Embed Size (px)
Citation preview

LETTER TO THE EDITOR
CURRENT ROLES OFADIPOFASCIAL ANTEROLATERALTHIGHFLAP IN HEAD AND NECK RECONSTRUCTIONS
To the Editor:It is with interest that we read the article pub-
lished by Wong and Wei, titled ‘‘Anterolateral ThighFlap,’’ in the May issue of Head and Neck.1 Thereport is focused on technical aspects regarding vas-cular and surgical anatomy and pitfalls of harvesting,giving an almost unique guide to flap rising. The an-terolateral thigh (ALT) flap can be classified in differ-ent clinical configurations equipped with well-definedindications based on the receiving site: fasciocutane-ous, myocutaneous, and cutaneous.2 The cutaneousvariant of this flap is harvested as thinned or ultra-thinned, depending on the defatting procedures, andits main advantage relies on the preservation of thedeep fascia, reducing the risk for muscle herniation.Because of the thinning procedures and the possibil-ity of harvesting a sensate flap (the lateral cutaneousfemoral nerve), the flap is ideal for reconstructingoral cavity defects. This flap can be harvested as aflow-through type 1 and type 2, making it feasible toreconstruct through-and-through defects of the man-dible. In 2003 V. Agostini and colleagues pioneeredthe concept of adipofascial anterolateral thigh (A-ALT) flap in oral cavity reconstruction: the firstreport describes a hemiglossectomy defect recon-structed with an adipofascial ALT flap.3 The A-ALTflap is harvested as a fasciocutaneous ‘‘leaf shape’’flap with 1- to 2-cm fascia around the pedicle to pre-serve the fascial plexus because the main blood sup-ply to the skin arises from the outer fascial layer,passing as fasciocutaneous or muscolocutaneous per-forators with branches perpendicularly oriented orradiated.4,5 The flap is thinned to fit the defect result-ing from tumor excision (extreme thinning should beavoided in anticipation of postoperative radiotherapy),and meticulous hemostasis is achieved before pediclesection. The main portion of the flap is reverse-sutured in the oral cavity at the level of the laminapropria of the native mucosa to obtain obstacle-freeadvancement of the neomucosa over the deep fascia.The vascular pedicle is tunneled into the neck wellprotected from saliva.4
The A-ALT flap represents a valid alternative tooral cavity reconstruction, supplying a functional,hairless tissue 45 days later, observing the principleof ‘‘replace tissue with like tissue’’ and avoiding the‘‘patch effect’’ of fasciocutaneous flaps.
The idea of reconstructing oral cavity defectsusing fascial flaps has been previously tested byothers who studied the remucosalization of the myo-fascial pectoralis major flap. The histologic resultsproved the flap was covered with a thin layer of squa-mous mucosa 1 month after surgery not influenced bypostoperative radiotherapy.6–8
Flap thinning has had a major impact in theWestern countries compared with Eastern countriesbecause of the higher incidence of obesity in the West.Alkureishi and colleagues experienced partial or totalnecrosis of the distal skin from the perforator ofthinned fasciocutaneous ALT flaps to oral cavityreconstructions, probably attributable to saliva inter-ference with the subdermal plexus.9,10
A-ALT advantages include volume preservationover time, thus maintaining the palatal contact andthe propulsive proprieties of a neo-tongue enhancingthe residual mobility and re-creation of the hyoidmandibular tension arch with improved stability ofthe larynx–hyoid bone complex. Because neomucosais a functional tissue, the lateral cutaneous femoralnerve dissection can be avoided. It does not precludemuscle harvesting (vastus lateralis/rectus medialis)in the mioadipofascial configuration for moredemanding reconstructions. Moreover, the A-ALTflap avoids prelamination with unjustified delayedtumor resection and double-paddle flaps to through-and-through defects of the cheek and the floor of themouth.
Twelve patients underwent reconstruction with
the A-ALT flap after squamous cell carcinoma resec-tion of the oral cavity between December 2005 and
August 2010 (Table 1). All patients underwent postop-erative radiotherapy with flap volume and functionmaintenance. To limit wound contraction and
impaired function, we always dissected more fasciacompared with soft tissue.
Thinning was uneventful, without partial or mar-ginal necrosis, and we did not experience fascial sloughthat required debridement. One patient presented ascarring bridle without functional loss after reconstruc-
tion of the entire mobile tongue, which did not requiresurgery, and patient 4 had an orocutaneous fistula withspontaneous healing. One flap failed as the result of ve-nous thrombosis, despite re-exploration. All underwentcomparative biopsies (colored with hematoxylin and eo-
sin stain) between the neomucosa and the native mu-cosa, showing a squamous epithelial lining and a mildinflammatory infiltrate charged to the lamina propria.Our results show the hot, cold, and touch sensitivities of
Head & Neck 33: 595–597, 2011Published online 7 March 2011 in Wiley Online Library(wileyonlinelibrary.com)DOI 10.1002/hed.21710VVC 2011 Wiley Periodicals, Inc.
Letter to the Editor HEAD & NECK—DOI 10.1002/hed April 2011 595

the neomucosa do not differ from those of the native.Small stromal nerve structures are detectable in biopsyspecimens using an immunohistochemical staining forS-100 protein.3,4 Both tissues were clinically unnotice-able, with excellent aesthetic outcome in tongue andfloor of mouth reconstructions.
Tommaso AgostiniVittorugo Agostini
Department of Plastic and ReconstructiveSurgery, CTO-AOUC
Florence, ItalyE-mail: [email protected]
Davide LazzeriPlastic and Reconstructive Surgery Unit
Hospital CisanelloPisa, Italy
REFERENCES
1. Wong C-H, Wei F-C. Anterolateral thigh flap. Head Neck2010;32:529–540.
2. Agostini T. Anterolateral thigh flap morbidity: considerationsand reflections on donor-site closure. Plast Reconstr Surg 2009;123:1133–1134.
3. Agostini V, Dini M, Mori A, Franchi A, Agostini T. Adipofascialanterolateral thigh free flap for tongue repair. Br J Plast Surg2003;56:614–618.
4. Agostini T, Agostini V. Further experience with adipofascial ALTflap for oral cavity reconstruction. J Plast Reconstr Aesthet Surg2008;61:1164–1169.
5. Agostini T, Agostini V. Adipofascial versus fasciocutaneous an-terolateral thigh flap in oral cavity reconstruction. Focus on thevascular supply. J Plast Reconstr Aesthet Surg 2009;62:e633–e634.
6. Moloy PJ. Reconstruction of intermediate sized mucosal defectswith the pectoralis major myofascial flap. J Otolaryngol 1989;18:32–35.
7. Johnson MA, Langdon JD. Is skin necessary for intraoral recon-struction with myocutaneous flaps? Br J Oral Maxillofac Surg1990;28:299–301.
8. Phillips JG, Postlethwaite K, Peckitt N. The pectoralis majormuscle flap without skin in intra-oral reconstruction. Br J OralMaxillofac Surg 1988;26:479–485.
9. Alkureishi LW, Shaw-Dunn J, Ross GL. Effects of thinning theanterolateral thigh flap on the blood supply to the skin. Br JPlast Surg 2003;56:401–408.
10. Ross GL, Dunn R, Kirkpatrick J, et al. To thin or not to thin:the use of the anterolateral thigh flap in the reconstruction of in-traoral defects. Br J Plast Surg 2003;56:409–413.
Reply:We thank Agostini and colleagues for their com-
ments on our paper. Certainly, the anterolateral thighflap harvested as an adipofascial flap has been success-ful in their hands, and I congratulate them for this. Ipersonally do not favor the adipofascial flap for defectsinvolving the oral cavity for the following reasons. First,skin with the dermis is very robust and allows secureplacement of sutures. This would ensure watertight clo-sure of the oral cavity, which is a crucial prerequisitefor reconstruction in this area. This is in stark contrastto the adipofascial tissue, which can be quite friable.Second, with regard to color match, mucosalization ofthe skin paddle occurs within 3 months, and this oftenbecomes quite indistinct from the surrounding oral mu-cosa (see Figure 1). Finally and most important, thevascularity of the fasciocutaneous flap resides primarily
in the dermis and the subdermal plexus. To discard themost vascular part of the flap, which we strive so hardto procure, seems counterintuitive. If debulking andthinning are required, I prefer to discard the less vascu-lar parts, ie, the subcutaneous fat portion of the flap.Numerous authors have noted this to be safe and effec-tive. With regard to the hair, which is an issue for intra-oral reconstruction, the proximal part of the thigh, withrelatively less hair, can be preferentially used based onthe A or B perforators as described by Yu.
That said, I would like to reiterate the main point ofthe report, which represents a significant advancementin the understanding of the vascular anatomy of the an-terolateral thigh flap. That is, the so-called variations ofthe anterolateral thigh flap can simply be classifiedinto: (1) the variation of the skin vessel supplying the
Table 1. Patients’ data.
Patient Age, y
Tumor
site
Tumor
classification (TNM)
Flap size,
cm
Fascia
lata, cm Complication
Diet
(1 wk postop)
Follow-up,
mo
1 50 MT T3N2M0 10 � 6 13 � 9 No Soft 112
2 75 MT T2N1M0 11 � 6 13 � 8 No Soft 71
3 60 RMT T3N2M0 10 � 5 13 � 7 No Liquid-soft 56
4 55 FOM T2N1M0 14 � 6 15 � 8 Orocutaneous fistula Soft 96
5 77 FOM T3N2M0 15 � 7 16 � 8 No Liquid-soft 52
6 63 PTC T3N2M0 10 � 6 13 � 6 Flap loss Soft 28
7 55 TL T3N2M0 10 � 6 13 � 8 No Soft 45
8 47 TL T2N1M0 10 � 7 13 � 9 No Liquid-soft 12
9 67 MT T3N2M0 10 � 7 13 � 9 Scarring bridle Liquid-soft 32
10 66 MT T3N1M0 10 � 6 12 � 8 No Soft 24
11 71 MT T2N2M0 8 � 5 11 � 7 No Soft 23
12 72 FTC T4N3M0 12 � 6 16 � 9 No Soft DOD
Abbreviations: MT, mobile tongue; RMT, retromolar trigone; FOM, floor of mouth; PTC, partial thickness cheek; TL, tonsillary lodge; FTC, full thickness cheek; DOD, died ofdisease.
596 Letter to the Editor HEAD & NECK—DOI 10.1002/hed April 2011

anterolateral thigh skin, which can be either myocuta-neous or septocutaneous, and (2) the pedicle of the flap.This can be either the descending or the oblique
branches of the lateral circumflex femoral artery (seeFigure 2). Once this aspect of the anatomy is appreci-ated, the flap can be safely harvested every time.
Chin-Ho Wong, MDDepartment of Plastic Reconstructive
and Aesthetic SurgerySingapore General Hospital
SingaporeE-mail: [email protected]: [email protected]
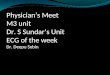
FIGURE 1. A hemiglossectomy defect reconstructed with a free
anterolateral thigh flap at 1 year postop. Mucosalization makes
the flap quite indistinct from the surrounding oral mucosa.
[Color figure can be viewed in the online issue, which is avail-
able at wileyonlinelibrary.com.]
FIGURE 2. The descending branch (above) and the oblique
branch (below) of the lateral circumflex femoral artery. Either
one can be safely used as the pedicle of the flap. [Color figure
can be viewed in the online issue, which is available at
wileyonlinelibrary.com.]
Letter to the Editor HEAD & NECK—DOI 10.1002/hed April 2011 597