Embed Size (px)
Citation preview

Critical Care Nephrology2018
Christoph Schwarz

AGENDA 2018
• Diagnostic Tools – kinetic GFR
• Hemodynamics 1: SPLIT-SALT-LICRA-SMART-SALT-ED
• Hemodynamics 2: Selepressin – Angiotensin II
• Kidney meets Liver
• Acid-Base: Chloride and Gaps
• GOMIC´s
• News

Kinetic GFR - BASIC
eGFR nur bei stabiler Nierenfunktion
kGFR: Berechnung der GFR basierend auf Kreatininänderung über eine bestimmte Zeitperiode (inkl. geschätzte Krea-Generationsrate)
Frage:
Ist die kGFR den AKIN-Kriterien überlegen?
Hat die kGFR einen anderen klinischen Nutzen?

Kinetic GFR vs. eGFR2
0,0
10,0
20,0
30,0
40,0
50,0
60,0
70,0
80,0
0 0,1 0,2 0,3 0,4 0,5 0,6 0,7 0,8 0,9 1 1,1 1,2 1,3 1,4 1,5 1,6 1,7 1,8 1,9
kGFR vs GFR2
KGFR CKD-MDRD 2
Bsp. Mann 70kg, 70 Jahre, Kreatinin-Anstieg um: 0,1-1,9mg/dl in 24 Stunden
delta S-Kreatinin (mg/dl)
GFR
(m
l/m
in)
AKIN 1
AKIN 2
AKIN 3

Kinetic GFR performs better than GFR-MDRD?
Vergleich eGFR-MDRD(1) vs. kGFR
ED O`Sullivan CKJ 2017
kGFR <30ml/min ist ein besserer Prädiktor für eine NET als eine eGFR-MDRD <30ml/min

kGFR + AKIN = ?
de Olivera Marques Critical Care 2017
Outcome bei baseline eGFR >70ml/min
kGFR < 30ml/min additiv prädiktiven Wert fürMortalität (unabh. AKIN)und für Notwendigkeit einerNET (bei AKIN3)

Hemodynamics - BASIC
Personalisierte Hämodynamik – Alter + Co-Morbiditäten
Was sollte gemessen werden?
– Blutdruck (MAP, DAP-CVP)
- Harnmenge
- Sono: Herz, Lunge, Pulswellenvariabilität,….
Wie sollte behandelt werden?
- Flüssigkeit
- Katechoamine
- Vasopressin, Angiotensin II

Effect of Individualized vs Standard Blood Pressure Management Strategies on Postoperative Organ Dysfunction Among High-Risk Patients Undergoing Major Surgery (INPRESS)
Patienten= 298, >50 Jahre, medium-high risk Patienten
elektive abdominelle OP,
Randomisiert: RR±10% präoperativ vs. RR >80 mmHg systol.
Intervention: Noradrenalin
Primärer composite Endpunkt: SIRS oder 1 „Organversagen“Futier E JAMA 2017

Futier E JAMA 2017

Selepressin, a novel selective vasopressin V1A agonist, is an effective substitute for norepinephrine in a phase IIa randomized, placebo-controlled trial in septic shock patients
Selepressin selektiv V1a Rezeptor (kein Effekt auf renalen V2 Rezeptor)
53 Patienten mit septischen Schock unter Noradrenalintherapie erhalten Selepressin vs.Placebo.
Endpoint: MAP > 60mmHg, beenden von Noradrenalin
Ru
ssel
l JA
Cri
tica
l Ca
re 2
01
7

Angiotensin II in shock
ATHOS-3
Indikation: Septischer Schock
Therapie: Noradrenalin >2µg/kg/min + ATII vs. Placebo
Patienten: 344
Primärer Endpunkt: RR 3 Stunden nach Beginn der ATII Therapie
Ziel MAP: in ersten 3h 75 mmHg, danach >65 mmHg
Laurence William Busse KI reports 2017
Khanna A NEJM 2017

ATHOS-3
Khanna A NEJM 2017
Endpunkt nach 3h:Anstieg des RR > 10mmHg oder MAP > 75mmHg:
AT II: 69%Placebo: 23%
SAE: idem
AKIN:4,9% (n=8) vs. 6,3% (n=11)

VolumentherapieSALINE vs. BALANCED SOLUTIONS
Chloride – Volume Therapy
Volumentherapie mit NaCl 0,9% - negative Effekte in vielen retrospektiven (Observations)Studien
Ära der randomisierten prospektiven Studien:
2016: SPLIT – kein Unterschied zwischen NaCl 0,9% und balancedsolutions (Niere und Mortalität)
2017: LICRA und SALT
2018: SMART und SALT-ED
2019: PLUS-Trial

LICRA „Limiting I.V. Chloride to Reduce AKI“
1136 Patienten nach Herz-Chirurgischen Eingriffen
2 Perioden mit Infusion von NaCl 0,9%
2 Perioden mit Infusion von balancierten Lösungen (1xRLA, 1xPlasmalyte)
Endpunkt: delta Kreatinin, Rate an AKIN2 und AKIN3
Ergebnis: kein Unterschied im Outcome (Niere, Mortalität)
McIlroy D; Intensive Care Med 2017

LICRA „Limiting i.v. Chloride to Reduce AKI“
ABER:
Intraoperativ: HLM – mit RLA gefüllt
ca. 50% der Patienten in der NaCl 0,9% Periode erhielten intraoperativ balancierte Lösungen
Postoperativ: Volumengabe: ca. 1500ml
McIlroy D; Intensive Care Med 2017

SALT – „isotonic Solution Administration Logistical Testing“
974 Patienten
– cluster randomized trial
NaCl 0,9% vs. balancierte Lösung
Infusionsmenge nach 7 Tagen:
ca.1300ml
Endpunkt:
MAKE30: kein Unterschied
Semler MW; Am J Respir Crit Care Med 2017
MAKE 30
• In-hospital mortality = Death prior to hospital discharge
• New receipt of RRT = Receipt of any modality of RRT prior to hospital discharge in a patient not known to have received RRT prior to ICU admission.
• Persistent renal dysfunction = Final plasma creatinine value before hospital discharge ≥ 200% of the baseline plasma creatinine value in a patient not known to have received RRT prior to ICU admission.

SMART - Balanced Crystalloids versus Saline in Critically Ill Adults15800 Patienten, NaCl0,9% vs. balanced solution
MAKE 30: Balanced crystalloid group:14.3% vs. saline group = 15.4% (OR 0.91; 95% CI 0.84-0.99)
NNT to avoid one MAKE 30 outcome is 94
Erhaltenes Volumen 1000ml (0-3300ml)
prespecified Subgruppenanalyse:
Sepsispatienten (NNT=20) und Patienten welche größere Mengen an Flüssigkeit erhielten hatten einen größeren Benefit von balancierten Lösungen
Semler MW NEJM 2018
driven by mortality

SALT-ED: Balanced Crystalloids versus Saline in Noncritically Ill Adults13347 Patienten, cross over trial, balanced solution vs. saline, unblinded, Infusionsmenge: in Median 1079 ml
Prim. outcome kein Unterschied
MAKE30: balanced vs. saline: 4.7% vs. 5.6%; OR 0.82 (0.70-0.95 p=0.01)
NNT to avoid one MAKE30 =111
Krea> 1,5mg/dl at admission: MAKE30: 28% vs. 37,6% (p<0.001)
Self WH NEJM 2018
driven by AKI
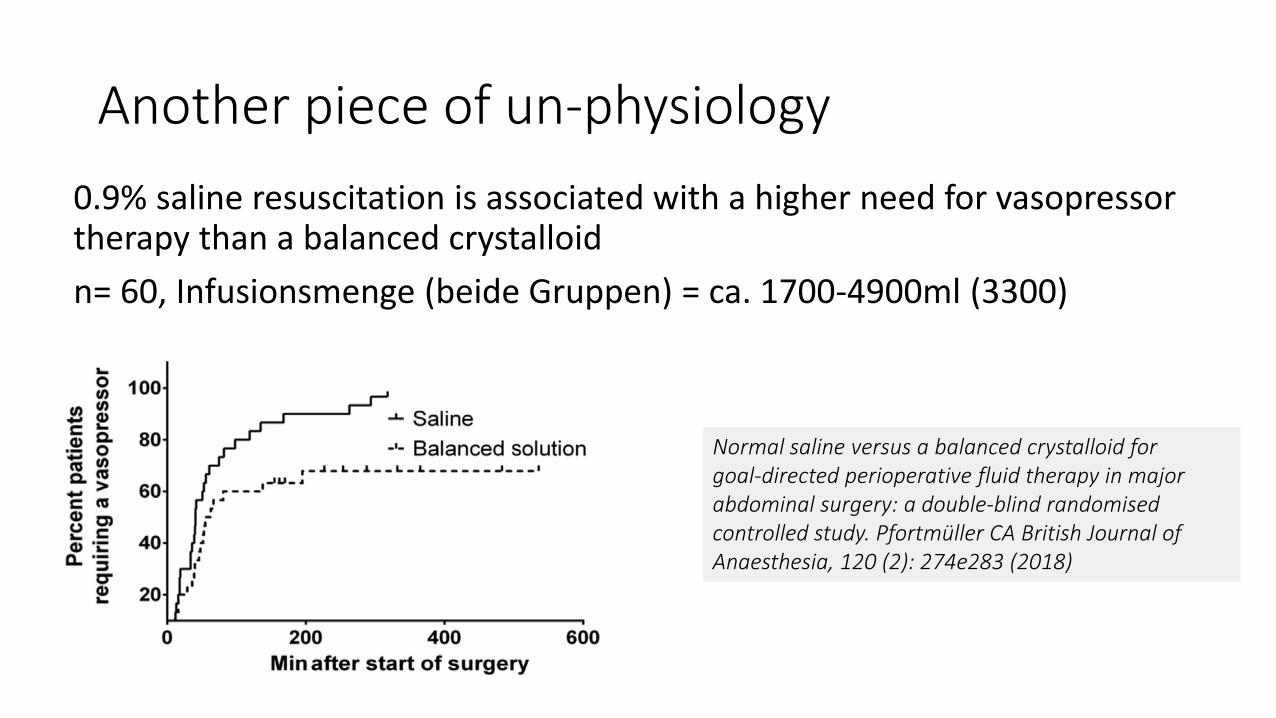
Another piece of un-physiology
0.9% saline resuscitation is associated with a higher need for vasopressor therapy than a balanced crystalloid
n= 60, Infusionsmenge (beide Gruppen) = ca. 1700-4900ml (3300)
Normal saline versus a balanced crystalloid forgoal-directed perioperative fluid therapy in majorabdominal surgery: a double-blind randomisedcontrolled study. Pfortmüller CA British Journal of Anaesthesia, 120 (2): 274e283 (2018)

The SMART and SALT-ED trials are massive, multiple-crossover trials
which compare saline versus balanced crystalloids among critically ill
and non-critical patients. Both studies found a 1% increase in death or
renal failure with the use of saline.
The combination of physiology, animal studies, numerous RCTs,
SMART, and SALT-ED indicate that it's time to stop resuscitating with
saline.
Normal saline is only for metabolic alkalosis
Plasmalyte and RLA are less alkaline than Elomel isoton
https://emcrit.org/pulmcrit/smart/

Chloride in ACID BASE

Kombinierte Störungen des SBHH Delta-Delta?
Chlorid: konstantes Verhältnis zu Na: Na-Cl = 36
Chlorid: inverses Verhältnis zu Bicarbonat: Na-Cl=HCO3 (+AG)
High Anion Gap Acidose:
Delta Bicarbonat – Delta AG = Na-Cl-36
>-6 = mixed high anion gap and normal anion gap metabolic acidosis
-6 to 6 = isolated high anion gap acidosis
>+ 6 = mixed high anion gap acidosis and metabolic alkalosis
Tsapenko, Oman medical journal 28.1 (2013): 73.

Beispiel: Patient mit KADC
BZ: 1368mg/dl,
Na: 134 mmol/l, Cl 85 mmol/l,
pH 7,31, HCO3: 13,4 mmol/l, pCO2: 27 mmHg
PAG: 35,6 mmol/l – deltaAG: 23,6mmol/l
deltaAG-deltaBic = 13 mmol/l
Na-Cl -36= 134-(85+36)= 13mmol/l
Kidney meets Liver

Leber und NiereCLF
A-CLF
AKI-non HRSAKI-HRS
ALF Liver Decompensation
Liver Decompensation
Type AType BType C
mit/ohne Nierenversagen
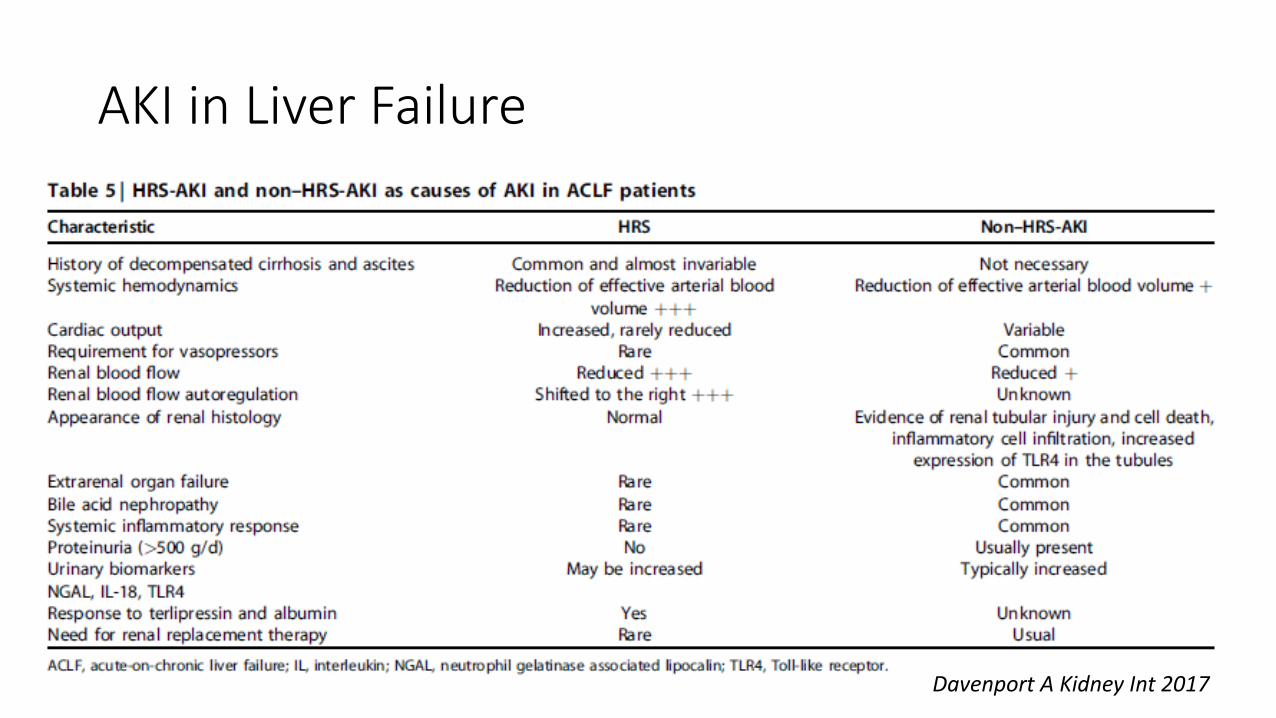
AKI in Liver Failure
Davenport A Kidney Int 2017

Serum copeptin at admission was significantly higher in patients with ACLF compared with those without (33 (14–64) vs. 11 (4–26) pmol/L; p < 0.001)
Kerbert AJ Critical Care 2017

547 akute Dekompensation der Leberzirrhose
290 (53%) AKI
AKIN 1 (n=197)
68%
AKIN 2 (n=55)
19%
AKIN 3 (n=38)
13%
29% *acute on chronic
70% ACLF
AKIN 1A(n=58)
29%
AKIN 1B*(n=139)
71%
Höhere Rate an Progression des AKINHöhere Rate an NETHöhere Rate an ACLFHöheres Stadium ACLF
renal recovery 90% renal recovery 50%
90 day survivalAKIN 1A 84%AKIN 1B 58%AKIN 2 48%AKIN 3 43%
Huelin P Clinical Gastroentereology and Hepatology 2017

Ist der Patient alt oder zu alt für eine ICU?

GOMIC´s- get out of my intensive care?
> 15% der ICU Patienten sind > 80 Jahre1
Hospital Mortality: 20% (vs. 13%)1
Frailty: erhöht das Mortalitätsrisiko (HR 1,54 CI1.38-1.73)2
Welcher ältere Patient soll auf die ICU?
Definierte Vorselektion von Patienten vs. übliche Prozedere:
61% vs. 34% Admission
Kein Einfluss auf Outcome – Hospital Mortality: 30 vs 20%3
1 Karakus A Intensive Care Medicine 20172 Flatten H Intensive Care Medicine 20173 Guidet B JAMA 2017

Nutrition-News
Early goal-directed nutrition versus standard of care in adult intensive care patients: The single-centre, randomised, outcome assessor-blinded EAT-ICU trial.
Eine frühe, hochkalorische Ernährung ist obsolet.
Prof. W. Druml: Nutrition in ICU „early conservative – late liberal“
Allingstrup MJ Intensive Care Med 2017

Pharmakinetic News
Caspofungin – keine Dosisanpassung bei CVVHD (Aguilar G CC 2017)
Meropenem: Bei Standarddosierung 3x1g i.v.:
100%T>MIC was 48.4% MIC values of 2 mg/L100%T>MIC was 20.6% MIC values of 8 mg/L
Meropenemkonzentration steigt mit Reduktion der GFR.
Online Kalkulator zur Evaluierung wie hoch die Wahrscheinlichkeit ist, das der behandelte Patient in Abhängigkeit von Nierenfunktion nicht imBereich der MIC liegt.
Ehmann L Crit Care 2017

Ehmann L Crit Care 2017