Embed Size (px)
Citation preview

Journal of Neurology, Neurosurgery, and Psychiatry, 1976, 39, 1-22
Craniopagus twins: surgical anatomy andembryology and their implications
J. E. A. O'CONNELL1
From the Department of Neurological Surgery, St. Bartholomew's Hospital, London
SYNOPSIS Craniopagus is of two types, partial and total. In the partial form the union is of limitedextent, particularly as regards its depth, and separation can be expected to be followed by the survivalof both children to lead normal lives. In the total form, of which three varieties can be recognized,the two brains can be regarded as lying within a single cranium and a series of gross intracranialabnormalities develops. These include deformity of the skull base, deformity and displacement ofthe cerebrum, and a gross circulatory abnormality. It is considered that these and other abnormalities,unlike the primary defect, which is defined, are secondary ones; explanations for them, based on
anatomy and embryology, are put forward. The implications of the various anomalies are discussedand the ethical aspects of attempted separation in these major unions considered.
The birth of conjoined twins is an infrequentoccurrence. Its incidence is estimated as one in50 000 births (Potter, 1961). The union is acephalic one in 2.0% which makes the incidenceof craniopagus twins one in 2.5 million births.The occurrence is thus a rarity, although, sincenumerous cases are not reported in the literature,it is likely that its frequency is greater than thesefigures indicate. Should the twins survive, thepossibility of their separation will be raised witha neurosurgeon and if the union is an extensiveone, as it commonly is, the problem is a daunt-ing one. Not only is it unlikely that the surgeonwill have had any previous experience of the con-dition, but until recent times there was little inthe literature to guide him. The first report(Grossman et al., 1953) described the separationof a pair of such twins with the survival of oneof them. Subsequently (O'Connell, 1964;O'Connell, 1968) came descriptions of separationoperations in three cases of total verticalcraniopagus, one of each pair surviving. Thisstudy of personal material has been made in thecertain knowledge that further attempts toseparate craniopagus twins will be made in theI Address for reprint requests: Fishing Cottage, ltchen Abbas, nearWinchester, Hampshire.(Accepted 16 July 1975.)
1
future. The practical problems resulting fromdisordered anatomy are discussed and theirsolution, complete or partial, described. Theabnormal anatomy is analysed and related toembryological development. The nature of theprimary congenital defect is discussed. A classi-fication of craniopagus is produced, differentia-ting partial from total unions so that confusionin the literature between the different types ofcase may be avoided in the future. Finally, theethical problems which arise in connection withthe surgical treatment of total vertical cranio-pagus are discussed.The material studied has been the records of
three personally treated cases of craniopagusmentioned above and previously reported. Forthe present paper, certain clinical features andresults of investigation as well as operativefindings are reconsidered. The postmortemstudies made in each of the twins of the secondand third pairs who died during surgery arecorrelated with the other findings. In addition,through the kindness of colleagues, postmortemstudies of another example of craniopagus, notseen during life, have been possible. The smallbut increasing literature dealing with cranio-pagus has been reviewed and where appropriaterelated to the present work.
Protected by copyright.
on October 13, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.39.1.1 on 1 January 1976. Dow
nloaded from

J. E. A. O'Connell
CLASSIFICATION OF CRANIOPAGUS
According to the site of the cephalic junction, ithas been customary to classify cases of cranio-pagus as parietal, frontal, or occipital, over 60%of them being parietal. This method of classifica-tion is inadequate since it makes no distinctionbetween unions of limited superficial extent anddepth and the extensive unions in which the twocranial cavities are in wide connection. It isproposed that the cases be placed in two groups,partial and total. In partial craniopagus, thesurface area of the heads involved is usuallyrelatively small and the crania may be intact andsimply fused in this area; or there may be acranial defect and the dura mater of the twinsbe in contact and possibly fused within thedefect; or the dura mater may be absent and theleptomeninges covering the related areas ofcerebra are in contact with one another. Theabnormality extends no deeper and is, in fact,simply a defect of cerebral coverings and fre-quently a limited one. It should be noted thatoccasionally the junction in partial craniopagusmay appear to be extensive, yet radiologicalexamination reveals that a layer of bone repre-senting the fused skulls of the twins extends overmuch of the junction. Such a superficial unionmust, of course, be classified as partial cranio-pagus. In total craniopagus there is an extensivearea of surface involvement and the cranialcavities are widely connected; indeed, the twobrains are contained within a common cranium.This leads to the very important alterations incerebral development and circulation which willbe described later in detail. Partial craniopagusis thus essentially an extracranial abnormalityand total vertical craniopagus a gross intracranialone. The partial unions may be frontal, parietal,or occipital; total craniopagus is, from itsnature, likely to be biparietal and, since it is a
very wide union, it is thought can better bedescribed as vertical.
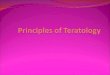
1. Partial craniopagusThree pairs of twins of this type have beenreported in the literature, all having beentreated surgically.The first of these (Voris et al., 1957) was a centralvertical union in which the dura mater of bothchildren was intact and a thin layer of skull separated
much of the dura mater of one twin from that of theother. The result after separation was excellent inone child but the other, whose superior sagittal sinuswas possibly injured at operation, has surviveddisabled and had repeated operations for cerebro-spinal fluid fistula and ventricular dilatation (Fig. Ia).The second pair (Baldwin and Dekaban, 1958) had afrontal union (Fig. 1 b); this was an oval area measur-ing 8.0 cm x 6.5 cm and united the children's rightfrontal regions. There was a dural defect within thisarea but intact leptomeninges covered the exposedfrontal cortex of each cerebrum. Separation andsurvival of both were achieved without defect andthey were developing well seven years later. In thethird pair (Wolfowitz et al., 1968), the union was alsoa frontal one but more localized (Fig. ic), so thatthere was some mobility of one head from the other.The essential of the operative procedure was theseparation of a relatively small area of dura mater ofone child from a similar area in the other, and thiswas achieved with the survival ofboth children. Fromwhat follows, it will be realized that such partialunions are an entirely different problem from thetotal ones.In addition to these three cases of localizedcraniopagus treated surgically in recent years,others must clearly have been born, if theincidence of craniopagus twins is one in two-and-a-half million births. Of a series of 22 cases(Robertson, 1953) two were frontal and fiveoccipital. Details are not available, but it islikely that several of these were cases of thepartial form. No doubt there have been otherreports of cases of localized craniopagusthroughout the world but the literature is not atrue guide to the frequency of such abnormalities.
2. Total craniopagusIn this variety the union is extensive. It iscommonly vertical and described in the literatureas parietal. However, very widespread unionscan occur elsewhere. Klar (1963) described anextensive frontal union and the author has seenradiographs of twins with an extensive parieto-occipitotemporal union. In some of the reportsof such extensive unions in situations other thanthe vertical one (Sapinski, 1966), it seems possiblethat the wide union was vertical at an earlydevelopmental stage. Later intrauterine forcesaltered the relationship of the long axes of theinfants to one another so that a gross angulationoccurred at the site of junction between the
2
Protected by copyright.
on October 13, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.39.1.1 on 1 January 1976. Dow
nloaded from

Craniopagus twins: surgical anatomy and embryology and their implications
4
I
J
..... .; ........ .. 4Fr . / .........._r >' >A
'^''M-. C--i<>wi;FR
a} X ';8
oV'.'x2 '' @}A Y .; f:
_E
i .t.fi. +kG
rIB
( 'C
K,.
FIG. 1 Partial craniopagus: (a) Voris et al. (1957); (b) Baldwin and Dekaban (1958); (c) Wolfowitz et al. (1968).
H.K
( 1i
( I-,)
$Al(p
Wv>%'.A..
3
VIV
Protected by copyright.
on October 13, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.39.1.1 on 1 January 1976. Dow
nloaded from

J. E. A. O'Connell
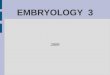
the skull is involved and the appearance is thatof a common cranium for the two brains.Examination of personal material suggests thataccording to the degree of rotation of one twin'shead on that of the other, around the longi-tudinal axis, three types of total vertical cranio-pagus can be distinguished. It might be expectedthat no such rotation would be present and thatthe faces of both twins would have an identicaldirection. However, for some reason, torsiondevelops in the tissues at the site of the unionand varying degrees of rotation of one head onthe other result. Three types of this form ofunion can be distinguished. In the first (type I),apart from minor tilting and rotation, bothchildren face in the same direction (Fig. 2). Intype II, the faces are on opposite sides of the
FIG. 2 Total cranioapgus: type L
heads. The literature contains numerous refer-ences to total vertical craniopagus. Most of thesedeal with cases in which no attempt at separationhad been made or in which, if such an attempthad been made, both children succumbed im-mediately. Robertson (1953) found referencesto 14 such cases and added one of his own.Other references and personal communicationsadd nine to this total and of this group of 24cases attempts at separation had been made insix but without a survivor from any of theoperations. In addition, there are the reports ofthe four surgically treated pairs already referredto in which there was one survivor from eachpair. This total of 28 cases of total verticalcraniopagus certainly must lack some of thosereported in the literature and it also seems certainthat there has been a considerably larger numbernever so reported.
In total vertical craniopagus the whole vault of
.,:,.,$ ..........t . > :::,;;.d'$ R.#.. e 9. . . .......... ..
fi 8s,;^ .. ...
.,.. .aR. ,,
..jt t:.>,,4. ::
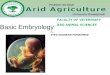
FIG. 3 Total craniopagus: type II.
4
AlIS kz-
4L
Protected by copyright.
on October 13, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.39.1.1 on 1 January 1976. Dow
nloaded from

Craniopagus twins: surgical aniatomy and embryology and their implications
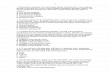
FIG. 4 Total craniopagus: type III.
conjoined skull, the long axis of one head beingrotated relative to that of the other through an
angle of 140° or more (Fig. 3). In the thirdvariety (type III), the angle of rotation of thelong axis of one head on that of the other isintermediate between that in the other types(Fig. 4). As will be shown later, these differencesof type are of considerable importance insofar as
the deformity of the brains and abnormality oftheir circulation are concerned.
If it be decided that an attempt to separate thetwins should be made, it is essential that a very
thorough investigation of intracranial anatomybe carried out, since unless the operation isplanned on the basis of such knowledge, it willalmost certainly fail completely. The mostinformative investigation is carotid angiography,which provides knowledge of the relationship of
the cerebra to the cranium, deformity of thecerebra, and the cerebral vascular circulation.This has been described by O'Connell (1964) andO'Connell (1968). In the past, until such in-vestigations had been made, no picture of theintracranial anatomy could be developed. Now,however, examination of our material suggeststhat it may be possible from clinical examinationto gain a picture of the intracranial abnormalitiesto be expected; thus one might predict the re-lationship of the cerebra to the cranium and thenature and presence of cerebral deformity. Thetype of vascular circulatory abnormality-especially venous ones-that is present mightalso be suggested. With this in mind, the anatomyof total vertical craniopagus will now be reviewedin some detail.
Abnormalities associated with total verticalcraniopagus and mechanism of their production
1. SCALP As a result of the junction, scalp at thevertex never develops. If separation is effected, it isclear that an enormous defect of scalp over the wholevertex of the head will result.
2. SKULL a. Vault There is no vault to eitherskull. The frontal, parietal, and occipital bones ofeach twin, which would normally provide this,articulate with one another around the equator ofthe common cranium. As in the case of the scalp,after separation is achieved there is left a large skulldefect, the whole vault being absent.
b. Base While clinical examination reveals noobvious abnormality here, at postmortem examina-tion well-marked abnormalities may be found. Thefirst example (Fig. 5) is the skull base of one of thepair of twins (type I) illustrated in Fig. 2. These werenot seen during life but colleagues provided theopportunity of making a postmortem examination.The drawing shows that the skull is extremely wideanteriorly with its maximum transverse measure-ment at the level of the anterior clinoid processes.Posteriorly, the petrous temporal bones give theimpression of having been rotated medially aroundtheir apices so that the posterior fossa is small asalso is the tentorium cerebelli, though its foramen isgreatly enlarged. The anterior and middle fossae arecapacious and the posterior cranium is small, theimpression being one of a pear-shaped skull base.The other skull base illustrated (Fig. 6) is that of thefatality in the third pair operated upon (type III:Fig. 4). There is gross asymmetry; the posteriormargins of the lesser sphenoidal wings make an
5
OP"
Protected by copyright.
on October 13, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.39.1.1 on 1 January 1976. Dow
nloaded from

J. E. A. O'ConnellW§.r
Tentorium cerebelli
FIG. 5 Base of skull: type I craniopagus.
oblique line passing posteriorly when followed fromleft to right. The left anterior and middle fossae arecapacious and separated by a shallow sphenoidalwing; those on the right are markedly smaller, thoughthe temporal fossa is deep. The petrous temporalbone on the right is displaced posteriorly and
galfi
Foramenmagnum
FIG. 6 Base of skull: type III craniopagus.
medially so that the posterior fossa is small on thisside. The skull base of the operative fatality in theother pair of type III craniopagus showed essentiallysimilar changes to those just described. There hasbeen no opportunity for postmortem examination ofthe skull base in type II cases (Fig. 3).What is the cause of these deformations of the
skull base? It is believed that they are related to thegrowth of the telencephalic vesicles. These diverticulaof the prosencephalic cavity of the embryo appearduring the fifth week of development. In relationshipto their prosencephalic site or origin they growanteriorly, superiorly, and posteriorly, coming inthis manner to cover in succession the diencephalon,mesencephalon, and upper metencephalon. Develop-ment inferiorly is less marked but the vesicles growmedially to come into contact with one another inthe midline above the neural tube. The wall of eachvesicle thickens and, as its surface area increases, itis thrown into the characteristic convolutions of thecerebrum. The force developed by this growthprocess is considerable. Thus, between the fifth and17th weeks the brain as a whole increases in size3 000 times; in the same period the proportion ofbrain weight of the cerebral vesicles to that of thewhole brain increases from 700 to 90%4; the thick-ness of the wall of the cerebral vesicle increases from1 mm to 20 mm (Hamilton and Mossman, 1972).The effect of such cerebral growth forces on the skullbase can best be considered when the cerebraldeformities occurring in these cases have beendescribed. While such deformities of the skull basemight appear to have no direct practical importance,it will be seen later that they help towards theunderstanding of the gross cerebral deformitieswhich, by their presence, may greatly increase thetechnical difficulties of operations to separate thesetwins. Moreover, these deformities are predictablefrom their relationship to the different types of totalvertical craniopagus.
3. CEREBRUM In cases of total vertical craniopagusthe two cranial cavities communicate so freely thatthe brains exist within a common cranium. As aresult, growth processes in one brain instead ofsimply producing skull enlargement give rise todeformation of the other brain and, of course, suchdeformation will be mutual. The development of thetelencephalic vesicle anteriorly and its extensionsuperiorly and posteriorly must mean that thedeforming growth forces are maximal in relationshipwith the anterior part of each brain. The type ofcerebral deformity which occurs depends upon thedegree of rotation of one head on the other, this, ofcourse, altering the relationships of the frontalportions of the two cerebra. As has been pointedout, three groups of cases can be differentiated; in
6
..........
Protected by copyright.
on October 13, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.39.1.1 on 1 January 1976. Dow
nloaded from

Craniopagus twins: surgical anatomy and embryology and their iinplications
type I the rotation of one head on the other isminimal and the faces are directed to the same side.In type II the rotation is maximal (140-180o) andthe faces are directed to opposite sides. In type IIIthe rotation is intermediate in degree between thatin the other two types.On the first group (type I: Fig. 2), the developing
frontal portions of the four cerebral hemispheres areintimately related in the anterior part of the con-joined cranium. What are thought to be the relation-ships of the developing cerebra at the 27 mm, 60-daystage are shown diagrammatically in Fig. 7. Thebrains illustrated are drawn from the reconstructionsof Hochstetter. As a result of the area of union,posterior development of the cerebrum will beimpaired. Development superiorly can occur an-terior to the union but will be restricted by similargrowth of the opposite twin's anterior cerebrum.As a result, the anterior cerebrum is enlarged inboth its vertical and transverse measurements, whilethe posterior cerebrum is small; the anteroposteriormeasurement of the brain is reduced. The lateral viewof such a brain is illustrated by Robertson (1953); a
Metencephalon -
FIG. 7 Development ofcerebral hemispheres in type Icraniopagus. Arrows indicate direction and magnitudeofgrowth forces.
basal view is seen in Fig. 8-this drawing being oneof the brains of the example of type I craniopaguspersonally examined post mortem. The cerebrum isshort and wide with relative increase in the size ofits anterior half. The skull base in this case is illus-trated in Fig. 5. The deformity has already beendescribed and is thought to be due to the increasedsize of the anterior cerebrum and stunted growth ofits posterior portion. This leads to a widening anddeepening of the anterior cranium and there isresulting stunting of its growth posteriorly (Fig. 7).The cerebral deformity in this type of total verticalcraniopagus is illustrated in the diagrammaticdrawing (Fig. 9).
In the second group (type II: Fig. 3), the faces areon opposite sides of the conjoined skull. What arethought to be the relationships of the developingcerebra again at the 27 mm, 60-day stage, are showndiagrammatically in Fig. 10. As in the previousgroup, growth of the cerebrum posteriorly will beimpeded but growth superiorly will be unopposedand the frontal portion of each cerebrum will towerupwards and perhaps make contact with the ten-torium of its twin. The posterosuperior developmentof each cerebrum will be reduced since its growthwill be impeded by that of the other twin's frontalcerebral area; each cerebrum will, in fact, be wedgeshaped. The appearances are well demonstrated bycarotid angiography in the case illustrated in Fig. 3.In Fig. 11 (a and b) the left carotid angiogram of one
FIG. 8 Base of brain type I craniopagus.
7
Protected by copyright.
on October 13, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.39.1.1 on 1 January 1976. Dow
nloaded from

J. E. A. O'Connell
FIG. 9 Cerebral deformity in type I craniopagus.
Te,/encephau
Mesen-,cepalon
Mee'rNlt
Ms.etencc;pi4ao
FIG. 10 Development of cerebral hemispheres intype IH craniopagus.
of the twins is seen in anteroposterior and lateralprojections; in the capillary phase the frontal towerand wedge shaped hemisphere are demonstratedclearly. The other three hemispheres showed asimilar deformity. As has been said, no postmortemexamination of the skull base of such a type IIcraniopagus has been studied. Since the anteriorportions of both cerebra are so early and fullydecompressed, it might be expected that the bonechanges would be less marked than in the othertypes. Figure 12 illustrates the cerebral deformity inthis type of total craniopagus. In the third group(type III: Fig. 4), rotation of the heads is intermediatein degree between that in the other two types, andmoreover since one vertex is, in a sense, placedacross the other, it will overlap one side of the otherhead. This is illustrated in Fig. 4, where it will beseen that the frontal region of each child is set on theright side of the other's vertex. It is believed that theearly development of the anterior cerebral region onthe right side of the other twin's right cerebralhemisphere will cause the latter to be displaced tothe left side of the cranium, the left cerebral hemis-phere being compressed beneath it. The right frontallobe will tower upwards as in the previous group andthe left one will be overlapped by it. The appearancesare best demonstrated again by means of carotidangiograms made in the first of the two pairs of suchtwins investigated in this way before separation. InFig. 13 (a and b) anteroposterior and lateral angio-grams after left carotid injection show the greatlycompressed left cerebral hemisphere. In Fig. 14 (aand b), similar projections after right carotidinjection are shown. The frontal tower is clearlyseen in the lateral projection and the overlap of theleft by the right hemisphere in the anteroposteriorone. A diagrammatic drawing of the cerebraldeformity in such type III cases is shown in Fig. 15.The skull base associated with this type of brain
deformity is seen in Fig. 6. The cerebrum of eachchild was displaced to the left across the skull base,the right hemisphere compressing the left one beneathit. This would explain the very large left anterior andmiddle fossae and the small right fossae. The deepright temporal fossa with medial displacement of thepetrous temporal bone might be explained as result-ing from pressure from the child's own right temporallobe with the addition of the right frontal tower ofthe opposite twin.
It is thought that these observations explain thedifferent types of cerebral deformity which occur intotal craniopagus and suggest the reasons for thedifferences, and also that they explain the associateddeformities of the cranial base. It thus appears that,in the four examples of total vertical craniopagusstudied, their classification into three groups provides
8
Protected by copyright.
on October 13, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.39.1.1 on 1 January 1976. Dow
nloaded from

Crantiopagus twins: surgical anatomy and embryology and their implications
( LI) (b)
FIG. 1 1 Left carotid angiogram: type II craniopagus: (a) anteroposterior, (b) lateral.
the basis for an explanation of the different deformi-ties of the cerebrum and cranium which have beenfound. The classification and explanation also appearapplicable to certain cases described in the literature-for example, Barbosa (1949), Robertson (1953),and Grossman et al. (1953). It may well apply to allcases but adequate information concerning these hasnot been available in such reports as have been seen.As has already been mentioned, in cases of extensiveunion in other situations than the vertical one,intrauterine forces may be responsible for producingangulation at a union which was at first a verticalone.
4. MENINGES a. Pachymeninges In the three per-sonally treated cases of total vertical craniopagusdescribed above, as well as the further case examinedpost morten, no layer of dura mater separated the
two brains. It must be supposed that the ectomeninxwhich gives rise to the dura mater and cranium isabsent from the area of contact between the cerebra,and dura mater is absent here as, of course, is theskull. In two of the cases a peripheral dural shelf,10-15 mm wide, projected into the line of contactbetween the two brains and contained importantvessels in its base. A similar fold was present on oneside only in the third treated pair: small foldsrepresenting the falces cerebri and joined at theirbases were present on the opposite side. In some ofthe cases described in the literature in which the faceswere directed to the same side (type I), a thin duralseptum extended between the related hemispheres,of one side only, to the midline. The falx cerebri wasvestigial in all cases; the vestiges were basal andanterior, apart from those in the case mentionedabove, in which-on one side only-small folds
9
Protected by copyright.
on October 13, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.39.1.1 on 1 January 1976. Dow
nloaded from

J. E. A. O'Connell
FIG. 12 Cerebral deformity in type II craniopagus.
representing the falces cerebri and fused at theirbases, were present.
In considering the dural deficiency, it must berecalled that this is not only a defect at the area ofcontact between the cerebra; it includes the absenceof hypoplasia of the falx cerebri and at times thedeformity of the tentorium cerebelli already referredto. As far as the falx cerebri is concerned, since theportion of the primitive meningeal layer which givesrise to the dura mater over the surface of theapposed cerebra is lacking, there is no possibility ofa falx developing here. Minor projections of duramater between the hemispheres may be seen in basalregions not directly involved in the union. This wasthe state of affairs in all the personally examinedcases. Around the periphery of the cranium a narrowcircumferential fold of dura mater projects for a
short distance between the two cerebra. This indeedwould represent the falx cerebri in such cases pro-jecting between the two brains instead of the twohemispheres of one brain. The tentorium cerebelli-unrelated to the defect-is in its normal position.However, as has been seen, it may be hypoplasticand its opening considerably enlarged. Such changesmay well be secondary to the absence of the falxcerebri which normally holds the centre of thetentorium superiorly and anteriorly; limitation of
the development of the cerebrum posteriorly mightalso contribute to the tentorial deficiency.
b. Leptomeninges During the separation of theapposed brains, it appeared that the interdigitatinggyri were, for the most part, covered by normalpia-arachnoid mater. However, in two of the cases,these layers appeared to be absent in some smallareas and cerebral continuity appeared to be presenthere. It had previously been noted that arterialanastomoses were present in these areas. In Fig. 17aa large arterial anastomosis between a branch of theinjected twin's middle cerebral artery and an arteryin her sister's brain is seen, as well as a smaller onemore posteriorly. A possible explanation for thesefindings will be suggested later.
5. VASCULAR CIRCULATION The cerebral vasculararchitecture in craniopagus can be clearly demons-trated by carotid angiography (Du Boulay, 1964).The most important angiographic findings from thecirculatory viewpoint will now be considered withreference to the first two pairs of twins coming underour care; these will be described and related to theoperative findings.
In Fig. 1 6a and b the arterial and venous phases ofa left carotid angiogram in one of the first pair oftwins treated (type II) is seen. The arteriogram(a) reveals normal but displaced arteries, the anteriorcerebral artery and its branches coursing superiorlyto supply the frontal tower. The middle cerebralartery and its branches are also displaced anteriorlyand superiorly-these changes indicating the de-formity of the hemispheres already discussed (Fig.12 and Fig. 11, a and b). Of greater importancefrom the circulatory aspect is the phlebogram (b).A group of large veins converge on a vascularchannel which passes along what proved at operationto be the line of contact of the cerebra around theperiphery of the junction. The united vessels thendischarge into the other twin's transverse sinus.There is but little evidence of venous drainage intothe injected child's own transverse sinus. The peri-pheral venous channel proved at operation to be acircumferential sinus in the base of the narrowmedially projecting dural fold which could beregarded as a representative of the falx cerebri butlying between the cerebra of the two children insteadof between the hemispheres of each one's cerebrum.It was noted that the dura mater in relationship withthis sinus contained large venous channels betweenits layers. Surprisingly, connections between veinson the cerebra themselves and the sinus over thegreater part of its length were inconspicuous, aswere arachnoid adhesions to it. The major drainageof blood from the exposed areas of cerebrum was
10
Protected by copyright.
on October 13, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.39.1.1 on 1 January 1976. Dow
nloaded from

Craniopagus twins: surgical anatomy and embryology and their implications
.4.c,,.>,>,,,,............................................................._~~~~~~~~~~~~~~~~~~~~~~~~~~~~~..... ..............e::#..... , :.::~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~,......
Z S p'^'~~X.
FI. 3 etcaoiaFgormyeIIcazoais a ttrpseir b ae-l
thus through a group of large veins passing directlyanteriorly to empty into the lateral sinus of theother twin either through or independently of thecircumferential sinus. In addition, in the midlinebetween the two cerebra there were some smallposteriorly directed veins passing through a lake ofcerebrospinal fluid, in the direction of each child'sown lateral sinus. Investigation of the other twin ofthis pair by carotid angiography revealed an exactlysimilar venous abnormality.
Figure 17 (a and b) are angiograms from thesecond pair of twins dealt with (type III). Thearteriogram (a) is right-sided and shows the upwardstretching of the anterior and middle cerebral arteriesoccasioned by the shape of the cerebral hemisphere.This arteriogram also demonstrates arterial anasto-moses between the branches of the two children'smiddle cerebral arteries-a large central and a
smaller posterior one. The phlebogram (b) is left-sided; as discussed under cerebral deformity, thishemisphere is compressed and overlain by the rightone and its outline suggests a normal shape. Againfrontal veins converge on a circumferential vein atthe line of apposition of the two left hemispheres,and the greater part of the flow is into the oppositetwin's transverse sinus.When the investigation of the first pair of twins
revealed this crossed venous drainage, it seemed thatthere could be little hope of separation withoutobstructing the venous return from both children'scerebra. Indeed, the possibility of venous graftingwas considered and preparations for it made pre-operatively. However, when exploration was carriedout it was found that instead of a superior sagittalsinus between each child's cerebral hemispheresthere was a circumferential venous sinus between the
I1I
Protected by copyright.
on October 13, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.39.1.1 on 1 January 1976. Dow
nloaded from

J. E. A. O'Connell
FIG. 14 Right carotid angiogram: type III craniopagus: (a) anteroposterior, (b) lateral.
two brains along the line of their contact and lyingwithin a small medially projecting dural fold. It wasfurther found that venous drainage from the cere-brum to which this fold was given was normallymaintained but severe venous infarction occurredin the brain of the other child. The anatomy of theperipheral sinus is indicated diagrammatically inFig. 18.No example of the third variety of total vertical
craniopagus (type I), that in which the faces areturned to the same side, has been encounteredclinically, so that the clear picture of the vasculaturewhich can be achieved by carotid angiography wasnot obtained, but a postmortem examination wascarried out on one such pair (Fig. 2). As the headswere separated during the examination, no peripheralvenous sinus nor any dural fold at the line of contact
of the cerebra was seen. Neither was there any durallayer between the brains nor any falx. Between thehemispheres of both children there was vascular piamater possibly containing veins. Related to the con-joined occipital areas of the cerebra, a venous lakewas seen but its detailed anatomy was not studied.In the example of this type of union treated by Gross-man et al. (1953) a dural septum separated thecerebral hemispheres on one side of the junction;three longitudinal veins passed posteriorly inrelationship with it. However, the anatomy of thesecerebral veins at their union with the two pairs oflateral sinuses was confused and occasioned difficultywhich was probably responsible for the death of onechild soon after operation. Thus in these (type 1)cases, although the positioning of the heads whichpredisposes to crossed venous circulation is absent,
12
Protected by copyright.
on October 13, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.39.1.1 on 1 January 1976. Dow
nloaded from

Craniopagus twins: surgical aniatomy and embryology and their implications
FIG. 15 Cerebral deformity in type III craniopagus.
the close relationship between veins draining thecerebra of both twins in the area of the torcularappears to make separation and the survival of botha difficult goal to achieve.
In considering the basis of the abnormalities in thevenous drainage of the cerebra, one can do no betterthan recall the statement of Streeter (1918) on thedevelopment of the vascular system of the brain:
'The development of the blood vessels of the head...demonstrates the important embryological principle ofwhat may be termed integrative development.... Thevascular apparatus does not, independently of itself, un-
fold into the adult pattern. On the contrary, it reactscontinuously in a most sensitive way to factors of itsenvironment, the pattern in the adult being the result ofthe series of the environmental influences which playedupon it during the embryonic period.'
The normal superior sagittal sinus arises from aplexus of veins which is situated in the sagittal planebetween the developing cerebra. This venousplexus lies in a well-marked layer of embryonictissue (ectomeninx) which later forms the duramater, that portion between the cerebral hemispheresgiving rise to the falx cerebri and that betweencerebrum and cerebellum to the tentorium cerebelli,the two being continuous beneath the posteriorcerebrum. As the cerebrum develops superiorly andposteriorly, the ectomeninx develops with it and anextension of the venous plexus is carried posteriorly
within it. This plexus is continuous with anothersimilar one in the embryonic tissue between thecerebrum and cerebellum from which the lateralsinus will develop. Thus, with the growth posteriorlyof the developing cerebral hemispheres, the falxcerebri with the sinuses within it is developed pro-gressively from before backwards. All the veins fromthe superior part of the lateral surface of thecerebrum drain into this superior sagittal sinus. Thesinus drains into the transverse sinus lying in themembrane between cerebrum and cerebellum. Thisis the residuum of the three dural plexuses whichdrained into the internal jugular vein. With thegrowth of the cerebrum posteriorly, it is tilted in thesame direction through 900 to gain the position ofthe adult lateral sinus, the portion distal to the bendbecoming the sigmoid sinus. As a result of the sameposterior development of the cerebrum the ecto-meninx between it and the cerebellum is compressedto form the tentorium cerebelli. In total verticalcraniopagus there is no ectomeninx at the site ofunion and no development of skull, dura mater, orfalx cerebri can occur in an area which is rapidlyincreasing in extent as a result of cerebral develop-ment. There can, therefore, be no sagittal venousplexus and a superior (or inferior) sagittal sinuscannot develop. However, at the line of appositionof the cerebral hemispheres of each child, a shallowinfolding of the ectomeninx occurs between thebrains, and contains a plexus in its base, formed byvenous tributaries from each brain. This representsthe superior sagittal sinus but is instead a circum-ferential one. Anteriorly and posteriorly, it joins thelateral sinuses of the twins. As the cerebra grow, thevenous ring of the circumferential sinus will growwith them. The great anterosuperior development ofthe twins' frontal cerebral areas will occasion asimilar displacement of the sinus. The relationshipof each twin's frontal tower to the opposite twin'stentorium will result in the enlargement and drainageof the major superior cerebral veins into the anteriorpart of the circumferential sinus or the tentorialplexus (lateral sinus) itself. Thus, much of thevenous drainage of each child's cerebrum, whichwould normally be carried posteriorly through itssuperior sagittal sinus to its own lateral sinus, is inthis manner directed into its twin's sinuses and heart.The remainder of the superficial venous drainage ofthe cerebra must be by way of the Sylvian andinferior cerebral veins. In the third variety ofcraniopagus in which crossed venous circulationdoes not occur superior sagittal veins have beenfound. These discharge into each twin's own lateralsinuses. No superior sagittal sinuses are present,however, and it appears that the arrangement ofveins at the tentorium may be complex.
13
Protected by copyright.
on October 13, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.39.1.1 on 1 January 1976. Dow
nloaded from

J. E. A. O'Connell
FIG. 16 Left carotid angiogram: circulation in type II craniopagus: (a) arteriogram, (b) phlebogram.
6. CEREBROSPINAL FLUID CIRCULATION In con-
sidering the problems which might result from an
attempt at separation ofcraniopagus twins, that of themaintenance of the cerebrospinal fluid circulationarises. While arachnoid villi occur in relationshipwith many of the intracranial venous sinuses,normally they are most conspicuous in relationshipwith the superior longitudinal sinus and its lacunae.These villi are present at birth or even earlier and bythe age of 3 years hypertrophic villi (arachnoidgranulations) may be numerous in the sinus (Clark,1920). When investigation shows an absence of thesinus, one is left wondering how the loss of this largearea of cerebrospinal fluid absorption can be com-
pensated for. Would separation be followed by a
cerebrospinal fluid fistula or would a communicatinghydrocephalus develop? During the separation ofthe first pair of twins, a lake of cerebrospinal fluidwas found between the cerebra over the shallowvertically compressed longitudinal cerebral fissures.In each case, a longitudinal vein draining blood from
both cerebral hemispheres passed posteriorly throughthis lake to the torcular region. There was littleadhesion between the circumferential dural shelf andits contained sinuses and the cerebral coverings. Itthus appeared to be a channel connecting the infants'lateral sinuses and receiving much of the blood fromtheir cerebral hemispheres. The site of major cere-brospinal fluid absorption was not exposed. Sincearachnoid villi project through the dura mater intosinuses rather than into veins unclothed by duramater, it must be supposed that the sinuses con-cerned were basal ones-lateral, cavernous, petrosal,sphenoparietal, etc. At all events, although in allcases a transient leak of cerebrospinal fluid occurredpostoperatively, this ceased after a short period andno defect of cerebrospinal fluid circulation has shownitself in subsequent years.
Progniostic and therapeutic implications ofabnormalities
The significance of the various abnormalities des-
14
Protected by copyright.
on October 13, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.39.1.1 on 1 January 1976. Dow
nloaded from

Craniopagus twins: surgical anatomy and embryology and their implications
I;a) (h)IFIG. 17 Bilateral carotid angiograms: circulation in type III craniopagus: (a) right arteriogram (showinganastomotic vessels), (b) Left phlebogramn.
cribed is revealed in their description. However, itmay clarify certain points if they are consideredindividually under the heading of their prognosticand therapeutic relevance.
1. SCALP In the personal cases the large scalp defectwas skilfully overcome by plastic surgery (Jayes,1964). Rotation flaps were utilized and the donorareas covered with split skin grafts. When skilledplastic surgery is available, the problem of scalpclosure does not affect prognosis or treatment.
2. SKULL a. Vault The vault of the skull is absentand an enormous skull defect exists after separation.It has been considered that no attempt to close thisdefect at the time of separation could be justified; itwould add to the difficulty of scalp replacement overthe brain and might predispose to infection. Indeed,
in each of the surviving children it has been thoughtthat a delayed cranioplasty was best avoided and anexternal prosthesis has been provided (Fig. 19, a andb). When the plastic hat is combined with a wigsome of the disadvantages of this form of protectionare diminished.
b. Skull base The deformity does not of itselfaffect prognosis or treatment. Were it to be discernedin skull radiographs, it would simply point to thecerebral deformities which give rise to it.
3. CEREBRUM In each of the three types of totalvertical craniopagus which have been described,well-marked deformity of the cerebrum was presentand differed according to the degree of rotation ofone head on the other. Recognition of such deformityis essential before any attempt at surgical separation
15
Protected by copyright.
on October 13, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.39.1.1 on 1 January 1976. Dow
nloaded from

J. E. A. O'Connell
Superior cerebralveins of twin A
sinus
FIG. 18 Anatomy of peripheral dural shelf andcircumferential sinus.
is made. In the first place, it will frequently meanthat the line of contact between the cerebra is not onan equatorial plane through the conjoined craniumbut a very different one. It is essential that, whenseparation is attempted, the line of the circum-ferential scalp incision follow the line of braincontact as closely as possible. Secondly, there maybe marked asymmetry between the cerebral hemis-pheres of each child. Unless this is understood,considerable difficulty may arise during the separa-tion and injury to the cerebrum in one or both chil-dren may occur, in the false belief that cerebralfusion is present.
4. MENINGES a. Pachymneninges The most ob-vious abnormality here is the large dural defect overthe whole of what would normally be the cranialvault when separation is effected. This was presentin all of the personally treated cases but from theliterature it appears that occasionally a thin durallayer is found to separate one hemisphere of onechild from the related one of the other child. In eachof the three surviving cases, reconstituted freeze-dried dura mater was sutured into the defect andwas of greatest value forming an excellent protec-tion for the cerebrum. Bearing in mind the very largearea of the defect, it must be realized that it would beextremely difficult to find in either child a sheet oftissue of adequate size and structure to close thedural gap. The other abnormality of the dura materwas the absence or hypopJasia of the falx cerebri.The reason for this has been suggested. Its importancelies in the fact that the superior sagittal sinus isabsent. Although some longitudinal veins may be
seen in the longitudinal cerebral fissure, being intra-dural, they are abnormal, being less protected frompressure changes and not providing a vessel suitablefor the reception of arachnoid villi. The absence ofthe falx cerebri has other consequences. In the firstplace, there is no barrier to cerebral displacementacross the midline such as the falx provides betweennormal hemicrania. This may explain the gross dis-placement of cerebrum seen in type III craniopagus.Secondly, the dural partition between the posteriorfossa and the rest of the cranium, the tentoriumcerebelli, may be flat instead of normally tented andhypoplastic with considerable enlargement of itsforamen. The fact that it is unsupported by the falxcerebri in the midline may well be in part responsiblefor these abnormalities.
b. Leptomeninges No important abnormality wasseen but the arachnoid may have been absent insome small areas and fusion of the cerebral tissuemay possibly have occurred here.
5. VASCULAR CIRCULATION The abnormalities herehave great prognostic importance and no doubtexplain the virtual impossibility in the present stateof knowledge of effecting separation with the survivalof both children in total vertical craniopagus, typesII and III. The only abnormality of the arterialsupply of the cerebrum is displacement of vessels inaccordance with the ccrebral deformity; this has noclinical importance. However, in the case of thevenous drainage the changes have the highest im-portance. The superior sagittal sinus will be absentin both twins in most cases and be replaced (in typesII and III craniopagus) by a circumferential sinuswhich unites the lateral sinuses in the two children.The relationship of this sinus to the cerebra has beendescribed above: it can carry blood posteriorly toits own lateral sinus from the large group of superiorcerebral veins which in each twin discharge into theopposite twin's lateral sinuses. If these veins leavingthe frontal tower are ligatured between the circum-ferential sinus and the second child's lateral sinusand if the complete circumferential sinus is nowdonated to the first child, cerebral venous drainagein that child remains intact. However, in the case ofthe second child when the same group of veins isligatured between its frontal pole and the circum-ferential and lateral sinuses, venous infarction of itscerebrum results. This has been the state of affairsin each of the three pairs personally operated upon.Indeed, in the third pair of twins treated, it was dis-covered at angiography that the venous ring of thecircumferential sinus included the central portionsof both lateral sinuses of each twin. In order tomaintain the integrity of the ring it was necessary to
16
Protected by copyright.
on October 13, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.39.1.1 on 1 January 1976. Dow
nloaded from

Craniopagus twins: surgical anatomy and embryology and their implications
(h)
FIG. 19 Photographs of surviving twin of third pair:(a) wearing prosthesis of ordinary type, aged 9 yr,(b) wearing prosthesis incorporated in wig, aged 10 yr.
donate these portions of these sinuses of one child tothe other. In the first type of craniopagus (Fig. 4), inwhich a crossed venous circulation is not present,difficulty with cerebral venous drainage still arises.There is no superior sagittal sinus and the longitu-dinal veins in its place may terminate posteriorly in avenous lake. In the single report of surgical treamentof such a case (Grossman et al., 1953), the technicaldifficulties experienced in dealing with this venousabnormality apparently led to the deterioration andearly death of one child.
6. CEREBROSPINAL FLUID CIRCULATION No ab-
normality of this has been noted in the personalseries of cases. The absence of a superior sagittalsinus as described above implies that other, probablybasal, sinuses replace this important vessel wherenormally a concentration of villi return cerebrospinalfluid to the bloodstream.
DISCUSSION
Before attempting to describe the essentialcongenital defect in craniopagus twins, it may behelpful to refer to some generally acceptedmodern embryological views. As in normal
17
Protected by copyright.
on October 13, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.39.1.1 on 1 January 1976. Dow
nloaded from

J. E. A. O'Connell
monozygotic twins so in craniopagus twinsgenetic factors influence the occurrence. Inaddition, animal experiments suggest thatenvironmental factors which slow the develop-ment of the embryo may play a part in thedevelopment of both separate and joined mono-vular twins. It is now believed that conjoinedtwins develop as a result of incomplete fission ofa single developing embryo and not fusion ofseparate embryos. It is further believed that theabnormality is established at the end of thesecond week of development (Benirschke andKim, 1973). This implies that, when the junctionis established, the anterior neuropore is stillpresent. It closes at the 26th day, its site beingsubsequently indicated by the lamina terminalis.The telencephalic vesicles appear at the 25th dayand, before this, the cutaneous ectoderm isseparated from the neural tube by a mesodermallayer, the meninx primitiva (Hamilton andMossman, 1972). This layer splits into an innerone, the endomeninx which forms the pia-arachnoid membrane, and an external one, theectomeninx, which forms the dura mater andskull. As the growing telencephalic vesicles meetin this tissue, they gain a leptomeningeal cover-ing from it but in total vertical craniopagus noectomeninx separates them. As a result, nodevelopment of a cranial vault with its durallining is possible.From the study of the material described, it is
believed that the congenital defect in total verticalcraniopagus is an area of absence of cutaneousectoderm (scalp) and ectomeninx (skull and duramater) at the site of the union. Around themargins of the defect the scalp, skull, and duramater of one child are fused with those of theother. The absence of dura mater at the vaultleads to a failure of development of the falxcerebri and possibly an abnormality of thetentorium cerebelli; more important, it meansthat the superior sagittal sinus cannot developand a gross abnormality of cerebral venousdrainage results. All the remaining abnormalitiesresult from mechanical pressure: these includedeformity of the skull base, cerebral deformityand displacement, leptomeningeal defects, andareas of cerebral fusion. In addition, it ispossible that cerebral dysfunction may be pro-duced by this pressure. The abnormalities of theskull base and cerebrum in the three types of
total vertical craniopagus have been describedabove and an explanation for them put forward.The other abnormalities will be considered, aftera brief further reference to partial craniopagus.
In partial craniopagus the congenital defectagain involves ectoderm (scalp) and ectomeninx(skull and dura mater). The superficial extent ofthe involvement is limited, however; it isfrequently no more than a few centimetres indiameter, although at times the area is moreextensive. More important is the depth of theinvolvement. At times only the cranial portionof the ectomeninx is involved with a simplejunction of crania and normal dura mater; orthe dura mater of one child may be adherent tothat of the other through the cranial defect; or alarger or smaller defect of the dura mater withinthe cranial defect permits contact of one child'spia-arachnoid membrane with that of the other.The growth of one brain in no way interfereswith that of the other and there are no forcesat work to prevent the development of the falxcerebri and superior sagittal sinus, or to producethe serious venous circulatory abnormality seenin total vertical craniopagus. As has been saidabove, partial craniopagus is essentially anextracranial abnormality.
Returning now to the discussion of totalcraniopagus, in separating the cerebra of thetwins it is noticeable that they are very closelyapposed with interdigitating gyri. For the mostpart a layer of pia-arachnoid mater covers eachhemisphere but in places it may appear to beabsent. In these small areas actual cerebralcontinuity between one child and the other hasbeen thought to be present. In considering thepossible cause of these areas of leptomeningealdefect and brain junction, their extent is solimited relative to the size of the junction thatthey cannot be regarded as part of the congenitaldefect itself, in existence since the second weekof development. It seems possible that pressuremight again provide the explanation. Normally,the arachnoid mater over the superior surface ofthe cerebral hemispheres is in contact with thesmooth dura mater lining the skull vault and willslide on it with the cerebral pulsations. In casesof craniopagus, the arachnoid covered hemis-pheres subject one another to a continuous andpulsating pressure. Forces of pressure and fric-tion could thus be active at the site of contact.
18
Protected by copyright.
on October 13, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.39.1.1 on 1 January 1976. Dow
nloaded from

Craniopagus twins: surgical anatomy and embryology and their implications
It is possible that these forces could produceminor tears in the serous membrane and therelated cerebral cortex and that vascularadhesions could unite the brains in such areas.
It is possible that the anatomical disturbanceslisted can be explained by pressure giving riseto brain displacement, deformity, and com-pression as well as small areas of meningealatrophy with superficial cerebral contusions. Itis also possible that compression could occasionphysiological disturbance. Thus psychologicaltesting of these infants has been carried outduring the months before the separationoperations when the necessary investigationswere in progress. During the latter part of thisperiod it has been found that performance fallsbelow that appropriate to the child's age(Franklin, 1964; Udall, 1975, personal com-munication). It had been supposed that this wassimply the result of restricted mobility withconsequent inability of each child to respondnormally to visual and auditory stimuli. Thedisadvantageous position from the psychologicalpoint of view is clear but is this the sole factor?
In the first year of life the weight of the brainincreases by 135%, growing therefore as rapidlyas it had done in utero. Does the fact that thewhole ofthe superior and part of the superolateralsurface ofthe cerebrum is in contact with anothercerebrum instead of the dural lined craniuminterfere with growth at this critical period? Thedisplacement and deformity of the cerebrawhich have been described, are such as to mouldthe skull base and it is probable that the cere-brum itself is subject to compression. If this beso, it is obvious that, if separation is to beattempted, it should be carried out with minimaldelay. However, a thorough preoperative in-vestigation remains essential if any measure ofsuccess is to be achieved.
It has been seen that partial craniopagusmust be clearly distinguished from the total form;in the absence of other serious abnormality,separation will always be indicated in the formergroup and there is an excellent prospect ofsurvival of both twins of each pair to leadnormal lives. Separation in cases of total verticalcraniopagus presents very great problems andthe observations on three personal cases set outabove describe an attempt to understand theseand solve them. Some problems-for example,
the maintenance of the cerebrospinal fluidcirculation-have no foundation. Others-scalpclosure, repair of the dural defect and protectionof the cerebrum in the absence of the cranialvault-can be solved. Understanding of thedeformities of the skull and brain has, it isbelieved, been achieved and this can be helpfulduring an attempt at separation. The abnor-mality of cerebral venous drainage has beendemonstrated and its embryological basissuggested. The importance of the circumferentialvenous sinus in those cases with a crossed venousdrainage (types II and III) has been indicated,and this knowledge makes possible preservationof the circulation through one brain. However,it has not been found possible to ensure thevenous drainage of the second child's cerebrumand consequently separation has only achievedone survivor. As has been seen, before the firstseparation operation, preparations for theinsertion of a vein graft from the frontal veinsof each child to its lateral sinus had been madebut the discovery of the circumferential sinuswas thought to make a graft unnecessary.Possibly this could be considered for the secondchild-that is, that without the circumferentialdural fold and its contained veins-in futureoperations, but the technical difficulties wouldbe great. Or it might be found possible to givehalf the circumferential sinus to one child andhalf to the other. A careful postmortem studyof twins with total vertical craniopagus in whomno attempt at separation had been made coulddemonstrate the exact relationship of thecircumferential to the lateral sinuses and showif such a sharing could be achieved. Anatomistshave long described the superior and inferioranastomotic cerebral veins. These connect thesuperficial middle cerebral vein, which drainsinto the cavernous sinus, to the superior sagittalsinus superiorly and the lateral sinus inferiorly.Such veins may be multiple in the adult and evenmore numerous in the fetus (O'Connell, 1934).It might be hoped that, in the absence of thesuperior sagittal sinus, blood might be drainedinferiorly through these anastomotic veins.However, it seems clear that the distortion ofthe cerebral hemispheres with anterosuperiorprojection of the frontal poles in each childcarries much of the venous drainage with it toits twin's lateral sinus. The problem has not
19
Protected by copyright.
on October 13, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.39.1.1 on 1 January 1976. Dow
nloaded from

J. E. A. O'Connell
been solved but recognition of a problem can bea step towards its solution. Such recognition hasresulted from the investigation and treatment ofthis personal series and it is hoped that this workwill provide other neurosurgeons with somelandmarks on the map of a largely unchartedterritory and lead to better results.The final great problem is the ethical one in the
treatment of total vertical craniopagus. Of thethree pairs of such twins dealt with personally,in the first one child died six months afteroperation and his brother survives aged 17years, without any gross neurological defect butretarded. Of the second pair, one died duringsurgery and the other when aged 6 years, beingseverely mentally deficient. Of the third pair,one again died during operation and the othernow aged 12 years, is an active, happy child witha marked left hemiparesis.The early fatality in each case resulted from the
cerebral venous circulatory impairment in thistwin of the pair explained above-and nosolution to this problem has so far been dis-covered. Can it then be justified to embark upona separation operation when death of one of thechildren seems inevitable? Before attempting toanswer this question the possibilities which existfor such children and their parents should becarefully considered. It must be stressed againthat apart from the union, which is a superficialone of scalp, skull, and dura mater, these infantsmay appear entirely normal, developing nor-mally from all points of view during the earlymonths after their birth. Indeed, there are reportsof such children being cared for at home by theirmothers at this stage. The children are in nosense monsters but the situation occasioned bythe junction is a monstrous one.
It must be recalled that the embryonicduplications which result from the splitting of asingle fertilized ovum are of several types. Whenthe results of the splitting are free and sym-metrical, identical twins result; but if asym-metrical, only one twin is normal and the other(acardius) depends upon it for its circulation.When the twins are joined they too may besymmetrical and each component a completeindividual; this is the group ofwhich craniopagusis a variety; the other members of it differ in thesite of the junction. When the components aresymmetrical and each less than a complete
individual-for example, bifurcation of thecranial or caudal end of the products of develop-ment-the term 'double monster' can appro-priately be used and, of course, there is nopossibility of surgical treatment here. When thejoined twins are unequal, one is a parasite withinor on the surface of the other. It will be seen thatthe present paper deals with the types of con-joined twins in which the components aresymmetrical and each a complete individual.There are three possible courses open to those
faced with the problem of total vertical cranio-pagus. Firstly, the twins may be allowed to dieat birth; secondly, they may be allowed todevelop in their united state; or, thirdly, anattempt may be made to separate them.As far as the first possibility is concerned, it
must be stressed that these infants can, apartfrom their union, with proper postnatal caredevelop into attractive babies. There is noquestion of unwarranted enthusiastic and ener-getic measures being required to ensure theirsurvival. Those who criticize attempts atseparation do so on the grounds that this is amisguided attempt to secure the survival of theunfit; they consider that the children should beallowed to die at birth. Such a view may seemrational in the abstract; it is a different matterwhen the surgeon is presented with the real lifeproblem. Partial craniopagus should always betreated surgically and with good prospects ofsaving both children to lead normal lives. In totalvertical craniopagus, with the knowledge whichhas now accumulated, it is clear that one childhas a prospect of survival after surgery. This willmake the suggestion that both be allowed to dieunacceptable to many. While at the present timethe survivor is left with defects, the possibility ofa worthwhile life exists for it. It is to be expectedthat improvements in technique will diminishthese defects and, indeed, in time may make thesurvival of both children a possibility.The second possibility-permitting the twins
to develop in their united state-derserves morecareful consideration. This course has beenfollowed in the past with survival of the twinsinto adult life. The union thus may constituteno threat to existence but what is the quality oflife of those so united? Much of it must bepassed in the horizontal position with strictlimitations as to the amount of possible rotation
20
Protected by copyright.
on October 13, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.39.1.1 on 1 January 1976. Dow
nloaded from

Crantiopagus twins: surgical aniatomy and embryology and their implications
to either side. Some examples of type I cranio-pagus have been trained to stand and walk butwith obvious difficulties and for limited periods;in types lI and III these difficulties would clearlybe increased. Such children can learn but thelimitations on the ability of each adequately toexplore its environment and respond normallyto stimuli of various types brings about an earlyfalling behind for their age group in the per-formance of psychological tests. Moreover, it isbelieved that each of the brains in the commoncranium, by displacing, compressing, and de-forming one another, contributes to defectiveintellectual development. Detailed reports of thecondition of such surviving twins are rarelypublished. A recent one (Todorov et al., 1974)described 24 year old craniopagus twins (type I).These showed gross intellectual retardation andeducation was virtually impossible. Such aban-donment of the twins to their appalling bondageis not, of course, in any sense a treatment;indeed, it ignores the fact that on physicalgrounds alone the union itself will lead tocontinued deterioration of intellect, at least forsome years after birth. The third possibility is toattempt surgical separation, and this is a majorundertaking. A thorough investigation to reviewthe intracranial anatomy in both twins willrequire many months for its completion andduring this period every effort must be made toovercome the physical and psychological handi-caps which the union can produce. The surgicalprocedure is a prolonged one, involving a largeteam. The measure of success achieved has beensmall-one long-term survivor from each pairand all with defects, neurological or intellectual.The early fatality after each operation resultedfrom cerebral venous circulatory impairment inthis twin of the pair. No solution for this problemhas been found in types II and III craniopagus,though possibly this disturbance of circulationmay be less likely in type I cases; however, nosuch case has been dealt with personally. In thepresent state of knowledge, then, surgicalseparation of the twins entails sacrifice of onechild in the hope of achieving survival and abetter life for the other. The decision to operateis thus a difficult and even agonizing one. Ofcourse there must be full discussion of the prob-lem between the parents and the physiciansconcerned and there must be complete agreement
as to the proper course to take; this will almostinvariably be in favour of operation. However,it is for the surgeon himself to decide upon whatis for him the right course in each case. Thejustification for such an operation lies in theknowledge that in postnatal life the union retardsintellectual development by the limitation itplaces on mobility and on the other activities ofthe developing child. Moreover, the disturbanceof highest brain function is contributed to by thecompression and displacement of each child'sbrain by that of its twin, one brain acting as atumour in its relationship with the other. Tobreak the union and prevent this progressivedeterioration at the earliest possible time is aproper course of action. If, as is true up to thepresent time, there is only one survivor, the gainfor this child can be great in terms of quality oflife and it justifies the loss of the twin, since thesurvival of the pair in the united state offers littlemore than existence to both.
I am much indebted to the Department of MedicalIllustration of St. Bartholomew's Hospital for the verynumerous photographs of our material which wereessential to this review of our experience. Several of thedrawings are based on these photographs and I am grate-ful to Mr Peter Jack of the Department for the care hehas given to this work as well as to his other drawings.
REFERENCES
Baldwin, M., and Dekaban, A. (1958). The surgical separa-tion of Siamese twins conjoined by the heads (cephalopagusfrontalis) followed by normal development. Journal ofNeurology, Neuirosurgery, and Psychiatry, 21, 195-202.
Barbosa, A. (1949). Tentative surgery in a case of cranio-pagus. Revista Brasileira de Cirurgia, 18, 1047-1050.
Benirschke, K., and Kim, C. K. (1973). Multiple pregnancy.Newv Englanid Jouirnal of Medicine, 1276-1284 and 1329-1336.
Clark, W. E. (1920). On the Pacchionian bodies. Jolurnal ofAnatomy, 55, 40-48.
Du Boulay, G. H. (1964). Radiological examination of twopairs of craniopagus twins. British Medical Jouirnal, 1,1339-1341.
Franklin, A. W. (1964). Paediatric care of craniopagus twins.British Medical Journal, 1, 1342-1344.
Grossman, H. J., Sugar, O., Greeley, P. W., and Sadove,M. S. (1953). Surgical separation in craniopagus. Jouirnalof the American Medical Association, 153, 201-207.
Hamilton, W. J., and Mossman, H. W. (1972). HuimanEmbryology, p. 478 and p. 533, 4th edn. Heffer: Cambridge.
Jayes, P. H. (1964). Plastic repair after separation of cranio-pagus twins. British Medical Jouirnal, 1, 1 1 44-1146.
Klar, E. (1963). Zur Trennung der Cranioencephalopagen.Archiv fiOr Klinische Chirurgie, 304, 883-889.
21
Protected by copyright.
on October 13, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.39.1.1 on 1 January 1976. Dow
nloaded from

J. E. A. O'Connell
O'Connell, J. E. A. (1934). Some observations on thecerebral veins. Brain, 57, 484-503.
O'Connell, J. E. A. (1964). Investigation and treatment ofcraniopagus twins. British Medical Jouirnal, 1, 1333-1338.
O'Connell, J. E. A. (1968). An operation to separate cranio-pagus twins. British Journal of Surgery, 55, 841-850.
Potter, E. L. (1961). Pathology of the Foetus and Infant, 2ndedn. Year Book Publishers: Chicago.
Robertson, E. G. (1953). Craniopagus parietalis. Archives ofNeurology and Psychiatry (Chic.), 70, 189-205.
Sapinski, W. (1966). A case of craniopagus. Wf`iadonzo&ciLekarskie, 19, 1733-1734.
Streeter, G. H. (1918). The developmental alterations of thevascular system of the brain of the human embryo.Embryology, no. 24. Carnegie Institute: Washington.
Todorov, A. G., Cohen, K. L., Spilotro, V., and Landau, E.(1974). Craniopagus twins. Journal of Neurology, Neuiro-surgery, and Psychiatry, 37, 1291-1298.
Voris, H. C., Slaughter, W. B., Christian, J. R., and Cayia,E. R. (1957). Successful separation of craniopagus twins.Journal of Neurosurgery, 14, 548-560.
Wolfowitz, J., Kerr, E. M., Leven, S. E., Walker, D. H., andWetten, K. B. (1968). Separation of craniopagus twins.South African Medical Journial, 42, 412-424.
22
Protected by copyright.
on October 13, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.39.1.1 on 1 January 1976. Dow
nloaded from