Embed Size (px)
Citation preview

Current Concepts Review
Operative Treatment of Primary AnteriorCruciate Ligament Rupture in Adults
Christopher D. Murawski, BS, Carola F. van Eck, MD, PhD, James J. Irrgang, PT, PhD, ATC, FAPTA,Scott Tashman, PhD, and Freddie H. Fu, MD, DSc(Hon), DPs(Hon)
Investigation performed at the Department of Orthopaedic Surgery, University of Pittsburgh School of Medicine, Pittsburgh, Pennsylvania
� Operative management of an acute anterior cruciate ligament (ACL) rupture may be required in young and activepatients to stabilize the knee and return patients to desired daily activities.
� ACL reconstruction should be performed anatomically.
� The majority of studies show no differences between anatomic single-bundle and double-bundle ACL recon-struction with respect to patient-reported outcome scores. Double-bundle reconstruction may provide superiorknee joint laxity measurements compared with the single-bundle technique.
� Following ACL reconstruction, the age and activity level of a patient are predictive of his or her time of return tosports and reinjury.
� Concomitant meniscal and/or cartilage damage at the time of surgery, in addition to a persistent knee motiondeficit, are associated with the development of osteoarthritis after ACL reconstruction.
Anterior cruciate ligament (ACL) rupture is a common injuryworldwide. Estimates suggest an annual incidence for ACL ruptureof thirty-five per 100,000 people of all ages1, with an approxi-mately two to eight-times higher risk in female athletes than inmale athletes2-7. These injuries often result in instability of theknee, increased joint laxity, and reduced activity and partici-pation, as well as an increased risk of knee osteoarthritis in thelong term8,9. Surgical reconstruction of the ACL is often rec-ommended, particularly in young and active patients, to facili-tate a return to the desired daily activities, including sports.
As the estimated annual health-care cost of ACL surgeryis $3 billion in the United States alone, providing patients with thebest potential for a successful outcome after ACL reconstruction
remains a topic of intense interest among clinicians and re-searchers10. In this review, a critical assessment of the evidencefor operative treatment of primary ACL rupture in adults (eighteenyears of age or older) is provided, including principles for decisionmaking, clinical outcomes, and guidelines for return to sports.
Anatomy and FunctionThe ACL is composed of two functional bundles, the antero-medial and posterolateral bundles, which are named for the lo-cation of their respective insertion sites on the tibia11,12. The tibialinsertion site of the ACL reveals a characteristic fan-shaped foot-print, whereas the femoral insertion site demonstrates a smaller,oval-shaped appearance13. The femoral insertion site is identifiable
Disclosure: None of the authors received payments or services, either directly or indirectly (i.e., via his or her institution), from a third party in support ofany aspect of this work. One or more of the authors, or his or her institution, has had a financial relationship, in the thirty-six months prior to submission ofthis work, with an entity in the biomedical arena that could be perceived to influence or have the potential to influence what is written in this work. Noauthor has had any other relationships, or has engaged in any other activities, that could be perceived to influence or have the potential to influence what iswritten in this work. The complete Disclosures of Potential Conflicts of Interest submitted by authors are always provided with the online version of the article.
Peer Review: This article was reviewed by the Editor-in-Chief and one Deputy Editor, and it underwent blinded review by two or more outside experts. The Deputy Editorreviewed each revision of the article, and it underwent a final review by the Editor-in-Chief prior to publication. Final corrections and clarifications occurred during one ormore exchanges between the author(s) and copyeditors.
685
COPYRIGHT � 2014 BY THE JOURNAL OF BONE AND JOINT SURGERY, INCORPORATED
J Bone Joint Surg Am. 2014;96:685-94 d http://dx.doi.org/10.2106/JBJS.M.00196

using the position of two osseous ridges on the medial wall ofthe lateral femoral condyle14-18. The lateral intercondylar ridge,or so-called resident’s ridge, denotes the anterior border of thefemoral insertion site. The lateral bifurcate ridge runs perpen-dicular to the lateral intercondylar ridge, between the femoralinsertion sites of the anteromedial and posterolateral bundles19.
Functionally, the anteromedial and the posterolateral bundlesbehave synergistically with knee flexion, whereby both antero-posterior and rotational stability of the knee are provided. In-dividually, the anteromedial bundle length remains constantthroughout the knee flexion-extension, attaining peak tensionbetween 45� and 60� of flexion20-22. In comparison, the postero-lateral bundle is tight in extension and loosens with flexion,thereby allowing axial rotation of the knee to occur. Varyingmechanical behaviors of the functional bundles of the ACL havebeen reported23,24.
A thorough understanding of the anatomy and functionof the native ACL is fundamental for the treatment of ACL in-juries. This understanding ultimately aids the surgeon in de-termining the most appropriate treatment strategy for a partialor complete rupture of the ACL.
Treatment of ACL InjuriesACL injuries can be managed with nonoperative or operativetreatment. The decision to recommend operative treatment foran acute ACL rupture is multifactorial and must be individualizedto each patient on the basis of his or her age25, desired activitylevel, and presence of potential concomitant injuries. In general,younger and more active patients are more likely to require sur-gery to return to functionally demanding activities. In the re-mainder of this review article, we focus on operative treatmentof ACL injuries. While rehabilitation after ACL reconstructionis an important aspect of the ultimate success after ACL recon-struction25-28, it is not a focus of this review.
Operative TreatmentOnce the decision to proceed with operative treatment of an ACLrupture is made, timing of the procedure becomes an importantvariable to consider. Preoperative range of motion, swelling,and quadriceps strength have been investigated as factors thatcan affect the ultimate success of ACL reconstruction29,30. Preop-erative swelling and limited range of motion have been related tothe development of arthrofibrosis after surgery 29.
Preoperative quadriceps strength deficits of >20% havebeen shown to significantly affect the two-year functional out-come of ACL reconstruction with bone-patellar tendon-boneautograft30. Moreover, it has been reported that preoperativequadriceps strength of >90% of that of the noninjured leg sig-nificantly increased postoperative strength two years after sur-gery compared with those with <75% of preoperative quadricepsstrength31. Rehabilitation prior to surgery should focus on re-gaining range of motion, reducing swelling, and strengtheningthe quadriceps.
Intraoperatively, the rupture pattern of the ACL should beconfirmed, and if a partial one-bundle rupture is evident, aug-mentation surgery should be considered32. Partial ACL ruptures
have been reported to occur in approximately 5% to 35% ofpatients32,33. Performing a one-bundle augmentation surgery car-ries the theoretical advantages of maintaining proprioceptivefibers, biomechanical strength, and biological healing potential34.Careful dissection and preservation of the native insertion sitescan facilitate determination of the appropriate tunnel location(s).
Presently, the majority of surgeons who perform ACL re-constructions do so using a single-bundle technique. The double-bundle technique is more commonly utilized in Europe andAsia than it is in the United States. Regardless, it is important tounderstand the double-bundle anatomy of the ACL so that sur-geons can perform an anatomic single-bundle or double-bundleACL reconstruction. In the event that a surgeon has experiencein performing double-bundle ACL reconstruction and considersthis as part of the preoperative planning process, the decision toperform anatomic single-bundle or double-bundle ACL recon-struction is based on several criteria. A comprehensive flowchartto assist surgeons in this decision has been previously described35.The variation in size of the tibial insertion site is one element toconsider36 (Fig. 1). A tibial insertion site size of <14 mm, measuredarthroscopically, makes it difficult to perform a double-bundlereconstruction35. Furthermore, arthritic changes, multiligamentinjury, severe bone bruising, open physes, and a narrow notchwidth are considered indications to perform single-bundle re-construction32. Variation in the shape of the notch can alsoinfluence whether two femoral tunnels can be drilled safely fordouble-bundle reconstruction37.
Typical graft options for ACL reconstruction include bone-patellar tendon-bone autograft, hamstring tendon autograft, quad-riceps tendon autograft, and allograft (Table I)38-40. Of these options,
Fig. 1
An arthroscopic ruler is used to measure the size of the tibial insertion site
in the sagittal plane, with the ACL tibial footprint shown dissected and the
anteromedial (AM) and posterolateral (PL) bundles marked with a stan-
dard, commercially available, arthroscopic radiofrequency ablationdevice.
686
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 96-A d NU M B E R 8 d A P R I L 16, 2014OP E R AT I V E TR E AT M E N T O F P R I M A RY AN T E R I O R
CRU C I AT E LI G A M E N T RU P T U R E I N AD U LT S
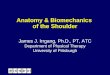
bone-patellar tendon-bone graft is not suitable for double-bundlereconstruction. For the purposes of preoperative planning, thesagittal thickness of the patellar and quadriceps tendons can bemeasured on magnetic resonance imaging (MRI) scans to pro-vide the surgeon with an idea as to potential graft size41. Studieshave also evaluated the use of MRI in predicting hamstring graftsize and have found that, while cross-sectional area measurementson MRI scans correlate positively with intraoperative graft size42,43,measurements of graft diameter do not42. Magnussen et al. foundthat a hamstring autograft size of £8 mm in diameter was asso-ciated with a higher rate of early revision than were those of>8 mm44. In patients having primary surgery, allograft may beused when there are concerns of donor site morbidity or cos-mesis. Fresh-frozen allografts are typically preferred over ir-radiated, chemically processed, or preserved grafts and provideresults equal to those of autografts45-47. Recent studies have,however, indicated higher rates of graft failure following ACLreconstruction with varying types of allograft, particularly inyounger active individuals desiring an early return to sport48-51.
Ultimately, daily activities and patient lifestyle influencegraft choice for an individual undergoing ACL reconstruction.For example, in a patient with daily activities that include kneeling(e.g., wrestling or religious practices), the use of a bone-patellartendon-bone autograft may be contraindicated because it is asso-ciated with a higher prevalence of anterior knee pain52.
Proper tunnel placement is critical in anatomic ACL re-construction. Nonanatomic tunnel placement has been previ-ously shown to decrease knee motion53 and to produce abnormalrotational knee kinematics during dynamic loading54. A recentstudy has evaluated the ACL tunnel positions used by twelve
surgeons and found a lack of agreement in the ideal position forsingle-bundle ACL tunnels55. Several intraoperative and post-operative methods have been described to evaluate tunnel place-ment. Postoperatively, anteroposterior and lateral radiographs
TABLE I Advantages and Disadvantages of Available Graft Choices for ACL Reconstruction
Graft Choice Advantages Disadvantages
Bone-patellar tendon-bone d Bone-to-bone healing in both tunnels d Not suitable for double-bundle reconstruction
d Comparable stiffness to native ACL d Risk of anterior kneeling pain
d Invasive, large incision
d Risk of patellar fracture
d Fixed length
d Weaker than native ACL
Hamstring d Ease of harvest d Soft-tissue healing
d Cosmesis d Graft size can be unpredictable
d Minimal donor site morbidity d Not suitable for certain athletes who relyheavily on their hamstring muscles
d Comparable strength to native ACLd Less stiffness than native ACL
Quadriceps tendon d Large graft d Invasive, large incision
d Can be used for single ordouble-bundle reconstruction
d Risk of patellar fracture
d Option of a one-sided bone block
Allograft d No donor site morbidity d Theoretical risk of disease transmission
d Available in various types and sizes d Longer healing time
d Increased risk of rerupture, especially in youngerpatients and irradiated grafts
Fig. 2
A standard 45� flexion weight-bearing posteroanterior (PA) radiograph,
made one year after single-bundle ACL reconstruction, demonstrating a
45� femoral tunnel angle relative to the long axis of the femur, suggestive
of anatomic tunnel placement41.
687
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 96-A d NU M B E R 8 d A P R I L 16, 2014OP E R AT I V E TR E AT M E N T O F P R I M A RY AN T E R I O R
CRU C I AT E LI G A M E N T RU P T U R E I N AD U LT S

can be used to evaluate tunnel angle and implant position.Illingworth et al. described a femoral tunnel angle measure-ment based on the long axis of the femur on an anteroposteriorradiograph, whereby an angle of <32.7� is likely to be nonan-atomic56 (Fig. 2). Postoperative MRI measurements of the in-sertion site, inclination angle, and length of the ACL can alsobe compared with those made preoperatively (Fig. 3). A three-dimensional computed tomography (CT) scan is presently con-sidered the gold standard for evaluation of tunnel placement57-59
(Figs. 4 and 5). Meuffels et al. demonstrated that three-dimensional measurements provided the highest reliability inthe evaluation of femoral and tibial tunnel placement60. More-over, a three-dimensional CT scan can be particularly useful inplanning for knees in which revision surgery may eventually berequired.
Clinical Outcomes After ACL ReconstructionA Level-I clinical trial by Frobell et al. randomized 121 physi-cally active adults to a structured rehabilitation program withearly ACL reconstruction or to a rehabilitation program alonewith the option of delayed ACL reconstruction61. At the two-year follow-up, the difference using a subscale of the Knee Injuryand Osteoarthritis Outcome Score (KOOS4) was a mean of 39.2for the early ACL reconstruction group and a mean of 39.4points for the rehabilitation and optional delayed reconstruc-tion group (p = 0.96). The rehabilitation and optional delayedreconstruction group had a higher rate of meniscal surgery thanthe early reconstruction group. Similar results were also foundwith recently reported five-year results of this trial62. In total, thirtypatients (51%) in the delayed reconstruction group ultimately
had ACL surgery. Therefore, nonoperative management maybe feasible in a well-defined cohort of patients with an acute ACLtear who have been counseled accordingly.
The outcomes of single-bundle and double-bundle recon-struction have been reported previously (Figs. 6 and 7). A recentCochrane review by Tiamklang et al. evaluated the effects ofsingle-bundle compared with double-bundle reconstructionsin adult patients in seventeen randomized and quasi-randomizedcontrolled trials63. The authors reported no detectable differ-ences between single-bundle and double-bundle reconstruc-tions in patient-reported outcomes up to five years after surgery.The two to five-year follow-up evaluation demonstrated im-provements in the International Knee Documentation Com-mittee (IKDC) knee examination, pivot-shift test, and knee laxitymeasurements on the KT-1000 arthrometer with double-bundlereconstruction. Single-bundle reconstructions had a higher rateof new meniscal injury. Importantly, methodological deficiencieswere prevalent in all trials included in the review and should beconsidered when evaluating the results of this study.
In a recent Level-I randomized controlled trial by Husseinet al., anatomic double-bundle ACL reconstruction was com-pared with anatomic single-bundle and conventional single-bundle ACL reconstructions with hamstring autograft64. Twohundred and eighty-one patients were prospectively followedfor a mean of 51.15 months after surgery. The patients in theanatomic double-bundle group had improved anteroposteriorlaxity (measured with the KT-1000 arthrometer) and rotationallaxity (pivot-shift test) compared with the anatomic single-bundlegroup; the anatomic single-bundle group had improved antero-posterior and rotational laxities compared with conventional
Fig. 3
Figs. 3-A, 3-B, and 3-C MRI scans of a knee that had an anatomic ACL reconstruction with bone-patellar tendon-bone autograft. Fig. 3-A Preoperative scan
showing initial measurements. The ACL length is also measured preoperatively. Figs. 3-B Sagittal scan, made three months postoperatively, showing
the tibial insertion site size and inclination angle measurements for comparison. Fig. 3-C A coronal oblique sequence, made three months postoperatively,
in the plane of the long axis of the ACL starting at the intercondylar roof of the Blumensaat line. This sequence can be used for graft evaluation after
ACL reconstruction.
688
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 96-A d NU M B E R 8 d A P R I L 16, 2014OP E R AT I V E TR E AT M E N T O F P R I M A RY AN T E R I O R
CRU C I AT E LI G A M E N T RU P T U R E I N AD U LT S

single-bundle reconstruction. The only significant difference inpatient-reported outcome was a higher Lysholm score in theanatomic double-bundle group in comparison with the con-ventional single-bundle group. There were no significant dif-ferences in patient-reported outcome scores in the comparisonof anatomic double-bundle with anatomic single-bundle recon-struction. In a second prospective comparative study (Level II),anatomic single-bundle reconstructions were compared withanatomic double-bundle reconstructions with hamstring au-tograft, with the procedures individualized on the basis of in-traoperative measurements of the native ACL tibial insertionsite size65. At a mean follow-up of thirty months after surgery, nodifferences between the groups were detected with respect tothe Lysholm and IKDC Subjective Knee Form scores or the resultsof the KT-1000 measurements and pivot-shift tests.
The majority of published studies have shown no dif-ferences between anatomic single-bundle and double-bundle ACLreconstruction in terms of patient-reported outcomes. Differ-ences may exist with regard to knee joint laxity measurements,
favoring double-bundle reconstruction. There is also some evi-dence to suggest that individualized surgery may facilitate similaroutcomes with respect to knee joint laxity, regardless of whethersingle or double-bundle reconstruction is performed. Furtherinvestigation is needed to confirm or dispute these findings.
The outcomes after one-bundle augmentation reconstruc-tion for partial rupture of the ACL have been reported in severalseries. Sonnery-Cottet et al. reported that reconstruction of theanteromedial bundle with preservation of the posterolateral bundlesignificantly decreased anteroposterior laxity (Telos stress ra-diography), while significantly increasing the IKDC SubjectiveKnee Form and Lysholm scores at a mean follow-up of twenty-six months66. Adachi et al. compared ACL augmentation surgeryin partial ACL tears and complete ACL reconstruction with com-plete ACL tears at a mean follow-up of 2.6 years67. The authorsreported augmentation surgery to be superior for joint stabil-ity and position sense. A recent systematic review found that
Fig. 4
Femoral and tibial three-dimensional CT reconstructions demonstrating
anatomic tunnel placement of a single-bundle ACL reconstruction.
Fig. 5
Femoral and tibial three-dimensional CT reconstructions demonstrating
anatomic tunnel placement of a double-bundle ACL reconstruction.
689
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 96-A d NU M B E R 8 d A P R I L 16, 2014OP E R AT I V E TR E AT M E N T O F P R I M A RY AN T E R I O R
CRU C I AT E LI G A M E N T RU P T U R E I N AD U LT S
the available evidence to support augmentation was weak butencouraging68.
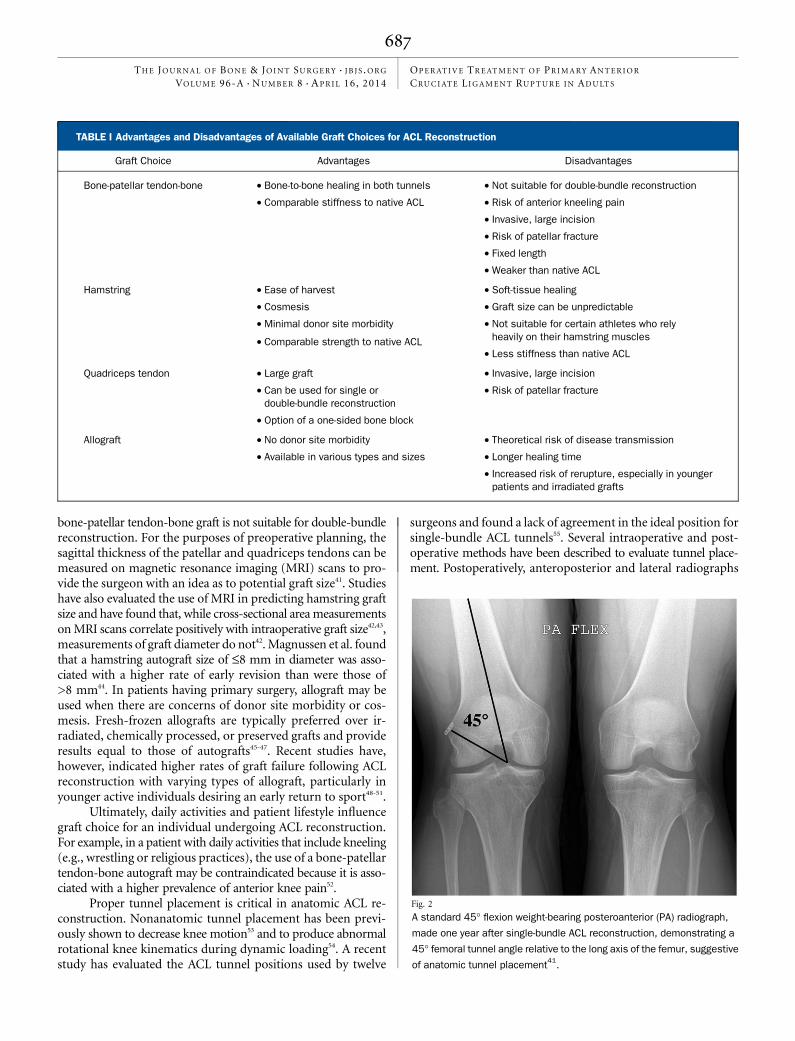
In Vivo Biomechanics After ACL ReconstructionIn vivo kinematic studies evaluate knee biomechanics withoutthe ‘‘time-zero’’ limitation of in vitro studies. They also enableserial assessment of the effects of healing on knee function afterACL reconstruction and can involve realistic weight-bearingactivities, such as running, jumping, and stair-climbing.
Georgoulis et al. compared ACL-reconstructed and con-tralateral, normal knees using conventional video-motion analysiswith surface markers69. While no differences were evident duringwalking, greater internal tibial rotation in the reconstructedknee was observed during more demanding pivoting tasks. Tashmanet al. used dynamic stereoradiography to assess knee kinematicsduring the stance phase of downhill running, and found greaterexternal rotation and adduction in ACL-reconstructed kneescompared with the contralateral, uninjured limbs54. The surgical
technique used for that study incorporated nonanatomic place-ment of the graft, demonstrating that nonanatomic ACL recon-struction fails to restore preinjury knee function under functionalloading conditions. Abebe et al. utilized biplanar fluoroscopyand MRI to evaluate knee function during a series of static jointpositions and reported that single-bundle reconstruction withanatomic femoral tunnel placement resulted in knee joint kine-matics that were more closely restored relative to the intact kneecompared with nonanatomic tunnel placement70.
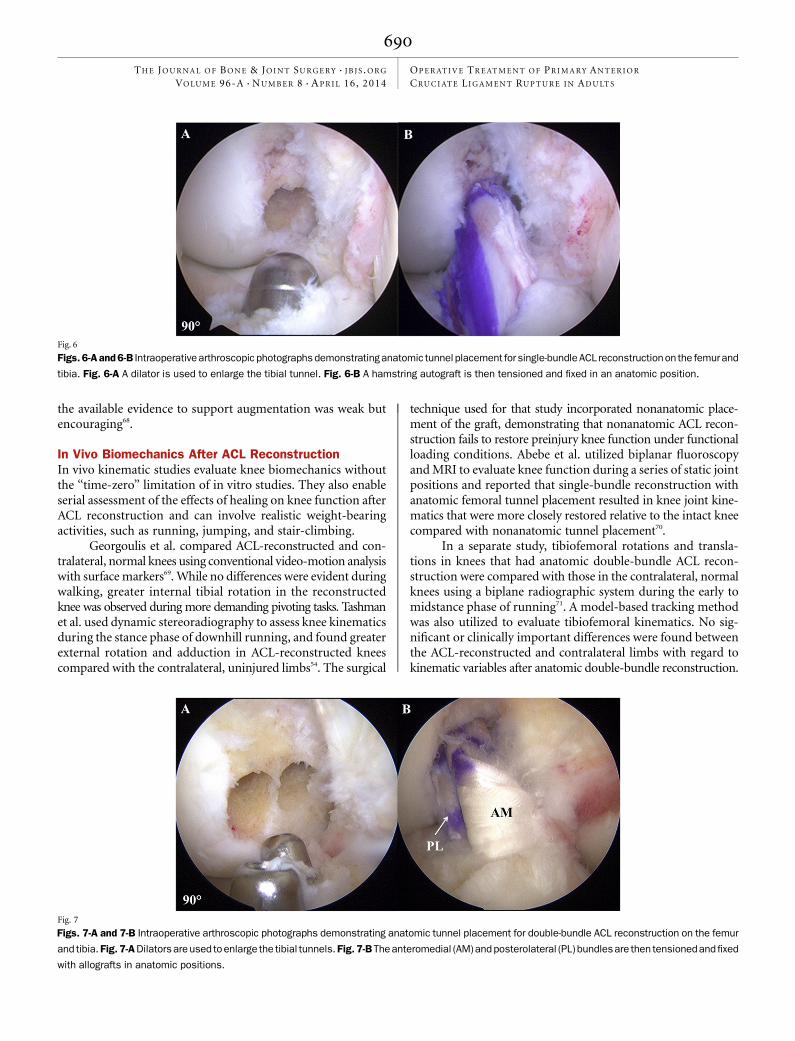
In a separate study, tibiofemoral rotations and transla-tions in knees that had anatomic double-bundle ACL recon-struction were compared with those in the contralateral, normalknees using a biplane radiographic system during the early tomidstance phase of running71. A model-based tracking methodwas also utilized to evaluate tibiofemoral kinematics. No sig-nificant or clinically important differences were found betweenthe ACL-reconstructed and contralateral limbs with regard tokinematic variables after anatomic double-bundle reconstruction.
Fig. 6
Figs. 6-A and 6-B Intraoperative arthroscopic photographs demonstrating anatomic tunnel placement for single-bundle ACL reconstructionon the femur and
tibia. Fig. 6-A A dilator is used to enlarge the tibial tunnel. Fig. 6-B A hamstring autograft is then tensioned and fixed in an anatomic position.
Fig. 7
Figs. 7-A and 7-B Intraoperative arthroscopic photographs demonstrating anatomic tunnel placement for double-bundle ACL reconstruction on the femur
and tibia. Fig. 7-A Dilators are used to enlarge the tibial tunnels.Fig. 7-B Theanteromedial (AM)and posterolateral (PL) bundlesare then tensionedandfixed
with allografts in anatomic positions.
690
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 96-A d NU M B E R 8 d A P R I L 16, 2014OP E R AT I V E TR E AT M E N T O F P R I M A RY AN T E R I O R
CRU C I AT E LI G A M E N T RU P T U R E I N AD U LT S

These results suggest that anatomic double-bundle reconstruc-tion may be effective for restoring knee function compared withthe uninjured side. It is not, however, known whether anatomicsingle-bundle reconstruction may produce results similar to an-atomic double-bundle reconstruction compared with the con-tralateral knee.
Return to Sports After ACL ReconstructionThe timing of return to sports after ACL reconstruction is mul-tifactorial. Graft choice is an important consideration with re-gard to whether there is bone-to-bone healing (bone-patellartendon-bone graft) or soft tissue-to-bone healing. In a systematicreview and meta-analysis, Ardern et al. assessed forty-eight studieswith a total of 5770 patients at a mean follow-up of 41.5 monthsafter ACL reconstruction72. In total, while 82% of the patientsreported returning to some level of sporting activity, 63% of thepatients returned to sports participation at the preinjury level,and only 44% returned to competitive sports. The leading reasongiven for not returning to sporting activity was fear of reinjury.
Brophy et al. evaluated the return to sports among soccerathletes and found that younger or male athletes were more likelyto return to play than were older or female athletes73. Smith et al.,who separately evaluated the return to the preinjury activity levelamong seventy-seven competitive athletes with a mean age oftwenty-one years (range, fifteen to thirty years), found that 71%(fifty-five) returned to preinjury activity levels by twelve monthsafter surgery74. Further research on return to sports should eval-uate the rate of return to the preinjury activity in terms of the type,frequency, intensity, and duration of participation.
Graft Failure After ACL ReconstructionGraft failure in the ipsilateral knee after ACL reconstruction andnative ACL rupture in the contralateral knee have been inves-tigated. A recent study from the Danish Knee Ligament Recon-struction Register compared anteromedial with transtibial femoraltunnel drilling during ACL reconstruction. Anteromedial dril-ling had a higher overall rate of revision surgery (5.16%) thantranstibial drilling (3.20%), with a relative risk of 2.04 (95% con-fidence interval, 1.39 to 2.99)75. Surgeons should use caution whenevaluating these results, given the tendency of the transtibialtechnique to place the graft in a nonanatomic position. Indi-viduals undergoing anatomic ACL reconstruction may be at higherrisk for graft failure, particularly with early return to activity,given the higher, closer to normal, in situ forces on an anatomi-cally placed graft76,77.
A recent study by Bourke et al. of patients undergoing ACLreconstruction with either bone-patellar tendon-bone or ham-string autograft found graft failure to be 11%, while contralateralACL rupture was 13%78. Graft choice did not affect failure rate.Other authors have also reported a higher risk of failure in thecontralateral ACL compared with the ipsilateral graft79. Shelbourneet al. followed 1415 patients for a minimum of five years afterACL reconstruction with bone-patellar tendon-bone autograftand found a lower patient age and higher activity level to beassociated with increased injury to either knee80. Returningto activity before six months postoperatively did not appear to
increase the risk for injury. In this particular study, the groupwith an age of less than eighteen years returned at a mean 4.6months after surgery. In a prospective analysis of failure inanatomic ACL reconstruction with allograft, van Eck et al. foundthat 48% (thirteen) of twenty-seven reruptures occurred withinnine months after surgery, before the patients had receivedclearance to return to sports51. Further investigation is requiredto determine factors affecting ACL graft failure, includingconsideration for graft healing. On the basis of the availableevidence, a lower patient age and higher activity level, but nottime to return to sport, appear to be predictive of reinjury.
Osteoarthritis After ACL ReconstructionThe development of osteoarthritis after ACL reconstruction is aconcern. Li et al. retrospectively investigated the predictors ofradiographic knee osteoarthritis after nonanatomic single-bundleACL reconstruction81. Radiographic osteoarthritis, defined as Kellgrenand Lawrence grade-2 changes in at least one compartment orgrade-1 changes in at least two compartments, were demonstratedby 39% (ninety-six) of 249 patients at a mean 7.86 years follow-up. The most optimal set of predictors for osteoarthritis werebody mass index, length of follow-up, prior medial meniscectomy,and medial chondrosis of grade 2 or greater. Separately, Roeet al. investigated differences in osteoarthritis rates in a consec-utive cohort of nonrandomized patients who underwent ACLreconstruction with hamstring or bone-patellar tendon-boneautograft82. At seven years of follow-up, 45% (twenty-four) of fifty-three patients in the bone-patellar tendon-bone group and 14%(seven) of fifty-one in the hamstring group showed signs of ra-diographic osteoarthritis (p = 0.002).
Several studies with longer-term follow-up have also beenperformed. Oiestad et al. prospectively evaluated knee functionand the prevalence of osteoarthritis in patients ten to fifteenyears after isolated ACL reconstruction and in patients who hadconcomitant meniscal and/or cartilage pathology 83. Radiographicassessment using the Kellgren and Lawrence classification systemrevealed that 80% of the patients in the concomitant pathologygroup had joint space narrowing of grade 2 or greater comparedwith 62% in the isolated group (p = 0.008). However, differenceswere not detectable between groups with respect to symptomaticosteoarthritis. In a separate study of the same cohort, Oiestad et al.reported that the prevalence of patellofemoral osteoarthritis was26.5% (forty-eight of 181 patients twelve years after reconstruction)and was associated with older age, increased symptoms, and greatertibiofemoral osteoarthritis, as well as reduced knee function84.
Salmon et al. also reported an association between de-generative joint changes and meniscectomy, increased kneejoint laxity, and loss of knee motion thirteen years after ACLreconstruction with bone-patellar tendon-bone autograft85. Sim-ilarly, Shelbourne et al. evaluated 780 patients undergoing ACLreconstruction with bone-patellar tendon-bone autograft and,at a minimum of five years of follow-up, found that the loss ofnormal knee flexion and extension was associated with an increasedrate of radiographic osteoarthritis86. In two separate studies ofpatients in whom concomitant knee pathology was absent atthe time of surgery, Shelbourne and Gray and Lebel et al. reported
691
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 96-A d NU M B E R 8 d A P R I L 16, 2014OP E R AT I V E TR E AT M E N T O F P R I M A RY AN T E R I O R
CRU C I AT E LI G A M E N T RU P T U R E I N AD U LT S

that the rate of osteoarthritis was 2% and 8%, respectively, beyondthe mean follow-up time of ten years87,88.
It is the general consensus of the available evidence thatmeniscal and/or cartilage damage and knee motion deficits aftersurgery are associated with the development and/or progres-sion of osteoarthritis after ACL reconstruction. Furthermore,patients without concomitant joint pathology at the time ofACL surgery appear to have a low rate of osteoarthritis, even atrelatively long-term follow-up. Continued investigation into thecause and development of osteoarthritis after ACL reconstruction,
including early recognition via advanced imaging modalities oridentification of relevant biomarkers, will be important.
In conclusion, operative management of acute ACL ruptureis common in young and active patients and can achieve pre-dictable outcomes (Table II). The use of double-bundle re-construction appears to provide no difference compared withsingle-bundle reconstruction in patient-reported outcomes. Theage and activity level of the patient are predictive of the return tosports and of reinjury. On the basis of the currently availabledata, the time to return to sports may not be predictive of reinjuryto the reconstructed ACL. Meniscal and/or cartilage pathologynoted at the time of ACL reconstruction, as well as a knee motiondeficit postoperatively, are associated with the developmentand/or progression of osteoarthritis. Future studies investigatingoperative methods for the treatment of ACL injuries are war-ranted. It is imperative that these studies be adequately poweredand use patient-relevant and sensitive outcome measures. n
Christopher D. Murawski, BSCarola F. van Eck, MD, PhDJames J. Irrgang, PT, PhD, ATC, FAPTAScott Tashman, PhDFreddie H. Fu, MD, DSc(Hon), DPs(Hon)Department of Orthopaedic Surgery,University of Pittsburgh School of Medicine,3471 Fifth Avenue, Suite 1011,Pittsburgh, PA 15213.E-mail address for F.H. Fu: [email protected].
References
1. Gianotti SM, Marshall SW, Hume PA, Bunt L. Incidence of anterior cruciate ligamentinjury and other knee ligament injuries: a national population-based study. J Sci MedSport. 2009 Nov;12(6):622-7. Epub 2008 Oct 02.2. Agel J, Arendt EA, Bershadsky B. Anterior cruciate ligament injury in nationalcollegiate athletic association basketball and soccer: a 13-year review. Am J SportsMed. 2005 Apr;33(4):524-30. Epub 2005 Feb 08.3. Arendt E, Dick R. Knee injury patterns among men and women in collegiatebasketball and soccer. NCAA data and review of literature. Am J Sports Med. 1995Nov-Dec;23(6):694-701.4. Arendt EA, Agel J, Dick R. Anterior cruciate ligament injury patterns amongcollegiate men and women. J Athl Train. 1999 Apr;34(2):86-92.5. Griffin LY, Agel J, Albohm MJ, Arendt EA, Dick RW, Garrett WE, Garrick JG, HewettTE, Huston L, Ireland ML, Johnson RJ, Kibler WB, Lephart S, Lewis JL, Lindenfeld TN,Mandelbaum BR, Marchak P, Teitz CC, Wojtys EM. Noncontact anterior cruciateligament injuries: risk factors and prevention strategies. J Am Acad Orthop Surg.2000 May-Jun;8(3):141-50.6. Hootman JM, Dick R, Agel J. Epidemiology of collegiate injuries for 15 sports:summary and recommendations for injury prevention initiatives. J Athl Train. 2007Apr-Jun;42(2):311-9.7. Sutton KM, Bullock JM. Anterior cruciate ligament rupture: differences betweenmales and females. J Am Acad Orthop Surg. 2013 Jan;21(1):41-50.8. Lohmander LS, Englund PM, Dahl LL, Roos EM. The long-term consequence ofanterior cruciate ligament and meniscus injuries: osteoarthritis. Am J Sports Med.2007 Oct;35(10):1756-69. Epub 2007 Aug 29.9. Lohmander LS, Ostenberg A, Englund M, Roos H. High prevalence of kneeosteoarthritis, pain, and functional limitations in female soccer players twelve yearsafter anterior cruciate ligament injury. Arthritis Rheum. 2004 Oct;50(10):3145-52.10. Brophy RH, Wright RW, Matava MJ. Cost analysis of converting from single-bundle to double-bundle anterior cruciate ligament reconstruction. Am J Sports Med.2009 Apr;37(4):683-7. Epub 2009 Feb 09.11. Girgis FG, Marshall JL, Monajem A. The cruciate ligaments of the knee joint.Anatomical, functional and experimental analysis. Clin Orthop Relat Res. 1975Jan-Feb;(106):216-31.
12. Odensten M, Gillquist J. Functional anatomy of the anterior cruciate liga-ment and a rationale for reconstruction. J Bone Joint Surg Am. 1985 Feb;67(2):257-62.13. Yasuda K, van Eck CF, Hoshino Y, Fu FH, Tashman S. Anatomic single- anddouble-bundle anterior cruciate ligament reconstruction, part 1: Basic science. Am JSports Med. 2011 Aug;39(8):1789-99. Epub 2011 May 19.14. Ferretti M, Ekdahl M, Shen W, Fu FH. Osseous landmarks of the femoralattachment of the anterior cruciate ligament: an anatomic study. Arthroscopy. 2007Nov;23(11):1218-25.15. Fu FH, Jordan SS. The lateral intercondylar ridge—a key to anatomic anteriorcruciate ligament reconstruction. J Bone Joint Surg Am. 2007 Oct;89(10):2103-4.16. Purnell ML, Larson AI, Clancy W. Anterior cruciate ligament insertions on thetibia and femur and their relationships to critical bony landmarks using high-resolutionvolume-rendering computed tomography. Am J Sports Med. 2008 Nov;36(11):2083-90. Epub 2008 Jul 28.17. Iwahashi T, Shino K, Nakata K, Otsubo H, Suzuki T, Amano H, Nakamura N.Direct anterior cruciate ligament insertion to the femur assessed by histology and3-dimensional volume-rendered computed tomography. Arthroscopy. 2010 Sep;26(9)(Suppl):S13-20. Epub 2010 Jul 29.18. Shino K, Suzuki T, Iwahashi T, Mae T, Nakamura N, Nakata K, Nakagawa S.The resident’s ridge as an arthroscopic landmark for anatomical femoral tunneldrilling in ACL reconstruction. Knee Surg Sports Traumatol Arthrosc. 2010 Sep;18(9):1164-8. Epub 2009 Nov 14.19. van Eck CF, Morse KR, Lesniak BP, Kropf EJ, Tranovich MJ, van Dijk CN, Fu FH.Does the lateral intercondylar ridge disappear in ACL deficient patients? Knee SurgSports Traumatol Arthrosc. 2010 Sep;18(9):1184-8. Epub 2010 Jan 20.20. Chhabra A, Starman JS, Ferretti M, Vidal AF, Zantop T, Fu FH. Anatomic,radiographic, biomechanical, and kinematic evaluation of the anterior cruciateligament and its two functional bundles. J Bone Joint Surg Am. 2006 Dec;88(Suppl 4):2-10.21. Gabriel MT, Wong EK, Woo SL, Yagi M, Debski RE. Distribution of in situ forces inthe anterior cruciate ligament in response to rotatory loads. J Orthop Res. 2004Jan;22(1):85-9.
TABLE II Grades of Recommendation for Operative Treatment ofPrimary Anterior Cruciate Ligament Rupture in Adults
Recommendation Grade of Evidence*
Operative treatment B
Single-bundle reconstruction C
Double-bundle reconstruction C
Autograft C
Allograft C
*Grade A indicates good evidence (Level-I studies with consistentfindings) for or against recommending the intervention; Grade B,fair evidence (Level-II or III studies with consistent findings) for oragainst recommending the intervention; Grade C, conflicting orpoor-quality evidence (Level-IV or V studies) not allowing a rec-ommendation for or against the intervention; and Grade I, there isinsufficient evidence to make a recommendation89.
692
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 96-A d NU M B E R 8 d A P R I L 16, 2014OP E R AT I V E TR E AT M E N T O F P R I M A RY AN T E R I O R
CRU C I AT E LI G A M E N T RU P T U R E I N AD U LT S

22. Tischer T, Ronga M, Tsai A, Ingham SJ, Ekdahl M, Smolinski P, Fu FH. Biome-chanics of the goat three bundle anterior cruciate ligament. Knee Surg SportsTraumatol Arthrosc. 2009 Aug;17(8):935-40. Epub 2009 Apr 09.23. Markolf KL, Park S, Jackson SR, McAllister DR. Anterior-posterior and rotatorystability of single and double-bundle anterior cruciate ligament reconstructions. J BoneJoint Surg Am. 2009 Jan;91(1):107-18.24. Markolf KL, Park S, Jackson SR, McAllister DR. Contributions of the postero-lateral bundle of the anterior cruciate ligament to anterior-posterior knee laxity andligament forces. Arthroscopy. 2008 Jul;24(7):805-9. Epub 2008 Apr 14.25. Eitzen I, Moksnes H, Snyder-Mackler L, Engebretsen L, Risberg MA. Functionaltests should be accentuated more in the decision for ACL reconstruction. Knee SurgSports Traumatol Arthrosc. 2010 Nov;18(11):1517-25. Epub 2010 Apr 22.26. Hensler D, Van Eck CF, Fu FH, Irrgang JJ. Anatomic anterior cruciate ligamentreconstruction utilizing the double-bundle technique. J Orthop Sports Phys Ther.2012 Mar;42(3):184-95. Epub 2012 Feb 29.27. Logerstedt DS, Snyder-Mackler L, Ritter RC, Axe MJ, Godges JJ; OrthopaedicSection of the American Physical Therapist Association. Knee stability and movementcoordination impairments: knee ligament sprain. J Orthop Sports Phys Ther. 2010Apr;40(4):A1-37.28. Kruse LM, Gray B, Wright RW. Rehabilitation after anterior cruciate ligamentreconstruction: a systematic review. J Bone Joint Surg Am. 2012 Oct 3;94(19):1737-48.29. Mayr HO, Weig TG, Plitz W. Arthrofibrosis following ACL reconstruction—reasonsand outcome. Arch Orthop Trauma Surg. 2004 Oct;124(8):518-22. Epub 2004 Aug 03.30. Eitzen I, Holm I, Risberg MA. Preoperative quadriceps strength is a significantpredictor of knee function two years after anterior cruciate ligament reconstruction.Br J Sports Med. 2009 May;43(5):371-6. Epub 2009 Feb 17.31. Shelbourne KD, Johnson BC. Effects of patellar tendon width and preoperativequadriceps strength on strength return after anterior cruciate ligament reconstruc-tion with ipsilateral bone-patellar tendon-bone autograft. Am J Sports Med. 2004Sep;32(6):1474-8. Epub 2004 Jul 20.32. Shen W, Forsythe B, Ingham SM, Honkamp NJ, Fu FH. Application of the ana-tomic double-bundle reconstruction concept to revision and augmentation anteriorcruciate ligament surgeries. J Bone Joint Surg Am. 2008 Nov;90(Suppl 4):20-34.33. Borbon CA, Mouzopoulos G, Siebold R. Why perform an ACL augmentation?Knee Surg Sports Traumatol Arthrosc. 2012 Feb;20(2):245-51. Epub 2011 Jun 09.34. Mifune Y, Ota S, Takayama K, Hoshino Y, Matsumoto T, Kuroda R, Kurosaka M, FuFH, Huard J. Therapeutic advantage in selective ligament augmentation for partial tearsof the anterior cruciate ligament: results in an animal model. Am J Sports Med. 2013Feb;41(2):365-73. Epub 2013 Jan 08.35. van Eck CF, Lesniak BP, Schreiber VM, Fu FH. Anatomic single- and double-bundle anterior cruciate ligament reconstruction flowchart. Arthroscopy. 2010 Feb;26(2):258-68.36. Kopf S, Pombo MW, Szczodry M, Irrgang JJ, Fu FH. Size variability of the humananterior cruciate ligament insertion sites. Am J Sports Med. 2011 Jan;39(1):108-13.Epub 2010 Sep 16.37. van Eck CF, Martins CA, Vyas SM, Celentano U, van Dijk CN, Fu FH. Femoralintercondylar notch shape and dimensions in ACL-injured patients. Knee Surg SportsTraumatol Arthrosc. 2010 Sep;18(9):1257-62.38. Steiner ME, Hecker AT, Brown CH Jr, Hayes WC. Anterior cruciate ligament graftfixation. Comparison of hamstring and patellar tendon grafts. Am J Sports Med.1994 Mar-Apr;22(2):240-6; discussion 246-7.39. Beynnon BD, Johnson RJ, Fleming BC, Kannus P, Kaplan M, Samani J, RenstromP. Anterior cruciate ligament replacement: comparison of bone-patellar tendon-bonegrafts with two-strand hamstring grafts. A prospective, randomized study. J Bone JointSurg Am. 2002 Sep;84(9):1503-13.40. Adam F, Pape D, Schiel K, Steimer O, Kohn D, Rupp S. Biomechanical propertiesof patellar and hamstring graft tibial fixation techniques in anterior cruciate ligamentreconstruction: experimental study with roentgen stereometric analysis. Am J SportsMed. 2004 Jan-Feb;32(1):71-8.41. Araujo P, van Eck CF, Torabi M, Fu FH. How to optimize the use of MRI in anatomicACL reconstruction. Knee Surg Sports Traumatol Arthrosc. 2013 Jul;21(7):1495-501.Epub 2012 Aug 15.42. Beyzadeoglu T, Akgun U, Tasdelen N, Karahan M. Prediction of semitendinosusand gracilis autograft sizes for ACL reconstruction. Knee Surg Sports TraumatolArthrosc. 2012 Jul;20(7):1293-7. Epub 2011 Nov 25.43. Wernecke G, Harris IA, Houang MT, Seeto BG, Chen DB, MacDessi SJ. Usingmagnetic resonance imaging to predict adequate graft diameters for autologoushamstring double-bundle anterior cruciate ligament reconstruction. Arthroscopy.2011 Aug;27(8):1055-9. Epub 2011 Jun 24.44. Magnussen RA, Lawrence JT, West RL, Toth AP, Taylor DC, Garrett WE. Graftsize and patient age are predictors of early revision after anterior cruciate ligamentreconstruction with hamstring autograft. Arthroscopy. 2012 Apr;28(4):526-31. Epub2012 Feb 01.45. Guo L, Yang L, Duan XJ, He R, Chen GX, Wang FY, Zhang Y. Anterior cruciateligament reconstruction with bone-patellar tendon-bone graft: comparison of autograft,fresh-frozen allograft, and g-irradiated allograft. Arthroscopy. 2012 Feb;28(2):211-7.
46. Rappe M, Horodyski M, Meister K, Indelicato PA. Nonirradiated versus irradiatedAchilles allograft: in vivo failure comparison. Am J Sports Med. 2007 Oct;35(10):1653-8. Epub 2007 May 21.47. Krych AJ, Jackson JD, Hoskin TL, Dahm DL. A meta-analysis of patellar tendonautograft versus patellar tendon allograft in anterior cruciate ligament reconstruction.Arthroscopy. 2008 Mar;24(3):292-8. Epub 2007 Nov 05.48. Borchers JR, Pedroza A, Kaeding C. Activity level and graft type as risk factors foranterior cruciate ligament graft failure: a case-control study. Am J Sports Med. 2009Dec;37(12):2362-7. Epub 2009 Aug 14.49. Kaeding CC, Aros B, Pedroza A, Pifel E, Amendola A, Andrish JT, Dunn WR, MarxRG, McCarty EC, Parker RD, Wright RW, Spindler KP. Allograft Versus AutograftAnterior Cruciate Ligament Reconstruction: Predictors of Failure From a MOONProspective Longitudinal Cohort. Sports Health. 2011 Jan;3(1):73-81.50. Singhal MC, Gardiner JR, Johnson DL. Failure of primary anterior cruciate liga-ment surgery using anterior tibialis allograft. Arthroscopy. 2007 May;23(5):469-75.51. van Eck CF, Schkrohowsky JG, Working ZM, Irrgang JJ, Fu FH. Prospective analysisof failure rate and predictors of failure after anatomic anterior cruciate ligament recon-struction with allograft. Am J Sports Med. 2012 Apr;40(4):800-7. Epub 2012 Jan 11.52. Leys T, Salmon L, Waller A, Linklater J, Pinczewski L. Clinical results and riskfactors for reinjury 15 years after anterior cruciate ligament reconstruction: a prospec-tive study of hamstring and patellar tendon grafts. Am J Sports Med. 2012 Mar;40(3):595-605. Epub 2011 Dec 19.53. Harner CD, Irrgang JJ, Paul J, Dearwater S, Fu FH. Loss of motion after anteriorcruciate ligament reconstruction. Am J Sports Med. 1992 Sep-Oct;20(5):499-506.54. Tashman S, Collon D, Anderson K, Kolowich P, Anderst W. Abnormal rotationalknee motion during running after anterior cruciate ligament reconstruction. Am JSports Med. 2004 Jun;32(4):975-83.55. McConkey MO, Amendola A, Ramme AJ, Dunn WR, Flanigan DC, Britton CL, WolfBR, Spindler KP, Carey JL, Cox CL, Kaeding CC, Wright RW, Matava MJ, Brophy RH,Smith MV, McCarty EC, Vida AF, Wolcott M, Marx RG, Parker RD, Andrish JF, JonesMH; MOON Knee Group. Arthroscopic agreement among surgeons on anterior cru-ciate ligament tunnel placement. Am J Sports Med. 2012 Dec;40(12):2737-46.Epub 2012 Oct 17.56. Illingworth KD, Hensler D, Working ZM, Macalena JA, Tashman S, Fu FH. A simpleevaluation of anterior cruciate ligament femoral tunnel position: the inclination angle andfemoral tunnel angle. Am J Sports Med. 2011 Dec;39(12):2611-8. Epub 2011 Sep 09.57. Bedi A, Musahl V, Steuber V, Kendoff D, Choi D, Allen AA, Pearle AD, Altchek DW.Transtibial versus anteromedial portal reaming in anterior cruciate ligament recon-struction: an anatomic and biomechanical evaluation of surgical technique. Ar-throscopy. 2011 Mar;27(3):380-90. Epub 2010 Oct 29.58. Forsythe B, Kopf S, Wong AK, Martins CA, Anderst W, Tashman S, Fu FH. Thelocation of femoral and tibial tunnels in anatomic double-bundle anterior cruciateligament reconstruction analyzed by three-dimensional computed tomography models.J Bone Joint Surg Am. 2010 Jun;92(6):1418-26.59. Lertwanich P, Martins CA, Asai S, Ingham SJ, Smolinski P, Fu FH. Anterior cruciateligament tunnel position measurement reliability on 3-dimensional reconstructedcomputed tomography. Arthroscopy. 2011 Mar;27(3):391-8. Epub 2010 Dec 03.60. Meuffels DE, Potters JW, Koning AH, Brown CH Jr, Verhaar JA, Reijman M.Visualization of postoperative anterior cruciate ligament reconstruction bone tunnels:reliability of standard radiographs, CT scans, and 3D virtual reality images. ActaOrthop. 2011 Dec;82(6):699-703. Epub 2011 Oct 17.61. Frobell RB, Roos EM, Roos HP, Ranstam J, Lohmander LS. A randomized trial oftreatment for acute anterior cruciate ligament tears. N Engl J Med. 2010 Jul 22;363(4):331-42.62. Frobell RB, Roos HP, Roos EM, Roemer FW, Ranstam J, Lohmander LS. Treat-ment for acute anterior cruciate ligament tear: five year outcome of randomised trial.BMJ. 2013;346:f232. Epub 2013 Jan 24.63. Tiamklang T, Sumanont S, Foocharoen T, Laopaiboon M. Double-bundle versussingle-bundle reconstruction for anterior cruciate ligament rupture in adults. Co-chrane Database Syst Rev. 2012;11:CD008413. Epub 2012 Nov 14.64. Hussein M, van Eck CF, Cretnik A, Dinevski D, Fu FH. Prospective randomizedclinical evaluation of conventional single-bundle, anatomic single-bundle, and ana-tomic double-bundle anterior cruciate ligament reconstruction: 281 cases with 3- to5-year follow-up. Am J Sports Med. 2012 Mar;40(3):512-20. Epub 2011 Nov 15.65. Hussein M, van Eck CF, Cretnik A, Dinevski D, FuFH. Individualized anterior cruciateligament surgery: a prospective study comparing anatomic single- and double-bundlereconstruction. Am J Sports Med. 2012 Aug;40(8):1781-8. Epub 2012 May 16.66. Sonnery-Cottet B, Panisset JC, Colombet P, Cucurulo T, Graveleau N, Hulet C,Potel JF, Servien E, Trojani C, Djian P, Pujol N; French Arthroscopy Society (SFA).Partial ACL reconstruction with preservation of the posterolateral bundle. OrthopTraumatol Surg Res. 2012 Dec;98(8)(Suppl):S165-70. Epub 2012 Nov 08.67. Adachi N, Ochi M, Uchio Y, Sumen Y. Anterior cruciate ligament augmentationunder arthroscopy. A minimum 2-year follow-up in 40 patients. Arch Orthop TraumaSurg. 2000;120(3-4):128-33.68. Papalia R, Franceschi F, Zampogna B, Tecame A, Maffulli N, Denaro V. Surgicalmanagement of partial tears of the anterior cruciate Knee Surg Sports TraumatolArthrosc. 2012 Dec 23. [Epub ahead of print].
693
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 96-A d NU M B E R 8 d A P R I L 16, 2014OP E R AT I V E TR E AT M E N T O F P R I M A RY AN T E R I O R
CRU C I AT E LI G A M E N T RU P T U R E I N AD U LT S

69. Georgoulis AD, Papadonikolakis A, Papageorgiou CD, Mitsou A, Stergiou N.Three-dimensional tibiofemoral kinematics of the anterior cruciate ligament-deficientand reconstructed knee during walking. Am J Sports Med. 2003 Jan-Feb;31(1):75-9.70. Abebe ES, Utturkar GM, Taylor DC, Spritzer CE, Kim JP, Moorman CT 3rd, GarrettWE, DeFrate LE. The effects of femoral graft placement on in vivo knee kinematicsafter anterior cruciate ligament reconstruction. J Biomech. 2011 Mar 15;44(5):924-9. Epub 2011 Jan 11.71. Tashman S, Araki D. Effects of anterior cruciate ligament reconstruction onin vivo, dynamic knee function. Clin Sports Med. 2013 Jan;32(1):47-59.72. Ardern CL, Webster KE, Taylor NF, Feller JA. Return to sport following anteriorcruciate ligament reconstruction surgery: a systematic review and meta-analysis ofthe state of play. Br J Sports Med. 2011 Jun;45(7):596-606. Epub 2011 Mar 11.73. Brophy RH, Schmitz L, Wright RW, Dunn WR, Parker RD, Andrish JT, McCarty EC,Spindler KP. Return to play and future ACL injury risk after ACL reconstruction insoccer athletes from the Multicenter Orthopaedic Outcomes Network (MOON) group.Am J Sports Med. 2012 Nov;40(11):2517-22. Epub 2012 Sep 21.74. Smith FW, Rosenlund EA, Aune AK, MacLean JA, Hillis SW. Subjective functionalassessments and the return to competitive sport after anterior cruciate ligamentreconstruction. Br J Sports Med. 2004 Jun;38(3):279-84.75. Rahr-Wagner L, Thillemann TM, Pedersen AB, Lind MC. Increased risk of revi-sion after anteromedial compared with transtibial drilling of the femoral tunnel duringprimary anterior cruciate ligament reconstruction: results from the Danish KneeLigament Reconstruction Register. Arthroscopy. 2013 Jan;29(1):98-105.76. Yagi M, Wong EK, Kanamori A, Debski RE, Fu FH, Woo SL. Biomechanicalanalysis of an anatomic anterior cruciate ligament reconstruction. Am J Sports Med.2002 Sep-Oct;30(5):660-6.77. Kato Y, Maeyama A, Lertwanich P, Wang JH, Ingham SJ, Kramer S, Martins CQ,Smolinski P, Fu FH. Biomechanical comparison of different graft positions forsingle-bundle anterior cruciate ligament reconstruction. Knee Surg Sports TraumatolArthrosc. 2013 Apr;21(4):816-23. Epub 2012 Mar 15.78. Bourke HE, Salmon LJ, Waller A, Patterson V, Pinczewski LA. Survival of theanterior cruciate ligament graft and the contralateral ACL at a minimum of 15 years.Am J Sports Med. 2012 Sep;40(9):1985-92. Epub 2012 Aug 06.79. Wright RW, Magnussen RA, Dunn WR, Spindler KP. Ipsilateral graft and con-tralateral ACL rupture at five years or more following ACL reconstruction: a systematicreview. J Bone Joint Surg Am. 2011 Jun 15;93(12):1159-65.
80. Shelbourne KD, Gray T, Haro M. Incidence of subsequent injury to either kneewithin 5 years after anterior cruciate ligament reconstruction with patellar tendonautograft. Am J Sports Med. 2009 Feb;37(2):246-51. Epub 2008 Dec 24.81. Li RT, Lorenz S, Xu Y, Harner CD, Fu FH, Irrgang JJ. Predictors of radiographicknee osteoarthritis after anterior cruciate ligament reconstruction. Am J Sports Med.2011 Dec;39(12):2595-603. Epub 2011 Oct 21.82. Roe J, Pinczewski LA, Russell VJ, Salmon LJ, Kawamata T, Chew M. A 7-yearfollow-up of patellar tendon and hamstring tendon grafts for arthroscopic anteriorcruciate ligament reconstruction: differences and similarities. Am J Sports Med.2005 Sep;33(9):1337-45. Epub 2005 Jul 07.83. Oiestad BE, Holm I, Aune AK, Gunderson R, Myklebust G, Engebretsen L,Fosdahl MA, Risberg MA. Knee function and prevalence of knee osteoarthritis afteranterior cruciate ligament reconstruction: a prospective study with 10 to 15 years offollow-up. Am J Sports Med. 2010 Nov;38(11):2201-10. Epub 2010 Aug 16.84. Øiestad BE, Holm I, Engebretsen L, Aune AK, Gunderson R, Risberg MA. Theprevalence of patellofemoral osteoarthritis 12 years after anterior cruciate ligamentreconstruction. Knee Surg Sports Traumatol Arthrosc. 2013 Apr;21(4):942-9. Epub2012 Aug 17.85. Salmon LJ, Russell VJ, Refshauge K, Kader D, Connolly C, Linklater J, Pinczewski LA.Long-term outcome of endoscopic anterior cruciate ligament reconstruction withpatellar tendon autograft: minimum 13-year review. Am J Sports Med. 2006May;34(5):721-32. Epub 2006 Jan 06.86. Shelbourne KD, Urch SE, Gray T, Freeman H. Loss of normal knee motion afteranterior cruciate ligament reconstruction is associated with radiographic arthriticchanges after surgery. Am J Sports Med. 2012 Jan;40(1):108-13. Epub 2011Oct 11.87. Shelbourne KD, Gray T. Minimum 10-year results after anterior cruciate ligamentreconstruction: how the loss of normal knee motion compounds other factors relatedto the development of osteoarthritis after surgery. Am J Sports Med. 2009 Mar;37(3):471-80. Epub 2008 Dec 04.88. Lebel B, Hulet C, Galaud B, Burdin G, Locker B, Vielpeau C. Arthroscopic recon-struction of the anterior cruciate ligament using bone-patellar tendon-bone autograft: aminimum 10-year follow-up. Am J Sports Med. 2008 Jul;36(7):1275-82. Epub 2008Mar 19.89. Wright JG, Einhorn TA, Heckman JD. Grades of recommendation. J Bone JointSurg Am. 2005 Sep 01;87(9):1909-10.
694
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 96-A d NU M B E R 8 d A P R I L 16, 2014OP E R AT I V E TR E AT M E N T O F P R I M A RY AN T E R I O R
CRU C I AT E LI G A M E N T RU P T U R E I N AD U LT S
journal of orthopaedic & sports physical therapy | volume 42 | number 11 | november 2012 | 893
[ research report ]
Anterior cruciate ligament (ACL) injuries commonly occur during sports-related activities that
require cutting and pivoting, with over 200 000 injuries reported in the United States each year.23
Most individuals elect to undergo surgi-cal reconstruction following injury to re-store knee function and facilitate return to sports participation.51,56 Although ACL reconstruction is thought to provide the athlete with the best opportunity to re-turn to preinjury levels of sports partici-pation,33 recent studies1,2,21,30,38,57 reported that between 8% and 50% of those with ACL reconstruction did not return to the same sports after surgery, even with fol-low-up times of up to 5 years.31 Moreover, as many as 70% of individuals previously involved in contact sports were unable to return to the same sports after sur-
TT STUDY DESIGN: Cross-sectional cohort.
TT OBJECTIVES: (1) To examine differences in clinical variables (demographics, knee impair-ments, and self-report measures) between those who return to preinjury level of sports participation and those who do not at 1 year following anterior cruciate ligament reconstruction, (2) to deter-mine the factors most strongly associated with return-to-sport status in a multivariate model, and (3) to explore the discriminatory value of clinical variables associated with return to sport at 1 year postsurgery.
TT BACKGROUND: Demographic, physical impair-ment, and psychosocial factors individually prohibit return to preinjury levels of sports participation. However, it is unknown which combination of factors contributes to sports participation status.
TT METHODS: Ninety-four patients (60 men; mean age, 22.4 years) 1 year post–anterior cruciate liga-ment reconstruction were included. Clinical vari-ables were collected and included demographics, knee impairment measures, and self-report ques-tionnaire responses. Patients were divided into “yes return to sports” or “no return to sports” groups based on their answer to the question, “Have you returned to the same level of sports as before your injury?” Group differences in demographics, knee impairments, and self-report questionnaire responses were analyzed. Discriminant function analysis determined the strongest predictors of group classification. Receiver-operating-char-
acteristic curves determined the discriminatory accuracy of the identified clinical variables.
TT RESULTS: Fifty-two of 94 patients (55%) report-ed yes return to sports. Patients reporting return to preinjury levels of sports participation were more likely to have had less knee joint effusion, fewer epi-sodes of knee instability, lower knee pain intensity, higher quadriceps peak torque-body weight ratio, higher score on the International Knee Documenta-tion Committee Subjective Knee Evaluation Form, and lower levels of kinesiophobia. Knee joint effusion, episodes of knee instability, and score on the International Knee Documentation Committee Subjective Knee Evaluation Form were identi-fied as the factors most strongly associated with self-reported return-to-sport status. The highest positive likelihood ratio for the yes-return-to-sports group classification (14.54) was achieved when patients met all of the following criteria: no knee ef-fusion, no episodes of instability, and International Knee Documentation Committee Subjective Knee Evaluation Form score greater than 93.
TT CONCLUSION: In multivariate analysis, the fac-tors most strongly associated with return-to-sport status included only self-reported knee function, episodes of knee instability, and knee joint effusion.
TT LEVEL OF EVIDENCE: Prognosis, level 2b. J Orthop Sports Phys Ther 2012;42(11):893-901, Epub 2 August 2012. doi:10.2519/jospt.2012.4077
TT KEY WORDS: ACL, kinesiophobia, return to sports
1Staff Physical Therapist, Shands Rehab Center, University of Florida Orthopaedics and Sports Medicine Institute, Gainesville, FL. 2Clinical Coordinator, Shands Rehab Center, University of Florida Orthopaedics and Sports Medicine Institute, Gainesville, FL. 3Orthopaedic Surgeon, Department of Orthopaedics and Rehabilitation, University of Florida, Gainesville, FL. 4Associate Professor and Assistant Department Chair, Department of Physical Therapy, University of Florida, Gainesville, FL. 5Associate Professor, Department of Physical Therapy, University of Florida, Gainesville, FL. Dr Chmielewski’s effort on this project was supported by a grant from the National Institutes of Health (K01-HD052713) and by the National Center for Medical Rehabilitation Research. This project was reviewed and approved by the Institutional Review Board at the University of Florida. Address correspondence to Trevor Lentz, Shands Rehab Center, University of Florida Orthopaedics and Sports Medicine Institute, 3450 Hull Road, Gainesville, FL 32611. E-mail: [email protected] T Copyright ©2012 Journal of Orthopaedic & Sports Physical Therapy
TREVOR A. LENTZ, PT1 • GIORGIO ZEPPIERI, JR., PT1 • SUSAN M. TILLMAN, PT2 • PETER A. INDELICATO, MD3
MICHAEL W. MOSER, MD3 • STEVEN Z. GEORGE, PT, PhD4 • TERESE L. CHMIELEWSKI, PT, PhD5
Return to Preinjury Sports Participation Following Anterior Cruciate Ligament
Reconstruction: Contributions of Demographic, Knee Impairment,
and Self-report Measures
42-11 Lentz.indd 893 10/17/2012 2:58:32 PM
Jour
nal o
f O
rtho
paed
ic &
Spo
rts
Phys
ical
The
rapy
®
Dow
nloa
ded
from
ww
w.jo
spt.o
rg a
t JO
SPT
on
Aug
ust 2
0, 2
014.
For
per
sona
l use
onl
y. N
o ot
her
uses
with
out p
erm
issi
on.
Cop
yrig
ht ©
201
2 Jo
urna
l of
Ort
hopa
edic
& S
port
s Ph
ysic
al T
hera
py®
. All
righ
ts r
eser
ved.

894 | november 2012 | volume 42 | number 11 | journal of orthopaedic & sports physical therapy
[ research report ]gery.47 Of those individuals who did re-turn to their prior sports, up to 21% were reported to have returned with major functional limitations that contributed to a reduced level of performance.49 For ex-ample, a study of running backs and wide receivers in the National Football League found that almost 80% returned to com-petition after ACL injury, but player per-formance, measured by power ratings, was reduced by one-third.10 Moreover, 22% of the athletes with ACL recon-struction in the National Basketball As-sociation did not return to a sanctioned National Basketball Association game af-ter surgery and, of those who did return, 44% experienced a decrease in standard statistical categories and player efficiency ratings.9 It has been suggested that the high incidence of poor return-to-sport outcomes following ACL reconstruction may be due to a lack of standardized re-turn-to-sport guidelines and incomplete resolution of physical and psychological impairments.3,32,36,37
Poor understanding of the important factors that determine a successful return to sports has contributed to variability in return-to-sport criteria.4,29 Many crite-ria have been developed based on expert opinion, empirical evidence, or factors identified as contributors to postop-erative self-reported disability following ACL reconstruction, including number of injured knee structures,48 quadriceps strength,32,45,58 knee pain intensity,32,58 knee flexion range of motion (ROM),32 single-leg hop performance,48,55,58 and pain-related fear of movement/reinju-ry.11,30-32 Although these factors have been associated with self-reported knee func-tion, it is unclear if they influence return to preinjury levels of sports participation following ACL reconstruction. Further-more, the relative importance of these factors is unknown. To our knowledge, no study to date has examined demo-graphic, knee impairment, and psycho-social measures in a multivariate model to determine the most important factors associated with return to preinjury levels of sports participation.
Understanding differences between individuals who do or do not return to sport after ACL reconstruction is the next step toward developing evidence-based return-to-sport rehabilitation guidelines and participation criteria. The purposes of this study were (1) to examine differ-ences in clinical variables (demograph-ics, knee impairments, and self-report measures) between those who return to preinjury level of sports participation and those who do not at 1 year following ACL reconstruction, (2) to determine the factors most strongly associated with return-to-sport status in a multivariate model, and (3) to explore the discrimina-tory value of clinical variables associated with return to sport at 1 year postsur-gery. Based on previous literature, we hypothesized that a combination of de-mographic, knee impairment, functional, and psychosocial measures would differ and discriminate between those who did and did not return to sports.
METHODS
Patients
Consecutive patients with ACL reconstruction seen for routine physician follow-up at 1 year post-
surgery at the University of Florida Orthopaedics and Sports Medicine In-stitute, Gainesville, FL, were eligible to participate. Patients were enrolled over a 3-year period between September 2007 and September 2010. Inclusion criteria were (1) unilateral arthroscopic ACL reconstruction, (2) age between 15 and 50 years, (3) time from injury to sur-gery of 12 months or less, and (4) prein-jury score of 5 or greater on the Tegner activity-level scale. Our age group was chosen to include individuals most likely to be involved in sports-related activities and undergo ACL reconstruction follow-ing ACL injury. We specified a preinjury Tegner activity level of at least 5 to target a population of patients who were, at a minimum, involved in recreational sports prior to injury. Potential patients were ex-cluded if they had (1) bilateral knee in-
jury, (2) prior knee ligament injury and/or surgery, (3) concomitant ligamentous injury greater than grade I, (4) articular cartilage repair procedure performed in conjunction with ACL reconstruction, or (5) inability to return to sports following surgery due to social reasons (too little time to participate in sports or a change in lifestyle).31 In communities with a high prevalence of college students, such as the one from which the present sample was drawn, it has been observed that some individuals choose not to return to sport due to too little time to participate in sports or to a change in lifestyle (they at-tend graduate school, graduate, get a job, start a family, etc). As a result, many of these individuals may not have the moti-vation or potential to return to sport due to influences other than their physical or psychological capabilities. Other exclu-sion criteria were chosen because they represent additional injuries or surgical procedures that may significantly affect the course of rehabilitation or functional outcome.48 Patients provided written in-formed consent, and the protocol for the study was approved by the University of Florida Institutional Review Board.
Surgical Procedure and Rehabilitation ProgramAll surgical procedures were performed arthroscopically by a board-certified or-thopaedic surgeon (P.A.I. or M.W.M.), using autograft or allograft tissue. The autograft sources were bone-patellar tendon-bone or semitendinosus and gracilis tendons. The allograft sources were tibialis anterior, tibialis posterior, or Achilles tendon. The surgical procedure, as well as graft selection process, for our surgeons has been previously published.13 Rehabilitation was not controlled in this study; however, the standard ACL recon-struction rehabilitation protocol used in our facility and given to patients under-going rehabilitation at outside facilities allows for immediate weight bearing and knee motion as tolerated. The empha-sis of the first 6 weeks of rehabilitation is on decreasing knee effusion, develop-
42-11 Lentz.indd 894 10/17/2012 2:58:33 PM
Jour
nal o
f O
rtho
paed
ic &
Spo
rts
Phys
ical
The
rapy
®
Dow
nloa
ded
from
ww
w.jo
spt.o
rg a
t JO
SPT
on
Aug
ust 2
0, 2
014.
For
per
sona
l use
onl
y. N
o ot
her
uses
with
out p
erm
issi
on.
Cop
yrig
ht ©
201
2 Jo
urna
l of
Ort
hopa
edic
& S
port
s Ph
ysic
al T
hera
py®
. All
righ
ts r
eser
ved.

journal of orthopaedic & sports physical therapy | volume 42 | number 11 | november 2012 | 895
ing quadriceps control, and regaining full knee motion. The next 6 weeks of rehabilitation are focused on increasing lower extremity muscle strength, muscle endurance, and neuromuscular control. Straight-ahead running is permitted at 12 weeks if (1) quadriceps strength sym-metry index is greater than 60%, (2) knee effusion is trace or less, (3) knee exten-sion ROM is equal to the contralateral side, (4) knee flexion ROM is within 5° of the contralateral side, and (5) aver-age knee pain is less than 2/10. Agility exercises are initiated at 18 weeks post-surgery following successful completion of a straight-ahead running program. Patients are allowed to return to sport when the following criteria are met: (1) knee ROM equal to the contralateral side, (2) quadriceps strength greater than 85% of the opposite knee based on isokinetic testing, (3) no knee effusion, and (4) completion of an agility and sport-spe-cific program. These criteria are typically met around 6 months postsurgery.
Testing OverviewPatients were tested at a routine 1-year clinical follow-up visit. A standardized testing protocol consisted of the collec-tion of demographic information, knee impairment measures, and self-report questionnaire responses. Testers were physical therapists with an average of 10.3 years (range, 5-17 years) of experi-ence in sports physical therapy. Data were recorded on standard forms and entered into an electronic database (Mi-crosoft Access 2007; Microsoft Corpora-tion, Redmond, WA).
Demographic InformationDemographic information included age, sex, weight, time from injury to surgery, graft type (autograft or allograft), con-comitant knee injuries, and time from surgery to follow-up. Concomitant inju-ries were diagnosed during the preop-erative physician evaluation or during surgery, and included meniscal injuries, chondral lesions, and collateral ligament injuries.
Knee Impairment MeasuresKnee Effusion Knee effusion was as-sessed with the stroke test and graded on a 5-point scale (none, trace, 1+, 2+, and 3+).50 This method of assessing knee effu-sion has a substantial interrater reliabil-ity (κ = 0.75).50
Knee ROM Knee flexion and extension passive ROM were measured in both the nonsurgical and surgical sides us-ing a standard goniometer. Side-to-side knee flexion and extension ROM deficits were calculated (nonsurgical-side ROM minus surgical-side ROM). Intertester reliability has been shown to be high for measurements of knee flexion ROM (in-traclass correlation coefficient [ICC] = 0.98) and knee extension ROM (ICC = 0.89-0.93) using a standard goniometer.8
Knee Ligament Laxity Testing To assess the integrity of the ACL graft, anterior displacement of the tibia was measured with a KT1000 knee ligament arthrome-ter (MEDmetric Corporation, San Diego, CA). The tibia was pulled to the end point of anterior translation while the knee was flexed to approximately 30°. The amount of anterior displacement was recorded in millimeters. Two trials were performed on each side and averaged. The differ-ence in values between the surgical and nonsurgical sides was recorded as the anterior knee joint laxity difference. The KT1000 has been shown to provide val-id44,46 and reliable measurements of ante-rior knee joint laxity (ICC = 0.91-0.93).7
Quadriceps Strength Testing Knee ex-tensor (quadriceps) strength was as-sessed with an isokinetic dynamometer (Biodex System 3; Biodex Medical Sys-tems, Shirley, NY). Prior to testing, pa-tients were given a 5-minute warm-up on a stationary bicycle. They were then seated and stabilized with a lap-and-thigh belt. The dynamometer arm was set to move through a range of 90° to 0° of knee motion at a speed of 60°/s. Test-ing was conducted on the nonsurgical side first. Patients performed 2 practice trials followed by 5 maximal-effort trials. Testing was then repeated on the surgi-cal side. The peak knee extensor torque
of 5 trials was recorded for each side. Two separate measures of quadriceps muscle performance were calculated. First, a quadriceps symmetry index was calcu-lated by normalizing the peak knee ex-tensor torque on the surgical side to that of the nonsurgical side and multiplying by 100. Second, the knee extensor torque-body weight ratio was calculated by di-viding knee extensor peak torque (ft·lb) of the surgical side by the subject’s body weight (lb). Isokinetic strength testing has been shown to be a reliable meth-od of quadriceps strength testing (ICC = 0.81-0.97)7 and sensitive to strength changes in the first 2 years following ACL reconstruction.45
Self-report QuestionnairesTegner Activity-Level Scale The Tegner activity-level scale is an 11-point grad-ing scale for work and sports activities.52 The scale rates activity level from 0 (sick leave or disability pension because of knee problems) to 10 (competitive sports such as soccer, football, or rugby at the national or elite level). Level 5 indicates participation in sport-related activities at the lowest recreational level. The scale was initially developed to measure activ-ity following knee ligamentous injury and has been validated for use following ACL injury.6 The Tegner scale has demonstrat-ed acceptable test-retest reliability (ICC = 0.80) after ACL reconstruction.6 At the time of follow-up testing, patients were asked to rate their current level of sports participation as well as to recall their pre-injury level of sports participation.Knee Pain Intensity Knee pain inten-sity was assessed with an 11-point visual numeric rating scale. Pain intensity rat-ings ranged from 0 (no pain) to 10 (worst imaginable pain). Patients were asked to rate their worst and best pain levels over the past 24 hours. They were also asked to rate their current level of pain. All 3 pain ratings were averaged to get a composite knee pain intensity score. The numeric rating scale has been shown to be a reliable method of pain intensity as-sessment (ICC = 0.74-0.76).14,34
42-11 Lentz.indd 895 10/17/2012 2:58:35 PM
Jour
nal o
f O
rtho
paed
ic &
Spo
rts
Phys
ical
The
rapy
®
Dow
nloa
ded
from
ww
w.jo
spt.o
rg a
t JO
SPT
on
Aug
ust 2
0, 2
014.
For
per
sona
l use
onl
y. N
o ot
her
uses
with
out p
erm
issi
on.
Cop
yrig
ht ©
201
2 Jo
urna
l of
Ort
hopa
edic
& S
port
s Ph
ysic
al T
hera
py®
. All
righ
ts r
eser
ved.

896 | november 2012 | volume 42 | number 11 | journal of orthopaedic & sports physical therapy
[ research report ]Episodes of Knee Instability Patients were asked, “How many episodes of giv-ing way or buckling at the knee have occurred since your surgery?” Possible answers included 0, 1, 2 to 5, and greater than 5.Tampa Scale for Kinesiophobia Kine-siophobia, or fear of movement/reinjury, was measured with the shortened version of the Tampa Scale for Kinesiophobia (TSK-11).59 Response items are related to somatic sensations (eg, “Pain always means I have injured my body”) and activity avoidance (eg, “I’m afraid that I might injure myself if I exercise”). Scores on the TSK-11 range from 11 to 44 points, with higher scores indicating greater pain-related fear of movement/reinjury. Good test-retest reliability (ICC = 0.81 and 0.93)20,59 has been reported for the TSK-11 in patients with chronic low back pain. The TSK-11 is a psychometrically stable instrument to assess fear of move-ment/reinjury in the later stages of reha-bilitation following ACL reconstruction.19
International Knee Documentation Committee Subjective Knee Evaluation Form Knee function was measured with the International Knee Documentation Committee Subjective Knee Evalua-tion Form (IKDC). The IKDC contains 10 items related to knee symptoms and physical function.26 Scores range from 0 to 100, with higher scores indicating less disability. An ICC of 0.94 and a standard-ized response mean of 0.94 have been re-ported for the IKDC across a broad range of knee pathologies, including ACL injury and ACL reconstruction.26,27
Return-to-Sport Status All patients were asked 2 questions regarding their return-to-sport status: (1) “Have you returned to sports or recreational activities since your surgery?” and (2) “Have you returned to the same level of sports as before your in-jury?” Because our purpose was to specif-ically examine return to preinjury levels of sports participation, patients were di-vided into return-to-sport-status groups based on their answer to the question, “Have you returned to the same level of sports as before your injury?” Those who
indicated that they had returned to the same level of preinjury sports participa-tion were designated Y-RTS (yes return to sports), and those who reported that they had not returned to the same level were designated N-RTS (no return to sports). Patients who reported that they had not returned to preinjury levels of sports participation were asked to pick their primary reason for not having returned from a list of options that included pain, swelling, fear of injury or lack of confi-dence, knee instability, muscle weakness, not yet cleared from doctor to return to sports, too little time to participate or had a change in lifestyle, and other. This an-swer represented the subject’s perceived reason for not being able to return to the preinjury level of sports participation.
Statistical AnalysisStatistical analyses were conducted with SPSS for Windows Version 13.0 (SPSS
Inc, Chicago, IL). Descriptive statistics were generated for all variables. We ana-lyzed the data in the following steps: (1) identification of clinical factors that dif-fered between groups based on return-to-sport status, (2) determination of the factors most strongly associated with return-to-sport status in a multivariate model, and (3) testing the discrimina-tory value of clinical variables associated with return-to-sport group allocation. An alpha level of .05 was used for inferential analyses.
For the first step, independent-sam-ples t tests determined group differences (Y-RTS versus N-RTS) in continuous variables, and chi-square tests were used for categorical variables. If any individu-al cells were below 5, we used the Fisher exact test instead of chi-square analysis. A 2-way repeated-measures analysis of variance was used to analyze preinjury-to-postsurgical changes in Tegner score
TABLE 1Demographic Variable Means and
Distributions for Y-RTS and N-RTS Groups*
Abbreviations: N-RTS, patients indicating they had not returned to preinjury levels of sports partici-pation; Y-RTS, patients indicating they had returned to preinjury levels of sports participation.*Values are mean SD.†Significance of difference between Y-RTS and N-RTS group means.
Measure Y-RTS (n = 52) N-RTS (n = 42) Total (n = 94) P Value†
Injury to surgery, d 70.6 56.6 80.4 66.5 75.0 61.0 .44
Preinjury Tegner score 8.4 1.6 8.3 1.6 8.4 1.5 .76
Postsurgical Tegner score 8.3 1.6 6.6 1.8 7.5 1.9 <.001
Surgery to follow-up, wk 50.9 4.0 49.5 5.7 50.2 4.8 .17
TABLE 2Distribution of Self-reported Primary
Reasons for Not Returning to Preinjury Levels of Sports Participation
Abbreviation: N-RTS, patients indicating they had not returned to preinjury levels of sports participation.
Primary Reason, n N-RTS, %
Pain 5 12
Swelling 3 7
Fear of injury or lack of confidence 19 45
Knee instability 4 10
Muscle weakness 5 12
Not yet cleared from doctor to return to sports 5 12
Other 1 2
42-11 Lentz.indd 896 10/17/2012 2:58:36 PM
Jour
nal o
f O
rtho
paed
ic &
Spo
rts
Phys
ical
The
rapy
®
Dow
nloa
ded
from
ww
w.jo
spt.o
rg a
t JO
SPT
on
Aug
ust 2
0, 2
014.
For
per
sona
l use
onl
y. N
o ot
her
uses
with
out p
erm
issi
on.
Cop
yrig
ht ©
201
2 Jo
urna
l of
Ort
hopa
edic
& S
port
s Ph
ysic
al T
hera
py®
. All
righ
ts r
eser
ved.
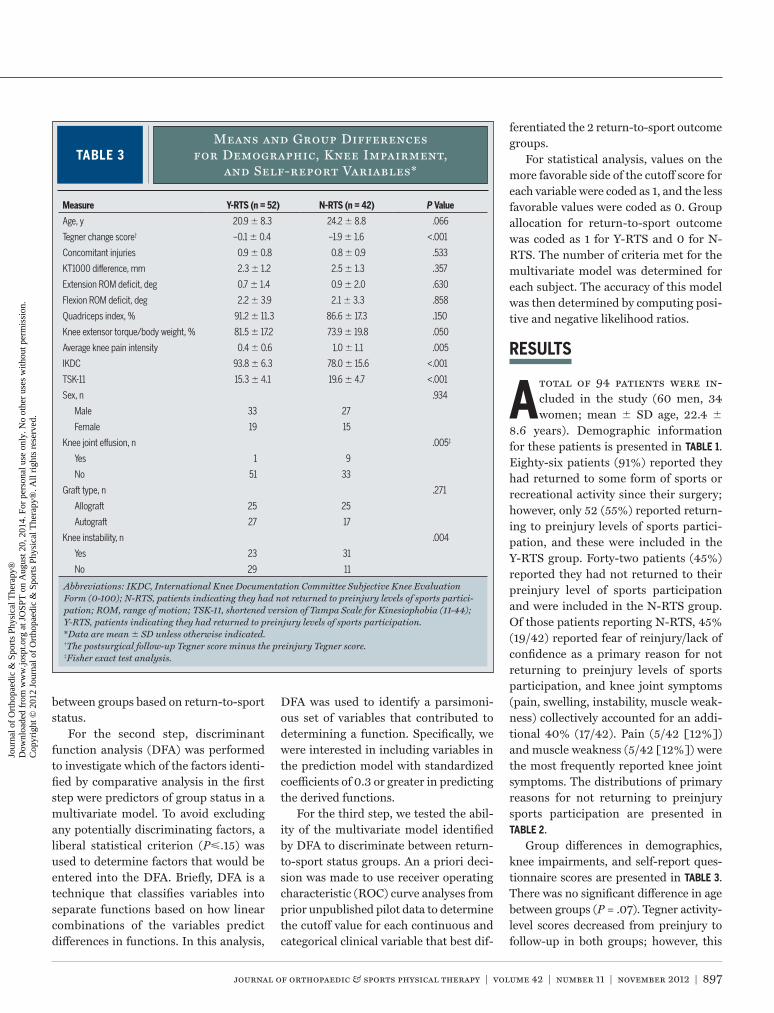
journal of orthopaedic & sports physical therapy | volume 42 | number 11 | november 2012 | 897
between groups based on return-to-sport status.
For the second step, discriminant function analysis (DFA) was performed to investigate which of the factors identi-fied by comparative analysis in the first step were predictors of group status in a multivariate model. To avoid excluding any potentially discriminating factors, a liberal statistical criterion (P.15) was used to determine factors that would be entered into the DFA. Briefly, DFA is a technique that classifies variables into separate functions based on how linear combinations of the variables predict differences in functions. In this analysis,
DFA was used to identify a parsimoni-ous set of variables that contributed to determining a function. Specifically, we were interested in including variables in the prediction model with standardized coefficients of 0.3 or greater in predicting the derived functions.
For the third step, we tested the abil-ity of the multivariate model identified by DFA to discriminate between return-to-sport status groups. An a priori deci-sion was made to use receiver operating characteristic (ROC) curve analyses from prior unpublished pilot data to determine the cutoff value for each continuous and categorical clinical variable that best dif-
ferentiated the 2 return-to-sport outcome groups.
For statistical analysis, values on the more favorable side of the cutoff score for each variable were coded as 1, and the less favorable values were coded as 0. Group allocation for return-to-sport outcome was coded as 1 for Y-RTS and 0 for N-RTS. The number of criteria met for the multivariate model was determined for each subject. The accuracy of this model was then determined by computing posi-tive and negative likelihood ratios.
RESULTS
A total of 94 patients were in-cluded in the study (60 men, 34 women; mean SD age, 22.4
8.6 years). Demographic information for these patients is presented in TABLE 1. Eighty-six patients (91%) reported they had returned to some form of sports or recreational activity since their surgery; however, only 52 (55%) reported return-ing to preinjury levels of sports partici-pation, and these were included in the Y-RTS group. Forty-two patients (45%) reported they had not returned to their preinjury level of sports participation and were included in the N-RTS group. Of those patients reporting N-RTS, 45% (19/42) reported fear of reinjury/lack of confidence as a primary reason for not returning to preinjury levels of sports participation, and knee joint symptoms (pain, swelling, instability, muscle weak-ness) collectively accounted for an addi-tional 40% (17/42). Pain (5/42 [12%]) and muscle weakness (5/42 [12%]) were the most frequently reported knee joint symptoms. The distributions of primary reasons for not returning to preinjury sports participation are presented in TABLE 2.
Group differences in demographics, knee impairments, and self-report ques-tionnaire scores are presented in TABLE 3. There was no significant difference in age between groups (P = .07). Tegner activity-level scores decreased from preinjury to follow-up in both groups; however, this
TABLE 3Means and Group Differences
for Demographic, Knee Impairment, and Self-report Variables*
Abbreviations: IKDC, International Knee Documentation Committee Subjective Knee Evaluation Form (0-100); N-RTS, patients indicating they had not returned to preinjury levels of sports partici-pation; ROM, range of motion; TSK-11, shortened version of Tampa Scale for Kinesiophobia (11-44); Y-RTS, patients indicating they had returned to preinjury levels of sports participation.*Data are mean SD unless otherwise indicated.†The postsurgical follow-up Tegner score minus the preinjury Tegner score.‡Fisher exact test analysis.
Measure Y-RTS (n = 52) N-RTS (n = 42) P Value
Age, y 20.9 8.3 24.2 8.8 .066
Tegner change score† –0.1 0.4 –1.9 1.6 <.001
Concomitant injuries 0.9 0.8 0.8 0.9 .533
KT1000 difference, mm 2.3 1.2 2.5 1.3 .357
Extension ROM deficit, deg 0.7 1.4 0.9 2.0 .630
Flexion ROM deficit, deg 2.2 3.9 2.1 3.3 .858
Quadriceps index, % 91.2 11.3 86.6 17.3 .150
Knee extensor torque/body weight, % 81.5 17.2 73.9 19.8 .050
Average knee pain intensity 0.4 0.6 1.0 1.1 .005
IKDC 93.8 6.3 78.0 15.6 <.001
TSK-11 15.3 4.1 19.6 4.7 <.001
Sex, n .934
Male 33 27
Female 19 15
Knee joint effusion, n .005‡
Yes 1 9
No 51 33
Graft type, n .271
Allograft 25 25
Autograft 27 17
Knee instability, n .004
Yes 23 31
No 29 11
42-11 Lentz.indd 897 10/17/2012 2:58:37 PM
Jour
nal o
f O
rtho
paed
ic &
Spo
rts
Phys
ical
The
rapy
®
Dow
nloa
ded
from
ww
w.jo
spt.o
rg a
t JO
SPT
on
Aug
ust 2
0, 2
014.
For
per
sona
l use
onl
y. N
o ot
her
uses
with
out p
erm
issi
on.
Cop
yrig
ht ©
201
2 Jo
urna
l of
Ort
hopa
edic
& S
port
s Ph
ysic
al T
hera
py®
. All
righ
ts r
eser
ved.

898 | november 2012 | volume 42 | number 11 | journal of orthopaedic & sports physical therapy
[ research report ]
decrease was found to be statistically sig-nificant in the N-RTS group only. Patients in the Y-RTS group had less presurgical-to-postsurgical change in Tegner score (P<.001), lower grade of knee joint effu-sion (P = .005), fewer episodes of knee instability (P = .004), lower knee pain intensity (P = .005), higher quadriceps peak torque-body weight ratio (P = .050), higher IKDC score (P<.001), and lower TSK-11 score (P<.001).
The clinical variables entered into DFA were knee joint effusion, episodes of knee instability, knee pain intensity, quadriceps peak torque-body weight ra-tio, IKDC score, and TSK-11 score. In this analysis, a statistically significant func-tion for determination of return-to-sport status was determined (Wilks’ λ = .571, P<.001). Investigation of the standardized coefficients indicated that the strongest contributors to this function were knee joint effusion (.519), episodes of knee in-stability (.357), and IKDC score (–.788).
The accuracy for the final multivari-ate model (range of clinical variables, 0-3) is reported in TABLE 4. Based on pri-or unpublished data, the following cutoff scores were set for each variable in the final multivariate model: effusion rated as none, no episode of instability, and IKDC score greater than 93. Likelihood ratio analysis indicated that meeting all 3 of the criteria resulted in a large shift (positive likelihood ratio, 14.54) in post-
test probability of being associated with Y-RTS status. Alternatively, meeting only 1 of the criteria reduced the post-test probability of being associated with Y-RTS status compared to pretest prob-ability (negative likelihood ratio, 0.16).
DISCUSSION
The purposes of this study were (1) to examine differences in clini-cal variables (demographics, knee
impairments, and self-report measures) between those who return to preinjury level of sports participation and those who do not at 1 year following ACL re-construction, (2) to determine the factors most strongly associated with return-to-sport status in a multivariate model, and (3) to explore the discriminatory value of clinical variables associated with return to sport at 1 year postsurgery. Although the majority of patients in our study had returned to sports following ACL recon-struction, only 55% reported they had returned to preinjury levels of sports par-ticipation at 1 year. We hypothesized that a combination of demographic, physical impairment, and psychosocial measures would differ and discriminate between those who reported participation in sports-related activities at preinjury lev-els and those who did not. This study identified a variety of factors that differed between groups based on return-to-sport
status, with knee impairment and self-re-ported function measures as the factors most strongly associated with returning to preinjury sports participation. These factors are potentially modifiable and should be considered when developing return-to-sport rehabilitation guidelines and participation criteria following ACL reconstruction.
Many of the factors that differed be-tween return-to-sport-status groups in this study, such as quadriceps strength, knee pain intensity, self-reported knee function, and fear of movement/reinjury, have also been associated with knee func-tion in prior studies.11,19,30-32,45,58 The lack of group differences in demographics in-dicates that nonmodifiable factors, such as age, sex, and concomitant injury, or po-tentially modifiable factors, such as graft type and time from injury to surgery, may not play a significant role in return-to-sport status. These findings support prior studies that have failed to show a strong relationship between demographic mea-sures and function.5,16,18,25,28,35,39,44,47 An interesting finding in this study was that quadriceps peak torque on the surgical side normalized to body weight differed between return-to-sport-status groups, but quadriceps symmetry index did not differ between groups. Prior studies have reported inconsistent results regarding the influence of quadriceps performance on functional outcomes.22,32,48,58 This in-consistency appears to be closely tied to the method by which quadriceps per-formance is measured or the outcome used22,32,48,58 and may be influenced by variability in rehabilitation programs. The results of this study indicate that though quadriceps strength normalized to body weight may be an important consideration when determining ability for return to sports, quadriceps strength asymmetry is not a discriminating fac-tor between return-to-sport groups. The importance of quadriceps symmetry, however, and its implication for reinjury should not be overlooked. Prior studies have demonstrated the predictive value of strength asymmetries for risk of rein-
TABLE 4 Multivariate Model Analysis*
Criteria Met, n Sensitivity Specificity
Positive Likelihood
Ratio
Negative Likelihood
Ratio Y-RTS Group N-RTS Group
0 1.00 0.00 1.00 Undefined 1 5
1 0.98 0.12 1.11 0.16 6 23
2 0.87 0.67 2.60 0.20 27 13
3 0.35 0.98 14.54 0.67 18 1
Abbreviations: N-RTS, patients indicating they had not returned to preinjury levels of sports partici-pation; Y-RTS, patients indicating they had returned to preinjury levels of sports participation.*Variables included in the model: no knee joint effusion, no episodes of knee instability, International Knee Documentation Committee Subjective Knee Evaluation Form (0-100) score greater than 93 (area under curve, 0.815; P<.001).
Patients Meeting Criteria, n
42-11 Lentz.indd 898 10/17/2012 2:58:38 PM
Jour
nal o
f O
rtho
paed
ic &
Spo
rts
Phys
ical
The
rapy
®
Dow
nloa
ded
from
ww
w.jo
spt.o
rg a
t JO
SPT
on
Aug
ust 2
0, 2
014.
For
per
sona
l use
onl
y. N
o ot
her
uses
with
out p
erm
issi
on.
Cop
yrig
ht ©
201
2 Jo
urna
l of
Ort
hopa
edic
& S
port
s Ph
ysic
al T
hera
py®
. All
righ
ts r
eser
ved.

journal of orthopaedic & sports physical therapy | volume 42 | number 11 | november 2012 | 899
jury,43 and it is commonly suggested that these asymmetries should be resolved prior to initiation of sports activities.36,41,42
Although some variables previously associated with function following ACL reconstruction, such as knee pain inten-sity,32,58 fear of movement/reinjury,11,30-32 and quadriceps strength,32,45,58 had bi-variate associations with return to pre-injury sport participation, they were not retained in multivariate analysis. Perhaps the most unexpected finding was the ex-clusion of fear of movement/reinjury from the model, because this has been strongly associated with return to sports participation in prior studies29,31 and was the most prevalent reason cited for not returning to sport in our sample. Some authors have speculated that psychoso-cial factors, such as fear of movement/reinjury, may help to explain the discrep-ancy between generally favorable knee scores and poor return-to-sport rates following surgery.2,3 It is plausible that fear of movement/reinjury may mediate the relationship between activity restric-tions and factors included in the model (ie, instability or self-reported function), yet not be identified as a significant in-dividual factor in multivariate analysis. Thus, concurrent assessment of pain-related fear of movement/reinjury and clinical measures may be unnecessary for prediction of return-to-sport status, be-cause no further variance was explained by inclusion of this construct in the mul-tivariate model.
A strength of this study is that it is the first, to our knowledge, to study the contributions of demographic, knee im-pairment, and psychosocial factors in a multivariate analysis for the determina-tion of return-to-sport status at 1 year postsurgery. This is an important step toward creating evidence to guide the development of rehabilitation programs and return-to-sport criteria to improve outcomes following ACL reconstruc-tion. There are several limitations of this study to consider when interpreting the results. This is a cross-sectional design; therefore, it remains to be proven if the
variables identified in this study will lon-gitudinally predict return-to-sport status at 1 year postsurgery. One year is gener-ally considered a short follow-up period after ACL reconstruction; however, it has been shown that, of those patients who return to sports, most do so within the first year.49 Furthermore, although most patients were released to return to sport at 6 months postsurgery, data on the tim-ing of return to sport for each individual patient were not collected or analyzed. Therefore, some patients might have had more or less time to be exposed to sport activities than others, which should be considered when interpreting the results.
The results of our study may not be applied universally to all patients follow-ing ACL reconstruction. Patient status as a coper or noncoper was not assessed, and it is plausible that different factors underlie functional recovery between these groups.17,24 Our exclusion criteria omitted those patients with concomitant ligamentous and articular cartilage dam-age requiring surgical procedures. Fur-thermore, patients who did not return for surgeon follow-up at 1 year postsurgery were not tested. This inherent selection bias should be considered when inter-preting these results.
A final limitation of our study is the use of a nonvalidated self-report mea-sure of return to sports participation. Most studies utilize self-report-of-func-tion questionnaires that measure knee performance across a wide spectrum of constructs,11,31,32,45,48,58 and comparisons are not often drawn between the abil-ity to return to preinjury levels of sports participation and the ability to return to sports, even at a reduced level.54 Objec-tive clinical comparison of preinjury to postsurgery levels of sports participation or performance also has its limitations due to variable measurements of profes-sional, amateur, and recreational athletic performance across sports. Although our methodology has not been validated, it has the potential to provide a more accu-rate estimation of sport-related function compared to preinjury levels.
Future studies should test the longitu-dinal validity of this model for prediction of return-to-sport status, as well as exam-ine other potentially important physical performance measures, impairment vari-ables, and psychological barriers related to return to sport. This study only exam-ined 1 psychosocial construct directly, and it is possible that other psychosocial factors may contribute more significantly to function in multivariate models.15,60 One such factor, self-efficacy, has been shown to be a preoperative predictor of outcome 1 year after ACL reconstruc-tion,53 and is predictive of improvements in knee pain intensity and self-reported function in the first 12 weeks following surgery.12 Future studies should examine the relationship of fear of movement/re-injury and other psychosocial constructs, such as self-efficacy, longitudinally and at follow-up times longer than 1 year to determine which constructs best predict return-to-sport status.
CONCLUSION
This study provides further in-sight into clinical variables that empirically discriminate between
individuals in return-to-sport groups. Results suggest that ongoing knee symp-toms following ACL reconstruction are associated with individuals returning to preinjury sports participation levels. These potentially modifiable factors rep-resent important targets for rehabilita-tion. Findings from this study should be considered in future longitudinal studies aimed at the development of return-to-sport rehabilitation guidelines and par-ticipation criteria. t
KEY POINTSFINDINGS: Patients reporting return to preinjury levels of sports participa-tion had less knee joint effusion, fewer episodes of knee instability, lower knee pain intensity, higher quadriceps peak torque-body weight ratio, higher IKDC scores, and lower TSK-11 scores. The strongest contributors to return-
42-11 Lentz.indd 899 10/17/2012 2:58:39 PM
Jour
nal o
f O
rtho
paed
ic &
Spo
rts
Phys
ical
The
rapy
®
Dow
nloa
ded
from
ww
w.jo
spt.o
rg a
t JO
SPT
on
Aug
ust 2
0, 2
014.
For
per
sona
l use
onl
y. N
o ot
her
uses
with
out p
erm
issi
on.
Cop
yrig
ht ©
201
2 Jo
urna
l of
Ort
hopa
edic
& S
port
s Ph
ysic
al T
hera
py®
. All
righ
ts r
eser
ved.

900 | november 2012 | volume 42 | number 11 | journal of orthopaedic & sports physical therapy
[ research report ]
REFERENCES
1. Aglietti P, Giron F, Buzzi R, Biddau F, Sasso F. Anterior cruciate ligament reconstruction: bone-patellar tendon-bone compared with double semitendinosus and gracilis tendon grafts. A prospective, randomized clinical trial. J Bone Joint Surg Am. 2004;86-A:2143-2155.
2. Ardern CL, Webster KE, Taylor NF, Feller JA. Return to the preinjury level of competitive sport after anterior cruciate ligament recon-struction surgery: two-thirds of patients have not returned by 12 months after surgery. Am J Sports Med. 2011;39:538-543. http://dx.doi.org/10.1177/0363546510384798
3. Ardern CL, Webster KE, Taylor NF, Feller JA. Return to sport following anterior cruciate ligament reconstruction surgery: a systematic review and meta-analysis of the state of play. Br J Sports Med. 2011;45:596-606. http://dx.doi.org/10.1136/bjsm.2010.076364
4. Barber-Westin SD, Noyes FR. Factors used to de-termine return to unrestricted sports activities after anterior cruciate ligament reconstruction. Arthroscopy. 2011;27:1697-1705. http://dx.doi.org/10.1016/j.arthro.2011.09.009
5. Biau DJ, Tournoux C, Katsahian S, Schranz P, Nizard R. ACL reconstruction: a meta-analysis of functional scores. Clin Orthop Relat Res. 2007:180-187. http://dx.doi.org/10.1097/BLO.0b013e31803dcd6b
6. Briggs KK, Lysholm J, Tegner Y, Rodkey WG, Kocher MS, Steadman JR. The reliability, valid-ity, and responsiveness of the Lysholm score
and Tegner activity scale for anterior cruciate ligament injuries of the knee: 25 years later. Am J Sports Med. 2009;37:890-897. http://dx.doi.org/10.1177/0363546508330143
7. Brosky JA, Jr., Nitz AJ, Malone TR, Caborn DN, Rayens MK. Intrarater reliability of selected clini-cal outcome measures following anterior cruci-ate ligament reconstruction. J Orthop Sports Phys Ther. 1999;29:39-48.
8. Brosseau L, Balmer S, Tousignant M, et al. Intra- and intertester reliability and criterion validity of the parallelogram and universal goniometers for measuring maximum active knee flexion and ex-tension of patients with knee restrictions. Arch Phys Med Rehabil. 2001;82:396-402. http://dx.doi.org/10.1053/apmr.2001.19250
9. Busfield BT, Kharrazi FD, Starkey C, Lombardo SJ, Seegmiller J. Performance outcomes of anterior cruciate ligament reconstruction in the National Basketball Association. Arthroscopy. 2009;25:825-830. http://dx.doi.org/10.1016/j.arthro.2009.02.021
10. Carey JL, Huffman GR, Parekh SG, Sennett BJ. Outcomes of anterior cruciate ligament injuries to running backs and wide receiv-ers in the National Football League. Am J Sports Med. 2006;34:1911-1917. http://dx.doi.org/10.1177/0363546506290186
11. Chmielewski TL, Jones D, Day T, Tillman SM, Lentz TA, George SZ. The association of pain and fear of movement/reinjury with function during anterior cruciate ligament reconstruc-tion rehabilitation. J Orthop Sports Phys Ther. 2008;38:746-753. http://dx.doi.org/10.2519/jospt.2008.2887
12. Chmielewski TL, Zeppieri G, Jr., Lentz TA, et al. Longitudinal changes in psychosocial factors and their association with knee pain and func-tion after anterior cruciate ligament reconstruc-tion. Phys Ther. 2011;91:1355-1366. http://dx.doi.org/10.2522/ptj.20100277
13. Clark JC, Rueff DE, Indelicato PA, Moser M. Primary ACL reconstruction using allograft tis-sue. Clin Sports Med. 2009;28:223-244. http://dx.doi.org/10.1016/j.csm.2008.10.005
14. Cleland JA, Childs JD, Whitman JM. Psycho-metric properties of the Neck Disability Index and Numeric Pain Rating Scale in patients with mechanical neck pain. Arch Phys Med Rehabil. 2008;89:69-74. http://dx.doi.org/10.1016/j.apmr.2007.08.126
15. da Menezes Costa L, Maher CG, McAuley JH, Hancock MJ, Smeets RJ. Self-efficacy is more important than fear of movement in mediating the relationship between pain and disability in chronic low back pain. Eur J Pain. 2011;15:213-219. http://dx.doi.org/10.1016/j.ejpain.2010.06.014
16. Ferrari JD, Bach BR, Jr., Bush-Joseph CA, Wang T, Bojchuk J. Anterior cruciate ligament reconstruction in men and women: an outcome analysis comparing gender. Arthroscopy. 2001;17:588-596.
17. Fitzgerald GK, Axe MJ, Snyder-Mackler L. Pro-
posed practice guidelines for nonoperative ante-rior cruciate ligament rehabilitation of physically active individuals. J Orthop Sports Phys Ther. 2000;30:194-203.
18. Freedman KB, D’Amato MJ, Nedeff DD, Kaz A, Bach BR, Jr. Arthroscopic anterior cruciate liga-ment reconstruction: a metaanalysis comparing patellar tendon and hamstring tendon auto-grafts. Am J Sports Med. 2003;31:2-11.
19. George SZ, Lentz TA, Zeppieri G, Lee D, Chmielewski TL. Analysis of shortened ver-sions of the Tampa Scale for Kinesiophobia and Pain Catastrophizing Scale for patients after anterior cruciate ligament reconstruction. Clin J Pain. 2012;28:73-80. http://dx.doi.org/10.1097/AJP.0b013e31822363f4
20. George SZ, Valencia C, Beneciuk JM. A psycho-metric investigation of fear-avoidance model measures in patients with chronic low back pain. J Orthop Sports Phys Ther. 2010;40:197-205. http://dx.doi.org/10.2519/jospt.2010.3298
21. Gobbi A, Francisco R. Factors affecting return to sports after anterior cruciate ligament reconstruction with patellar tendon and ham-string graft: a prospective clinical investiga-tion. Knee Surg Sports Traumatol Arthrosc. 2006;14:1021-1028. http://dx.doi.org/10.1007/s00167-006-0050-9
22. Greenberger HB, Paterno MV. Relationship of knee extensor strength and hopping test performance in the assessment of lower ex-tremity function. J Orthop Sports Phys Ther. 1995;22:202-206.
23. Griffin LY, Agel J, Albohm MJ, et al. Noncontact anterior cruciate ligament injuries: risk factors and prevention strategies. J Am Acad Orthop Surg. 2000;8:141-150.
24. Hartigan EH, Axe MJ, Snyder-Mackler L. Time line for noncopers to pass return-to-sports criteria after anterior cruciate ligament reconstruction. J Orthop Sports Phys Ther. 2010;40:141-154. http://dx.doi.org/10.2519/jospt.2010.3168
25. Hjermundrud V, Bjune TK, Risberg MA, Enge-bretsen L, Årøen A. Full-thickness cartilage lesion do not affect knee function in patients with ACL injury. Knee Surg Sports Traumatol Arthrosc. 2010;18:298-303. http://dx.doi.org/10.1007/s00167-009-0894-x
26. Irrgang JJ, Anderson AF, Boland AL, et al. Devel-opment and validation of the International Knee Documentation Committee Subjective Knee Form. Am J Sports Med. 2001;29:600-613.
27. Irrgang JJ, Anderson AF, Boland AL, et al. Responsiveness of the International Knee Docu-mentation Committee Subjective Knee Form. Am J Sports Med. 2006;34:1567-1573. http://dx.doi.org/10.1177/0363546506288855
28. Järvelä T, Kannus P, Järvinen M. Anterior cruci-ate ligament reconstruction in patients with or without accompanying injuries: a re-examina-tion of subjects 5 to 9 years after reconstruc-tion. Arthroscopy. 2001;17:818-825.
29. Kvist J. Rehabilitation following anterior cruci-
to-sport status allocation were self-reported knee function (IKDC score), frequency of knee instability, and knee joint effusion.IMPLICATIONS: Self-report and knee im-pairment variables differentiate those who are able to return to preinjury levels of sports participation from those who are not at 1 year postsurgery, possi-bly identifying targets to address during rehabilitation.CAUTION: This study included only pa-tients with primary ACL reconstruction, without concomitant ligamentous or articular cartilage damage requiring repair. Thus, the results of our study may not be applied universally to all patients following ACL reconstruction. The variables identified in this study should be tested in longitudinal stud-ies to determine their ability to predict sport-related outcomes.
42-11 Lentz.indd 900 10/17/2012 2:58:40 PM
Jour
nal o
f O
rtho
paed
ic &
Spo
rts
Phys
ical
The
rapy
®
Dow
nloa
ded
from
ww
w.jo
spt.o
rg a
t JO
SPT
on
Aug
ust 2
0, 2
014.
For
per
sona
l use
onl
y. N
o ot
her
uses
with
out p
erm
issi
on.
Cop
yrig
ht ©
201
2 Jo
urna
l of
Ort
hopa
edic
& S
port
s Ph
ysic
al T
hera
py®
. All
righ
ts r
eser
ved.

journal of orthopaedic & sports physical therapy | volume 42 | number 11 | november 2012 | 901
MORE INFORMATIONWWW.JOSPT.ORG@
ate ligament injury: current recommenda-tions for sports participation. Sports Med. 2004;34:269-280.
30. Kvist J, Ek A, Sporrstedt K, Good L. Fear of re-injury: a hindrance for returning to sports after anterior cruciate ligament reconstruc-tion. Knee Surg Sports Traumatol Arthrosc. 2005;13:393-397. http://dx.doi.org/10.1007/s00167-004-0591-8
31. Lee DY, Karim SA, Chang HC. Return to sports after anterior cruciate ligament reconstruction – a review of patients with minimum 5-year follow-up. Ann Acad Med Singapore. 2008;37:273-278.
32. Lentz TA, Tillman SM, Indelicato PA, Moser MW, George SZ, Chmielewski TL. Factors associated with function after anterior cruciate ligament reconstruction. Sports Health. 2009;1:47-53. http://dx.doi.org/10.1177/1941738108326700
33. Marx RG, Jones EC, Angel M, Wickiewicz TL, Warren RF. Beliefs and attitudes of members of the American Academy of Orthopaedic Surgeons regarding the treatment of ante-rior cruciate ligament injury. Arthroscopy. 2003;19:762-770.
34. Mintken PE, Glynn P, Cleland JA. Psychometric properties of the Shortened Disabilities of the Arm, Shoulder, and Hand Questionnaire (QuickDASH) and Numeric Pain Rating Scale in patients with shoulder pain. J Shoulder Elbow Surg. 2009;18:920-926. http://dx.doi.org/10.1016/j.jse.2008.12.015
35. Möller E, Weidenhielm L, Werner S. Outcome and knee-related quality of life after anterior cruciate ligament reconstruction: a long-term follow-up. Knee Surg Sports Traumatol Arthrosc. 2009;17:786-794. http://dx.doi.org/10.1007/s00167-009-0788-y
36. Myer GD, Paterno MV, Ford KR, Hewett TE. Neu-romuscular training techniques to target deficits before return to sport after anterior cruciate ligament reconstruction. J Strength Cond Res. 2008;22:987-1014. http://dx.doi.org/10.1519/JSC.0b013e31816a86cd
37. Myer GD, Paterno MV, Ford KR, Quatman CE, Hewett TE. Rehabilitation after anterior cruciate ligament reconstruction: criteria-based progres-sion through the return-to-sport phase. J Orthop Sports Phys Ther. 2006;36:385-402. http://dx.doi.org/10.2519/jospt.2006.2222
38. Nakayama Y, Shirai Y, Narita T, Mori A, Kobayas-hi K. Knee functions and a return to sports ac-tivity in competitive athletes following anterior cruciate ligament reconstruction. J Nihon Med Sch. 2000;67:172-176.
39. Ott SM, Ireland ML, Ballantyne BT, Willson JD, McClay Davis IS. Comparison of outcomes be-tween males and females after anterior cruciate ligament reconstruction. Knee Surg Sports Trau-matol Arthrosc. 2003;11:75-80. http://dx.doi.org/10.1007/s00167-003-0348-9
40. Pantano KJ, Irrgang JJ, Burdett R, Delitto A, Harner C, Fu FH. A pilot study on the relation-
ship between physical impairment and activity restriction in persons with anterior cruciate ligament reconstruction at long-term follow-up. Knee Surg Sports Traumatol Arthrosc. 2001;9:369-378. http://dx.doi.org/10.1007/s001670100239
41. Paterno MV, Rauh MJ, Schmitt LC, Ford KR, Hewett TE. Incidence of contralateral and ipsilat-eral anterior cruciate ligament (ACL) injury after primary ACL reconstruction and return to sport. Clin J Sport Med. 2012;22:116-121. http://dx.doi.org/10.1097/JSM.0b013e318246ef9e
42. Paterno MV, Schmitt LC, Ford KR, Rauh MJ, Myer GD, Hewett TE. Effects of sex on compensatory landing strategies upon return to sport after anterior cruciate ligament reconstruction. J Or-thop Sports Phys Ther. 2011;41:553-559. http://dx.doi.org/10.2519/jospt.2011.3591
43. Paterno MV, Schmitt LC, Ford KR, et al. Biome-chanical measures during landing and postural stability predict second anterior cruciate liga-ment injury after anterior cruciate ligament reconstruction and return to sport. Am J Sports Med. 2010;38:1968-1978. http://dx.doi.org/10.1177/0363546510376053
44. Rangger C, Daniel DM, Stone ML, Kaufman K. Diagnosis of an ACL disruption with KT-1000 arthrometer measurements. Knee Surg Sports Traumatol Arthrosc. 1993;1:60-66.
45. Risberg MA, Holm I, Tjomsland O, Ljunggren E, Ekeland A. Prospective study of changes in im-pairments and disabilities after anterior cruciate ligament reconstruction. J Orthop Sports Phys Ther. 1999;29:400-412.
46. Robnett NJ, Riddle DL, Kues JM. Intertester reliability of measurements obtained with the KT-1000 on patients with reconstructed anterior cruciate ligaments. J Orthop Sports Phys Ther. 1995;21:113-119.
47. Roos H, Ornell M, Gärdsell P, Lohmander LS, Lindstrand A. Soccer after anterior cruciate liga-ment injury—an incompatible combination? A national survey of incidence and risk factors and a 7-year follow-up of 310 players. Acta Orthop Scand. 1995;66:107-112.
48. Ross MD, Irrgang JJ, Denegar CR, McCloy CM, Unangst ET. The relationship between participa-tion restrictions and selected clinical measures following anterior cruciate ligament reconstruc-tion. Knee Surg Sports Traumatol Arthrosc. 2002;10:10-19. http://dx.doi.org/10.1007/s001670100238
49. Smith FW, Rosenlund EA, Aune AK, MacLean JA, Hillis SW. Subjective functional assess-ments and the return to competitive sport after anterior cruciate ligament reconstruction. Br J Sports Med. 2004;38:279-284.
50. Sturgill LP, Snyder-Mackler L, Manal TJ, Axe MJ. Interrater reliability of a clinical scale to assess knee joint effusion. J Orthop Sports Phys Ther. 2009;39:845-849. http://dx.doi.org/10.2519/jospt.2009.3143
51. Swirtun LR, Eriksson K, Renström P. Who choos-es anterior cruciate ligament reconstruction and why? A 2-year prospective study. Scand J Med Sci Sports. 2006;16:441-446. http://dx.doi.org/10.1111/j.1600-0838.2005.00505.x
52. Tegner Y, Lysholm J. Rating systems in the evalu-ation of knee ligament injuries. Clin Orthop Relat Res. 1985:43-49.
53. Thomeé P, Währborg P, Börjesson M, Thomeé R, Eriksson BI, Karlsson J. Self-efficacy of knee function as a pre-operative predictor of outcome 1 year after anterior cruciate ligament recon-struction. Knee Surg Sports Traumatol Arthrosc. 2008;16:118-127. http://dx.doi.org/10.1007/s00167-007-0433-6
54. Thomeé R, Kaplan Y, Kvist J, et al. Muscle strength and hop performance criteria prior to return to sports after ACL reconstruction. Knee Surg Sports Traumatol Arthrosc. 2011;19:1798-1805. http://dx.doi.org/10.1007/s00167-011-1669-8
55. Thomeé R, Neeter C, Gustavsson A, et al. Variability in leg muscle power and hop perfor-mance after anterior cruciate ligament recon-struction. Knee Surg Sports Traumatol Arthrosc. 2012;20:1143-1151. http://dx.doi.org/10.1007/s00167-012-1912-y
56. Thorstensson CA, Lohmander LS, Frobell RB, Roos EM, Gooberman-Hill R. Choosing surgery: patients’ preferences within a trial of treatments for anterior cruciate ligament injury. A qualitative study. BMC Musculo-skelet Disord. 2009;10:100. http://dx.doi.org/10.1186/1471-2474-10-100
57. Wiger P, Brandsson S, Kartus J, Eriksson BI, Karlsson J. A comparison of results after arthroscopic anterior cruciate ligament re-construction in female and male competitive athletes. A two- to five-year follow-up of 429 pa-tients. Scand J Med Sci Sports. 1999;9:290-295.
58. Wilk KE, Romaniello WT, Soscia SM, Arrigo CA, Andrews JR. The relationship between subjec-tive knee scores, isokinetic testing, and func-tional testing in the ACL-reconstructed knee. J Orthop Sports Phys Ther. 1994;20:60-73.
59. Woby SR, Roach NK, Urmston M, Watson PJ. Psychometric properties of the TSK-11: a shortened version of the Tampa Scale for Kine-siophobia. Pain. 2005;117:137-144. http://dx.doi.org/10.1016/j.pain.2005.05.029
60. Woby SR, Urmston M, Watson PJ. Self-efficacy mediates the relation between pain-related fear and outcome in chronic low back pain patients. Eur J Pain. 2007;11:711-718. http://dx.doi.org/10.1016/j.ejpain.2006.10.009
42-11 Lentz.indd 901 10/17/2012 2:58:41 PM
Jour
nal o
f O
rtho
paed
ic &
Spo
rts
Phys
ical
The
rapy
®
Dow
nloa
ded
from
ww
w.jo
spt.o
rg a
t JO
SPT
on
Aug
ust 2
0, 2
014.
For
per
sona
l use
onl
y. N
o ot
her
uses
with
out p
erm
issi
on.
Cop
yrig
ht ©
201
2 Jo
urna
l of
Ort
hopa
edic
& S
port
s Ph
ysic
al T
hera
py®
. All
righ
ts r
eser
ved.