Embed Size (px)
Citation preview

IEEE TRANSACTIONS ON INFORMATION TECHNOLOGY IN BIOMEDICINE, VOL. 16, NO. 1, JANUARY 2012 31
Cross-Layer Ultrasound Video Streaming OverMobile WiMAX and HSUPA Networks
Ali Alinejad, Student Member, IEEE, Nada Y. Philip, Member, IEEE,and Robert S. H. Istepanian, Senior Member, IEEE
Abstract—It is well known that the evolution of 4G-based mo-bile multimedia network systems will contribute significantly tofuture mobile healthcare (m-health) applications that require highbandwidth and fast data rates. Central to the success of suchemerging applications is the compatibility of broadband networks,such as mobile Worldwide Interoperability For Microwave Access(WiMAX) and High-Speed Uplink Packet Access (HSUPA), andespecially their rate adaption issues combined with the acceptablereal-time medical quality of service requirements. In this paper,we address the relevant challenges of cross-layer design require-ments for real-time rate adaptation of ultrasound video streamingin mobile WiMAX and HSUPA networks. A comparative perfor-mance analysis of such approach is validated in two experimentalm-health test bed systems for both mobile WiMAX and HSUPAnetworks. The experimental results have shown an improved per-formance of mobile WiMAX compared to the HSUPA using thesame cross-layer optimization approach.
Index Terms—Cross-layer design, e-health, High-Speed UplinkPacket Access (HSUPA), mobile broadband, mobile healthcare (m-health), mobile Worldwide Interoperability For Microwave Access(WiMAX), wireless telemedicine.
I. INTRODUCTION
MOBILE healthcare (m-health) is an evolving paradigmthat brings together the evolution of emerging wireless
communications and network technologies with the concept of“connected healthcare” anytime and anywhere [1].
In recent years, the extensive volume of research work anddevelopments in areas of 4G multimedia networks has not beenreflected in parallel work dedicated to 4G-based m-health sys-tems. The recent advances in broadband mobile networks haveresulted in the development of several new multimedia applica-tions based on these emerging technologies. However, in com-parison, the 4G-based m-health domain and medical broadbandapplications have received less attention compared to other areasin m-health. Real-time mobile ultrasound streaming and med-
Manuscript received December 10, 2010; revised March 9, 2011; acceptedMay 1, 2011. Date of publication May 12, 2011; date of current versionFebruary 3, 2012. This work was supported by Islamic Azad University,Islamshahr Branch, Iran, and OxfordBranch, U.K., and by the British Coun-cil the Development Partnerships in Higher Education Programme (DelPHE)and UK-India Education and Research Initiative (UKIERI).
A. Alinejad is with the Islamic Azad University, Islamshahr Branch,Islamshahr, Iran, and Oxford Branch, Oxford, OX29 4DA, U.K., andalso with the Mobile Information and Network Technologies Centre,Kingston University, London, KT1 2EE, U.K. (e-mail: [email protected],[email protected]).
N. Y. Philip and R. S. H. Istepanian are with the Mobile Information andNetwork Technologies Centre, Kingston University, London, KT1 2EE, U.K.(e-mail: [email protected]; [email protected]).
Color versions of one or more of the figures in this paper are available onlineat http://ieeexplore.ieee.org.
Digital Object Identifier 10.1109/TITB.2011.2154384
ical diagnostics are considered one such evolving broadbandm-health application that has major clinical benefits for differ-ent telemedical scenarios. For example, the use of such servicesfor providing expert real-time diagnostics in remote areas, suchas in developing countries, is vital for enhancing healthcare ser-vices in these regions. However, these emerging wireless com-munications and network technologies need to be further vali-dated and tested especially from the medical quality of service(m-QoS) perspective and their adaptability to clinical and real-time diagnostics constraints and conditions. The concept of m-QoS is defined in an earlier work as the “Augmented require-ments of critical mobile health care applications with respect tothe traditional wireless Quality of Service (QoS) requirements”[2]. In general, the provision of diagnostically acceptable end-to-end m-QoS requirements will become an important factor forWorldwide Interoperability For Microwave Access (WiMAX)and High-Speed Downlink Packet Access/High-Speed Up-link Packet Access (HSDPA/HSUPA) networks especially fortheir potential acceptability for bandwidth demanding m-healthapplications.
It is well known that optimized m-QoS enhancement for adap-tive medical video streaming is one of the key factors for suchend-to-end diagnostically acceptable services. There are severalrelevant works that address the issues of video streaming in mul-timedia networks [3]–[5]. It is well known that the IEEE 802.16e(mobile WiMAX) standard aims to provide broadband connec-tivity to mobile users in wireless metropolitan area networkenvironments [6]. This standard can provide great potential fordifferent m-health applications that require higher operationaldata rates with clinically acceptable remote diagnostic qualityand potential cost-effective solutions [7]. On the other hand,the recent deployment of HSUPA systems represents an en-hancement of earlier Wideband Code Division Multiple Access(W-CDMA) networks with a higher data rate, improved spectralefficiency, and greater system capacity to provide improved con-nectivity conditions for robust m-health applications. Further-more, the recent developments in Long Term Evolution (LTE)are another path toward 4G systems that will be deployed in thenext four years. The focus of this paper is on the current deploy-able networks in this evolution process. To date, there is no studythat compares the end-to-end broadband m-health solutions us-ing an optimized cross-layer design (CLD) approach for mobileWiMAX and HSUPA networks. The need to develop such anapproach with adaptable characteristics to the available networkstreaming conditions whilst providing an acceptable m-QoSs inreal-time conditions is key to any successful 4G m-health appli-cations. To achieve this, we present a new cross-layer approachbased on a reinforcement learning (CRL) algorithm for real-timemedical video streaming for both mobile WiMAX and HSUPA
1089-7771/$26.00 © 2011 IEEE
32 IEEE TRANSACTIONS ON INFORMATION TECHNOLOGY IN BIOMEDICINE, VOL. 16, NO. 1, JANUARY 2012
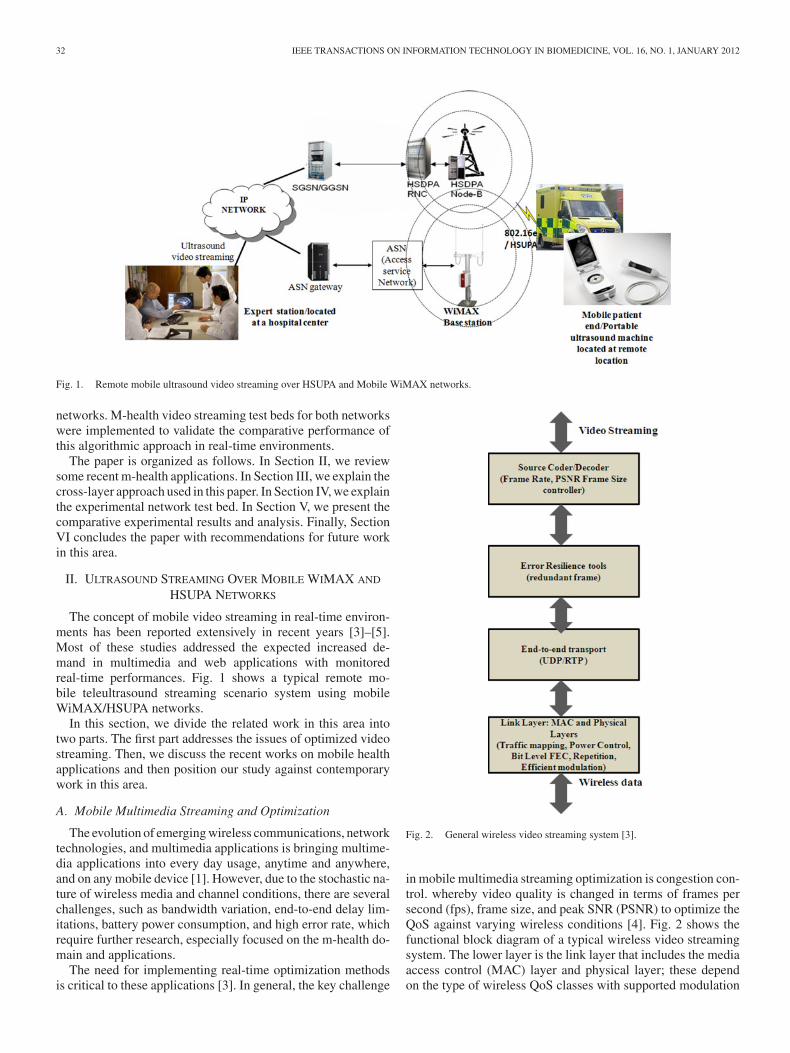
Fig. 1. Remote mobile ultrasound video streaming over HSUPA and Mobile WiMAX networks.
networks. M-health video streaming test beds for both networkswere implemented to validate the comparative performance ofthis algorithmic approach in real-time environments.
The paper is organized as follows. In Section II, we reviewsome recent m-health applications. In Section III, we explain thecross-layer approach used in this paper. In Section IV, we explainthe experimental network test bed. In Section V, we present thecomparative experimental results and analysis. Finally, SectionVI concludes the paper with recommendations for future workin this area.
II. ULTRASOUND STREAMING OVER MOBILE WIMAX AND
HSUPA NETWORKS
The concept of mobile video streaming in real-time environ-ments has been reported extensively in recent years [3]–[5].Most of these studies addressed the expected increased de-mand in multimedia and web applications with monitoredreal-time performances. Fig. 1 shows a typical remote mo-bile teleultrasound streaming scenario system using mobileWiMAX/HSUPA networks.
In this section, we divide the related work in this area intotwo parts. The first part addresses the issues of optimized videostreaming. Then, we discuss the recent works on mobile healthapplications and then position our study against contemporarywork in this area.
A. Mobile Multimedia Streaming and Optimization
The evolution of emerging wireless communications, networktechnologies, and multimedia applications is bringing multime-dia applications into every day usage, anytime and anywhere,and on any mobile device [1]. However, due to the stochastic na-ture of wireless media and channel conditions, there are severalchallenges, such as bandwidth variation, end-to-end delay lim-itations, battery power consumption, and high error rate, whichrequire further research, especially focused on the m-health do-main and applications.
The need for implementing real-time optimization methodsis critical to these applications [3]. In general, the key challenge
Fig. 2. General wireless video streaming system [3].
in mobile multimedia streaming optimization is congestion con-trol. whereby video quality is changed in terms of frames persecond (fps), frame size, and peak SNR (PSNR) to optimize theQoS against varying wireless conditions [4]. Fig. 2 shows thefunctional block diagram of a typical wireless video streamingsystem. The lower layer is the link layer that includes the mediaaccess control (MAC) layer and physical layer; these dependon the type of wireless QoS classes with supported modulation

ALINEJAD et al.: CROSS-LAYER ULTRASOUND VIDEO STREAMING OVER MOBILE WiMAX AND HSUPA NETWORKS 33
and coding schemes. Layers 2 and 3 prepare end-to-end con-nectivity and extra error resilience approaches. The upper layeris used to decode/encode video streaming and has rate controlto provide optimal video traffic [5], [8]. Since making a deci-sion in one layer sometimes affects QoS parameters in otherlayers, in this situation, one system so-called cross layer can bein charge of making a decision or giving a QoS solution. Hence,the cross-layer approach is used to combine the parameters andmechanisms at different layers optimally to find a solution forimproved QoS support at given network dynamics and limitedresources [9]. A summary of the different cross-layer approachesused in mobile multimedia systems is presented in Section III.
B. 3.5G/WiMAX Mobile Health Systems
In recent years, numerous works have addressed m-healthsystems and applications. A detailed review of these can befound in [10]. However, two critical issues need to be consideredfor any future 4G-based m-health systems.
1) The future networks are required to provide an effectiveand very accurate diagnosis and remote analysis, espe-cially with bandwidth demanding services such as real-time teleultrasonography applications. It is well knownthat the evolution of mobile telecommunication systemsfrom 3G to LTE technology will facilitate the provisionof such faster data transfer rates and high quality videostreaming.
2) The QoS issues and their guarantee to provide reliable4G m-health services with clinically acceptable qualityalso need to be considered. For 4G-based m-health sys-tems to be accepted clinically, especially by healthcare ser-vices, these must provide the end users (patients, health-care providers) with an acceptable diagnostic quality fromthe doctors and clinical end perspective.
In general, m-health applications can be categorized as real-time applications and nonreal-time applications. Real-time ap-plications include transfer of electrocardiography, blood pres-sure, oxygen saturation, medical images, and medical videodata. Nonreal-time m-health applications include access to ad-ministrative files and electronic health records, access to drugstore data bases, queries to medical report warehouses, etc. [11],[12].
However, different m-health scenarios such as emergencytelemedicine, mobile patient monitoring, mobile medical data,mobile robotic system, posthospital care, teleconsultation col-laborative, and medical information management services needspecific QoS indices. These applications are summarized inTable I and described elsewhere [7], [11].
Historically, the first generation of wireless communicationtechnology aimed to provide analogue voice services, the secondgeneration aimed to provide digital voice services, the thirdgeneration aimed to provide mobile multimedia services, andthe fourth generation aims to provide high data rate serviceswith reliable broadband communication systems [13], [14].
The introduction of 3.5G or HSDPA represented the en-hancement of W-CDMA networks with higher data transferspeeds, improved spectral efficiency, and greater system capac-ity [15]. With a theoretical downlink peak of 14.4 Mb/s (typ-ically around 1.4 Mb/s) and an uplink of 384 kb/s, emerging
TABLE IM-HEALTH SERVICE QOS REQUIREMENTS [7], [11]
TABLE IIWIMAX QOS PARAMETERS IN DIFFERENT CLASSES [22]
m-health systems can benefit from these downlink data transferspeeds that were previously only feasible on wired communica-tion networks. HSUPA is the 3G Partnership Project (3GPP’s)release 6, introduced in 2006 to improve the uplink data rate ofHSDPA, and offers an enhanced data rate, fast packet retrans-mission mechanisms, and reduced packet latencies with an up-link data rate up to a theoretical maximum of 5.6 Mb/s [16].
From the QoS perspective, the 3GPP defines four generalQoS classes [3], [17]: conversational, streaming, background,and interactive. The main QoS parameters that are consideredin High Speed Packet Access networks are guaranteed bit rate(GBR), scheduling priority indicator, and discard timer (DT).
The streaming traffic class has a higher priority than the back-ground and interactive classes; all streaming connections shouldbe served prior to all interactive connections, and GBR can be setaccording to the required bit rate. DT is the maximum delay timein Node-B and it is set based on the QoS requirements [3], [18].
The other wireless network technology, Mobile WiMAX, isbased on the IEEE 802.16e standard [19], [20]. The objectiveof the Mobile WiMAX standard is to fill the gap between thewireless LANs (which provide a very high data rate with short-range coverage) and the 3G cellular systems (that provide highlymobile long-range coverage but a low data rate) [21].
In general, IEEE 802.16 has five QoS service classes, clas-sified as follows [22]: Unsolicited Grant Scheme, Real-TimePolling Service (rtPS), Extended rtPS, Non rtPS, and BestEffort.
Table II compares the different WiMAX QoS service classes[22].
In this paper, we consider the m-QoS issues in terms of imagequality (PSNR), frame rate, frame size, and end-to-end delay tovalidate the performance of the two networks from the perspec-tive of these parameters. The relevant details of m-QoS conceptare described elsewhere [2].

34 IEEE TRANSACTIONS ON INFORMATION TECHNOLOGY IN BIOMEDICINE, VOL. 16, NO. 1, JANUARY 2012
Fig. 3. Different cross-layer approaches. (a) Top down. (b) Bottom up. (c) Ap-plication centric. (d) MAC centric. (e) Integrated [23], [24].
III. OPTIMIZED CLD FOR MEDICAL VIDEO STREAMING
In this section, we describe briefly the different CLD cate-gories used in wireless video streaming. Further details on thistopic are detailed in [22]–[24]. We then describe the Q-learningapproach used in the CLD and applied to the medical videostreaming.
A. Wireless Cross-Layer Adaption Scheme
The CLD refers to protocol and model architecture design,which exploit the dependence between layers to obtain optimumgains. This is not against the layering concepts; actually it isan attached model to the open system interconnection OSI)model [22].
Cross-layer systems use different models and algorithms thatdepend on the architecture that is being used in such imple-mentation. In this part, we are going to review the cross-layerarchitectures and choose one particular model that fits best forthe medical scenario.
In general, cross-layer systems perform three major tasks:data abstracting, optimizing, and reconfiguration. Abstractionand reconfiguration strictly depend on the system model and theinteraction between the layers, and optimization algorithms andprotocols are used for allocating the optimal solution. The mostsignificant cross-layer models are shown as follows [23].
1) Top-Down Approach: Fig. 3(a) shows a top-down ap-proach: in this model, the upper layers dictate the QoS strategyto the lower layers; in other words, the optimizer takes a decisionbased upon the application’s QoS requirements to reconfigurethe MAC layer, and consequently, the optimizer reconfigures thephysical layer to provide the required service to the MAC layer.However, this model has been used in most existing systemsand the implementation is relatively simple; it cannot guaranteefinding the best solution.
2) Bottom-Up Approach: This model is shown in Fig. 3(b):in this approach, the optimizer is trying to insulate the upperlayers from the lower layers’ service variations. The optimizerconfigures the upper layers based on lower layer states to mini-mize the side effect of lower layer variations. For example, theapplication’s parameters will be set according to the MAC layerstatus.
3) Application-Centric Approach: In this model, the opti-mizer, which is located in the application layer, reconfigureslayers in a top-down (or bottom-up) manner, based on the ap-plication layer requirements. However, this model, due to theslower rate of changes in the upper layers rather than the lowerlayers, cannot be adapted for the real time changes within thelower layers. This model is shown in Fig. 3(c).
4) MAC-Centric Approach: Fig. 3(d) shows the MAC-centric approach: this model is similar to the application-centricmodel; the application layer provides its requirements and statesto the MAC layer, and the MAC layer optimizes its own param-eters, and consequently, optimizes the physical layer accordingto data abstracted from the physical layer. This model has afaster reaction time than the application-centric approach.
5) Integrated Approach: Fig. 3(e) shows the integrated ap-proach: this model takes an optimal decision based on all infor-mation, parameters, and requirements, which are received fromthe different layers. Despite other approaches, all layers cansend their required quality, and there is not only a unique layerto dictate the quality to the other layers.
Therefore, this model should provide different requirementsfor different layers; this makes this approach the best suit-able method for the current application. However, this approachneeds a real-time optimization method to provide the optimallayer values.
In general, a cross layer can add computation complexitiesfor finding the optimal QoS strategy because the number ofQoS strategies is increasing in comparison to layer architecture.Formulas (1)–(3) show this fact [25]
SLayerd =∑
Li ∈L
SLi(1)
SCL = ΠLi ∈LSLi. (2)
Then
SLayerd ≤ SCL (3)
where SLayerd and SCL are QoS strategies in layered and cross-layer architecture, respectively, L is set of the layers, and Li isith layer. In this paper, for decreasing real-time computationalcomplexity, we use a RL algorithm.
B. Problem Formulation and the Q-Learning Approach
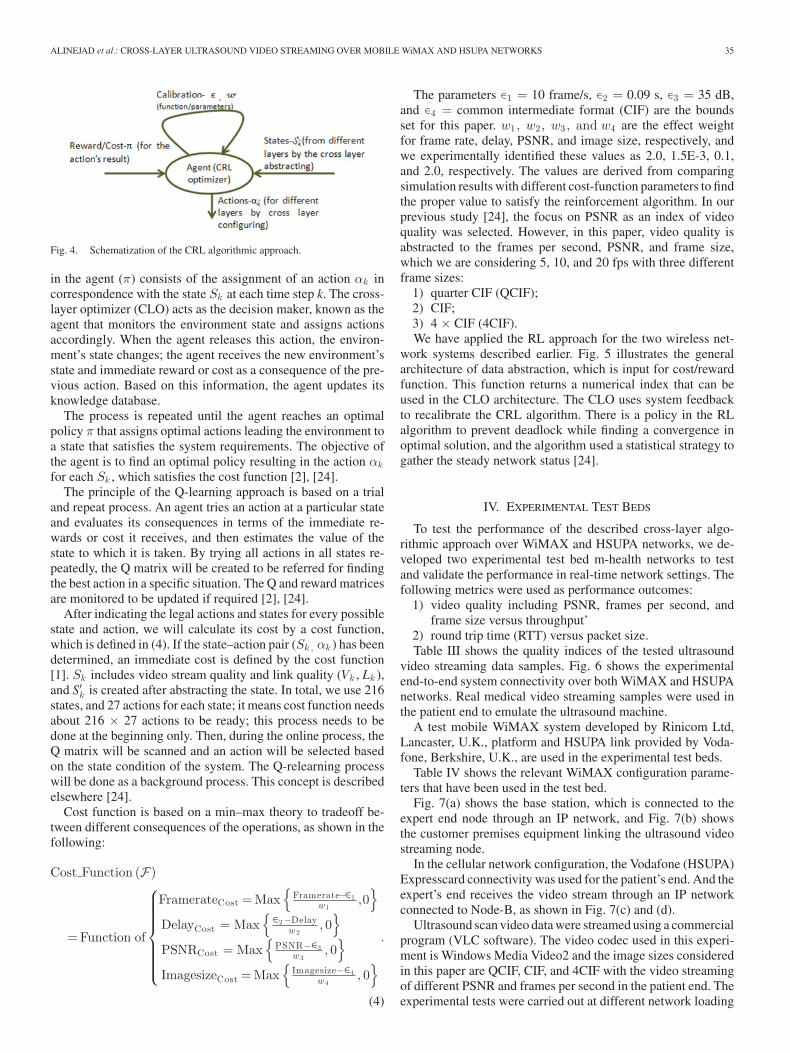
As explained in the earlier section, we adopted the use ofQ-learning as an RL method to find the best action for dif-ferent cross-layer parametric variations. In this approach, RLagents learn how to act so as to maximize a numerical rewardsignal. The process of optimizing in cross layer is based on adiscrete-time Markov decision process, which is a stochasticprocess modeled by a finite number of states S. For each stateS, a finite set of actions A is possible. By selecting the actionαk ∈ A at the time step k, we incur a cost/reward c(Sk , αk ).The schematization of this method is shown in Fig. 4. A policy
ALINEJAD et al.: CROSS-LAYER ULTRASOUND VIDEO STREAMING OVER MOBILE WiMAX AND HSUPA NETWORKS 35
Fig. 4. Schematization of the CRL algorithmic approach.
in the agent (π) consists of the assignment of an action αk incorrespondence with the state Sk at each time step k. The cross-layer optimizer (CLO) acts as the decision maker, known as theagent that monitors the environment state and assigns actionsaccordingly. When the agent releases this action, the environ-ment’s state changes; the agent receives the new environment’sstate and immediate reward or cost as a consequence of the pre-vious action. Based on this information, the agent updates itsknowledge database.
The process is repeated until the agent reaches an optimalpolicy π that assigns optimal actions leading the environment toa state that satisfies the system requirements. The objective ofthe agent is to find an optimal policy resulting in the action αk
for each Sk , which satisfies the cost function [2], [24].The principle of the Q-learning approach is based on a trial
and repeat process. An agent tries an action at a particular stateand evaluates its consequences in terms of the immediate re-wards or cost it receives, and then estimates the value of thestate to which it is taken. By trying all actions in all states re-peatedly, the Q matrix will be created to be referred for findingthe best action in a specific situation. The Q and reward matricesare monitored to be updated if required [2], [24].
After indicating the legal actions and states for every possiblestate and action, we will calculate its cost by a cost function,which is defined in (4). If the state–action pair (Sk , αk ) has beendetermined, an immediate cost is defined by the cost function[1]. Sk includes video stream quality and link quality (Vk , Lk ),and S′k is created after abstracting the state. In total, we use 216states, and 27 actions for each state; it means cost function needsabout 216 × 27 actions to be ready; this process needs to bedone at the beginning only. Then, during the online process, theQ matrix will be scanned and an action will be selected basedon the state condition of the system. The Q-relearning processwill be done as a background process. This concept is describedelsewhere [24].
Cost function is based on a min–max theory to tradeoff be-tween different consequences of the operations, as shown in thefollowing:
Cost Function (F)
= Function of
⎧⎪⎪⎪⎪⎪⎪⎨
⎪⎪⎪⎪⎪⎪⎩
FramerateCost = Max{
Framerate−∈1w 1
,0}
DelayCost = Max{∈2 −Delay
w 2, 0
}
PSNRCost = Max{
PSNR−∈3w 3
, 0}
ImagesizeCost = Max{
Imagesize−∈4w 4
, 0}
.
(4)
The parameters ∈1 = 10 frame/s, ∈2 = 0.09 s, ∈3 = 35 dB,and ∈4 = common intermediate format (CIF) are the boundsset for this paper. w1 , w2 , w3 , and w4 are the effect weightfor frame rate, delay, PSNR, and image size, respectively, andwe experimentally identified these values as 2.0, 1.5E-3, 0.1,and 2.0, respectively. The values are derived from comparingsimulation results with different cost-function parameters to findthe proper value to satisfy the reinforcement algorithm. In ourprevious study [24], the focus on PSNR as an index of videoquality was selected. However, in this paper, video quality isabstracted to the frames per second, PSNR, and frame size,which we are considering 5, 10, and 20 fps with three differentframe sizes:
1) quarter CIF (QCIF);2) CIF;3) 4 × CIF (4CIF).We have applied the RL approach for the two wireless net-
work systems described earlier. Fig. 5 illustrates the generalarchitecture of data abstraction, which is input for cost/rewardfunction. This function returns a numerical index that can beused in the CLO architecture. The CLO uses system feedbackto recalibrate the CRL algorithm. There is a policy in the RLalgorithm to prevent deadlock while finding a convergence inoptimal solution, and the algorithm used a statistical strategy togather the steady network status [24].
IV. EXPERIMENTAL TEST BEDS
To test the performance of the described cross-layer algo-rithmic approach over WiMAX and HSUPA networks, we de-veloped two experimental test bed m-health networks to testand validate the performance in real-time network settings. Thefollowing metrics were used as performance outcomes:
1) video quality including PSNR, frames per second, andframe size versus throughput’
2) round trip time (RTT) versus packet size.Table III shows the quality indices of the tested ultrasound
video streaming data samples. Fig. 6 shows the experimentalend-to-end system connectivity over both WiMAX and HSUPAnetworks. Real medical video streaming samples were used inthe patient end to emulate the ultrasound machine.
A test mobile WiMAX system developed by Rinicom Ltd,Lancaster, U.K., platform and HSUPA link provided by Voda-fone, Berkshire, U.K., are used in the experimental test beds.
Table IV shows the relevant WiMAX configuration parame-ters that have been used in the test bed.
Fig. 7(a) shows the base station, which is connected to theexpert end node through an IP network, and Fig. 7(b) showsthe customer premises equipment linking the ultrasound videostreaming node.
In the cellular network configuration, the Vodafone (HSUPA)Expresscard connectivity was used for the patient’s end. And theexpert’s end receives the video stream through an IP networkconnected to Node-B, as shown in Fig. 7(c) and (d).
Ultrasound scan video data were streamed using a commercialprogram (VLC software). The video codec used in this experi-ment is Windows Media Video2 and the image sizes consideredin this paper are QCIF, CIF, and 4CIF with the video streamingof different PSNR and frames per second in the patient end. Theexperimental tests were carried out at different network loading
36 IEEE TRANSACTIONS ON INFORMATION TECHNOLOGY IN BIOMEDICINE, VOL. 16, NO. 1, JANUARY 2012
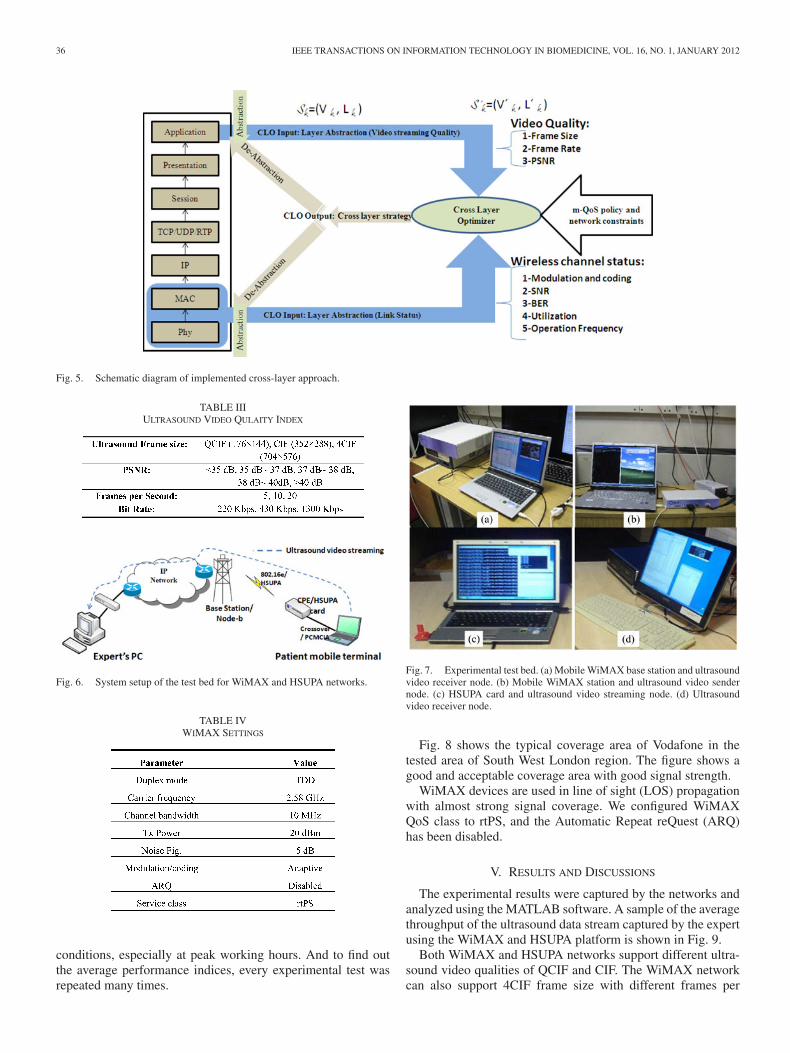
Fig. 5. Schematic diagram of implemented cross-layer approach.
TABLE IIIULTRASOUND VIDEO QULAITY INDEX
Fig. 6. System setup of the test bed for WiMAX and HSUPA networks.
TABLE IVWIMAX SETTINGS
conditions, especially at peak working hours. And to find outthe average performance indices, every experimental test wasrepeated many times.
Fig. 7. Experimental test bed. (a) Mobile WiMAX base station and ultrasoundvideo receiver node. (b) Mobile WiMAX station and ultrasound video sendernode. (c) HSUPA card and ultrasound video streaming node. (d) Ultrasoundvideo receiver node.
Fig. 8 shows the typical coverage area of Vodafone in thetested area of South West London region. The figure shows agood and acceptable coverage area with good signal strength.
WiMAX devices are used in line of sight (LOS) propagationwith almost strong signal coverage. We configured WiMAXQoS class to rtPS, and the Automatic Repeat reQuest (ARQ)has been disabled.
V. RESULTS AND DISCUSSIONS
The experimental results were captured by the networks andanalyzed using the MATLAB software. A sample of the averagethroughput of the ultrasound data stream captured by the expertusing the WiMAX and HSUPA platform is shown in Fig. 9.
Both WiMAX and HSUPA networks support different ultra-sound video qualities of QCIF and CIF. The WiMAX networkcan also support 4CIF frame size with different frames per
ALINEJAD et al.: CROSS-LAYER ULTRASOUND VIDEO STREAMING OVER MOBILE WiMAX AND HSUPA NETWORKS 37
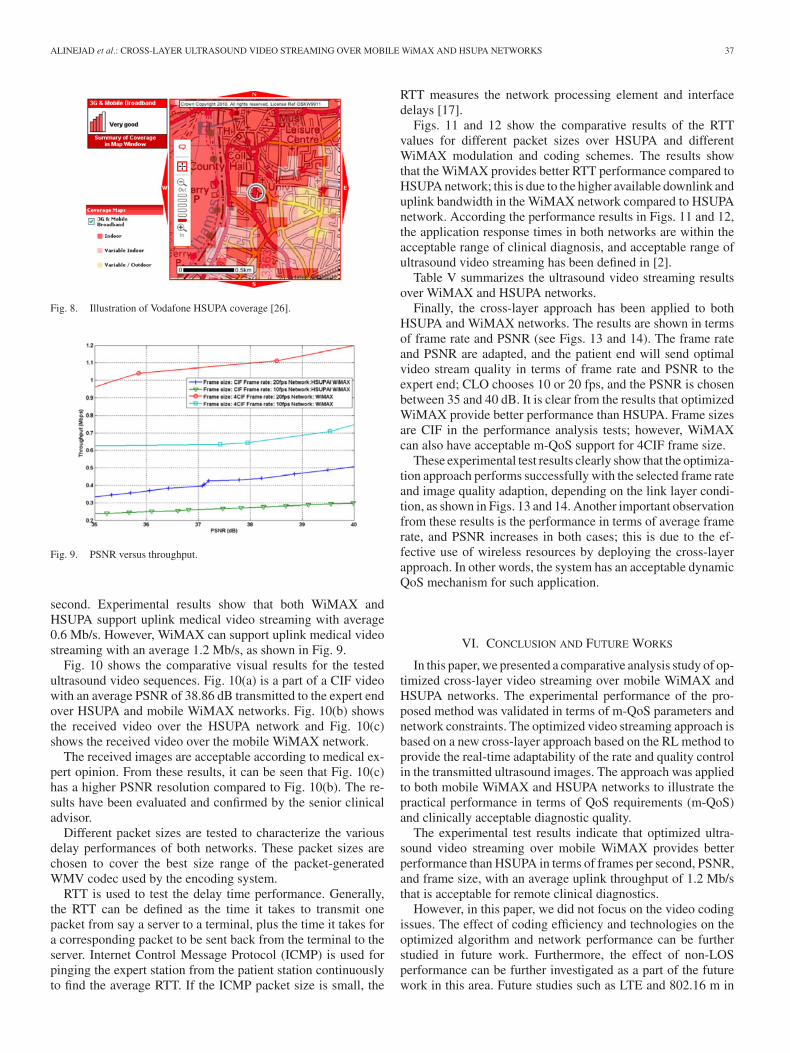
Fig. 8. Illustration of Vodafone HSUPA coverage [26].
Fig. 9. PSNR versus throughput.
second. Experimental results show that both WiMAX andHSUPA support uplink medical video streaming with average0.6 Mb/s. However, WiMAX can support uplink medical videostreaming with an average 1.2 Mb/s, as shown in Fig. 9.
Fig. 10 shows the comparative visual results for the testedultrasound video sequences. Fig. 10(a) is a part of a CIF videowith an average PSNR of 38.86 dB transmitted to the expert endover HSUPA and mobile WiMAX networks. Fig. 10(b) showsthe received video over the HSUPA network and Fig. 10(c)shows the received video over the mobile WiMAX network.
The received images are acceptable according to medical ex-pert opinion. From these results, it can be seen that Fig. 10(c)has a higher PSNR resolution compared to Fig. 10(b). The re-sults have been evaluated and confirmed by the senior clinicaladvisor.
Different packet sizes are tested to characterize the variousdelay performances of both networks. These packet sizes arechosen to cover the best size range of the packet-generatedWMV codec used by the encoding system.
RTT is used to test the delay time performance. Generally,the RTT can be defined as the time it takes to transmit onepacket from say a server to a terminal, plus the time it takes fora corresponding packet to be sent back from the terminal to theserver. Internet Control Message Protocol (ICMP) is used forpinging the expert station from the patient station continuouslyto find the average RTT. If the ICMP packet size is small, the
RTT measures the network processing element and interfacedelays [17].
Figs. 11 and 12 show the comparative results of the RTTvalues for different packet sizes over HSUPA and differentWiMAX modulation and coding schemes. The results showthat the WiMAX provides better RTT performance compared toHSUPA network; this is due to the higher available downlink anduplink bandwidth in the WiMAX network compared to HSUPAnetwork. According the performance results in Figs. 11 and 12,the application response times in both networks are within theacceptable range of clinical diagnosis, and acceptable range ofultrasound video streaming has been defined in [2].
Table V summarizes the ultrasound video streaming resultsover WiMAX and HSUPA networks.
Finally, the cross-layer approach has been applied to bothHSUPA and WiMAX networks. The results are shown in termsof frame rate and PSNR (see Figs. 13 and 14). The frame rateand PSNR are adapted, and the patient end will send optimalvideo stream quality in terms of frame rate and PSNR to theexpert end; CLO chooses 10 or 20 fps, and the PSNR is chosenbetween 35 and 40 dB. It is clear from the results that optimizedWiMAX provide better performance than HSUPA. Frame sizesare CIF in the performance analysis tests; however, WiMAXcan also have acceptable m-QoS support for 4CIF frame size.
These experimental test results clearly show that the optimiza-tion approach performs successfully with the selected frame rateand image quality adaption, depending on the link layer condi-tion, as shown in Figs. 13 and 14. Another important observationfrom these results is the performance in terms of average framerate, and PSNR increases in both cases; this is due to the ef-fective use of wireless resources by deploying the cross-layerapproach. In other words, the system has an acceptable dynamicQoS mechanism for such application.
VI. CONCLUSION AND FUTURE WORKS
In this paper, we presented a comparative analysis study of op-timized cross-layer video streaming over mobile WiMAX andHSUPA networks. The experimental performance of the pro-posed method was validated in terms of m-QoS parameters andnetwork constraints. The optimized video streaming approach isbased on a new cross-layer approach based on the RL method toprovide the real-time adaptability of the rate and quality controlin the transmitted ultrasound images. The approach was appliedto both mobile WiMAX and HSUPA networks to illustrate thepractical performance in terms of QoS requirements (m-QoS)and clinically acceptable diagnostic quality.
The experimental test results indicate that optimized ultra-sound video streaming over mobile WiMAX provides betterperformance than HSUPA in terms of frames per second, PSNR,and frame size, with an average uplink throughput of 1.2 Mb/sthat is acceptable for remote clinical diagnostics.
However, in this paper, we did not focus on the video codingissues. The effect of coding efficiency and technologies on theoptimized algorithm and network performance can be furtherstudied in future work. Furthermore, the effect of non-LOSperformance can be further investigated as a part of the futurework in this area. Future studies such as LTE and 802.16 m in

38 IEEE TRANSACTIONS ON INFORMATION TECHNOLOGY IN BIOMEDICINE, VOL. 16, NO. 1, JANUARY 2012
Fig. 10. Ultrasound images PSNR 38.86. (a) Original image. (b) Received image over HSUPA network. (c) Received image over Mobile WiMAX network.
Fig. 11. RTT results of different ultrasound video stream packet sizes overWiMAX.
Fig. 12. RTT results of different ultrasound video stream packet sizes overHSUPA.
TABLE VPERFORMANCE RESULTS OVER MOBILE WIMAX AND HSUPA
Fig. 13. Frame rate comparison of optimized WiMAX and HSUPA.
Fig. 14. PSNR comparison of optimized WiMAX and HSUPA networks.
m-health applications are also ongoing as part of this researchstudy.
ACKNOWLEDGMENT
The authors would like to thank Dr. N. Amso from CardiffUniversity Medical School for his medical advice and for pro-viding the relevant medical images and ultrasound video data.The authors are also grateful to Vodafone R&D, Mr. NigelJefferies, and Rinicom Ltd., for their equipment support to thispaper.
ALINEJAD et al.: CROSS-LAYER ULTRASOUND VIDEO STREAMING OVER MOBILE WiMAX AND HSUPA NETWORKS 39
REFERENCES
[1] R. S. H. Istepanian, E. Jovanov, and Y. T. Zhang, “M-health: Beyondseamless mobility for global wireless healthcare connectivity—Editorial,”IEEE Trans. Inf. Technol. Biomed., vol. 8, no. 4, pp. 405–414, Dec.2004.
[2] R. S. H. Istepanian, N. Philip, and M. G. Martini, “Medical QoS provi-sion based on reinforcement learning in ultrasound streaming over 3.5Gwireless systems,” IEEE J. Sel. Areas Commun., Piscataway, NJ: IEEEPress, vol. 27, no. 4, pp. 566–574, May 2009.
[3] M. Etoh and T. Yoshimura, “Advances in wireless video delivery,” Proc.IEEE, vol. 93, no. 1, pp. 111–122, Jan. 2005.
[4] G. Cheung, W. Tan, and T. Yoshimura, “Real-time video transport opti-mization using streaming agent over 3G wireless networks,” IEEE Trans.Multimedia, vol. 7, no. 4, pp. 777–785, Aug. 2005.
[5] S. Chemiakina, L. Antonio, F. Forti, R. Lallo, J. Peterson, and A. Terzani,“QoS enhancement for adaptive streaming services over WCDMA,”IEEE J. Sel. Areas Commun., vol. 21, no. 10, pp. 1575–1584, Dec.2003.
[6] Y. Zhang and H. Chen, Mobile WiMAX: Toward Broadband WirelessMetropolitan Area Networks. New York: CRC Press, 2008.
[7] D. Niyato, E. Hossain, and J. Diamond, “IEEE 802.16/WiMAX-basedbroadband wireless access and its application for telemedicine/e-healthservices,” IEEE Wireless Commun., vol. 14, no. 1, pp. 72–83, Feb.2007.
[8] M. Alasti, B. Neekzad, J. Hui, and R. Vannithamby, “Quality of servicein WiMAX and LTE networks,” IEEE Commun. Mag., vol. 48, no. 5,pp. 104–111, May 2010.
[9] Q. Zhang and Y.-Q. Zhang, “Cross-layer design for QoS support in mul-tihop wireless networks,” Proc. IEEE, vol. 96, no. 1, pp. 64–76, Jan.2008.
[10] E. Guainella, E. Borcoci, M. Katz, P. Neves, M. Curado, F. Andreotti, andE. Angori, “WiMAX technology support for applications in environmen-tal monitoring, fire prevention and telemedicine,” in Proc. IEEE MobileWiMAX Symp., Mar., 2007, pp. 125–131.
[11] D. Komnakos, D. Vouyioukas, I. Maglogiannis, and P. Constantinou1,“Performance evaluation of an enhanced uplink 3.5G system for mobilehealthcare applications,” Int. J. Telemed. Appl., vol. 2008. pp. 1–11,(Article ID 417870).
[12] A. Zvikhachevskaya, G. Markarian, and L. Mihaylova, “Quality of serviceconsideration for the wireless telemedicine and e-health services,” in Proc.IEEE Wireless Commun. Netw. Conf., Budapest, Hungary, Apr. 2009,pp. 1–6.
[13] B. Fong A. C. M. Fong, P. B. Rapajic, and G. Y. Hong, “Mobiletelemedicine for accident and emergency scenes in tropical regions,”WSEAS Trans. Commun., vol. 2, pp. 361–364, Oct. 2003.
[14] L. Chin-Feng, “Mobile telemedicine: A survey study,” J. Med. Syst.,vol. 2, pp. 1–10, 2010.
[15] 3GPP TS 25.308 V5.4.0 (2002–10) High Speed Downlink Packet Access(HSDPA) Stage 2—Release 5.
[16] N. Hallam-Baker, “Challenges of the evolving 3G technology,” Aeroflex,Hertfordshire, U.K., 2006.
[17] H. Holma and A. Toskala, Eds., HSDPA/HSUPA for UMTS, 1st ed. NewYork: Wiley, 2006.
[18] C. Johnson, Radio Access Networks for UMTS. New York: Wiley, 2008.[19] S. J. Vaughan-Nichols, “Achieving wireless broadband with WiMAX,”
IEEE Comp., vol. 37, no. 6, pp. 10–13, Jun. 2004.[20] S. M. Cherry, “WiMAX and Wi-Fi: Separate and unequal,” IEEE Spec-
trum, vol. 41, no. 3, pp. 18–22, Mar. 2004.[21] K. H. Teo, Z. Tao, and J. Zhang, “The mobile broadband WiMAX stan-
dard,” IEEE Signal Process. Mag., vol. 24, no. 5, pp. 144–148, Sep.2007.
[22] K. Chen and J. Roberto B. De Marca, MobileWiMAX. New York: Wiley,2008.
[23] S. Van Der and S. N. Sai, “Cross-layer wireless multimedia transmission:Challenges, principles, and new paradigms,” IEEE Wireless Commun.,vol. 12, no. 4, pp. 50–58, 1536–1284, 2005.
[24] A. Alinejad, N. Philip, and R. S. H. Istepanian, “Reinforcement learningalgorithm for optimised cross layer medical video streaming over WiMAXnetworks,” in Proc. 7th Int. Symp. Commun. Syst., Netw. Digit. SignalProcess., Newcastle upon Tyne, U.K, 2010, pp. 862–866.
[25] S. Milani and G. Calvagno, “A low-complexity cross-layer optimizationalgorithm for video communication over wireless networks,” IEEE Trans.Multimedia, vol. 11, no. 5, pp. 810–821, Aug. 2009.
[26] Vodafone.[Online].Available:http://www.vodafone.co.uk/personal/price-plans/network-and-coverage/ uk-coverage-map/ [accessed 2010, Oct. 10].
Ali Alinejad (S’10) is currently working toward thePh.D. degree in the Faculty of Computing, Informa-tion System and Mathematics, Kingston University,London, U.K.
Since 2003, he has been a Lecturer at Islamic AzadUniversity, Islamshahr Branch, Islamshahr, Iran. Hiscurrent research interests include broadband wirelessaccess, m-health, and cross layer.
Mr. Alinejad is a member of the Mobile Infor-mation and Network Technologies Research Centre(MINT), Kingston University, and a student member
of the IEEE Engineering in Medicine and Biology Society.
Nada Y. Philip (M’05) received the Ph.D. degreefrom the Faculty of Computing, Information Sys-tem and Mathematics, Kingston University, London,U.K., in 2008.
She is currently a Lecturer at Kingston Univer-sity, where she is also a research staff with the Mo-bile Information and Network Technologies ResearchCentre (MINT). She is also Honorary Tutor at St.George’s University of London, London. She is theauthor or coauthor of more than 20 journal and confer-ence papers. Her research interests include data com-
munication, networking and information technology in healthcare, and medicalapplications.
Dr. Philip is a member of the Institute of Engineering Technology.
Robert S. H. Istepanian (SM’96) received the Ph.D.degree from the Department of Electronic and Electri-cal Engineering, Loughborough University, Leices-tershire, U.K., in 1994.
He is currently a Professor of Data Communi-cations at Kingston University, London, where he isalso the founder and Director of the Mobile Infor-mation and Network Technologies Research Centre(MINT) Since then, he has held several academicand research academic posts in U.K. and Canadaincluding senior lectureships in the Universities of
Portsmouth, Portsmouth, U.K., and Brunel University, Middlesex, U.K. Hewas also an Associate Professor in the University of Ryerson, Toronto, ON,Canada, and an Adjunct Professor at the University of West Ontario, ON. He iswidely recognized as the founder of the concept of mobile health (m-health). Hewas the 2008 Leverhulme distinguished Visiting Fellow at the Centre for Globale-health Innovation, University of Toronto, Toronto, and the University’s HealthNetwork. He is the author or coauthor of more than 170 refereed journal andconference papers, and has edited three books including chapters in the areas ofmobile communications for healthcare, m-health technologies, and biomedicalsignals processing.
Dr. Istepanian is an investigator and coinvestigator of several Engineering andPhysical Sciences Research Council and European Union (UN) research grantson m-health and e-health projects. He leads several EU–Information SocietyTechnologies and e-Ten projects in the areas of mobile healthcare. He was onseveral IEEE Transactions and international journals’ editorial boards includingIEEE TRANSACTION ON INFORMATION TECHNOLOGY IN BIOMEDICINE (1997–2011), IEEE TRANSACTIONS ON NANOBIOSCIENCE, and IEEE TRANSACTIONS
ON MOBILE COMPUTING, and International Journal Of Telemedicine and Appli-cations and Journal of Mobile Multimedia. He was also a Guest Editor of sev-eral special issues of the IEEE Transactions including IEEE TRANSACTIONS ON
INFORMATION TECHNOLOGY IN BIOMEDICINE (on seamless mobility for health-care and m-health systems, 2005) and IEEE TRANSACTIONS OF NANOBIO-SCIENCE (on microarray image processing, 2004). He was the cochairman ofthe United Kingdom/Republic of Ireland chapter of the IEEE Engineering inMedicine and Biology in 2002. He also presented numerous keynote lecturesin international conferences in Europe, Canada, and USA. He was also on thetechnical committee and chaired several national and international conferencesin U.K. (The Institution of Engineering and Technology) and Canada, includingIEEE conferences including the Telemed conferences of the Royal Society ofMedicine, London, the 2000 World Medical Congress, Chicago. and the IEEEEngineering in Medicine and Biology International Annual Conferences (IEEE-EMBS 1997, 1998, 1999, 1906, 2007, and 2008). He is a Fellow of the Instituteof Engineering Technology (formerly IEE). He is also a member on severalexperts and grants review committees including UK (DOM, Wellcome Trust,and BUPA), Canada, Ireland, and USA.





























