Embed Size (px)
Citation preview
Covid 19 (Sars Cov 2)Presentazione 02.09.2020Prospettiva Pneumologica

Sars Cov 2SARS-CoV-2 (2019-nCoV) is a respiratorycoronavirus that causes the disease COVID-19
Aerosol transmission was a dominant contributor to COVID-19 infection. A more comprehensiveepidemiological analysis (Emerg Infect Dis 2020 Aug 21;26(11)) suggested that transmission waslikely a common source event and due to closecontact

Transmission is highly efficient:
Droplet is the primary mode of transmission is mostsettings.
Airborne/aerosol transmission possible, but probably notthe primary mechanism in most settings (see JAMA 2020 Jul 13. doi: 10.1001/jama.2020.12458)
with potential for transmission from aerosol generatingprocedures such as nasophayngeal swab sampling, intubation, invasive and non-invasive ventilation, nebulizers, high-flow oxygen nasal cannula, bronchoscopy

Prevention measures
Systematic review and meta-analysis (Lancet, published online June 1, 2020) of social distancing, N95 respirators, surgical masks, eyeprotection in community and healthcare settings indicates that each
provides a level of protection against COVID-19.
Frequent handwashing (alcohol-based sanitizer and/or soap and water)
Sanitize common surfaces

Community responsibility
Social distancing (1m somewhat protective, at least 6 feet / 1.8 meterpreferred)
WEAR A FACE MASK IN PUBLIC WHEN IN THE PRESENCE OF OTHERS: Protective of yourself and others by preventing spread of nasal/respiratory droplets
AVOID CROWDS, CONGESTED PLACES, particularly indoor spaces(restaurants, bars, churches), which continue to be transmission focalpoints
Respiratory hygiene, i.e., cover nose and mouth when sneezing or coughing
Avoid touching eyes, nose, mouth

Healthcare Personnel
Personal protective equipment (PPE) when caring for a patient with COVID-19
Patients not undergoing aerosol generating procedures: N95 respiratorpreferred, surgical mask acceptable; face shield, gown, gloves
Patient undergoing nasopharyngeal swab, aerosol generatingprocedures: N95 respirator or PAPR, face shield, gown, gloves

Presentation / symptoms:
Common presenting signs and symptoms (See CDC listing of symptoms):headache, arthralgias / myalgias, fatigue. fever. cough, shortness of breath, loss of taste and/or smell, nausea / vomiting, diarrhea, sore throat, "fuzzythinking", deliriumOne week to 10 days prodrome, which may progress to difficulty breathing atany time, often in the second week.Average 8 days to development of dyspnea and average 9 days to onset of pneumonia/pneumonitis.Key presentation vitals (at triage): temp > 38ºC (30.7%), O sat < 90% (20.4%), heart rate > 100 beats/min (43.1%)Approximately 15% of patients will develop severe disease with 5% requiringmechanical ventilation.
Testing Recommendations
Asymptomatic individuals with recent known or suspected exposure to SARS-CoV-2 to control transmission.
Individuals with signs or symptoms consistent with COVID-19
Asymptomatic individuals without known or suspected exposure to SARS CoV-2 in special settings that can lead to rapid spread (e.g., long-term care facilities, correctional/detention facilities, homeless shelters,
congregate work or living settings)
Selected individuals being tested to determine resolution of infection (e.g., test-based strategy for early return to work for healthcare providers, immunocompromised patients)
Individuals being tested for purposes of public health surveillance for SARS-CoV-2

RT-PCR and nucleic acid amplification testsFor diagnosis of active COVID-19 infection (See IDSA Guidelines athttps://www.idsociety.org/practice-guideline/covid-19-guideline-diagnostics; excellent review of current state of diagnostic testing in AnnIntern Med 2020;172:726;
Specimen: upper respiratory nasopharyngeal (NP) swab preferred (seeCDC interim guidelines (above) and JAMA 2020 Mar 11. doi: 10.1001/jama.2020.3786 for yields of different specimen types).
Test kits: The U.S. FDA has issued Emergency Use Application (EUA) letters for a growing list of SARS CoV-2 / COVID-19 diagnostic tests. Accuracy and/or reliability remains highly variable.
TreatmentPrimary Regimens
Patients with hypoxia
Remdesivir (U.S. FDA Emergency Use Authorization 05/01/2020) (SeeComments and provider Fact Sheet). Randomized trial demonstratingefficacy (for possible remdesivir drug-drug interaction, see Remdesivir)
Adult dosing (wt > 40 kg): 200 mg IV loading dose on day 1, then 100 mg IV daily maintenance dose
Infuse each dose over 30-120 min
5 day course if not on ventilation/ECMO. If no clinical improvement at 5 days, extend to 10 days
10 day course for patients on mechanical ventilation/ECMO

Dexamethasone (see Comments)
6 mg once daily IV or po x 10 days for patients on supplemental oxygenor receiving mechanical ventilation
Do not use in patients who do not require supplemental oxygen or mechanical ventilation: no benefit, possible harm (see Comments).

Critical Care Considerations
Critical illness, hospitalized in ICU, on mechanical ventilation. For suuggestedinterventions see NIH COVID-19 Treatment GuidelinesFluids: balanced crystalloidsPressors: norepi > vasopression/epi; cardiogenic shock - dobutamine; notdopamineSteroids:Refractory shock: consider low dose hydrocortisoneDexamethasone: see Primary Regimens aboveAnti-inflammatory: acetaminophen and/or ibuprofenAnti-thrombolytic therapy guidelines hereAntiviral therapy for SARS CoV-2: Remdesivir (See Primary Regimens, above)
Laboratory Testing:
In non-hospitalized patients with COVID-19, there are currently no data to support the measurement of coagulation markers (e.g., D-dimers, prothrombin time, platelet count, fibrinogen) (AIII).
In hospitalized patients with COVID-19, hematologic and coagulation parameters are commonly measured, although there are currently insufficient data to recommend for or against using this data to guide management decisions (BIII).

Chronic Anticoagulant and Antiplatelet Therapy:
• Patients who are receiving anticoagulant or antiplatelet therapies for underlying conditions should continue these medications if theyreceive a diagnosis of COVID-19 (AIII).
Venous Thromboembolism Prophylaxis and Screening:
For non-hospitalized patients with COVID-19, anticoagulants and antiplatelet therapy should not be initiated for prevention of venousthromboembolism (VTE) or arterial thrombosis unless there are otherindications (AIII).
Hospitalized adults with COVID-19 should receive VTE prophylaxis per the standard of care for other hospitalized adults (AIII). A diagnosis of COVID-19 should not influence a pediatrician’s recommendations about VTE prophylaxis in hospitalized children (BIII). Anticoagulant or antiplatelettherapy should not be used to prevent arterial thrombosis outside of the usual standard of care for patients without COVID-19 (AIII

Treatment:
Patients with COVID-19 who experience an incident thromboembolicevent or who are highly suspected to have thromboembolic disease ata time when imaging is not possible should be managed with therapeutic doses of anticoagulant therapy as per the standard of care for patients without COVID-19 (AIII).
Patients with COVID-19 who require extracorporeal membrane oxygenation or continuous renal replacement therapy or who havethrombosis of catheters or extracorporeal filters should be treated with antithrombotic therapy per the standard institutional protocols for those without COVID-19 (AIII).

Infection with the novel coronavirus SARS-CoV-2 and the resulting syndrome coronavirus disease (COVID-19) hasbeen associated with inflammation and a prothromboticstate, with increases in fibrin, fibrin degradationproducts, fibrinogen, and D-dimers.1,2 In fact, thesemarkers have been associated with worse clinicaloutcomes.3,4 Although the true incidence of thesecomplications among those with different severities of disease is not completely defined, there have beenreports of increased incidence of thromboembolicdisease associated with COVID-19 in patients in the intensive care unit (ICU).

Co-infection (Lancet Microbe online 24 Apr 2020, Cleve Clin J Med online May 2020)
Bacterial and fungal co-infection
Meta-analysis of 28 studies (22 from China, 2 US, 1 UK, I Spain, 1 Singapore, 1 Thailand) with 3448 hospitalized patients between 12/25/19 and 3/31/20 (ClinMicrobiol Infect 220; Jul 22;S1198-
743X(20)30423-7): Overall bacterial infection rate of 7.1% with 3.5% of patientsinfected at presentation and with 15.5% of patients developing secondarybacterial infections over the course of illness.
Rates of infection in critically ill patients and fatal cases were 8.1% and 11.6%, respectively. 71% of patients received systemic antibacterial therapy. Mostcommon bacterial species (n=41 total)
identified in infected patients were Mycoplasma spp. (29.3%), Haemophilusinfluenzae (19.5%), Pseudomonas aeruginosa (12.2%), Enterobacteriaceae(30%).
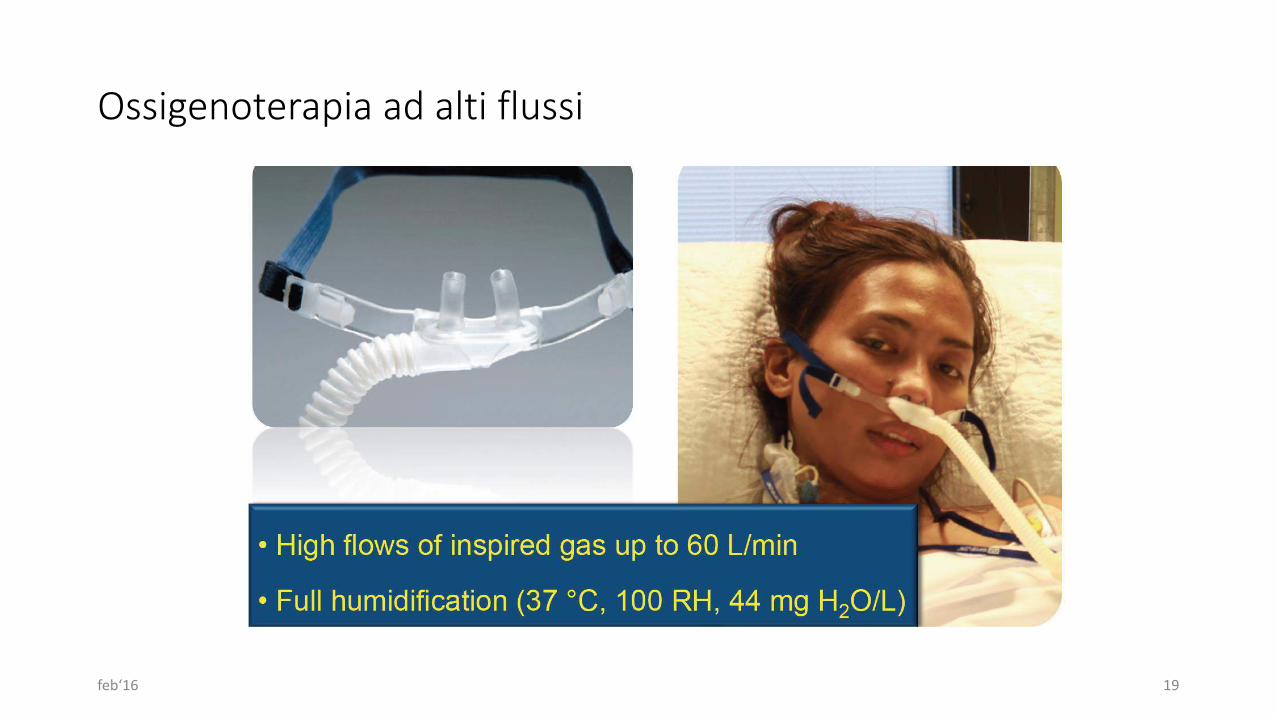
Ossigenoterapia ad alti flussi
feb‘16 19

HFOT vs ossigenoterapia convenzionale: Erogazione più stabile e accurata di ossigeno
feb‘16 20

HFOT: come funziona
• Effetto sul Vt
• Effetto sulla frequenza respiratoria
• Riduzione dello spazio morto
• Aumento della pressione di fine espirazione
• Aumento del volume telespiratorio polmonare
feb‘16 21

Ct scan
The detection of COVID-19 chest CT imaging is very high among symptomatic individuals at high risk, especiallyusing thin-section chest CT. The most common CT features in patients affected by COVID-19 includedground glass opacities and consolidation involving the bilateral lungs in a peripheral distribution.

Gattinoni Based on detailed observation of several cases and
discussions with colleagues treating these patients, we
hypothesize that the different COVID-19 patterns found
at presentation in the emergency department depend on
the interaction between three factors: (1) the severity of
the infection, the host response, physiological reserve and
comorbidities; (2) the ventilatory responsiveness of the
patient to hypoxemia; (3) the time elapsed between the
onset of the disease and the observation in the hospital

COVID-19 pneumonia, Type LAt the beginning, COVID-19 pneumonia presents with
the following characteristics: Low elastance. The nearly normal compliance indicates
that the amount of gas in the lung is nearly normal
Low ventilation-to-perfusion (VA/Q) ratio. Since the gas volume is nearly normal, hypoxemia may be bestexplained by the loss of regulation of perfusion and
by loss of hypoxic vasoconstriction. Accordingly, at this stage, the pulmonary arterypressure should be near normal.
Low lung weight. Only ground-glass densities are present on CT scan, primarily locatedsubpleurally and along the lung fissures. Consequently, lung weight is
only moderately increased.
Low lung recruitability. The amount of non-aerated tissue is very low; consequently, the recruitability is low [5].
The possible key feature
which determines the evolution of the disease, other than
the severity of the disease itself, is the depth of the negative
intrathoracic pressure associated with the increased
tidal volume in spontaneous breathing. Indeed, the combination
of a negative inspiratory intrathoracic pressure
and increased lung permeability due to inflammation
results in interstitial lung edema.
COVID-19 pneumonia, Type HThe Type H patient:
•• High elastance. The decrease in gas volume due to increased edema accounts for the increased lung elastance.
•• High right-to-left shunt. This is due to the fraction of cardiac output perfusing the non-aerated tissuewhich develops in the dependent lungregions due to the increased edema and superimposed pressure.
•• High lung weight.
Quantitative analysis of the CT
scan shows a remarkable increase in lung weight
(> 1.5 kg), on the order of magnitude of severe ARDS
•• High lung recruitability. The increased amount of non-aerated tissue isassociated, as in severe ARDS, with increased recruitability

The Type H pattern, 20–30% of patients in our series,
fully fits the severe ARDS criteria: hypoxemia, bilateral
infiltrates, decreased the respiratory systemcompliance,
increased lung weight and potential for recruitment.

The first step to reverse hypoxemia is through an
increase in FiO2 to which the Type L patient responds
well, particularly if not yet breathless.

In Type L patients with dyspnea, several noninvasive
options are available: high-flow nasal cannula
(HFNC), continuous positive airway pressure (CPAP)
or noninvasive ventilation (NIV). At this stage, the
measurement (or the estimation) of the inspiratory
esophageal pressure swings is crucial [13].

The magnitude of inspiratory pleural pressures
swings may determine the transition from the Type
L to the Type H phenotype. As esophageal pressure
swings increase from 5 to 10 cmH2O—which are
generally well tolerated—to above 15 cmH2O, the
risk of lung injury increases and therefore intubation
should be performed as soon as possible.

Once intubated and deeply sedated, the Type Lpatients, ifhypercapnic, can be ventilated with volumes greater than6 ml/kg (up to 8–9 ml/kg), as the high compliance resultsin tolerable strain without the risk of VILI. Prone positioning should be used only as a rescue maneuver, asthe lung conditions are “too good” for the prone position effectiveness, which is based on improved stress and strainredistribution. The PEEP should be reduced to 8–10 cmH2O, given that the recruitability is low and the risk of hemodynamic failure increases at higher levels. An earlyintubation may avert the transition to Type H phenotype

Type H patients should be treated as severe ARDS,
including higher PEEP, if compatible with hemodynamics,
prone positioning and extracorporeal support.
Terapia inalatoria
Va proseguita la terapia in attoOccorre evitare la nebulizzazioneMDI Dpi SMI sono da preferire
Danni Cronici
Bassa incidenza di danni permanenti nel polmone, in genere secondari a barotraumi per intubazione o ventilazione meccanica.

Follow up
Indispensabile l’organizzazione di follow up clinici e funzionali respiratori.I nostri dati sono favorevoliCritica ed indispensabile l’abolizione del tabagismo
Vaccinazioni
Indispensabile la vaccinazione antipneumococcica dapprima con prevenar 13 e successivamente con PneumovaxVaccinazione antinfluenzale Vaccinazione specifica per Sars Cov 2 appena disponibile