Upload
others
View
0
Download
0
Embed Size (px)
Citation preview
COUNSELLING
INSIGHTS INTO
CLINICALApril 2014
Published by the BC Association of Clinical Counsellorsto enhance mental health in British Columbia and beyond...
Social-Emotional Learning in our Schools
Counselling Clients with Fibromyalgia
A Constructivist Approach to Counselling
Taking Emotionally Focused Therapy from the Bedroom to
the Boardroom
Outcomes Monitoring and BC Clinical Counsellors
Panic Attacks, Antidepressants and Postmodernism
Stalking in the Mental Health Professions
Dreams in Clinical Practice
Non-Verbal Client Content Viewed As Cues and Clues
Thinking throughConfidentiality
Insights into Clinical Counselling - April 2014
2
C O N T E N T S
The Insights into Clinical Counselling team wishes to thank the outstanding writers who contributed
to this edition of our magazine:
Stacey Burnard, Leslie Ellis, Marilyn Fitzpatrick, Sarah Flynn,
Larry Green, Megan Hughes, Gabriela Ionita, Terra Kowalyk, Clive Perraton Mountford, Seth Raymond,
Kristine Rea, Jennifer Storey
Insights Into CLINICAL COUNSELLING is published three times per year:April – August – December
NEXT ISSUE:
Article Submission: April 25, 2014Ads Submission Window: May 16-23, 2014Insert Submission Window: July 14-18, 2014
SUBMISSION CONTACTS:
ArticlesMichelle Morand, EditorE-mail: [email protected]: (778) 990-4606Ads & InsertsUri Sanhedrai, PublisherE-mail: [email protected] • Tel: (604) 988-5066
POLICIES & GUIDELINES
Advertising and InsertsPolicies and guidelines for placing advertising and inserts in Insights Into CLINICAL COUNSELLING Magazine can be obtained from BCACC’s website (www.bc-counsellors.org/iicc-magazine) or from the publisher, email: [email protected], Tel: (604) 988-5066Articles For Contributing Writers’ Guidelines visit www.bc-counsellors.org/iicc-magazine or contactAina Adashynski, Editorial CoordinatorE-mail: [email protected], Tel: 1-800-909-6303 ext. 4
IICC MAGAZINE TEAM
Editor: Michelle MorandTel: (778) [email protected] Creative Director/Art Director/Publisher:Uri Sanhedrai Tel: (604) [email protected] Coordinator: Aina AdashynskiTel: (250) 595-4448 or 1-800-909-6303, ext. [email protected]
Thank you for your interest in Insights Into CLINICAL COUNSELLING
BCACC 1-800-909-6303
Non-Verbal Client Content Viewed As Cues and Clues: Clinical Anecdotes from an Attachment Perspective (Page 3)Sarah Flynn updates us on the practice of attachment theory and how we can better understand, and make use of, what is not being (or cannot yet be) verbalized, to enhance our clients’ ability to identify and fulfill their needs.
Educational Transformation: Social-Emotional Learning (SEL) in our Schools (Page 6) Stacey Burnard presents an education on the current literature on Social-Emotional Learning, its use in BC schools, and its life-long benefits to students and societies worldwide.
Counselling Clients with Fibromyalgia (Page 8)Megan Hughes presents a detailed exploration of Fibromyalgia and offers some key considerations and suggestions for supporting clients with this illness.
Imposition of Order into Tales of Woe: A Constructivist Approach to Counselling (Page 10)Seth Raymond is our narrator and we are flies on the wall, in a counselling session where the client is in high distress and a constructivist approach provides structure, support and hope.
Ethically Speaking – It Looked like a Good Idea: Thinking through Confidentiality (Page 14)Clive Perraton Mountford, BCACC’s chair of ethics and ethics consultant offers his first installment in a new and ongoing column that will address key issues of ethics pertaining to the profession of counselling. In this article Clive covers the issue of confidentiality in peer supervision and in professional writing.
Taking EFT from the Bedroom to the Boardroom: How the Principles of Emotionally Focused Therapy Provide a Roadmap to Productively Navigate Emotions in the Business Environment (Page 18)Kristine Rea illustrates some key concepts of EFT and how these concepts can be effectively applied in our professional environment and that of our clients.
Outcomes Monitoring and British Columbia Clinical Counsellors (Page 20)In this paper, Terra Kowalyk, Gabriela Ionita and Marilyn Fitzpatrick of McGill University share their research findings regarding the benefits experienced by clients when their therapists utilize specific tools for monitoring treatment outcomes vs. counsellor subjective assessment.
An Observation on Panic Attacks, Antidepressants and Postmodernism (Page 22)Larry Green explores the topic of anxiety and invites us to consider a cultural/environmental perspective on the cause of anxiety and depression.
Hurting the Healers: Stalking in the Mental Health Professions (Page 24) Some of you may recall being asked to participate in a study on the experience of stalking. In this article Jennifer Storey presents a brief synopsis (and link to the full study) of her research findings and the prevalence, impact and potential areas for enhanced counsellor education and protection.
Love and Enjoy the Dream: Why and how to use Dreams in Clinical Practice (Page 26)In this article, Leslie Ellis explores current clinical research as well as the history of dream analysis in psychiatry and counselling. She then provides some concrete suggestions for the use of dreams in our practice with clients.
Article References (Page 31)
Community Pages (Page 33)
Insights into Clinical Counselling - April 2014
3
Or they are inconsistent? Because infants are thoroughly dependent on their caregivers, they must adapt to them. Infants accommodate the idiosyncratic strengths and/or weaknesses of their caregivers by adopting behavioral strategies (which are in essence, affect regulating strategies).
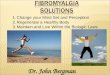
In attachment theory, three primary behavioral strategies have been identified. These include the so-called secure, avoidant and ambivalent strategies. Wallin explains:Confident of their mothers’ responsiveness, secure infants could well afford to be attuned to their own attachment-related feelings and needs: They could be aware of and could express them. Avoidant infants, anticipating mother’s rejection and their own anger in response, could afford neither to be aware of nor to express their attachment-related feelings and needs: Hence the avoidant strategy of inhibiting or minimizing such internal experiences. Ambivalent infants, responding to their mother’s unpredictable availability, apparently developed a strategy for amplifying or maximizing both the awareness and the expression of their attachment related feelings and needs as if to ensure continuing care.v
Thus the avoidant strategy involves a hypo-activating adaptation (downplaying) of attachment needs and behaviors and the ambivalent strategy involves a hyper-activating adaptation (escalating) of attachment needs and behaviors to fit the care giving environment infants find themselves in.
Infants and caregivers communicate through a “body language” such as touch, tone, gestures, facial expressions, eye contact and action tendencies. Spoken language generally begins gradually around the second year of life. However, the brain
This article explores the idea that, for clients who have had insecure childhoods, healing and growth can be facilitated by thinking of therapy as a reparative attachment relationship and by deliberately tuning into non-verbal interactive dynamics.
Attachment Theory and Non-Verbal CommunicationAttachment theory explains how a person’s internal emotional world and external interpersonal behavior is related to the environment, threat and the need for security throughout the lifespan.i Our first “environment” is the one we inhabit as infants at a time when we are utterly dependent on our primary caregivers for all of our physical and emotional needs. Our attachment to caregivers in infancy is a biological necessity.
Security for an infant means having physical proximity to caregivers to provide food, warmth and protection etc., but also emotional availability to provide affect regulation (the monitoring and modifying of states of emotional arousal to remain within tolerable limits).ii Affect regulation involves caregivers recognizing, identifying, modulating (as needed), and reflecting upon (as development permits) the emotional experience of their child, as neither infants nor children can do this on their own. When caregivers actively soothe states of distress and encourage states of comfort and pleasure they are modulating affect.iii When this happens consistently, infants (and children) will experience the attachment relationship as a source of relief, comfort, and pleasure wherein emotions are welcome, understandable and manageable.iv
But, what happens when caregivers are not responsive to their infant’s needs for soothing and protection? For example, if caregivers are generally angry in response to distress?
By Sarah Flynn, MREM, MA, RCC, Contributing Writer
Non-Verbal Client Content Viewed As Cues and Clues: Clinical Anecdotes from an Attachment Perspective
SECURE ATTACHMENT
Confident of their mothers’ responsiveness, secure infants could
well afford to be attuned to their own attachment-related feelings
and needs: They could be aware of and could express them.
Avoidant infants, anticipating mother’s rejection and their own anger in response, could afford
neither to be aware of nor to express their attachment-related
feelings and needs: Hence the avoidant strategy of inhibiting or minimizing
such internal experiences.
Ambivalent infants, responding to their mother’s unpredictable
availability, apparently developed a strategy for amplifying or
maximizing both the awareness and the expression of their attachment
related feelings and needs as if to ensure continuing care.
AVOIDANT STRATEGIES AMBIVALENT STRATEGIES
Insights into Clinical Counselling - April 2014
the usefulness of their counsellors and he had reached that point with me. Not wanting to come across as disappointed or defensive (which I was a bit), I outwardly graciously accepted his termination of me. Then an extended awkwardness hung in the air. He kept asking me in various ways if I thought I could be of more assistance to him and I kept reassuring him that he should trust his own intuition about it.
Gradually it dawned on me that he needed me to tell him that I had more to offer him. Because of his upbringing, it was outside his relational repertoire to know how to ask for more, what that “more” might be or how to trust that I would not disappoint him (as had his parents) if he allowed himself to ask for, need, or want it.
Beginning to grasp the enactment at play, I said, “I am feeling this interesting pushing and pulling going on right now. You say you don’t want more therapy with me (action: pushing), but then ask me to tell you that I have more to offer you (action: pulling). Does this fit with your experience of what is happening right now?” He said, “Yeah, especially the pushing and pulling part, my girlfriend tells me I do that all the time.” For this to be reparative for him, I had to demonstrate that it was okay for him to want/need more from me even if he didn’t know what that was yet; we would figure it out together, and I would not let him down.
EmbodimentsThe ambivalent and the avoidant attachment strategies are associated in adulthood with quite distinct bodily expressions. The ambivalent (hyper-activating) strategy usually involves an internal physiology which includes sympathetic nervous
Client may caus
e the
therapist to e
xperience
that which the
y
feel or think, b
ut cannot
know, name, o
r
experience d
irectly.
4
structures which encode memory in a verbally accessible, symbolic form don’t generally come online until the third year of life.vi The period prior to this is referred to as infantile amnesia, because memory cannot be consciously retrieved. Nonetheless experience from this period is “remembered,” is highly formative, and will be experienced later as a sense of knowing how to be and how to be with others.vii
This type of memory is referred to as procedural or implicit memory; it is non-verbal, non-symbolic, and generally unavailable for conscious recall or reflection. Its content involves procedures, emotional responses, and patterns of behavior. When this type of memory is activated the person has a sense of unconsciously “knowing how” and of “familiarity with” rather than of conscious recollection. These memories can be a therapeutic gold mine because they contain unarticulated content about the self and about the self in relationship.
Reparative Attachment: The Potential of Therapy It stands to reason that those feelings, thoughts and behaviors which might jeopardize crucial attachment relationships would be defensively excluded from awareness and behavior and that those which sustain and protect it would be emphasized. It also stands to reason that a new attachment relationship could offer new and distinct possibilities for what can be safely known, felt and acted upon. To the extent that a therapist has the capacity to facilitate, witness, tolerate, integrate and reflect on that which was historically off limits, new facets of a client can be encouraged to emerge. Thought of in this way, therapy has the potential to permit a client to “risk feeling what he is not supposed to feel and knowing what he is not supposed to know” by explicitly deconstructing (reflecting on) past attachment patterns while experientially creating new ones in the present.viii
So how do attachment oriented therapists access that which is disavowed, unknown, undeveloped and not available for conscious or symbolic recall in their clients? The answer to this question leads to the realm of ‘non-verbalizable’ experience and non-verbal communication.
A shorthand for working with implicit relational material is to consider that what we cannot put into words we often either enact with others, embody somehow, or evoke in others.ix I will explain each of these and then offer clinical anecdotes to illustrate them.
EnactmentsAn enactment involves the dynamic interactions which result from the words spoken, i.e., the relational effects of the words. Do they push us away or draw us near? Pull us into the past or move us toward the future? Do they obfuscate or reveal?
I once had a client who was a troubled, bright young man. He was the oldest of three and he was furious with his parents particularly for ‘parentifying’ him in his youth. He and I had good rapport and we were making considerable progress. About ten sessions into therapy he told me he could not believe he was able to be so open with me or how much he was learning about himself. Then, surprisingly, at our very next session he announced that he was finished with therapy. He explained maturely that he believed that clients eventually outgrow
Insights into Clinical Counselling - April 2014
system dominance, a low threshold for nervous system arousal, and diminished cortical control over emotional reactions.x Outwardly there is a tendency toward more pronounced and demonstrative facial and bodily gestures, a preference for physical proximity and for postures involving moving forward and reaching out. Physical movements tend to be less contained and sometimes agitated.xi
The avoidant (hypo-activating) strategy inwardly tends to involve a deactivation of the sympathetic nervous system, a bias toward left-hemisphere cortical processing and parasympathetic nervous-system activation.xii The outward bodily expression of this strategy often involves more restricted movement, less facial expressiveness and limited direct eye contact. It also tends to be associated with pulling back or pushing away and other movements associated with withdrawal as well as diminished bodily responsiveness to relational overtures.xiii
The young man discussed above had an avoidant strategy. He rarely made direct eye contact. When asked about feelings of need or vulnerability, he would often pull back his torso, neck and head and extend his arms straight out in front of him with his palms facing out, his eyes closed and his head shaking “no.”
One day I asked him if he would do an experiment with me: To simply look directly into my eyes for as long as he could tolerate it. After balking, he tried it a few times. Each time he was able to maintain eye contact with me a little bit longer and, as he did so, I said really simple encouraging things like “good” and “that’s it.” I also reflected back to him what I noticed about changes in his face, his breathing and how he held his body. For example, I noted that his shoulders came down a little with one of his exhales and that his eyes and his jaw softened a bit and so on.
While engaged in this exercise, it was as though we fell under some sort of dyadic spell together with all of his awareness focused on staying present with me in this unfamiliar way and all of mine on simply noticing and reflecting back what I witnessed. Afterwards, crying slightly, he told me how hard it was for him to look and me without thinking that I might “just disappear right before his eyes.” Later, he asked me how he could know that our relationship wouldn’t end in a wrenching and painful way as so many of his others had. A long and important conversation followed.
EvocationsClients may also evoke in (meaning relocate to and cause someone else to experience) that which they feel or think but cannot know, name or experience directly. Recent neuroscientific developments have shed some light on how evocations take place. The human brain comes equipped with “mirror” neurons which permit us to sense the emotions and intentions of those with whom we interact. Mirror neurons make emotions contagious explains Goleman, by “letting the feelings we witness flow through us, helping us get in sync and follow what’s going on. We ‘feel’ the other in the broadest sense of the word; sensing their sentiments, their movements, their sensations, and their emotions as they act inside us...we become like the other – at least a bit.”xiv
I had this experience with a client who was an elderly woman who spent a lot of time in her apartment knitting, sewing and doing artwork. She came to see me because she had convinced herself that she had developed a “mental illness.” While she talked (and talked and talked), she had precious few words to describe what she thought was the problem. All she could tell me is that “it” would come over her and she would not be able to enjoy anything, and then “it” would disappear as mysteriously as “it” appeared.
She claimed she was not depressed or anxious. We spent many sessions trying to discern what “it” was, what preceded “it” when “it” happened, what contributed to the abating of “it” and so on, but we got nowhere. In each progressive session she talked more and I talked less. Usually this would be good, but nothing of therapeutic value was transpiring and I was finding it very hard to stay present with her.
She also kept testing the boundaries of our relationship by trying to involve me in her social life. I explained repeatedly that it was not possible and then she would try again from another angle. Feeling exasperated one day, I said, “You know, I am feeling really stuck and confused right now; I want to help and attend to you in the ways that I am able, but it is almost as though I am not really here with you somehow, like you could just be talking to yourself. There is no a back and forth rhythm to our conversations.”
She looked like she had seen a ghost. She said, “How strange, that is exactly how I feel at home when “it” comes over me. I feel all alone with nothing but my own stories and thoughts spinning around in my head. I feel lonely, stuck and confused.” It wasn’t until I tapped into the experience she was evoking in me that either of us knew what she needed help with.
ConclusionThese anecdotes illustrate how therapists can use attachment theory to work with non-verbal client communication by thinking of it as cues and clues to undeveloped relational potential awaiting expression through a reparative therapeutic dynamic. They each involve an interactive tension between repeated experience and reparative experience and the forces acting toward familiarity, stasis and restriction of relational experience and those acting toward exploration, change and expansion of relational experience. “We find aspects of ourselves in the minds of others,” says Wallin. “Whether in the course of childhood development or psychotherapy...the self is discovered (or perhaps created) primarily as it is recognized and understood by others...in a relationship of attachment.”xv
BiographySarah Flynn, MREM, MA, RCC is a therapist in private practice (Synergia Counselling/Consulting) in the neighbourhood of Fernwood in Victoria, BC. She specializes in attachment issues, relational trauma, dissociative processes, non-verbal communication, and helping those with loved ones with mental illness. Feel free to contact her with questions or comments by phone at 888-316-0819 (toll free) or by email at [email protected], or visit (www.synergiacounselling.com) for more articles and other material.
5
Insights into Clinical Counselling - April 2014
in our classrooms is on building these social-emotional assets of cooperative play, self-regulation and perspective taking. In that model, the first few years of educational focus is solely on building emotional competencies, relegating the pursuit of academics to the latter elementary years.
Social-emotional learning is not only about student wellness and building internal assets for life success, but it is also teacher wellness. Educators are the models for our children. We must be passionate about teaching for children to be engaged in learning. Our dropout rates are significantly high, and are a global concern. In Europe, a term, NEET, has been developed to capture youth who have become disengaged, not educated, employed or in training programs.5 We need to make some changes to how we are educating our children and youth.
Rita Pierson,6 a veteran educator suggests that children do not learn from people they don’t like. For teachers to open up our hearts and create these caring conditions for learning, we have to be socially, emotionally and physically healthy ourselves. We need to develop self-awareness, social-awareness and self-management skills. Equally true to parenting, it is critical that we are responsive rather than reactive and impulsive, in our problem solving and in our interactions with kids as these encounters are all opportunities for learning.
Teachers are considered “stress hardy” if they remain in the profession more than 5 years. They are “on” all the time. The demands are increasing: From a multitude of diverse learning styles, and increased accountability measures, to a changing partnership with parents. We teach who we are; we need to be ever so mindful of what we convey to our students and of how we do so.
6
We need to build relationships and classrooms that are welcoming, challenging, inclusive, and promote risk-taking. A key to improving the academic achievement of our students in the 21st Century is the degree of relational trust established with adults. Safe and caring climates of relationships in our classroom/homes will encourage children to pursue their creativity and passions to become independent, life-long learners. We need to “work with” our children, not “to” as in the traditional, compliance-based model of education.7
It is the delivery of these SEL skills through instruction, and mostly through modeling and action, that builds social citizenship in our youth. This occurs through a continuum of offerings in our schools and in our homes, from daily interactions of smiling and saying “hello,” to integrating concepts into our curriculum such as, examining acts of pro-social behaviours in literature, analyzing the cost-benefits and ripple effect of aid to Third World countries in maths, to school-wide community initiatives or programs that focus on conflict resolution and generosity. SEL is a method of developing sustainable internal assets in our children and youth so they can make choices that reflect strong moral values, rather than reacting to consequences for a given act or behaviour.
The Ministry of Education in British Columbia is currently developing three cross-curricular competencies, one of which specifically highlights social-emotional competencies: They are critical and creative thinking skills; communication (language and digital literacy) skills; and personal and social competencies.
To find success in this ever changing and interdependent world, students require a new skill set. They require resiliency, and according to Carol Dweck, they need a growth mindset:
Social-emotional learning (SEL): A relatively new concept to the educational world, but now a much regarded, necessary element in any curriculum. Social-emotional learning is a philosophy, a lens, into how we interact with others. It is Education for the Heart.1Aristotle aptly wrote, “Educating the mind without educating the heart is no education at all.” Research states that schools that create learning environments that help students and staff develop greater social and emotional competency, help ensure academic and personal outcomes for students, as well as higher levels of teaching and work satisfaction for staff.2
“Social-emotional learning is the process of developing students’ social-emotional competencies, that is, the knowledge, skills, attitudes, and behaviours that individuals need to make successful choices.”3
According to leading researchers at the Collaborative Association for Academic, Social-Emotional Learning (CASEL) is comprised of five competency areas including: Self-awareness, self-regulation, social awareness and perspective taking, relationships skills and responsible decision-making.
Social-emotional learning is the process through which we learn to recognize and manage emotions, care about others, make good decisions, behave ethically and responsibly, develop positive relationships, and avoid engaging in negative behaviours.
Building these types of internal assets, through providing classroom climates of relationships and caring, allows students to pursue their passions by taking risks and learning to manage failure, which is critical to the potential success of students.
We only need to look to the Finland educational model4 to see the successful outcomes that accrue when the focus
By Stacey Burnard, MA, MBA, B.Ed., Contributing Writer
Educational Transformation: Social Emotional Learning (SEL) in our Schools
Insights into Clinical Counselling - April 2014
7
That you can succeed through hard work, and are able to manage, and in fact, view failure as a learning opportunity. They require an understanding of emotional literacy as workplaces now demand these “soft skills” of social relatedness.
School districts are beginning to undertake more SEL programming as well as organically develop improved cultures of caring in their schools. Secular mindfulness programs, such as the MINDUP program, which are supported by neuroscience research, are bringing mindfulness, listening and the honing of attention back to schools. Concepts such as acts of kind-ness, acts of gratitude and giving back to the community through acts of generosity and outreach are supporting students in recognizing the satisfaction of giving and building community and social citizenship. Interest in the area of self-regulation is burgeoning as the need for emotional modulation and attentiveness has increased.
Should schools be teaching it?
Education is in a transformational time. Education must include the so-called “soft” skills not just the “hard,” academic knowledge. In order to be successful we need to know our strengths/weaknesses, effectively work in teams, and thereby understand perspective and empathy, make decisions that are not only based on critical analysis and must be effectively communicated, but reflect compassionate understanding, and we must be able to overcome obstacles and persevere.
BiographyStacey Burnard, MA, MBA, B.Ed, Yukon, Canada has worked in the field of educational for 20 years. With a background in clinical psychology she has held posi-tions in the area of special education, behaviour specialist, educational psychologist and social-emotional learning. She has written for Insights into Clinical Counselling and a number of BCTF magazines, some of her FASD articles are required reading at a Masters level at UBC and she has published Putting the Pieces Together: Building a Curriculum of Caring in 2008 and has presented at FNESC, BCTF conferences and the CCBD International conference in U.S. [email protected]
Social-emotional learning is the process through which we learn to recognize and manage emotions, care about others, make good decisions, behave
ethically and responsibly, develop positive relationships, and avoid engaging in negative behaviours.
Insights into Clinical Counselling - April 2014
Counselling Clients With
Fibromyalgia
8
Insights into Clinical Counselling - April 2014
Insights into Clinical Counselling - April 2014
9
This multitude of symptoms and lack of definitive understanding causes havoc when clients are attempting to come up with a diagnosis for what is wrong. It can often take years of testing and re-testing to recognize and understand symptoms as a cohesive set rather than as individual problems, and to formulate a useful diagnosis. Often, by the time they reach the counsellor’s practice, clients have experienced repeated frustrations, disappointments and dead ends in their search for answers and relief.
Despite the wide ranging symptomology, the client demographic I see tends toward a “type.” Typically, but not always, clients with FM tend to be female, in their 30s-40s, educated, articulate and, most significantly, highly motivated to achieve their goals. Some self-identify as Type A. Most tend toward perfectionism, with a coping style leaning toward a reinforcing negative belief such as: “It’s not enough;” “I can do more;” or “I have to be better.” Some
will even recognize that they feel they must prove themselves to the world as being “good enough.” Often this involves comparisons, or fear of social judgment from others.The “not enough” belief is typically, but not always, transmitted through social learning from a family-culture entailing a lack of verbal processing of feelings or con-scious self-reflection, or lack of awareness of the impact of stress on the self (self-care).
Female clients tend to have female relatives who model this lack of self-care coping style coupled with high standards and a judgmental or “should-ing” approach to self and others. Several studies indicate that women who have a family member with FM are more likely to have FM themselves,
but the exact reason for this, whether it is heredity, shared environmental factors, learned coping strategies or all three, is unknown.
Most clients report some kind of illness in their childhood or adolescence, and then report years of productivity, achievement and “can do” energy in their lives in their 20’s. Because of these boon years, the belief system of “I am good when I do more,” is reinforced as the right approach. However, most clients then report one or a series of stressful incidents in close succession, either positive or negative (marriage, illness, birth of child, loss of job, job stress, death of family member, moving, financial stress), and their picture changes.
The first incidence of FM or first episode, typically goes unrecognized or ignored in favour of the preferred coping strategy of “I can do more,” or “If I work harder I will get through this.” Repeated incidences of worsening FM flare-ups are ignored, “pushed through,” or misunderstood until the FM worsens to the point that the client can no longer overcome them; their coping strategy no longer works. At this point, clients with FM engage with the medical system in their coping fashion of “I can beat this,” or “If I work hard enough I can solve this.” Sadly, however, diagnosing and treating FM is not straightforward, nor does it produce desired effects in a timely fashion.
In the field of chronic pain, there are some conditions that seem to appear frequently in the make-up of my clients. Among these conditions is Fibromyalgia. While the demographic of clients with Fibromyalgia (FM) seems to fit a pattern, the condition itself can be challenging to work with; FM is better understood today, however its origins and course remain only theorized by medical professionals.
The word “Fibromyalgia” comes from the Latin for fibrous tissue (fibro) and the Greek for muscle (myo) and pain (algia). It is a chronic condition which effects up to 2% of Canadians (Arthritis Society) and is characterized by both physical and cognitive symptoms. Physical symptoms include widespread pain, diffuse tenderness (allodynia), swelling, muscle spasms and tightness, numbness or tingling, stiffness, digestive disorders (FM is often misdiagnosed or co-morbid with Irritable Bowel Syndrome) and fatigue. Cognitive symptoms include difficulty concentrating, poor memory, inattentiveness (“fibro fog”), anxiety, depression, irritability, and heightened sensory sensitivity (bright lights, smells, colours etc).
The cause of fibromyalgia is as yet unknown in the medical research community; however there are a number of theorized commonalities and these can be seen in the typical FM client. Often, the onset of FM is associated with a physically or emotionally stressful or traumatic event, such as an automobile accident or loss of loved one. I have found that a period of intense stress is a hallmark of FM in my clients.
A theory which has been borne out in my clients is a past history of viral infection. Some clients have had pneumonia, or mononucleosis, or some viral illness in which they were physically debilitated and severely ill. It is theorized that FM is the result of a compromised immune system response resulting from viral damage at an earlier time in life. This damage, accompanied by the onset of stress, causes the nervous system to malfunction and produce a variety of seemingly unrelated symptoms.
Along these lines, researchers are also examining how the Central Nervous System (CNS) processes pain. Research suggests that FM as well as some other chronic pain conditions, is caused by a problem in how the body processes pain, or more precisely, a hypersensitivity to stimuli that normally are not painful (called central sensitivity). After an injury or illness, the brain can begin to be oversensitive to pain stimuli and can begin to sense pain where there normally would not be. It is possible that the nervous system is put into overdrive, causing pain, and that this neurological communication is out of balance in people with FM.
Researchers at the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS) are currently looking at genetic possibilities, speculating a genetic influence on the regulation of painful stimuli. According to this theory, people with FM may have a gene or genes that cause them to react strongly to stimuli that most people would not perceive as painful. There have already been several genes identified that occur more commonly in FM patients.
By Megan Hughes, MA, RCC, Contributing Writer
Insights into Clinical Counselling - April 2014
Insights into Clinical Counselling - April 2014
Clinical Hypnosis for this work, as it can be quite distressing to examine long-held beliefs and an alienated or negative relationship with self.
Making lifestyle changes reflects a new approach to self. Often, clients will need guidance regarding sleep and the development of sleep routines in order to facilitate as much replenishing rest as possible. Many people with FM have problems such as pain, restless legs syndrome, or brainwave irregularities that interfere with restful sleep. Without restful sleep, fatigue and other symptoms are worsened.
As well, physical exercise and adequate nutrition is directly related to self-care, and typically the client with FM has not created time in their lives for a regular routine of healthy diet and exercise; the last thing a client will be motivated to do is exercise when they are feeling pain and fatigue, or choose to eat nutritionally when they are craving stress-foods.
However, research has repeatedly shown that regular exercise is one of the most effective treatments for FM. Exercise helps to regulate hormone levels, increase circulation and decrease stress, all of which are good for reducing inflammation and perceptions of pain. Clients with FM should be encouraged to find a non-impact physical activity that is tolerable to them (swimming, walking, tai chi, yoga) and start gently, slowly increasing duration and intensity over time.
The underlying belief system that encompasses all of these lifestyle changes and which is so important for a client with FM to accept involves changing her approach to life and herself from that of “doing” to that of “being.” It can be extremely difficult for high-achievers to be satisfied with accepting “being” as their standard of achievement when their families, their lives and their self of selves have been built on “doing.”
There can be resistance and pain in this idea, a belief that it is fine for others, but that it is “not enough” for them just to be a happy, healthy person. They grieve the loss of their ability to “push through” and dominate the tough parts of life and they worry that others will judge them as failing. This line of counselling can sometimes lead to questions of faith, belief and meaning, in the clients’ efforts to orient themselves around something other than relying on their own individual ability and achievements for their sense of satisfaction in life.
Learning how to self-care means ultimately learning how to live with their diagnosis. FM is not a condition that is curable or that in time will go away. Once a client has reached the tipping point, it seems the CNS simply does not fully recover. Therefore, clients must learn how to be in constant fluid communication with their bodies, their lives and themselves.
BiographyMegan Hughes has been a Registered Clinical Counsellor in Vancouver working primarily in the areas of PTSD and chronic pain for 15 years. Megan’s research in these areas has been published in the Journals of Counselling and in the Journal of EMDR (pending publication). She is certified to use EMDR and Clinical Hypnosis with chronic pain and with PTSD, and utilizes these modalities successfully with children and adolescents as well. She can be reached at Vancouver Counselling and Pain Management at 604-734-2779 or [email protected].
10
Despite approaching specialists and appointments with a “can do” attitude, clients typically don’t experience the fast results they are used to; their self-image of highly capable, effective and achieving starts to erode; there are few other strategies to employ other than the favoured one, and it now causes increased pain and debilitation. They can begin to experience intense anxiety, distress and depression, and over time wider areas of life are affected. Losses due to illness mount up and coping is not adequate: Employment, finances, relationship, sense of self, goals, dreams, life plans.
It is at this point that I usually see a client with FM for treatment. The medical system has, in time, provided a diagnosis, however, clients tend to want to “get back on track” to their previous functioning, a desire which reflects the resistance to letting go of their original coping strategy. They often report feeling “like a failure” at not being able to solve this problem, and feeling diminished and vulnerable if they are dependent on parents or spouse for support. They know that something has to change, but they don’t know what or how.
It is important at this point to ensure the client has an adequate team of health professionals to work with. They will need a physician aware of their diagnosis, a Registered Massage Therapist, or Physical Therapist, sometimes nutritionist and therapist. Optimally all professionals will be aware of and educated about the presentation, effects and course of FM. Therapeutically, working with clients with FM requires understanding the losses they have incurred due to their own body’s manifesting pain and discomfort for what seems to be no reason, and understanding the resulting secondary losses.
Often I work with clients firstly to foster a positive relationship with their bodies, as they can feel alienated from themselves, sometimes even beginning to dis-integrate their self-images by viewing their bodies as separate, or as being their enemy. When they begin to reintegrate with their bodies, the process, and their own pain, they can then work to let go of coping strategies which no longer work for them, and to develop new approaches to themselves.
This work must be as holistic as possible, meaning, we must try to help them deal with different areas of change in their lives at the same time; coping with pain and bodily sensations, renewing self-image, grieving losses, providing strategies for self-care and relationships, and reorienting to life.
The challenge of FM is that the client is undergoing massive change, in all areas of life. Their previous strategy of working through pain and challenge involved compartmentalizing their own needs in favour of achieving goals. In learning a new strategy, compartmentalization must be abandoned in favour of viewing their lives as a system in which each area is of equal value.
Learning how to value self-care is an area of great challenge. There can be tremendous guilt or frustration regarding spending time on themselves when there are external things “to do.” Learning how to focus on the self requires clients to come to terms with a lifetime of unmet needs, negative messages and reinforced behaviours. It also means reorienting and learning to value bodily cues that were ignored in the past. And it often means re-examining relationships with others, including family of origin. I sometimes utilize EMDR or
Insights into Clinical Counselling - April 2014
Insights into Clinical Counselling - April 2014
11
By Seth Raymond, MEd, RCC, Contributing Writer
Imposition of Order into Tales of Woe
His employer “insisted” he come to counselling because his work was suffering. The employer is an idiot and has no understanding.
Jim’s wife, Mary, has left him and is refusing him access to his children. She is poisoning his children against him and is threatening to call the police if Jim continues to insist he has the right to see his children. His children refuse to talk to him and the school has phoned his wife when he tried to take them out of school. He’s not leaving his house, damned if he will. His wife can go to hell and her friends too. And how is he going to live without her – she’s his whole life? She’s demanding money and gone to a lawyer. She’s a backstabbing bitch.
Beth lets Jim unload; only occasionally putting an oar into the outpouring to interrupt particularly unhelpful spots in Jim’s narrative. She will intentionally ask a question that is outside of the immediate context of what Jim is talking about. This will stall the negative flow and necessitate a reordering of his thought and emotion. Beth’s interruptions and redirects are annoying to Jim. Annoyance at the counsellor at this stage, as long as it is kept within acceptable limits, is okay.
Beth: Wait. How many children do you have?Jim: Two. Billy and Kathy.Beth: Both kids from … you and Mary?Jim: Yes. What the hell you think?
More outpouring about all the wonderful things he has contributed to the marriage and how they aren’t appreciated. This is immediately followed by more examples of Mary’s bad behaviour.
Beth: And their ages? What grades are your kids at in school?Jim: Billy is 5 in kindergarten and Kathy is ... 7, I think, in grade 2. She’s daddy’s girl. Her teacher stinks. I don’t know how many times her mother and I have gone to the school this year to complain about Ms. Hatchet’s yelling at her.
The world is not just out there, and our task is not to just become better and better at describing and understanding it. Instead each individual creates their world through cooperative interaction with the externality which is not them. Our willingness to engage in this mutual exchange and our openness to adjust our understanding and behaviour to better align with externality is a measure of our personal agency.
The inability or unwillingness to modify our engagement with our world so as to maintain an appropriate alignment results in unproductive behaviour and inappropriate understandings. This degradation in agency can be addressed in counselling. Strengthening a client’s agency will encourage that client to correct misalignments in behaviour, emotion, and understanding.
To explore this process directly, let us drop in on the first session with Jim, a married, employed man in his mid-30s.
Jim has never been to counselling before and is just coming through the door into the counselling room followed by his counsellor, Beth. Beth has just met Jim in the waiting room and she directs him to a chair on the other side of the coffee table.
They both sit. Beth indicates the thin, closed file sitting on the coffee table, “Well Jim, you’ve signed the necessary forms. Have you any questions regarding confidentiality?” Jim shakes his head. “About counselling and how it works?” Jim again shakes his head. “Okay, I want to reassure you that our conversations will be confidential … with the limitation of danger or harm to others which I must divulge to prevent anyone getting hurt.”
Jim looks around the office. Beth continues, “Well okay, I’ve read the intake notes and they indicate you are having marital difficulties. Is that correct?”
Jim takes this question as the cue to immediately launch into a rambling account of his troubles.
Insights into Clinical Counselling - April 2014
12
rationality. She could start expanding on any of these. Jim continues.
Jim: She lies to the children about me. Says I’m to blame for her leaving. She’s making me out to be a monster. The kids won’t even come to the phone – or she says they won’t.Beth: So you think she’s lying about you? You think she’s being dishonest?Jim: She’s a liar!Beth: So honesty is important to you?Jim: Yes, of course, honesty is important to me. What do you think? You think I like liars? You need honesty in any relationship. And she’s not being honest.Beth: Has your wife always been dishonest? Because you have a strong commitment to honesty, I can’t see how you would marry her in the first place if she’s typically a dishonest person.Jim: No, she is usually honest … but she’s way off kilter now.Beth: Hmmm. If your wife was being honest, in this situation … you know like she usually is about everything else … what would she be saying differently than she is saying now?Jim: What?Beth: Let’s imagine your wife was being honest about leaving you. Can you imagine that? Now, keeping her strict honesty in mind, tell me what she would say to me if she was sitting right there where you are now. What would she tell me was the reason she left you?
Beth has decided to latch onto the value of honesty. Jim never introduced the concept openly but he has strongly accepted Beth’s expansion of the notion. Here Beth is deliberately and openly imposing order onto the sessional experience of both Jim and herself. Heretofore Jim’s upset and his impassioned story telling has dominated the session. To this point Beth has kept her interactions lightly directive. Now she has chosen this point to begin the process of quieting Jim’s turmoil. She has noticed the client’s weak expression of value, blocked the client rushing past without noticing it, and directed his attention to the concept of honesty.
At this important juncture, Beth’s intent and Jim’s are quite different. Jim pounces on the notion of honesty as simply another way to condemn his wife’s behaviour; the counsellor uses the notion to halt the narrative flow and steer it in a different direction. The counsellor has entered a pivotal difference into the interaction between her and the client.
Beth has asked Jim to imaginatively be his wife and give an honest account from her point of view of the breakup. This is, for all intents and purposes, an impossible task for him at this stage. Beth has brought Jim’s outpouring to a full stop. She has challenged Jim’s whole account so far. Beth waits. To proceed Jim has to apply thought; he has to consider his templates. This is Beth’s first open attempt to jump start Jim’s stalled sense of agency.
Now Jim may very well balk at being asked to imaginatively give an honest statement of his wife’s position. Good. Or he may even attempt such an amazing thing; also good. Or he may tentatively start to correct some of his more theatrical statements about his wife. Good too. It is to be expected that
Nothing has helped -Beth: Sorry to interrupt, but continue with your account of your marital situation.
After a slight hesitation, Jim continues.
Jim: I came home from work and she’s gone! With my kids! A lousy note that said she was going with the kids to Brenda’s. That’s her so-called “frieeeeend.” Ha! That bitch has to take a lot of the blame for this. She’s never liked me. She’s poisoned -Beth: How … how … sorry to interrupt again, how long have you and your wife been together?Jim: Since high school. We married the same year we graduated from high school.Beth: And her name again?Jim: What? Mary. Mary is my wife’s name.Beth: No. No. I meant your wife’s friend’s name. What was her name again?Jim: Brenda. Miss oh-so perfect Brenda.
The outpouring continues, but the flow is lessening. Jim expands on his working two jobs when they were first married so they could afford a mortgage. He continues with a story about taking Kathy to dance classes twice a week because Mary needs some time to herself.
Beth has quickly realized that Jim has “lost” his sense of agency. He gives the agency for the control of his emotions to his wife and her actions.
Personal agency is the ability to impose structure and meaning onto sensation, the necessity to make judgements and choices, and finally the competency to take helpful action. Jim has given up on much of his personal agency and instead is simply reacting to circumstances that have overwhelmed him. Beth starts looking for remnants of personal agency in Jim’s account; traces of important meaning templates that Jim uses to organize his understanding and action. Values are one such template. They are universal and most importantly from a counselling viewpoint, are easily extracted from the narrative flow. Beth is alert and starts a search process by deliberately steering Jim’s narrative.
Beth: Sorry to interrupt again. I’m just trying to get a complete picture of your situation. Your workplace asked you to come in to counselling, I believe. Did they suggest you take some time off or something?Jim: No they bloody didn’t. I’m one of their best men; I give good value for my wages. I’m being considered for promotion.Beth: So why were you asked to go see a counsellor? Was there a change in your performance at work?Jim: I shouted at the foremen. He’s a jerk who’s always on my case. I just lost it. He’s an annoying little ferret and I told him what I thought of him for once.Beth: Oh I see. So your supervisors at work have noticed you’re not your usual self, because I presume you haven’t done such a thing before?Jim: No. I’m always calm and reasonable.
Beth notices a possible value template: hard work with perhaps the corollaries of fairness, ambition, pride, self-control, and
Insights into Clinical Counselling - April 2014
Jim will continue to dress himself in white armor and his wife in the dragon suit for some time. Not important at this juncture.
What is important has already occurred. He has allowed himself to be taken out of his self-directed horror show in which he is the powerless victim. He is, in one way or another, honestly or not, imposing order onto his experience by applying the value of honesty onto his account of the matter. He is changing his remembrance of what has occurred up to now in this “whole wife leaving him” matter and, with the assistance of the counsellor, he will change his future engagement with it. In other words, he is regaining his agency.
Beth is running out of session time. She wants at least 5 minutes left at the end of the hour to write up some notes and provide a bit of transition for herself before she sees her next client who is likely already sitting in the waiting room. She wants Jim to further capitalize on the change in perspective in which she has engaged him. She furtively checks the time, 8 to 10 minutes before she has to have him out the door.
Beth: Well Jim, we are running out of time. We need to finish off this session by ensuring you’ve gotten something useful you can take out of here with you. What has been helpful to you in this session?Jim: Umm… It felt good to be able to tell someone what my wife is doing to me.Beth: I’m glad of that, but no, just unloading your hurt doesn’t help you. It may make you feel better temporarily, but it doesn’t change your situation. What can you take away from here that will help you? What can you do to improve your situation?
Now Jim may not be able to voice what Beth wishes from him. Indeed since most of the session was spent dealing with the Jim’s emotional outpouring, and furthermore he is still in a highly stressed state, this is not surprising. But Beth is not really expecting him to provide an answer, pleasant if he did, but she expects he will not be able to do so. No, what Beth is doing is interrupting the exit of the client.
Jim will not just physically go out the door. It is likely he will rapidly re-establish his exaggerated fiction of himself as the victim of a villainous wife unless Beth anticipates this process and addresses it now. This is the purpose of her question, “What can you do to improve your situation?” She is going to give a last boost to Jim’s newly awakened, barely functioning sense of agency: A last highlighting of his need to meaningfully engage with what is happening in his life. She is going to more clearly state what he has to do. She is going to spell it out for Jim.
Beth: What can you do to improve your situation?Jim: I don’t really see …Beth: You’re a man who values honesty. Is this true?Jim: Yes. I try to be an honest person.Beth: Good. Good. To me that is the most powerful thing I learned about you today. You’re an honest man. And I’m sure you have other admirable qualities that we were unable to uncover this session.Jim: I’m … a good … person.Beth: I’m sure you are. And you’re going to need all those
good qualities to get through this situation. You tell me you want to get back together with your wife. You tell me she’s angry and unreasonable.Jim: She’s a nightmare, she’s – Beth: Sorry to interrupt, but we’re right out of time here. If your wife is angry, does it work to get angry at her right back? (Jim shakes his head.) If she won’t listen to you, does it help if you yell louder? (Jim shakes his head.) You know the woman. (Jim nods.)Beth: (Pause) If you want any chance of getting her back, she has to calm down. (Jim nods.) What are you going to have to do?Jim: Not be so angry maybe?Beth: (Rising, client rises also) Yes. Yes. You have to start seeing this angry, hurt woman. You know her. You’ve been together for years and years. React to her in ways you know will not make her more upset. You can do this. Not seeing your kids this week is not the issue. Look long term. You want her back. What can you do to make that more likely?Jim: Umm …?Beth: (Walking with Jim towards the door) Well, I’m sorry I have another client waiting. I think you have some good ideas on how to improve things. (Client nods.) If you want another session, talk to the receptionist on your way out or phone in later. If you return, I’m going to ask you what you have been doing to calm down the situation. What YOU are doing, not what Mary has been doing. You understand that? (Jim nods) It has been a pleasure meeting you. Bye now.
Beth returns to the coffee table and begins to scribble a few notes. (Time in session: 56 minutes.)
Notes - Session #1:Relationship breakdown. Blaming. Feels situation is out of his control. Introduced honesty - accepted. Some small pull back from immersion. Another possibility is self-control – he lost it at work. Ended with praising his strengths and the need for him to make the situation better. If returns, ask Jim what he has done to improve things. How has he improved things at work?
Finished with her notes, Beth closes the file, puts it under her arm and enters the hallway. She gives the file to the receptionist on her way by and picks up Client’s B file – a returnee. In the waiting room she makes nodding contact with her next client who puts down a magazine. The client and Beth proceed to the counselling room.
Let us recap what Beth has accomplished in this first session with Jim. Besides allowing Jim to unburden himself and join with her, she has weakened Jim’s tendency to fabricate an unhelpful account of his present circumstances. She has directed his attention back to himself and what he can do that would be helpful. She has rekindled his sense of being in control and having certain qualities which he admires in himself and others. And finally she has provided structure for the next session if Jim should return.
BiographySeth Raymond is retired from his position as a Behaviour Specialist for School District No. 57. Seth has worked as an EFAP counsellor and as a clinician in Child and Youth Mental Health. He is currently providing consultation and counselling support in Prince George.
13
Insights into Clinical Counselling - April 2014
14
email service, and even if they do, there is a new factor to consider.
Recent news stories graphically describe routine targeting of email communication by American, British, and other Anglophone security services. In the words of the Guardian correspondent Jack Schofield:Following the Snowden revelations, no data held online by any American company can now be considered private, and this could include any site running in the .com domain. Given the apparent complicity of the British secret services, I’d assume it also applies to data held online by any UK service providers as well. (www.theguardian.com/technology/askjack/2013/aug/15/gmail-google-email-privacy)
If you really want secure email, you probably have to source an email service in no way beholden to authorities who might inquire into your correspondence, ensure that the service offers encrypted connection, and encrypt your email content at source. Otherwise, in the words of a friend who advises local government in the UK: Don’t put anything in an email which you would not wish to see on the front page of your local newspaper.Hence my first response when the supervision group plan was described: Hold that email! The front page of the local newspaper, or an equivalent, is almost certainly going to violate Principle 1, item 17 of the
How will others view this? What meanings will it be seen to have? What might its long-term consequences be?Interrogate any plan or course of action, and these kind of questions can lead in surprising and unexpected directions.
Now add a concern to do what is ethically and legally right. Season it with a desire to maintain personal and professional integrity.
Acknowledge the very reasonable need to maintain a reputation. Stir in a necessary measure of creativity. Professional decision-making is not simple.
A PlanIt is just this potential for complexity that prompts BCACC to offer an Ethics and Standards consulting service to members. Two heads usually are better than one. And as the person currently supplying that second head, I was recently invited to help think through a plan, and a set of possible actions, with important ramifications.
On the face of it, the plan was laudable: Hold a meeting of counsellors at which aspects of current clinical practice would be discussed, ideas and resources shared, and mutual professional support provided.
Keep a record of the issues and ideas discussed at the meeting.
Share this record by email with other local counsellors in order to more widely distribute knowledge and
insights derived from the meeting and encourage attendance at future meetings.In other words, the plan was to set up what I think of as a “peer supervision group,” record its proceedings, and then distribute the proceedings by email. Those proceedings would, of course, not contain the names of any clients.
Holding peer supervision groups, and sharing ideas and resources, is a great idea. It clearly puts into practice Principle 2, item 5 of the Code of Ethical Conduct:To practice the Principle of Responsible Caring, RCCs will… Engage in continuous learning and professional development based on ongoing assessment of needs.However, keeping a record of proceedings and distributing it by email is an entirely different matter.
Email Multiplies ComplexityIt was the email aspect of this plan which prompted an invitation to me to help think it through. Combining counselling with email generates complexities that counsellors need to tread warily amongst. They mostly have to do with privacy and confidentiality. BCACC offers a comprehensive Standard for the Use of Technology in Counselling with extensive guidance on the use of email by counsellors. It is well worth reading. Here, I shall focus only on those issues directly relevant to the current peer supervision group plan.
Simply put, email communication is only secure and can, therefore,
only be consistent with confidentiality requirements, if one of the following holds:The email is itself encryptedThe email is being sent between two parties who are both using email services which utilize encrypted connectionEncrypted email is encrypted on the sender’s computer using a key or password shared with the recipient. The recipient unlocks the email once it lands.
There are shareware and inexpensive programs to make this possible. Their downside is that every message must be separately encrypted and the key made available to recipients. Encrypted connection is available when a website address is preceded in the browser’s address bar by a lock icon. I just logged into the Exchange email service I use, clicked on that lock icon thing, and here is what I read:Connection Encrypted: High-grade Encryption… The page you are viewing was encrypted before being transmitted over the Internet.
Encryption makes it very difficult for unauthorized people to view information traveling between computers. It is therefore very unlikely that anyone read this page as it traveled across the network.
In other words, if I send an email to someone who is using a similarly protected email service, we have a reasonable expectation of confidentiality. But it is essential that the recipient is using such an email service. Not everyone does use secure
By Clive Perraton Mountford, Contributing Writer
It Looked Like a Good Idea: Thinking Through Confidentiality
ETHICALLY SPEAKING
Insights into Clinical Counselling - April 2014
15
Insights into Clinical Counselling - April 2014
that get us into trouble are benign ones—the plan in question is contrary to Principle 1, item 1 of the Code of Ethical Conduct.
Sometimes, No Notes is BestIt will probably now come as no surprise that I went beyond advising against sharing the proceedings of a clinical supervision group by email or even snail-mail. I advised against keeping any record of those proceedings.
My reasoning was as follows: Such a record would be illegitimate unless all parties referenced by it were to consent to it; Obtaining that consent would be a cumbersome business; The cumbersome business would be made worse by a nasty, logical difficulty involved.
The difficulty kicks in when we seek consent from a group of clients who are not known to each other. To be able to say that a client has consented to their counsellor sharing a document referencing them, it is reasonable to require that:• The client has read and understood the document;• The client consents to all references to themselves;• The client is not being influenced by a need or a desire to please the person making the request;• The client is cognisant of all probable short and long-term consequences of acceding to the request.
But how can the document be shared with all persons referenced by the document prior to those persons giving their consent to sharing? It cannot.
Perhaps there are ways around this catch-22 type situation, but they are not going to be simple. Easier to say: Records of the proceedings
Code of Ethical Conduct:To practice the principle of Respect for All Persons and Peoples, RCCs will… Ensure the privacy and confidentiality of client information in accordance with legal principles and professional standards.
Furthermore, if BCACC is involved in distributing such an email, then BCACC is arguably on the wrong side of the Personal Information Protection Act.
With Good Intent The counsellors putting together the peer supervision group plan had a response to all this, and it showed that confidentiality had been considered. To paraphrase: We’ve removed all names and identifiers from the document we plan to email. I read the document.
Names were absent, but there remained sufficient detail to enable identification by someone who already knew a person being discussed in the document.
Think of it this way: If I was your client, and you put a discussion of my psychopathology into the public domain, and I read it, and I identified myself, I would be very unhappy. I would have reason to be very unhappy unless I had clearly, freely, and explicitly consented to that distribution.
Had the clients discussed at that peer supervision group meeting given such consent? Some had given a consent that might be considered to extend to the plan, and some had not. Even those who had provided some measure of consent had arguably not done so in full recognition of the possible long-term consequences of the plan.Therefore, with entirely good intent, the counsellors
planning distribution of a record of their group meeting were risking:Serious damage to their relationships with the clients discussed; Ethical transgression; and Possible legal transgression.
I advised that the only possible way to distribute the document would be by entirely secure means to no one other than participants. Even then, I added, I would have misgivings about doing so.
Suppose that a secure form of email transmission was used. There would still remain a need for each recipient to ensure secure storage of that electronic data upon its arrival at their computer. The ways to do that are to:Store the download in an encrypted form; Download email to an encrypted hard drive; or Download email to an encrypted mailbox.
Given that each recipient meets one of these requirements—or even if snail-mail was used for delivery—information could still somehow go astray. For sure, taking all reasonable precautions against straying should protect against ethical or legal transgression, but it cannot protect against damage to relationship.
It’s All about Respect…The root difficulty here—and the real problem with the plan at hand—has nothing to do with technology or email. It is that the peer supervision group records would involve counsellors:Sharing information about their clients with other
professionals; and Committing that information to writing without the full knowledge or informed consent of the clients involved.
Sharing information is essential to supervision and professional support in all its forms, and supervision and professional support are profoundly to be encouraged. Principle 1, item 18 of the Code of Ethical Conduct states: To practice the principle of Respect for All Persons and Peoples, RCCs will…
Engage in appropriate consultation and supervision.At the same time, we must always let our clients know that
we engage in supervision. We must explain that our work and relationship with them may be discussed in a supervisory context subject to the same confidentiality guidelines as our work with them. We must let our clients know that we keep clinical records. We must be sure that they consent to these things.
We are required by Practice Standards and to some extent by law, to do all this. But perhaps most simply we are required by Principle 1, item 1, of the Code of Ethical Conduct to:Demonstrate respect for the unique worth and inherent dignity of all human beings.It would be contrary to this respect, and contrary to the dignity of our clients, to discuss them in a context unknown to them or commit details of our work together to documents they do not know about.
Really, the issue is that simple.
With the best of intentions—and so often the intentions
16
Don’t put anything in an email which
you would not wish to see on the front
page of your local newspaper.
Insights into Clinical Counselling - April 2014
and inherent dignity of all human beings to be a party to someone exposing themselves in this kind of way.
In fact, everything I have concluded in this discussion can be derived pretty directly from the requirement to demonstrate that respect.To conclude, then, I offer the following suggestion: Hold tight to respect for the unique worth and inherent dignity of your clients, your colleagues, and yourself.
So far as you can, foster it in yourself and in your colleagues. Interrogate plans and actions thoroughly in light of it. Ask whether your unique worth and dignity would be compromised if you were on the receiving side of the plan or action.Professional decision-making is not simple, but if this is where you clearly and explicitly ground those decisions, you are unlikely to go far wrong.
BiographyClive Perraton Mountford is BCACC’s Board appointed Ethics and Standards consultant. He is available most days to discuss matters pertaining to Ethics, Standards, and clinical practice with RCC’s. To contact him either email [email protected] or call BCACC Head Office for his contact information. Clive has a PhD in Philosophy and undergraduate degrees in Philosophy and Early Education from UBC. His counsellor training was at the University of East Anglia and involved an MA in Counselling Research plus Post-Graduate Diplomas in Person-Centered Counselling and Experiential Psychotherapy. Clive is a counselling therapist and supervisor in private practice, an applied ethicist, and a focusing teacher. He is active in BCACC as Chair of the Ethics and Standards Committee, member of the Executive Committee, and a member of the Continuing Competency Committee.
2417
The first prong is to obtain informed, reflective consent consistent with the four bulleted points outlined above.
Personally, I talk through my plan with the client or ex-client before writing anything. Then I ask them to read and consider all passages which involve them. I suggest that they think ahead, if possible, to a time far in the future when our work together is a relatively distant memory and ask themselves how this planned publication might appear to them then.
In addition, I only approach clients I believe well able to make a free, informed choice, and clients who are likely to feel the same way about their choice in 20 years’ time.
Consistent with all this, I sent a draft of this article to a spokesperson for the supervision group counsellors. In the feedback accompanying permission to publish was the following: “You gave me a new standard for confidentiality: Does the person giving consent have a full understanding of what they are agreeing to now, and how it could be shared in the future, and in what format?” Exactly.
The second prong of the recommended approach involves being especially careful what actually goes in print.
When information about the client is not directly relevant to what is being discussed, then it is not to be shared. When information about the client can be changed without compromising what is being discussed, thus further shielding identity, changing it is a good plan. If what I am writing does end up on the front page of
of supervision groups shall not be kept.
A record can certainly be kept of resources which have been discussed, of general approaches to issues which have been found effective, and so forth. The record which should not be kept is the one which in any way references or might possibly identify a particular individual.
Publications and TestimonialsThis meets the request I received to help think through the supervision group plan, but it leaves an outstanding difficulty.
Those of us who theorise and write about counselling often refer to clients and our work with clients in our articles and books. An article or book is, to use my earlier comparison, equivalent to the front page of the local newspaper.
Does it follow that it is ethically wrong to refer to clients and to work with clients in articles and in books? If so, a lot of influential people are in a lot of trouble.Theorising and writing about counselling can be classed as research, and the Code of Ethical Conduct, Principle 1, items 23 and 24 tell us that we should: Respect the right of clients... and research participants… to safeguard their own dignity.
Obtain informed consent for all research activities that involve more than minimal risk of harm…
Publications can cause harm to those who are written about in them, and so both of these requirements apply to articles and books. In order to satisfy them—and perhaps to go a little beyond them—I recommend a two-pronged approach.
the newspaper—Dream on, Clive!—then I don’t want anybody other than my client knowing who I am writing about.
Of course, there are many counsellors with no desire to ever write an article or book involving their work. But suppose you are commissioning a new website, and you want some words from the “horse’s mouth.” In other words, you wish to use testimonials.
Not only are testimonials a kind of publication—and subject to everything above—the Standard for Promoting and Advertising Services tells us that:An RCC should never… Solicit testimonials, expressly or by implication, from clients or other persons who, because of their particular circumstances, may be vulnerable to undue influence.
What client, dealing with the kinds of issues clients come to clinical counselling with, is not vulnerable in this way?
Remember, a testimonial is worthless unless attributed, and attribution will be equivalent to a person stating on the front page of their local newspaper that they are in therapy with a given counsellor.
I recommend not using testimonials from clients. In an article or a book, a client’s identity can be carefully protected. In an advertisement, it cannot.
Conceptually SimpleWe can reach the same conclusion about what is ethically appropriate by once again invoking the 1st item of the 1st Principle of the Code of Ethical Conduct. It is contrary to demonstrating respect for the unique worth
Insights into Clinical Counselling - April 2014
In order to communicate effectively, build strong team bonds and solve problems, professional relationships have traditionally been established on a premise of logic, reason and emotional, distance explains Kristina Jackson, an EFT therapist working with organizations.1 The problem with this common business premise is that it contravenes research on effective employee engagement. Brain research
demonstrates that when human beings sense any kind of threat, including an emotional or relational threat, the brain responds on an emotional level long before it even registers a thought. The brain resorts to knee jerk (emotional) reactions in this split second and cognitive abilities are inhibited. This fact means that learning how to harness emotion productively, as well as understanding how to keep it from hijacking our interactions and our performance, is key to getting desired results in a work environment.
The principles of Emotionally Focused Therapy provide a roadmap that reveal and clarify underlying emotions embedded in our reactions in the workplace and provide choices on how to navigate those emotions and reactions effectively with others. This article breaks down the components of the EFT roadmap and transposes them to the workplace, providing a blue-print for optimal communication and maximum organizational productivity. Application of EFT to effective leader-ship is expanded upon in a companion article at www.vcfi.ca.
By Kristine Rea, MA, RCC, Contributing Writer
This article will apply Attachment Theory and EFT concepts to the workplace by describing:
1) The roadmap called the “Infinity Loop”2/ “The Crazy 8;”2) Interpersonal dynamics – How to communicate well ;3) Using the roadmap for emotion regulation – “Keeping calm to carry on;”
I will talk about the power of effective engagement in the workplace and its necessity to corporate productivity and I will illustrate using a case scenario.
So Why Does an Emotional Hijack Happen and how can EFT Help?
Jim Coen’s work with FMRI’s and the brain (functional MRI technology that measures brain activity) demonstrates that we are hardwired for connections. We evolved in clans and groups, and we perform best when we are well connected to “our group.”3 Connection with other people regulates emotion; it helps us keep calm. Disconnection, therefore, from our group creates anxiety and our brain reads that dis-connect as a threat. I argue that “our group” at work is no exception. Focusing solely on financial gain in an organization and not additionally paying attention to the wellbeing of people can lead to physical and psychological breakdown of your key asset.
“When the drive to achieve financial goals is not balanced by the bonding to people, there is a danger of many physical, psychological and social consequences that include psychosomatic stress, addiction, burnout and depression.”4
All of these factors produce anxiety and negatively impact our ability to perform at our best. When we feel too much stress we lose cognitive efficiency, impacting our ability to learn new things and produce new ideas.
18
In addition, when anxiety is too high, people become hesitant to share ideas, speak up and collaborate.5
George Kohlrieser describes this concept in his book Care to Dare. “When you play to win you provide a high focus on relationships as well as a high level of challenge so that both you and your followers can reach the highest levels of performance. You are there to cover others’ backs and, at the same time, you challenge your followers with tough feedback and high expectations. Since they feel both safe and challenged, they will feel free to explore, be creative and take the risks inherent in innovation.”6 EFT addresses these issues by showing us how to diffuse emotion that overwhelms us and how to connect and communicate with others in a way that promotes collaboration and productivity.
How EFT Can Help Us:
The EFT roadmap depicts communication between two people as being like an infinity loop: What you say and how you say it evokes a reaction in me and vice versa, creating a self-perpetuating feedback loop.
For example, the more I criticize or attack you, the more likely you are to shut down and withdraw. The more you withdraw, the more I will probably get upset that you won’t engage my complaint. This, in turn, is likely to lead to me becoming more critical and attacking, and to you, in turn, withdrawing even more. When this behaviour occurs it creates an emotional loop that in EFT we call the infinity loop, and that in the work setting, I call the “Crazy 8.” This loop can also occur with both parties withdrawing and/or both attacking, either scenario of which creates tension. As we saw from the research, this anxiety-producing tension results in reduced sharing of ideas, a thwarting of the creative process,
From the Bedroom to the Boardroom: How the Principles of Emotionally Focused Therapy (EFT) Provide a Roadmap
to Productively Navigate Emotions in the Business Environment
the brain responds on an emotional level long before it even registers a thought
Insights into Clinical Counselling - April 2014
19
The reaction we have to the other person’s behavior is called the reactive emotion.
These top three elements happen faster than we can register thoughts and are based on our brain’s very rapid assessment of what the other person is doing and why (assessment of our immediate threat.)
limitations in cognitive flexibility and ultimately, an overall decline in problem solving abilities and productivity.
The infinity loop Crazy 8 roadmap can reveal and decipher exactly what is going on in this communication pattern. Picture an infinity loop with a horizontal line through the middle of it. It can help to draw this on a piece of paper.
There are six elements to map for each person down either side of the infinity loop. The section above the horizontal line represents the visible elements in a person’s behavior: Behavior, Meaning/Perception; and Reactive Emotion, in that order from top to bottom. The three elements below the line represent what is happening internally that is generally not seen: Underlying Emotion; Relational Significance; and Needs.
The Infinity Loop (Crazy 8) Explained:
Above the line behavior refers to our behavior in awkward, tense, moments of conflict. Meaning refers to our perception: How I make sense of your behavior or what I assume it to mean.
Behaviour: Lashing out/cutting remarksPerception: Pam and team dislike him
Reactive Emotion: Anger
Underlying Emotion: Fear of not belongingRelational Significance: Doesn’t belong
Needs: Value affirmed
PERSON 1
• Behaviour• Meaning/Perception
• Reactive Emotion
• Underlying Emotion• Relational Significance
• Needs
PERSON 2
• Behaviour• Meaning/Perception• Reactive Emotion
• Underlying Emotion• Relational Significance• Needs
Behaviour: Avoiding MarkPerception: She is doing something wrongReactive Emotion: Intimidated, frustrated, embarrassed
Underlying Emotion: Fear of inadequacy wrongRelational Significance: She is doing something wrongNeeds: Intimidated, frustrated, embarrassed
PAMMARK
MAY BE VISIBLE:
THE INFINITY LOOP / CRAZY 8
MAY BE INVISIBLE:
MAY BE VISIBLE:
MAY BE INVISIBLE:
Below the line is a more painful underlying emotion.
A reactive emotion usually shows up first and helps protect and distract us from feeling the more vulnerable underlying emotion. Often the person themselves is not aware there is another emotion underneath the reactive emotion.
The relational significance feeding the underlying emotion is based on how the situation affects our connection to the other person.
Finally, driving this process is our needs. As human beings we all have needs for affiliation or belonging (connection). Emotion in its proper
function is a source of information that helps us tune into our needs and helps show us how to take care of ourselves and others in an optimal way. Properly functioning emotion, therefore, helps us function at our most productive.
In the workplace, a sense of fulfillment of these needs may include a sense of belonging to the team, a sense of belonging to something greater than oneself, and a need to be valued and affirmed for contribution, ideas and as a person. Once team members understand all six components of the infinity loop for each individual, they can more easily see how they are affecting each other and fueling the Crazy 8.
Case scenario:
Below, the Crazy 8 scenario is broken down with a case example.
Mark is a talented employee but he has a real rough edge; he constantly throws out barbs to everyone around him. Nobody wants to work with Mark so they usually avoid engaging him, and they definitely do not include him in any social activities. This is especially true with Pam who feels very insecure around Mark and avoids him at all cost. She takes his barbs very personally and feels inadequate around him. The more Mark lashes out in anger, the more Pam withdraws and avoids.
The tension between Mark and Pam affects the whole team and, as a whole, the team has become increasingly unproductive. Below is the breakdown of what is going on in the Crazy 8.
Page 30
Insights into Clinical Counselling - April 2014
20
By Terra Kowalyk, MA Candidate, Gabriela Ionita, MA, Ph.D. Candidate, Marilyn Fitzpatrick, MEd, Ph.D., Contributing Writers
How do we know when we are effective as psychotherapists? Do we wait for clients to tell us they are doing better? Do we use clinical judgment? Many professions have objective measures that evaluate success. For example, educators can point to the grades of students, physicians to symptom improvement, and courtroom lawyers to judicial decisions. Psychotherapists typically deal with ambiguous data
and have a proud tradition of developing and refining clinical judgment to assess progress.
In 2011, the Canadian Psychological Association (CPA) Task Force on
Evidence-Based Practice of Psychological Treatments underlined the continuing importance of clinical judgment to evidence-based practice (EBP), “practitioners are required to exercise their professional judgment when providing treatment”1 (p.11). However, the CPA’s definition of EBP also includes the idea of progress monitoring (PM) and feedback. The Task Force called for “the monitoring and evaluation of services provided to clients throughout treatment”1 (p. 7).
The developing emphasis on outcomes or progress monitoring (PM) can be traced to emerging evidence that clinical judgment is skewed toward what we want to see.2 As clinicians, it is normal to want all our clients to benefit. However, clinicians are not skilled at identifying