-
Available online 21 August 2006
Abstract
the normal r iagnosis ofPV. Th R testfor the sitive.The use
http://france.elsevier.com/direct/PATBIO/
Pathologie Biologie 55 (2007) 92104
LectNovemb
* CorrE-ma
0369-81doi:10.1ere is a significant overlap of serum EPO levels
in PV versus control and controls versus SE. The specificity of a
JAK2 V617F PCdiagnosis of MPD is high (near 100%), but only half of
ET and MF (50%) and the majority of PV (up to 97%) are JAK2 V617F
po
of
ure Iner 18esponil ad
14/$016/jEEC assays were performed. The diagnostic impact of low
serum EPO levels (ELISA assay) in a large study of 186 patange
(< 3.3 IU/l) had a sensitivity specificity and positive
predictive value of 87%, 97% and 97.8%, respectively, for the dThe
clinical criteria for the diagnosis of essential thrombocythemia
(ET) according to the polycythemia vera study group (PVSG) do
notdistinguish between ET and thrombocythemia associated with early
stage PV and prefibrotic chronic idiopathic myelofibrosis (CIMF).
Theclinical criteria of the PVSG for the diagnosis of polycythemia
vera (PV) only detects advanced stage of PV with increased red cell
mass. Thebone marrow criteria of the World Health Organization
(WHO) are defined by pathologists to explicitly define the
pathological criteria for thediagnostic differentiation of ET, PV,
and prefibrotic and fibrotic CIMF. As the clinical PVSG and the
pathological WHO criteria show significantshortcomings, an updated
set of European Clinical and Pathological (ECP) criteria combined
with currently available biological and molecularmarkers are
proposed to much better distinct true ET from early PV mimicking
ET, to distinguish ET from thrombocythemia associated
withprefibrotic CIMF, and to define the various clinical and
pathological stages of PV and CIMF that has important therapeutic
and prognosticimplications. Comparing the finding of clustered
giant abnormal megakaryocytes in a representative bone marrow as a
diagnostic clue toMPD, the sensitivity for the diagnosis of MPD
associated with splanchnic vein thrombosis was 63% for increased
red cell mass, 52% for lowserum EPO level, 72% for EEC, and 74% for
splenomegaly indicating the superiority of bone marrow
histopathology to detect masked early andovert MPD in this setting.
The majority of PV and about half of the ET patients have
spontaneous EEC, low serum EPO levels and PRV-1 over-expression and
are JAK2 V617F positive. The positive predictive value for the
diagnosis of PV of spontaneous growth of endogenous
erythroidcolonies (EEC) of peripheral blood (PB) and bone marrow
(BM) cells is about 8085% when either PB or BM EEC assays, and up
to 94% whenBM and PB ients belowbiological markers
ternational Symposiu, 2005, Hopital Avicding author.dress:
postbus@good
- see front matter .patbio.2006.06.002Current diagnostic
criteria for the chronic myeloproliferativedisorders (MPD)
essential thrombocythemia (ET),
polycythemia vera (PV) and chronic idiopathic myelofibrosis
(CIMF)
Critres diagnostiques actuels des syndromes myloprolifratifs
(SMP),thrombocytmie essentielle (TE), polyglobulie de Vaquez
(PV)
et mylofibrose idiopathique (MFI)
J.J. Michielsa,d,*, Z. Bernemaa, D. Van Bockstaeleb, H. De
Raevec, W. Schroyensa
aDepartment of Hematology, University Hospital Antwerp
Wilrijkstraat 10, 2650 Edegem/Antwerp, BelgiumbDepartment of
Molecular Genetics, University Hospital Antwerp, Antwerp,
Belgium
cDepartment of Pathology University Hospital Antwerp, Antwerp,
BelgiumdGoodheart Institute, Hematology, Hemostasis and Thrombosis
Research Center,
Rotterdam, MPD Center Europe, Erasmus Tower, Veenmos 13, 3069 AT
Rotterdam, The Netherlandsincluding JAK2 V617 PCR test, serum EPO,
PRV-1, EEC, leukocyte alkaline phosphatase score and peripheral
m on The V616F JAK2 mutation: A major step forward in the
pathogenesis and management of myeloproliferative disorders,enne
and Paris 13 University.
heartcenter.demon.nl (J.J. Michiels).
2006 Elsevier Masson SAS. All rights reserved.
-
h sePDs
(Te peagne prellelini, lag
iati%)
ia
and the megakaryocytes. Not only is PV a chronic disorder
giedisorder in which erythrocytosis, leukocytosis and
thrombocy-tosis are all simultaneously present [1]. In PV, all
stops toblood production in the bone marrow seem to have been
pulledout. The marrow is crowded with great numbers of nucleatedred
cells and granulocytes in all stages of maturation withmarked
hyperplasia and clustering of enlarged mature mega-karyocytes. Some
cases however show only a moderate eleva-tion of erythrocytes with
an extreme degree of thrombocytosis,while in others the leukocyte
counts may be at or close to leu-kemic levels, with only slight
increase in red cells or platelets.As to the etiology of trilinear
myeloproliferation in PV, Dame-shek proposed two highly speculative
possibilities one, the pre-sence of excessive bone marrow
stimulation by an unknownfactor or factors and two, a lack or a
diminution in the normalinhibitory factor or factors [1]. This
original view and hypoth-esis of Dameshek is recently confirmed by
the discovery of theJAK2 V617F mutation by James, Ugo, Casadevall
and Vainch-enker in Paris, France [2] demonstrating that the V617F
muta-tion induces a loss of inhibitory activity of the JH2
pseudoki-nase part on the JH1 kinase part of JAK2 leading to
enhancedactivity of the normal JH1 kinase activity of JAK2,
whichmakes the mutated hematopoietic stem cells hypersensitive
to
stages in the natural history of PV (Fig. 1) [3,4]:
stage 1). Pure erythrocythemia is featured by
increasedhemoglobin, hematocrit and red cell mass with normal
leu-kocytes, thrombocytes and spleen size, which is labeled
asidiopathic erythrocytosis by Pearson and Whetherley-Mein[5] and
Najean et al. [6]. This category of early PV maycomprise about
2030% of the cases at time of presentation;
stage 2). The polycythemic stage of PV is featured
bythrombocythemia, erythrocythemia and no or slight
myeloidmetaplasia, leukocytosis and/or splenomegaly (Fig. 1);
stage 3). Myeloid metaplasia in PV patients presents withno or
different grades of reticulin and collagen fibrosis inthe bone
marrow and progressive splenomegaly duringlong-term follow in about
one third of the cases;
stage 4). The polycythemic stage with various degrees
mye-lofibrosis and splenomegaly following PV may elapse 525 years
before a period of normal red cell values so-called spontaneous
remission of PV occurs. This stagemust be considered as the
beginning of spent phase PVand may last a few to several years. At
this point the spleenis frequently large and very firm to
palpation, the liver isenlarged to a moderately degree in most
patients, thrombo-without any evidence of invasiveness but it is a
total marrowblood parameters combined with bone marrow
histopathology has a higstages of ET, PV and CIMF in JAK2 V617F
positive and negative M 2006 Elsevier Masson SAS. All rights
reserved.
Rsum
Les critres cliniques de diagnostic de la thrombocytmie
essentielleformes dbutantes avec thrombocytose de PV et de MFI. Ces
critres nune claire augmentation du volume globulaire. Les critres
OMS de dipar les pathologistes pour clairement diffrencier TE, PV,
MFI au staddiagnostiques utilisant les marqueurs biologiques et
molculaires actudbutantes de PV et de MFI mimant les TE, et de
dfinir les stades cconsquences pronostiques et thrapeutiques. Sont
notamment discutsdu dosage drythropotine, de lexistence de colonies
rythrodes ou mla mutation V617F de JAK2. Lutilisation de ces
marqueurs en assocdiagnostiquer avec une haute sensibilit et
spcificit (proches de 100V617F JAK2 positifs ou ngatifs. 2006
Elsevier Masson SAS. All rights reserved.
Keywords: Myeloproliferative disorders; Essential
thrombocythemia; Polycythemcolony assay; JAK2 V617F mutation; Bone
marrow pathology
Mots cls : Thrombocytmie ; Polyglobulie ; JAK2 ; Biopsie
mdulllaire
1. Introduction
In 1950, William Dameshek presented an original view onthe
physiopathology and course of polycythemia vera (PV) [1].He
described PV as a chronic disorder of the bone marrowcharacterized
by excessive production of blood cells by themarrow elements i.e.
the nucleated red cells the granulocytes
J.J. Michiels et al. / Patholohematopoietic growth factors TPO
EPO, IGF1, SCF and GCSFresulting in trilinear
myeloproliferation.nsitivity and specificity (almost 100%) to
diagnose the early and overt.
E) dvelopps par le PVSG ne permettent pas de distinguer les TE
desrmettent par ailleurs que le diagnostic de formes patentes de
PV, avecostic des SMP incluent la biopsie mdullaire, avec des
critres dfinisfibrotique ou fibrotique. Nous proposons une mise
jour des critresment disponibles, dans le but de distinguer des TE
pures les formesques et anatomopathologiques de PV et MFI, ce qui a
dimportantesvaleur des donnes morphologiques sur la biopsie de
moelle osseuse,acaryocytaires spontanes, de lhyperexpression du gne
PRV-1, et deon avec les donnes morphologiques de la moelle osseuse
permet deles stades patents mais aussi prcoces de TE, PV et MFI,
quils soient
vera; Myeloid metaplasia; Myelofibrosis; Erythropoietin;
Endogenous erythroid
2. The concept of PV as a trilinear MPD
Wasserman proposed in 1954 a hypothetical concept for thecourse
of PV[3,4]. Accordingly PV is characterized by
initialerythrocytosis (erythrocythemia), which is usually
accompa-nied by leukocytosis of normal mature granulocytes
(leuko-cythemia) with increased leukocyte alkaline
phosphatasescore, by thrombocytosis (thrombocythemia),
splenomegaly,and plethora. Wasserman distinguished at least five
subsequent
Biologie 55 (2007) 92104 93cythemia is frequent and may be
pronounced with bizarreand giant platelets, and white cells are
usually increased
-
Based on extended clinical experience and review of
theliterature, Glaser and Walker [7] concluded that the
transitionof PV to myelofibrotic myeloid metaplasia occurs, but
whetherpost-PV is the same or distinct from agnogenic myeloid
meta-plasia (AMM) or chronic idiopathic myelofibrosis (CIMF)
stillremains an open question and has never been solved in a
pro-spective clinicopathological study, which nowadays
becomespossible by the use of new molecular and biological
markersincluding PRV-1 expression and JAK2 V617F mutation [2].
3. Clinical, laboratory and pathological featuresof the MPDs
J.J. Michiels et al. / Pathologie Biologie 55 (2007) 9210494with
granulocytic leukocytosis (leukocythemia) accompa-nied by a small
percentage of immature forms;
stage 5). Post-PV myeloid metaplasia shows various degreesof
leuko-erythroblastosis of the peripheral blood and mayprogress to
extreme myelofibrosis with a dry tap on aspira-tion and massive
splenomegaly (Fig. 1). At this end-stagehistopathology of bone
marrow biopsy shows a similar pic-ture and can not been
differentiated from agnogenic myeloidmetaplasia with no previous
history of PV [1,2].
Fig. 1. The evolution and dynamics of the disease process in
polycythemia vera(PV) according to the concept Wasserman, who
defined PV as a trilinearmyeloproliferative disorder with various
degrees of erythrocythemia, thrombo-cythemia, leukocythemia and
prefibrotic myeloid metaplasia as initial stagesfollowed by spent
phase PV and dry tap myelofibrosis after long-term follow-up in
about one third of the cases [3,4].
Table 1The World Health Organization (WHO) [24] and the European
Clinical and Patholthrombocythemia: ET
Clinical criteria Pathological critePersistent increase of
platelet count WHO and ECP
Increase of dispehyperlobulated nreticulin
A typical ET pict
ECP: > 400 109/lWHO: > 600 109/lECP
Presence of large or giant platelets in peripheral blood
smear
ECP
Absence of any underlying disorder for reactive
thrombocytosis
ECP
No proliferation oWHO and ECP
No peripheral blood, bone marrow and cytogenetic evidence ofPV,
CML, CIMF, MDS or reactive thrombocytosis
ECP
Absence of any cytogenetic abnormality
Molecular biolog
Clonality studies:
Acquired: JAK2
Congenital: polyTPO, cMPL geneIn the 1980s and 1990s the German
pathologists Burkhardtet a1 [8], Georgii et al. [912] and Thiele et
al. [1318] havedescribed typical histopathological features from
bone marrowbiopsy material for the diagnosis and classification of
each ofthe 3 different Ph-negative MPDs essential
thrombocythemia(ET), PV and AMM. Georgii et al. [9,10] and Thiele
et al.[13,14] drew attention to an authentic chronic
megakaryocyticgranulocytic myeloproliferation (CMGM) as a separate
patho-logical entity among the MPD, distinct from ET and
distinctfrom chronic myeloid leukemia (CML) or
myelodysplasticsyndrome (MDS). This condition has been described in
1996as Philadelphia-chromosome negative chronic
megakaryocyticgranulocytic myeloproliferation (CMGM) by Georgii et
al. [11,12] and as prefibrotic CIMF by Thiele et al. [18]. Since
theearly 1980s Michiels and Juvonen [1921] combined clinicaland
pathological features by including bone marrow histo-pathology as a
pathognomonic, diagnostic clue to each of theMPDs. In 1997, the
thrombocythemia vera study Group(TVSG) extended the clinical
criteria of the polycythemiavera study Group (PVSG) for the
diagnoses of ET and PV byincluding bone marrow histopathology as a
diagnostic clue andspecific feature of ET, PV (Tables 1 and 5A)
[21]. Thiele et al.[22,23] improved the TVSG criteria for ET, PV
and added theCologne criteria for prefibrotic, early fibrotic and
overt fibroticstages of CIMF (Table 2). These clinical and
pathological cri-teria were diagnostic for MPD [2023] and inspired
the WorldHealth Organization (WHO) [24] to clearly define the
patholo-gical bone marrow criteria for the differentiation between
true
ogical (ECP) [25] criteria for the diagnosis of acquired or
congenital essential
ria
rsed or loosely clustered, predominantly enlarged mature
megakaryocytes withuclei and mature cytoplasm, normal cellularity,
no or borderline increase of
ure excludes PV, AMM, CML, MDS, and reactive thrombocytosis
r immaturity of granulo- or erythropoiesisy: ECP
polyclonal or monoclonal
V617F positive or negativeclonal and JAK2 V617F negative ,
caused by gain of function mutation ofs or of unknown etiology
-
al and Pathological (ECP) [25] Criteria for the diagnosis of
prefibrotic and early
criteria, WHO, ECPakaryocytic and granulocytic
myeloproliferation (CMGM) [912,20] and no ortion of erythroid
precursors. Abnormal clustering and increase in atypical giant
tomegakaryocytes containing bulbous (cloud-like) hypolobulated
nuclei and
turation defects
sensus on grading of myelofibrosis (MF) [80]rotic CIMF: focal
fine reticulin with no intersections (cross-over) and only rarein
fibersfibroas,is
olog
pos
toge
gie Biologie 55 (2007) 92104 95ET, classical PV, and prefibrotic
and fibrotic stages of CIMF.The WHO criteria are essentially drawn
by internationalexperts in bone marrow morphology but not
clinicians. Toovercome the shortcomings of the clinical PVSG and
thepathological WHO [24] criteria, Michiels and Thiele [25,26]have
defined a set of European Clinical and Pathological(ECP) criteria,
which by including the available biologicaland molecular markers
(Tables 1, 2, 5B, 7, 8) will much betterallow to diagnose and
classify each of early and overt stages ofthe MPDs ET, PV and CIMF
[25,26].
4. WHO pathological criteria for the diagnosis of ET, PVand
CIMF
A typical bone marrow picture according to the WHO [24]for true
ET affects mainly of megakaryocytic cell lineage,shows increased
numbers of loosely clustered enlarged, maturemegakaryocytes with
hyperploid staghorn-like nuclei togetherwith normal cellularity,
normal erythropioesis, and normalgranulopoiesis, no increase of
reticulin fibrosis, and there is
Table 2The World Health Organization (WHO) [24] and the updated
European Clinicfibrotic agnogenic myloid metaplasia (AMM)
Clinical criteria, ECP PathologicalNo preceding or allied other
subtype of myeloproliferativedisorders CML or MDS.Main presenting
feature of prefibroticCIMF is thrombocythemia and slight
splenomegaly, no dry tapon bone marrow aspiration and diagnosed as
ET according tothe PVSG.
Chronic megrelative reducmedium sizeddefinitive ma
Clinical and laboratory features European conNormal hemoglobin
or slight anemia, grade I: hemoglobin > 12g/dl
MF 0: Prefibcourse reticul
Slight or moderate splenomegaly on ultrasound scan or CT MF 1:
Earlyperipheral are
Thrombocytosis, platelets in excess of 400, 600 or even1000
109/l
Note that MF
No leuko-erythroblastosis
No tear drop erythrocytes
Molecular bi
JAK2 V617F
Screen for cy
J.J. Michiels et al. / Patholono peripheral blood, bone marrow
and cytogenetic evidenceof typical and atypical chronic myeloid
leukemias (CML),PV, myelodysplastic syndrome (MDS) or reactive
thrombocy-tosis (Table 1) [2026]. A typical bone marrow picture for
trueET excludes any other MPD, as well as typical and atypicalCML,
MDS and reactive thrombocytosis.
A typical bone marrow picture according to the WHO [24]for a
prefibrotic form of CIMF is characterized by a
prominentgranulocytic and megakaryocytic myeloproliferation
(CMGM)[11,12,20] and no or borderline increase in reticulin
(CIMF-0,Table 2). The prevalence of the (left-shifted) neutrophil
andmegakaryocytic lineage is associated with reduction
andmaturation arrest of erythroid precursors. Most
conspicuous,however is the fact that the megakaryopoiesis is
characterizednot only by a disturbance of bone marrow
histotopography(loose to dense clustering and translocation to the
endostealborders), but also by striking abnormalities of
maturation.The immature megakaryocytes in prefibrotic CIMF consist
ofvariations in size including giant forms and deviations of
thenuclear-cytoplasmic ratio accompanied by bulbous and
hyper-chromic cloud-like nuclei, which are never seen in ET and
PV.Thiele et al. [18,2736] demonstrated that prefibrotic and
earlyfibrotic CIMF usually presents with thrombocythemia (falseET),
which has to be distinguished from true ET because clin-ical
features, natural history and prognosis significantly differ(Table
2). The prefibrotic stage of CIMF is not only associatedwith
pronounced thrombocythemia, but also show no leuko-erythroblastic
blood picture, normal or increased LAF-scoreand no or minimal
splenomegaly (Table 2) [18,2736], andtherefore diagnosed as ET
according to the PVSG [37,38] cri-teria (Tables 14).
A typical picture in the bone marrow according to the WHO[24]
pathognomonic and diagnostic for PV is featured byincrease of
clustered enlarged mature megakaryocytes compar-able to ET, and a
moderate to marked increased cellularity,erythropoiesis and
granulopoiesis (i.e. panmyelosis) (Table 5A,5B) [2026]. Bone marrow
features in polycythemic stage ofPV show a hypercellular bone
marrow of prominent erythroid
tic CIMF: loose network of reticulin with intersections,
especially inno collagenizationnot a disease but secondary to
AMM
y:
itive or negative
netic abnormalitiesprecursor cells and neutrophil granulopoiesis
in addition tomegakaryocytes proliferation with loose arrangements
of clus-tered megakaryocytes. Megakaryocytes do not only show
dif-ferent sizes, but fail to exhibit significant maturation
defects.The megakaryocytes in PV usually have a rather
pleiomorphicappearance with wide ranges of sizes including small
and giantforms. A typical PV picture of the bone marrow is seen
in
Table 3PVSG [38] criteria for the diagnosis of ET
Platelet count > 600 x 109/l: 1986 No known cause of Reactive
Thrombocytosis Normal hemoglobin and red cell mass to exclude overt
PV Stainable iron bone marrow to exclude PV No features of MDS in
bone marrow smear and biopsy Absence of Ph1+ chromosome (brc/abl)
to exclude CML Collagen fibrosis of bone marrow is allowedup to
-
onoc
one
sedB
B
gieTable 4ET according to PVSG [38] compared to WHO [24] and ECP
[25] criteria
ET PVSG Hereditary ET True ETIncludes Incidence < 0.001
2030Serum EPO Normal Normal
Platelet / > 400 ECP> 600 WHO
Erythrocytes N NHematocrit N NBone marrow: ET picture ET
pictureMegakaryocytes Normal large / giant and matureSplenomegaly
JAK2 V617F Neg: EEC Neg: PVR-1 Not applicable Clonality polyclonal
polyclonal m
Table 5AExtension of the PVSG [39] criteria of polycythemia vera
(PV) by including b
The Rotterdam Criteria of Polycytemia Vera PropoA1 Raised red
cell mass
males > 36mL/KgA2 Absence of any cause of secondary
erythrocytosis by clinical and
laboratory investigations
J.J. Michiels et al. / Patholo96classical PV according to the
PVSG [39], in erythrocythemiaor idiopathic erythrocytosis, in early
or latent PV and inmasked PV (Fig. 2 and Tables 6 and 7)
[25,26,4044]. In con-genital polycythemia (CP) and secondary
erythrocytosis (SE),in which increased erythropoiesis is present,
the number, size,morphology and distribution of megakaryocytes in
bone mar-row smears and biopsies remain normal [2023,40,41].
5. Current clinical and pathological criteriafor the diagnoses
of ET PV and CIMF
Since 1975 the minimum criterion of the Polycythemia VeraStudy
Group (PVSG) for the diagnosis of ET was 1000 109/l(1 million)
[37]. In 1985, we demonstrated that the majority ofsymptomatic ET
patients diagnosed by increase and clusteringof enlarged
megakaryocytes in bone marrow biopsies, had pla-telet counts
between 400 and 1000 109/l (below 1 million).This prompted the PVSG
to lower the platelet count for thediagnosis of ET to the arbitrary
minimum of 600 (Table 3)[38]. We could consistently demonstrate
that the arbitraryminimum of 600 109/l platelets according to the
PVSG andWHO overlooks early stage MPD at platelets between 400
and600 with no or slight splenomegaly, with no or low serumEPO, and
typical MPD features in the bone marrow consistent
A3 Histopathologie of bone marrow biopsy increase of: Ba.
cellularity, panmyelosisb. enlarged megakaryocytes with hyperploid
nuclei;c. reticulin fibers (optional)
BA1 + A2 + A3 is consistent with early stage PV (so-called
"idiopathic erythrocytosA1 + A2+ A3 + any one from category B
establishes overt PVA3 + B1 is consistent with essential
thrombocythemiaA3 + B3 and/or B4 is consitent with a primary
myeloproliferative disorderEarlyl PV Prefibrotic CIMFMimicking ET
False ET2030 4060Decreased Normal
> 400 ECP > 400 ECP> 600 ECP > 600 WHON/ N/N/ N/PV
picture MMM picture
abnormal ++ ++ ++
lonal Monoclonal Monoclonal
marrow histopathology as a diagnostic clue to early and overt
stages PV [21]
by the thrombocithemia Vera Study group (TVSG)1
Thrombocytosis
Platelet count > 400 109/L2 Granulocytes > 10 109/L and/or
raised neutrophil alkaline
phosphatase score of > 100 in the absence of fever or
infection
Biologie 55 (2007) 92104with early ET (Table 1), early PV
mimicking ET (Tables 4,5A, 5B and 6) or prefibrotic CIMF or
unclassifiable MPD(Tables 1 and 3).
The PVSG criteria for ET [38] is a diagnosis of exclusion
ofreactive thrombocytosis, PV, MDS and Ph1+ CML but includesby
definition thrombocythemia associated with prefibrotic andearly
fibrotic CIMF (Table 3) [1723]. The WHO [24] and theECP [25]
criteria for the diagnoses of ET extend the PVSG[34] criteria by
including histopathology from bone marrowbiopsies as a positive
criterion of MPD and as powerful toolto differentiate between true
ET, false ET and early PVmimicking ET (Table 4). Comparing the WHO
and ECP withthe PVSG criteria for the diagnosis of ET show that the
PVSGcriteria fail to distinguish ET from early PV mimicking
ET[4044] and fail to distinguish ET from usually
pronouncedthrombocythemia associated with prefibrotic CIMF (Tables
4)[2325,3336]. In consideration of disease-related complica-tions
occurring at low platelet counts, the arbitrarily chosenlimit for
platelet count (> 600 10/l) by the PVSG (Table 3)[38] and WHO
(Table 1) [24] has been reduced to 400 109/lin the ECP [25] (Table
1) criteria for ET. The PVSG [38] cri-teria for ET, when compared
to the WHO [24] and ECP [25]criteria, also include early PV
mimicking ET (Tables 4 and 6)[4044].
3 Splenomegaly on palpation or isotope/ultrasound scan
4 Erythroid colony formation in absence of EPO: spontaneous
EECis")
-
RCMean
dl in
gieTable 5BDiagnosis of PV according to the PVSG, WHO and ECP
criteria
PVSG [39] WHO [24]Criteria Major criteria Major criteriaA1 Red
cell mass: RCM Red cell mass:Overt
PV
Male > 36 ml/kg
Female > 32 ml/kg
> 25% above m
normal valueor Hb > 18.5 g/
J.J. Michiels et al. / PatholoThe PVSG have used increased red
cell mass proposed byDameshek in 1950 [1] as the main inclusion
criterion for diag-nosis of PV in the PVSG 01 study since 1969 [4],
whichbecame a main diagnostic criterion for the diagnosis of
PVsince 1975 (Tables 5A, 5B) [39]. Increased red cell mass isnot
specific, because it includes patients with PV,
congenitalpolycythemias (CP), and secondary erythrocytosis
(SE),thereby introducing a main differential diagnostic problemand
the need of extensive laboratory investigations [45,46].
women
Latent PV
A2 Normal arterial oxygen saturation > 92% Absence
secondaryA3 Splenomegaly on palpation Splenomegaly on pA4 Clonal
evidence othA5 Spontaneous EECCriteria Minor criteria Minor
criteriaB1 Platelets > 400 Platelets > 400B2 Leukocytes >
12 Leukocytes > 12B3 Bone marrow biopsy has been disregarded
by
the PVSG and included by the TVSG as adiagnostic clue for early
and overt PV [21]
Bone marrow biops
Increased cellularityferation and clustermorphic) megakary
B4 Raised LAP score Low serum EPODiagnosis DiagnosisA1 + A2 +
A3
A1 + A2 + two from B
A1 + A2 + any othe
A1 + A2 + two fromManifest PV:
Increased RCM
Manifest PV:
Increased RCM
Table 6Clinical staging of Polycythemia Vera: therapeutic
implications
Polycythemia Vera EvolutionStaging of PV as one
distinctdisease
ECP 1 Aspirin/phlebotomy ECP 2 Aspirin/ph
initial PV mimicking ET ErythrocythemicIncidence (%) 2025
2025Hemoglobin g/dl N/ Serum EPO
Hematocrit Male 0.43- < 0.51 Male > 0.51Female 0.42- <
0.48 Female > 0.48
Red cell mass N Thrombocytes (x 109/l) >400600 <
400Leukocytes (x 109/l) N NSpleen on echogram N15 cm NBone marrow:
PV picture PV pictureJAK2 V617F + +EEC + +PRV-1 LAF score
Myelofibrosis (MF) 0 0ECP [25]Clinical criteria
Red cell mass optional> 25% above mean normal value
men, Hb > 16.5 g/dl in or Hb > 18.5 g/dl in men
Biologie 55 (2007) 92104 97The PVSG [39] postulated three major
and four minor criteria(Table 5B) to ensure that patients who
entered the PVSG pro-spective trial indeed were suffering from PV
and not from con-genital polycythemia or secondary erythrocytosis
[39].Increased red cell mass corresponded with high
hematocritvalues between 0.50 and 0.75 [39] (ECP stage 3 and 4
Table 6),which according to the PVSG 01 study [39] was
associatedincreased platelet count in two third and with major
thrombosisin one third of more than 400 PV patients at time of
diagnosis
Hb > 16.5 g/dl in womenRed cell mass normaland Ht < 0.51
in men
Ht < 0.48 in femaleerythrocytosis Absence of secondary
erythrocytosisalpation Splenomegaly on CT or ultrasound (> 12
cm)er than Ph1+ or BCR/ABL Clonal evidence other than Ph1+ or
BCR/ABL
Spontaneous EECClinical criteriaPlatelets > 400
109/lLeukocytes >12 109/l
y with typical PV picture
with trilineage myeloproli-ing of small to giant
(pleio-ocytes
Bone marrow biopsy with typical PV picture
Increased cellularity with trilineage myeloproli-feration and
clustering of small to giant (pleio-morphic) megakaryocytesLow
serum EPODiagnosis
r from A
B
B3 plus any other of the clinical criteria
Manifest PV:
Increased RCM
Early stage PV:
RCM Normal
Manifestationlebototm ECP 3 PVSG WHO A/P ECP4 PVSG WHO
IFN/HU
PV Thrombo/erythro/leukocythemic PV4060
> 400 > 1,000N > 15N15 cm > 15 cmPV picture PV MF
picture+/++ ++/LOH+ + 0/1 1/2
-
[4,39]. The thrombocythemia vera study group (TVSG,Table 5A)
[21] extended the PVSG criteria by including bonemarrow
histopathology, which prompted pathologists to definethe WHO [24]
and clinicians to define ECP [25] criteria for thediagnosis of
early or masked PV and overt and advancedstages of PV (Tables 4 and
6).
According to the TVSG [21] criteria in Table 5A a typicalPV
picture of the bone marrow is seen in 4 different categoriesof MPD
patients.
First, the combination of a typical PV picture, increased
redcell mass, high hematocrit and one of the B criteria (Table
5A)is consistent with classical PV according the PVSG [39] andWHO
[24] and as advanced stage 3 and 4 PV when applyingthe ECP [25]
criteria (Table 6).
J.J. Michiels et al. / Pathologie98Second, a typical PV picture
of the bone and increased redcell mass, high hematocrit but with
normal platelet count andspleen size is consistent with
erythrocythemia according toWasserman [3] (Fig. 1), diagnosed as
idiopathic erythrocytosisby the PVSG criteria [5,6], and diagnosed
as erythrocythemicPV according to WHO [24] and stage 2 ECP [25]
when com-bined with serum EPO levels and EEC (Tables 5B and 6).
Incontrast to the PVSG [39] criteria, both the WHO [24] andECP [25]
criteria clearly differentiates between PV, CP andSE without the
need of red cell measurement in PV, and witha clear indication for
red cell mass measurement in CP and SE[21,25,26].
Third, a typical PV picture of the bone marrow with ahematocrit
in the upper limit of normal but with increased pla-telet count is
consistent with ET according to PVSG [39] andWHO [24] but diagnosed
as early stage 1 PV mimicking ETaccording to the ECP [25] criteria
(clinical case 2, Fig. 2 andTables 4, 5A, 5B and 6) [25]. Early
stage 1 PV usually pre-sents with microvascular disturbances at
platelet count inexcess of 400 109l, increased LAF score, low serum
EPO,spontaneous EEC and no or slight splenomegaly (Tables 4and 6)
[26].
Fourth, the combination of a typical PV picture, normal redcell
mass, normal hemoglobin and hematocrit, normal plateletbut slowly
progressive splenomegaly, granulocytosis or even
Fig. 2. The evolution and dynamics of the disease process in
polycythemia vera(PV) according to Thiele et al. [4044] indicating
the sequential occurrence of
the early initial stage of PV mimicking ET, the overt
polycythemic stage ofclassical PV, and progression to post-PV
myeloid metaplasia or leukemia asterminal stages in about one third
of the cases.slight anemia is not consistent with either ET, PV but
withunclassifiable MPD or masked PV [21]. Such cases of
unclas-sifiable MPD and masked PV are overlooked by clinicians
andmay comprises about one quarter of patients with a typical
PVpicture of the bone marrow. Such cases may present withthrombotic
complications including splanchnic vein thrombosis[47,48], are
described as masked PV [48,49], and frequentlyshow spontaneous EEC
as the clue to the atypical presentationof MPD. Masked ET or PV may
progress to so-called classi-cal CIMF without overt PV.
Using clusters of pleiomorphic giant megakaryocytes inbone
marrow biopsy as a reference standard for the diagnosisMPD, a
French study demonstrated that 46 out of 128 conse-cutive patients
with splanchnic (hepatic, portal or mesenteric)vein thrombosis had
features of MPD [48]. These 46 MPDpatients with splanchnic vein
thrombosis had hepatic veinthrombosis (Budd Chiari syndrome) in 19
and portal or mesen-teric vein thrombosis in 27 [48]. As compared
to a positivebone marrow finding of clustered giant megakaryocytes
diag-nostic for MPD, the sensitivity for the diagnosis of MPD
asso-ciated with splanchnic vein thrombosis was 63% for
increasedred cell mass, 52% for low serum EPO level, 72% for
EEC,and 74% for splenomegaly indicating the superiority of
bonemarrow histopathology to detect masked early and overt stagesof
MPD in this setting [48].
Thiele et al. [4044] confirmed the sequential occurrence ofearly
PV mimicking ET, overt and advanced stages of PV(Fig. 2 and Table
6). The WHO [24] and ECP [25] criteriaclearly differentiate PV from
CP, SP, and ET from reactivethrombocytosis, initial PV and
prefibrotic CIMF. The PVSG[39] and the WHO [24] criteria used
increased red cell as amandatory main criterion (Table 5B), which
is a very crudeand therefore overlook by definition early PV
mimicking trueET (ECP stage 1 in Table 6) and the erythrocythemic
phase(ECP stage 2 in Table 6) of PV, formerly labeled as
idiopathicerythrocytosis [5,6]. Accumulating data from the
literatureshow that spontaneous endogenous erythroid colony
formation(EEC) [5153], low serum EPO [5460] and PRV-1 expres-sion
[6164] are the hall mark of PV. About 50% of ETpatients according
to the PVSG are EEC positive [51,6569],PRV-1 positive [6164], and
may be associated with lowserum EPO [50,5759] indicating early PV
mimicking ET(Tables 6 and 7). The reports on EEC/PRV-1 positive ET
diag-nosed according to the PVSG [39] may have with low serumEPO
and therefore represent early ECP stage 1 of PV (Tables 6and 7).
The cohorts of early ECP stage 1 and 2 PV and theovert ECP stage 3
PV patients are featured by spontaneousEEC, positive PRV-1, low
serum EPO levels and a typicalPV bone marrow picture (Fig. 2 and
Tables 6 and 7) [5466].Both the early (ECP stage 1 and 2) and overt
(ECP stage 3) PVpatients are at high-risk for potential minor and
major vascularcomplications, because they present with elevated
plateletcount mimicking true ET [65,66]. EEC/PRV-1 positive
ETpatients according to PVSG criteria have a high risk of
devel-
Biologie 55 (2007) 92104oping microvascular and major thrombotic
complication ascompared to EEC/PRV-1 negative ET [65,66].
PRV-1-negative
-
sis o
Pl P
f
P
A
N
P
P
P
P
P
D
C
P
Ps
gieET comprises a pathophysiologically distinct subgroup of
trueET patients with no features of early PV, who are at lower
riskfor the development of thrombotic complications and for
emer-gence of PV [66]. Early or initial PV (or forme fruste of
PV)according to updated ECP criteria in Table 7 is typically
fea-tured by a PV picture in the bone marrow, positive results
forEEC and PRV-1, and/or low serum Epo levels, and a highthrombotic
risk, which is related to increase of hypersensitiveplatelet counts
(thrombocythemia) and slight increase of hema-tocrit up to 0.50,
and therefore candidates for low dose aspirinand phlebotomy (Table
6).
Spontaneous growth of endogenous erythroid colonies(EEC) and
serum erythropoietine (EPO) levels are important,but have
insufficient diagnostic specificity and sensitivity asisolated
parameters to differentiate between PV and SE. Thereliability of
peripheral blood (PB) and bone marrow (BM)EEC was investigated in a
multicenter study including 140patients (80 PV according to the
PVSG, 54 SE, 6 idiopathic
Table 7The updated European Clinical and Pathological (ECP)
Criteria for the Diagno
Clinical (C) criteria suspected for PVC 1. Classical PV: Red
Cell Mass optional Hemoglobin > 18.5/> 16.5 g/dmale/female
Hematocrit (Ht) > 51/> 48% male/female
C 2. Early or latent stage PV
Hematocrit (Ht): 0.450.51 male and 0.430.48 female
C 3. Low plasma Epo level (ELISA)
C 4. Persistent increase of platelet count: grade I: 4001500,
grade II: > 1500.
C 5. Splenomegaly on palpation or on ultrasound echogram (>12
cm length indiameter).
C 6. Granulocytes > 10 109/l or Leukocytes > 12 109/l
and/or raised LAP-score or increased PRV-1 expression in the
absence of fever or infection.
C 7. Platelet-mediated microvascular ischemic, thrombotic
complications
C 8. Typical PV signs and symptoms of hypervolumemia
C 9. Itching, fatigue, upper abdominal complaints
C 10. Absence of any cause of secondary erythrocytosis.
J.J. Michiels et al. / Patholoerythrocytosis) and 10 healthy
controls [52]. PB and BMEEC were positive for 81% and 84% of PV
patients, and94% of PV were diagnosed when BM and PB EEC assayswere
performed with a specificity of near 100%. The diagnos-tic impact
of low serum EPO levels (ELISA assay) was eval-uated in a
multicenter study including 186 patients (116 PVaccording to the
PVSG, 66 SE and 4 idiopathic erythrocytosis)[60]. The majority of
PV patients displayed a serum levelbelow the normal range of 3.3
IU/l with a sensitivity of 87%(101/116), a specificity of 97% and a
positive predictive valueof 97.8%. Statistical analysis (ROC
curves) could define twothresholds allowing a specific and correct
diagnosis of PV byEPO values below 1.4 IU/l and SE by EPO values
above 13.7IU/l. Only 66% (65/99) of PV and 20% (13/66) of SE
werediagnosed with these cut-off points, indicating an overlap
ofserum EPO in PV versus control and controls versus SE
[60].Histopathology from bone marrow biopsies clearly
distin-guishes PV from congenital polycythemias (CP) or
secondaryerythrocytosis (SE) with a sensitivity and specificity of
morethan 95% to almost 100% [4044].6. Myelofibrosis (MF) versus
chronic idiopathicmyelofibrosis (CIMF)
Prefibrotic CIMF according to WHO [24] and ECP [25] is adual
mixed proliferation of increased granulopoiesis and
mega-karyopoiesis dominated by immature giant megakaryocyteswhich
are conspicuously enlarged due to increase of nuclearas well as
cellular size with bulky and irregular roundish-shaped nuclei,
so-called cloud-like nuclei, which are neverseen in ET and PV
(Table 2) [2236]. The PVSG criteria forthe diagnosis of ET include
prefibrotic or early fibrotic CIMF,which is usually associated with
pronounced thrombocythemia(false ET) (Table 4) [33,77]. Classical
CIMF is defined as aclinicopathological entity not preceded by any
other MPD,CML or MDS and characterized by various degrees of
anemia,splenomegaly, a leuko-erythroblastic blood picture with
teardrop-shaped erythrocytes and dry tap on bone marrow aspira-tion
due to various degrees of bone marrow collagen fibrosis or
f Early, Overt and Advanced Stage Polycythemia Vera (PV)
athological (P)criteria diagnostic for PV1. Bone marrow
pathology: increased cellularity with trilineage myeloproli-
eration (i.e. panmyelosis).
roliferation and clustering of small to giant (pleiomorphic)
megakaryocytes.
bsence of stainable iron.
o pronounced inflammatory reaction (plasmacytosis, cellular
debris).
2. Bone marrow biology: spontaneous erythroid colony (EEC)
formation.
3. Molecular biology: heterozygous or homozygous JAK2 V617F
mutation.
1 + P2 + P3 = true PV [1,2,91].
1 or P2 plus P3 plus C1 is classical PV
1 or P2 plus P3 plus any of C2 to C10 is early PV mimicking
ET
iagnosis PV:
1 plus P1 and P2 or C1 and P2 plus any other criterion establish
classical PV
1 and C2 plus any other C criterion establish masked, or early
PV
1, 2, 3 plus C1, 3 plus none of the others is consistent with
erythrocythemictage of PV
Biologie 55 (2007) 92104 99osteosclerosis (Table 8) [7076]. All
studies and reports in theliterature on CIMF up to date have
disregarded and excludedjust by definition the prefibrotic and
early reticulin fibroticstage of CIMF (Table 2).
MF is not a disease because reticulin and collagen fibrosisare
produced by polyclonal fibroblasts as the consequence ofcytokines
released from the clonal granulocytic and megakar-yocytic
proliferative cells in PV and CIMF. The well-knownBaumeister
scoring system was developed on aspirated bonemarrow samples [78].
The Manoharan system scores thedegree of reticulin derived bone
marrow biopsy [79]. A scoringsystem based on morphometric analysis
(point intersectionwith an ocular grid) and quality of fibers
(reticulin and col-lagen fibers) and the bone marrow fiber density
(fine or coursereticulin and some or course bundles of collagen)
have beenproposed by Georgii et al. [1113] and by Thiele et al.
[18,23]. All these different scoring systems for MF use
differentcriteria for grading of reticulin and collagen, are
subjectiveand not comparable by lack of strict criteria. A panel of
experi-enced European pathologists and a foreign expert reached
a
-
consensus on how to grade bone marrow fibrosis (myelofibro-sis:
MF) in bone marrow biopsies of patients with CIMF or PV[80].
Grading of MF was simplified by using four easily repro-ducible
categories including differentiation between reticulinand collagen
[80]. According to defined standardized semi-quantitative grading
of reticulin and collagen fibrosis in thebone marrow, MF can
reliably be graded at the pathologicalbone marrow level as 0 in
prefibrotic, as 1 in early fibrotic,as 2 in classical fibrotic and
as 3 in classical sclerotic CIMF(Tables 2 and 8) [80].
MF is not a feature of true ET and very few ET patients
willdevelop myelofibrosis during long-term follow-up [11,12,8183].
MF is present in only a minority of PV patients at time
ofdiagnosis, but all stages of myelofibrosis have been
observedduring long-term follow-up [11,12,81,82]. As compared to
anormal or near normal life expectancy in true ET and PV,
pre-fibrotic and early fibrotic CIMF with maturation defects
ofenlarged dense clustered megakaryocytes (pronounced
dysme-gakaryopoiesis) are featured by slowly progressive
myelofibro-sis (MF) progressive splenomegaly, thrombocytopenia
and/or
ities [89]. The Lille scoring system is derived from
patientswith classical CIMF or agnogenic myeloid metaplasia(AMM)
and based on two adverse prognostic factors namelyhemoglobin <
10 g/dl and leukocytes count < 4 or> 30 109/l88. The Lille
score is widely used and able to sepa-rate patients with advanced
(classical) CIMF into three groupswith low (score 0), intermediate
(score 1) and high risk (score 2) of progressive disease and loss
of life expectancy. TheCologne score is derived from patients with
prefibrotic, earlyfibrotic and classical CIMF and uses age (70
years), hemoglo-bin (10 g/dl), platelets (< 300 109/l) and
leukocytes(> 20 109/l) myeloblasts (> 2%) or erythroblasts
(> 2%) asfactors with prognostic impact. The Cologne scoring
systemreveals a strong discriminating power and is applicable for
pre-fibrotic and early CIMF (CIMF 0-1) as well as advanced stagesof
CIMF (CIMF 2-3). Applying the Lille score to a cohort of458
patients with prefibrotic or early fibrotic CIMF (CIMF 0-1), 398
belonged to the low risk group with a very good prog-nosis (60%
survival after 15 years) and only 57 and 4 belongedto the
intermediate and high risk group with a much less favor-
clas
P, D
Ba
Acd
E
Mt
Ma
H
Ol
E
J.J. Michiels et al. / Pathologie Biologie 55 (2007)
92104100anemia and a significantly shortened life expectancy as
com-pared to a normal or near normal life expectancy in ET and
PV[8487]. It is reasonable to assume that the prognosis of CIMFmay
depend on the grade of MF in the bone marrow at time ofdiagnosis or
evaluation. Early CIMF with MF grade 0 (prefi-brotic) and grade 1
(early fibrotic) show a more favorable prog-nosis than advanced
stage CIMF with grade 3 MF. However,the survival curves of CIMF
patients with grade 0, 1 and 2 arenot significantly different. Age,
anemia, leukocyte and plateletcounts, but not the degree of MF
(except MF grade 3 and ahypocellular bone marrow) appeared to be
the most reliableand important parameters for prognosis and
survival [8789].The Sheffield scoring system is based on age,
hemoglobin(10g/dl) and the presence or absence of cytogenetic
abnormal-
Table 8The WHO [24] and updated ECP [25,26] Criteria for the
clinical diagnosis of
ClinicalNo preceding or allied other subtype of
myeloproliferative disorders ET, PVCML, CMML atypical CML or
MDS.
Intermediate clinical stage
Anemia grade II:
hemoglobin > 10g/dl
Definitive leuko-erythroblastic blood picture and/or tear drop
erythrocytes
Various degrees of thrombocythemia or normal platelet counts
Various degrees of splenomegaly
No adverse signsa
Advanced clinical stage
Anemia grade III:
hemoglobin < 10 g/l
Various degrees of thrombocytopenia
plus one or more adverse signsa
Molecular biology
JAK2 V617 positive: post-PV MM?
JAK2 V617F negative: classical CIMF?
Screen for cytogenetic abnormalities
a Adverse signs: age > 70 years, hemoglobin < 10 g/dl,
myeloblasts PB > 2%, ery
0 109/l, severe constitutional symptoms, massive splenomegaly,
cytogenetic abnoable prognosis (less than 50% survival after 5
years) [87].There may be an observer disagreement with regard to
the
classification and natural history of prefibrotic and early
CIMFand its differentiation from true ET [87,90]. Those cases
withprefibrotic CIMF and slight dysmegakaryocytopoiesis are
fea-tured by slowly progressive myelofibrosis and splenomegalyand
have a life expectancy close to normal similar as in PV[87].
Discussions between clinicians and pathologists revealthat
diagnostic differentiation between true ET and thrombo-cythemia as
the presenting feature of prefibrotic MM withslight maturation
defect of enlarged clustered megakaryocytes(slight
dysmegakryopoiesis) and no or slight increased cellular-ity is
subjective and due to a rather high inter-observer dis-agreement
between pathologists [87,90].
sical fibrotic or sclerotic chronic idiopathic myelofibrosis
(CIMF)
athologicalry tap on bone marrow aspiration is consistent with
MF grade 2 or 3.
one marrow pathology: megakaryocytic and granulocytic
myeloproliferationnd relative reduction of erythroid
precursors.
bnormal clustering and increase in atypical giant to medium
sized megakaryo-ytes containing clumsy (cloud-like) lobulated
nuclei and definitive maturationefects.
uropean consensus on grading of myelofibrosis (MF) [80]
F 2, manifest CIMF: Diffuse increase in reticulin with extensive
intersec-ions and only focal bundles of collagen. Hypercellular
bone marrow
F 3, overt CIMF: Diffuse and dense increased reticulin with
extensive inter-ctions with course bundles of collagen and
significant osteosclerosis.
ypercellular bone marrow
steomyelosclerosis: Slerosis, endophytic bone formation and
decreased cellu-arity.
ndstage hypocellular bone marrowthro-normoblasts PB > 2%,
leukocytosis > 2 0 109/l, thrombocytopenia < 30rmalities.
-
7. The molecular etiology of the MPDs ET PV and MF
As to the etiology of trilinear myeloproliferation in
PV,Dameshek proposed in 1950 two highly speculative possibili-ties:
the presence of excessive bone marrow stimulation by anunknown
factor or factors, and a lack or a diminution in thenormal
inhibitory factor or factors [1]. The JAK2 V617F muta-tion reflects
a gain of function mutation, which is in line withthe concept of
Dameshek [1] that all stops to blood produc-tion in the bone marrow
seem to have been pulled out, whichnow appears to due to one
factor, the JAK2 V617F mutationdiscovered Vainchenker et al. [91]
and rapidly confirmed byseveral investigators [9296]. The JAK2
V617F mutationcauses hypersensitivity of hematopoietic progenitor
cells togrowth factors, which readily can explain the trilinear
myelo-proliferation and the interrelationships between ET, PV
and
whether the JAK2 V617F mutation, homozygous in particularor
additional genetic events and/or the use of potential leuke-mogenic
drugs contribute to the leukemic transformation ofMPDs.
The current concept is that heterozygous JAK2 V617Fmutation with
increased kinase activity is enough for megakar-yocyte
proliferation and increased hypersensitive plateletscomplicated by
platelet-mediated microvascular events withno or slightly increased
erythropoiesis in ET and in early PVmimicking ET (Table 9) [2].
Homozygous JAK2 mutation withpronounced kinase activity is
associated with trilinear mega-karyocyte, erythroid and
granulocytic myeloproliferation, mye-loid metaplasia and secondary
myelofibrosis (MF) with themost frequent clinical picture of
classical PV complicated bymajor thrombosis on top of the
platelet-mediated microvascularthrombotic syndrome of
thrombocythemia (Table 9). The
cell
pa
e 0
Microvascular Macrovascular
J.J. Michiels et al. / Pathologie Biologie 55 (2007) 92104
101Thrombosis ThrombosisCIMF (Table 9) [2,9799]. Applying the PVSG
criteria, 4250% of the ET patients, 4267% of CIMF patients, 7292%of
PV patients have the mutated the JAK2 allele as detectedby DNA
sequencing [9296]. A much higher frequency ofJAK2 of 97% in PV,
4957% in ET and 57% in CIMF wasdescribed in three studies that used
allele-specific polymerasechain reaction (PCR) analysis
[94,96,100,101]. The presenceof the JAK2 V617F mutation was
strongly correlated withPRV-1 over expression and the ability to
form spontaneousEEC in all three subtypes of MPD (Tables 6 and 7)
[102,103]. The JAK2 V617F mutation was absent in more than600
healthy controls, in patients with Ph1+ CML, in patientswith
reactive thrombocytosis [9296], and in patients with denovo AML,
CLL, B-ALL and T-ALL [96,104]. The mutationhas been found rarely in
MDS (3/116 = 2.6%) [92,96], hyper-eosinophilic syndrome (2/145 =
1.4%) [92,96,105,106], butsomewhat more frequent in chronic
myelomonocytic leukemia,and atypical CML 31/408 = 7.6%)
[92,96,105,106]. The JAK2V617F mutation is rather frequent in
unclassified MPD(13/53 = 25%) [96] and frequent in AML with
preceding MPD(12/22 = 55%) [106]. The latter finding arises a key
question
Table 9Molecular etiology of platelet-mediated microvascular
thrombosis, increased redVainchenker & Michiels 2005
JAK2 V617F gain of function mutation in trilinear hematopoietic
cells of MPDStep 1 V617F+ Step 12 V617F++
LOH Spontanuous SpontanuousCFU-MK / EEC EEC, CFU-MKET PV
Increase of enlargedhypersensitive platelets
Increase of hematocrit to abovhigher platelets
Already at platelet >400
Clinical Step 1 Clinical Step 2Aspirin sensitive
Aspirin/Phlebotomy
See figures 1 and 2 regarding the natural history of true PV
according to Wassermsequential occurrence of heterozygous and
homozygousV617F mutation can readily explain the progression of
ETand early PV to overt PV and may explain at least in part
theaccompanied granulocytic proliferation, leukocyte
activation(increased LAP score and PRV-1 expression),
leukocytosis(leukocythemia), and secondary myelofibrosis (Table 9)
[1,2].
Depending on the set of laboratory tests and diagnostic
cri-teria used, the population of the MPD patients defined as ET,PV
and CIMF are heterogeneous at the molecular and biologi-cal level
(Tables 1, 2, 7, 8). As the JAK2 V617F mutation isthe cause of a
distinct trilinear MPD in its manifold clinicalmanifestations
during long-term follow-up [2], the specificityof a positive JAK2
V617F PCR test for the diagnosis ofMPD is high (near 100%), but
only half of ET and CIMF (sen-sitivity 50%) and the majority of PV
(sensitivity 8597%) areJAK2 V617F positive. Kiladjian et al. [107]
searched for theJAK2 V617F mutation in a cohort of 44 female ET
patientswith previously documented clonality data
(X-chromosomeinactivation pattern: XCIP assay). The mutation was
found infour of the nine patients with polyclonal hematopoiesis
(prob-ably due to better sensitivity of mutation detection than
XCIPassays), in 13 of the 31 patients with monoclonal
hematopoi-
mass and secondary myelofibrosis in JAK2 V617F positive MPDs ET,
PV, MF
tients is detectable in platelets, erythroblast and
granulocytesStep 12 V617F++
LOH
Myeloid Metaplasia: MMLeukocyte activationPVR-1 = LAF
.45-0.50: PV Leukocythemia/cytokinesFatigue, splenomegaly,
unclassified MPD,MMM
Clinical Step 3 Secondary MF: 30%
Thrombosis ThrombosisConstitutional symptoms
IFN/Hydroxyurea
an and Thiele.
-
[7]
[8]
[9]
[10
[11
[12
[13
[14
[15
[16
[17
[18
[19
[20
[21
[22
[23
[24
[25
gie Bioesis and in two of the four patients with undetermined
clonalitystatus due to non-random XCIP. These results show that
themajority of patients with ET according to the PVSG withoutV617F
JAK2 mutation have nevertheless a clonal hematopoie-tic stem cell
disease. Combining results of JAK2 sequencingand XCIP assays
allowed demonstration of a clonal prolifera-tion in 90% of ET
cases. Buck et al. [108] observed a lowerincidence of 25% JAK2
V617F positivity in patients with trueET according to the WHO and
ECP criteria (personal commu-nication). In a large prospective
study of 806 ET patients diag-nosed according to the PVSG criteria,
about half of the ETpatients (53%) were JAK2 V617F positive. ET
patients posi-tive for the JAK2 V617F mutation have higher
hemoglobinlevel and a significantly higher rate of transformation
into PVduring follow-up as compared to ET patients negative for
theJAK2 V617F mutation [108]. Comparing the laboratory fea-tures of
JAK2 V617 positive ET and JAK2 V617 negativeET patients in the PT-1
study clearly showed that JAK2V617 positive ET is featured by
higher values for hemoglobin,hematocrit, neutrophil counts, lower
values for serum EPOlevels, serum ferritine and MCV, and
hypercellularity of thebone marrow in biopsy material indicating
that JAK2 V617positive ET patients diagnosed according to the PVSG
criteriarepresent a forme fruste of PV [108] consistent with early
PVmimicking ET (ECP stage 1 in Table 6). In contrast, the
JAK2negative ET patients had significantly higher platelet
countsand showed a clinical picture of true ET with normal serumEPO
levels and increased of clustered megakaryocytes in anormocellular
bone marrow consistent with a diagnosis oftrue ET (Table 1). These
clinical data indicate that JAK2V617F mutation defines one disease
with several sequentialsteps of ET, PV and MF during long-term
follow-up (Table 9).Patients with either JAK2 V617F positive or
negative prefibro-tic and fibrotic CIMF may represent two distinct
entities with arelated etiology for one and the same disorder. Bone
marrowhistopathology when used in combination with specific
mar-kers like JAK2 V617F, serum EPO, PRV-1, EEC, peripheralblood
parameters has a high sensitivity and specificity (almost100%) to
detect each of the early stages of MPD and to differ-entiate
between ET, PV and CIMF in both JAK2 V617F posi-tive and negative
MPDs.
References
[1] Dameshek W. Physiopathology and course of polycythemia vera
asrelated to therapy. J Am Ass Med 1950;142:7907.
[2] James C, Ugo V, Casadevall N, Constantinescu SN, Vainchenker
WA.JAK2 mutation in myeloproliferative disorders: pathogenesis and
thera-peutic and scientific prospects. Trends Mol Med 2005 (On
line).
[3] Wasserman LR. Polycthemia vera, its course and treatment:
relation tomyeloid metaplasia and leukemia. Bull N Y Acad Med
1954;30:34375.
[4] Wasserman LR, Berk PD. Berlin NI. Polycythemia vera and the
myelo-proliferative disorders. Philadelphia: WB Saunders; 1995
(ISBN 0-7216-4213-6).
[5] Pearson TC, Wetherley-Mein G. The course and complications
of idio-
J.J. Michiels et al. / Patholo102pathic erythrocytosis. Clin Lab
Haematol 1979;1:18996.[6] Najean Y, Triebel F, Dresch C. Pure
erythrocytosis: reappraisal of a
study of 51 patients. Am J Hematol 1981;10:12936.[26Glaser RM,
Walker RI. Transitions among the myeloproliferative disor-ders. Ann
Intern Med 1969;71:285307.Burkhardt R., Bartl R., Jaeger K., Frisch
B., Kettner G., Mahl G., SundM. Chronic myeloproliferative
disorders. Path Res Pract 1084;179:131-186.Georgii A, Vykoupil KF,
Thiele J. Chronic megakaryocytic granulocy-tic myelosis: CMGM.
Virch Arch A Path Anat Histol 1980;389:25368.
] Georgii A, Vykoupil KF, Buhr T, Choritz H, Doehler U, Kaloutsi
V,Werner M. Chronic myeloproliferative disorders in bone marrow
biop-sies. Path Res Pract 1990;186:327.
] Georgii A, Buhr T, Buesche G, Kreft A, Choritz H.
Classification andstaging of Ph-negative myeloproliferative
disorders by histopathologyfrom bone marrow biopsies. Leuk Lymphoma
1996;22(Suppl 1):1529.
] Georgii A, Buesche G, Kreft A. The histopathology of chronic
myelo-proliferative diseases. Bailires Clin Haematol
1998;11:72149.
] Thiele J, Ballard AC, Georgii A, Vykoupil KF. Chronic
megakaryocyticgranulocytic myelosis: An electron microscopic study.
Megakaryocytesand thrombocytes. Virch Arch 1977;373:191211 (Path
Anat Histol).
] Thiele J, Holgado S, Choritz H, Georgii A. Density
distribution and sizeof megakaryocytes in inflammatory reactions of
the bone marrow (mye-litis) and chronic myeloproliferative
disorders. Scand J Haematol 1983;31:32941.
] Thiele J, Zankovich R, Schneider G, Kremer B, Fischer R, Diehl
V.Primary (essential) thrombocythemia versus polycythemia vera
rubra.A histomorphometric analysis of bone marrow features in
trephine biop-sies. Analyt Quat Cytol Histol 1988;10:37582.
] Thiele J, Zankovich R, Steinberg T, Kremer B, Fischer R, Diehl
V. Pri-mary (essential) thrombocythemia versus hyperplastic stages
of agno-genic myeloid metaplasia with thrombocytosis: a critical
evaluation ofclinical and histomorphological data. Acta Haematol
1989;81:192202.
] Thiele J, Wagner S, Degel C, et al. Megakaryocyte precursors
(pro- andmegakaryoblasts) in bone marrow tissue from patients with
reactivethrombocytosis, polycythemia vera and primary (essential)
thrombo-cythemia. Virch Arch 1990;58:295302 (Cell Pathol).
] Thiele J, Kvasnicka HM, Werden C, Zankovich R, Diehl V,
Fischer R.Idiopathic primary osteo-myelofibrosis: A
clinico-pathological study on208 patients wit special emphasis on
evolution of disease features, dif-ferentiation from essential
thrombocythemia and variables of prognosticimpact. Leuk Lymphoma
1996;22:30317.
] Michiels JJ. The myeloproliferative disorders. An historical
appraisaland personal experiences. Leuk Lymphoma 1996;22(Suppl
1):114.
] Michiels JJ. Diagnostic criteria of the myeloproliferative
disorders(MPD) essential thrombocythemia, polycythemia vera and
chronicmegakaryocytic granulocytic metaplasia. Neth J Med
1997;51:5764.
] Michiels JJ, Juvonen E. Proposal for revised diagnostic
criteria ofessential thrombocythemia and polycythemia vera by the
Thrombo-cythemia Vera Study Group. Semin Thromb Hemostas
1997;23:33947.
] Thiele J, Kvasnicka HM, Fischer R. Histochemistry and
morphometryon bone marrow biopsies in chronic myeloproliferative
disorders: aidsto diagnosis and classification. Ann Hematol
1999;78:495506.
] Thiele J, Kvasnicka HM, Diehl V, Fischer R, Michiels JJ.
Clinicopatho-logical diagnosis and differential criteria of
thrombocythemias in var-ious myeloproliferative disorders by
histopathology, histochemistryand immunostaining from bone marrow
biopsies. Leuk Lymphoma1999;33:20718.
] WHO classification of the chronic myeloproliferative diseases
(CMPD)polycythemia vera, chronic idiopathic myelofibrosis,
essential thrombo-cythemia and CMPD unclassifiable. WHO
Classification of Tumours.Tumours of Haemtopoiesis and Lymphoid
Tissues. Lyon: IARC;2001. p. 3142.
] Michiels JJ, Thiele J. Clinical and pathological criteria for
the diagnosisof essential thrombocythemia, polycythemia vera and
idiopathic myelo-fibrosis (agnogenic myeloid metaplasia). Int J
Hematol 2002;76:133
logie 55 (2007) 9210445.] Michiels JJ. Bone marrow
histopathology and biological markers as
specific clues to the differential diagnosis of essential
thrombocythemia,
-
[27
[28
[29
[30
[31
[32
[33
[34
[35
[36
[37
[38
[39
[40
[41
[42
[43
[44
[45
[46
[47
[48
[49
[50
[51
[52
[53
[54
[55
[56
[57
[58
[59
[60
[61
[62
[63
[64
[65
[66
[67
gie Biopolycythemia vera and prefibrotic or fibrotic myeloid
metaplasia.Hematol J 2004;5:93102.
] Thiele J, Kvasnicka HM, Boeltken B, Zankovich R, Diehl V,
Fischer R.Initial (prefibrotic) stages of idiopathic (primary)
myelofibrosis (IMF): aclinicopathological study. Leukemia
1999;13:174117428.
] Thiele J, Kvasnika HM, Zankovich R, Diehl V. Relevance of bone
mar-row features in the differential diagnosis between essential
thrombo-cythemia and early stage idiopathic myelofibrosis.
Haematlogica 2000;85:112634.
] Thiele J, Kvasnicka HM, Zankovich R, Diehl V. Clinical and
morpho-logical criteria for the diagnosis of prefibrotic idiopathic
(primary) mye-lofibrosis. Ann Hematol 2001;80:1605.
] Thiele J, Kvasnicka HM, Zankovich R, Diehl V. Early stage
idiopathic(primary) myelofibrosis: current issues of diagnostic
features. LeukLymphoma 2002;43:103641.
] Thiele J, Kvasnicka HM. Diagnostic differentiation of
essential throm-bocythemia from thrombocythemia associated with
chronic idiopathicmyelofibrosis by discriminate analysis of bone
marrow features. HistolHistopathol 2003;18:93102.
] Thiele J, Kvasnicka HM, Schmitt-Graeff A, Diehl V. Dynamics
offibrosis in chronic idiopathic (primary) myelofibrosis during
therapy: afollow-up on 308 patients. Leuk Lymphoma
2003;44:94953.
] Thiele J, Kvasnicka HM. Chronic myeloproliferative disorders
withthrombocythemia: a comparative study of two classifications
systems(PVSG-WHO) on 839 patients. Ann Hematol 2003;82:14852.
] Thiele J, Kvasnicka HM. Prefibrotic chronic myelofibrosis a
diagnos-tic enigma? Acta Haematol 2004;111:1559.
] Thiele J, Kvasnicka HM, Diehl V. Standadization of bone marrow
fea-turesdoes it work in hematopathology for histological
discriminationof different disease patterns? Histopathol
2005;20:63344.
] Thiele J, Kvasnicka HM, Orazi A. Bone marrow histopathology
inmyeloproliferative disorderscurrent diagnostic approacj.
SeminHematol 2005;42:18495.
] Laszlo J. Myeloproliferative disorders (MPD): myelofibrosis,
myelo-sclerosis, extramedullary hematopoiesis, undifferentiated MPD
andhemorrhagic thrombocythemia. Semin Hematol 1975;12:40932.
] Murphy S, Iland H, Rosenthal D, Laszlo J. Essential
thrombocythemia:an interim report from the Polycythemia Vera Study
Group. SeminHematol 1986;23:17782.
] Berlin NI. Diagnosis and classification of the polycythemias.
SemHematol 1975;12:33951.
] Thiele J, Kvasnicka HM, Zankovich R, Diehl V. The value of
bonemarrow histopathology for the differentiation between early
stage poly-cythemia vera and secondary (reactive) polycythemias.
Haematologica2001;86:36874.
] Thiele J, Kvasnicka HM, Muehlhausen K, Walter S, Zankovich
R,Diehl V. Polycythemia rubra vera versus secondary polycythemias.
Aclinicopathological evaluation of distinctive features in 199
patients.Pathol Res Pract 2001;197:7784.
] Thiele J, Kvasnicka HM, Diehl V. Bone marrow features of
diagnosticimpact in erythrocytosis. Ann Haematol 2005;84:3627.
] Thiele J, Kvasnicka HM, Diehl V. Initial (latent) polycythemia
verawith thrombocytosis mimicking essential thrombocythemia. Acta
Hae-matol 2005;113:2139.
] Thiele J, Kvasnicka HM. Diagnostic impact of bone marrow
histo-pathology in polycythemia vera (PV). Histol Histpathol
2005;20:31728.
] Tefferi A. Polycythemia vera: a comprehensive review and
clinicalrecommendations. Mayo Clin Proc 2003;78:17494.
] McMullin MF, Bareford D, Campell P, Green AR, et al.
Guidelines forthe diagnosis, investigation and management of
polycythaemia/erythro-cytosis. Br J Haematol 2005;130:17495.
] De Stefano V, Teofili L, Leone G, Michiels JJ. Spontaneous
erythroid
J.J. Michiels et al. / Patholocolony formation as the clue to an
underlying myeloproliferative disor-der in Budd-Chiari syndrome or
portal vein thrombosis. Semin ThrombHemostas 1997;23:4118.] Chait
Y, Condat B, Cazals-Hatem D, et al. Relevance of the
criteriacommonly used to diagnose myeloproliferative disorders in
patientswith splanchnic vein thrombosis. Br J Haematol
2005;129:55360.
] Liu E, Jelinek J, Pastore YD, Guan Y, Prchal JF, Prchal JT.
Discrimina-tion of polycythemias and thrombocythemias by novel,
simple accurateclonality assays and comparison with PRV-1
expression and BFU:Eresponse to erythropoietin. Blood
2003;101:3294301.
] Shih L-Y, Lee C-T. Identification of masked polycythemia vera
frompatients with idiopathic marked thrombocytosis by endogenous
ery-throid colony assay. Blood 1994;83:7448.
] Westwood NB, Pearson TC. Diagnostic applications of
haematopoieticprogenitor culture techniques in polycythaemias and
thrombocythae-mias. Leuk Lymphoma 1996;22:95103.
] Dobo I, Donnard M, Giridon F, Mossuz P, et al. Standardization
andcomparison of endogenous erythroid colony assays performed
withbone marrow or blood progenitors for the diagnosis of
polycythemiavera. Hematol J 2004;5:1617.
] Florensa L, Besses C, Zamora L, Bellosillo B, Espinet B,
Serrano S,et al. Endogenous erythroid and megakaryocytic
circulating progenitors,HUMARA clonality assay, and PRV-1
expression are useful tools fordiagnosis of polycythemia vera and
essential thrombocythemia. Blood2004;103:24278.
] Messinezy M, Westwood NB, El-Hemaida I, Marsden JT, Sher-wood
RS, Pearson TC. Serum erythropoietin values in erythrocytosisand in
primary thrombocythaemia. Br J Haematol 2002;117:4753.
] Cotes PM, Dore CJ, Tin JA, Lewis SM, Messinezy M, Pearson
TC,et al. Determination of serum immunoreactive erythropoietin in
theinvestigation of erythrocytosis. N Engl J Med 1986;315:2837.
] Birgegard G, Wide L. Serum erythropoietin in the diagnosis of
poly-cythemia and after phlebotomy treatment. Br J Haematol
1992;81:6036.
] Messinezy M, Westwood NB, Woodstock SP, Strong RM, Pearson
TC.Low serum erythropoietin: a strong diagnostic criterion of
primary poly-cythaemia even at normal haemoglobin levels. Clin Lab
Haematol1995;17:21720.
] Carneskog J, Kutti J, Wadenvik H, Lundberg PA, Lindstedt G.
Plasmaerythropoietin by high-detectability immunoradiometric assay
inuntreated patients with polycythemia vera and essential
thrombocythe-mia. Eur J Haematol 1998;60:27882.
] Griesshammer M, Kubanek B, Beneke H, Heimpel H, Bangerter
M,Bergmann L, Shrezenmeier H. Serum erythropoietin and
thrombopoie-tin levels in patients with essential thrombocythemia.
Leuk Lymphoma2000;36:5338.
] Mossuz P, Giridon F, Latger-Cannoard V, Dobo I, et al. In:
Diagnosticvalue of serum erythropoietin level in patients with
absolute erythrocy-tosis. Haematlogica; 2004. p. 11948.
] Temerinac S, Klippel S, Strunck E, Rder S, Lbbert M, Lange
M,et al. Cloning of PRV-1, a novel member of the uPAR receptor
super-family, which is over expressed in polycythemia rubra vera.
Blood2000;95:256976.
] Pahl HL. Towards a molecular understanding of polycythemia
rubravera. Eur J Biochem 2000;267:3395401.
] Klippel S, Strunck E, Termerinac S, et al. Quantification of
PRV-1expression, a molecular marker for the diagnosis of
polycythemia vera.Blood 2001;98:470a.
] Pahl HL. Polycythaemia vera: will new markers help us answer
oldquestions? Acta Haematol 2002;108:12031.
] Johanson P, Andreason B, Safai-Kutti S, Wennstrom L, Palmqvist
L,Rickson A, et al. The presence of a significant association
between ele-vated PRV-1 mRNA expression and low plasma
erythropoietin concen-tration in essential thrombocythemia. Eur J
Haematol 2003;70:35862.
] Griesshammer M, Klippel S, Strunk E, Temeric S, Mohr U,
Heimpel H,et al. PRV-1 mRNA expression discriminates two types of
essentialthrombocythemia. Ann Hematol 2004;83:36470.
] Juvonen E, Ikkala E, Oksanen K, Ruutu T. Megakaryocyte and
ery-
logie 55 (2007) 92104 103throid colony formation in essential
thrombocythemia and reactivethrombocytosis: diagnostic value and
correlation to complications. Br JHaematol 1993;83:1927.
-
[69
[70
[71
[72
[73
[74
[75
[76
[77
[78
[79
[80
[81
[82
[83
[84
[85
[86
[87
[88
[90
[91
[92
[93
[94
[95
[96
[97
[98
[99
[10
[10
[10
[10
[10
[10
[10
[10
[10genous megakaryocyte and erythroid colony formation from
blood inessential thrombocythemia. Leukemia 1995;9:2713.
] Jantunen R, Juvonen E, Ikkala E, Oksanen K, Anttila P, Jormila
P, et al.Essential thrombocythemia at diagnosis: causes of
diagnostic evaluationand presence of positive diagnostic findings.
Ann Hematol 1998;77:1016.
] Reilly JT. Pathogenesis of idiopathic myelofibrosis: present
status andfuture directions. Br J Haematol 1994;88:18.
] Tefferi A, Silverstein MN, Nol P. Agnogenic myeloid
metaplasia.Semin Hematol 1995;22:32733.
] Barosi G, Ambrosetti A, Finelli, et al. The Italian consensus
conferenceon diagnostic criteria for myelofibrosis with myeloid
metaplasia. Br JHaematol 1999;104:7307.
] Barosi G. Myelofibrosis with myeloid metaplasia: diagnostic
definitionand prognostic classification for clinical studies and
treatment guide-lines. J Clin Oncol 1999;17:295470.
] Tefferi A. Myelofibrosis with myeloid metaplasia. N Engl J Med
2000;342:125565.
] Dingli D, Mesa RA, Tefferi A. Myelofibrosis with myeloid
metaplasia:new developments in pathogenesis and treatment. Intern
Med 2004;43:5407.
] Thiele J, Kvasnicka HM, Diehl V. Bone marrow CD34+
progenitorcells in Philadelphia chromosome-negative chronic
myeloproliferativedisorders: a clinicopathological study on 575
patients. Leuk Lymphoma2005;46:70915.
] Florena AM, Tripodi C, Iannitto E, Porcasi R, Ingrao S, Franco
V.Value of bone marrow biopsy in the diagnosis of essential
thrombo-cythemia. Haematologica 2004;89:9119.
] Bauermeister DE. Quantification of bone marrow reticulin. Am J
ClinPathol 1971;56:2431.
] Manoharan A, Smart RC, Pitney WR. Prognostic factors in
myelofibro-sis. Pathology 1982;14:44561.
] Thiele J, Kvasnicka HM, Facchetti F, Franco V, Van Der Walt J,
OraziA. European consensus for grading of bone marrow fibrosis and
assess-ment of cellularity in myeloproliferative disorders.
Haematologica 2005;90:112832.
] Buhr T, Georgi A, Choritz H. Myelofibrosis in chronic
myeloprolifera-tive disorders. Incidence among subtypes to the
Hannover Classifica-tion. Patol Res Pract 1993;189:12132.
] Thiele J, Kvasnicka HM, Schmitt-Graeff A, Zankovich R, Diehl
V.Follow-up examinations including sequential bone marrow biopsies
inessential thrombocythemia (ET): a retrospective
clinicopathologicalstudy of 120 patients. Am J Hematol
2002;70:28391.
] Kreft A, Buesche G, Ghalibafian M, Buhr T, Fischer T,
Kirkpatrick CJ.The incidence of myelofibrosis in essential
thrombocythemia, poly-cythemia vera and chronic
idiopathicmyelofibrosis: a retrospective eva-luation of sequential
bone marrow biopsies. Acta Haematol 2005;113:13743.
] Thiele J, Kvanicka HM, Schmitt-Graeff A, Diehl V. Dynamics of
fibro-sis in chronic idiopathic (primary) myelofibrosis during
therapy: afollow-up study on 309 patients. Leuk Lymphoma
2003;44:94953.
] Buhr T, Buesche G, Choritz H, Langer F, Kreipe H. Evolution of
mye-lofibrosis in chronic idiopathic myelofibrosis as evidenced in
sequentialbone marrow biopsy specimens. Am J Clin Pathol
2003;119:1528.
] Thiele J, Kvasnicka HM. Hematopathologic findings in chronic
idio-pathic myelofibrosis. Semin Oncol 2005;32:38094.
] Michiels JJ, Kvasnicka HM, Thiele J. Myeloproliferative
Disorders:current perspectives on diagnostic criteria,
histopathology and treat-ment. Munich Germany: Verlag ME Uwe
Grunwald; 2005 (ISBN 3-9898075-6-8).
] Dupriez B, Morel P, Demory JL, Lai JL, Simon M, Plantier I, et
al.Prognostic factors in agnogenic myeloid metaplasia: a report on
195cases with a bew scoring syste. Blod 1996;88:10138.management.
Blood Rev 1997;11:23342.] Michiels JJ. Clinical, pathological and
molecular features of myelopro-
liferative disorders: MPD 2005 and beyond. Hematology (Am
SocHematol Educ Program) 2005;10(Suppl 1):21523.
] James C, Ugo V, Le Couedic PF, Staerk J, Delhommeau F, Lacout
C,et al. A unique clonal JAK2 mutation leading to constitutive
signallingcauses polycythemia vera. Nature 2005;434:11448.
] Levine RL, Wadleigh M, Cools J, Ebert BL, Wernig G, Huntly
BJ,et al. Activating mutation in the tyrosine kinase JAK2 in
polycythemiavera, essential thrombocythemia and myeloid metaplasia
with myelofi-brosis. Cancer Cells 2005;7:38797.
] Kralovics R, Passamonti F, Buser AS, Teo SS, Tiedt R, Passweg
JR,et al. A gain-of-function mutation of JAK2 in myeloproliferative
disor-ders. N Engl J Med 2005;352:177990.
] Baxter EJ, Scott LM, Campbell PJ, East C, Fourouclas N,
Swanton S,et al. Acquired mutation of the tyrosine kinase in human
myeloproli-ferative disorders. Lancet 2005;365:105461.
] Zhao R, Xing S, Li Z, Fu X, Li Q, Krantz AS, et al.
Identification of anacquired JAK2 mutation in polycythemia vera. J
Biol Chem 2005;29.
] Kaushanky K. On the origin of the chronic myeloproliferative
disorders:it makes all sense. Blood 2005;105:418790.
] Goldman JM. A unifying mutation in chronic myeloproliferative
disor-ders. N Engl J Med 2005;352:17445.
] Cazzola M, Skoda R. Gain of function, loss of control. A
molecularbasis for chronic myeloproliferative disorders.
Haematologica HematolJ 2005;90:8714.
] Jones AV, Kreil S, Xoi K, Waghorn K, Curtis C, Zhang L, et al.
Wide-spread occurrence of the JAK2 V617F mutation in chronic
myeloproli-ferative disorders. Blood 2005;106:21628.
0] Wolanskyj AP, Lasho TL, Schwager SM, McClure RF, Wadleigh
M,Lee SJ, et al. JAK2 V617 mutation in essential thrombocythaemia:
clin-ical associations and long-term relevance. Br J Haematol
2005;131:20813.
1] Antonioli E, Guglielmelli P, Pancrazzi A, Bogani C, Verrucci
M, Pon-ziani V, et al. Clinical implications of the JAK2 V617F
mutation inessential thrombocythemia. Leukemia 2005;19:18479.
2] Goerttler PS, Steimle C, Maerz E, Johanson PL, Andreasson B,
Gries-shammer M, et al. The JAK2 V617F mutation, PRV-1 over
expressionand EEC formation define a similar cohort of MPD
patients. Blood2005;106:28624.
3] Kralovics R, Teo SS, Buser AS, et al. Altered gene expression
in mye-loproliferative disorders correlates with activation of
signalling by theV617F mutation of JAK2. Blood 2005;106:33746.
4] Levine RL, Loriaux M, Huntly BJP, Loh ML, et al. The JAK2
V617Factivating mutation occurs in chronic myelomonocytic leukemia
andacute myeloid leukemia, but not in acute lymphoblastic leukemia
orchronic lymphocytic leukemia. Blood 2005;106:33779.
5] Steensma DP, Dewald M, Lasho TL, Powell HL, McClure RF.
LevineRL et al. The JAK2 V617F activating tyrosine kinase mutation
is aninfrequent event in both atypical myeloproliferative disorders
and themyelodysplastic syndrome. Blood 2005;106:12079.
6] Jelinek J, Oki Y, Gharibyan V, Bueso-Ramos C, Prchal JT,
VerstovsekS, et al. JAK2 mutation 1849G >T is rare in acute
leukemias but can befound in CMML, Philadelphia-chromosome negative
CML and mega-karyocytic leukemia. Blood 2005 [Epub ahead of
print].
7] Kiladjian JJ, Elkassar N, Hetet G, Balitrand N et al.
Analysis of JAK2mutation in essential thrombocythemia (ET) patients
with monoclonaland polyclonal X-chromosome inactivation patterns
(XCIPs). Blood(Suppl Abstract 807-II).
8] Campbell P, Scott LM, Buck G. Definition of subtypes of
essentialthrombocythaemia and relation to polycythaemia vera based
on JAK2V617F mutation status: a prospective study. Lancet
2005;366(9501):194553.[68] Florensa L, Bessis C, Woessner S, Sole
F, Acin P, Pedro C, et al. Endo- [89] Reilly JT. Idiopathic
myelofibrosis: pathogenesis, natural history and
J.J. Michiels et al. / Pathologie Biologie 55 (2007)
92104104
Current diagnostic criteria for the chronic myeloproliferative
disorders (MPD) essential thrombocythemia (ET),
polycythe..IntroductionThe concept of PV as a trilinear
MPDClinical, laboratory and pathological features of the MPDsWHO
pathological criteria for the diagnosis of ET, PV and CIMFCurrent
clinical and pathological criteria for the diagnoses of ET PV and
CIMFMyelofibrosis (MF) versus chronic idiopathic myelofibrosis
(CIMF)The molecular etiology of the MPDs ET PV and MFReferences









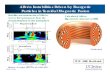



![Zgbc F B Dmavfbg ©BBBªBBBBBBBBBBBBBBBBBB ]karatevolkhov.ru/Pervenstvo_MLBI_2018.pdf · ^h dx klZjr_ dx dx klZjr_ dx 8 - e_l FZevqbdb ^h dx\dexqbl_evgh ^h dx\dexqbl_evgh >_\hqdb](https://img.dokumen.tips/doc/110x75/5ec420b3644640007216892f/zgbc-f-b-dmavfbg-bbbbbbbbbbbbbbbbbbbbb-h-dx-klzjr-dx-dx-klzjr-dx-8-el.jpg)