Embed Size (px)
Citation preview

5/7/2017
1
Cardio-Pulmonary Exercise TestingCardio-Pulmonary Exercise Testing
Madhav Swaminathan, MD, MMCiProfessor of AnesthesiologyDuke University Health SystemDurham, NC
Madhav Swaminathan, MD, MMCiProfessor of AnesthesiologyDuke University Health SystemDurham, NC
Disclosures
• None
Overview: What it isOverview: What it is
Rationale: Why we need itRationale: Why we need it
Process: How it is doneProcess: How it is done
InterpretationInterpretation
Clinical applicationsClinical applications
Key pointsKey points
Outline
Overview Rationale Process Interpretation Clinical applications Key points
• Functional ability– O2 supply to tissues
– CO2 clearance
• Stress on this system has predictive value
• Simulation of the surgical experience to test functional ability for stress tolerance
What is CPET?
CV CapacityCV Capacity InternalInternalExternalExternal
Overview Rationale Process Interpretation Clinical applications Key points
At a basic level
O2O2
CO2CO2
VQ Matching
• Exercise induces– Increase in ventilation
– Increase in perfusion
• Disease states will affect either or both
• Testing can detect mismatches
Must matchMust match
Overview Rationale Process Interpretation Clinical applications Key points
5/7/2017
2
IntegratedIntegrated
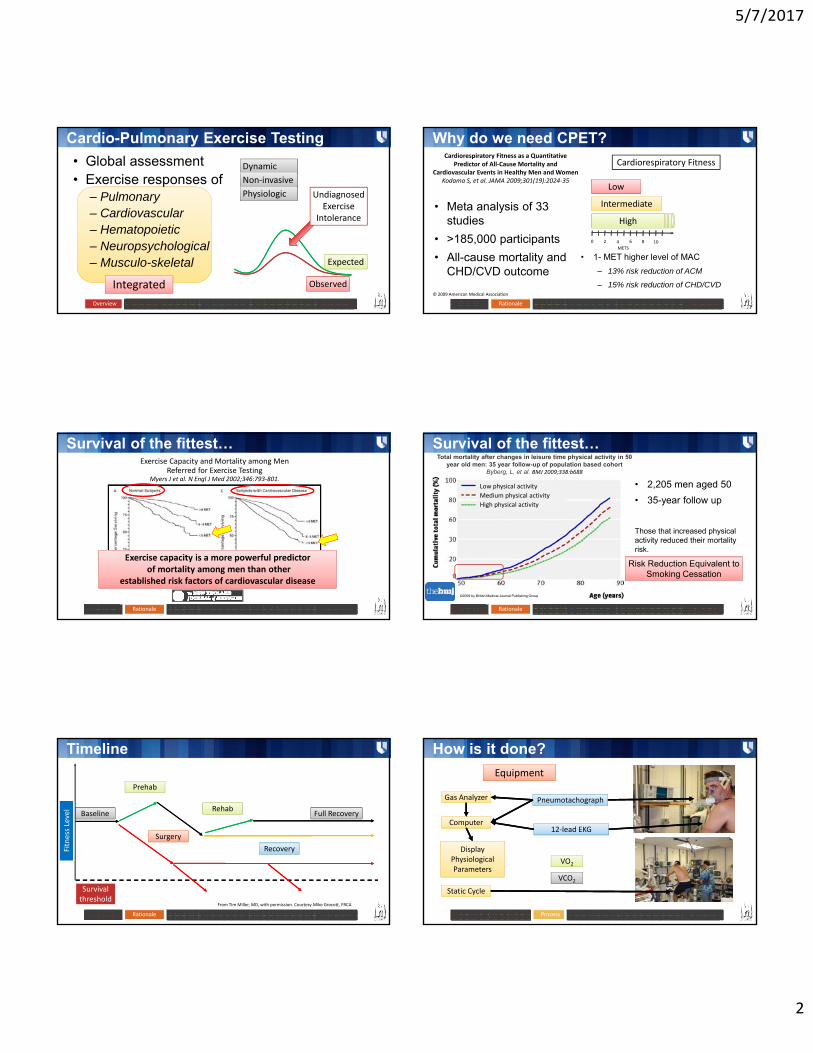
Cardio-Pulmonary Exercise Testing
• Global assessment• Exercise responses of
– Pulmonary– Cardiovascular– Hematopoietic– Neuropsychological– Musculo-skeletal
Overview Rationale Process Interpretation Clinical applications Key points
DynamicDynamic
Non‐invasiveNon‐invasive
PhysiologicPhysiologic
ObservedObserved
ExpectedExpected
Undiagnosed Exercise
Intolerance
Why do we need CPET?
• 1- MET higher level of MAC
– 13% risk reduction of ACM
– 15% risk reduction of CHD/CVD
Overview Rationale Process Interpretation Clinical applications Key points
Cardiorespiratory Fitness as a Quantitative Predictor of All‐Cause Mortality and
Cardiovascular Events in Healthy Men and WomenKodama S, et al. JAMA 2009;301(19):2024‐35
© 2009 American Medical Association
Cardiorespiratory Fitness
LowLow
IntermediateIntermediate
HighHigh
0 2 4 6 8 10
METS
• Meta analysis of 33 studies
• >185,000 participants
• All-cause mortality and CHD/CVD outcome
Survival of the fittest…
Overview Rationale Process Interpretation Clinical applications Key points
Years of follow up Years of follow up
Exercise Capacity and Mortality among Men Referred for Exercise Testing
Myers J et al. N Engl J Med 2002;346:793‐801.
Exercise capacity is a more powerful predictorof mortality among men than other
established risk factors of cardiovascular disease
Exercise capacity is a more powerful predictorof mortality among men than other
established risk factors of cardiovascular disease
Survival of the fittest…
Low physical activity
Medium physical activity
High physical activity
Overview Rationale Process Interpretation Clinical applications Key points
©2009 by British Medical Journal Publishing Group
Total mortality after changes in leisure time physical activity in 50 year old men: 35 year follow-up of population based cohort
Byberg, L, et al. BMJ 2009;338:b688
• 2,205 men aged 50
• 35-year follow up
Those that increased physical activity reduced their mortality risk.
Risk Reduction Equivalent to Smoking Cessation
Risk Reduction Equivalent to Smoking Cessation
Timeline
BaselineBaseline Full RecoveryFull Recovery
RecoveryRecovery
Survival thresholdSurvival threshold
SurgerySurgery
PrehabPrehab
RehabRehab
From Tim Miller, MD, with permission. Courtesy Mike Grocott, FRCA
Overview Rationale Process Interpretation Clinical applications Key points
Fitness Level
Fitness Level
How is it done?
Overview Rationale Process Interpretation Clinical applications Key points
EquipmentEquipment
Gas AnalyzerGas Analyzer
ComputerComputer
DisplayPhysiological Parameters
DisplayPhysiological Parameters
PneumotachographPneumotachograph
12‐lead EKG12‐lead EKG
VO2VO2
VCO2VCO2
Static CycleStatic Cycle

5/7/2017
3
How is it done?
Overview Rationale Process Interpretation Clinical applications Key points
EquipmentEquipment
Gas AnalyzerGas Analyzer
ComputerComputer
DisplayPhysiological Parameters
DisplayPhysiological Parameters
Static CycleStatic Cycle
How is it done?
Overview Rationale Process Interpretation Clinical applications Key points
EquipmentEquipment
Gas AnalyzerGas Analyzer
ComputerComputer
DisplayPhysiological Parameters
DisplayPhysiological Parameters
Static CycleStatic Cycle
• Breath‐by‐breath gas analysis–Oxygen uptake ‐ VO2
–CO2 production ‐ VCO2
• Graded exercise challenge–Treadmill vs. bike
• Peak Oxygen Consumption (VO2 max)• Anaerobic Threshold (AT)
Cardiovascular
Measurements
• Max aerobic capacity (VO2max)
• Anaerobic Threshold (AT)
• Oxygen Pulse (VO2/HR)
• Vent Equivalents (VE)
– Oxygen (VE/VO2)
– Carbon Dioxide (VE/VCO2)
Work RateWork Rate
HRHR
NIBPNIBP
Gas Exchange
Respiratory
VO2VO2
VCO2VCO2
SpO2SpO2
VTVT
VEVE
RRRR
Overview Rationale Process Interpretation Clinical applications Key points
CalculationsMaximal Aerobic Capacity
Work RateWork Rate
VO2VO2
VCO2VCO2
HRHR
NIBPNIBP
VTVT
VEVE
Gas Exchange
Cardiovascular
Respiratory
SpO2SpO2
RRRR
Overview Rationale Process Interpretation Clinical applications Key points
• Defines the limits of the CPS
• C.O x [C(a-v)O2]
• Max exercise has been performed AND
• Max effort has been given
• Implies limit of individual physiology
– Peak VO2 – exercise capacity in CVD
– MAC in apparently healthy
CalculationsVentilatory ThresholdWork RateWork Rate
VO2VO2
VCO2VCO2
HRHR
NIBPNIBP
VTVT
VEVE
Gas Exchange
Cardiovascular
Respiratory
SpO2SpO2
RRRR
Overview Rationale Process Interpretation Clinical applications Key points
• Submaximal index of exercise capacity
• VE increases exponentially relative to VO2
• VE required to eliminate CO2
• Point at which O2 requirements exceed supply – anaerobic metabolism begins –lactate production rises
• Occurs at approx. 45-65% VO2max
• Not under voluntary control. Not affected by psychological factors
CalculationsVentilatory ThresholdWork RateWork Rate
VO2VO2
VCO2VCO2
HRHR
NIBPNIBP
VTVT
VEVE
Gas Exchange
Cardiovascular
Respiratory
SpO2SpO2
RRRR
Overview Rationale Process Interpretation Clinical applications Key points
Lactate ThresholdLactate
Threshold
Anaerobic ThresholdAnaerobic Threshold

5/7/2017
4
CalculationsVentilatory ThresholdWork Rate
VO2
VCO2
HR
NIBP
VT
VE
Gas Exchange
Cardiovascular
Respiratory
SpO2
RR
Overview Rationale Process Interpretation Clinical applications Key points
Interpretation
Overview Rationale Process Interpretation Clinical applications Key points
CourtesyTim Miller, MD
Interpretation
Overview Rationale Process Interpretation Clinical applications Key points
Variable Normal Value
VO2Max >84% predicted
VT/AT >40% of VO2Max (up to 80%)
HR >90% age predicted
BP <220/90
O2 Pulse (VO2/HR) >80%
Resp Rate <60/min
VE/VCO2 (at VT) <34
PaO2 > 80 mm Hg
P(A‐a)O2 <35 mm Hg
In specific clinical settings
Overview Rationale Process Interpretation Clinical applications Key points
Measurement CHF COPD ILD Obesity Deconditioning
VO2Max ↓ ↓ ↓ ↓ for IBW ↓
VT ↓ N or ↓ N or ↓ N N or ↓
Peak HR Variable N or ↓ ↓ N or ↓ N or ↓
O2 Pulse ↓ N or ↓ N or ↓ N ↓
VE/VCO2 ↑ ↑↑ ↑ N N
PaO2 N Variable ↓ N or ↑ N
P(A‐a)O2 N Variable or ↑ ↑ ↓ N
Interpretation When to apply CPET?
Overview Rationale Process Interpretation Clinical applications Key points
• Exercise tolerance• CV disease• Respiratory disease• Preoperative evaluation• Pulmonary rehab• Disability assessment• Pre-thoracic transplant
• Triage postop location
• Predict complication risk
• Predict mortality
• Prehab
• Triage postop location
• Predict complication risk
• Predict mortality
• Prehab

5/7/2017
5
Survival/risk threshold
Overview Rationale Process Interpretation Clinical applications Key points
VT/AT NPeriop
Mortality
>11 ml/min/Kg 132/187 0.8%
<11 ml/min/kg 55/187 18%
<11 ml/min/kg + Ischemia
8/19 42%
• 187 elderly patients• Abdominal surgery• Overall mortality = 7.5%
0
10
20
30
40
50
60
70
80
90
<8 8‐10.9 11‐13.9 >14
VT and Survival
Non‐Survivors Survivors Older et al. Chest 1993; 104:101‐04
Triage Postop Location
Overview Rationale Process Interpretation Clinical applications Key points
0
1
2
3
4
5
6
7
8
9
10
5.1‐8 8.1‐11 11.1‐14 >14
Overall & CV Mortality
CV Mortality Non‐CV Mortality Older et al. Chest 1999; 116:355‐362
• 548 Patients > 60y
• Abdominal surgery
• Postop location (ICU/HDU/Ward) assigned on basis of preop VT+ischemia
• Mortality = 3.9%
• 548 Patients > 60y
• Abdominal surgery
• Postop location (ICU/HDU/Ward) assigned on basis of preop VT+ischemia
• Mortality = 3.9%
Older et al. Chest 1999; 116:355‐362
CPET result Postop location %
AT <11 ICU 28
AT >11 with either myocardial ischemia
or VE/VO2 > 35
HDU 21
All other patients General ward 51
• 21 died (19 were triaged to either ICU/HDU)
• 14/19 had VT<11
• 0% CV mortality among ward admissions
• 21 died (19 were triaged to either ICU/HDU)
• 14/19 had VT<11
• 0% CV mortality among ward admissions
Triage Postop Location
Overview Rationale Process Interpretation Clinical applications Key points
Predict Risk/Complications
2
Cardiorespiratory Fitness Predicts Mortality and Hospital Length of Stay After Major Elective
Surgery in Older People.Snowden et al.
Ann Surg. 257(6):999‐1004, June 2013.
© 2013 Lippincott Williams & Wilkins, Inc. Published by Lippincott Williams & Wilkins, Inc.
FIGURE 2 . Age, fitness, and mortality rates from hepatobiliary surgery in 389 patients (Fit = Anaerobic Threshold >10 mL/kg/min, Unfit = Anaerobic Threshold <10 mL/kg/min).
Overview Rationale Process Interpretation Clinical applications Key points
• 389 Patients mean 66y
• Hepato-biliary surgery
• VT/AT was most significant predictor of mortality
• Normal card-pulm fitness – same hospital or ICU LOS regardless of age
• Old + unift = highest LOS and mortality
Does intervention improve outcome?
2
Effects of presurgical exercise training on cardiorespiratory fitness among patients undergoing
thoracic surgery for malignant lung lesionsJones, LW, et al.
Cancer. 2007; 110(3):590–598
Overview Rationale Process Interpretation Clinical applications Key points
• 25 patients with operable lung cx
• 5 endurance sessions @ 60-
100% Peak VO2
• CPX at baseline, immed before
and 30d after surgery
• Modest increase in peak VO2
• Some benefit in those who had >80% adherence
• Fitness level decreased after surgery, but not below baseline
• Modest increase in peak VO2
• Some benefit in those who had >80% adherence
• Fitness level decreased after surgery, but not below baseline
Lung cancerLung cancer
Does intervention improve outcome?
2
Therapeutic Validity and Effectiveness of Preoperative Exercise on Functional Recovery after Joint
Replacement: A Systematic Review and Meta‐AnalysisHoogeboom, TJ, et al. PLOS One 7(5): e38031
Overview Rationale Process Interpretation Clinical applications Key points
• 737 patients from12 trials
• Resistance, aerobic or functional
exercise in TKR and THR
• 2.5 times/week x 6 weeks
• No beneficial effects on postop functional recovery
• Therapeutic validity of exercise regimes was questionable
• Poor quality data
• Larger trials needed…
• No beneficial effects on postop functional recovery
• Therapeutic validity of exercise regimes was questionable
• Poor quality data
• Larger trials needed…
Total Joint ReplacementTotal Joint
Replacement

5/7/2017
6
Does intervention improve outcome?
2
Impact of preoperative change in physical function on postoperative recovery: Argument supporting
prehabilitation for colorectal surgeryMayo NE, et al.
Surgery 2011. 150(3): 505‐514
Overview Rationale Process Interpretation Clinical applications Key points
• Reanalysis of a prehab RCT
• Primary outcome - 6MWT
• Secondary outcomes – mental health/complications
• 95 patients completed prehab
• 75 also assessed postop (9 w)
Colorectal surgeryColorectal surgery
Does intervention improve outcome?
2Overview Rationale Process Interpretation Clinical applications Key points
• 33% improved
• Mental health, exercise capacity
• Women less likely to improve
• Preop improvement more likely to return to baseline
• 29% deteriorated – more complications
• “Meaningful” changes in functional capacity achieved
• Those with poor capacity should consider prehab
• 33% improved
• Mental health, exercise capacity
• Women less likely to improve
• Preop improvement more likely to return to baseline
• 29% deteriorated – more complications
• “Meaningful” changes in functional capacity achieved
• Those with poor capacity should consider prehab
Colorectal surgeryColorectal surgeryImpact of preoperative change in physical function on
postoperative recovery: Argument supporting prehabilitation for colorectal surgery
Mayo NE, et al. Surgery 2011. 150(3): 505‐514
Does intervention improve outcome?
2
The effects of preoperative exercise therapy on postoperative outcome: a systematic review
Valkenet, K et al. Clinical Rehabilitation. 2011;25(2):99‐111
Overview Rationale Process Interpretation Clinical applications Key points
• 12 studies – JR (n=7),
abdominal (n=1),
cardiac (n=4)
• Methodological quality
rated using PEDro
scale
• Preop Exercise: improves LOS in Card/Abd, not in JR
• Inspiratory muscle training: reduces postop pulm complications
• Use intervention in targeted manner
• Preop Exercise: improves LOS in Card/Abd, not in JR
• Inspiratory muscle training: reduces postop pulm complications
• Use intervention in targeted manner
Overall?Overall?
How do you get one for your patient?
• Order the CARD Cardiopulmonary Stress Test
• Call 919-684-2080 to schedule
• Managed by CDU
2Overview Rationale Process Interpretation Clinical applications Key points
How do you get one for your patient?
• Order the CARD Cardiopulmonary Stress Test
• Call 919-684-2080 to schedule
• Managed by CDU
2Overview Rationale Process Interpretation Clinical applications Key points
Equipment
https://www.davismedical.com/Products/T2100‐Treadmill‐for‐GE‐Stress‐Monitors__GER‐TRE‐T2100.aspx
GE T2100 Treadmill. (GE Inc)
VIAsprint™ 150P and Ergoselect 600 Recumbent Ergometer (BD Inc, NJ)
http://www.carefusion.com/our‐products/respiratory‐care/metabolic‐carts‐cpet‐and‐energy‐expenditure/exercise‐accessories/viasprint‐150p‐bicycle
http://www.carefusion.com/our‐products/respiratory‐care/metabolic‐carts‐cpet‐and‐energy‐expenditure/metabolic‐carts/vmax‐encore‐metabolic‐cart
Vmax® Encore Metabolic Cart with complete PFT system (BD Inc, NJ)
2Overview Rationale Process Interpretation Clinical applications Key points

5/7/2017
7
Report
2Overview Rationale Process Interpretation Clinical applications Key points
Peri-Operative Enhancement Team (POET)
CPETCPET
Take home points
• Preoperative functional capacity is a
powerful predictor of adverse outcome
• CPX testing can detect subtle and overt
reductions in functional capacity
• Interventions have yielded marginal results
• Reductions in LOS and complications in
selected groups have offered hopehttp://learningradiology.com/graphics/takehomepoint.gif
2Overview Rationale Process Interpretation Clinical applications Key points
Recommended reading1. Balady GJ, et al. Clinician's Guide to cardiopulmonary exercise testing in adults: a
scientific statement from the American Heart Association. Circulation. 2010 Jul 13;122(2):191-225.
2. American Thoracic Society, American College of Chest Physicians. ATS/ACCP Statement on cardiopulmonary exercise testing. Am J Respir Crit Care Med. 2003 Jan 15;167(2):211-77.
3. Forman DE, et al. Cardiopulmonary exercise testing: Relevant but under used. Postgrad Med. 2010 Nov;122(6): 68-66.
4. Arena R, et al. Ordering a cardiopulmonary exercise test for your patient: Key considerations for the physician. Future Cardiol. 2011 Jan;7(1):55-60.
5. Ridgway ZA, et al. Cardiopulmonary exercise testing: a review of methods and applications in surgical patients. Eur J Anaesthesiol. 2010 Oct;27(10):858-65.
Thank you!
Special thanks to Tim Miller, MDSpecial thanks to Tim Miller, MD





























