Embed Size (px)
Citation preview

CRANIAL NERVESMatt Vreugde
What are Cranial Nerves?
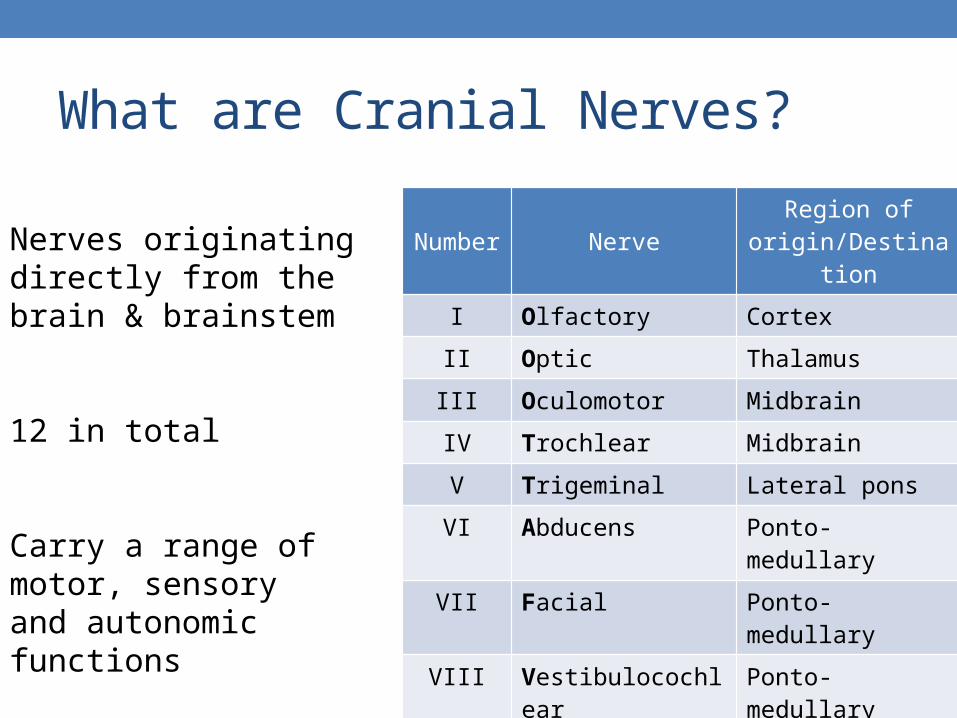
Number NerveRegion of
origin/Destination
I Olfactory Cortex
II Optic Thalamus
III Oculomotor Midbrain
IV Trochlear Midbrain
V Trigeminal Lateral pons
VI Abducens Ponto-medullary
VII Facial Ponto-medullary
VIII Vestibulocochlear Ponto-medullary
IX Glossopharyngeal Lateral medulla
X Vagus Lateral medulla
XI Accessory Spinal cord C1-C5
XII Hypoglossal Ventral medulla
Nerves originating directly from the brain & brainstem
12 in total
Carry a range of motor, sensoryand autonomic functions

CN I - Olfactory• Frequently gets damaged,
frequently regenerates
• Dysfunction = anosmia
• Ask “has there has been any change in your sense of smell or taste”?
• Test each nostril separately with familiar, non-pungent odours
SENSORY - Smell

CN II - Optic• Site of lesion determines
signs and symptoms
• Test if vision is intact in both eyes • acuity (snellen chart), visual
fields (direct confrontation), colour vision (ishihara plates), pupillary light reflexes, accommodation, fundoscopy.
• Learn the pathway, don’t forget left and right
SENSORY - Vision

CN III - Oculomotor• Superior, medial & inferior recti,
inferior oblique & levator palpebrae superioris
• Ciliary muscle – constrictor pupillae
• Test eye movements – H pattern
• Check for ptosis
• Look if pupils are equal and appropriately dilated
• Check for nystagmus (slow)
Motor – Eye & upper eyelid
Parasympathetic – Pupil constriction

CN IV & VI – Trochlear and Abducens
• Trochlear => Superior oblique
• Dysfunction can cause torsional diplopia and strabismus
• Abducens => lateral rectus
• Dysfunction causes inability to abduct eye
• Diplopia when looking towards side of affected eye
Motor – Eye Movement

CN V – Trigeminal
• Sensation:• Va – top of head, forehead and
ocular regions, bridge of the nose, nasal cavity, lacrimal glands, BLINKING!
• Vb – temple, lower eyelid, cheek and upper mandible (palate, upper pharynx, upper teeth and upper lip)
• Vc – lower jaw, lower face, side of head and ant 2/3 tongue, and floor of mouth
• Test by prodding the face or blowing into their eye
• Palpate maseter and temporalis and clench jaw
Sensory – Facial touch, pain and temp
Motor – Muscles of mastication, tensor
tympani

CN VII – Facial
• Lesions can be transient (Bell’s Palsy), ask patient to smile
• TEST: Eyebrows up, eyes shut, puff your cheeks, smile you….• Test against resistance
• Ask about taste changes, tinnitus/hyperacusis • (no, don’t yell in their ears)
Sensory – external acoustic meatus, taste to ant 2/3 tongue
Motor – Facial expression, stapedius, some muscles in neck
Parasymp – Lacrimal glands & Submandibular+sublingual glands
Two Zulus Bit My Cat

CN VIII – Vestibulocochlear
• If isolated sensorineural lesion think acoustic neuroma or other cerebellopontine angle tumour
• TEST: Rinne’s and Webers
• Ask about vertigo, difficulty with their balance etc.
Sensory – Hearing and Balance

CN IX – Glossopharyngeal
• Lesions can cause loss of taste and gag reflex ipsilaterally (sign, not symptom), dysphagia.
• Test together with vagus nerve
Sensory – Middle ear, pharynx, post 1/3 tongue taste & sensation
Motor – Stylopharyngeus & laryngeal muscles
Parasympathetic – Parotid GlandOther – Chemo and bareceptor
information from carotid bodies and sinus

CN X – Vagus
• “The wanderer”
• Test gag reflex (who doesn’t have one?), listen to voice, say AHHH & check uvula.
• Symptoms may be hoarse voice, dysphagia.
Sensory – larynx, oesophagus, bronchi, lungs, heart, foregut&midgut
Motor – Pharyngeal & laryngeal muscles, vocal cords
Parasympathetic – Heart, lungs, gastric system, abdominal viscera (foregut/midgut)
Other – Aortic body chemoreceptors and aortic arch baroreceptors

CN XI – Accessory
• Really anatomists?
• Easily damaged in neck surgery.• Check for wasting of trapezius
then ask patient to shrug shoulders and rotate neck against resistance
• Symptoms are weakness of shoulder and arm elevation, and weakness of head when turning.
• Remember your LMN (ipsilateral) and UMN (contralateral)
Motor – Spinal: SCM, upper trapezius
Cranial: Striated muscle of soft palate, pharyx
and larynx

CN XII – Hypoglossal
• Girl’s best friend
• To test, stick tongue out and assess. Wasting, fasciculations, power (push inside of cheek), is it deviating?
• Difficulty in chewing, speaking and swallowing. Patient will have atrophy of the tongue.
Motor – Tongue muscles