Embed Size (px)
Citation preview
1
June 5th, 2020
COVID-19 Physician Town Hall
2
ReflectionDave Hurter, VP of Governmental Programs and Alternative Payment Methods
Mark Collins, CIN Medical Director
3
In the stillness of your presence, you can feel your own formless and timeless reality as the
unmanifested life that animates your physical form. You can then feel the same life deep within
every other human and every other creature. You look beyond the veil of form and separation.
This is the realization of oneness. This is love. ~ Eckhart Tolle

4
9 Minutes of SolidarityCheck with your local CMO to see where the gathering is occurring.
5
Opening RemarksDon Franke, SVP, Population Health and CEO, AMITA Health Care Networks
6
These physician town halls are offered for all
AMITA Health physicians —independent, CIN and
Medical Group.
The content for each session is developed in
conjunction with AMITA physician leaders.
Topics are identified based on calls to the AMITA
COVID physician hotline and through contact with
AMITA physician leadership.
Please let us know what topics you would like
covered in future sessions and encourage your
colleagues to join.
7
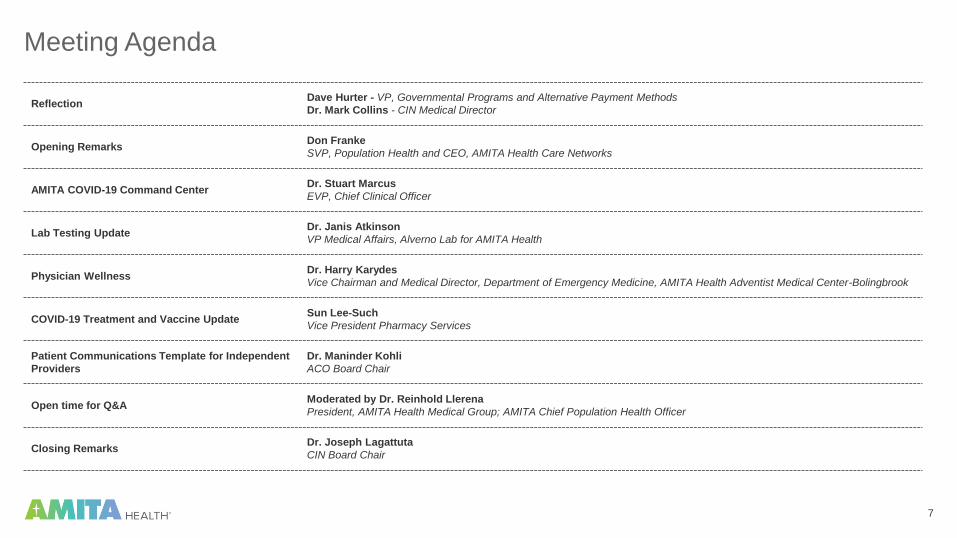
Meeting Agenda
ReflectionDave Hurter - VP, Governmental Programs and Alternative Payment Methods
Dr. Mark Collins - CIN Medical Director
Opening RemarksDon Franke
SVP, Population Health and CEO, AMITA Health Care Networks
AMITA COVID-19 Command CenterDr. Stuart Marcus
EVP, Chief Clinical Officer
Lab Testing UpdateDr. Janis Atkinson
VP Medical Affairs, Alverno Lab for AMITA Health
Physician WellnessDr. Harry Karydes
Vice Chairman and Medical Director, Department of Emergency Medicine, AMITA Health Adventist Medical Center-Bolingbrook
COVID-19 Treatment and Vaccine UpdateSun Lee-Such
Vice President Pharmacy Services
Patient Communications Template for Independent
Providers
Dr. Maninder Kohli
ACO Board Chair
Open time for Q&AModerated by Dr. Reinhold Llerena
President, AMITA Health Medical Group; AMITA Chief Population Health Officer
Closing RemarksDr. Joseph Lagattuta
CIN Board Chair

8
Physician Hotline Phone Number
224.273.3900 from 8am to 5pm weekdays for the foreseeable future
Physician Hotline Email
Additional Resources & Playbooks Online
AMITAhealth.org/covid-19-AMITA
AMITA Health COVID-19 Physician Resources

9
Submit Questions Via WebEx Q&A BoxUtilize the Q&A functionality through WebEx on your computer or through the mobile app to submit questions
for the Q&A portion of the agenda.
Computer WebEx App Mobile WebEx App

10
AMITA COVID-19 Command Center Dr. Stuart Marcus, EVP, Chief Clinical Officer

11
AMITA Health COVID-19 Daily Dashboard
Updated: June 4th, 2020

12
Re-emergence Trends Week 1-4Data through June 3rd, 2020, with re-emergence having begun May 11th.
ED Visits Trend IP Surgery Trend
OP Surgery TrendAcute IP Admissions
13
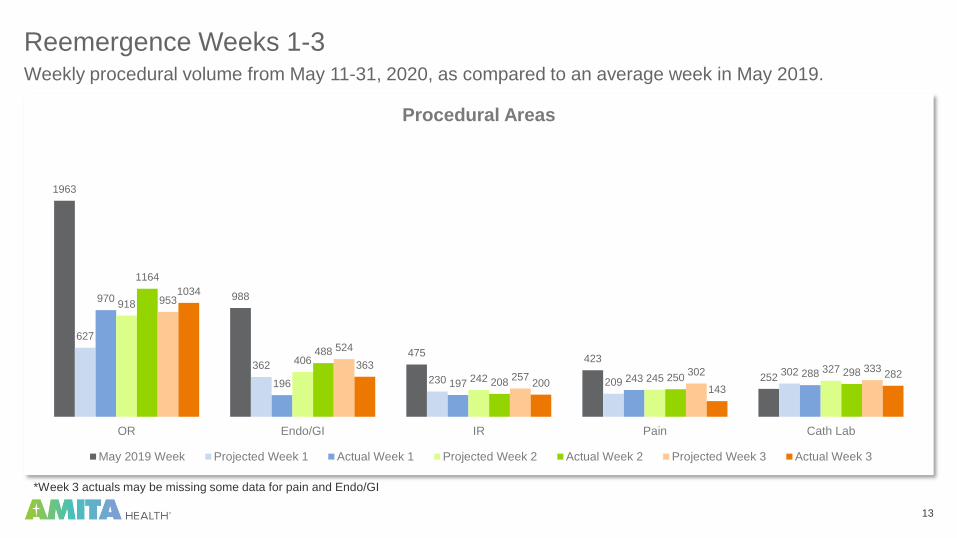
Reemergence Weeks 1-3Weekly procedural volume from May 11-31, 2020, as compared to an average week in May 2019.
*Week 3 actuals may be missing some data for pain and Endo/GI
1963
988
475423
252
627
362
230 209302
970
196 197243 288
918
406
242 245327
1164
488
208 250298
953
524
257 302 333
1034
363
200143
282
OR Endo/GI IR Pain Cath Lab
Procedural Areas
May 2019 Week Projected Week 1 Actual Week 1 Projected Week 2 Actual Week 2 Projected Week 3 Actual Week 3
14
Lab Testing UpdateDr. Janis Atkinson, VP Medical Affairs, Alverno Lab for AMITA Health

15
Turn Around Times: COVID 19 PCR Hours
0
10
20
30
40
50
60
70
25-May 26-May 27-May 28-May 29-May 30-May 31-May 1-Jun 2-Jun 3-Jun
Missed Reagent Delivery Due to Road Blockage
(Historical Note: Our TAT was 4-6 days from ARUP /IDPH on March 16)

1616
Alinity M
Now Online

17
New Test at Core Lab
• Interleukin-6 (IL-6)• A cytokine which is often elevated in severe cases of
COVID-19
• Correlates with pulmonary involvement, fever, CRP,
Ferritin and D-Dimer
• Can be used in the assessment of patients for Actemra
therapy
• Will be available next week at the Core Lab with a 12-24
hour Turn around time
18
Update on R and D Team Studies at Alverno
• Nasal collection method has been validated
• Either Nasal or NP Swabs acceptable for testing
• With this change, outpatient labs and Alverno service centers can support current drive-
through NP collections
Nasal swab versus NP swab for High Sensitivity COVID-19 PCR:

19
AMITA Health Regional Drive-Thru Test and Respiratory CentersAMITA Health is offering drive-through COVID-19 testing, as well as comprehensive respiratory assessments
in a safe, controlled environment for physicians, support staff, associates, and patients who have been
screened and deemed appropriate for testing or evaluation. Orders are required.
Mount Prospect1754 W. Golf Rd.
Mt. Prospect, IL 60056
Phone: 224.265.9000 or
224.265.9010;
press 2 (for Immediate Care)
Fax: 224.265.9041
Lincolnwood7380 N. Lincoln
Lincolnwood, IL 60712
Phone: 847.568.7400
Fax: 847.568.7440
Chicago / Archer6084 S. Archer Ave., Floor 1
Chicago, IL 60638
Phone: 224.273.6000
Fax: 224.273.6099
7
8
9
Note: AHMG PCPs should schedule internally through their Epic or Athena EMRs
1
2
9
7
9
3
Respiratory CentersDrive-Thru Test Centers
Hoffman EstatesAMITA Health St.
Alexius Medical Center
Hoffman Estates
EvanstonAMITA Health Saint
Francis Hospital
Evanston
JolietAMITA Health Saint
Joseph Medical Center
Joliet
1
2
3
ChicagoAMITA Health Saints
Mary and Elizabeth
Medical Center
La GrangeAMITA Health Adventist
Medical Center La
Grange
ChicagoAMITA Health
Resurrection Medical
Center Chicago
4
4
New Center
6
5
6
5
20
Studies in progress . . .
• COVID-19 IgG Antibody Cross Reactivity Study
• Patients with non-COVID-19 coronaviruses have been identified and will be donating samples this week
• Study anticipated to be completed soon
• Study results will provide test specificity
• ID Now in the Asymptomatic population
• Due to the temporary shortage of ID Now kits, study is taking more time than anticipated
• By FDA, the ID Now is not recommended for asymptomatic patient groups so a study to contradict this
would have to be powered by a large # of patients
21
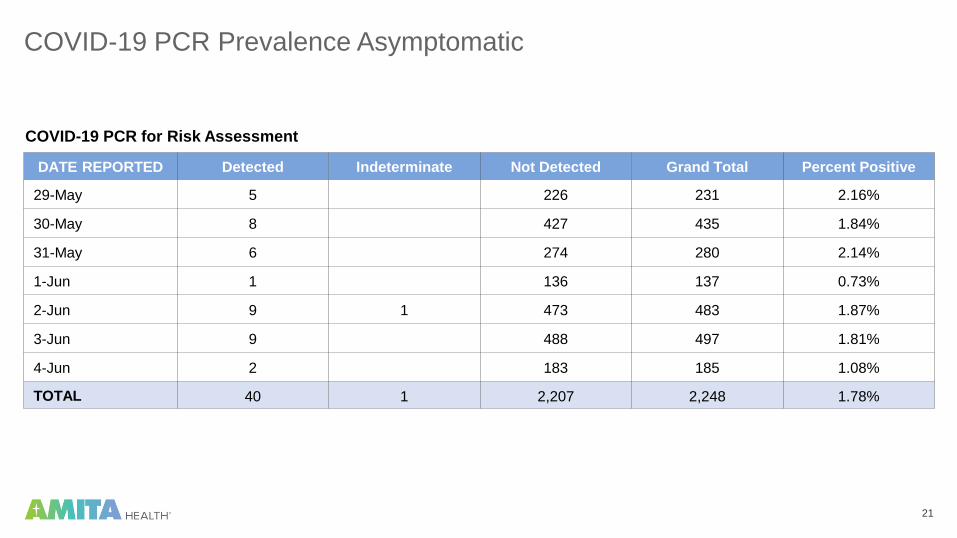
COVID-19 PCR Prevalence Asymptomatic
COVID-19 PCR for Risk Assessment
DATE REPORTED Detected Indeterminate Not Detected Grand Total Percent Positive
29-May 5 226 231 2.16%
30-May 8 427 435 1.84%
31-May 6 274 280 2.14%
1-Jun 1 136 137 0.73%
2-Jun 9 1 473 483 1.87%
3-Jun 9 488 497 1.81%
4-Jun 2 183 185 1.08%
TOTAL 40 1 2,207 2,248 1.78%
22
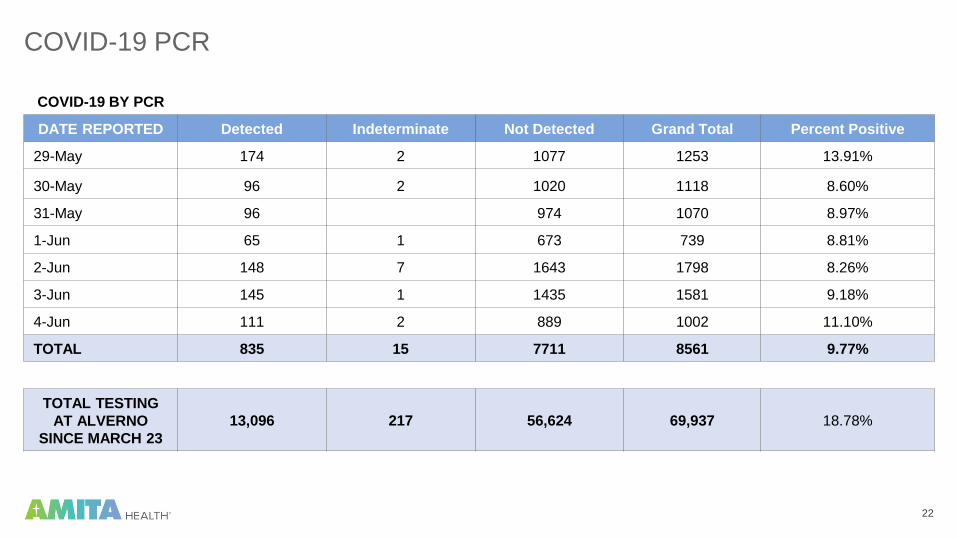
COVID-19 PCR
COVID-19 BY PCR
DATE REPORTED Detected Indeterminate Not Detected Grand Total Percent Positive
29-May 174 2 1077 1253 13.91%
30-May 96 2 1020 1118 8.60%
31-May 96 974 1070 8.97%
1-Jun 65 1 673 739 8.81%
2-Jun 148 7 1643 1798 8.26%
3-Jun 145 1 1435 1581 9.18%
4-Jun 111 2 889 1002 11.10%
TOTAL 835 15 7711 8561 9.77%
TOTAL TESTING
AT ALVERNO
SINCE MARCH 23
13,096 217 56,624 69,937 18.78%
23
Physician WellnessDr. Harry Karydes, Vice Chairman and Medical Director, Department of Emergency Medicine,
AMITA Health Adventist Medical Center-Bolingbrook

24

25

26
www.medicinerevived.com

27

29
Podcast
• Episode 27: 5 Ways to Ease Stress Amid Crisis
• Episode 28: Doctor, Are You At Risk for Second Victim Syndrome?
• Episode 29: 6 Ways to Cope after a Patient Death
• Episode 31: Compassion Fatigue? There is a Better Way
• Episode 38: Growth Begins When You Embrace Uncertainty
30
COVID-19 Treatment and Vaccine UpdateSun Lee-Such, Vice President Pharmacy Services
31
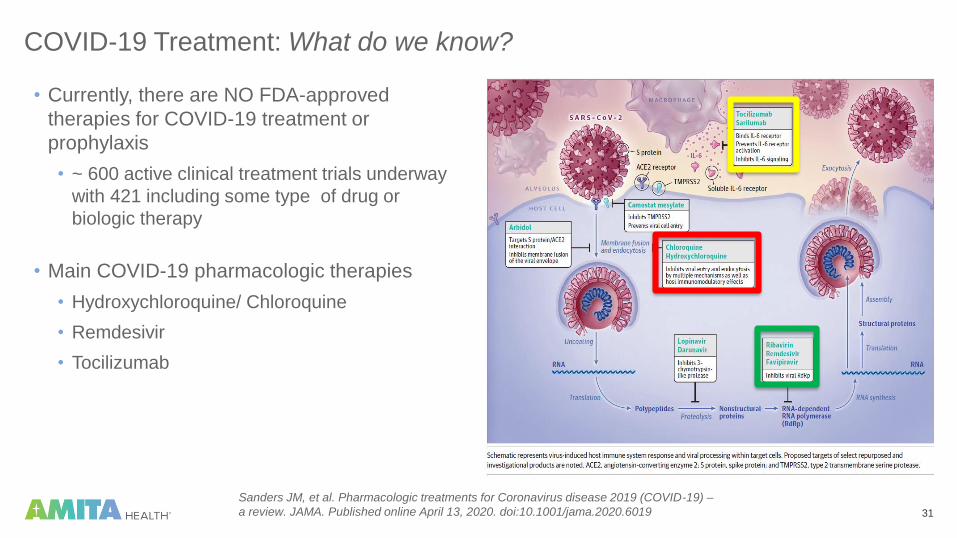
COVID-19 Treatment: What do we know?
• Currently, there are NO FDA-approved
therapies for COVID-19 treatment or
prophylaxis
• ~ 600 active clinical treatment trials underway
with 421 including some type of drug or
biologic therapy
• Main COVID-19 pharmacologic therapies
• Hydroxychloroquine/ Chloroquine
• Remdesivir
• Tocilizumab
Sanders JM, et al. Pharmacologic treatments for Coronavirus disease 2019 (COVID-19) –
a review. JAMA. Published online April 13, 2020. doi:10.1001/jama.2020.6019
32
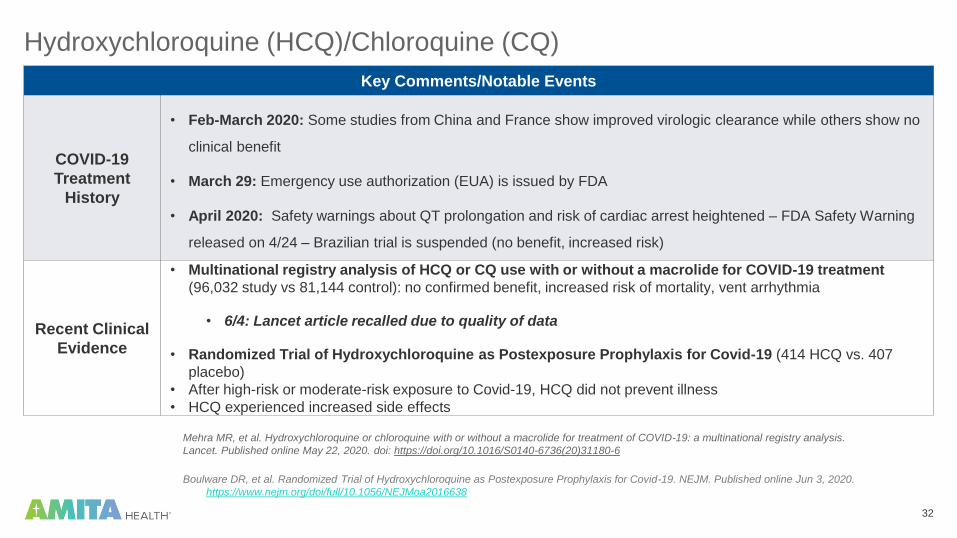
Hydroxychloroquine (HCQ)/Chloroquine (CQ)
Key Comments/Notable Events
COVID-19
Treatment
History
• Feb-March 2020: Some studies from China and France show improved virologic clearance while others show no
clinical benefit
• March 29: Emergency use authorization (EUA) is issued by FDA
• April 2020: Safety warnings about QT prolongation and risk of cardiac arrest heightened – FDA Safety Warning
released on 4/24 – Brazilian trial is suspended (no benefit, increased risk)
Recent Clinical
Evidence
• Multinational registry analysis of HCQ or CQ use with or without a macrolide for COVID-19 treatment
(96,032 study vs 81,144 control): no confirmed benefit, increased risk of mortality, vent arrhythmia
• 6/4: Lancet article recalled due to quality of data
• Randomized Trial of Hydroxychloroquine as Postexposure Prophylaxis for Covid-19 (414 HCQ vs. 407
placebo)
• After high-risk or moderate-risk exposure to Covid-19, HCQ did not prevent illness
• HCQ experienced increased side effects
Mehra MR, et al. Hydroxychloroquine or chloroquine with or without a macrolide for treatment of COVID-19: a multinational registry analysis.
Lancet. Published online May 22, 2020. doi: https://doi.org/10.1016/S0140-6736(20)31180-6
Boulware DR, et al. Randomized Trial of Hydroxychloroquine as Postexposure Prophylaxis for Covid-19. NEJM. Published online Jun 3, 2020.
https://www.nejm.org/doi/full/10.1056/NEJMoa2016638

33
Hydroxychloroquine (HCQ) /Chloroquine (CQ)
Key Comments/Notable Events
AMITA
Historical Use
• Mid-March to mid-April: 150-200 patients on HCQ system-wide daily
• End of April to mid-May: 30-50 patients on HCQ system-wide daily
• Current use: ≤ 15 patients on HCQ system-wide daily
National Guideline
Statements
• NIH: Insufficient clinical data to recommend either for or against use; Recommends against
using high-dose HCQ/CQ therapy
• WHO: Should not be administered as treatment or prophylaxis outside of the context of
clinical trials
• IDSA: Should only be used in the context of a clinical trial
AMITA
COVID-19 Treatment
Recommendation from
CDTF
• AVOID USE – Risks outweigh benefit

34
Remdesivir: What is it?
• Inhibits viral duplication by inhibiting
RNA-dependent RNA-polymerase
• Was initially being studied for
management of an Ebola virus
outbreak
• Has potent activity in vitro against
Coronaviruses including SARS-CoV-2
– shown to be effective vs. MERS and
SARS

35
Remdesivir in COVID-19 Treatment – Timeline
Remdesivir
available
through
Compassionate
Use Program
•Results from China
showed that
remdesivir can
efficiently inhibit
SARS-CoV-2 in vitro
•Manufacturer Gilead
allows
compassionate use
program based on
severity of disease
for COVID-19
patients
Compassionate
Use Program
Halted for
Expanded Use
Program
NIH NIAID Trial
Preliminary
Results
Released
HHS notification
Of Distribution
Through
State
Departments –
IDPH Memo
IDPH
Releases
Phase 2 & 3 of
Remdesivir EUA
Distribution
Jan-
Feb
2020
Mid-late
May 2020
March
22,
2020
April
29,
2019
May 1,
2020
May 9,
2020
FDA Grants
Emergency
Use
Authorization
•COVID-19 activity surges in the US and overwhelms Gilead
•Decision to change to Expanded Access Program
•Compassionate use ceases EXCEPT for pregnant patients and children < 18 years old
•Release of NIH NIAID preliminary results showing decreased LOS of 11 days vs. 15 days in remdesivir patients
•No published article available on the details
•FDA grants
emergency use
authorization (EUA)
for remdesivir for
use in hospitalized
COVID-19 patients
•Gilead announces
they will donate 1.5
million doses
worldwide for
COVID-19 pandemic
efforts
•Government will be
in charge of
distribution plans
•After initial week of distribution, FEMA and HHS determine that state depts will determine distribution
• IDPH does not receive any supply until Phase 2 - gets 150 cases
•AMITA receives 8 cases – CDTF sets initial criteria – 10 patients start treatment
• IDPH releases Phase 2 & 3 where 668 total cases were given to IL
•AMITA receives shipments at ALL hospitals – now have supply for overall total of 740 treatment courses
•CDTF relaxes criteria
36
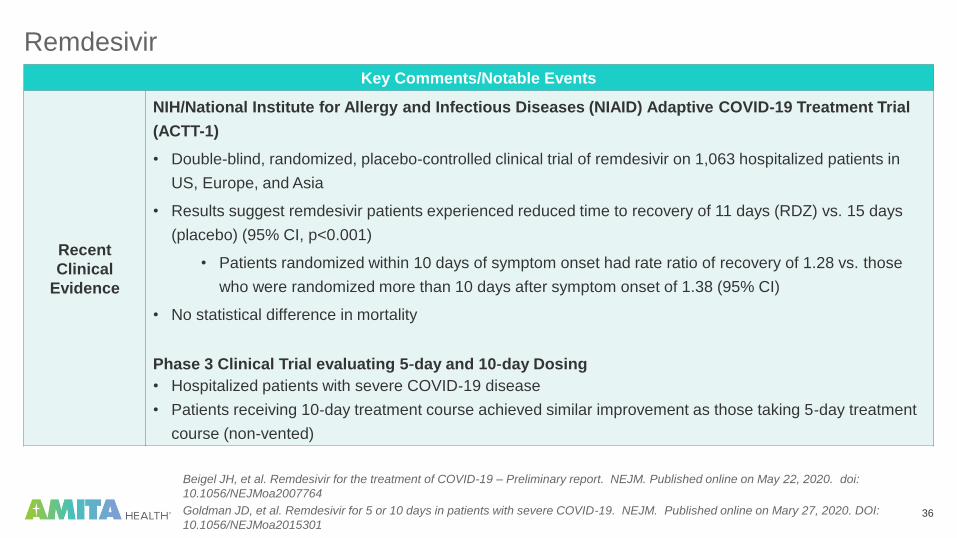
Remdesivir
Key Comments/Notable Events
Recent
Clinical
Evidence
NIH/National Institute for Allergy and Infectious Diseases (NIAID) Adaptive COVID-19 Treatment Trial
(ACTT-1)
• Double-blind, randomized, placebo-controlled clinical trial of remdesivir on 1,063 hospitalized patients in
US, Europe, and Asia
• Results suggest remdesivir patients experienced reduced time to recovery of 11 days (RDZ) vs. 15 days
(placebo) (95% CI, p<0.001)
• Patients randomized within 10 days of symptom onset had rate ratio of recovery of 1.28 vs. those
who were randomized more than 10 days after symptom onset of 1.38 (95% CI)
• No statistical difference in mortality
Phase 3 Clinical Trial evaluating 5‐day and 10‐day Dosing
• Hospitalized patients with severe COVID‐19 disease
• Patients receiving 10‐day treatment course achieved similar improvement as those taking 5‐day treatment
course (non-vented)
Beigel JH, et al. Remdesivir for the treatment of COVID-19 – Preliminary report. NEJM. Published online on May 22, 2020. doi:
10.1056/NEJMoa2007764
Goldman JD, et al. Remdesivir for 5 or 10 days in patients with severe COVID-19. NEJM. Published online on Mary 27, 2020. DOI:
10.1056/NEJMoa2015301
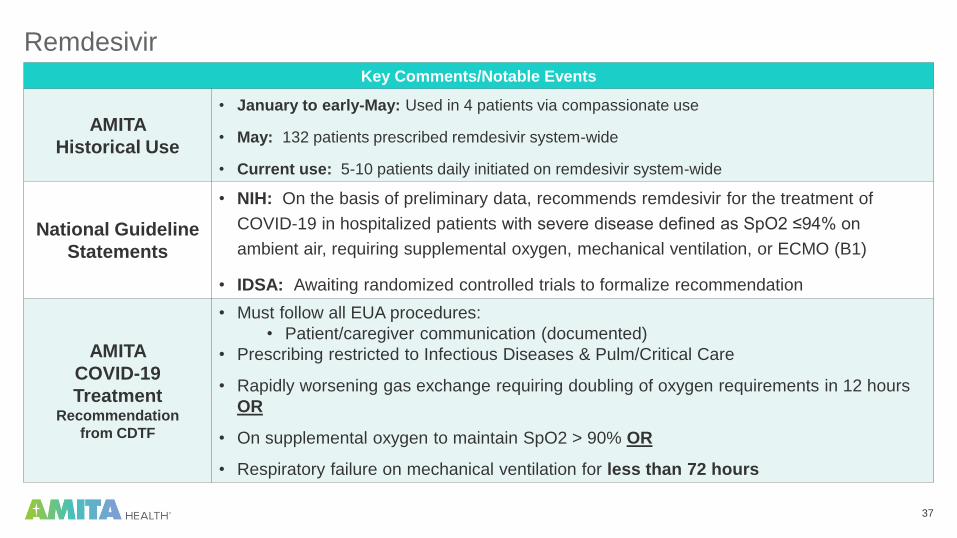
37
RemdesivirKey Comments/Notable Events
AMITA
Historical Use
• January to early-May: Used in 4 patients via compassionate use
• May: 132 patients prescribed remdesivir system-wide
• Current use: 5-10 patients daily initiated on remdesivir system-wide
National Guideline
Statements
• NIH: On the basis of preliminary data, recommends remdesivir for the treatment of
COVID-19 in hospitalized patients with severe disease defined as SpO2 ≤94% on
ambient air, requiring supplemental oxygen, mechanical ventilation, or ECMO (B1)
• IDSA: Awaiting randomized controlled trials to formalize recommendation
AMITA
COVID-19
TreatmentRecommendation
from CDTF
• Must follow all EUA procedures:
• Patient/caregiver communication (documented)
• Prescribing restricted to Infectious Diseases & Pulm/Critical Care
• Rapidly worsening gas exchange requiring doubling of oxygen requirements in 12 hours
OR
• On supplemental oxygen to maintain SpO2 > 90% OR
• Respiratory failure on mechanical ventilation for less than 72 hours
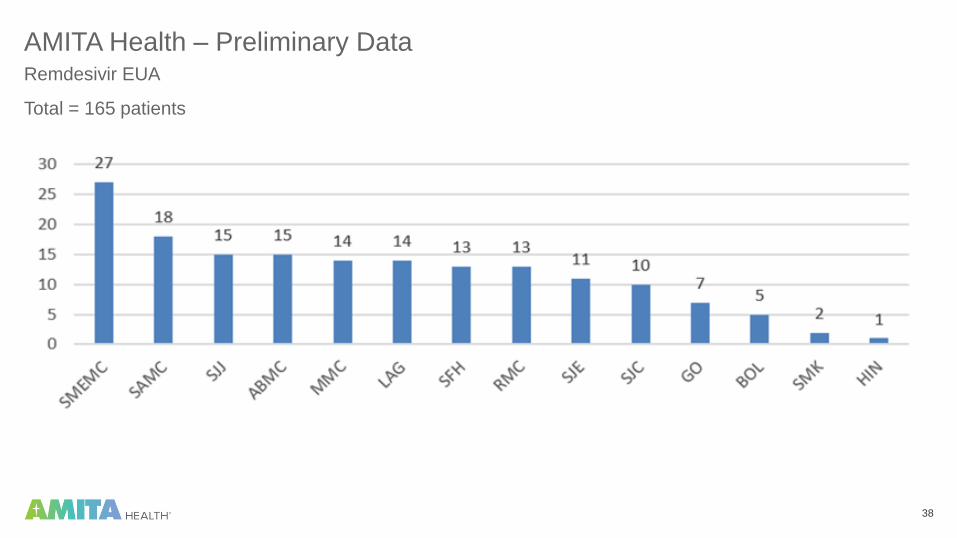
38
AMITA Health – Preliminary DataRemdesivir EUA
Total = 165 patients
39
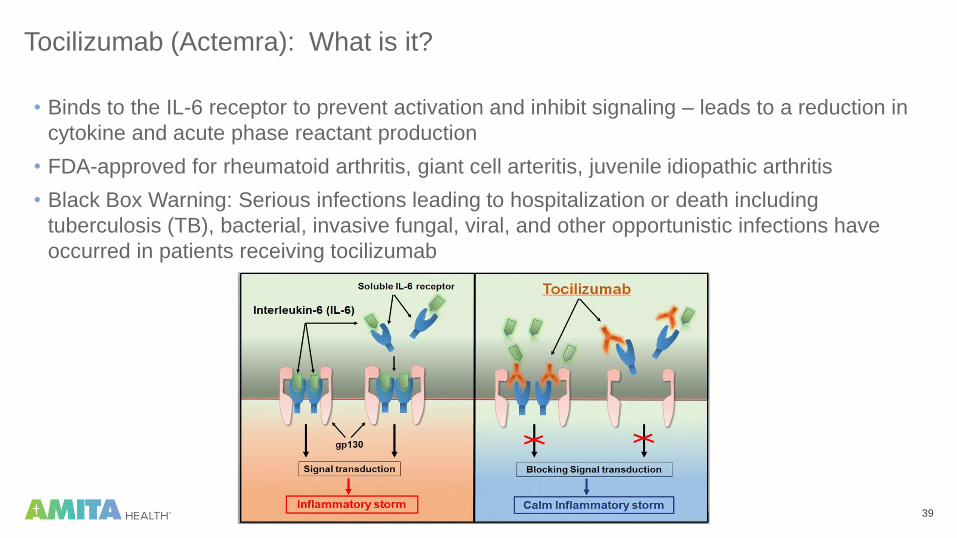
Tocilizumab (Actemra): What is it?
• Binds to the IL-6 receptor to prevent activation and inhibit signaling – leads to a reduction in
cytokine and acute phase reactant production
• FDA-approved for rheumatoid arthritis, giant cell arteritis, juvenile idiopathic arthritis
• Black Box Warning: Serious infections leading to hospitalization or death including
tuberculosis (TB), bacterial, invasive fungal, viral, and other opportunistic infections have
occurred in patients receiving tocilizumab

40
Tocilizumab (Actemra)Key Comments/Notable Events
COVID-19
Treatment
History
• Feb-March 2020: Reports from China that tocilizumab was part of clinical treatment protocols, especially in severe
and critical patients
• April 2020: Small studies from China and Italy showing improved clinical outcomes as an effective treatment to
reduce mortality; severity and progression of inflammatory response seen in COVID-19 made tocilizumab an
attractive option in critical COVID-19 cases
Recent
Clinical
Evidence
Unclear
Benefit
• Retrospective study in severe COVID-19 non-ICU patients with hyper-inflammatory features with 28 day follow-up
• Review of 65 patients: 32 received tocilizumab vs. 33 who did not
• No statistically difference in clinical improvement and mortality:
• Clinical improvement reached in 22 (69%) of tocilizumab group vs. 20 (61%) in control group
• 4 (13%) tocilizumab patients (1 candidemia) vs. 4 (12%) in control group
• 5 (16%) of toclizumab group died vs. 11 (33%) of control group
• Authors’ conclusion: At day 28, clinical improvement and mortality were not statistically different when given
tocilizumab vs. standard care
Corrado Campochiaro, et al., Efficacy and safety of tocilizumab in severe COVID-19 patients: a single-centre
retrospective cohort study. Eur J Int Med. doi: https://doi.org/10.1016/j.ejim.2020.05.021.

41
Tocilizumab (Actemra)
Key Comments/Notable Events
Recent Clinical
Evidence
Increased Risk
• Observational study at U of Chicago/Rush in COVID-19 ICU patients
• Review of 60 patients: 28 received tocilizumab vs. 32 who did not
• Tocilizumab was associated with higher incidence of secondary bacterial infections including
hospital-acquired pneumonia & ventilator-associated pneumonia (64.3% vs. 31.3% p=0.010).
• 2 tocilizumab patients with fungal infections (mucor PNA and sinusitis) vs. none in control group
• No evidence of benefit was seen
• Authors’ conclusion:
• While there may be a subset of patients who may potentially benefit from tocilizumab, current
evidence does not support its routine use for COVID-19.
• Findings raise concerns about the use of tocilizumab in the presence of an infection to attenuate
cytokine release syndrome
Kimmig LM, Wu D, Gold M, et al. IL6 Inhibition in critically ill COVID-19 patients is associated with increased secondary
infections. Prepublication. https://www.medrxiv.org/content/10.1101/2020.05.15.20103531v1.
42
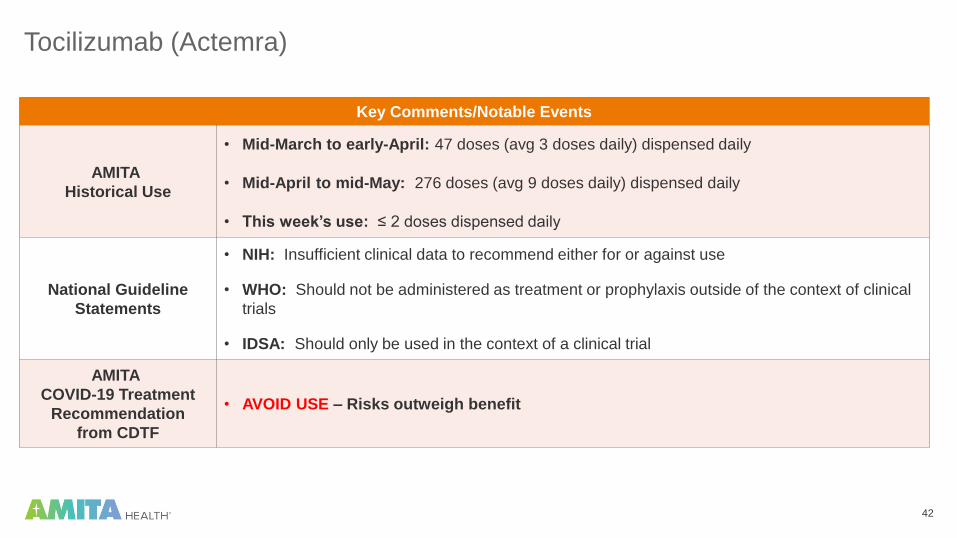
Tocilizumab (Actemra)
Key Comments/Notable Events
AMITA
Historical Use
• Mid-March to early-April: 47 doses (avg 3 doses daily) dispensed daily
• Mid-April to mid-May: 276 doses (avg 9 doses daily) dispensed daily
• This week’s use: ≤ 2 doses dispensed daily
National Guideline
Statements
• NIH: Insufficient clinical data to recommend either for or against use
• WHO: Should not be administered as treatment or prophylaxis outside of the context of clinical
trials
• IDSA: Should only be used in the context of a clinical trial
AMITA
COVID-19 Treatment
Recommendation
from CDTF
• AVOID USE – Risks outweigh benefit

43
COVID-19: First Do No Harm
Editorial in the American Thoracic Society
“[W]e believe that the widespread use of clearly
experimental therapies being reported in patients with
SARS CoV-2 is dangerous and unjustified. There is a real
risk that mortality rates are higher than they need to be
because of toxic, ineffective therapy. Clinicians must not
succumb to the impulse to “do something else” but instead
stick to evidence-based therapies and, if possible, enroll
their patients into adaptive clinical trials”
https://www.atsjournals.org/doi/full/10.1164/rccm.202004-1153ED
44
SARS-CoV-2 Prevention: Vaccine Development
• Genome sequence of SARS-CoV-2 published on 1/11/2020
• More than 100 projects internationally are working on potential vaccines for SARS-CoV-2
• As of 6/2/2020, ten candidate vaccines tested in clinical trials in human
• Current state of clinical evaluation/regulatory status range from Phase 1 to Phase 2b/3
• Additional 123 candidate vaccines undergoing preclinical evaluation
• First human trial started in early March in China
• Phase 1 trial results were published on the safety of the adenovirus type 5 vectored COVID-19 (Ad5-
nCoV) vaccine in 108 patients
• Tolerable and immunogenic at 28 days post-vaccination
• Efficacy and further published data are pending
https://www.who.int/who-documents-detail/draft-landscape-of-covid-19-candidate-vaccines
Zhu F, et al. Safety, tolerability, and immunogenicity of a recombinant adenovirus type-5 vectored COVID-19 vaccine: a dose-
escalation, open-label, non-randomized, first-in-human trial. Lancet. Published online on May 22, 2020. https://doi.org/10.1016/S0140-
6736(20)31208-3
45
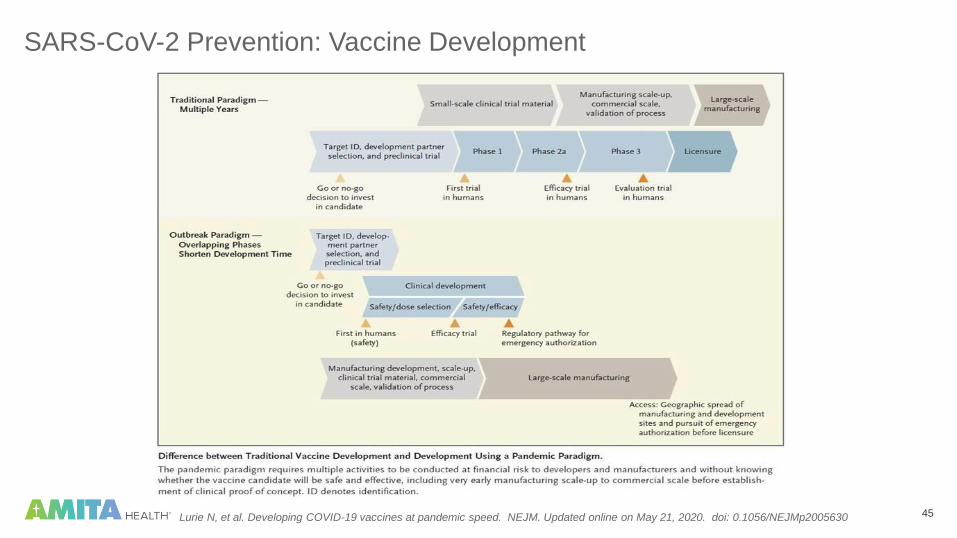
SARS-CoV-2 Prevention: Vaccine Development
Lurie N, et al. Developing COVID-19 vaccines at pandemic speed. NEJM. Updated online on May 21, 2020. doi: 0.1056/NEJMp2005630

46
SARS-CoV-2 Vaccine Development
Lurie N, et al. Developing COVID-19 vaccines at pandemic speed. NEJM. Updated online on May 21, 2020. doi: 0.1056/NEJMp2005630

47
Vaccine Development Timeline
• Many efforts to fast-track by the FDA, still unknown when a vaccine may be available for
widespread use
• Most optimistic report (out of the University of Oxford) suggests vaccine may be ready by
September
• Many experts caution vaccine in 12 to 18 months may be difficult to achieve without
pandemic paradigm model
48
Communications Template for Independent ProvidersDr. Maninder Kohli, ACO Board Chair

49
Patient Communications Template for Independent Providers
Microsoft Word
Document
Double click icon to view document in Microsoft Word →
AMITAhealth.org/covid-19-AMITA
50
Open Q&AModerated by Dr. Reinhold Llerena, President, AMITA Health Medical Group; AMITA Chief Population Health Officer
51
Open Q&A
AMITA COVID-19 Command CenterDr. Stuart Marcus
EVP, Chief Clinical Officer
Lab Testing UpdateDr. Janis Atkinson
VP Medical Affairs, Alverno Lab for AMITA Health
Physician Wellness
Dr. Harry Karydes
Vice Chairman and Medical Director, Department of Emergency Medicine,
AMITA Health Adventist Medical Center-Bolingbrook
COVID-19 Treatment and Vaccine UpdateSun Lee-Such
Vice President Pharmacy Services
Computer WebEx App Mobile WebEx App
Submit Questions Via WebEx Q&A Box
Presenters
52
Closing RemarksDr. Joseph Lagattuta, CIN Board Chair

53
Updated for June: Extending Help to Our Providers and AssociatesAMITA Health Behavioral Medicine and Spiritual Care teams continue to provide internal virtual peer support groups. These
groups provide psychological and spiritual support, as well as self-care recommendations in a safe, confidential forum.
Therapists facilitate and assist with steering participants to additional resources. Open sharing and interaction is encouraged.
Weekly
Through JuneTopic Time Facilitator Call 331.303.8777
Monday Medical Resident (and all others) Support 7:30-8:30am Dr. Arianna Timko Passcode: 179391585
Monday Anxiety, Grief and Exhaustion Support 3-4pm Chris McCarthy Passcode: 117075094
Tuesday Surviving to Thriving 3-4pm Fr. Jim Swarthout Passcode: 449311082
Wednesday Providers Dealing with Death, Dying and Difficult Decisions 7-8amDr. Cliff Saper and Victoria
Storm, Music TherapistPasscode: 6978305272
Wednesday Anxiety, Grief, and Exhaustion Support 9-10amDr. Brenda Papierniak and Dr.
Tricia Mckinney Passcode: 216779082
Wednesday Facing the Pandemic When You are Living Alone 4:30-5:30pm Christina Lobraco and Lisa Tamez Passcode: 565011744
Thursday Anxiety, Grief and Exhaustion Support 7:30-8:30am Lisa Tamez Passcode: 981274379
Thursday Anxiety, Grief and Exhaustion Support 12-1pm Lauren Bantner Passcode: 621911086
Friday Parenting During the Pandemic: Finding a Work/Life Balance 9-10am Jackie Rhew and Dr. Cece Horan Passcode: 66929398
Friday Anxiety, Grief, and Exhaustion Support 12-1pmChristina Lobraco and Victoria
Storm, music therapist Passcode: 593396039
If your work group, program, unit, or department staff wish to have your own virtual peer support group at a time you designate,
contact Clifton.saper@amitahealth for a request form.

54
CME Credit for AMITA Health COVID-19 Physician TownhallsThe evaluation survey needs to be completed for each session attended for credit dating back to 3/27. GME
will issue certificates each month, stating the total CME awarded for said month.
Evaluation Link: https://www.surveymonkey.com/r/MedStaffTownHall
AMITA Health Resurrection Medical Center designates this Activity for a
maximum of 1 AMA PRA Category 1 credit(s)TM. Physicians should only claim credit commensurate
with the extent of their participation in the activity
AMITA Health Resurrection Medical Center is accredited by the Illinois State
Medical Society to sponsor continuing medical education for physicians.
None of our speakers today have any sponsorship disclosures to report
55
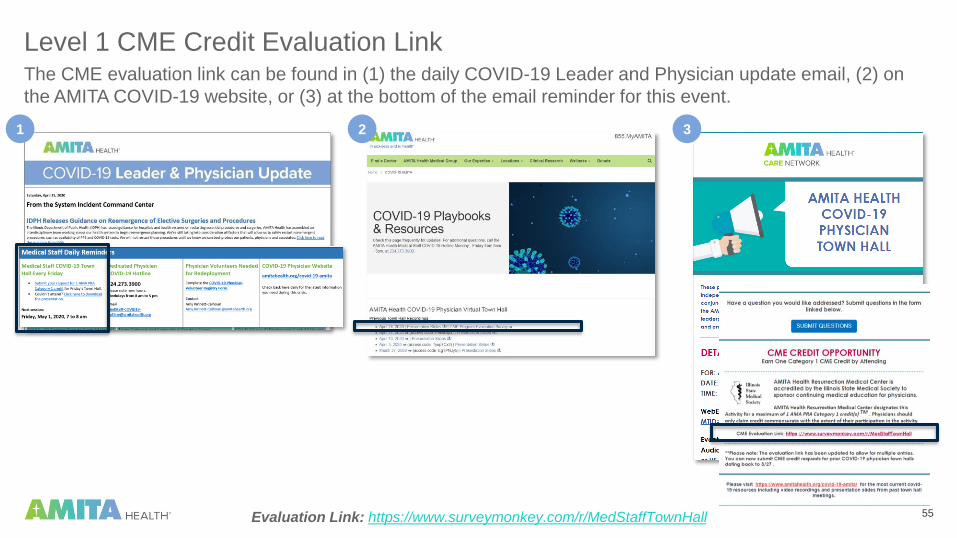
Level 1 CME Credit Evaluation LinkThe CME evaluation link can be found in (1) the daily COVID-19 Leader and Physician update email, (2) on
the AMITA COVID-19 website, or (3) at the bottom of the email reminder for this event.
31 2
Evaluation Link: https://www.surveymonkey.com/r/MedStaffTownHall
56
Thank you!
AMITA COVID-19 Physician Hotline Phone Number
224.273.3900 from 8am to 5pm weekdays for the foreseeable future
AMITA COVID-19 Physician Hotline Email
AMITA COVID-19 Resources & Playbooks AMITAhealth.org/covid-19-AMITA