Embed Size (px)
Citation preview

Costs and Benefits of Antithrombotic Therapy in Atrial Fibrillation in England: An Economic Analysis based on GRASP-AF
Marion KerrInsight Health Economics for NHS Improving Quality
Improving QualityNHS

Improving QualityNHS
Acknowledgem
ents
2
We would like to acknowledge PRIMIS who helpeddevelop the GRASP-AF tool in partnership with NHSIQ and who freely provided the software tools to runGRASP-AF and upload data. We would also like toacknowledge the practices that have voluntarilyuploaded data to the CHART Online database, withoutwhom this report would not have been possible.
“
“
Executive Summary
1. We estimate that more than 900,000 people in England (1.74% of the population) have atrial fibrillation (AF). AF is associated with increased risk of stroke and heart failure, and with premature mortality, independent of other known risk factors.
2. We use an extract from the GRASP-AF dataset, covering 13% of the population of England, to estimateEngland-level prevalence and prescribing patterns. Based on GRASP-AF and evidence from clinical studies,we develop a Markov model to estimate the long-term impact of antithrombotic prescribing in AF onstroke and major bleed incidence, mortality, quality-adjusted life years (QALYs), and National HealthService (NHS) and social care costs.
3. We estimate that around 16,100 strokes a year, including 4,400 fatal strokes, are averted in peoplewith AF who are taking warfarin (or warfarin plus aspirin). Fatal strokes are defined as those in which thepatient dies within 30 days. However, disabling strokes also increase the risk of death over the longerterm. Owing to the reduction in disabling strokes associated with warfarin, further deaths are averted.Total deaths in people with AF who are taking warfarin (or warfarin plus aspirin) are reduced by anestimated 4,800 over a one-year perspective. However, while these medications reduce stroke risk andmortality, they do increase the risk of bleeding. We estimate that there are 2,800 excess major bleeds ayear in people with AF who are taking warfarin or warfarin plus aspirin.
4. Recent National Institute for Health and Care Excellence (NICE) guidelines recommend that theCHA2DS2-VASc algorithm should be used to assess stroke risk in people with AF, and that anticoagulantsshould be offered to those with a CHA2DS2-VASc score of 2 or more, taking bleeding risk into account.However, in our dataset only around half of those who meet the prescribing criteria (53.60%) are takinganticoagulants. For 8.74%, it is recorded that anticoagulants are contraindicated or declined. It is likelytherefore that there are substantial numbers of people with AF who would benefit from anticoagulationtherapy but are not receiving it.
5. Our model suggests that if warfarin were prescribed for all those in England with a CHA2DS2-VAScscore of 2 or more (apart from those for whom the record states that anticoagulants are contraindicatedor declined) a further 11,600 AF-related strokes, including 3,200 fatal strokes, would be averted eachyear. There would be an additional 1,500 excess bleeds, and the total number of deaths in people withAF, over a one-year perspective, would be reduced by 3,500.
6. Our analysis suggests that warfarin prescribing for people with AF is associated with an overall reduction in the NHS cost of AF-related care, as savings from averted strokes exceed the combined cost oftreatment and associated major bleeds. We estimate that, over a lifetime, 0.30 strokes are averted, 0.79QALYs are gained and net savings of more that £2,400 are generated for the NHS per person with AFtreated with warfarin. We estimate that if everyone in England with a CHA2DS2-VASc score of 2 or more(apart from those for whom the record states that anticoagulants are contraindicated or declined) receivedwarfarin, the NHS would save approximately £124 million a year, relative to current patterns of care. Thereare further estimated savings to social care.
7. While the focus in this paper is on NHS and social care costs, strokes associated with AF will also entailcosts for individuals and their carers, and for society through losses in employment and productivity, andtax and benefit effects. If these effects were considered, it is likely that the overall savings from avertedstrokes would be higher than those estimated here.
Improving QualityNHS
Executive Summ
ary
3

Introduction
1. The prevalence of atrial fibrillation (AF) has been estimated at 1-2% of the population in the developedworld.1,2,3,4 AF is associated with increased risk of stroke and heart failure, and with premature mortality,independent of other known risk factors.5,6
2. Current management of AF is focused on rate/rhythm control and reduction of stroke risk, primarilythrough anticoagulation therapy. In the English NHS the Quality and Outcomes Framework (QOF) has,since 2006-07, provided financial incentives to general practitioners for the formation of AF registers, andfor treatment of the condition with anticoagulation or antiplatelet therapy. The QOF data for 2012-13indicate that 849,407 people in England had diagnosed AF, a population prevalence of 1.5%.
3. The National Institute for Health and Care Excellence (NICE) has recently issued guidelines recommending that the CHA2DS2-VASc algorithm should be used to assess stroke risk in people with AF, and that anticoagulants should be offered to those with a CHA2DS2-VASc score of 2 or more, takingbleeding risk into account.7 Anticoagulation should also be considered for men with a CHA2DS2-VAScscore of 1, again taking bleeding risk into account. The guidelines recommend that aspirin monotherapyshould not be offered solely for stroke prevention to people with atrial fibrillation.
4. The CHA2DS2-VASc algorithm is a point system in which 2 points are assigned for a history of stroke ortransient ischaemic attack (TIA), or age ≥75; and 1 point each is assigned for age 65–74 years, a history ofhypertension, diabetes, recent cardiac failure, vascular disease and female sex.
5. In this paper we examine antithrombotic prescribing patterns for people with AF in England, based ondata from 1,016 GP practices uploaded to the Guidance on Risk Assessment and Stroke Prevention forAtrial Fibrillation (GRASP-AF) dataset in 2011 and 2012. We estimate the impact of warfarin, and warfarinplus aspirin prescribing on stroke incidence and on NHS and social care costs, and the potential impact ofprescribing warfarin to all those with a CHA2DS2-VASc score of 2 or more. In a supplementary appendixwe also provide illustrative analysis of the impact on stroke incidence and costs of aspirin monotherapy.
Methods
1. Details of AF status and care were obtained from GRASP-AF for 1,016 GP practices in England. Together, these practices provide primary care to 7.1 million people, approximately 13% of the population of England. Data were uploaded to GRASP-AF between November 2011 and July 2012.
2. The GRASP-AF dataset provides pseudonymised patient-level data on AF status, age, gender,CHA2DS2-VASc score, prior stroke status and antithrombotic prescribing for GP practices that choose toparticipate.
3. The age distribution of patients in practices included in the data extract was compared with that reported for the population of England in Office for National Statistics (ONS) mid-year data for 2012.8
AF prevalence estimates from the GRASP-AF dataset were applied to the ONS population of England by 5-year age-band. The resulting AF prevalence estimates for England were compared with the prevalencerecorded in QOF for 2012-13.
4. The distribution of patients with AF in England in 2012-13 by CHA2DS2-VASc score and prior strokestatus was estimated by applying the GRASP-AF proportions to the 2012-13 AF prevalence estimates forEngland. The volumes of anticoagulant and antiplatelet prescribing were estimated by applying theGRASP-AF proportions by CHA2DS2-VASc score and prior stroke status.
Improving QualityNHS
Introduction | Methods
4
5. A Markov model was built to estimate the impact of warfarin monotherapy, and warfarin plus aspirincombination therapy on stroke incidence, mortality, QALYs and NHS and social care costs. The model wasalso used to estimate the impacts of aspirin monotherapy. However, there is uncertainty regarding theefficacy of aspirin in reducing stroke risk in AF. In a recent meta-analysis, the estimate for the impact ofaspirin did not reach statistical significance at the 95% level.9 For this reason, the results of the aspirinmonotherapy analysis are provided in a supplementary appendix to this paper. Care should be taken ininterpreting the aspirin results owing to the uncertainty surrounding the meta-analysis estimate.
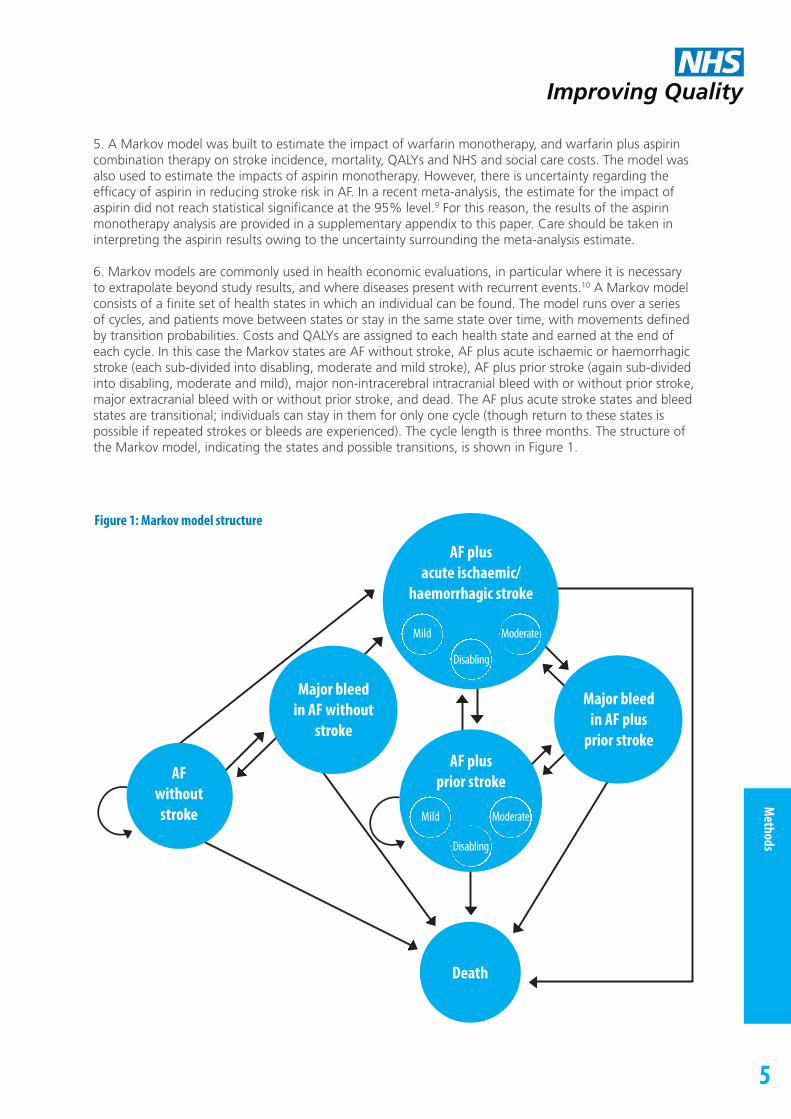
6. Markov models are commonly used in health economic evaluations, in particular where it is necessaryto extrapolate beyond study results, and where diseases present with recurrent events.10 A Markov modelconsists of a finite set of health states in which an individual can be found. The model runs over a seriesof cycles, and patients move between states or stay in the same state over time, with movements definedby transition probabilities. Costs and QALYs are assigned to each health state and earned at the end ofeach cycle. In this case the Markov states are AF without stroke, AF plus acute ischaemic or haemorrhagicstroke (each sub-divided into disabling, moderate and mild stroke), AF plus prior stroke (again sub-dividedinto disabling, moderate and mild), major non-intracerebral intracranial bleed with or without prior stroke,major extracranial bleed with or without prior stroke, and dead. The AF plus acute stroke states and bleedstates are transitional; individuals can stay in them for only one cycle (though return to these states ispossible if repeated strokes or bleeds are experienced). The cycle length is three months. The structure ofthe Markov model, indicating the states and possible transitions, is shown in Figure 1.
Improving QualityNHS
Methods
5
Figure 1: Markov model structure
Death
AF plusprior stroke
Major bleedin AF plus
prior stroke
Major bleedin AF without
stroke
AF plusacute ischaemic/
haemorrhagic stroke
Mild Moderate
Disabling
Mild Moderate
Disabling
AF withoutstroke

7. In cost effectiveness analysis it is customary to express costs and effects over the lifetime of a representative patient. Indeed, for the estimation of QALY effects it is necessary to take such a long-termperspective. However, decision-makers often wish also to understand costs over shorter timescales. In thispaper we therefore present long-run (“lifetime”) cost and QALY impacts, and also one-year cost impacts.The representative patient is taken to be 78 years old at model outset, based on the median age inGRASP-AF.
8. The baseline risk of ischaemic stroke without antithrombotic treatment was estimated by CHA2DS2-VASc score for the GRASP-AF population, using risks estimated in a recent Swedish study.11
9. There are a number of challenges in estimating the baseline risk of major bleeds, and the effect of treatment on this risk. Published estimates of major bleed rates in patients taking oral vitamin K antagonists such as warfarin range from 1.3 to 7.2% a year.12 These differences may reflect variation in anumber of factors, including study populations, stability of international normalised ratio (INR) values,methodology, definition and classification. Relatively few studies have examined bleed rates in patientswho are not receiving antithrombotics. Some studies have included intracerebral haemorrhage withstroke, rather than with bleeds, some have included all intracranial bleeds with stroke, while others haveclassified all intracranial bleeds as major bleeds rather than strokes. In their 2007 meta-analysis, Hart et al.did not estimate the impact of warfarin or aspirin versus placebo or control on the relative or absolute riskof intracranial bleeds, owing to the large proportion of empty cells in individual trial data.9
10. However, in spite of these difficulties we felt it was important to try to model intracerebral haemorrhages (taken to be equivalent to haemorrhagic strokes) discretely; while such haemorrhages arefar less frequent than ischaemic strokes, mortality rates are very high (more than 50% in manystudies).13,14 We estimated the rate of all intracranial bleeds in patients with AF on warfarin at 0.73% peryear, based on a weighted average from 16 randomised trials summarized by Lip et al.12 Most of thesestudies did not distinguish between intracerebral and other intracranial bleeds. The RE-LY trial (which wasincluded in the 16) reported that 46% of intracranial bleeds were intracerebral. (The rate of intracranialbleeds in this trial was 0.76%).14 Applying this proportion to the overall estimate derived from the 16trials, we estimate the rate of intracerebral haemorrhage in warfarin at 0.34%, and the rate of otherintracranial haemorrhage at 0.39%.
11. Of the 16 studies summarized by Lip at al., one provided an estimate of the rate of intracranial bleedin the absence of warfarin.15 This study estimated a crude rate ratio of 1.96 (95% CI 1.25-3.03) for intracranial bleed in those taking warfarin, relative to the non-warfarin group. It should be noted thatsome of the non-warfarin group were taking aspirin. The study did not provide discrete data for the aspirin and non-antithrombotic sub-groups. A US study of 13,559 people with AF reported that the risk ofintracerebral haemorrhage was 1.81 times higher in patients on warfarin than in those who were not onwarfarin.16 Applying these proportions to the estimates of bleed rates in warfarin set out in paragraph 10,we estimate the baseline risk of all intracranial bleeds without warfarin at 0.37%, and the baseline risk ofintracerebral bleed at 0.19%.
12. No studies were identified which provided discrete intracerebral haemorrhage risk estimates byCHA2DS2-VASc score or prior stroke status, though some studies have suggested that the absolute increase in risk for intracranial haemorrhage due to warfarin therapy remains fairly stable across thromboembolic risk categories.16 GRASP-AF does not classify patients using HAS-BLED or other bleed risk measures.
13. Hart et al. estimated in their meta-analysis that warfarin was associated with an absolute increase inthe risk of major extracranial bleeds of 0.3% per year, relative to control or placebo, and this figure wasused in the model.9
14. The impact of warfarin on the combined endpoint of stroke and intracranial bleed risk was estimatedby Hart et al. in their 2007 meta-analysis findings at minus 64%.9 Adjusting that figure for the increase inrisk of intracranial bleeds, we estimate the reduction in ischaemic stroke risk to be 66.88% for patientswith prior stroke and 69.70% for those without prior stroke.
Improving QualityNHS
Methods
6

15. We have assumed that ischaemic stroke reduction in the case of treatment with both warfarin and antiplatelets is the same as for warfarin alone. The hazard ratio for major bleeds in combined therapy relative to warfarin monotherapy is taken to be 1.53.18 It should be noted that this approach mayunderestimate the risk of intracranial haemorrhage when both warfarin and aspirin are taken. Somestudies have suggested that the relative risk of intracranial haemorrhage in warfarin and aspirincombination therapy, relative to warfarin monotherapy, may be up to 2.4.19
16. We followed the practice of Ali et al. in defining minor bleeds as those that do not require medical intervention.20 We did not model any cost or outcome impacts for these events.
17. Thirty-day ischaemic stroke mortality rates in AF for those without antithrombotic therapy, for patientson warfarin, and for those on aspirin were estimated from a US study.21 Thirty-day mortality rates afterhaemorrhagic stroke and other intracranial bleeds were taken from the RE-LY trial.14 Hazard ratios forsubsequent death after non-fatal ischaemic stroke, haemorrhagic stroke and other major bleeds weretaken from the Atrial Fibrillation Clopidogrel Trial with Irbesartan for Prevention of Vascular Events (ACTIVE)-W Trial.22 Mortality risk in AF in the absence of stroke or major bleed, was estimated from ONSLife Tables by gender and year of age. The overall mortality rates predicted in the model for people onwarfarin were validated by comparing with meta-analysis findings on the absolute reduction in all-deathrisk.9
18. The NHS costs of the first 90 days of care for mild, moderate, disabling and fatal strokes were estimated from a recent UK study on stroke in AF.23 The impact of stroke in AF on social care costs formild, moderate, and disabling strokes was estimated from the same report. The study also providedestimates of the difference between ongoing post-stroke (after 90 days) and pre-stroke NHS costs.However, these estimates were not statistically significant at the 95% level. We therefore excluded themfrom our base-case analysis, but have included them in sensitivity analysis.
19. The proportion of disabling strokes in AF, by treatment modality, was taken from Hart et al.9 Of theremainder, the distribution of moderate and mild strokes in patients with AF was taken from the US Framingham study.24
20. The mean costs of major extracranial bleeds and non-intracerebral intracranial bleeds were estimatedfrom NHS Reference Costs.25 The weighted mean cost of admission episodes grouped to HRGs FZ38G-P,Gastrointestinal Bleed (£1,092) was used to estimate the cost of extracranial bleeds. The weighted meancost of admission episodes grouped to HRGs AA23C-G, Haemorrhagic Cerebrovascular Disorders (£2,589)was used to estimate the cost of non-intracerebral intracranial bleeds. (While these HRGs are labeled ascerebrovascular, ICD 10 codes I60 and I62.0, covering subarachnoid and subdural haemorrhages respectively, are also grouped to these HRGs).
21. The costs of medications were taken from the British National Formulary (BNF).26 The mean daily doseof warfarin was assumed to be 4mg.27 Warfarin tablets are available in 0.5mg, 1 mg, 3mg, and 5mgdoses. The cost of the medication varies substantially, depending on the combination of tablets used toadminister a given dose, as shown in Table 1.
Table 1: Annual cost of warfarin medication, by dose and tablet combination Source: BNF 6426
Improving QualityNHS
Methods
7
Dose and cost Tablet combination
4mg daily dose 8 x 0.5mg 4 x 1mg 1 x 1mg + 1 x 3mg 2 x 0.5mg + 1 x 3mg
Annual cost £174.16 £44.84 £22.42 £54.75
6mg daily dose 12 x 0.5mg 2 x 3mg 1 x1mg + 1 x 5mg 2 x 0.5mg + 1 x 5mg
Annual cost £261.24 £22.42 £23.20 £55.53

22. It is assumed here that 4mg is provided as 1 x 3mg tablet plus 2 x 0.5mg tablets, to allow for doseadjustment. We have also set out the cost of a 6mg dose, for a variety of tablet combinations (Table 1). If6mg is delivered as 1 x 5mg and 2 x 0.5mg tablets, the cost is similar to that for 4mg delivered as 1 x 3mgtablet plus 2 x 0.5mg tablets (£55.53, as compared with £54.75). We did not therefore explore in themodel separate costs for provision of a 6mg daily dose. The mean daily aspirin dosage was taken to be75mg, and the annual cost was estimated at £6.19.
23. The annual cost of warfarin management, including anticoagulation testing for dose adjustment, hasbeen estimated in studies at £73.99-£115.60 (after conversion to 2012-13 prices).20,28 The mean value(£94.80) was used in our base case analysis. It is reported, however, that there is considerable variation inthe cost of warfarin management. In sensitivity analysis we therefore used a range of values for warfarinmonitoring, as recommended in a recent NICE guideline.29
24. Quality of life in patients with atrial fibrillation and in those who have had strokes was estimatedusing the EQ-5D standardised measure of health status. Measures were drawn from studies that usedweights derived from UK population preferences.30,31,32
25. Cost and QALY impacts were estimated for current prescribing patterns for patients withCHA2DS2-VASc score ≥2, based on GRASP-AF data. Cost and QALY impacts were also modelled forprescribing of warfarin for all those with CHA2DS2-VASc score ≥2 for whom anticoagulants are notcontra-indicated or declined.
26. All costs are expressed in 2012-13 prices. Where necessary, costs were updated using the Hospital andCommunity Health Services Pay and Prices index. Future costs and QALYs are discounted at 3.5% a year.
27. A summary of parameters used in the Markov model is provided in Appendix 1, Tables A1.1 and A1.2.
Improving QualityNHS
Methods
8

Improving QualityNHS
Results
9
8%
7%
6%
5%
4%
3%
2%
1%
0%
0 - 4
Perc
enta
ge of
pop
ulat
ion
5 - 9
10 -1
4
15 -1
9
20 -2
4
25 -2
9
30 -3
4
35 -3
9
40 -4
4
45 -4
9
50 -5
4
55 -5
9
80 -8
4
85 -8
9
90 +
60 -6
4
65 -6
9
70 -7
4
75 -7
9
Age
GRASP-AF
ONS
Results
Prevalence and prescribing
1. The GRASP-AF dataset recorded 128,293 people with AF in participating practices, a prevalence of1.81%. The age distribution of patients in these practices is broadly similar to that reported for England inONS, although a somewhat larger proportion of the GRASP-AF population than the ONS population isaged 65+ (17.56%, as compared with 16.44% in ONS (Figure 2)).
Figure 2: Age distribution by quinary age-band, GRASP-AF, and ONS 2012
2. The prevalence of AF in GRASP-AF ranges from 0.01% in those aged 0-29 years to 15.06% in thoseaged ≥ 80 years.
3. Adjusting for the difference in age distribution, the prevalence of AF in England based on GRASP-AF isestimated at 1.74% in 2012 (929,856 people), as compared with 1.52 % (849,407 people) recorded inQOF in 2012-13. QOF data exclude patients who are considered to have “AF resolved”. If this group wereremoved from GRASP-AF the estimated age-adjusted prevalence for England would be 1.51%. Patientswith “AF resolved” are included in the analyses reported in this paper.
4. Of AF patients in GRASP-AF, 18.14% had a prior stroke, a further 66.00% had a CHA2DS2-VASc score≥ 2 without prior stroke, 7.64% were men with CHA2DS2-VASc score = 1, 2.40% were women withCHA2DS2-VASc score = 1, and 5.81% had CHA2DS2-VASc score = 0.
5. Of those with CHA2DS2-VASc score ≥2, 53.60% were prescribed anticoagulants. For 8.74%, the recordstated that anticoagulants were contra-indicated or had been declined (Table 2). Of those in this groupreceiving anticoagulants, 99.00% were receiving warfarin.

Table 2: Prescribing of anticoagulants for AF patients in GRASP-AF
6. Anticoagulant and antiplatelet combination therapy was prescribed for 7.78% of those withCHA2DS2-VASc score ≥ 2, and a further 35.63% were on antiplatelet monotherapy. No antithromboticswere prescribed for 10.76% of the group (Table 3).
Table 3: Prescribing of anticoagulants and antiplatelets, GRASP-AF
7. If it is assumed that the prevalence of AF and the distribution of CHA2DS2-VASc scores in England is thesame as the age-adjusted estimates from GRASP-AF, it is estimated that there were 783,592 people inEngland in 2012-13 with diagnosed AF and a CHA2DS2-VASc score ≥ 2, and 71,519 men with aCHA2DS2-VASc score = 1.
CHA2DS2-VASc ≥ 2 Men with CHA2DS2-VASc = 1
Patients 107,949 9,810
Anticoagulants Warfarin 53.07% 42.33%
Acenocoumarol 0.32% 0.24%
Dabigatran etexilate 0.12% 0.19%
Phenindione 0.09% 0.06%
Rivaroxaban 0.00% 0.01%
Apixaban 0.00% 0.00%
Anticoagulants contra-indicated 5.44% 2.13%
Anticoagulants declined 3.30% 1.81%
No anticoagulants and anticoagulants not contra-indicated or declined
37.66% 53.21%
CHA2DS2-VASc ≥ 2 Men with CHA2DS2-VASc = 1
Anticoagulant only 45.82% 36.80%
Anticoagulant and antiplatelet 7.78% 6.04%
Antiplatelet only 35.63% 36.22%
Neither anticoagulant nor antiplatelet 10.76% 20.94%
Improving QualityNHS
Results
10

Estimated baseline stroke risk
8. Stroke risk in the absence of antithrombotic therapy was estimated by applying stroke risks for eachCHA2DS2-VASc score (2-9) observed in a recent Swedish study11 to the GRASP-AF population, as shown inTable 4.
Table 4: Stroke risk by CHA2DS2-VASc score (Source: Friberg et al.11), and distribution of patients in GRASP-AF with andwithout prior stroke
9. Given the distribution of patients by CHA2DS2-VASc score in GRASP-AF, we estimate the overall annual ischaemic stroke risk for the population with CHA2DS2-VASc score ≥ 2 at 4.75% for primary strokeand 9.38% for secondary stroke, in the absence of antithrombotic therapy. This compares withmeta-analysis findings for the general AF population (not differentiated by CHA2DS2-VASc score) of 4.1% for primary stroke and 13% for secondary stroke, again in the absence of antithrombotic therapy.9
It should be noted, however, that the meta-analysis includes haemorrhagic strokes, whereas the Swedishstudy does not.
10. If it is assumed that the prevalence of AF and the distribution of CHA2DS2-VASc scores in England isthe same as the age-adjusted estimates from GRASP-AF, the Markov model estimates that, without anyantithrombotic therapy, there would have been 45,608 strokes (ischaemic and haemorrhagic) in peoplewith AF with CHA2DS2-VASc score ≥ 2 in England in 2012-13, equivalent to 5.8 for every 100 patients.
Stroke, QALY and cost impacts per person treated, by treatment modality
11. It is customary in health economic analysis to estimate cost and benefit impacts relative to the nextbest treatment option. In the case of warfarin in AF, there is uncertainty as to whether the next best option is no treatment or treatment with aspirin. As indicated above, the meta-analysis estimate of theimpact of aspirin on stroke risk did not reach statistical significance at the 95% level.9 Recent EuropeanSociety of Cardiology (ESC) guidelines state that “The evidence for effective stroke prevention with aspirin in AF is weak, with a potential for harm”.4 As indicated above, NICE has recommended that aspirin monotherapy should not be offered solely for stroke prevention to people with atrial fibrillation.7
Improving QualityNHS
Results
11
Distribution of people with AF in GRASP-AF (% of those with CHA2DS2-VASc score ≥ 2)
CHA2DS2-VASc score Prior stroke No prior stroke Stroke risk (Friberg et al.)
2 374 (0.35%) 20,051 (18.57%) 2.5
3 1,264 (1.17%) 27,191 (25.19%) 3.7
4 3,550 (3.29% 24,765 (22.95%) 5.5
5 6,578 (6.09%) 10,008 (9.27%) 8.4
6 7,357 (6.82%) 2,371 (2.20%) 11.4
7 3,206 (2.97%) 286 (0.26%) 13.1
8 829 (0.77%) 0 (0.00%) 12.6
9 119 (0.11%) 0 (0.00%) 14.4

12. In view of this uncertainty, and the NICE recommendation that aspirin monotherapy should not be offered for stroke prevention in AF, we have taken no treatment as the next best option in this paper. Inthe Appendix we provide illustrative figures for the potential impact of aspirin on stroke. It should benoted, however, that these estimates are based on the (non-significant) estimates from meta-analysis. We cannot be confident, at the 95% level, that aspirin reduces the risk of stroke in AF.
13. The Markov model estimates that, over a lifetime perspective, 0.30 strokes (combined ischaemic and haemorrhagic) are averted and 0.79 QALYs gained per person treated with warfarin, relative to noantithrombotic treatment. Of averted strokes, more than a quarter (0.08 per person treated) are fatalstrokes. There are 0.05 excess bleeds (extracranial and non-intracerebral intracranial). NHS and social carecosts related to AF are reduced over both a one-year and lifetime perspective, owing to reduced stroke incidence (Table 5). More details of the NHS cost impact are shown in Table 6.
Table 5: Estimated one-year and lifetime stroke, major bleed, QALY and cost impacts per person treated with warfarinmonotherapy, relative to no antithrombotic therapy
Table 6: Estimated one-year and lifetime NHS cost impacts of treatment, major bleeds and averted strokes per persontreated with warfarin monotherapy, relative to no antithrombotic therapy
14. Fatal strokes are defined as those in which the patient dies within 30 days. However, disabling strokesalso increase the risk of death over the longer term. Owing to the reduction in disabling strokes associatedwith warfarin, further deaths are averted. The model estimates that absolute all-cause one-year mortalityis 1.17% lower with warfarin than with no treatment. This estimate may be compared with meta-analysisfindings that warfarin is associated with a 1.6% reduction in all-cause annual mortality.9
15. For those treated with warfarin and aspirin combination therapy, stroke reduction is lower than forthose on warfarin monotherapy, owing to the increased risk of haemorrhagic stroke. The rate of othermajor bleeds is also higher, and NHS net savings are lower than on warfarin monotherapy (Table 7). Moredetails of the NHS cost impact are shown in Table 8.
Improving QualityNHS
Results
12
Strokes Bleeds QALYs NHS costs Social care costs
One-year impact -0.039 0.006 0.007 -£412 -£94
Lifetime impact -0.298 0.048 0.794 -£2,408 -£1,379
Treatment cost Excess major bleeds Averted strokes
One-year impact £139 £8 -£559
Lifetime impact £1,129 £66 -£3,603

Table 7: Estimated one-year and lifetime stroke, major bleed, QALY and cost impacts per person treated with warfarinand aspirin combination therapy, relative to no antithrombotic therapy
Table 8: Estimated one-year and lifetime NHS cost impacts of treatment, major bleeds and averted strokes per persontreated with warfarin and aspirin combination therapy, relative to no antithrombotic therapy
Estimated clinical and cost impacts of GRASP-AF prescribing patterns
16. If it is assumed that the prevalence of AF and the distribution of CHA2DS2-VASc scores in England arethe same as the age-adjusted estimates from GRASP-AF, and prescribing patterns are also as in GRASP-AF,it is estimated that 415,834 people with CHA2DS2-VASc score ≥ 2 were on warfarin in 2012-13. Of thisnumber, it is estimated that 356,086 were on warfarin monotherapy, and 59,748 were taking bothwarfarin and aspirin. For a monotherapy group of this size, it is estimated that 13,906 strokes, including3,801 fatal strokes, would be averted through warfarin in a year, and 106,231 strokes, including 29,449fatal strokes, over a lifetime perspective. It is estimated that the number of deaths from all causes wouldbe reduced by 4,185 over a one-year perspective. The model predicts that there would be an additional2,183 non-intracerebral bleeds in a year and 16,935 over a lifetime. Annual net savings to the NHS fromaverted strokes are estimated at £147 million over one year, and £858 million over a lifetime perspective.There are additional estimated savings to social care (Table 9). More details of the NHS cost impact areshown in Table 10. Impacts for the warfarin and aspirin combination therapy cohort are shown in Tables11 and 12.
Table 9: Estimated one-year and lifetime stroke, major bleed, QALY and cost impacts for a cohort of 356,086 peopletreated with warfarin monotherapy, relative to no antithrombotic therapy
Improving QualityNHS
Results
13
Strokes Bleeds QALYs NHS costs Social care costs
One-year impact -0.037 0.011 0.006 -£379 -£92
Lifetime impact -0.284 0.081 0.754 -£2,181 -£1,305
Treatment cost Excess major bleeds Averted strokes
One-year impact £145 £12 -£536
Lifetime impact £1,167 £100 -£3,448
Strokes Bleeds QALYs NHS costs Social care costs
One-year impact -13,906 2,183 2,330 -£146,747,063 -£33,450,628
Lifetime impact -106,231 16,935 282,892 -£857,627,384 -£490,997,377
Improving QualityNHS
Results
14
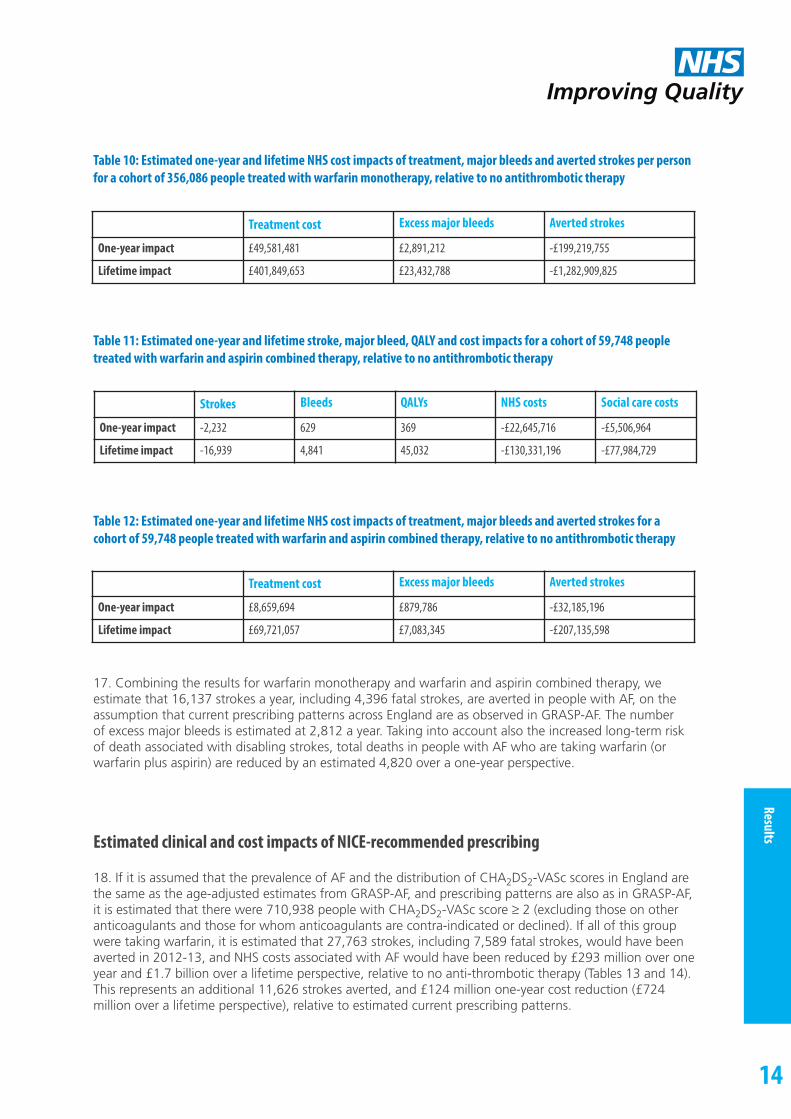
Table 10: Estimated one-year and lifetime NHS cost impacts of treatment, major bleeds and averted strokes per personfor a cohort of 356,086 people treated with warfarin monotherapy, relative to no antithrombotic therapy
Table 11: Estimated one-year and lifetime stroke, major bleed, QALY and cost impacts for a cohort of 59,748 peopletreated with warfarin and aspirin combined therapy, relative to no antithrombotic therapy
Table 12: Estimated one-year and lifetime NHS cost impacts of treatment, major bleeds and averted strokes for a cohort of 59,748 people treated with warfarin and aspirin combined therapy, relative to no antithrombotic therapy
17. Combining the results for warfarin monotherapy and warfarin and aspirin combined therapy, we estimate that 16,137 strokes a year, including 4,396 fatal strokes, are averted in people with AF, on theassumption that current prescribing patterns across England are as observed in GRASP-AF. The number of excess major bleeds is estimated at 2,812 a year. Taking into account also the increased long-term riskof death associated with disabling strokes, total deaths in people with AF who are taking warfarin (orwarfarin plus aspirin) are reduced by an estimated 4,820 over a one-year perspective.
Estimated clinical and cost impacts of NICE-recommended prescribing
18. If it is assumed that the prevalence of AF and the distribution of CHA2DS2-VASc scores in England arethe same as the age-adjusted estimates from GRASP-AF, and prescribing patterns are also as in GRASP-AF,it is estimated that there were 710,938 people with CHA2DS2-VASc score ≥ 2 (excluding those on otheranticoagulants and those for whom anticoagulants are contra-indicated or declined). If all of this groupwere taking warfarin, it is estimated that 27,763 strokes, including 7,589 fatal strokes, would have beenaverted in 2012-13, and NHS costs associated with AF would have been reduced by £293 million over oneyear and £1.7 billion over a lifetime perspective, relative to no anti-thrombotic therapy (Tables 13 and 14).This represents an additional 11,626 strokes averted, and £124 million one-year cost reduction (£724 million over a lifetime perspective), relative to estimated current prescribing patterns.
Treatment cost Excess major bleeds Averted strokes
One-year impact £49,581,481 £2,891,212 -£199,219,755
Lifetime impact £401,849,653 £23,432,788 -£1,282,909,825
Strokes Bleeds QALYs NHS costs Social care costs
One-year impact -2,232 629 369 -£22,645,716 -£5,506,964
Lifetime impact -16,939 4,841 45,032 -£130,331,196 -£77,984,729
Treatment cost Excess major bleeds Averted strokes
One-year impact £8,659,694 £879,786 -£32,185,196
Lifetime impact £69,721,057 £7,083,345 -£207,135,598

Improving QualityNHS
Results
15
Table 13: Estimated one-year and lifetime stroke, major bleed, QALY and cost impacts for a cohort of 710,938 peopletreated with warfarin monotherapy, relative to no antithrombotic therapy
Table 14: Estimated one-year and lifetime NHS cost impacts of treatment, major bleeds and averted strokes per personfor a cohort of 710,938 people treated with warfarin monotherapy, relative to no antithrombotic therapy
Sensitivity analyses
19. It is known that the cost of INR management for people taking warfarin is subject to considerablelocal variation. The Evidence Review Group for a 2012 NICE technology appraisal proposed that three values for annual INR monitoring should be used in sensitivity analysis (£115.14, £241.54 and £279.36).29
In sensitivity analyses 1-3 we have used these values, updated to 2012-13 prices (£117.83 in sensitivityanalysis 1, £247.18 in sensitivity analysis 2, and £285.89 in sensitivity analysis 3).
20. In all three scenarios, the estimated net cost impact for the NHS is negative, meaning that estimatedsavings from averted strokes exceed the cost of AF- associated treatment and monitoring. However, netsavings are lower than in the base case (Tables 15 and 16). With the highest estimated level of INR monitoring costs, net annual savings to the NHS for care associated with AF are 43% lower than the base case estimate over a one-year perspective, and 58% lower over a lifetime. Net social care costs are unaffected.
Table 15: Sensitivity analyses 1-3: Estimated one-year and lifetime NHS cost impacts per person treated with warfarin monotherapy, relative to no antithrombotic therapy, with annual INR monitoring costs of £115.14, £241.54 and £279.36
Strokes Bleeds QALYs NHS costs Social care costs
One-year impact -27,763 4,359 4,651 -£292,985,574 -£66,785,332
Lifetime impact -212,095 33,811 564,803 -£1,712,282,662 -£980,293,204
Treatment cost Excess major bleeds Averted strokes
One-year impact £98,991,138 £5,772,404 -£397,749,115
Lifetime impact £802,306,697 £46,784,371 -£2,561,373,729
Net NHS cost impact
Base case Sensitivity 1 Sensitivity 2 Sensitivity 3
One-year impact -£412 -£391 £270 -£234
Lifetime impact -£2,408 -£2,241 -£1,297 -£1,015

Improving QualityNHS
Results
16
Table 16: Sensitivity analyses 1-3: Estimated one-year and lifetime NHS cost impacts for a cohort of 710,938 peopletreated with warfarin monotherapy, relative to no antithrombotic therapy, with annual INR monitoring costs of£115.14, £241.54 and £279.36 per person treated
21. Another key area of uncertainty is the marginal cost of ongoing NHS care for people with AF whohave experienced strokes. A recent study reported that the mean annual cost of post-stroke care washigher than that of pre-stroke care for all levels of stroke severity in people with AF.23 However, the differences were not significant at the 95% level. In the light of this uncertainty, we did not include ongoing NHS costs in our base case. In sensitivity analysis 4, we use the mean differences between pre- and post-stroke care annual costs from this study, updated to 2012-13 prices (£413 for mild stroke,£894 for moderate stroke, £3,270 for disabling stroke). Using these estimates of post-stroke costs, thesaving to the NHS for AF-associated care increases relative to base case by 26% over a one-year perspective, and 64% over a lifetime.
Table 17: Sensitivity analysis 4: Estimated one-year and lifetime NHS cost impacts for warfarin monotherapy, relativeto no antithrombotic therapy, including estimated post-stroke NHS costs
Net NHS cost impact
Base case Sensitivity 1 Sensitivity 2 Sensitivity 3
One-year impact -£292,985,574 -£277,741,418 -£192,121,293 -£166,498,138
Lifetime impact -£1,712,282,662 -£1,592,879,823 -£922,243,388 -£721,545,000
Per person treated For 356,086 people For 710,938 people
One-year impact -£519 -£184,678,126 -£368,716,250
Lifetime impact -£3,939 -£1,402,582,163 -£2,800,303,680

Improving QualityNHS
Discussion
17
Discussion
1. The estimates of AF-associated prescribing, expenditure and outcomes set out in this paper have been based on extrapolations from the GRASP-AF dataset, which provides details of AF status, age, gender, CHA2DS2-VASc score, prior stroke status and antithrombotic prescribing. The extract used for thisreport covered patients in more than a thousand GP practices. These practices together provide care toapproximately 13% of the population of England. England-level estimates of prevalence have been standardised to match the national age-distribution as recorded in ONS. GRASP-AF does not provide otherdemographic data such as ethnicity or deprivation, and it has therefore not been possible to standardisefor these variables.
2. Estimates of the impact of prescribing on stroke incidence, QALYs and costs are estimated by means ofa Markov model. The outputs of such a model are highly sensitive to the parameters used. For this reason we have aimed to set out details of parameters and sources transparently. These are summarised inthe Methods section, and further detail is provided in Appendix 1. We have also carried out sensitivityanalyses in areas where variable parameters are subject to particular uncertainty or variability.
3. Our analysis suggests that more than 900,000 people in England have AF (1.74%). Of this group,around 84% have a CHA2DS2-VASc score ≥ 2 (a population prevalence of 1.46%). We estimate that current levels of warfarin (or warfarin plus aspirin) treatment in this group are associated with preventionof around 16,100 strokes a year, including 4,400 fatal strokes.
4. The number of excess major bleeds associated with warfarin, or warfarin plus aspirin prescribing forthis group is estimated at around 2,800 a year. (This excludes intracerebral bleeds, which are included inthe stroke estimate). Taking into account also the increased risk of death associated with disabling strokein those who have survived to 30-days, total deaths in people with AF are reduced by an estimated 4,800over a one-year perspective. The absolute reduction in the one-year death rate for those on warfarinmonotherapy is estimated at 1.17%. The reduction in all-cause annual mortality associated with warfarinhas been estimated at 1.6% in meta-analysis.9 It is possible therefore that our model under-estimates thereduction in deaths associated with warfarin prescribing.
5.Over a lifetime perspective, our model estimates that 0.30 strokes are averted and 0.79 QALYs gainedper person treated with warfarin.
6. Recent NICE guidelines recommend that patients with a CHA2DS2-VASc score ≥ 2 should be offeredanticoagulation therapy. However, only just over half (53.60%) of people with a CHA2DS2-VASc score ≥ 2in our dataset are prescribed warfarin or other anticoagulants. For a further 8.74% of this group, it isrecorded that anticoagulants are contraindicated or declined. There may therefore be substantial numbersof people with AF who would benefit from anticoagulation therapy but are not receiving it. Our modelsuggests that if warfarin were prescribed for all those with a CHA2DS2-VASc score of ≥ 2, apart fromthose for whom it is contraindicated or declined, approximately 11,600 further AF-related strokes, including 3,200 fatal strokes, would be averted each year in England. There would be an additional 1,500excess bleeds, and the total number of deaths in people with AF, over a one-year perspective, would bereduced by a further 3,500.
7. Our analysis suggests that warfarin prescribing for people with AF is associated with a net reduction inthe cost to the NHS of AF-related care. This reduction arises because the saving through averted strokesexceeds the costs of treatment and of associated major bleeds. The one-year saving to the NHS from warfarin (or warfarin plus aspirin) prescribing at the levels shown in our dataset for those who have AF inEngland is estimated at £169 million, and the lifetime saving at £988 million. If warfarin were prescribedfor all those with a CHA2DS2-VASc score ≥ 2, apart from those for whom it is contraindicated or declined,the estimated saving to the NHS on AF-related care is £293 million over one year, and £1.7 billion over alifetime perspective. There are further estimated savings to social care.

Improving QualityNHS
Discussion
18
8. There is uncertainty regarding the efficacy of aspirin on stroke prevention in AF. Meta-analysis findingsreport a non-significant 19% reduction in stroke incidence (compared with a 64% reduction with warfarin).9 NICE has recommended that aspirin monotherapy should not be offered solely for stroke prevention to people with atrial fibrillation. In view of this recommendation, and the statistical uncertainty,we have presented analysis of aspirin in a separate appendix. Based on a 19% reduction in stroke incidence, we estimate that over a one-year perspective aspirin would be associated with a reduction instroke incidence of 0.015 per person treated, compared with 0.039 for warfarin. Estimated overall NHScosts rise with aspirin treatment, owing to an increase in the proportion of strokes that are haemorrhagic, an increase in other major bleeds, and an increase in the proportion of disabling strokes. In economic parlance, warfarin dominates aspirin as a therapy for stroke prevention in AF.
9. The recent NICE guideline also recommends that anticoagulants should be considered for men with aCHA2DS2-VASc score of 1. There is little evidence on baseline stroke risk in this group, or on the impact ofanticoagulation. We did not feel that the evidence base was sufficiently robust to support estimation ofcosts and benefits for this group. Further clinical studies are needed on the potential for stroke reductionthrough anticoagulation in this group.
10. New oral anticoagulants (dabigatran etexilate, rivaroxaban and apixaban) have recently been approvedby a number of international bodies, including NICE in England and Wales, for stroke prevention in sub-groups of the AF population. In both cases the product cost is considerably higher than that of warfarin. The manufacturers of these drugs state that there is no requirement for regular anticoagulationtesting for dose adjustment with these medications.
11. The GRASP-AF data extract used for our paper covered the period from November 2011 to July 2012,and the NICE recommendations on these new agents were published toward the end of this period. Notsurprisingly, therefore, use of these agents in the period covered by our study was very low (approximately0.22% of total anticoagulant use in people with CHA2DS2-VASc score ≥ 2). In this paper, therefore, wehave not modelled the cost or impacts of prescribing of the new oral anticoagulants. It is likely, however,that in the future there will be a need for further study on the impact of these agents on stroke risk in theAF population in England, and associated costs.
12. There is variation in the cost of warfarin monitoring, and these costs have a substantial impact onoverall net cost estimates. A recent NICE technology appraisal used three values for warfarin monitoring insensitivity analyses. The value used in our base case is drawn from study evidence, and is lower than thevalues used by NICE. We have used the NICE values in our sensitivity analyses. For all of these values, weestimate that warfarin is associated with a reduction in the NHS cost of AF-associated care.
13. Given the variation in the cost of such monitoring around the country, the overall cost impact of warfarin prescribing will also vary from place to place. There may be potential in places wherecosts are particularly high to provide monitoring services more efficiently, thus increasing the overall costeffectiveness of treatment.
14. There is also a need for further study on the cost of warfarin monitoring in people with AF. Since thecost effectiveness of medications is estimated with reference to the next best option, understanding thetrue cost of warfarin is important not only for assessment of the costs and savings of warfarin itself, but isalso an important factor in determining the cost effectiveness of alternative medications.
15. It is hoped that this paper will provide a foundation for local analysis and decision-making onantithrombotic prescribing in AF.

Improving QualityNHS
Appendix 1
19
Transitionprobabilities
No antithrombotics(baseline)
Warfarin Warfarin andaspirin
Aspirin (See Appendix)
Ischaemic stroke (annual)
Primary 4.75%, Secondary 9.38% (Estimated by applyingCHA2DS2-VASc risks (Friberg et al.11), toCHA2DS2-VASc distribution in GRASP-AF)
Primary 1.44%, Secondary 3.11% (Relative risk reduction:64% (Hart et al.9), adjusted for impact onhaemorrhagic stroke, applied to baseline risks estimated above.
As for warfarin Primary 3.81%, Secondary 7.53% (Risk reduction: 19% non significant (Hart et al.9)applied to baseline risksestimated above.
Haemorrhagic stroke(annual)
0.19% Estimated by applying ratio of intracerebral haemorrhagein warfarin and non-warfarin patients inSinger et al16. to estimatedrisk with warfarin shown in cell below.
0.34% Overall rate of intracranial bleeds estimated by takingweighted average from 16 studies cited in Lip et al12. (0.73%), proportion ofthese that are intracerebralestimated from Hart el al.14
(46%)
Hazard ratio 1.53, relative to warfarin alone (Steinberg et al.18)
0.19% - Overall rate of intracranial bleeds takenfrom Flaker et al.34 (0.41%),proportion that are intracerebral assumed as for warfarin
Other intracranial bleeds
0.18% Estimated by applying rate ratio for intracranial bleed in warfarin and non-warfarinpatients from Go et al.15 torisk of intracranial bleed inwarfarin estimated bytaking weighted averagefrom 16 studies cited by Lipet al.12, and subtractingestimated haemorrhagicstroke risk for non-warfarinpatients
0.39% Overall rate of intracranial bleeds estimated by takingweighted average from 16 studies cited in Lip et al12 (0.73%), proportion ofthese that are not intracerebral estimatedfrom Hart et al.14
(54%)
Hazard ratio 1.53, relative to warfarin alone (Steinberg et al.18)
0.22% - Overall rate of intracranial bleeds takenfrom Flaker et al.34 (0.41%),proportion that are not intracranial assumed as for warfarin
Stroke severity forstrokes survived beyond 30 days (Combined ischaemicand haemorrhagic)
60% disabling (Hart et al.9), of remainder moderate:mild ratio = 1:2.95 (Lin et al.24)
60% disabling (Hart et al.9),of remaindermoderate:mild ratio =1:2.95 (Lin et al.24)
Assumed as for warfarin 65% disabling: (13% reduction in disablingstrokes, 29% reduction innon-disabling strokes (Hart et al.9)), of remaindermoderate:mild ratio =1:2.95 (Lin et al.24)
30-day ischaemic stroke mortality
24% (Hylek et al.21) 16% for INR <2 (62% oftotal), 6% for INR ≥2(Hylek et al.21)
Assumed as for warfarin 15% (Hylek et al.21)
Appendix 1
Table A1.

Improving QualityNHS
Appendix 1
20
Transitionprobabilities
No antithrombotics(baseline)
Warfarin Warfarin andaspirin
Aspirin (See Appendix)
30-day haemorrhagicstroke mortality
Assumed as for warfarin 41% (Hart et al.14) Assumed as for warfarin 15% (Hylek et al.21)
30-day mortality, other intracranialbleeds
Assumed as for warfarin 29% (Hart et al.14) Assumed as for warfarin Assumed as for warfarin
Excess major extracranial bleed (annual)
0 (reference) 0.3% increase relative to no antithrombotics (Hart et al.9)
Hazard ratio 1.53, relative to warfarin alone (Steinberg et al.18)
0.2% increase relative tono antithrombotics (Hart et al.9)
Stroke mortality post30-days (Combined ischaemic and haemorrhagic)
Disabling stroke: HR 14.3, relative to no stroke. Non-disabling stroke: no significant difference in mortality riskrelative to no stroke (De Caterina et al.22)
Non-stroke mortality AF all-cause mortality rate estimated using RR all-cause mortality in AF 1.5 (men). 2.2 (women) (Stewart et al.5) and applied to ONS life tables by year of age, further adjusted to remove stroke mortality (Hylek et al.21, De Caterina et al.22)
Table A1.2: Cost estimates and sources for Markov model
NHS costs Social care costs
Warfarin Annual cost: Medication = £54.75 (BNF), Management = £94.80 (Ali et al.20 Jowett et al.28)adjusted for inflation (PSSRU33). Sensitivity analyses 1 – 3, Management costs: £117.83,£247.18, £285.89 respectively (NICE29)
Aspirin Annual cost: Medication = £6.19 (BNF26)
Warfarin and aspirin
Annual cost: Medication = £60.94 (BNF26), Management = £94.80 (Ali et al.20 Jowett etal.28) adjusted for inflation (PSSRU33)
Fatal stroke £3,312 (Luengo-Fernandez et al.23), adjusted for inflation (PSSRU33)
Disabling stroke First 90-day cost: £26,240 (Luengo-Fernandez et al.23), adjusted for inflation (PSSRU33). Sensitivity analysis 4: ongoing annual costs £3,270 (Luengo-Fernandez et al.23), adjusted for inflation (PSSRU33)
Annual cost: £23,101 (Luengo-Fernandez et al.23), adjusted for inflation (PSSRU33)
Moderate stroke First 90-day cost: £19,212 (Luengo-Fernandez et al.23), adjusted for inflation (PSSRU33). Sensitivity analysis 4: ongoing annual costs £894 (Luengo-Fernandez et al.23), adjusted for inflation (PSSRU33)
Annual cost: £11,527 (Luengo-Fernandez et al.23), adjusted for inflation (PSSRU33)
Mild stroke First 90-day cost: £3,683 (Luengo-Fernandez et al.23), adjusted for inflation (PSSRU33). Sensitivity analysis 4: ongoing annual costs £414 (Luengo-Fernandez et al.23), adjusted for inflation (PSSRU33)
Annual cost: £1,020 (Luengo-Fernandez et al.23), adjusted for inflation (PSSRU33)
Major intracranialbleed (excluding intracerebral)
£2,589 (NHS Reference Costs25, HRGs AA23C-G)
Major extracranialbleed
£1,092 (NHS Reference Costs25 HRGs FZ38G-P)

Improving QualityNHS
Appendix 2
21
Appendix 2
The impact of aspirin monotherapy on stroke risk in AF
1. There is uncertainty regarding the efficacy of aspirin in reducing stroke risk in AF. Meta-analysissuggests that aspirin monotherapy may be associated with a 19% reduction in stroke risk.9 However, thisestimate did not reach statistical significance at the 95% level. Recent NICE guidelines on AF recommendthat aspirin monotherapy should not be offered solely for stroke prevention to people with atrialfibrillation. Recent European Society of Cardiology (ESC) guidelines state that “The evidence for effectivestroke prevention with aspirin in AF is weak, with a potential for harm”.4
2. In this appendix, we provide estimates from the Markov model for the impact of aspirin on stroke andmajor bleed incidence, on QALYs and on NHS costs.
3. The stroke impacts are estimated from the (non-significant) meta-analysis results. Care should be takenin interpreting the aspirin results owing to the uncertainty surrounding the meta-analysis estimate.
4. The rate of intracranial bleeds is estimated at 0.41%.34 No studies were identified which estimated thediscrete rate of intracerebral bleeds in people with AF taking aspirin monotherapy. It was thereforeassumed that 46% of intracranial bleeds are intracerebral, as for warfarin. The rate of excess extracranialbleeds (0.2%) was taken from Hart et al.9
5. Thirty-day ischaemic stroke mortality was estimated at 15%.21 The proportion of disabling strokes wasestimated at 65%, based on meta-analysis findings that disabling strokes are reduced by 13% andnon-disabling strokes by 29%, relative to no treatment.9 The annual cost of aspirin treatment (£6.19) wastaken from BNF.26 Further details of inputs to the Markov model are provided in Appendix 1, Tables A1.1and A1.2.
6. The Markov model indicates that the number of strokes prevented per person treated is lower withaspirin than with warfarin, and the QALY gain is lower, over both a one-year and lifetime perspective.While the cost of treatment is very low, the model suggests that overall NHS costs rise with aspirintreatment, while they fall with warfarin (Table A2.1). The increase in costs arises because of an increase inthe proportion of strokes that are haemorrhagic, an increase in other major bleeds, and an increase in theproportion of disabling strokes. In economic parlance, warfarin dominates aspirin as a therapy for strokeprevention in AF, producing greater health gain and higher net savings.
Table A2.1: Estimated one-year and lifetime stroke, major bleed, QALY and cost impacts per person treated with aspirinmonotherapy, relative to no antithrombotic therapy
7. If it is assumed that prescribing patterns are as in GRASP-AF, it is estimated that in 2012-13 there were279,229 people with CHA2DS2-VASc score ≥2 receiving antiplatelet monotherapy. Table A2.2 sets out estimated stroke, major bleed, QALY and cost impacts on the assumption that all these patients were taking aspirin.
Strokes Bleeds QALYs NHS costs Social care costs
One-year impact -0.015 0.002 0.004 £55.62 -£23.55
Lifetime impact -0.108 0.020 0.339 £563.08 -£212.72

Improving QualityNHS
Appendix 2
22
Table A2.2: Estimated one-year and lifetime stroke, major bleed, QALY and cost impacts for a cohort of 279,229 peopletreated with aspirin monotherapy, relative to no antithrombotic therapy
Strokes Bleeds QALYs NHS costs Social care costs
One-year impact -4,221 636 1,020 £15,530,401 -£6,574,742
Lifetime impact -30,268 5,680 94,572 £157,229,118 -£59,397,707

Improving QualityNHS
References
23
References
Go AS, Hylek EM, Phillips KA, Chang Y, Henault LE, Selby JV, et al. Prevalence of diagnosed atrial fibrillation in1adults: national implications for rhythm management and stroke prevention: the AnTicoagulation and Risk Factorsin Atrial Fibrillation (ATRIA) Study. JAMA : the journal of the American Medical Association. 2001;285(18):2370-5.
Naccarelli GV, Varker H, Lin J, Schulman KL. Increasing prevalence of atrial fibrillation and flutter in the United2States. The American journal of cardiology. 2009;104(11):1534-9.
Majeed A, Moser K, Carroll K. Trends in the prevalence and management of atrial fibrillation in general practice in3England and Wales, 1994-1998: analysis of data from the general practice research database. Heart.2001;86(3):284-8.
Camm AJ, Lip GY, De Caterina R, Savelieva I, Atar D, Hohnloser SH, et al. 2012 focused update of the ESC4Guidelines for the management of atrial fibrillation: an update of the 2010 ESC Guidelines for the management ofatrial fibrillation. Developed with the special contribution of the European Heart Rhythm Association. Europeanheart journal. 2012;33(21):2719-47.
Stewart S, Hart CL, Hole DJ, McMurray JJ. A population-based study of the long-term risks associated with atrial 5fibrillation: 20-year follow-up of the Renfrew/Paisley study. The American journal of medicine.2002;113(5):359-64.
Benjamin EJ, Wolf PA, D'Agostino RB, Silbershatz H, Kannel WB, Levy D. Impact of atrial fibrillation on the risk of6death: the Framingham Heart Study. Circulation. 1998;98(10):946-52.
Atrial fibrillation: The management of atrial fibrillation, NICE Clinical Guideline 180, June 20147http://www.nice.org.uk/nicemedia/live/14573/68045/68045.pdf Last accessed 19/06/14
Annual Mid-year Population Estimates for England and Wales, Mid 2012. Office for National Statistics 20128http://www.ons.gov.uk/ons/publications/re-reference-tables.html?edition=tcm%3A77-319259 Last accessed 28thMay 2014
Hart RG, Pearce LA, Aguilar MI. Meta-analysis: antithrombotic therapy to prevent stroke in patients who have 9nonvalvular atrial fibrillation. Annals of internal medicine. 2007;146(12):857-67.
Gray AM, Clarke PM, Wolstenholme JL, Wordsworth S. Applied Methods of Cost-effectiveness Analysis in Health10Care OUP 2011
Friberg L, Rosenqvist M, Lip GY. Evaluation of risk stratification schemes for ischaemic stroke and bleeding in 18211678 patients with atrial fibrillation: the Swedish Atrial Fibrillation cohort study. European heart journal.2012;33(12):1500-10.
Lip GY, Andreotti F, Fauchier L, Huber K, Hylek E, Knight E, et al. Bleeding risk assessment and management in12atrial fibrillation patients: a position document from the European Heart Rhythm Association, endorsed by the European Society of Cardiology Working Group on Thrombosis. Europace : European pacing, arrhythmias, and cardiac electrophysiology : journal of the working groups on cardiac pacing, arrhythmias, and cardiac cellular electrophysiology of the European Society of Cardiology. 2011;13(5):723-46.
Fang MC, Go AS, Chang Y, Hylek EM, Henault LE, Jensvold NG, et al. Death and disability from warfarin- 13associated intracranial and extracranial hemorrhages. The American journal of medicine. 2007;120(8):700-5.
Hart RG, Diener HC, Yang S, Connolly SJ, Wallentin L, Reilly PA, et al. Intracranial hemorrhage in atrial fibrillation14patients during anticoagulation with warfarin or dabigatran: the RE-LY trial. Stroke; a journal of cerebral circulation. 2012;43(6):1511-7.
Go AS, Hylek EM, Chang Y, Phillips KA, Henault LE, Capra AM, et al. Anticoagulation therapy for stroke 15prevention in atrial fibrillation: how well do randomized trials translate into clinical practice? JAMA: the journal ofthe American Medical Association. 2003;290(20):2685-92.

Improving QualityNHS
References
24
Singer DE, Chang Y, Fang MC, Borowsky LH, Pomernacki NK, Udaltsova N, et al. The net clinical benefit of 16warfarin anticoagulation in atrial fibrillation. Annals of internal medicine. 2009;151(5):297-305.
Pisters R, Lane DA, Nieuwlaat R, de Vos CB, Crijns HJ, Lip GY. A novel user-friendly score (HAS-BLED) to assess171-year risk of major bleeding in patients with atrial fibrillation: the Euro Heart Survey. Chest. 2010Nov;138(5):1093-100. Epub 2010 Mar 18. PubMed PMID: 20299623.
Steinberg BA, Kim S, Piccini JP, Fonarow GC, Lopes RD, Thomas L, et al. Use and associated risks of concomitant18aspirin therapy with oral anticoagulation in patients with atrial fibrillation: insights from the Outcomes Registryfor Better Informed Treatment of Atrial Fibrillation (ORBIT-AF) Registry. Circulation. 2013;128(7):721-8.
Hart RG, Benavente O, Pearce LA. Increased risk of intracranial hemorrhage when aspirin is combined with 19warfarin: A meta-analysis and hypothesis. Cerebrovascular diseases. 1999;9(4):215-7.
Ali A, Bailey C, Abdelhafiz AH. Stroke prophylaxis with warfarin or dabigatran for patients with non-valvular atrial20fibrillation-cost analysis. Age and ageing. 2012;41(5):681-4
Hylek EM, Go AS, Chang Y, Jensvold NG, Henault LE, Selby JV, et al. Effect of intensity of oral anticoagulation on21stroke severity and mortality in atrial fibrillation. The New England journal of medicine. 2003;349(11):1019-26.
De Caterina R, Connolly SJ, Pogue J, Chrolavicius S, Budaj A, Morais J, et al. Mortality predictors and effects of22antithrombotic therapies in atrial fibrillation: insights from ACTIVE-W. European heart journal.2010;31(17):2133-40.
Luengo-Fernandez R, Yiin GS, Gray AM, Rothwell PM. Population-based study of acute- and long-term care costs23after stroke in patients with AF. International journal of stroke : official journal of the International Stroke Society.2013;8(5):308-14.
Lin HJ, Wolf PA, Kelly-Hayes M, Beiser AS, Kase CS, Benjamin EJ, et al. Stroke severity in atrial fibrillation. The24Framingham Study. Stroke; a journal of cerebral circulation. 1996;27(10):1760-4.
NHS Reference Costs 2012-13 https://www.gov.uk/government/publications/nhs-reference-costs-2012-to-201325Last accessed 16th June 2014
British National Formulary 64, September 2012, BMJ Group and Pharmaceutical Press, London 26
Garcia D, Regan S, Crowther M, Hughes RA, Hylek EM. Warfarin maintenance dosing patterns in clinical practice:27implications for safer anticoagulation in the elderly population. Chest. 2005;127(6):2049-56.
Jowett S, Bryan S, Murray E, McCahon D, Raftery J, Hobbs FD, et al. Patient self-management of anticoagulation28therapy: a trial-based cost-effectiveness analysis. British journal of haematology. 2006;134(6):632-9.
Dabigatran etexilate for the prevention of stroke and systemic embolism in atrial fibrillation NICE technology 29appraisal guidance 249, 2012
Berg J, Lindgren P, Nieuwlaat R, Bouin O, Crijns H. Factors determining utility measured with the EQ-5D in 30patients with atrial fibrillation. Quality of life research : an international journal of quality of life aspects of treatment, care and rehabilitation. 2010;19(3):381-90.
Dorman PJ, Waddell F, Slattery J, Dennis M, Sandercock P. Is the EuroQol a valid measure of health-related quality31of life after stroke? Stroke; a journal of cerebral circulation. 1997;28(10):1876-82.
Dolan P, Gudex C, Kind P, Williams A. A Social Tariff for EuroQol: Results from a UK General Population Survey,32Discussion Paper 138, Centre of Health Economics, University of York, 1995
Curtis L. Unit Costs of Health and Social Care, Personal and Social Services Research Unit, 201333http://www.pssru.ac.uk/project-pages/unit-costs/2013/ last accessed 04/07/14
Flaker GC, Eikelboom JW, Shestakovska O, Connolly SJ, Kaatz S, Budaj A, et al. Bleeding during treatment with34aspirin versus apixaban in patients with atrial fibrillation unsuitable for warfarin: the apixaban versus acetylsalicylic acid to prevent stroke in atrial fibrillation patients who have failed or are unsuitable for vitamin Kantagonist treatment (AVERROES) trial. Stroke; a journal of cerebral circulation. 2012;43(12):3291-7





























