Embed Size (px)
Citation preview

CambridgePolymer Group, Inc.
Testing, Consultation, and Instrumentation for Polymeric Materials
Assessing the Cleanliness of Medical Devices
Stephen Spiegelberg
AMI’s Medical Grade Polymers 2010

Background of Cambridge Polymer Group
• Contract research company formed in 1996• Core competencies
– polymer R&D– test methodology development– instrumentation design
• Biomedical community– bone cement– crosslinked polyethylene– spine– eye– vascular– product recalls– cleanliness of medical devices

Sterile is not the same as Clean
• Sterile: live microorganisms content is below acceptable levels– Bacteria, yeast, fungi, molds, viruses– Sterility Assurance Limit (SAL): probability that an implant will
remain nonsterile following sterilization • 10-6 (one in a million)
• Clean: non-live residue content is below acceptable levels– Pyrogens – dead but deadly– Chemicals– Particulate matter

Sterile is not the same as clean
Methods of Sterilization
Detergent Wash
Alcohol Wash
Acid Passivation
Air blasting
High pressure rinses
Sonication
Methods of Cleaning
Glutaraldehyde
Ethylene oxide
Steam/Dry Heat*
Plasma
Ionizing radiation*
*issues with polymeric devices

Case Study I
• In 2000, Sulzer Orthopedics noticed higher than normal revision surgeries on their InterOp Acetabular Shell
• High failure rate in isolated manufacturing group
Explanted hip components showed little tissue ingrowthinto the porous titanium backing, even after 11 months of in vivo use.
Spiegelberg, Deluzio, Muratoglu, Trans Orthopedic Research Society, 2003

InterOp Acetabular ShellCementless fixation: relies on osseointegration in porous titanium structure

What Happened?
Independent Research Team
Pathologists Manufacturing Experts Analytical Labs
Believed to be related to a manufacturing residue
Try to identify type of residue in order to determine best analytical technique
Design sample preparation procedure to extract and quantify residue
Validate extraction and analysis technique
Determine resolution levels

Preliminary Information
• Suspected that a residue was on implants
• Introduction believed to be from machining lubricants
• Received sample lubricants from manufacturer

Protocols
• Extract residue from component
– solvent selection
• Analyze mass of residue with quantified technique
• Identify composition
• Look for trends with manufacturing

Solvent Selection
-1
0
1
2
3
4
5
400900140019002400290034003900
wavenumber [cm-1]
abso
rban
ce [A
.U.]
oilCarbon tetrachlorideChloroform
Select solvent that does not have an IR absorption band in the region of the target materialGood solvent for target material
C Cl
Cl
Cl
Cl
oil
Carbon tetrachloride
HH

Extraction Protocol
Protocol on web site: www.campoly.com
Carbon tetrachloride
Sonicate for 1 hour
Rinse component
Concentrate solution(77 C)

Calibration Curve for Oil
A = 325.27cR2 = 0.9967
0
10
20
30
40
50
60
70
0 0.05 0.1 0.15 0.2 0.25
hydrocarbon concentration [wt.%]
A28
19-2
992
cm-1
Oils A, I, K, F, D
1 mm path lengthAreas baseline-corrected
A = αbc

Validation StudyPorous titanium test samples coated with known amounts of oil
Oil Measurement Validation Study
0
5
10
15
20
25
30
35
40
45
1 2 3 4 5 6 7 8 9 10
sample
oil c
onte
nt [m
g]
Applied Oil
0
5
10
15
20
25
30
35
40
45
1 2 3 4 5 6 7 8 9 10
Meas ured Oil C on ten t
Oil
cont
ent [
mg]
Corrections for hydrocarbons in solvent

Oil in Shelf-Stored Components
• Examined oil content in over 500 acetabular shells
• Grouped component lots by manufacturing history

Manufacturing Procedure
Machine titanium
shell
Apply porouscoating
Group1
Nitric acidpassivation
High temperaturesintering
Detergentwash&rinse
Group2
Peg chamfer
Group3
ID turn
Group4
No passivation

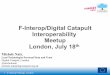
Manufacturing History Analysis
0
10
20
30
40
50
60
70
80
1260000 1280000 1300000 1320000 1340000 1360000 1380000 1400000 1420000 1440000 1460000
Lot Number
Oil
Con
tent
(mg)
Group1Group2Group3Group4
passivation
88% of failures
no passivation
No statistical dependence of oil content on manufacturing history

Oil Removal by Nitric Acid Passivation
0
10
20
30
40
50
60
70
Control Passivation Only
Res
idua
l Oil
Con
tent
[mg]
A SeriesK SeriesAIK Series
1 hour soak in 27 vol.% nitric acid
• Nitric acid passivation does not remove measurable quantities of oil

Histopathology of Tissue from 113 InterOp Shells
• Acute and chronic inflammation in periprosthetic tissue, with an abundance of lymphocytes, granulation tissue, neutrophils, and giant cells. Staining was highly positive for IL-1b and Il-6 activity [1].
• Inflammation was found in the capsule as well, and was not therefore relegated to tissue in direct contact with the device.
• Concluded that a substance in the oil, rather than the oil itself, was responsible for the inflammation [1, 2].
1. Campbell, P.M., J; Catelas, I. Examination of Recalled Inter-Op Acetabular Cups for Cause of Failure. in Society for Biomaterials. 2002. Tampa, FL.2. Campbell, P.M., J; Catelas, I. Histopathology of tissues from Inter-Op acetabular sockets. in 48th Annual Meeting of the Orthopaedic Research Society. 2002.

3 Week Rabbit Study
Tissue response in rabbits injected with Oil I
Tissue response in InterOppatients
Acute Inflammation No Yes
Chronic Inflammation 82.1% Extensive
Eosinophils 96.4% Minimal
Giant Cells 14.3% Abundant
Fibrunous Exudate No Yes
Lipogranuloma 82.1% No
Granulation Tissue No Abundant
Lipid Droplets 46.4% No
Metal No Yes
Other Foreign Body 3.6% Yes
Fibrous Tissue 42.9% Yes
Necrosis 3.6% Yes
Only 2 pathological markers were shared in the two studies
Bloebaum, R.D., E.L. Whitaker, J. Szakacs, and A. Hofmann. The tissue response to an injection of gamma sterilized mineral oil in rabbits. in 49th Annual Meeting of the Orthopaedic Research Society. 2003. New Orleans, LA.

Nitric Acid + Oil
-0.1
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
10001100120013001400150016001700180019002000
w avenum ber [cm -1]
abso
rban
ce [A
.U.]
residue-top layer (primarily oil)residue-bottom layer (primarily acid)oil A
removed
new
removed
• There is a modest chemical change in the oil with exposure to acid• GC/MS analysis on residues was inconclusive•Cytotoxicity testing on the residues came back negative

Could Endotoxins be the culprit?• Histopathology of endotoxins produced a similar tissue response as
that observed in the Inter-Op tissue [1].
• Nitric acid passivation can reduce the levels of endotoxins adhered to titanium samples [2].
• Endotoxins were found in the sump water of the machine shop
• Trace amounts could be stationed at the oil-tissue interface, enough to prevent osseointegration
a lipopolysaccharide (LPS) produced from Gram-negative bacteria
1. Greenfield, E.M., Y. Bi, A.A. Ragab, V.M. Goldberg, J.L. Nalepka, and J.M. Seabold, Does endotoxin contribute to aseptic loosening of orthopedic implants? J. Biomed. Mater Res, Part B: Appl. Biomater., 2005. 72B: p. 179-185.2. Merritt, K., S.A. Brown, and V.M. Hitchins. Ability of nitric acid or acetone to inactivate bacterial lipopolysaccharide (LPS). in 28th Annual Meeting Transactions of the Society for Biomaterials. 2002

Conclusion of Case I Study
• Oil present on all manufactured lots tested, including those with successful outcomes
– Specific manufacturing history associated with failed implants
• Explanation of clinical response
– not related to absolute level of oil
– appears to be related to nitric acid passivation step
• Most likely culprit was an adherent endotoxin that was delivered via the oil, and was not inactivated by nitric acid passivation

Case Study II: Residue Identification
• What manufacturing residues are introduced?
– Release agents
– Lubricants/coolants
– Polishing compounds
– Cleaning agents
– Particulate debris
– Eluants from packaging
– Chemicals from gloves
• Identification allows the manufacturer to identify and control the source of the residue production

Further Identification of Residues
Analytical techniques
– FTIR indicates quantity of oil, but not identity
• Sum of all parts
– Soluble residue: Gas Chromatography/Mass Spectroscopy
– Insoluble residue: Energy dispersive spectroscopy (EDS)

GC/MS Analysis of Residues
• Catalogued all compounds that may have come into contact with machined components
• Identified which residue composition was present on component
• Identify what manufacturing step introduces residueRoughing Pump Oil approximatechemical composition concentration %octadecane 1nonadecane 11-hentetracontanol 11-chloro-octadecane 1117-pentatriacontene 17(1-butylhecadecyl)-cyclohexane 191-octadecanethiol 6(2-hexyloctyl)-cyclopentane 9N-methyl-N-[4-[4-methoxyl-1-hexahydropridyl]-2-butynyl]-acetamide 71',4 dihydroxy-2,3' dimethyl-, (-)-[1,2'-binaphthalene]-5,5',8,8'-tetrone 251-docosene 3
*GC/FID: approx. 1-10 ppm

Insoluble Residue
• Scanning Electron Microscopy
• Energy Dispersive X-ray Spectroscopy (EDS or EDXA)
– Qualitative/semi-quantitative
– particulate matter adhered to carbon tape, then analyzed in Phillips XL-30 FEG SEM.

EDS Analysis of Extracted Residue
vanadium titanium
10 microns
silica iron sodium

Conclusions to Case II
• Manufacturers have techniques to identify type of residue
• Source of residue in manufacturing process

Case Study III: Residue on Explants
• Can we extract and identify manufacturing residues on explanted devices?
• Possibly identify source of implant failure

Explant Analysis
• Problem: biological tissue are hydrocarbon-based
• Look very similar to hydrocarbon-based manufacturing residues under FTIR
O
O
C C
H
H
C
H
H
H
H
H
O
O
C CH
H
CH
H
HH
O
O
C C
H
H
C
H
H
HCH
C
C
H
10
10
10
triglyceride
-1
-0.5
0
0.5
1
1.5
2
2.5
3
3.5
4
24002500260027002800290030003100320033003400
wavenum ber [cm -1]
abso
rban
ce [A
.U.]
oillipids
H-C Stretch
H
H
C
H
H
HCC
H
H
H 10
mineraloil

Explant Analysis
• Remove lipids from solution
• Protocol similar to shelf-stored analysis
– Sonication with carbon tetrachloride
– Evaporation
– Filtration
• Isolates manufacturing hydrocarbons from lipids and most other biological residues
– infra-red analysis

Explant Analysis
Pre-doped devices extracted in presence of 5 grams of acetabular tissue
0
10
20
30
40
50
60
70
80
90
shell 1 shell 2
oil c
onte
nt [m
g]
Applied amountMeasured amountno filtration

Cadaver Analysis
• Shells were doped with known amounts of oil, then placed in cadavers for 24 hours
• Extraction, then filtration

Cadaver Analysis
Cadaver Specimens
0
5
10
15
20
25
30
35
40
45
az197 az198 az199 az200 az201
oil c
onte
nt [m
g]
0
500
1000
1500
2000
2500
3000
3500
4000
4500
resi
due
mas
s [m
g]
0
5
10
15
20
25
30
35
40
45
az197 az198 az199 az200 az201
oil c
onte
nt [m
g]
0
500
1000
1500
2000
2500
3000
3500
4000
4500
resi
due
mas
s [m
g]
ir-measurementApplied oilresidue content-gravimetric
0
5
10
15
20
25
30
35
40
45
az197 az198 az199 az200 az201
oil c
onte
nt [m
g]
0
500
1000
1500
2000
2500
3000
3500
4000
4500
resi
due
mas
s [m
g]
ir-measurementApplied oilresidue content-gravimetric

Identification of Extracted Residue from Explant
• FTIR provides limited information on structure of hydrocarbons– Data provided from labs that show hydrocarbons on all explants
(3000 cm-1)– Immediately conclude that these are manufacturing residues– Presence of carbonyls indicate these are probably fatty acids (1700
cm-1)– Systemic long-chain hydrocarbons(1,2)
• GC/MS identifies specific composition of hydrocarbons
1. Liber, A.F. and H.G. Rose, Saturated hydrocarbons in follicular lipidosis of the spleen. Arch. Path., 1967. 83: p. 116-122.2. Rose, H.G. and A.F. Liber, Accumulation of saturated hydrocarbons in human spleens. J. Lab. & Clin. Med., 1966. 68(3): p. 475-483.

GC/MS on Explant Residues
Nitrazepam: sleep medication
Fenclofenac: non-steroidal anti-inflammatory drug
TricoseneTranylcypromine: is a non-hydrazine monoamine oxidase inhibitor, an antidepressant and antimanic (brand name Parnate)

Elemental Analysis of Explants
• Manufacturing residue and tissue analysis directly on explant
• Scanning electron microscopy/Energy dispersive spectroscopy
• No damage to explant (non-destructive)

Elemental Analysis of Explants

Case III: Explant Analysis Summary
• Validated techniques to quantify manufacturing hydrocarbon content
• Residue composition can be analyzed with GC/MS
• Surface residue can be analyzed directly on devices
• Tissue composition can be identified (elements)

How Clean is Clean Enough?
• Determined by:– Analytical detection limits– Achievable with commercial cleaning
processes– Cost of cleaning
• Not possible to remove all residue– Levels that do not elicit an adverse
biological response• Application area in the body• Size of device

ASTM Activities• ASTM activities on cleanliness issues of
medical devices (F04.15.17)
– Passed first standard on assessing cleanliness (ASTM F2459)
– WK15532: Guide for Assessment of Contamination and Residues on Medical devices
• Compilation of known assays for residues, including endotoxins
– WK13292: Standard Practice/Guide for Shipping Possibly Infectious Materials, Tissues, and Fluids

Conclusions
• Acceptable levels?
Good historical success of medical device = acceptable levels of residues

Acknowledgements
• Dr. Gavin Braithwaite• Dr. Orhun Muratoglu• Denise Saltojanes• Partial funding from Sulzer Orthopedics
Visit our web site www.campoly.com for downloadable application notes and presentations