makes an impression on the barium filled
oesophagus.

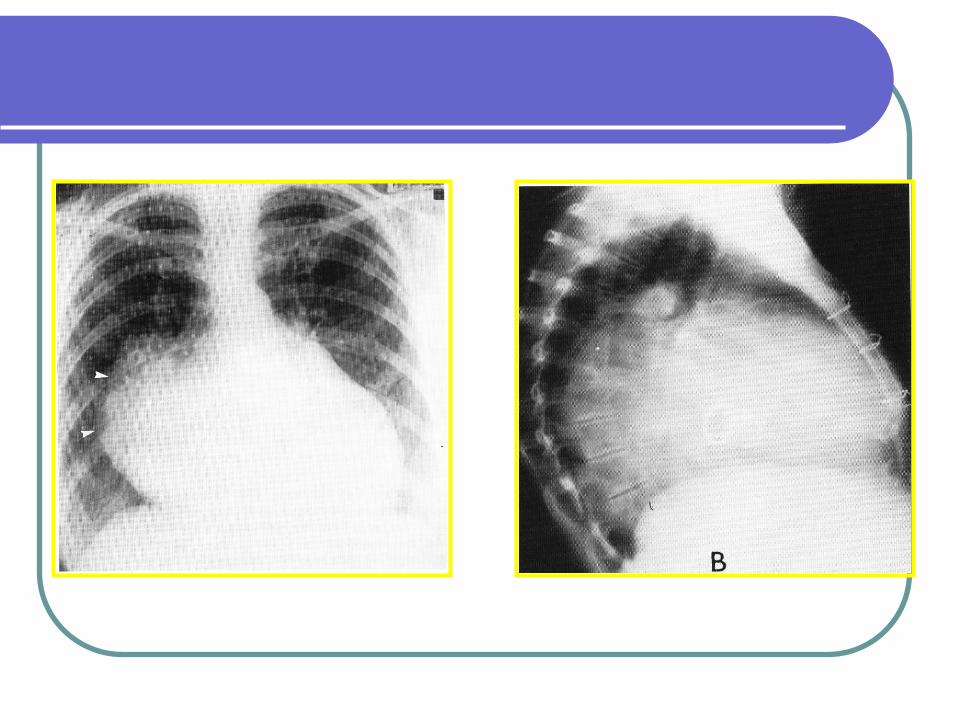
MR
Severe MR disease
.Left atrial appendage
is large , producing a
convex bulge (arrow).
The heart is
considerably enlarged

VSD

RIGHT VENTRICULAR
ENLARGEMENT
May also be seen in mitral disease due
to increased pulmonary resistance
secondary to pulmonary congestion
Also seen in congenital cardiac lesions
associated with pulmonary stenosis or L-
R shunts.
Pulmonary disease with chronic airway
obstruction

RV
Lifting and rounding of the apex
Filling of the retrosternal airspace

Rt Ventricle enlargement

Mitral valve disease
1) Mitral stenosis(ms)
Almost always rheumatic in origin.
In the elderly, heavy calcification of the valve
apparatus can cause ms.
A rare congenital form of ms is also
recognized.
In rheumatic ms the valve orifice is slowly
diminished by progressive fibrosis,
calcification of valve leaflets, and fusion of the
cusps and subvalvular apparatus.

Ms cont
Flow of blood from left atrium to left ventricle
is restricted and left atrial pressure rises
leading to pulmonary venous congestion and
breathlessness.
There is dilatation and hypertrophy of the left
atrium and left ventricular filling becomes
more dependent on left atrial contraction.
mitral orifice is about 5cm sq and may be
reduced to 1cm sq or less in severe ms.
Investigations
ECG: features of rt ventricular
hypertrophy, left atrial hypertrophy and
fibrillations.
CXR: enlargement of left atrium and its
appendage.
-enlargement of main pulm artery.
-features of pulmonary venous
congestion.

MS

MS

MR
LUNG FIELDS
CONGESTION-due to pulmonary venous hypertension following left heart lesions resulting in back pressure on the lung. Causes include; LV failure and mitral valve disease.
CXR
Diversion of blood from the lower to the upper zones of the lung in an erect PA film of the chest

Cont…
Pulmonary oedema with interstitial or
alveolar involvement
Septal lines- Kelly A,B and C
Lamellar effusions
Alveolar oedema is often perihilar with
blurring of the central lung areas (bat’s
wing appearance)
Pleural effusions may be seen.

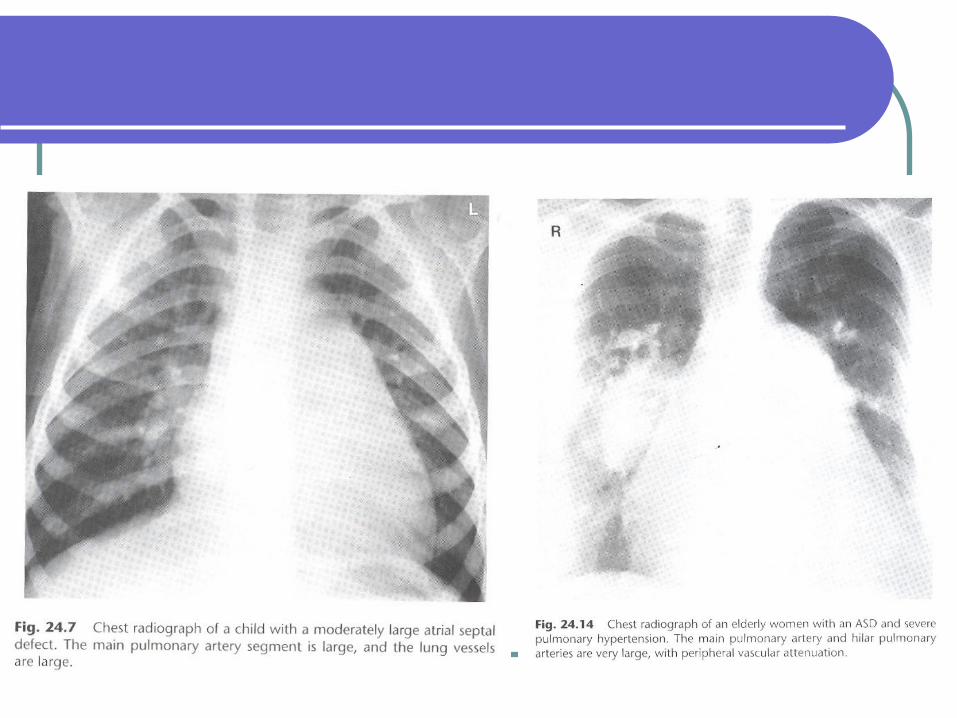
PULMONARY PLETHORA
Seen in conditions of high pulmonary flow mainly due to congenital L-R shunts.
Both arteries and veins become prominent with end on vessels close to the hilum being particularly well seen, and distal vessels extending to the lung periphery
PAH (pulmonary arterial hypertension) may develop in long standing ASD, increased resistance caused by severe pulmonary venous HTN

Cont……..
PAH may develop acutely following
massive pulmonary embolus or from
chronic multiple pulmonary emboli.
PAH also occurs in chronic pulmonary
disease with chronic airways obstruction

X-Ray Findings-ASD
Enlarged
pulmonary
vessels
Normal-sized
left atrium
Normal to
small aorta.

ASD

PULMONARY OLIGAEMIA
Occurs when there is obstruction to the
pulmonary outflow at or below the
pulmonary valves.
It may be seen in R-L shunt as in
tetralogy of Fallot


PERICARDIAL EFFUSION
May be classified as
1.Inflammatory
-TB -Supprative
-Rheumatic -Viral
2.Non-inflammatory
-heart failure -myocardial infarction
-Uraemia -Haemopericardium
3.Malignant

Pericardial effusion
The radiological diagnosis can be difficult
unless the fluid is more than 200 mls.
R.F
Enlarged globular heart
Masking of the hilar
U/S is diagnostic
CT or MRI may show the effusion

CXR-pericardial effusion

Congestive cardiac failure
Heart failure occurs when a patient with
significant heart disease develops signs
and symptoms of low cardiac output,
pulmonary congestion, or systemic
venous congestion

CCF-CAN BE
LT sided
RT sided
Biventicular

Radiological features
Cardiomegaly
Enlarged hilar vessels
Prominence of upper lobe vessels
Septal or Kerley B lines
Ground glass appearance of alveolar
oedema
Pleural effusion

Upper lobe diversion of blood

CCF

Kerley A & B lines

CXR
LA myxoma. Large
heart with all chambers
involved . There is
interstitial pulmonary
oedema.

LT ATRIAL MYXOMA

Ischaemic heart disease
Almost always due to atheroma and its
complications particularly thrombosis.
Risk factors:-
-age -male sex -family history
-smoking -hypertension
-diabetes mellitus -obesity
-sedentary life style -diet

Plain radiographs:-
- normal
Myocardial perfusion studies:-
scintiscans of the heart are taken at
rest and after exercise.
Thallium 201 is taken up by viable
perfused myocardium.
Thallium 201 is injected during exercise
test with immediate exercise images and
perfusion images 3 hrs later, after resting
Myocardial Ischaemia
IMAGING FEATURES


Myocardial perfusion
study.
Thallium scan
showing reversible
anterior myocardium
ischaemia.
Images are cross-
sectional tomograms
of the left ventricle.



CORONARY CT ANGIOGRAPHY
Indications
Recent onset chest pain
High cholesterol levels
High blood pressure
Family history of coronary artery disease
Smoking
Diabetes mellitus

CCTA


THE
END



![NASA Visible Infrared Imaging Radiometer Suite …...1 NASA Visible Infrared Imaging Radiometer Suite Level-1B Product User Guide August 2019 [Version 2.0] Level-1 and Atmosphere Archive](https://img.dokumen.tips/doc/110x75/5f02a2497e708231d4053dc4/nasa-visible-infrared-imaging-radiometer-suite-1-nasa-visible-infrared-imaging.jpg)



![-ravichandran@uiowa.edu] CVS Health (CVS) September … · Through the above service, CVS helps clients in designing ... Improvement, and Modernization ... prescriptions at CVS Pharmacy](https://img.dokumen.tips/doc/110x75/5b5140327f8b9a056a8bdae7/-ravichandranuiowaedu-cvs-health-cvs-september-through-the-above-service.jpg)





















