Embed Size (px)
Citation preview

ORIGINAL PAPER
Cost of care for colorectal cancer in Ireland: a health care payerperspective
L. Tilson • L. Sharp • C. Usher • C. Walsh • Whyte S • A. O’Ceilleachair •
C. Stuart • B. Mehigan • M. John Kennedy • P. Tappenden • J. Chilcott •
A. Staines • H. Comber • M. Barry
Received: 30 August 2010 / Accepted: 17 May 2011 / Published online: 3 June 2011
� Springer-Verlag 2011
Abstract
Objective Management options for colorectal cancer
have expanded in recent years. We estimated average
lifetime cost of care for colorectal cancer in Ireland in
2008, from the health care payer perspective.
Method A decision tree model was developed in Micro-
soft EXCEL. Site and stage-specific treatment pathways
were constructed from guidelines and validated by expert
clinical opinion. Health care resource use associated with
diagnosis, treatment and follow-up were obtained from the
National Cancer Registry Ireland (n=1,498 cancers diag-
nosed during 2004–2005) and three local hospital databases
(n=155, 142 and 46 cases diagnosed in 2007). Unit costs
for hospitalisation, procedures, laboratory tests and radio-
therapy were derived from DRG costs, hospital finance
departments, clinical opinion and literature review.
Chemotherapy costs were estimated from local hospital
protocols, pharmacy departments and clinical opinion.
Uncertainty was explored using one-way and probabilistic
sensitivity analysis.
Results In 2008, the average (stage weighted) lifetime cost
of managing a case of colorectal cancer was €39,607. Aver-
age costs were 16% higher for rectal (€43,502) than colon
cancer (€37,417). Stage I disease was the least costly
(€23,688) and stage III most costly (€48,835). Diagnostic
work-up and follow-up investigations accounted for 4 and 5%
of total costs, respectively. Cost estimates were most sensi-
tive to recurrence rates and prescribing of biological agents.
Conclusion This study demonstrates the value of using
existing data from national and local databases in con-
tributing to estimating the cost of managing cancer. The
findings illustrate the impact of biological agents on costs
of cancer care and the potential of strategies promoting
earlier diagnosis to reduce health care resource utilisation
and care costs.
Keywords Colorectal cancer � Cost � Health care
resources � Chemotherapy
JEL Classification I10 � I11
Introduction
The costs to the health system associated with the diag-
nosis, treatment and follow-up of colorectal cancer patients
are substantial [1–6]. The average expenditure on cancer
care in Europe in 2004 was estimated at 6.4 per cent of
L. Tilson (&) � C. Usher � C. Walsh � M. Barry
National Centre for Pharmacoeconomics, St James’s Hospital,
Dublin 8, Ireland
e-mail: [email protected]
L. Sharp � A. O’Ceilleachair � H. Comber
National Cancer Registry Ireland, Cork Airport Business Park,
Cork, Ireland
C. Walsh
Department of Statistics, Trinity College Dublin, Dublin, Ireland
W. S � P. Tappenden � J. Chilcott
School for Health and Related Research, University of Sheffield,
Sheffield, UK
C. Stuart � B. Mehigan � M. John Kennedy
St James’s Hospital, Dublin, Ireland
M. John Kennedy
Academic Unit of Clinical and Molecular Oncology,
Trinity College Dublin, Dublin, Ireland
A. Staines
School of Nursing, Dublin City University, Dublin, Ireland
123
Eur J Health Econ (2012) 13:511–524
DOI 10.1007/s10198-011-0325-z

total health care costs [7]. However, expenditure on cancer
care varies greatly within and between countries. Even
though cancer causes a large economic burden, only a few
countries have actually estimated how large these costs
really are. A previous supplement of this journal, which
focused on colorectal cancer and its burden in a number of
OECD countries, highlights the need for detailed country-
specific colorectal cancer costing studies [8, 9].
Each year, over a million new cases of colorectal cancer
are diagnosed worldwide [10]. Around two-thirds of the
incident cases occur in the developed areas of the world,
where colorectal cancer is the third most common cancer in
men and the second most common in women. Incidence
and mortality for colorectal cancer differ significantly
between European countries. Ireland has one of the highest
incidence rates in men and women in Europe. Similar
variation is evident in mortality rates [11]. Within Europe,
only countries in Central and Eastern Europe had a higher
colorectal cancer mortality rate for men than Ireland. The
mortality rate for women ranks in the middle of the
European countries. The demographic changes occurring in
most developed populations mean that the burden of
colorectal cancer is expected to increase dramatically in
coming decades. In Ireland, the number of new cases is
projected to rise by 79% in men and 56% in women
between 1998–2002 and 2020, mainly as a result of pop-
ulation ageing [12]. Survival has been rising over the past
10–15 years, and 5-year relative survival is now around
54% [13].
Surgery remains the cornerstone of colorectal cancer
treatment, and recent years have seen advances in surgical
techniques [14, 15]. Radiotherapy is recommended for
some rectal cancers if the clinical stage is involved, with
trials indicating that preoperative, compared to postopera-
tive, administration may improve local control and result in
lower toxicity and reduced rectal cancer deaths [16, 17].
Co-administration of chemotherapy can improve response
[18, 19]. For colon cancer, adjuvant chemotherapy is rou-
tine for stage III disease and for many patients with
advanced disease [20–23] and might also benefit stage II
patients with poor prognostic features, such as lymph node
involvement [23]. Over the past decade, there has been a
marked increase in the complexity of chemotherapy, for
example, from 5-fluorouracil (5-FU) with or without leu-
covorin to multi-agent regimens containing capecitabine,
irinotecan or oxaliplatin. Second- and third-line options for
treating metastatic disease have been developed [1]. In
addition, biological targeted agents, bevacizumab and
cetuximab, were approved for the treatment of metastatic
disease in 2004 [24]. It seems likely that the advances in
treatment will have had a notable impact on costs, espe-
cially in view of the high acquisition costs of the combined
chemotherapy regimens and biological agents [23].
As highlighted previously in this journal, there is often
poor-quality data on colorectal cancer expenditure [9]. As
well as being a key component of the overall economic
burden associated with colorectal cancer morbidity and
mortality, such data are needed to (a) understand the
magnitude of financial and productive resources that must
be mobilised to effectively care for colorectal cancer
patients and (b) as inputs to cost-effectiveness analyses of
cancer prevention, screening and treatment programs. This
is one of the first studies to estimate treatment costs since
biological therapies came into common usage. It is also the
first study to provide an in-depth description of the cost of
managing colorectal cancer in Ireland from the perspective
of the health care payer.
This study was performed as part of a health technology
assessment to evaluate the cost-effectiveness of a popula-
tion-based colorectal cancer–screening programme in
Ireland [25]. In January 2010, a national population-based
colorectal cancer–screening programme for men and
women in Ireland was approved by the Minister for Health
and Children. Screening is to be introduced for the 55- to
74-year age group on a two yearly cycle using the faecal
immunochemical test (FIT) as the primary screening tool.
The cost estimates that were derived in this study were
used in the evaluation of cost-effectiveness of the screening
programme.
Methods
Costs associated with the diagnosis, treatment and follow-
up of colorectal cancer were estimated. These cost esti-
mates were combined to derive average costs per person of
managing colorectal cancer over a 5-year time horizon. We
chose a 5-year time frame as this is the normal period of
follow-up for colorectal cancer in Ireland. A decision tree
model of colorectal cancer treatment pathways was
constructed. Health care resources for the management of
colorectal cancer were identified from a variety of sources.
Resource use items were valued using Irish unit cost data.
These estimates were used to populate the treatment
pathways. Estimates were produced for colon and rectal
cancer separately and combined, and by stage on diagnosis.
Treatment pathways
We developed separate treatment pathways for each stage
of colon and rectal cancer, based on national data and
international guidelines (Fig. 1) [18, 21, 26–28]. While it
was recognised that some patients may have very indi-
vidualised treatment, these pathways were intended to
represent the treatment course of a ‘‘typical’’ patient with a
particular disease site and stage. The pathways were
512 L. Tilson et al.
123

validated by the Expert Advisory Group that was convened
to provide advice and oversee the health technology
assessment [25]. The multidisciplinary Expert Advisory
Group comprised 22 members, including consultants in
colorectal surgery, gastroenterology, medical oncology and
radiation oncology and colorectal cancer specialist nurses,
from several treatment centres across Ireland [25]. The
group reviewed the pathways and confirmed that they
represent usual care for patients with a particular disease
site and stage in the Irish setting. This was undertaken by
individual assessment and group discussion at a plenary
meeting of the group.
The pathways were implemented as a (static) decision
tree model in Microsoft EXCEL. The cumulative probabil-
ities in each pathway sum to one. A detailed description of
the pathway of the treatment of stage I colon cancer illus-
trates how the treatment cost (€18,613) was derived using
resource use and cost estimates from national and local
databases (Fig. 1. Costs of diagnosis (€1,346) and follow-up
(€3,503) are added to this figure to give a total cost estimate
for stage I colon cancer (€23,462). The pathways for the
other stages of colon cancer and for rectal cancer are pre-
sented (Fig. 2), and the same approach was applied to derive
cost estimates for each stage and cancer site.
Health care resources
Resource use estimates were derived from several sources
including the National Cancer Registry Ireland (NCRI),
local hospital databases and protocols, literature review and
expert clinical opinion. Data were obtained from the NCRI
on all primary invasive colorectal cancers (ICDO2 C18-
C20) diagnosed in Ireland during 2004–2005 (n = 4,268),
by site, stage at diagnosis and treatment received. The
probability of a patient receiving the following therapies,
alone and in combination, was tabulated by site and stage
at diagnosis: (a) local excision; (b) colon/rectal resection;
(c) liver or lung resection; (d) chemotherapy; (e) radio-
therapy; (f) other procedures (e.g. stents, GI bypass)
(Figs. 1, 2). Dates of procedures were used to categorise
chemotherapy and radiotherapy by whether it was deliv-
ered pre- or postoperatively. Details about type, dose and
duration of chemotherapy and radiotherapy, and follow-up
surveillance were not available and were derived from
other sources.
Three university teaching hospitals provided informa-
tion on individual patients seen in 2007 (hospital 1:155
colorectal patients; hospital 2:142 colorectal patients; and
hospital 3:46 rectal patients). These datasets were primarily
used to derive estimates of resource use associated with
diagnosis/work-up, which were subsequently verified by
the expert clinical group. They also included some infor-
mation on radiotherapy and chemotherapy regimens, but
since patient numbers were small, these figures were sup-
plemented and verified by expert clinical opinion.
Diagnosis
It was assumed from expert opinion that 30% of patients
would present at hospital as emergency cases with the
remainder referred to an outpatient clinic via their general
practitioner. All patients would have a CEA test, full blood
count, coagulation and biochemistry. Based on NCRI data,
90% would be biopsied. From literature review, 90%
would have colonoscopy with those who were unfit for
colonoscopy (10%), or in whom the colonoscopy was
incomplete (3% of total) undergoing CT colonography
[25, 29, 30]. All colon cancer patients would have a CT
scan. From local data, 10% of all patients would have a PET
scan. One-third of rectal cancer patients would have rigid
sigmoidoscopy. Rectal cancer patients are also assumed to
undergo CT scans of the thorax, abdomen and pelvis and an
MRI, and 15% would have transrectal ultrasound (TUS).
Surgical resection
Based on NCRI data, an estimated 5% of stage I colon and
rectal cancers would undergo local excision; the remainder
Fig. 1 Treatment pathway and
total cost of stage I colon cancer
treatment
Cost of care for colorectal cancer in Ireland 513
123

of stage I cancers, all stage II and III colon cancers and
[80% of stage II or III rectal cancers would have a
resection. Over half stage IV colon cancers (53%) and 60%
of stage IV rectal cancers were assumed to be inoperable,
and 10% of these were assumed to have a stoma, stent or a
bypass to relieve obstruction or other symptomology. Of
the operable cancers, it was estimated that most (85% of
colon;[87% of rectal) would have a bowel resection only,
with the remainder (15% of colon; 13% of rectal) having
both a bowel resection and a lung or liver resection for
metastatic disease.
Chemotherapy
It was assumed that no stage I rectal cancer patients would
receive chemotherapy. From NCRI data, an estimated 6%
of stage I, 28% of stage II, 58% of stage III and 27% of
stage IV colon cancers and an estimated 21% of stage II,
26% of stage III and 13% of stage IV rectal cancers would
receive adjuvant chemotherapy (without radiotherapy).1
Based on hospital protocols and expert opinion, we
assumed 80% of patients would be given FOLFOX (5-FU,
leucovorin, oxaliplatin) as first-line treatment, with the
remainder prescribed capecitabine (Xeloda�), both for
6 months. From expert opinion, we assumed that 67% with
stage IV disease would receive biological agents with
chemotherapy, with FOLFOX plus bevacizumb (Avastin�)
administered as first-line therapy (for an average of
3 months) and FOLFIRI (5-FU, leucovorin, irinotecan)
with cetuximab as second-line treatment (for 5 months on
average).
Fig. 2 a. Treatment pathways
for stage I-IV colon cancer.
b. Treatment pathways for stage
I-III rectal cancer. c Treatment
pathways for stage IV rectal
cancer
1 The proportions for each site and stage are derived by summing the
probabilities for adjuvant chemotherapy (without radiotherapy) in the
decision trees (Fig. 2). For example: The proportion of Stage II RCpatients that receive adjuvant chemotherapy was estimated asfollows: (0.044 ? 0.129 ? 0.034) = 21%.
514 L. Tilson et al.
123

Radiotherapy
It was assumed that stage I patients would not undergo
radiotherapy. It was estimated, from NCRI data augmented
by expert opinion, that 80% of stage II and III and 27% of
operable stage IV rectal cancers would receive preopera-
tive radiotherapy. Approximately 70% would be given
combined chemoradiation (long-course therapy (i.e. 45–50
Gray in 25 fractions over 5 weeks) with 5-FU infusion
(225 mg/m2 per day administered as a continuous infusion
for 5–6 weeks)), with the remainder receiving long-course
radiotherapy alone. If patients received preoperative
radiotherapy, it was assumed that it would not be given
postoperatively. From NCRI data, it was estimated that
18% of resected stage II and 34% of resected stage III
cancers who did not have preoperative radiotherapy would
receive postoperative long-course radiotherapy.
Recurrence
Data on recurrence were obtained from systematic litera-
ture review of population-based registries or patient series,
since individual clinical series and most trials may not be
generalisable. Six population-based series were identified
[31–36]. From these, it was assumed that stage I cancer
would not recur. The 5-year recurrence rate was assumed to
Fig. 2 continued
Cost of care for colorectal cancer in Ireland 515
123

be 27% for stage II and 56% for stage III colon cancer [33]
and 20 and 36% for stage II and stage III rectal cancer,
respectively [34, 37].The cost of treating recurrence was
assumed to be the same as the cost of managing stage IV
disease, and these costs were included in the overall cost of
managing stage II and III disease.
Follow-up
Follow-up protocols were obtained from three Irish
teaching hospitals and combined based on expert opinion
[38]. Follow-up was assumed to consist of three-monthly
outpatient attendances (including a CEA test) for the first
6 months, followed by 6-monthly attendances for a further
18 months and then annual visits until year 5. It was
assumed that patients would have a CT scan at years 1, 2
and 5 and a colonoscopy at years 1, 3 and 5. Stages I–III
disease would be followed for 5 years, with a proportion of
stage II and III cases dropping out because of recurrence.
Stage IV patients were assumed to be followed up for
15 months (mean survival of stage IV colorectal cancer
patients) [39, 40].
Valuation of resources
Costs associated with diagnosis, hospitalisation, surgery,
radiotherapy, chemotherapy, supportive care, clinician
visits, other health care professional staff costs, laboratory
Fig. 2 continued
516 L. Tilson et al.
123

costs, other ancillary medications and follow-up were
included. Costs were calculated from the perspective of
the health care payer. All costs were adjusted to the year
2008 using the Consumer Price Index for health (Central
Statistics Office www.cso.ie), and any costs derived from
other jurisdictions (e.g. UK) were converted to Euro
using the average annual exchange rate published by the
European Central Bank. Costs of follow-up in years 2–5
post-surgery were discounted at an annual rate of 4%
(the standard discount rate recommended for Ireland)
[41].
Unit cost data for inpatient procedures were obtained
from 2006 diagnosis-related group (DRG) costs provided
by the National Casemix Unit of the Health Service
Executive (HSE) [42] (Table 1). The weighted average
DRG costs were estimated using activity data from the
Casemix Unit. For example, the cost of a rectal resection
was estimated from the weighted average of the cost of
rectal resection with catastrophic complication or comor-
bidity (CCC) (DRG G01A 250 cases, €24,253/case) and
rectal resection without CCC (DRG G01B 590 cases,
€14,682/case) and then inflated to 2008 price year. Unit
costs for diagnostic procedures, laboratory tests and
outpatient appointments were obtained from a University
Teaching Hospital. Cost of radiotherapy was based on a
study by Ploquin and Dunscombe [43] and confirmed by
local expert radiotherapy clinical opinion. The cost of best
supportive care was obtained from a study conducted by
Guest et al. [44].
Full details of the derivation of the costs of chemo-
therapy regimes are available elsewhere [25]. Briefly, the
ingredient cost (excluding VAT), as well as the pharma-
cist’s and pharmacy technician’s time to compound the
chemotherapy, was obtained from a University Teaching
Hospital (Table 2). Drug acquisition costs were based on
an individual with a body surface area of 1.75 m2 or a body
weight of 75 kg, with allowance for wastage. Costs of
ancillary medications (e.g. anti-emetics) were obtained
from MIMS Ireland [45]. Staff costs for nursing and
pharmacy staff as well as clinical consultants were
estimated from the Department of Health and Children
consolidated salary scales. Monitoring costs (e.g. labora-
tory tests) and hospital visits were also included in the cost
estimates for chemotherapy. Patients receiving oral thera-
pies were assumed to attend one outpatient appointment
each cycle.
Table 1 Unit cost data
included in the model (€ 2008)
CEA carcinoembryonic antigen,
CT computed tomography, DRGdiagnostic-related group, 5FU5-fluorouracil, GIgastrointestinal, HSE Health
Service Executive, MRImagnetic resonance imaging,
PET positron emission
tomography, PHI Private Health
Insurer, TUS transrectal
ultrasound, UTH University
Teaching Hospital
Description of test/treatment/procedure (source) Unit cost
Accident and emergency visit (HSE) € 334
Outpatient visit (HSE) € 169
Biopsy/histopathology (PHI) € 130
CT scan (UTH) € 106
CT thorax, abdomen and pelvis (UTH) € 119
Colonoscopy (DRG G44C, G44O and G43O) € 649
CT colonography (PHI) € 550
Rigid sigmoidoscopy [DRG G11S (daycase)] € 903
MRI (pelvis) (HSE) € 467
TUS (PHI) € 160
PET scan (UTH/PHI/expert opinion) € 1,700
CEA test (UTH) € 13
Full blood count (UTH) € 18
Coagulation (UTH) € 52
Biochemistry (UTH) € 59
Preoperative/postoperative radiotherapy (Ploquin and Dunscombe [44]/expert opinion) € 5,250
Chemotherapy in combination with radiotherapy (5FU infusion) (UTH) € 5,580
Chemotherapy post-radiotherapy (5FU infusion ? folinic acid) (UTH) € 5,000
Rectal resection (DRG G01A/B) € 18,933
Colon resection (DRG G02A/B) € 17,974
GI stoma/stent/bypass (DRG G05A/B/S and G0511A/B/S) € 2,887
Lung resection (DRG E01A/B) € 16,744
Liver resection (DRG H01A/B) € 22,959
Minor GI procedure (local excision) (DRG G05A/B/S) € 9,057
Best supportive care (Guest et al. [45]) € 3,290
Cost of care for colorectal cancer in Ireland 517
123

Estimation of total costs per patient of managing
colorectal cancer
Total costs of colon and rectal cancer by stage were cal-
culated. The costs of diagnosis, treatment and follow-up
were estimated separately and summed to give a total cost
for each stage. Total costs of diagnosis for colon and rectal
cancer were estimated by multiplying the unit cost of each
resource item (e.g. MRI scan, biopsy) by the probability of
occurrence.
Total costs of treatment were estimated by multiplying
the unit costs by the probabilities in each of the treatment
pathways (Fig. 2). A detailed description of the method
used to estimate total cost of treating stage I colon cancer is
illustrated in Fig. 1. The cost of each resource item is
weighted by its probability of occurrence, and a total
treatment cost is derived. Costs of follow-up were esti-
mated by multiplying the unit cost of each resource item
(e.g. colonoscopy, CEA test) by the probability of
occurrence.
Table 2 Cost of chemotherapy regimens (2008)
Description Cost of 1 cycle Duration of treatment Total cost
Pre-operative chemo-radiation
5FU infusion in combination with radiotherapy € 5,580 6 weeks € 5,580
Radiotherapy € 5,250 N/A € 5,250
Total cost € 10,830
Postoperative chemoradiation
5FU infusion in combination with radiotherapy € 5,580 6 weeks € 5,580
Chemotherapy post-radiotherapy (5FU infusion ? folinic acid) € 5,000 3 9 6 week cycles € 15,000
Radiotherapy € 5,250 N/A € 5,250
Total cost € 25,830
Adjuvant chemotherapy
FOLFOX (80%) € 3,743 6 months € 17,966
Capecitabine (20%) € 885 6 months € 1,062
Total cost € 19,028
Chemo- and biological therapy for metastatic disease
FOLFOX ? bevacizumab (100%) € 6,085 3 months € 18,255
FOLFIRI ? cetuximab (100%) € 11,778 5 months € 59,265
Total costa € 77,520
5FU 5-fluorouracila Three months FOLFOX/bevacizumab and 5 months FOLFIRI/cetuximab
Table 3 Summary of costsa of managing colorectal cancerb by site, stage and disease phase (€ 2008), base-case estimates and 95% confidence
intervals (CI) from probabilistic sensitivity analysis
Site Stage I Stage II Stage III Stage IV Overall stage
weighted cost
Colon cancer
(95% CI)
€ 23,462
(€22,818–€24,459)
€ 35,059
(€25,904–€51,227)
€ 48,186
(€36,469–€67,970)
€ 31,744
(€26,966–€39,872)
€37,417
(€29,871–€50,618)
Rectal cancer
(95% CI)
€ 24,089
(€16,284–€38,492)
€ 40,950
(€32,754–€55,430)
€ 49,987
(€41,233–€66,492)
€ 45,237
(€40,292–€53,196)
€43,502
(€36,872–€55,402)
Colorectal cancer
(95% CI)
€ 23,688
(€20,900–€28,590)
€ 37,180
(€30,285–€48,032)
€ 48,835
(€40,548–€62,582)
€ 36,602
(€32,774–€42,962)
€39,607
(€33,843–48,980)
Treatment phase Stage I Stage II Stage III Stage IV Overall stage weighted cost
Diagnosis € 1,634 € 1,634 € 1,634 € 1,634 € 1,634
Treatment € 18,550 € 32,900 € 45,407 € 33,656 € 35,918
Follow-up € 3,503 € 2,646 € 1,794 € 1,311 € 2,055
a Future costs discounted at 4% per annumb All cancers that are not detected through screening; assuming 64% of cancers arise in the colon and 36% in the rectum and 11% are stage I,
25% stage II, 35% stage III and 29% stage IV
518 L. Tilson et al.
123

Total costs including diagnosis, treatment and follow-up
were calculated. For stage II and III cancers, the cost of
recurrence was also included.
Sensitivity analysis
One-way and probabilistic sensitivity analyses were
undertaken to explore the impact of parameter uncertainty
on the total cost estimates. The parameters included in the
one-way sensitivity analysis were those that were consid-
ered to be associated with most uncertainty, or likely to be
major cost drivers. Costs of chemotherapy and biological
agents were varied by 20% around the base-case value. The
proportion of eligible patients receiving a biological agent
was assumed to be 0, 20 or 80%, compared with 67% in the
base-case. The duration of treatment with FOLFIRI and
cetuximab was assumed to be 3 or 8 months, compared
with 5 months in the base-case. The recurrence rates for
stage II and stage III disease were assumed to be 20%
higher or lower than the base-case values. Finally, all unit
costs were simultaneously varied by 20% around their
base-case values.
Probabilistic sensitivity analysis (PSA) was conducted
by running the model with 1,000 different parameter sets
and calculating the cost estimates for each simulation. In
each simulation, the value for each parameter was sampled
from its probability distribution. The choice of probability
distribution was based on consideration of the properties of
the parameters and the data informing them. The proba-
bilities associated with each branch in the treatment path-
ways were modelled using Beta distributions, where the
parameters of the Beta distributions were chosen according
to the number of individuals observed in each pathway.
The total sample size was 4268, which corresponds to the
data from the NCRI database. Direct medical costs were
specified as log-normal distributions as they are con-
strained to be positive, continuous and highly skewed. For
the DRG costs, the coefficient of variation used to derive
the log-normal distribution was derived from the sample
size on which the DRGs were based. The proportion of
rectal and colon cancers and stage distributions were also
based on national data from the NCRI. Uncertainty in
recurrence rates was accounted for using Beta distributions,
which were parameterised with the sample size from the
relevant studies [33, 34]. Confidence intervals for the dif-
ferent sites and stages, as well as the average (stage
weighted) cost of colorectal cancer, were derived from the
probabilistic sensitivity analysis.
Results
Estimated costs per person of managing colorectal
cancer
Costs by stage at diagnosis
The estimated costs per person over a 5-year period varied
by stage (Table 3). Stage I disease was least costly to
manage and stage III disease most costly. Managing a case
of stage IV disease costs, on average, 25% less than man-
aging a case diagnosed at stage III. For all stages, the cost of
managing rectal cancer exceeded that for managing colon
cancer. The greatest difference was between stage IV dis-
ease (43% higher for rectal than colon for stage IV disease).
Costs by disease phase
The cost associated with diagnosis, treatment and follow-
up accounted for an average of 4, 91 and 5% of the total
costs, respectively (Table 3). Costs of diagnosis, treatment
and follow-up were estimated to be higher for rectal than
colon cancers. Costs of treatment and follow-up varied by
site and stage of disease. Costs of treatment accounted for
78% of stage I costs, 88% of stage II, 93% of stage III and
92% of stage IV disease. They were highest for stage III
cases. Follow-up costs, by contrast, were highest for stage I
cases.
Sensitivity analysis
The 95% confidence interval for the average (stage
weighted) cost per person of managing a case of colorectal
cancer over a 5-year period (base-case: €39,607) was
Table 4 Average costsa of managing colorectal cancerb by stage at diagnosis and proportion of eligible patients receiving biological agents
Stage at diagnosisc Base-case 0% treated with biological agents 20% treated with biological agents 80% treated with biological agents
Stage II €37,180 €34,295 €35,156 €37,739
Stage III €48,835 €43,249 €44,916 €49,918
Stage IV €36,602 €24,040 €27,790 €39,039
a Future costs discounted at 4% per annumb assumed 64% of cases are in the colon and 36% in the rectumc Stage I costs were invariant because no patients received biological agents
Cost of care for colorectal cancer in Ireland 519
123
estimated from the probabilistic sensitivity analysis and
ranged from €33,300 to €49,900 (Table 3).
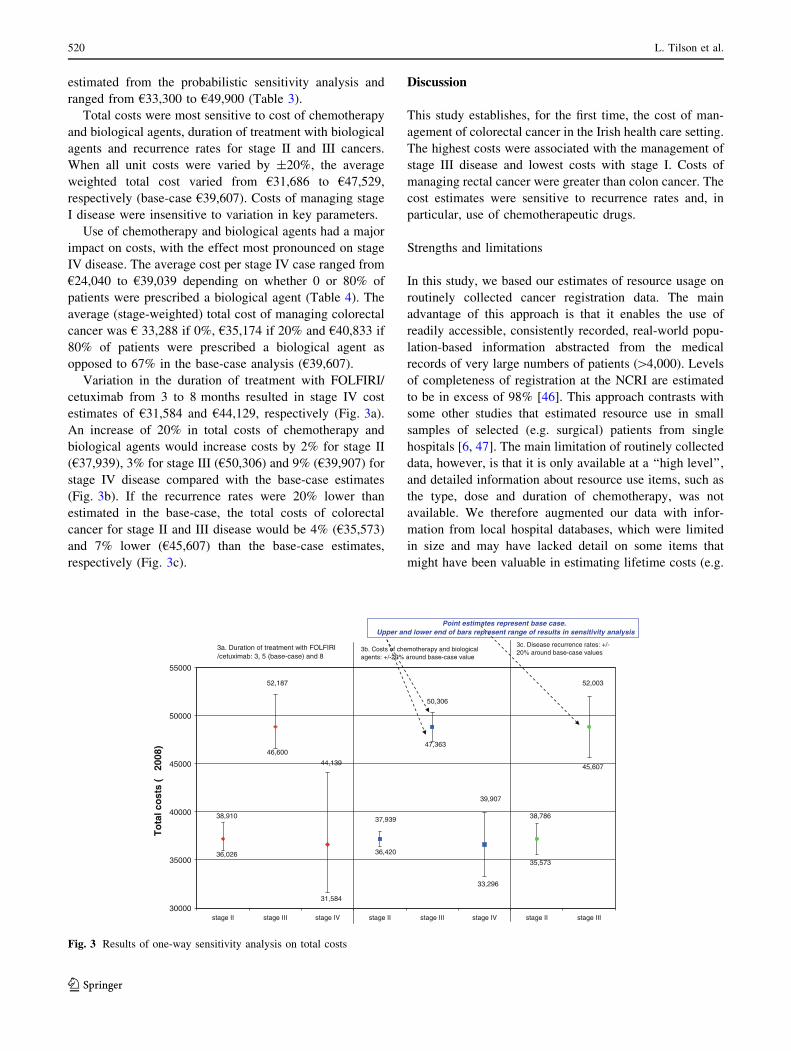
Total costs were most sensitive to cost of chemotherapy
and biological agents, duration of treatment with biological
agents and recurrence rates for stage II and III cancers.
When all unit costs were varied by ±20%, the average
weighted total cost varied from €31,686 to €47,529,
respectively (base-case €39,607). Costs of managing stage
I disease were insensitive to variation in key parameters.
Use of chemotherapy and biological agents had a major
impact on costs, with the effect most pronounced on stage
IV disease. The average cost per stage IV case ranged from
€24,040 to €39,039 depending on whether 0 or 80% of
patients were prescribed a biological agent (Table 4). The
average (stage-weighted) total cost of managing colorectal
cancer was € 33,288 if 0%, €35,174 if 20% and €40,833 if
80% of patients were prescribed a biological agent as
opposed to 67% in the base-case analysis (€39,607).
Variation in the duration of treatment with FOLFIRI/
cetuximab from 3 to 8 months resulted in stage IV cost
estimates of €31,584 and €44,129, respectively (Fig. 3a).
An increase of 20% in total costs of chemotherapy and
biological agents would increase costs by 2% for stage II
(€37,939), 3% for stage III (€50,306) and 9% (€39,907) for
stage IV disease compared with the base-case estimates
(Fig. 3b). If the recurrence rates were 20% lower than
estimated in the base-case, the total costs of colorectal
cancer for stage II and III disease would be 4% (€35,573)
and 7% lower (€45,607) than the base-case estimates,
respectively (Fig. 3c).
Discussion
This study establishes, for the first time, the cost of man-
agement of colorectal cancer in the Irish health care setting.
The highest costs were associated with the management of
stage III disease and lowest costs with stage I. Costs of
managing rectal cancer were greater than colon cancer. The
cost estimates were sensitive to recurrence rates and, in
particular, use of chemotherapeutic drugs.
Strengths and limitations
In this study, we based our estimates of resource usage on
routinely collected cancer registration data. The main
advantage of this approach is that it enables the use of
readily accessible, consistently recorded, real-world popu-
lation-based information abstracted from the medical
records of very large numbers of patients ([4,000). Levels
of completeness of registration at the NCRI are estimated
to be in excess of 98% [46]. This approach contrasts with
some other studies that estimated resource use in small
samples of selected (e.g. surgical) patients from single
hospitals [6, 47]. The main limitation of routinely collected
data, however, is that it is only available at a ‘‘high level’’,
and detailed information about resource use items, such as
the type, dose and duration of chemotherapy, was not
available. We therefore augmented our data with infor-
mation from local hospital databases, which were limited
in size and may have lacked detail on some items that
might have been valuable in estimating lifetime costs (e.g.
30000
35000
40000
45000
50000
55000
stage II stage III stage IV stage II stage III stage IV stage II stage III
To
tal c
ost
s (€
200
8)
3a. Duration of treatment with FOLFIRI /cetuximab: 3, 5 (base-case) and 8
3b. Costs of chemotherapy and biological agents: +/-20% around base-case value
3c. Disease recurrence rates: +/-20% around base-case values
€ 38,910 € 37,939
€ 36,026
€ 47,363
€ 50,306
€ 31,584
€ 44,139
€ 46,600
€ 52,187
€ 38,786
€ 45,607
€ 52,003
€ 33,296
€ 39,907
€ 36,420
€ 35,573
Point estimates represent base case. Upper and lower end of bars represent range of results in sensitivity analysis
Fig. 3 Results of one-way sensitivity analysis on total costs
520 L. Tilson et al.
123

adverse effects, such as line complications). Where data
were lacking, we obtained resource use estimates from
literature review and expert opinion including practicing
colorectal surgeons, gastroenterologists, medical and radi-
ation oncologists, and oncology nurses from several large
hospitals across Ireland. Estimating resource use accurately
is a challenge for all cost-of-illness studies. Ideally, data
should be collected prospectively from a large and repre-
sentative sample of patients, but this is not always possible.
Frequently, investigators have to strike a balance between
collecting very detailed data on a small number of patients
and using less detailed data on a very large numbers of
patients.
This study was undertaken from the health care payer
perspective, consequently direct non-medical costs, such as
patient transport costs associated with treatment and lost
productivity from time off work, were not included. In
Ireland, 45% of breast, lung and prostate cancer patients
have been shown to incur out-of-pocket expenses for see-
ing consultants, 72% incurred travel costs associated with
treatment appointments, and 29 and 39% paid for
prescription or over-the-counter supportive medications,
respectively [48]. Moreover, most cancer patients are
absent from work during treatment [48–50]. Therefore, our
cost estimates for the management of colorectal cancer are
conservative.
International comparisons
In the past 15 years, several studies have reported stage-
specific costs of colorectal cancer treatment [4, 6, 39, 47].
In addition to these, Jansman et al. [1] reviewed studies
relating to North America and Europe from 1996 to 2006.
It is difficult to compare overall costs between studies
because of differences in cost perspective, type of costs
included, length of follow-up and whether disease recur-
rence and/or follow-up surveillance was included.
Furthermore, diagnostic and treatment pathways differ
between health care settings and have changed over time
[9]. As an illustration of the effect of the latter, a US study
(2006) suggested that lifetime costs of treatment of meta-
static colorectal cancer were close to $100,000 [51], which
reflects at least a doubling of the costs compared with
studies performed during the 1990s [2].
Our observation that the costs for rectal cancer are 16%
higher than those for colon cancer is consistent with find-
ings reported from three other studies from the United
States, Switzerland and France [3, 6, 52]. This is likely to
be mainly due to (chemo)radiotherapy for rectal cancer
patients. Consistent with studies based on US SEER and
Medicare data [52, 53], we found that costs were highest
for patients with stage III disease. This is probably because
the risk of recurrence is greatest for these patients, so the
total management cost includes initial treatment costs plus,
for a proportion, costs of treating recurrent disease. Our
overall costs estimates are somewhat higher than those
reported in a 2008 French study (mean cost of €24,966 for
first year) [3], although the difference was less for stage I
and IV disease than for stages II and III. Unlike the current
study, the French study did not include costs of recurrence,
which was a notable component of our estimated costs for
stage II and III tumours. Similar issues pertain when our
estimates are compared with those based on an Australian
study [19], where Australian estimates were limited to
costs in the first year post-diagnosis. Costs in Ireland were
more than double those estimated for England (£8,300,
£12,441, £19,076 and £11,946 for stages I–IV, respec-
tively, based on 2004 cost data, but these figures related to
individuals diagnosed several years ago [39, 40]. A recent
small study in Switzerland estimated that the cost of
treatment was €32,718 (US$40,230) for rectal cancer and
€26,910 (US$33,079) for colon cancer, lower than in the
current study, but these figures also relate to patients
diagnosed over a decade ago [6].
Chemotherapy and biological agents
Significant advances have been made in colorectal cancer
chemotherapy over the past decade. Oral analogues of
fluorouracil (capecitabine) as an alternative to intravenous
5-FU/folinic acid, for example, have led to less costly
delivery. In addition, in European countries, rates of util-
isation of chemotherapy in colorectal cancer have
increased substantially over time [54, 55]. In Ireland, in
1994, 20% of patients received chemotherapy rising to
more than 35% of colon cancer patients and almost 50% of
rectal cancer patients by 2002 [56]. Both of these trends
have increased the costs of treatment substantially over the
past decade and provide another explanation for the higher
treatment costs in our study than in some older European
studies.
Targeted biological therapies have been associated with
improved outcomes for patients with metastatic disease
[24]. There appears to be a wide variation in prescribing
and access to such treatments across Europe [9] and
regional differences within some countries. The costs of
these regimes are a concern for health care providers.
Schrag (2004) pointed out that the acquisition costs of
5-FU, with folinic acid, were $US63 (2004 prices) for
8 weeks of treatment, compared with more than $30,000
for 8 weeks of treatment with combinations of irinotecan,
oxaliplatin, bevacizumab or cetuximab [57]. The current
study is one of the first to estimate treatment costs since
biological therapies came into common usage, and this is
another reason why our costs exceed most other European
studies.
Cost of care for colorectal cancer in Ireland 521
123

It is now recommended that cetuximab should be pre-
scribed for a particular subgroup of patients based on the
results of the Kirsten Rat Sarcoma (KRAS) mutation test
[58]. This measure could help to reduce the costs of
treatment with biological agents by targeting treatment to
those most likely to respond. On the other hand, more
biological agents are becoming available for colorectal
cancer; panitumumab for example was approved in 2007.
In addition, recent research suggests that biological agents
might be effective in patient subgroups who would previ-
ously have had limited treatment options (e.g. older
patients with metastatic disease considered unsuitable for
first-line combined chemotherapy [59]). If confirmed, these
expensive treatments will likely be disseminated more
widely. Thus, it seems likely that in the foreseeable future,
treatment costs will continue to rise.
Implications
Around half of colorectal cancers diagnosed in Ireland are
stage III or IV at diagnosis, and similar distributions have
been reported elsewhere in Europe [9]. Survival is highly
dependent on stage. The substantially lower costs of
treating stage I and II disease highlights the potential of
strategies for detecting disease at an earlier stage to reduce
health care resource utilisation. In January 2010, the
implementation of a national population-based colorectal
cancer–screening programme in Ireland was announced.
Screening will be introduced for the 55- to 74-year age
group on a two yearly cycle using the faecal immuno-
chemical test (FIT) as the primary screening tool. The costs
derived in this paper fed into a health technology assess-
ment which showed that FIT-based screening had the
potential to deliver a substantial change in the stage
distribution of cases diagnosed in the population and would
be considered a highly cost-effective health care interven-
tion [25]. Thus, screening (and perhaps also other strategies
to promote early presentation and diagnosis) provides one
way to control the ever-increasing costs of cancer care.
Conclusion
This study demonstrates the value of using existing data
from national and local databases in contributing to
estimating the costs of managing cancer. Our high cost
estimates illustrate the major impact that newer chemo-
therapeutic regimes, incorporating biological agents, has
had on the cost of cancer care. The observed lower costs of
treating early-stage disease highlights the potential to
reduce health care resource utilisation and costs of cancer
care by implementing strategies to detect colorectal cancer
at earlier stages.
Acknowledgments We are grateful to the Expert Advisory Group,
HTA Directorate and Board of the Health Information and Quality
Authority for their input into this study. The views expressed are not
necessarily those of the Health Information and Quality Authority.
We are particularly grateful to those individuals who provided data.
We would also like to thank numerous individuals for helpful dis-
cussions and input; these individuals are listed in the full HTA report
(available at: www.hiqa.ie) [25]. This study was funded by the Health
Information and Quality Authority and the Health Research Board.
The authors have no conflicts of interest to declare.
References
1. Jansman, F., Postma, M., Brouwers, J.: Cost considerations in the
treatment of colorectal cancer. Pharmacoeconomics 25, 537–562
(2007)
2. Brown, M., Riley, G., Potosky, A., Etzioni, R.: Obtaining long-
term disease specific costs of care: application to medicare en-
rollees diagnosed with colorectal cancer. Med. Care 37,
1249–1259 (1999)
3. Clerc, L., Joosts, V., Lejeune, C., et al.: Cost of care of colorectal
cancers according to health care patterns and stage at diagnosis in
France. Eur J Health Econ 9, 361–367 (2008)
4. Warren, J., Yabroff, K., Meekins, A., Topor, M., Lamont, E.,
Brown, M.: Evaluation of trends in the cost of initial cancer
treatment. J. Natl Cancer Inst. 100, 888–897 (2008)
5. Benson, A.: Epidemiology, disease progression, and economic
burden of colorectal cancer. J Manag Care Pharm 13, S5–S18
(2007)
6. Delco, F., Egger, R., Bauerfeind, P., Beglinger, C.: Hospital
health care resource utilisation and costs of colorectal cancer
during the first 3-year period following diagnosis in Switzerland.
Aliment. Pharmacol. Ther. 21, 615–622 (2005)
7. Jonnson, B., Wilking, N.: A global comparison regarding patient
access to cancer drugs. Ann. Oncol. 18(Suppl 3), 1–77 (2007)
8. Kanavos, P., Schurer, W.: The burden of colorectal cancer: pre-
vention, treatment and quality of services. Eur J Health Econ
10(Suppl 1), S1–S3 (2010)
9. Kanavos, P., Schurer, W.: The dynamics of colorectal cancer
management in 17 countries. Eur J Health Econ 10(Suppl 1),
S115–S129 (2010)
10. Parkin, D.M., Bray, F., Pisani, P.: Global cancer statistics, 2002.
CA Cancer J Clin 55, 74–108 (2005)
11. International Agency for Research on Cancer. Colorectal cancer
incidence and mortality worldwide in 2008 (http://globocan.iarc.
fr/factsheets/cancers/colorectal.asp), 2008. Accessed Jan 2011
12. National Cancer Registry. Trends in Irish cancer incidence
1994–2002, with projections to 2020. Report of the National
Cancer Registry, Cork, Ireland (http://www.ncri.ie), 2006.
Accessed April 2010
13. Verdecchia, A., Guzzinati, S., Francisci, S., et al.: EUROCARE
working group survival trends in European cancer patients
diagnosed from 1988 to 1999. Eur. J. Cancer 45, 1042–1066
(2009)
14. Kuhry, E., Schwenk, W., Gaupset, R., Romild, U., Bonjer, J.:
Long-term outcome of laparoscopic surgery for colorectal cancer:
a cochrane systematic review of randomised controlled trials.
Cancer Treat. Rev. 34, 498–504 (2008)
15. Salz, T., Sander, R.S.: The effect of hospital and surgeon volume
on outcomes for rectal cancer surgery. Clin Gastroenterol Hepatol
6, 1185–1193 (2008)
16. Colorectal Cancer Collaborative Group: Adjuvant radiotherapy
for rectal cancer: a systematic overview of 8, 507 patients from
22 randomised trials. Lancet 358, 1291–1304 (2001)
522 L. Tilson et al.
123

17. Sauer, R., Becker, H., Hohenberger, W., et al.: Preoperative
versus postoperative chemoradiotherapy for rectal cancer.
N. Engl. J. Med. 351, 1731–1740 (2004)
18. Scottish Intercollegiate Guidelines Network (SIGN). Manage-
ment of colorectal cancer. A national clinical guideline. No.67
(http://www.sign.ac.uk/guidelines/fulltext/67/index.html), 2003.
Accessed March 2010
19. Australian Cancer Network Colorectal Cancer Guidelines Revi-
sion Committee: Guidelines for the prevention, early detection
and management of colorectal cancer, 2nd edn. The Cancer
Council Australia and Australian Cancer Network, Sydney (2005)
20. National Institute for Health and Clinical Excellence. Guidance
on the use of capecitabine and tegafur with uracil for metastatic
colorectal cancer. NICE Technology Appraisal 61 (http://www.
nice.org.uk), 2003. Accessed March 2010
21. National Institute for Health and Clinical Excellence. Irinotecan,
oxaliplatin and raltitrexed for the treatment of advanced colo-
rectal cancer. Review of technology appraisal 33.Technology
Appraisal 93 (http://www.nice.org.uk), 2005. Accessed March
2010
22. Gravalos, C., Garcia-Escobar, I., Garcia-Alfonso, P., Cassinello,
J., Malon, D., Carrato, A.: Adjuvant chemotherapy for stages II,
III and IV of colon cancer. Clin. Transl. Oncol. 11, 526–533
(2009)
23. Andre, T., Sargent, D., Tabernero, J., et al.: Current issues in
adjuvant treatment of stage II colon cancer. Ann. Surg. Oncol. 13,
887–898 (2006)
24. Rajpal, S., Venook, A.P.: Targeted therapy in colorectal cancer.
Clin Adv Hematol Oncol 4, 124–132 (2006)
25. Health Information and Quality Authority. A health technology
assessment of a population-based colorectal cancer screening
programme in Ireland (http://www.hiqa.ie), 2009. Accessed April
2010
26. National Comprehensive Cancer Network. Rectal cancer clinical
practice guidelines in oncology (Version 1)(2006b) (http://www.
nccn.org), Accessed April 2010
27. National Comprehensive Cancer Network. Colon cancer Clinical
Practice Guidelines in Oncology (Version 1)(2006a) (http://www.
nccn.org), Accessed March 2010
28. Association of Coloproctology of Great Britain and Ireland:
Guidelines for the management of colorectal cancer. 3rd Edn.
(2007) (http://www.acpgbi.org.uk), Accessed April 2010
29. Segnan, N., Senore, C., Andreoni, B., et al.: SCORE 2 Working
Group-Italy. Baseline findings of the Italian multicenter ran-
domised controlled trial of ‘‘once-only sigmoidoscopy’’. J. Natl
Cancer Inst. 94, 1763–1772 (2005)
30. Shah, H., Paszat, L., Saskin, R., Stukel, T., Rabeneck, L.: Factors
associated with incomplete colonoscopy: a population-based
study. Gastroenterology 132, 2297–2303 (2007)
31. Di Gregorio, C., Benatti, P., Losi, L., et al.: Incidence and sur-
vival of patients with Dukes’ A (stages T1 and T2) colorectal
carcinoma: a 15-year population-based study. Int. J. Colorectal
Dis. 20, 147–154 (2005)
32. Kapiteijn, E., Marijnen, C.A., Colenbrander, A.C., et al.: Local
recurrence in patients with rectal cancer diagnosed between 1988
and 1992: A population-based study in the west Netherlands. Eur.
J. Surg. Oncol. 24, 528–535 (1998)
33. Manfredi, S., Bouvier, A., Lepage, C., Hatem, C., Dancourt, V.,
Faivre, J.: Incidence and patterns of recurrence after resection for
cure of colonic cancer in a well defined population. Br. J. Surg.
93, 1115–1122 (2006)
34. Pahlman, L., Bohe, M., Cedermark, B., et al.: The Swedish rectal
cancer registry. Br. J. Surg. 94, 1285–1292 (2007)
35. Sjovall, A., Granath, F., Cedermark, B., Glimelius, B., Holm, T.:
Loco-regional recurrence from colon cancer: A population-based
study. Ann. Surg. Oncol. 14, 432–440 (2007)
36. Wibe, A., Carlsen, E., Dahl, O., et al.: Nationwide quality
assurance of rectal cancer treatment. Colorectal Dis 8, 224–229
(2006)
37. Heriot, A., Kumar, D.: Rectal cancer recurrence: factors and
mechanisms. Colorectal Dis 2, 126–136 (2000)
38. de Zeeuw, N., Keane, F., Neary, P.: Nurse-led protocol driven
colorectal cancer follow-up clinic. Mod Med Irish J Clin Med 37,
16–19 (2007)
39. Tappenden P, Eggington S, Nixon R, Chilcott J, Sakai H, Karnon
J.: Colorectal cancer screening options appraisal: cost-effective-
ness, cost-utility and resource impact of alternative screening
options for colorectal cancer. Report to the English Bowel Cancer
Working Group (2004)
40. Tappenden, P., Chilcott, J., Eggington, S., Sakai, H., Karnon, J.,
Patnick, J.: Option appraisal of population-based colorectal can-
cer screening programmes in England. Gut 56, 677–684 (2007)
41. Health Information and Quality Authority. Draft guidelines for
the economic evaluation of health technologies in Ireland
(http://www.hiqa.ie/media/pdfs/Draft_economic_guidelines_
consultation_0710.pdf), 2010. Accessed August 2010
42. Health Service Executive (HSE) Casemix Unit: Ready reckoner
of acute hospital inpatient activity and costs (summarised by
DRG) relating to 2006 costs and activity. Annual Report Part 3.
(2008)
43. Ploquin, N., Dunscombe, P.: The cost of radiation therapy.
Radiother. Oncol. 86, 217–223 (2008)
44. Guest, J., Ruiz, F., Greener, M., Trotman, I.: Palliative care
treatment patterns and associated costs of healthcare resource use
for specific advanced cancer patients in the UK. Eur J Cancer
Care 15, 65–73 (2006)
45. Monthly Index of Medical Specialities (MIMS): Ireland. (August
2008)
46. National Cancer Registry. Cancer in Ireland, 1994 to 1998:
incidence, mortality, treatment and survival. Report of the
National Cancer Registry, Cork, Ireland (http://www.ncri.ie),
2001. Accessed April 2010
47. Neymark, N., Adriaenssen, I.: The costs of managing patients
with advanced colorectal cancer in 10 different European centres.
Eur. J. Cancer 35, 1789–1795 (1999)
48. Timmons, A., Sharp, L., Carsin, A.E., et al.: The cost of having
cancer: a survey of patients with cancer in Ireland. J. Epidemiol.
Community Health 63(Suppl 2), 46 (2009)
49. Drolet, M., Maunsell, E., Mondor, M., et al.: Work absence after
breast cancer diagnosis: a population-based study. CMAJ 173,
765–771 (2005)
50. Bradley, C.J., Oberst, K., Schenk, M.: Absenteeism from work:
the experience of employed breast and prostate cancer patients in
the months following diagnosis. Psychooncology 15, 739–747
(2006)
51. Paramore, L., Thomas, S., Knopf, K., et al.: Estimating costs of
care for patients with newly diagnosed metastatic colorectal
cancer. Clin Colorectal Cancer 6, 52–58 (2006)
52. Fireman, B.H., Quesenberry, C.P., Somkin, C.P., et al.: Costs of
care for cancer in a health maintenance organisation. Health Care
Financ Rev 18, 51–76 (1997)
53. Ramsey, S.D., Berry, K., Etzioni, R.: Lifetime cancer-attributable
cost of care for long-term survivors of colorectal cancer. Am.
J. Gastroenterol. 97, 440–445 (2002)
54. Bouhier, K., Maurel, J., Lefevre, H., Bouin, M., Asrsene, D.,
Launoy, G.: Changing practices for diagnosis and treatment of
colorectal cancer in Calvados: 1990–1999. Gastroenterol Clin
Biol 28, 371–376 (2004)
55. Van Steenbergen LN, Elferink MA, Krijnen P, et al.: Improved
survival of colon cancer due to improved treatment and detection:
a nationwide population-based study in The Netherlands
1989–2006. Ann Oncol. 2010 May 3 [Epub ahead of print]
Cost of care for colorectal cancer in Ireland 523
123
56. Carsin, A.E., Sharp, L., Cronin-Fenton, D., O’Ceilleachair, A.,
Comber, H.: Inequity in colorectal cancer treatment and out-
comes: a population-based study. Br. J. Cancer 99, 266–274
(2008)
57. Schrag, D.: The price tag on progress: chemotherapy for colo-
rectal cancer. NEJM 351, 317–319 (2004)
58. Patil, D., Fraser, C., Plesec, T.: KRAS testing and its importance
in colorectal cancer. Curr Oncol Rep 12, 160–167 (2010)
59. Feliu, J., Safont, M.J., Salud, A., Losa, F., Garcia-Giron, C.,
et al.: Capecitabine and bevacizumab as first-line treatment in
elderly patients with metastatic colorectal cancer. Br. J. Cancer
102, 1468–1473 (2010)
524 L. Tilson et al.
123





























