Embed Size (px)
Citation preview
637
Cross-leg free muscle flaps for reconstruction of open fractures of the tibia
P. D. Hodgkinson, M. Andhoga, G. R. Wilson and N. R. McLean Department of Plastic and Reconstructive Surgery, Newcastle General Hospital, Newcastle upon Tyne, UK
In fwo patients in whom the injured leg was not suitable for reconsfruction using a routine free tissue fransfer, a cross-leg free muscle flap was used, i.e. the vessels of a free muscle flap were anastomosed to donor vessels on the uninjured leg and the muscle flap used to reconstruct a defect on the opposite leg. Both operations were successful, with the transferred muscle becoming well vascularized from the recipient bed at the site of injury. In both cases, we of the uninjured leg to transfer the free flap caused minimal morbidity.
Injury, 1994, Vol. 25,637-640, December
Introduction
It is generally accepted that severe open tibial fractures (Gustilo grade IIIB) require flap reconstruction. Local flaps are not reliable enough to be used in the acute phase (Small and Mollan, 1992) and even some time after the injury an appropriate and safe local flap may not be available. Successful wound closure, using the microvascular transfer of free muscle flaps soon after the injury, was described by Godina (1986). This has now become the ‘gold standard’ of treatment in many centres and further reports from France1 et al. (1992) and Small and Mollan (1992) have shown excellent results from similar early treatment. Occasionally the injured leg is not suitable for either a local flap or a microvascular anastomosis, particularly in the presence of major vessel damage where direct anastomosis to the local vasculature may endanger the survival of the foot.
In their major series France1 et al. (1992) have shown that reconstruction should be performed within 15 days of injury for the best results. However, many patients still present late to the reconstructive surgeon, often after multiple local procedures and prolonged periods of bedrest. By this stage there may be chronic osteomyelitis and absent superficial venous drainage in the required site of vessel anastomosis, in combination with deep venous thrombosis, and this may endanger the potential survival of the transferred tissue or necessitate the use of long-vein grafts. In these cases the alternatives are a cross-leg flap or amputation. If amputation is to be avoided and the former option is chosen, a ‘traditional’ cutaneous, fasciocutaneous or muscle cross-leg flap raised on the uninjured leg may create a substantial donor site defect and cause further anxiety to the patient.
0 1994 Butterworth-Heinemann Ltd 0020-1383/94/100637-04
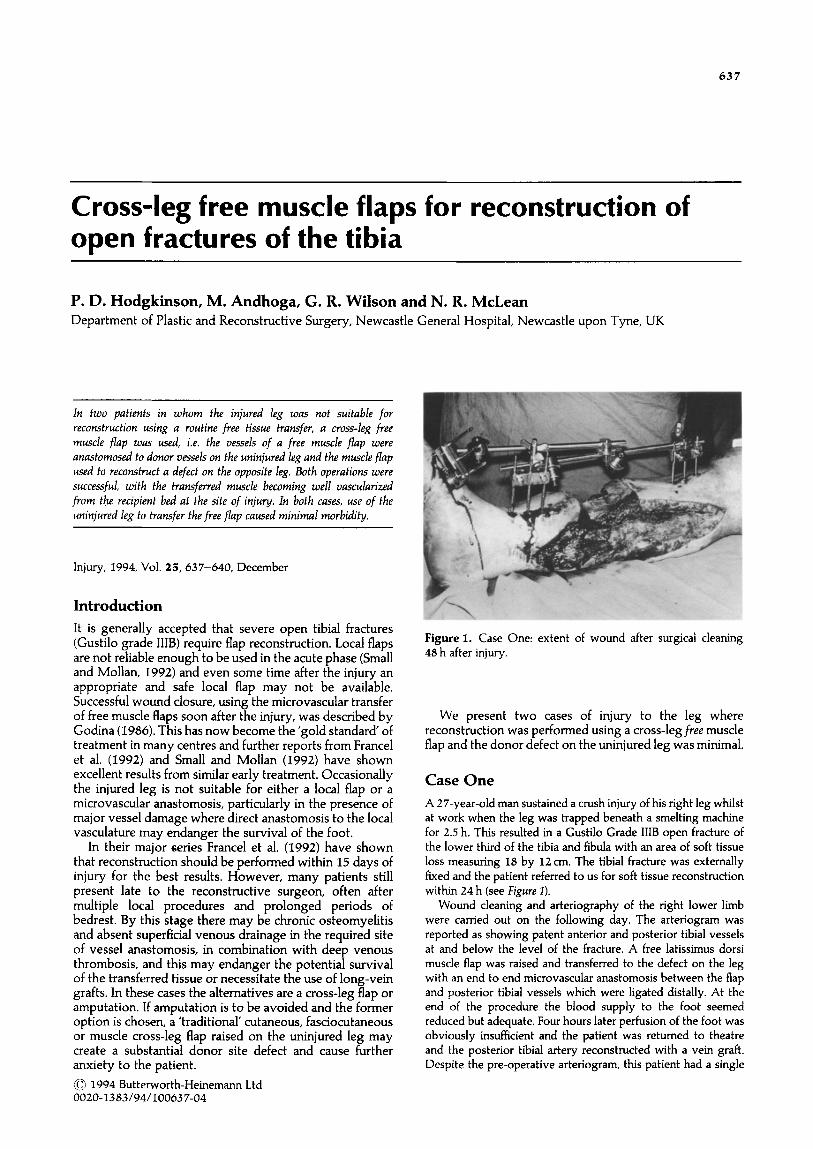
Figure 1. Case One: extent of wound after surgical cleaning
48 h after injury.
We present two cases of injury to the leg where reconstruction was performed using a cross-leg free muscle flap and the donor defect on the uninjured leg was minimal.
Case One
A 27-year-old man sustained a crush injury of his right leg whilst at work when the leg was trapped beneath a smelting machine for 2.5 h. This resulted in a Gustilo Grade IIIB open fracture of the lower third of the tibia and fibula with an area of soft tissue loss measuring 18 by 12cm. The tibia1 fracture was externally fixed and the patient referred to us for soft tissue reconstruction within 24 h (see Figure I).
Wound cleaning and arteriography of the right lower limb were carried out on the following day. The arteriogram was reported as showing patent anterior and posterior tibia1 vessels at and below the level of the fracture. A free latissimus dorsi muscle flap was raised and transferred to the defect on the leg with an end to end microvascular anastomosis between the flap and posterior tibia1 vessels which were ligated distally. At the end of the procedure the blood supply to the foot seemed reduced but adequate. Four hours later perfusion of the foot was obviously insufficient and the patient was returned to theatre and the posterior tibia1 artery reconstructed with a vein graft. Despite the pre-operative arteriogram, this patient had a single

638 Injury: International Journal of the Care of the Injured (1994) Vol. 25/No. 10
arterial supply to the foot. Attempts to revascularize the muscle flap were abandoned.
Ten days later the opposite latissimus dorsi was raised and this time the flap vessels were anastomosed to the posterior tibia1 vessels of the uninjured limb. These vessels were exposed through a posteriorly based flap just above the ankle, so designed that the microvascular anastomoses would be covered by this skin flap posteriorly and the muscle flap anteriorly (see Figttre2). The muscle flap was covered by split thickness skin graft. The two legs were fixed together using external skeletal fixation and cross-bracing of both tibiae.
Intermittent cross-clamping of the flap using a soft bowel clamp was commenced at 4 weeks. After 7 days of increasing
duration of clamping, and presumed intermittent vascular occlu-
sion, the vascular pedicle was ligated under local anaesthetic. This was followed a week later by division of the muscle and healed skin graft bridge, inset of the flap and removal of the external fixation frame. One week later the patient was transfer- red back to the care of the orthopaedic surgeons with all wounds
healed (see Figure 3). Review at 3 months showed that all the wounds were well
Figure 2. Case One: cross-leg free flap in situ showing the small inset for microvascular anastomosis on the uninjured leg (top right) and the large flap inset on the injured leg (left side of picture).
Figure 3. Case One: muscle flap after division of pedicle and inset covered by well healed skin graft and small donor defect on other leg (very bottom of picture).
healed and stable. Unfortunately the tibia1 fracture remained ununited and bone grafting was performed via a posterior approach without difficulty.
Case Two
A 17-year-old man sustained a fracture of the pelvis, right femur and right tibia in a high-speed motor-cycle accident. The tibia1 fracture was open with an 8 by 8 cm area of skin loss in the lower third of the leg. Fasciotomies of the right calf were performed at the receiving hospital, as well as external fixation of the pelvic, femoral and tibia1 fractures. Split thickness skin grafting of all wounds was performed subsequently. The tibia1 wound and fasciotomy wounds became infected and the graft was lost. The patient was transferred to our care for soft tissue reconstruction some 10 days after the injury. Over the next 10 days his wounds were excised and regrafted, apart from the area of exposed tibia1 fracture (see Figures 4 and 5). Arteriography was performed, and demonstrated patent anterior and posterior tibia1 vessels beyond the fracture, although both appeared compressed. It was felt that the long and short saphenous veins had been lost at the time of the fasciotomies and there was a high probability of thrombosis within the deep venous system.
At operation, a free rectus muscle flap was raised on the inferior epigastric vessels. The posterior tibia1 artery and long saphenous vein were exposed in the uninjured leg just above the
Figure 4. Case Two: lower limb wounds on medial side at time of first cleaning after transfer to our care - open fracture is the most inferior wound on the anteromedial shin.
Figure 5. Case Two: close-up of open fracture.
Hodgkinson et al.: Cross-leg free muscle flaps 639
ankle by raising a posteriorly based flap as before, and an end-to-end microvascular anastomosis was performed. The legs were fixed together using external skeletal fixation, the rectus
muscle flap was laid into the defect on the right leg and the exposed muscle bridge covered with split thickness skin graft.
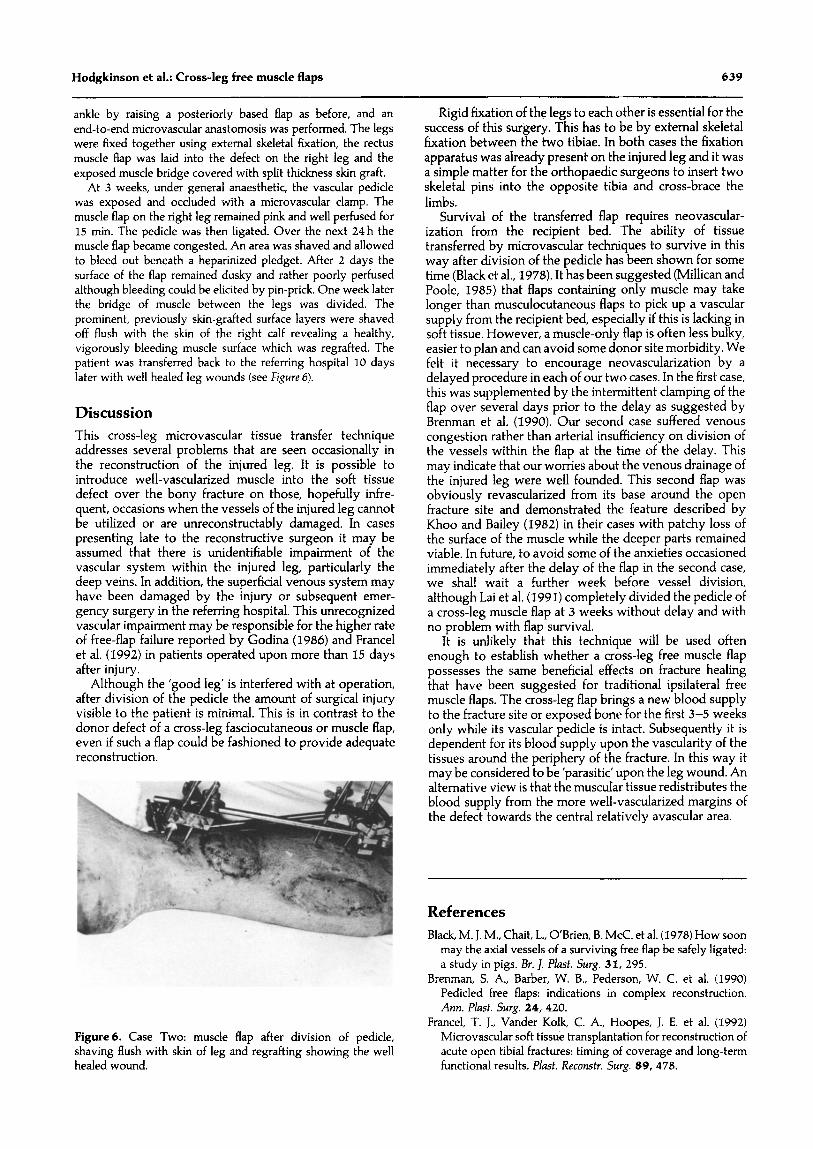
At 3 weeks, under general anaesthetic, the vascular pedicle was exposed and occluded with a microvascular clamp. The muscle flap on the right leg remained pink and well perfused for 15 min. The pedicle was then ligated. Over the next 24 h the muscle flap became congested. An area was shaved and allowed to bleed out beneath a heparinized pledget. After 2 days the surface of the flap remained dusky and rather poorly perfused although bleeding could be elicited by pin-prick. One week later the bridge of muscle between the legs was divided. The prominent, previously skin-grafted surface layers were shaved off flush with the skin of the right calf revealing a healthy, vigorously bleeding muscle surface which was regrafted. The patient was transferred back to the referring hospital 10 days later with well healed leg wounds (see Figure 6).
Discussion
This cross-leg microvascular tissue transfer technique addresses several problems that are seen occasionally in the reconstruction of the injured leg. It is possible to introduce well-vascularized muscle into the soft tissue defect over the bony fracture on those, hopefully infre- quent, occasions when the vessels of the injured leg cannot be utilized or are unreconstructably damaged. In cases presenting late to the reconstructive surgeon it may be assumed that there is unidentifiable impairment of the vascular system within the injured leg, particularly the deep veins. In addition, the superficial venous system may have been damaged by the injury or subsequent emer- gency surgery in the referring hospital. This unrecognized vascular impairment may be responsible for the higher rate of free-flap failure reported by Godina (1986) and France1 et al. (1992) in patients operated upon more than 15 days after injury.
Although the ‘good leg’ is interfered with at operation, after division of the pedicle the amount of surgical injury visible to the patient is minimal. This is in contrast to the donor defect of a cross-leg fasciocutaneous or muscle flap, even if such a flap could be fashioned to provide adequate reconstruction.
Figure6. Case Two: muscle flap after division of pedicle, shaving flush with skin of leg and regrafting showing the well healed wound.
Rigid fixation of the legs to each other is essential for the success of this surgery. This has to be by external skeletal fixation between the two tibiae. In both cases the fixation apparatus was already present on the injured leg and it was a simple matter for the orthopaedic surgeons to insert two skeletal pins into the opposite tibia and cross-brace the limbs.
Survival of the transferred flap requires neovascular- ization from the recipient bed. The ability of tissue transferred by microvascular techniques to survive in this way after division of the pedicle has been shown for some time (Black et al., 1978). It has been suggested (Millican and Poole, 1985) that flaps containing only muscle may take longer than musculocutaneous flaps to pick up a vascular supply from the recipient bed, especially if this is lacking in soft tissue. However, a muscle-only flap is often less bulky, easier to plan and can avoid some donor site morbidity. We felt it necessary to encourage neovascularization by a delayed procedure in each of our two cases. In the first case, this was supplemented by the intermittent clamping of the flap over several days prior to the delay as suggested by Brenman et al. (1990). Our second case suffered venous congestion rather than arterial insufficiency on division of the vessels within the flap at the time of the delay. This may indicate that our worries about the venous drainage of the injured leg were well founded. This second flap was obviously revascularized from its base around the open fracture site and demonstrated the feature described by Khoo and Bailey (1982) in their cases with patchy loss of the surface of the muscle while the deeper parts remained viable. In future, to avoid some of the anxieties occasioned immediately after the delay of the flap in the second case, we shall wait a further week before vessel division, although Lai et al. (1991) completely divided the pedicle of a cross-leg muscle flap at 3 weeks without delay and with no problem with flap survival.
It is unlikely that this technique will be used often enough to establish whether a cross-leg free muscle flap possesses the same beneficial effects on fracture healing that have been suggested for traditional ipsilateral free muscle flaps. The cross-leg flap brings a new blood supply to the fracture site or exposed bone for the first 3-5 weeks only while its vascular pedicle is intact. Subsequently it is dependent for its blood supply upon the vascularity of the tissues around the periphery of the fracture. In this way it may be considered to be ‘parasitic’ upon the leg wound. An alternative view is that the muscuIar tissue redistributes the blood supply from the more well-vascularized margins of the defect towards the central relatively avascular area.
References
Black, M. J. M., Chait, L., O’Brien, B. McC. et al. (1978) How soon may the axial vessels of a surviving free flap be safely ligated: a study in pigs. Br. 1. Plasf. Surg. 31, 295.
Brenman, S. A., Barber, W. B., Pederson, W. C. et al. (1990) Pedicled free flaps: indications in complex reconstruction. Ann. Plast. Surg. 24, 420.
Francel, T. J., Vander Kolk, C. A., Hoopes, J. E. et al. (1992) Microvascular soft tissue transplantation for reconstruction of acute open tibia1 fractures: timing of coverage and long-term functional results. P&f. Recmstr. Surg. 89, 478.

640 Injury: International Journal of the Care of the Injured (1994) Vol. 25/No. 10
Godina, M. (1986) Early microsurgical reconstruction of com- plex trauma of the extremities. Plust. Reconstr. Surg. 78, 285.
Khoo, C. T. K. and Bailey, B. N. (1982) The behaviour of free muscle and musculocutaneous flaps after early loss of axial blood supply. Br. 1. Plast. Surg. 35,~.
IA C-S., Lin S-D., Chou C-K. et al. (1991) Use of a cross-leg free muscle flap to reconstruct an extensive burn wound involving a lower extremity. Burns 17, 510.
Millican, P. G. and Poole, M. D. (1985) Peripheral neovascular- isation of muscle and musculocutaneous flaps. Br. J PZast. Surg. 38,369.
Small J. 0. and Mollan R. A. B. (1992) Management of the soft tissues in open tibial fractures. Br. J. PZusf. Swg. 45, 571.
Paper accepted 9 June 1994.
Requests for reprinfs shod be addressed to: Peter D. Hodgkinson, Senior Registrar in Plastic Surgery, Welsh Centre for Bums and Plastic Surgery, Morriston Hospital, Morriston, Swansea SA6 6NL, UK.





























